Embed Size (px)
Citation preview

UPDATE ARTICLE
Pediatric anxiety disorders: from neuroscience toevidence-based clinical practiceGiovanni Abrahao Salum,1,2,3 Diogo Araujo DeSousa,1 Maria Conceicao do Rosario,3,4
Daniel Samuel Pine,5 Gisele Gus Manfro1,2,3
1Anxiety Disorders Outpatient Program for Child and Adolescent Psychiatry, Hospital de Clınicas de Porto Alegre (HCPA), Universidade
Federal do Rio Grande do Sul (UFRGS), Porto Alegre, RS, Brazil. 2Graduate Program in Medical Sciences: Psychiatry, UFRGS, Porto Alegre,
RS, Brazil. 3National Science and Technology Institute for Developmental Psychiatry for Children and Adolescents (INCT), Conselho Nacional
de Desenvolvimento Cientıfico e Tecnologico (CNPq). 4Child and Adolescent Psychiatry Unit, Department of Psychiatry, Universidade Federal
de Sao Paulo (UNIFESP), Sao Paulo, SP, Brazil. 5National Institutes of Mental Health (NIMH), Intramural Research Program, Emotion and
Development Branch.
The objective of this narrative review of the literature is to describe the epidemiology, etiology,pathophysiology, diagnosis, and treatment of pediatric anxiety disorders. We aim to guide clinicians inunderstanding the biology of anxiety disorders and to provide general guidelines for the properdiagnoses and treatment of these conditions early in life. Anxiety disorders are prevalent, associatedwith a number of negative life outcomes, and currently under-recognized and under-treated. Theetiology involves both genes and environmental influences modifying the neural substrate in acomplex interplay. Research on pathophysiology is still in its infancy, but some brain regions, such asthe amygdala and the prefrontal cortex, have been implicated in fear and anxiety. Current practice isto establish diagnosis based purely on clinical features, derived from clinical interviews with the child,parents, and teachers. Treatment is effective using medication, cognitive behavioral therapy, or acombination of both. An introduction to the neuroscience behind anxiety disorders combined with anevidence-based approach may help clinicians to understand these disorders and treat them properlyin childhood.
Keywords: Child; adolescent; anxiety disorders; obsessive-compulsive disorder
Introduction
Pediatric anxiety disorders refer to a collection ofsyndromes characterized by dysfunctional fear and/oranxiety affecting children and adolescents. Fear can bedefined as a negative emotional state triggered by thepresence of a stimulus that has the potential to causeimmediate harm, while anxiety can be defined as anemotional state in which the threat is not immediatelypresent but is anticipated. Both of these emotions areadaptive and essential for survival. They are accompa-nied by cognitive representations, physical symptoms,and behavioral modifications that prepare the individual todeal with danger (fear response). Fear and anxiety areconsidered dysfunctional when intensity, duration, and/orfrequency are not proportional to the eliciting threat, andthereby cause interference, disabilities, impairment, and/or distress that are judged clinically excessive.
Anxiety disorders in childhood and adolescence areassociated with a variety of negative outcomes, includinglower educational achievement and failure to attenduniversity.1 They affect children’s functioning with peers,
school personnel, and family,2,3 are associated withgeneral psychosocial impairment and disabilities2,3 aswell as with childhood suicide risk even when they arepresent in subthreshold levels.4 Pediatric anxiety dis-orders can also persist and continue to create inter-ference as the child matures into early adulthood,especially when associated with depression.5 Later inlife, anxiety disorders are associated with poorer qualityof life,6 suicide,7 and increased mortality due to cardio-vascular diasease,8 generating a high societal burdenand costs.9 Despite high prevalence and associationswith various negative outcomes, childhood anxiety israrely recognized by parents and children as a medicalproblem, leading a minority of affected individuals toreceive the care they need.10,11 Furthermore, physicianscan fail to recognize pediatric anxiety in children who dopresent for care, and even when anxiety is recognized, itis frequently treated sub-optimally.9,12,13
The objective of this review was to describe theepidemiology, etiology, pathophysiology, diagnosis, andtreatment of pediatric anxiety disorders. Given the factthat anxiety disorders more often co-occur and given theamount of similarities among these syndromes, this paperbroadly discusses ideas that are relevant to anxietydisorders as a group.14 Moreover, when consideringindividual conditions, the review focuses in depth on fourspecific disorders: separation anxiety (SeAD), social
Correspondence: Giovanni Abrahao Salum, Hospital de Clınicas dePorto Alegre, Rua Ramiro Barcelos, 2350/2202, CEP 90035-003,Porto Alegre, RS, Brazil.E-mail: [email protected]
Revista Brasileira de Psiquiatria. 2013;35:S3–S21� 2013 Associacao Brasileira de Psiquiatria
doi:10.1590/1516-4446-2013-S108

anxiety (SoAD), generalized anxiety (GAD), and panic(PD) disorders. Evidence related to specific phobias(SPs), obsessive-compulsive (OCD), and posttraumaticstress (PTSD) disorders, when relevant, is also incorpo-rated though in less detail.
Epidemiology
Prevalence
Anxiety disorders as a group constitute the most commonmental health problem in childhood and adolescence,15
affecting from 2.5 to 30% of youths.15-18 Large variationsin prevalence rates are observed among studies. Whilethe exact reasons for such variations remain unclear,most experts attribute them to methodological factorssuch as cross-study differences in the age of subjects,assessment instruments, information source, diagnosticsystem used, or variations in the application of thediagnostic criteria.19-22 Nevertheless, cross-cultural varia-bility in prevalence rates for anxiety is also likely to occur,given large differences in risk factor profiles and culturalbeliefs.20,21,23 One reasonable estimate for the globalprevalence of any anxiety disorder in the age range of 3to 17 years, adjusted for differences in methodologicalfactors, is 7.2%.24 There is no nationally representativestudy for pediatric anxiety in Brazil. The available studiesare limited to cities in the South and Southeast, wherereported prevalence is approximately 5%.25,26
Prevalence for each anxiety disorder is heavilydependent on the age range of the sample and on theage of onset patterns of each disorder. SeAD and SPhave the earliest age of onset, with half of the casesemerging before ages 5 and 8, respectively. SoAD andOCD typically emerge at early adolescence, with half ofthe cases emerging before ages 12 and 14, respectively.GAD is also common in early adolescence and less wellstudied than the other disorders, due to changes indiagnostic criteria over time. Nevertheless, current dataplace the median age of onset in late adolescence, by theages of 16-18 years. Agoraphobia, PD and PTSD are lowprevalence conditions in childhood, with higher preva-lence rates in late adolescence and early adults (medianage of onset 17, 19 and 22, respectively).15 Beyond dataon age trends, anxiety disorders have also been linked toother demographic factors. Gender is probably the mostfrequent demographic correlate of pediatric anxiety. Thefemale/male gender ratio for almost all anxiety disorder is2:1 to 3:1.27 Most studies have shown an associationbetween anxiety and lower instruction levels and worsesocioeconomic status19 but no association has beenfound with urbanization or ethnicity.16,19 Table 1 depictsthe prevalence found in two Brazilian studies and othertwo representative samples in the United States andEurope.
Natural course
Prospective studies have shown that 60-80% of adultswith full criteria for anxiety disorders report signs ofearlier, pediatric anxiety.29 Despite the fact that most
affected adults have signs of anxiety as children, inchildren followed prospectively, anxiety disorders havevariable natural course. This course typically involves oneof four trajectories: 1) spontaneous long-term remission(e.g., childhood SeAD that totally disappears in anotherwise typically developing adolescent who maturesto become a healthy adult); 2) strict homotypic continuity(e.g., SoAD in childhood persisting into SoAD in adult-hood); 3) broad homotypic continuity (e.g., SeAD inchildhood predicting PD in adulthood); and 4) sequentialheterotypic comorbidity (e.g., SoAD in childhood predict-ing latter development of major depression in adult-hood).15,19,30,31 The latter two trajectories involve acourse that has been characterized as waxing andwaning over time,32 oscillating between threshold andsubthreshold clinical conditions (resulting in high rates ofrecurrence rather than chronicity).33
The frequency of each one of these courses is highlyvariable from one longitudinal study to another.1,5,29,32,34-42
Broadly we can say that about one-third of anxiouschildren achieve a long-term remission, another third partpersists with strict or broad anxiety continuity (frequentlyaccompanied by comorbid disorders), and about one-thirdremits from anxiety and develops a sequential heterotypiccomorbidity (mainly with major depression and substanceabuse).1,29,38,40 Among a variety of potential moderatorsof the natural history, unfavorable natural courses havebeen associated with female gender, symptom severity,duration of illness, early age of onset, severe avoidanceand associated impairment, parental history of psycho-pathology, and inhibited temperament.15,43
Etiology and pathophysiology
Mental disorders reflect individual differences in brainfunction.31,44,45 Those differences are a result of acomplex combination of factors that ultimately representthe distal effects of risk genes and/or environmentalcomponents (etiological factors). These etiological riskfactors act on neural circuits (neural substrates) duringbrain development and cause quantitative and/or quali-tative abnormalities in brain functions (pathophysiologicalprocesses). This deviation from typical trajectories ofbrain development results in emotional and behavioralmanifestations of psychiatric disorders.46
Genes and environment
Family studies have shown that anxiety disorders arefamilial,47,48 whereas twin studies demonstrated thatanxiety disorders are heritable49 and that the proportionof the phenotypic variability explained by genetic factors(heritability) for anxiety disorders ranges from 25-60%.49-52
In general, this represents modest heritability for apsychiatric condition, clearly meaningful but lower thanfor highly heritable conditions, such as attention deficithyperactivity disorder (ADHD) or autism.53 In addition, onestudy54 investigating common childhood psychiatric dis-orders found that a general set of genes might nonspeci-fically influence risk for childhood psychiatric disorders,
GA Salum et al.S4
Rev Bras Psiquiatr. 2013;35(Suppl 1)

Tab
le1
Dia
gnostic
crite
ria
for
pedia
tric
anxie
tydis
ord
ers
and
epid
em
iolo
gy
28
Pre
vale
nce
(%)
Sim
plif
ied
DS
M-I
Vdia
gnost
iccrite
ria
Child
ren
Adole
scents
Age
of
onset
Genera
lized
anxie
tydis
ord
er
(GA
D)
A-
Anxie
tyand
excess
ive
worr
y,
most
of
the
days,
about
anum
ber
of
events
for
at
least
6m
onth
s.
