Embed Size (px)
Citation preview

PEDIATRIC APPROACH TO PSYCHOSOMATIC MEDICINE -~,~
N. G. :Moju.~m~R, ?vl.B.c.a.e. (Cal.), >.c.H. (London.)
Calcutta
I have chosen a very unusual subject for discussion as I. feel it to be an important one. The cinema directors, adver- tisers, writers, artists, in fact everybody who is te make a living in this world is utilising psycholo~7 for their trade but we doctors, who come face to face with the results of stress and strain of life, are feeling shy of the subject of psychology.
It is not possible to deal with a new subject adequately ill a short article like this and I arn going to limit nay discussions to three points only. These are: what is psychosomatic medi- cine, whether problems of psychosomatic medicine present before a pediatrician, and what should be the approach of a pediatrician to such a problem.
B A S I S OF PSYCHOSOMA'IIC )r
We must realise that man is not a machine in spite of DESCaI~TE'S mechanistic theory of man gaining ground in certain parts of the world. Man's actions are more complex than that of an engine. How complex are the relations between the events of life, repressions, maladjustments and somatic diseases is very ill understood. But a few general observations may be made here.
That a sick man is a sad man is well known but it is not generally realised that a sad man is also a sick man. We know, however, that our skin bristles up when angry, it becomes damp when afraid. We also know that all goes wrong if the morning does not start right in the home, and we find everything rotten everywhere and lack of success haunts us throughout the day, we feel absolutely washed out and we do not feel like doing any work. We feel that our psyche has got complete possession of our soma. While this is true for our- selves, while by forced introspection we arrive at this conch>
* From Chit taranjan Shishu-Sadan (Children's Hospital), Calcutta. Read at the Scientific Section of the Re-union of Medical ('ollege, Calcutta, 195r.

I I 2 l,(t.ia;i Jom';~al of Pediatrics
sion in our m~l dejccled moo(Is, w~, forget lllis factor com- pletely when we arc faced with a patient who presents a baffling symptom to us. We pin our faith on the dissections that we (lid in the ana tomy hall, the experiments thai we carried out in the physiology ('lass and anything that is not answerable by these are nothing but nleta.physics to ~Js. Hence it will bc interesting to have a pee t) at what goes on behind the scene.
We take food, we chew it, swallow it, and then become oblivious about it unless something goes wrong; then we start refusing food (anorexia), or bring it out (vomiting), or hur ry it through the intestinal canal (diarrhoea), or if there is any obstruction lo the passage we find constipation and colic. \Vc (:all on the doctor; he examines, finds out the cause, treats and all become well again. But in certain cases the doctor does not find any cause though the patient is in agony. Here the psyche has come into action. This can be: illustrated by the following simple diagram.
A
�9 o6~C AL C O
1 / ~ " . , \
Y 't,
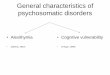
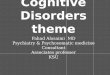
FI<,. i. .\ is the has(" line and B is tim normal threshold for internal
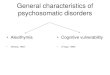
NORMAL THRESHOLD R - ,
A
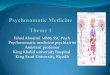
Fro. z . - -Here the normal threshold has come down to B~ as a result
activities. So long as the activity the normal activities within tile shad- curve remains below 13, no disease ed arPa produce symptom. Tn ensues but as the curve goes above ' understal,.d the basis of these B, the activities of the shaded t• symptoms, a psychosomatic approach Ilroduce disease. This can be amelio- is necessary (after Simeons). rated by d,'ugs and nther medica- l r l o n t s .
If we take the base line of our inlernal activities as A and 13 the line of consciousness of these activities, then so long as our internal acdvi ty curve remains below B, ail is well. As soon as the curve goes above B, body registers a protest by giving rise to pain and disease. In these cases the doctor cures the patient by drugs and other medicaments. But in certain cases, the line B comes down, the threshold of con- sciousness for internal activities come down (as shown in fig. 2)

Pediatric approach to psychosomatic medicine---Mo]umdar II3
and the body registers protest even when there is no physio- logical disorder. What are precisely the factors which con- tribute to the lowering of this threshold has not been completely explored. But it has been shown that the choice of the parti- cular organ may not always be accidental. The patient unconsciously regards the appropriate organ for the expression of his psyclaic ailments. As pointed out by WEST, " there is a relation between failure of instinctual satisfaction and dysfunc- tion of appropriate systems of the body " He further notes, " how often frustration of self-expression--and particularly the expression of aggressiveness--is to be found in cases of bronchospasm. The asthmatic ma~ be stifled with rage, though this is usually the last thing to appear upon the surface". He continues, "again we find complexes concerning fear of death appearing in cardiac neuroses, particularly in palpita- tions with multiple extra-systoles, effort syndromes and sub- sternal discomfort ......... Doubts and anxieties about physical security or the sinews of war are the frequent lot of patients with peptic ulceration." The clinical manifestations depend, therefore, on the organ chosen by the psyche.; if the heart is chosen we have neurocirculatory asthenia; in case the gastrointestinal tract is involved we get functional vomiting, dyspepsia, mucous colitis; in case the skin is attacked there originates the various dermatoses and so on.
It is the business of psychosomatic medicine to find out the reasons of the line B coming down and to formulate the best way to put it back to its original place. So we can define psychosomatic medicine in terms of HALl.mAY, as bodily dis- orders " whose nature can be appreciated only when emotional disturbances ......... are investigated."
Clinically, HURST, WITTKOWER, JELLIFFE, StIORVON and others have reported amelioration of symptoms by psycho- therapy. The influence of psyche over our digestive functions have been proved in the laboratory, amongst others, by PAVLOV, WITTKOWER and WOLI-FE and WOLFF.
In this short discussion I hope I have been able to tell you what I mean by psychosomatic inedicine and we can now see that it has come to stay and with the increase in the stress and strain of civilisation, the number and the variations in the psychosomatic manifestations will be multiplied.
3

