Embed Size (px)
Citation preview

Pediatric Bone Marrow Transplant Recipients with Acute Kidney Injury
Stuart L. Goldstein, MDAssociate Professor of PediatricsBaylor College of Medicine

Pediatric AKI Risk Factors:Stem Cell Transplant Recipients
AKI in stem cell transplantation results from: Nephrotoxic medications Radiation nephritis (post-SCT HUS) Veno-occlusive disease (hepatorenal syndrome) Sepsis
Early pediatric study1 (1975-88) revealed 50% AKI rate after SCT
Recent studies describe AKI epidemiology in pediatric SCT with lower TBI doses
1. Van Why SK et al: Bone Marrow Transplant 7:383, 1991

AKI in SCT Patients: Timing
Early AKI (0 to 60 days)Acute tubular necrosis (ATN)Veno-occlusive disease (VOD)Septic shockNephrotoxic medications
Late onset AKI (3 to 12 months)Cyclosporine/tacrolimus toxicityRadiation nephritisSepsis

Prospective single center study of 66 patients who received SCT over a 2 year period
AKI defined as SCr doubling in first 3 months Cyclosporine given to 60 patients
IV (2 mg/kg/dose) for 30 days Orally (6 mg/kg/day) 3-6 months 200 pg/ml target level

21% AKI rate Conditioning regimen nor
malignancy associated with AKI
VOD, CYA trough >200, foscarnet use associated with AKI development
AKI associated with CKD development (OR 8.0) at one year

Pediatric SCT Recipients with AKI
Lane et al (1994) (n=30) Sepsis most common cause of AKI and death Factors associated with persistent renal failure
> 10% Fluid Overload (%FO) > 3 pressors Hyperbilirubinemia
Todd et al (1994) (n=54) Increased mortality
Multiple organ system failure Primary pulmonary parenchymal disease

Pediatric Studies of BMT Recipients with ARF
Bunchman et al (2001) (n=26)BMT pts with ARF requiring RRT had
42% survival rate Greater survival for those required only HD
(78%) compared to PD (33%) or HF (21%)Outcome of children requiring RRT
directly related to the underlying diagnosis as well as their requirement for pressors

Retrospective evaluation of 226 children who received RRT for AKI from 1992-1998
26 patients with SCT Pressor use surrogate marker for patient
severity of illness Survival defined at PICU discharge


AKI and Fluid Overload
SCT pts with AKI are at risk for serious sequlae of FOPre-transplant conditioning causes small
vessel injury and extravascular fluid extravasation
Need for large volume requirement blood products total parenteral nutrition multiple antibiotics

% FO at CVVH initiation =[ Fluid In - Fluid OutICU Admit Weight ] * 100%
Fluid In = Total Input from ICU admit to CRRT initiationFluid Out = Total Output from ICU admit to CRRT initiation

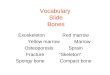
Lesser % FO at CVVH (D) initiation was associated with improved outcome (p=0.03)
Lesser % FO at CVVH (D) initiation was also associated with improved outcome when sample was adjusted for severity of illness (p=0.03; multiple regression analysis)
Mean+SEMean-SE
Mean
OUTCOME
%F
O a
t CV
VH
Initi
atio
n
0
5
10
15
20
25
30
35
40
45
Death Survival
p = 0.03

Seven center study from the ppCRRT Registry
116 patients with MODS PRISM 2 score used to
assess patient severity of illness
Survival defined at PICU discharge

Retrospective single center review of SCT patient AKI fluid/RRT management algorithm Furosemide infusion at 5% fluid overload RRT at 10% fluid overload
AKI defined as doubling of SCr or >10% FO from hospital admission
29 patients with 32 AKI episodes in 272 SCTs 4 patients with 2nd AKI (all died) 1 patient with pre-renal azotemia 3 patients with non-oliguric AKI First AKI rate of 11%

272 pts received allogeneic BMT All received chemo/radio therapy for pre-
transplant conditioning and GVHD prophylaxis
Underlying diseases: AML, ALL, aplastic anemia, CML, NHL, HL, VAHS, leukodystrophy and myelodysplastic syndrome

AKI CharacteristicsEtiology
Acute tubular necrosis (n=1) Nephrotoxic meds (n=16) ATN/Septic shock+Nephrotoxicity (n=9)
Kidney function Mean baseline Cr: 0.62 + 0.36 mg/dl Mean peak Cr: 3.51 + 1.62 mg/dl Mean lowest GFRest: 30.5 + 13.5
ml/min/1.73m2

ICU Characteristics23/26 with ICU admissionMean Pediatric risk mortality (PRISM) score
10.5 + 5 (5-20)Mean maximum % FO : 9 + 5% (3 -18%)14/26 with renal replacement therapy (RRT)
11/14 received CRRT 3/14 received intermittent HD


Clinical Variables Survival Non-Survival p
Always <10% FO 7/11 (64%) 3/15 (20%) < 0.03
Ventilation 6/11 (55%) 14/15 (93%) < 0.05
PRISM score >10 2/8 (25%) 11/15 (73%) < 0.05
Pressor >1 2/11 (18%) 8/15 (53%) 0.07
Sepsis 7/11 (63%) 13/15 (86%) 0.17
RRT treated 4/11 (36%) 10/15 (66%) 0.13

All patients who remained >10% FO despite starting RRT died
All survivors maintained/re-attained <10% FO Mechanical ventilation and PRISM score >10
at ICU admission correlated with patient death Despite prospective intention to prevent
severe FO, survival was <50% in pediatric BMT patients with ARF


51/370 patients in the ppCRRT with SCT 28/51 male AKI/CRRT causes
Multi-factorial (33%) Respiratory (18%) Sepsis (16%) VOD (16%) MODS (12%) Nephrotoxins (8%)


Non-survivors succumbing to primary pulmonary process and not excessive FO?

Patients requiring ventilatory support has lower survival (13/37 vs. 10/14, p<0.05)
Patients with MODS had nearly two-fold increase in mortality
Patients who received some convective CRRT had improved survival (17/29 versus 6/22, p<0.05)

Stanford ICU/BMT/CRRT study 10 patients with ARDS
6 BMT, 3 chemotherapy, 1 hemophagocytosis Serum creatinine 0.2 to 1.2 mg/dL in six children Serum creatinine 1.7 to 2.4 mg/dL in four children
CVVHDF initiated coincident with intubation regardless of fluid status or renal function (one exception) 3000 ml/1.73m2/hour 13 +/- 9 days
DiCarlo JV et al: J Pediatr Hematol Oncol. 2003 25:801-5

Stanford ICU/BMT/CRRT study
9/10 patients successfully extubated 8/10 patients survived
4/6 BMT patients survived4/4 Chemotherapy patients survived
Conclusion: early initiation of hemofiltration for intubated BMT patients may prevent progressive inflammatory lung injury and/or worsening fluid overload
DiCarlo JV et al: J Pediatr Hematol Oncol. 2003 25:801-5

CRRT for Pediatric SCT Summary
Most studies still demonstrate poor survival for this population
Early initiation of CRRT and aggressive diuresis to prevent fluid overload seems to be necessary, but not sufficient for pediatric SCT patients with AKI
Early CRRT may blunt the inflammatory response and prevent need for intubation or increase likelihood of extubation