B-
Worr
yis
difficult
tocontr
ol.
C-
At
least
one
of
the
follo
win
g:
1)
restlessn
ess;
2)
easily
fatigued;
3)
diffic
ulty
concentr
atin
gor
min
dgoin
gbla
nk;
4)
irrita
bili
ty;
5)
musc
lete
nsi
on;
6)
sle
ep
dis
turb
ance.
TA
U:
0.4
PE
L:
1.4
NC
S:
2.2
ED
SP
:0.8
ED
SP
:19
years
Socia
lanxie
tydis
ord
er
(SoA
D)
A-
Mark
ed
and
pers
iste
nt
fear
of
socia
lor
perf
orm
ance
situatio
ns
when
exposed
tounfa
mili
ar
people
or
pote
ntia
lhum
iliation/e
mbarr
assm
ent
(must
occu
rw
ith
peers
,not
just
with
adults
).B
-E
xposure
toth
efe
are
dsocia
lsituatio
npro
vokes
anxie
ty(e
.g.,
cry
ing,
tantr
um
s,
freezin
g,
or
shrinkin
g).
D-
Socia
lor
perf
orm
ance
situations
are
avoid
ed
or
faced
with
inte
nse
anxie
tyor
dis
tress.
F-
At
least
6m
onth
s.
TA
U:
0.7
PE
L:
0.1
NC
S:
9.1
ED
SP
:3.5
ED
SP
:12.5
years
Separa
tion
anxie
tydis
ord
ers
(SeA
D)
A-
Excess
ive
anxie
tyw
hen
aw
ay
from
hom
eor
from
att
achm
ent
figure
sor
when
separa
tion
isanticip
ate
d,
with
at
least
thre
eof
the
follo
win
g:
1)
dis
tress;
2)
worr
yabout
losin
gor
harm
befa
lling
att
achm
ent
figure
s;3)
worr
yth
at
an
unto
ward
event
will
lead
tosepara
tion;
4)
relu
ctance
/refu
salto
go
toschoolor
els
ew
here
;5)
fearf
ul/r
elu
ctant
tobe
alo
ne
or
withoutatt
achm
entfigure
s;6)
relu
ctance
/refu
salt
ogo
tosle
ep
withoutan
attachm
entfigure
or
tosle
ep
aw
ay
from
hom
e;
7)
nig
htm
are
sw
ith
separa
tion;
8)
physic
alsym
pto
ms.
B-
At
least
4w
eeks.
TA
U:
1.4
PE
L:
0.7
NC
S:
7.6
ED
SP
:4.5
years
Panic
dis
ord
er
(PD
)A
-R
ecurr
ent
unexp
ecte
dpanic
att
acks
(i.e
.,in
tense
anxie
tyof
sudden
onset
and
brief
dura
tion),
with
at
least
one
of
them
follo
wed
by
at
least
1m
onth
of
at
least
one
of
the
follo
win
g:
1)
concern
about
additio
nalatt
acks;
2)
worr
yabout
the
implic
ations/c
onsequence
sof
the
attack;
3)
sig
nific
ant
change
inbehavio
rre
late
dto
the
attacks.
B-
Pre
sence
or
absence
of
agora
phobia
(diffe
rentialdia
gnosis
for
PD
with
or
without
agora
phobia
).
TA
U:
0.0
PE
L:
0.0
NC
S:
2.3
ED
SP
:1.6
ED
SP
:18.5
years
Speci
fic
phobia
s(S
P)
A-
Mark
ed
and
pers
iste
ntexcess
ive
or
unre
asonable
fear
cued
by
the
pre
sence
or
anticip
ation
ofa
specifi
cobje
ctor
situatio
n(e
.g.,
flyin
g,
heig
hts
,anim
als
,in
jection,
blo
od).
B-
Exposure
toth
ephobic
stim
ulu
spro
voke
sanxie
ty(e
.g.,
cry
ing,
tantr
um
s,
freezin
g,
or
clin
gin
g).
D-
Phobic
situ
ation(s
)is
(are
)avoid
ed
or
faced
with
inte
nse
anxie
tyor
dis
tress;
F-
At
least
6m
onth
s.
TA
U:
1.0
PE
L:
1.4
NC
S:
19.3
ED
SP
:2.3
ED
SP
:7
years
Obsessiv
e-
com
puls
ive
dis
ord
er
(OC
D)
A-
Either
obsessio
ns
(i.e
.,re
petitive
intr
usiv
e/inappro
priate
thoughts
,im
puls
es,
or
att
em
pts
toig
nore
,suppre
ss,
or
neutr
aliz
eth
em
with
oth
erth
oughts
or
actions)
or
com
puls
ions
(i.e
.,re
petitiv
ebehavio
rsor
menta
lacts
,or
accord
ing
toru
les,
and
tore
duce
dis
tress
or
pre
vent
event)
.C
-O
bsessio
ns/c
om
puls
ions
cause
mark
ed
dis
tress
and
are
tim
econsum
ing
(.1
hour
aday).
TA
U:
0.1
PE
L:
0.1
ED
SP
:0.7
ED
SP
:14.5
years
Posttra
um
atic
str
ess
dis
ord
er
(PT
SD
)
A-
Past
exp
osure
toa
traum
atic
eve
nt
respondin
gw
ithin
tense
fear,
help
lessn
ess,
horr
or,
or
dis
org
aniz
ed
or
agita
ted
behavi
or.
B-
Re-e
xperience
ofth
etr
aum
atic
eventth
rough
atle
ast
one
ofth
efo
llow
ing:1)
intr
usiv
ere
colle
ctions
ofth
eeventor
repetit
ive
pla
yof
the
traum
a;
2)
dre
am
sof
the
event
or
frig
hte
nin
gdre
am
s;
3)
feelin
gas
ifth
etr
aum
atic
event
were
recurr
ing;
4and
5)
inte
nse
psyc
holo
gic
aldis
tress
or
physio
logic
alre
activity
at
exposure
toin
tern
alor
exte
rnalcues
that
resem
ble
an
aspect
of
the
traum
atic
event.
C-
Avoid
ance
ofstim
uli
asso
cia
ted
with
the
traum
aand
num
bin
gofgenera
lresponsiv
eness,w
ith
atle
ast
thre
eofth
efo
llow
ing
(notpre
sentbefo
reth
etr
aum
a):
1)
eff
ort
sto
avoid
thoughts
,fe
elin
gs,or
convers
atio
ns
rela
ted
toth
etr
aum
a;
2)
eff
ort
sto
avoid
activ
itie
s,
pla
ces,
or
people
that
aro
use
recolle
ctions
of
the
traum
a;
3)
inabili
tyto
recall
aspects
of
the
traum
a;
4)
mark
edly
dim
inis
hed
inte
rest
or
part
icip
ation
insig
nific
ant
activitie
s;
5)
feelin
gof
deta
chm
ent
from
oth
ers
;6)
restr
icte
dra
nge
of
aff
ect;
7)
sense
of
afo
reshort
ened
futu
re.
D-
Incr
ease
daro
usa
l(n
ot
pre
sent
befo
reth
etr
aum
a),
with
at
least
two
of
the
follo
win
g:
1)
diff
iculty
falli
ng
or
stayi
ng
asl
eep;2)irrita
bili
tyor
outb
urs
tsofanger;
3)
diff
iculty
conce
ntr
atin
g;4)
hyp
erv
igila
nce;5)
exa
ggera
ted
start
lere
sponse
.E
-M
ore
than
1m
onth
.
TA
U:
0.1
PE
L:
0.1
NC
S:
5.0
ED
SP
:1.3
ED
SP
:22.5
years
Dia
gnostic
crite
ria
for
all
anxie
tydis
ord
ers
:th
efo
cus
ofth
eanxie
tysym
pto
ms
isnotconfined
tofe
atu
res
ofanoth
er
menta
ldis
ord
er.