114 Indian Journal o] Pediatrics
PEDIATRICL~',I AND "rite PSYCftOSOMATIC MEDICINE
We now come to the second question: does a psychoso- matic problem come before a pediatrician ? And if so in which form does it come ?
Considering the growth of homo sapiens from amoeba, it is really strange that the child is able to adjust so well to an unknown civilisation, which demanded of the hmnan race so much sacrifice. Like amoeba he starts his lite as an unicellular organism and travels millions of years of human experience within a comparitively small space of time and but for the 'organic m e mory ' of BUTLER, he would have perished long before he could come before a pediatrician for amelioration of symptoms! (By 'organic memory' BUTLER means all the experiences in time bound up in bodily structures). So it is but natural that the child sometimes unconsciously makes a wrong solution of a problem presented to his mind.
To make the matter more complex the parents and the doctors make quite a lot of fuss about the symptoms the child presents, which makes a profound impression on the mind of the child. The matter becomes more complicate_d as the child himself normally passes through a changing kaleidoscope of growth and development, which again is gravely influenced by the mental factors of the child. This distorts the clinical picture, sometimes beyond recognition. To understand that a thin child is not fattening because he is not happy or an asth- matic gets its attacks when he wants the mother to leave the baby for him or a child starts vomiting because he is to attend to too many things at the same time--reading, writing, danc- ing, singing; requires deep thought and sympathy. And one who fails to appreciate the underlying factors, considers these symptoms as malingering. There is probably no other harm- ful attitude of mind in a doctor than mistrust in the conscious manifestations of the unconscious deliberations of the child. He might be wrong, but he has got a problem to be solved, where our help is necessary.
In my practice I often come across problems of psycho- somatic medicine in children who would not eat, who vomit, who are light sleepers, who cannot conform to group discipline and hence cannot go to school, who steal and_ so on. I have been able to trace psychosomatic factors in asthmatic

Pedialric approach lo psychosomatic mediclne--.Mojmndar 115
children, in eczematous subjects and in infants suffering from pyrexia of unknown origin.
KAXNER has classitied these manifestations into three groups : - -
(a) Those in which personality difficulties express them- selves clearly as whole dysfunctions of the individual. This includes mental defect, emotional disorders (temper tantrums), antisocial trends (disobedience, lying, stealing), disorders of sleep and feeding (anorexia).
(b) Those in which personality difficulties express them- selves in the form of involuntary part dysfunctions. Examples in this group are headache (due to fatigue eitln.,ei after excite- ment or overwork), vomiting, constipation, diarrhoea, enuresis.
(c) Those in which personality diffmulties fcrm essential features or sequelae of physical illness, e.g., encephalitis, hypothyroidism.
PEDIATRIC APPI?OACH
I have now come to the last point. Let us, in the light of the above discussions, now formulate the pediatric approach to these problems. These can be summarised as fol lows:--
I. If a child presents a symptom for which no organic cause exists, his developmental progress must be reviewed with all the events of his life and development put into proper perspective.
2. The child should be considered as a whole. A grow- ing child who is adjusting himself to the environment cannot be considered as a ' c a s e ' of such and such a disease.
3. It must be reaiised by the practitioner that a child belongs to the family al)d reflects in a 'pure' state what goes on in the family. He has not learnt to hide nor has he learnt to evaluate the price of exp0sure of family tangles. Hence many of the unsolved somatic problems in the child may have their roots in the unsolved tension in the family circle.
4. To arrive at a diagnosis is not easy; good deal of trouble, patience, and tact is necessary and apparent smart- ness in the doctor will ruin the prospect of diagnosis as the patient and his parents will shut up iike an oyster before an apparently superior man.

II6 Indian, Journal o/Pediatrics
5. To diagnose rightly does not mean that cure is within our grasp, as much work is to be done to put the environment right. Even educated and enlightened parents would have their own unconscious motives in putting obstacles in your way. It requires persistent but tactful, slow but steady effort, a sympathetic and friendly influence to put things right.
6. Before any adjustment in the life of the child is attempted, all organic defects found by physical examination, e.g., bad teeth, infected tonsils, must be corrected, whether they contribute directly to the presenting problem or not.
7. Lastly the pediatrician, if he realises the profound influence of psyche over soma, will be very careful how he handles his patients during examination and treatment. For many more of our gestures, talks, interjections, worries, anxieties, surprises and gloating over pathological findings m the child, are carefully assessed by him than is commonly understood. A special care must be taken of the possible effects of prolonged illness or hospital treatment. It is very easy to give an imaginative child an imaginary illness which he may carry in his brain throughout his life all due to our carelessness.
t~E1; E R E N C E S :
:BUTLER, S.--quoted by Jelliffe. FIALLIDAY, J. L.--Lancet , 2: 692, :943. IIURST, A.--Seale IIayne, Neurological Studies, London, :9:9. JELLIFFE, S. E.--Sketches in Psychosomatic Medicine, New York, 1939. KAt,'NER, L.---Child Psychiatry, Charles C. Thomas, Illinois, I947. SHORVO~, H. S., ROOK, A. J., \VII, KIXSO~,', 1). S.--Brit . M. J., 2"- :30o, :95o. SI.~Eo,','s, A. T. W. ),:astering your nerves, D. B. Tarporevala Sons & Co. Ixt.
Bombay, :95o. WEST, R.--Lancet , 1" :o25, :950. \VIYTKOWER, E . - - ] . Merit. Sci., 81: 537, :935. WOLF, S. and WOLFF H. G.- -Human Gastric Functions, Oxford University
Press, New York, 1944.