The
anxie
tysym
pto
ms
cause
clin
ically
sig
nific
antdis
tress
or
impairm
entin
socia
l,fa
mily
,school,
or
oth
er
import
antare
as
offu
nct
ionin
g.T
he
dis
turb
ance
isnotdue
toth
eeff
ects
ofa
substa
nce,genera
lmedic
alc
onditio
n,or
anoth
er
menta
ldis
ord
er.
ED
SP
=E
arly
Develo
pm
enta
lS
tages
of
Psychopath
olo
gy
(Com
posite
-In
tern
ational-
Dia
gnostic
Inte
rvie
w-
CID
I,lif
etim
e,
ages
14-2
4);
GS
M=
Gre
at
Sm
oky
Mounta
ins
Stu
dy
(Child
and
Adole
scent
Psychia
tric
Assess
ment
-C
AP
A,
3-m
onth
pre
vale
nce
,ages
9-1
6);
NC
S=
NationalC
om
orb
idity
Surv
ey
-A
dole
scent
(CID
I,lif
etim
e,
ages
13-1
8);
PE
L=
Pelo
tas
Stu
dy
(Develo
pm
ent
and
Well-
Bein
gA
ssess
ment
-D
AW
BA
,curr
ent,
ages
11-1
2);
TA
U=
Taubate
Stu
dy
(DA
WB
A,
curr
ent,
ages
7-1
4).
Pediatric anxiety disorders S5
Rev Bras Psiquiatr. 2013;35(Suppl 1)

whereas two additional sets of genes might influence riskfor two more narrow aspects of illness, reflecting still broadrisks for internalizing and externalizing disorders, respec-tively. Environmental factors generally involve non-sharedenvironment effects; meaning factors that tend to makeindividuals within a family appear different. Such factorsinclude aspects of an individual child’s school environ-ment, the unique stressors he or she experiences, andtheir social situation. This is somewhat consistent with thegeneralist genes, specialist environment model, i.e., thatcommon psychopathology mostly share their geneticliability, but are differentiated by non-shared experiences.
Twin studies that specifically focused on pediatricanxiety also support the role of both genes andenvironment, but the role of the shared environment alsoappears to be significant with lower genetic effects.These types of studies focus more narrowly on specificpresentations of anxiety, in contrast to studies morebroadly examining varieties of psychopathology. Thesemore narrow studies are incapable of specifying whatgenes and environmental factors are particularly note-worthy for pediatric anxiety. Nevertheless, no twin studyis capable of clarifying how any set of genes andenvironments affects the brain unless the study directlyassesses brain function. It is only through effects on thebrain that genes and the environment can ultimatelyresult in emotional and behavioral abnormalities.48
Candidate gene studies search for specific loci at thegenome. While these have been criticized as beingvulnerable to type I errors, they have identified severalrisk genes for anxiety disorders55; however, consistentwith type I errors, a recent review suggested thatavailable work resulted in ‘‘not a single instance ofreplication.’’56 Genome-wide association studies (GWAS)search the entire genome for signs of association. Whenperformed properly, these are less vulnerable to type Ierrors. To date, five such GWAS have been performed onanxiety disorders,57-62 though none of these focuses onchildren. Among the five, two of them produced sig-nificant results. Otowa et al.59 found two genes thatachieved genome-wide significance (transmembraneprotein 16B and plakophilin 1), but a subsequent studyfailed to replicate these findings in PD patients.58,63 Inanother study, a variant in the retinoid-related orphanreceptor alpha gene (RORA) showed genome-widesignificance for PTSD.61 In addition to these five GWASinvestigations, other studies have investigated the excessof rare copy number variations (CNVs), which are relativelarge segments of DNA that are either deleted orduplicated. In this area, the only study on PD failed tofind genome-wide significance.64
While each of these genetic strategies has advantages,they also are relatively insensitive to many mechanisms.For example, available evidence finds signs of complexgene-environment interplay in anxiety disorders,65-69 andmost research on genetics is poorly suited for capturingsuch effects. Genes and environments shape anxiety andother behaviors through a complex interplay, as it hasbeen shown through three specific relationships: 1) gene-environment interaction (genetically influenced sensitivity
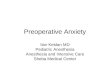
to specific environments); 2) gene-environment correla-tion (genetic influences on individual variation in people’sexposure to particular environments); 3) epigenetics(environmental moderation of the effects of genesthrough influences in gene expression).70 As under-standing of genes and the environment accrue, thecomplexity of these three sets of relationships is likelyto appear even greater. This suggests that, for anxietyand other so-called complex behaviors influenced bymultiple factors, the effects of genes are far fromdeterministic and cannot be dissociated from the effectsof the child’s environmental conditions. Figure 1 illus-trates these complex relationships.
Pathophysiological processes and neural substrate
Despite a considerable advance over the last years, littleis known about the neural underpinnings of anxietydisorders in children and adolescents. Most of the workin this area focuses on information processing functionsinvolved in emotional processing (in particular threatprocessing) and cognitive control.31,71
The state of knowledge about mental processesinvolved in pediatric anxiety is currently limited.Nevertheless, tentative conclusions about existing rela-tionships can be drawn. In particular, a set of dysfunc-tional mental processes has been linked to pediatricanxiety and associated traits, such as the early-child-hood temperament of behavioral inhibition. Thesedysfunctional processes can be classified into fivegroups of information-processing functions: 1) threat-attention interaction (a tendency for anxious children toautomatically orient their attention towards or awayfrom threats)72; 2) threat appraisal (a tendency foranxious children to classify and respond to neutral orharmless stimuli as if they are dangerous)73; 3) memoryand learning processes (a tendency for anxious indivi-duals to learn different associations among safe anddangerous stimuli, as presented in fear conditioning andextinction experiments)73-75; 4) social evaluative pro-cesses (a tendency for anxious children to becomeconcerned about peer evaluation)76; 5) increasedsensitivity to rewards (a tendency for anxiety childrento more strongly alter their behavior when trying toachieve rewards).77,78
This set of findings suggests that anxiety disordersinvolve dysfunctional processes in various emotional andcognitive processes, each of which is in turn regulated byseveral brain regions that may support anxiety disorderpathophysiology.31,71 Some of the regions include: theamygdala, several portions of the prefrontal cortex -particularly the ventrolateral and dorsomedial divisions -and dysfunctions in the basal ganglia, particularly inpatients with OCD.31,71,79,80
Parenting, life events, and modeling/learning
Several studies have linked various environmental factorsto risk for anxiety. These factors include features of thehome, such as overprotective/over-controlling parenting
GA Salum et al.S6
Rev Bras Psiquiatr. 2013;35(Suppl 1)

style,81,82 as well as features that can occur either withinor outside of the home, such as stressful life events.83,84
Nevertheless, the evidence so far is limited regarding thedirection of these associations. For example, one couldhypothesize that some parents who are themselvesalready anxious might also respond to their child’s anxietyor other signs of vulnerability with parenting practices thatmay further reinforce the child’s difficulties, such asfailure to encourage infant social responsiveness.17,85 Inother words, such environmental factors could eitherpredispose to anxiety in children or children who are atrisk for anxiety may behave in such a way that theseenvironmental factors are preferentially elicited. Kender &Baker found that stressful life events, parenting, family,environment, social support, peer interactions, andmarital quality are significantly influenced by geneticfactors with heritability estimates ranging from 0.07 to0.3968 - suggesting that associations between anxiety and
parenting or other environmental factors may be geneti-cally mediated. Other studies found that the effect ofparenting was only partially genetically mediated with animportant role of non-shared environment.86 In addition,some authors suggest that some fears may arise as aresult of modeling and vicarious learning (i.e., learningthrough observation of a parent fearful response in athreatening situation for her/him)87-89 and verbal transmis-sion of threat information about novel objects.90,91
However, more experimental studies are needed to betterunderstand these phenomena.
Research on influences of parenting in psychiatricdisorder illustrates that risk and causality in psychiatryare extremely complex phenomena.68,69,92-96 In addition,heterogeneity within anxiety disorders is an importantfactor to consider. Two individuals with similar clinicalmanifestations may have different dysfunctionalprocesses, and the same dysfunctional process may be
Figure 1 Schematic representation of the etiological and pathophysiological process related to anxiety disorders. E1, mainenvironmental effects (E); G1, main genetic effects (G); E2xG2, example of gene environment interaction (GxE; geneticsensitivity to specific environments); E4RG4, example of epigenetic regulation (Epi; environmental regulation of geneexpression); E5«G5, example of gene environment correlation (rGE; genetic influences on individual variation in people’sexposure to particular environments). Genes and environments influence the developing brain. Dysfunctional circuits in theneural substrate result in deficient information processing that ultimately affect individuals’ thoughts, emotions, and/orbehaviors. Extreme dysfunctions in such system produce functional impairment and are interpreted as anxiety disorders.
Pediatric anxiety disorders S7
Rev Bras Psiquiatr. 2013;35(Suppl 1)

responsible for different clinical manifestations. Newinitiatives, such as the Research Domain Criteria(RDoC),97,98 are attempting to clarify the ways in whichunderlying neural substrates of mental disorders con-tribute to dimensional traits that are expressed in specificbehaviors and that cut across current operationalizationof psychopathology.
Dimensional aspects of anxiety
As noted above, fear and anxiety are adaptive responsesto potential threats. The expression of these symptomscan range from normative to pathological behavioraccording to the frequency, intensity, duration and/orinterference in functioning. Therefore, anxiety disordersmay lie at the extreme end of a continuum, rather thaninvolve symptoms that are exclusive to pathologicalconditions. As such, anxiety disorders would representa variation in degree but not in kind.99 This would imply aview of normal and pathological anxiety as falling along adimension, with diagnostic thresholds reflecting clinicaland societal burden rather than discontinuous pathophy-siological states. If this view of anxiety is correct, it wouldbe quite important to study the normal development offears and learn to recognize temperaments that areclosely related to psychopathology in infants. Two suchfactors associated with anxiety are behavioral inhibitionand anxiety sensitivity.
Normal development of fears
Because the development of fear circuitry occurs early,fear responses can be observed very early in life. Thereare changes in the context of normative fear over thecourse of development, typically from immediate andconcrete stimuli during infancy to anticipatory, abstract,and more global stimuli that characterize adolescentfears. During infancy and toddlerhood, most infantsdevelop a fear of loss and shyness to strangers thatpeaks around 8 to 12 months of age, as is expressed bywariness around unfamiliar people.100,101 These fearsare often followed by separation anxiety that peaksaround 10 to 18 months marked by distress about beingseparated from parents. For most children, those fearsdisappear around 2 to 3 years of age. Early childhood(pre-school age) is characterized by normative fearsrelated to specific threats, such as meteors, clouds,blood, end of the world, being kidnapped, fairies, loss oforientation, and dying or death of others. School age ismarked by similar fears, including those directed towardswind, darkness, water, domestic animals, insects,ghosts, death, and disease, germs, natural disasters,traumatic events, harm to self or others, school anxiety,and performance anxiety. Adolescence is characterizedby fear of negative evaluation and fear of rejection frompeers. All normative fears typically decrease with ageand are transient. In adolescence, stability begins tobecome apparent. Increases in prevalence of phobic andanxiety disorders parallel decreases in normativefears.71
Behavioral inhibition and anxiety sensitivity
Given the dimensional and developmental nature ofinternalizing psychopathology, researchers have consid-ered whether certain types of temperaments observedvery early in life predict later risk for pediatric anxiety.102
Most of this work has focused on infants who displayheightened reactions to novelty and heightened sensitiv-ity to stimulus variations. Some such infants mature tobecome toddlers who withdraw from novel or unfamiliarsocial situations. This group of toddlers is said to manifestthe temperament of behavioral inhibition. This tempera-ment places the child at risk for SoAD.103,104 A recentmeta-analysis showed that behavioral inhibition wasassociated with a seven-fold increased risk for developingSoAD. Given that 15% of infants are classified asbehaviorally inhibited and about half of them will developsocial anxiety this is one of the most consistent riskfactors for social anxiety.103 Anxiety sensitivity is anotherdimensionally distributed trait that, like behavioral inhibi-tion, has been linked to pediatric anxiety. Anxietysensitivity involves beliefs that anxious symptoms willhave harmful physical, psychological, or social conse-quences to the individual. Some studies suggest that thistrait predicts PD more specifically than other forms ofanxiety, expressed later in life.105,106 Although thesedimensional traits are often seen as risk factors, analternative conceptualization is that they represent alter-native manifestations of overt anxiety disorders, as theyare expressed in younger children.
Clinical manifestations and diagnosis
Despite the dimensional perspective of fear and anxiety,diagnostic and clinical decisions (e.g., to treat or not totreat) are categorical and require a classificatory system.According to the DSM-IV, most of the anxiety disordershave the same diagnostic criteria for children, adoles-cents or adults, with some minor variations in presenta-tion (Table 1).
Screening
Some researchers argue that screening for anxietydisorder should be universal (applied to every childirrespective of their symptoms). Despite that, from apublic health perspective, only targeted screening may bepossible, and it is not clear whether universal screeningwould be in the best interest of patients. Therefore,screening may be most helpful among children whopresent with complaints about excessive fears, extremeshyness, frequent worries or rituals - some kind ofemotional distress.
Diagnostic procedures and differential diagnosis
The diagnosis of pediatric anxiety disorder is based onclinical evaluations. First, normal fears should be differ-entiated from pathological fears. The best way of doing thisis evaluating whether fears are: 1) developmentally
GA Salum et al.S8
Rev Bras Psiquiatr. 2013;35(Suppl 1)

expected or not; 2) appear with intensity, duration, andfrequency that is higher than expected for the same age;and 3) whether the fears result in distress and impairment.
Second, pathological fears should not be betterexplained by co-occurring symptoms of another psychia-tric disorder, by a co-occurring medical disease, or due tothe influences of use/abuse of alcohol and/or otherpsychoactive substances (as well as not due to with-drawal). Therefore, it is crucial to investigate the situa-tions and context in which the anxiety symptomsmanifest.
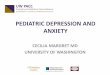
Third, primary anxiety should be classified according tothe type of anxiety disorder. Anxiety disorders share incommon several clinical features, namely dysfunctionalcognitions, physical symptoms, and behavioral dysfunc-tions such as avoidance - one of the core symptomaticcharacteristics of all anxiety disorders. However narrowlydefined in diagnostic manuals, specific anxiety disordersalso exhibit a substantial degree of phenotypic hetero-geneity. Each anxiety disorder has a symptomaticsignature. For treatment purposes, it is useful todetermine the main anxiety disorder as the condition thatproduces the greatest distress, impairment, and inter-ference in the child’s life. Figure 2 describes the coresymptomatic features of the main pediatric anxietydisorders.
Comorbidity
Pediatric anxiety disorders and other childhood psychia-tric conditions frequently co-exist in the same patient, aphenomenon known as comorbidity. In clinically referredsamples, comorbidity is often the rule rather than theexception,108 with more than half of the patients havingmore than one anxiety disorder. In community samples,anxiety also increases the chance of having additionalpsychiatric diagnoses such as major depression (oddsratio [OR] = 8.2; 95%CI 5.8-12), ADHD (OR = 3.0; 95%CI2.1-4.3), and oppositional defiant disorder/conduct dis-order (OR = 3.1; 95%CI 2.2-4.6).109 Anxiety disordersand substance abuse and dependence in childhoodappear not to be related, but this comorbidity increasedramatically in adolescents and adults, notably in sub-jects with social anxiety.110 Therefore a search forcomorbidity is imperative when evaluating children withanxiety. This includes a specific search for symptoms ofmajor depression (including suicidal ideation), substanceabuse and dependence, ADHD, and oppositional defiantdisorder. Two other conditions that are not necessarilydisorders but are rather specific behaviors also frequentlypresent in anxious children. These conditions areselective mutism, which is the failure to speak in specificsetting despite full use of language at home, and schoolrefusal, which is the failure to attend to school.
The high degree of comorbidity between anxietydisorders, as a group, and depression is clearly notable.In terms of associations between depression and one oranother specific anxiety disorder, evidence is mixed interms of whether associations are particularly strong withspecific conditions. Some studies showed particularly
strong associations with GAD, potentially reflecting asingular higher order structure for the two conditons.111
Other findings appear less specific and more stronglyreflecting developmental variations.38
Assessment
A proper assessment of psychiatric symptoms in child-hood involves information derived from the child,parents, and teachers. Particularly for anxiety disorders,the child information is extremely valuable. Since someof the symptoms involve emotions, cognitions, andbehaviors that may not involve the parent, it is imperativeto consider the child’s report. Younger children may havedifficulties communicating their symptoms as well astheir associated distress and impairments to the physi-cian.15 In these cases, parental and teacher informationmay be more valuable, but clinicians still should bevigilant for signs of avoidance expressed by the child.The clinician should be aware that parents often look forhelp with unexplained physical complaints reflectingheightened arousal (headaches, stomachaches, nau-sea, vomiting, diarrhea, muscle tension, and difficultywith sleep) that may indicate an underlying pediatricanxiety.112
As mentioned above, the diagnosis of any anxietydisorder is clinical. Although several studies link anxietyto various biological or genetic factors, the magnitude ofthese associations is far too small to be of clinical usewhen evaluating individual children. Some structuredinterviews and/or rating scales may be helpful to: 1)screen for anxiety symptoms in non-specialized settings;2) assess symptom severity; and 3) monitor treatmentgains. Table 2 depicts a variety of clinician, self andparent rated instruments that may be useful in researchand clinical practice.
Treatment
Both medication and psychotherapy are effective in thetreatment of pediatric anxiety symptoms. Literature isreviewed below in four specific areas: 1) non-OCDanxiety disorders (SeAD, SoAD, GAD, and PD); 2)OCD; 3) PTSD; 4) SP.
Because PD is exceptionally rare in childhood andadolescence, insufficient evidence exists from controlledstudies to guide treatment.155 Therefore, clinical manage-ment of PD is often considered as an extension of thecurrently available evidence for more common and betterstudied anxiety disorders (e.g., SeAD, SoAD and GAD).SPs are also highly comorbid with other anxiety dis-orders. When isolated, treatment should use cognitivebehavioral therapy (CBT), with exposure to the fearedobject combined with cognitive techniques during theexposure (whether in vivo, imaginary, or virtual) thatfacilitate extinction. Too few studies examine efficacy ofmedication in SP to inform recommendations, probablybecause CBT, the less invasive interventions, is typicallyeffective. Evidence regarding the treatment of PTSD andother consequences of trauma in children most deeply
Pediatric anxiety disorders S9
Rev Bras Psiquiatr. 2013;35(Suppl 1)

examines CBT, where again, evidence of efficacy isstrong.156 Because the few studies examining medicationefficacy in pediatric PTSD are generally equivocal, CBTshould be the first-line treatment in children presentingwith posttraumatic anxiety.157 Due to a more specializedcharacterization of the PTSD treatment, this topic will notbe further discussed here. Additional information can befound elsewhere.157
Medication + psychoeducation
Placebo-controlled clinical trials demonstrate efficacy forselective serotonin reuptake inhibitors (SSRIs; fluoxetine,fluvoxamine, paroxetine, and sertraline) in both pediatricOCD and non-OCD disorders.158 Some trials alsosupport the use of serotonin and norepinephrine reuptakeinhibitor (SNRI) venlafaxine for non-OCD disorders.158
Figure 2 Algorithm for the diagnostic assessment of pediatric anxiety disorders (based on Salum et al.107). ADHD = attentiondeficit hyperactivity disorder; ODD = oppositional defiant disorder
GA Salum et al.S10
Rev Bras Psiquiatr. 2013;35(Suppl 1)

Tab
le2
Instr
um
ents
for
the
assessm
ent
of
anxie
tysym
pto
ms
and
dia
gnosis
of
anxie
tydis
ord
ers
inchild
ren
and
adole
scents
Clin
icalin
str
um
ents
for
the
dia
gnosis
of
pedia
tric
anxie
ty
Instr
um
ent
Rate
r(info
rmant)
Dia
gnosis
Estim
ate
dtim
eD
iagnostic
syste
m
Psy
chom
etr
icpro
pert
ies
(for
anxie
tydis
ord
ers
sect
ion
when
availa
ble
separa
tely
)
Relia
bili
tyV
alid
ity
K-S
AD
S*
(E/P
L)1
13-1
15
Clin
icia
n(C
,P
,C
LIN
)C
urr
ent/lif
etim
e--
DS
M-I
VT
R:
0.8
0(c
urr
ent)
;0.6
0(lifetim
e)
IR:
93%
-100%
(curr
ent)
;100%
(lifetim
e);*k
=0.9
(anxie
ty)
--
DA
WB
A*
26,1
16,1
17
Lay/C
linic
ian
(C,
P,
T,
CLIN
);C
OM
P(C
,P
,T
,C
LIN
)
Curr
ent
30-5
0m
inD
SM
-IV
;IC
D-1
0IR
:*k
=0.9
1(inte
rnaliz
ing)
CO
NV
:0.1
3-0
.48
(DIS
C-I
V);
0.2
3-0
.48
(CA
PA
);dia
gnosed
cases
pro
bably
more
severe
than
DIS
C-I
Vand
CA
PA
DIS
CR
:hig
her
rate
of
dia
gnosis
ina
clin
icth
an
ina
com
munity
sam
ple
(OR
=13.3
)C
hIP
S*
118,1
19
Clin
icia
n(C
,P
,C
LIN
)C
urr
ent
20-5
0m
inD
SM
-IV
+P
sychoso
cia
lstr
essors
IR:
0.9
0-1
.00
CO
NV
:hig
hle
vels
ofagre
em
entw
ith
DIC
Aand
clin
icia
n’s
dia
gnosi
s
DIS
C-I
V116,1
20
Clin
icia
n(C
,P
,C
LIN
);C
OM
P(C
,P
,C
LIN
)C
urr
ent
70
min
DS
M-I
V;
ICD
-10
TR
:0.4
8-0
.86
CO
NV
:13-0
.48
(DA
WB
A);
0.2
1-0
.61
(CA
PA
)D
ICA
-IV
121,1
22
Clin
icia
n(C
,P
,C
LIN
);C
OM
P(C
,P
,C
LIN
)C
urr
ent
30-1
20
min
DS
M-I
V--
--
ISC
A123
Clin
icia
n(C
,P
,C
LIN
)C
urr
ent
45-9
0m
in(C
);120-1
5m
in(P
)D
SM
-IV
IR:
0.9
5--
AD
IS-C
124,1
25
Clin
icia
n(C
,P
,C
LIN
)C
urr
ent
--D
SM
-IV
(focus
on
anxie
tydis
ord
ers
)T
R:
0.8
0to
0.9
2IR
:0.8
0-1
.00
--
CA
PA
116,1
26,1
27
Clin
icia
n(C
,P
,C
LIN
)C
urr
ent
60
min
DS
M-I
V;
ICD
-10
TR
:0.7
4-0
.79
CO
NV
:0.2
3-0
.48
(DA
WB
A);
0.2
1-0
.61
(DIS
C-I
V)
PA
PA
128
Clin
icia
n(P
,C
LIN
);C
OM
P(P
,C
LIN
)C
urr
ent
100
min
DS
M-I
V;
ICD
-10
+R
DC
-PA
;D
C:
0-3
RT
R:
0.7
4--
CID
I-A
16,1
29
Lay
(C);
CO
MP
Curr
ent/lif
etim
e2.5
hours
(C)
DS
M-I
V;
ICD
-10
--C
ON
V:
Are
aU
nder
the
Curv
e.
0.7
9(K
SA
DS
-PL)
Ratin
gscale
sfo
rth
easse
ssm
ent
of
anxie
tysym
pto
ms
within
abro
ad
anxie
tyconstr
uct
Sca
leR
ate
rN
um
ber
of
item
sE
stim
ate
dtim
e
Psy
chom
etr
icpro
pert
ies
Relia
bili
tyV
alid
ityC
uto
ff
ST
AI-
C*
130,1
31
Self
20
(sta
te)
+20
(tra
it)20
min
----
--R
CM
AS*
132,1
33
Self
37
15
min
IC:
0.8
3-0
.85
*IC
:0.8
5*T
R:
0.8
8
----
BA
I-Y
134
Self
20
10
min
----
--
Rating
scale
sfo
rth
eassess
ment
of
anxie
tysym
pto
ms
of
various
anxie
tydim
ensio
ns
Sca
leR
ate
rItem
sE
stim
ate
dtim
eD
imensio
ns
of
evalu
atio
n
Psychom
etr
icpro
pert
ies
Relia
bili
tyV
alid
ityC
uto
ff
PA
RS
135,1
36
Clin
icia
n(C
,P
,C
LIN
)50
+7-ite
mseverity
scale
20-3
0m
inG
A;
SoA
;S
eA
IC:
0.6
4T
R:
0.5
5IR
:0.9
7
CO
NV
:0.6
1(C
GI-
S)
DIV
G:
0.1
8-0
.33
(CD
RS
)T
RE
AT
:8-1
0(8
4-9
4%
SE
NS
;82-9
0%
SP
EC
)
Continued
on
next
page
Pediatric anxiety disorders S11
Rev Bras Psiquiatr. 2013;35(Suppl 1)

Tab
le2
Continued
Rating
scale
sfo
rth
eassessm
ent
of
anxie
tysym
pto
ms
of
various
anxie
tydim
ensio
ns
Sca
leR
ate
rIt
em
sE
stim
ate
dtim
eD
imensio
ns
of
evalu
atio
n
Psychom
etr
icpro
pert
ies
Relia
bili
tyV
alid
ity
Cuto
ff
SC
AR
ED*
137-1
40
Self
and
pare
nt
41
15
min
GA
;P
AN
IC-S
OM
AT
;S
eA
;S
oA
;S
CH
OO
LIC
:0.9
0*IC
:0.9
0T
R:
0.8
6*T
R:
0.8
1
*C
ON
V:
0.8
1(M
AS
C)
*D
IVG
:0.5
8(C
DI)
DIS
CR
:anxie
tydis
ord
ers
vs.
oth
er
psyc
hia
tric
dis
ord
ers
*D
ISC
R:
anxie
tydis
ord
ers
vs.
contr
ol
DX
:o
26
(71%
SE
NS
;61-7
1%
SP
EC
)*D
X:o
23
(81.8
%S
EN
S;
52.0
%S
PE
C)
SC
AS*
141-1
43
Self
and
pare
nt
38
15
min
GA
;P
AN
IC-A
G;
SeA
;S
oA
;O
C;
FE
AR
S
IC:
0.9
2T
R:
0.6
0C
ON
V:
0.7
1(R
CM
AS
)D
IVG
:0.4
8(C
DI)
DIS
CR
:anxie
tydis
ord
ers
vs.
contr
ol
DX
:o
40
boys
ages
8-
11;o
33
boys
ages
12-
15;o
50
girls
ages
9-1
1;
o39
girls
ages
12-1
5M
AS
C144
Self
and
pare
nt
39
15
min
SO
MA
T;
HA
;S
eA
;S
oA
IC:
0.9
0T
R:
0.7
9-0
.93
CO
NV
:0.6
3(R
CM
AS
)D
IVG
:0.1
9(C
DI)
--
Rating
scale
sfo
rth
eassess
ment
of
anxie
tysym
pto
ms
of
aspecifi
canxie
tydim
ensio
n
Sca
leR
ate
rIt
em
sE
stim
ate
dtim
eD
imensio
nof
evalu
atio
n
Psychom
etr
icpro
pert
ies
Relia
bili
tyV
alid
ity
Cuto
ff
LS
AS
-CA
145
Clin
icia
n(C
,P
,C
LIN
)24
--S
oA
IC:
0.9
5-0
.97
TR
with
IR:
0.9
4C
ON
V:
0.7
5(S
PA
I-C
)D
IVG
:0.3
8(C
DR
S-R
)D
ISC
R:
soci
alphobia
vs.
oth
er
anxie
tydis
ord
ers
and
contr
ol
DX
:o
23
socia
lphobia
vs.
contr
ol(9
5.9
%S
EN
S;
100%
SP
EC
);o
30
socia
lphobia
vs.
oth
er
anxie
tydis
ord
ers
(91.8
%S
EN
S;
65.2
%S
PE
C)
SP
AI-
C*
146-1
49
Self
26
--S
oA
IC:
0.9
5/*0.9
4T
R:0.6
3-0
.86
/*0.7
8D
ISC
R:
socia
lphobia
vs.
contr
ol
*D
ISC
R:
soci
alphobia
vs.
contr
ol
DX
:o
19
(30%
FN
;26%
FP
)C
Y-B
OC
S150-1
52
Clin
icia
n(C
,P
,C
LIN
),self
and
pare
nt
81
+10-ite
mseve
rity
scale
--O
CIC
:0.8
7-0
.90
IR:
0.8
4T
R:
0.7
9
CO
NV
:0.6
2(L
OI-
CV
)D
IVG
:0.3
4(C
DI)
;0.3
7(C
MA
S)
TR
EA
T:
14
(91%
SE
NS
;90%
SP
EC
)
DY
BO
CS*
153
Clin
icia
n(C
,P
,C
LIN
)88
+3
item
seve
rity
for
each
OC
sym
pto
m
40
min
OC
D:
aggre
ssiv
e,
sym
metr
y,
conta
min
ation,
hoard
ing,
mis
cella
neous
IC:
.0.9
3IR
:.
0.9
8C
ON
V:
0.7
9(Y
BO
CS
)D
IVG
:lo
wP
ears
on
coeff
icie
nts
with
HA
M-A
,H
AM
-D,
YG
TS
S
--
FS
SC
-R154
Self
80
--F
EA
RS
IC:
0.9
4-0
.95
TR
:0.5
5-0
.82
CO
NV
:0.4
6-0
.51
(ST
AI-
C)
DIS
CR
:schoolphobia
vs.
contr
ol
--
AD
IS-C
=A
nxie
tyD
isord
ers
Inte
rvie
wS
chedule
for
Child
ren;A
G=
agora
phobia
;B
AI-
Y=
Beck
Anxie
tyIn
vento
ryfo
rY
outh
;C
=child
ren
as
info
rmant;
CA
PA
=C
hild
and
Adole
scentP
sychia
try
Ass
essm
ent;
CD
I=
Child
ren’s
Depre
ssio
nIn
vento
ry;
CD
RS
=C
hild
ren’s
Depre
ssio
nR
atin
gS
cale
;C
DR
S-R
=C
hild
ren’s
Depre
ssi
on
Ratin
gS
cale
,R
evis
ed;
CG
I-S
=C
linic
alG
lobal
Impre
ssio
n,
Severity
Sca
le;
ChIP
S=
Child
ren’s
Inte
rvie
wfo
rP
sychia
tric
Syndro
mes;
CID
I-A
=C
om
posite
Inte
rnationalD
iagnostic
Instr
um
ent,
Adole
scent
adapta
tion;
CLIN
=finalclin
icia
nim
pre
ssio
n;
CY
-BO
CS
=C
hild
ren
Yale
-Bro
wn
Obsessiv
e-C
om
puls
ive
Sca
le;
CO
MP
=com
pute
r-assi
ste
d;
CO
NV
=converg
ent;
DA
WB
A=
Develo
pm
ent
and
Wellb
ein
gA
ssessm
ent;
DIC
A=
Dia
gnostic
Inte
rvie
wfo
rC
hild
ren
and
Adole
scents
;D
ISC
-IV
=D
iagnostic
Inte
rvie
wS
chedule
for
Child
ren,
Fourt
hE
diti
on;
DIS
CR
=dis
crim
inant;
DIV
G=
div
erg
ent;
DX
=crite
ria
toth
edia
gnosis
of
pedia
tric
anxie
tydis
ord
ers
;D
YB
OC
S=
Dim
ensio
nalY
ale
-Bro
wn
Obsessiv
e-C
om
puls
ive
Sca
le;
FE
AR
S=
specifi
cphobia
s;F
SS
C-R
=F
ear
Surv
ey
Sch
edule
for
Child
ren,
Revis
ed;G
A=
genera
lized
anxie
ty;F
N=
fals
enegatives;F
P=
fals
epositiv
es;H
A=
harm
avoid
ance;H
AM
-A=
Ham
ilton
Anxie
tyR
ating
Scale
;H
AM
-D=
Ham
ilton
Depre
ssio
nR
ating
Scale
;IC
=in
tern
alconsis
tency;
IR=
inte
rrate
r;IS
CA
=In
terv
iew
Schedule
for
Child
ren
and
Adole
scents
;K
-SA
DS
-E=
Sch
edule
for
Aff
ective
Dis
ord
ers
and
Schiz
ophre
nia
for
Sch
ool-A
ge
Child
ren,
Epid
em
iolo
gic
Vers
ion;K
-SA
DS
-PL
=S
chedule
for
Aff
ectiv
eD
isord
ers
and
Sch
izophre
nia
for
Sch
ool-A
ge
Child
ren,P
resentand
Lifetim
eV
ers
ion;LO
I-C
V=
The
Leyto
nO
bsessio
nalI
nvento
ry,
Child
Vers
ion
Surv
ey
Form
;LS
AS
-CA
=Lie
bow
itz
Socia
lA
nxie
tyS
cale
for
Child
ren
and
Adole
scents
;M
AS
C=
Multi
dim
ensio
nalA
nxie
tyS
cale
for
Child
ren;
OC
=obsessio
ns-c
om
puls
ions;
OC
D=
obsessiv
e-c
om
puls
ive
dis
ord
er;
P=
pare
ntas
info
rmant;
PA
PA
=P
re-S
choolA
ge
Psychia
tric
Ass
essm
ent;
PA
NIC
=panic
att
acks;
PA
RS
=P
edia
tric
Anxie
tyR
ating
Sca
le;R
CM
AS
=R
evis
ed-C
hild
ren’s
Manifest
Anxie
tyS
cale
;R
DC
-PA
=R
esearc
hD
iagnostic
Crite
ria,
Pre
schoolA
ge;
SC
AR
ED
=S
cre
en
for
Child
Anxie
tyR
ela
ted
Em
otio
nalD
isord
ers
;S
CA
S=
Spence
Child
ren’s
Anxie
tyS
cale
;S
CH
OO
L=
schoolphobia
;S
eA
=separa
tion
anxie
ty;S
EN
S=
sensib
ility
;S
OM
AT
=som
atic/
physic
alsym
pto
ms;
SoA
=socia
lanxie
ty;S
PA
I-C
=S
ocia
lP
hobia
and
Anxie
tyIn
vento
ryfo
rC
hild
ren;
SP
EC
=specifi
city;
ST
AI-
C=
Sta
te-T
rait
Anxie
tyIn
vento
ryfo
rC
hild
ren;
T=
teacher
as
info
rmant;
TR
=te
st-
rete
st;
TR
EA
T=
crite
ria
tore
mis
sio
n/r
esponse
totr
eatm
ent;
Y-B
OC
S=
Yale
-Bro
wn
Obsessiv
e-C
om
puls
ive
Sca
le;
YG
TS
S=
Yale
Glo
balT
icS
everity
Sca
le.
*In
str
um
ent
with
publis
hed
refe
rence
of
transla
tion/c
ross-c
ultu
raladapta
tion
toB
razil
and
psyc
hom
etr
icpro
pert
ies
of
the
Bra
zili
an
vers
ion;
--In
form
ation
not
availa
ble
or
restr
icte
dto
the
instr
um
ent’s
manual.
GA Salum et al.S12
Rev Bras Psiquiatr. 2013;35(Suppl 1)

Regarding tricyclic antidepressants (TADs), one placebo-controlled study supported the effectiveness of clomipra-mine in the treatment of OCD,159 as did two studies inchildren with school refusal.30 The magnitude of medica-tion response can be quantified using various metrics.The so-called number-needed-to-treat (NNT) is emergingas a current standard. With this metric, estimates are thatapproximately four patients should be using the afore-mentioned drugs in the anxiety disorders treatment inorder to one to achieve clinical response rates (n=14studies/2,102 patients; medication 58.1% vs. placebo31.5%; RR = 1.9; NNT = 4).158 This represents a verystrong, robust clinical effect, relative to other conditions.For example, the NNT in either pediatric or adultdepression for most medication treatments is not half aspotent. There is evidence of the decrease in all anxietysymptoms with these medications. There is no directevidence that any of these medications offer betterresponses to treatment or are better tolerated.158
However, a mixed comparison meta-analysis found thatbetween SSRIs and venlafaxine, venlafaxine was lessefficacious than fluvoxamine and paroxetine and lesstolerated than fluvoxamine, paroxetine, and sertraline.160
Besides the SSRIs and venlafaxine, three studiesabout the use of imipramine among patients with anxietydisorders have demonstrated its effectiveness in non-OCD disorders.161 However, TADs are consideredsecondary choices due to their less favorable adverseeffects and the fact that they require continuous monitor-ing of blood and cardiac irregularities.158 There is noevidence supporting the use of benzodiazepines in thetreatment of pediatric anxiety disorders.162
It is vital to emphasize that psychoeducation is anessential part of the treatment of anxiety disorders.Psychoeducation includes the explanation of the char-acteristics of the symptoms, course, treatment strategies,potential side effects, duration of treatment, etc.Moreover, it is critical to verify that the patient is usingthe medication adequately. More frequent visits in thebeginning of the treatment (weekly, fortnightly) or aphone-based follow-up are good alternatives to ensureand increase treatment compliance. An algorithm tochoose among the therapeutic options is depicted inFigure 3. The most used first-line medications in thetreatment of anxiety disorders, their usage, and adverseeffects are shown in Table 3.
Psychotherapy
CBT is the approach with stronger evidence of effective-ness as compared to waiting lists or attention controlinterventions for both OCD163-165 and non-OCD pediatricanxiety disorders.164-166 The overall effect size of CBT forpediatric anxiety in a meta-analysis involving 48 studies(n=3,740) was 0.66 (compared to passive control 0.77and to active control 0.39; both significant), demonstrat-ing a key role of non-specific factors.164 The effect sizefor non-CBT interventions was not significant.164
Treatment target CBT (specific to one anxiety disorder)and individual treatments (as opposed to groups) had a
larger effect size than treatment targeting several anxietydisorders and group CBT.164 Clinical trials have alsoshown that CBT may have better results for treating OCDwhen family members are involved to reduce the levels offamily accommodation (the different ways that familymembers may respond to the patient’s symptoms byfacilitating avoidance, assisting on ritualistic behaviors, orinadvertently participating in rituals).167
Combined treatment
Two large studies have evaluated the combined treatmentas compared to the monotherapy and placebo compo-nents.108,168 For non-OCD anxiety disorders, theCBT+sertraline combined treatment was more effectivethan both monotherapy conditions and the placebocondition.108 For OCD, the combined treatment was moreeffective than the sertraline monotherapy and the placeboconditions, but there was no difference between thecombined treatment and the CBT monotherapy.168 Datafrom this study investigating moderator factors of thesetherapy conditions have demonstrated that, for patientswith a family history of OCD, the combined treatment or thesertraline monotherapy condition are preferable.169
Conversely, for patients with comorbid OCD and ticdisorders - a frequent comorbidity -, the combinedtreatment or the CBT are preferable.170 Moreover, inthese cases, the combination of SSRI and alpha-adrener-gic agonists or anti-psychotics might be an option.171
Other treatments and future perspectives
Innovative treatments for anxiety disorders have beendeveloped from the neuroscience field, such as the d-cycloserine combined with behavioral techniques172 andthe attentional bias modification treatment.173,174
Regulators of glutamatergic neurotransmission, such asriluzole175 and N-acetylcysteine,176 have also beenexamined in adolescents diagnosed with OCD.Although promising, these treatments do not yet presentlong-term outcomes and are currently restricted toresearch settings.
Studies in adults and children have demonstrated thatinterventions focusing on the individual’s lifestyle, such asphysical exercise, are associated with improvements inanxiety and depressive symptoms,177-179 and exerciseshould be encouraged. Evidence from studies with adultsamples have also stated that complementary treatmentswith kava,180 valerian,181 passiflora,182 meditation,183 orhealing touch184 have inconclusive benefits in thetreatment of anxiety disorders, with not enough evidenceto recommend their use.
Monitoring, refractoriness, referring
Due to the unfavorable natural history of anxiety disorders,it is highly important to monitor anxiety symptoms andpotential side effects objectively and systematically.185
Some studies have suggested that SSRI treatments mightlead to an increase in suicidality among children. Further
Pediatric anxiety disorders S13
Rev Bras Psiquiatr. 2013;35(Suppl 1)

Figure 3 Algorithm for the management of pediatric anxiety disorders (based on Salum et al.107). CBT = cognitive behavioraltherapy; GAD = generalized anxiety disorder; OCD = obsessive-compulsive disorder; PD = panic disorder; PTSD =posttraumatic stress disorder; SeAD = separation anxiety disorder; SoAD = social anxiety disorder; SP = specific phobias;SNRI = serotonin and norepinephrine reuptake inhibitor; SSRI = selective serotonin reuptake inhibitor
GA Salum et al.S14
Rev Bras Psiquiatr. 2013;35(Suppl 1)

Tab
le3
Main
dru
gs
used
inth
etr
eatm
ent
of
pedia
tric
anxie
tydis
ord
ers
Dru
g(G
RA
DE
)
Dru
guse
recom
mendations
Child
/Adole
sc
,12
years
OR
Adole
sco
12
years
with
low
weig
ht
Dru
guse
recom
mendatio
ns
Adole
sc
with
norm
alw
eig
ht
OR
Child
ren
with
OC
DM
ain
chara
cte
ristics
(advanta
ges/
dis
adva
nta
ges)
SS
RI
Indic
ations:
non-O
CD
anxie
tydis
ord
ers
(GA
D,
SoA
D,
SeA
D)
+P
Dand
OC
DC
ontr
a-indic
ations:
MA
OI
use,
pim
ozid
euse,
hypers
ensi
tivity
toth
edru
gM
ost
com
mon
advers
eeff
ects
of
the
cla
ss:
nause
a,headache,dro
wsin
ess,in
som
nia
,diz
zin
ess,decre
ased
appetite
,abdom
inalpain
,nerv
ousness,exce
ssiv
esw
eatin
g,
dry
mouth
,tr
em
or,
decre
ased
sexu
aldesire,
dela
yed
eja
cula
tion,
anorg
asm
ia,
restle
ssness,
asth
enia
,abnorm
alpla
tele
taggre
gation,
and
ble
edin
g.
Flu
oxetine
(B)
Pill
s:
10
and
20
mg
Ora
lsolu
tion:
20
mg/m
L
Reco
mm
endatio
n:
start
with
asi
ngle
dose
of
5m
g/d
ay
inth
em
orn
ing
mealfo
r1
week,
incr
ease
to10
mg/d
ay
and
wait
for
thera
peutic
resp
onse
(4-6
weeks
),w
ithin
crease
sin
dose
(+5
mg/d
ay
each
week)
acc
ord
ing
tocl
inic
alre
sponse
and
tole
rance
until
the
maxi
mum
dose
of20-3
0m
g/d
ay,
acc
ord
ing
toage
and
weig
ht.
Recom
mendation:
sta
rtw
ith
asin
gle
dose
of
10
mg/d
ay
inth
em
orn
ing
mealfo
r1
week,
incre
ase
to20
mg/d
ay
and
wait
for
thera
peutic
response
(4-6
weeks),
with
incre
ases
indose
(+10
mg/d
ay
each
week)
accord
ing
toclin
icalre
sponse
and
tole
rance
untilth
em
axi
mum
dose
of
40-6
0m
g/d
ay,
acco
rdin
gto
age
and
weig
ht.
-C
om
ple
xm
eta
boliz
atio
n(inhib
itsp450
CY
P2D
6and
CY
P3A
4)
-A
mong
SS
RIs
,it
isth
elo
ngest
HL
(HL
=4-6
days
;m
eta
bolit
e=
4-1
6days
)-
Am
ong
SS
RIs
,it
isth
em
ost
stim
ula
nt
-In
gestio
nw
ith
food
reduces
nausea
-A
ppro
ved
by
the
FD
Afo
rdepre
ssio
nand
OC
Din
child
ren
Flu
voxam
ine
(A)
Pill
s:
100
mg
Reco
mm
endatio
n:
start
with
asi
ngle
dose
of
25
mg/d
ay
atnig
htm
eals
(no
chew
ing),
incr
ease
to50
mg/d
ay
and
wait
for
thera
peutic
resp
onse
(4-6
weeks
),w
ithin
crease
sin
dose
(+25
mg/d
ay
each
week)
acc
ord
ing
tocl
inic
alre
sponse
and
tole
rance
until
the
maxi
mum
of200
mg/d
ay,
acc
ord
ing
toage
and
weig
ht.
Ifa
dosa
ge
hig
her
than
50
mg/d
ay
isnece
ssary
,th
edaily
dose
should
be
div
ided
intw
o(larg
er
part
at
nig
ht)
.
Recom
mendation:
sta
rtw
ith
asin
gle
dose
of
50
mg/d
ay
at
nig
ht,
incre
ase
to100
mg/d
ay
and
wait
for
thera
peutic
response
(4-6
weeks),
with
incre
ases
indose
(+50
mg/d
ay
each
week)
acco
rdin
gto
clin
icalre
sponse
and
tole
rance
until
the
maxi
mum
dose
of
300
mg/d
ay,
accord
ing
toage
and
weig
ht.
Ifa
dosage
hig
her
than
100
mg/d
ay
isnecessary
,th
edaily
dose
should
be
div
ided
intw
o,
with
the
larg
er
part
at
nig
ht.
-D
rug
absorp
tion
incre
ase
sw
hen
ingeste
dw
ith
food
(but
itshould
not
be
chew
ed)
-S
hort
HL
=15
hours
(in
hig
her
dosage,it
must
be
used
intw
odaily
dose
s).
-It
pre
sents
are
lativ
epro
babili
tyof
causin
gw
ithdra
walsyndro
me
Paro
xetine
(C)
Pill
s:
10,
20,
and
30
mg
Recom
mendatio
n:
sta
rtw
ith
asin
gle
dose
of
5m
g/d
ay
inth
em
orn
ing
for
1w
eek,
incre
ase
to10
mg/d
ay
and
wait
for
thera
peutic
response
(4-6
weeks),
with
incre
ases
indose
(+5
mg/d
ay
each
week)
accord
ing
toclin
icalre
sponse
and
tole
rance
untilth
em
axi
mum
dose
of
50-6
0m
g/d
ay,
acco
rdin
gto
age
and
weig
ht.
Recom
mendation:
sta
rtw
ith
asin
gle
dose
of
10
mg/d
ay
inth
em
orn
ing
for
1w
eek,
incre
ase
to20
mg/d
ay
and
wait
for
thera
peutic
response
(4-6
weeks),
with
incre
ase
sin
dose
(+5
mg/d
ay
each
week)
acco
rdin
gto
clin
icalre
sponse
and
tole
rance
untilth
em
axi
mum
dose
of
40-6
0m
g/d
ay,
acco
rdin
gto
age
and
weig
ht.
-C
om
ple
xm
eta
boliz
ation
(substa
ntially
inhib
itsp450
[CY
P2D
6])
-A
mong
SS
RIs
,it
isth
ele
ss
stim
ula
ntand
the
most
sedative
-A
mong
SS
RIs
,it
isth
eone
with
more
anticholin
erg
iceffects
-S
hort
HL
=21
hours
(with
dra
walsyndro
me)
Sert
ralin
e(A
)P
ills:
25,
50,
and
100
mg
Reco
mm
endatio
n:
start
with
asi
ngle
dose
of
12.5
mg/d
ay
inth
em
orn
ing
mealfo
r1-2
weeks
,in
crease
to25
mg/d
ay
and
wait
for
thera
peutic
resp
onse
(4-6
weeks
),w
ithin
crease
sin
dose
(+12.5
mg/d
ay
each
week)
acc
ord
ing
tocl
inic
al
resp
onse
and
tole
rance
until
the
maxi
mum
dose
of
200
mg/d
ay,
acc
ord
ing
toage
and
weig
ht.
Recom
mendation:
sta
rtw
ith
asin
gle
dose
of
25
mg/d
ay
inth
em
orn
ing
mealfo
r1-2
weeks,
incre
ase
to50
mg/d
ay
and
wait
for
thera
peutic
response
(4-6
weeks),
with
incre
ases
indose
(+25
mg/d
ay
each
week)
accord
ing
toclin
ical
response
and
tole
rance
untilth
em
axim
um
dose
of
200
mg/d
ay,
accord
ing
toage
and
weig
ht.
-F
ew
dru
gin
tera
ctio
ns
(few
eff
ects
p450
[CY
P2D
6]a
nd
min
imum
effect
sp450
[CY
P3A
4])
-A
mong
SS
RIs
,it
isth
eone
thatm
ost
causes
nause
a-
Itcan
be
stim
ula
nt
-D
rug
absorp
tion
incre
ase
sw
hen
ingeste
dw
ith
food
-A
vera
ge
HL
=26
hours
(+m
eta
bolit
e64-1
04
hours
)
SN
RI
Indic
ations:
non-O
CD
anxie
tydis
ord
ers
(GA
D,
SoA
D,
SeA
D)
Contr
ain
dic
ations:
hypers
ensiti
vity
toM
AO
IM
ost
com
mon
advers
eeffects
:w
eig
ht
loss,
nause
a,
insom
nia
,tr
em
or,
sexualdysf
unction,
sw
eatin
g,
dry
mouth
,ble
edin
g,
hig
hblo
od
pre
ssure
.
Venla
faxin
eIR
(D)
(im
media
tere
lease)
Venla
faxin
eX
R(C
)(e
xte
nded
rele
ase)
Pill
s:
37.5
,75,
and
150
mg
Recom
mendatio
n:
sta
rtw
ith
adose
of
37.5
mg/d
ay
for
1-2
weeks,
incre
ase
to75
mg/d
ay
and
wait
for
thera
peutic
response
(4-6
weeks),
with
incre
ases
indose
(+37.5
mg/d
ay
each
week)
acco
rdin
gto
clin
icalre
sponse
and
tole
rance
untilth
em
axim
um
dose
of
112.5
mg/d
ay,
accord
ing
toage
and
weig
ht.
Imm
edia
tere
lease:
2daily
doses.
Ext
ended
rele
ase:
sin
gle
dose
(in
the
morn
ing).
Recom
mendation:
sta
rtw
ith
adose
of
37.5
mg/d
ay
for
1w
eek,
incre
ase
to75
mg/d
ay
and
wait
for
thera
peutic
response
(4-6
weeks),
with
incre
ases
indose
(+37.5
mg/d
ay
each
week)
accord
ing
toclin
icalre
sponse
and
tole
rance
untilth
em
axi
mum
dose
of
225
mg/d
ay,
accord
ing
toage
and
weig
ht.
Imm
edia
tere
lease:
2daily
doses.
Ext
ended
rele
ase:
sin
gle
dose
(in
the
morn
ing).
-M
inim
um
effects
p450
-F
requent
withdra
walsyndro
me
Incre
ase
inart
erialp
ressure
(when
dosage
ishig
her
than
225
mg)
-It
isim
port
antt
om
onito
rgro
wth
and
weig
htl
oss
-T
here
isno
evid
ence
of
eff
ectiveness
inpedia
tric
OC
D-
Ext
ended
rele
ase
(XR
)dru
gs
cannotb
ediv
ided
Based
on
Salu
met
al.
107
FD
A=
Food
and
Dru
gA
dm
inis
tration;
GA
D=
genera
lized
anxie
tydis
ord
er;
HL
=half
lifetim
e;
MA
OI
=m
onoam
ine
oxid
ase
inhib
itors
;O
CD
=obsessiv
e-c
om
puls
ive
dis
ord
er;
PD
=panic
dis
ord
er;
SeA
D=
separa
tion
anxie
tydis
ord
er;
SN
RI
=sero
tonin
and
nore
pin
ephrine
reupta
kein
hib
itor;
SoA
D=
socia
lanxie
tydis
ord
er;
SS
RIs
=sele
ctiv
esero
tonin
reupta
ke
inhib
itors
.R
efe
rence
s:U
pT
oD
ate
Onlin
eP
edia
tric
Dru
gIn
form
atio
n(h
ttp://w
ww
.upto
date
.com
).E
vidence
was
eva
luate
dth
rough
the
GR
AD
Equalit
ysy
stem
(A=
hig
h;B
=m
odera
te;C
=lo
w;D
=ve
rylo
w).
Pediatric anxiety disorders S15
Rev Bras Psiquiatr. 2013;35(Suppl 1)

studies have demonstrated that the benefits of treatinganxiety disorders largely outweigh the potential risksrelated to the increase of suicidal ideation, which, althoughserious, is a rare event in the treatment of patients withanxiety disorders.186 Nevertheless we underscore theneed to monitor continuously suicidal thoughts and suicidalbehaviors in this population.
There is a lack of consistent evidence regarding thebest way to deal with refractory anxiety disorders or thebest sequence of treatments to be applied. Overall, therecommendation is to optimize the medication dosage,since some patients only respond at higher doses (e.g.,slow metabolizers, OCD patients). If there is no responseafter 4 to 6 weeks of treatment and after the dosageoptimization, it is possible to: 1) change medicationswithin the same class (e.g., fluoxetine for sertraline) or 2)change the previous medication for another one from adifferent class (e.g., fluoxetine for venlafaxine).187
In public health systems, specialized treatment isrecommended in cases in which: 1) patients have shownrefractoriness to two previous therapeutic alternatives; 2)patients have severe chronic disorders, including highlevel of impairment, unusually frequent avoidance beha-viors and agoraphobia that do not respond to psycho-tropic and clearly require behavioral therapy or CBT; and3) patients present persistent suicidal ideation.
Preschool children treatment and prevention
Most of the currently available evidence regarding thetreatment of pediatric anxiety disorders is based onstudies with school-aged children. However, there is acurrent trend to offer treatment for younger children(preschoolers), hoping that earlier diagnoses may pre-vent later psychiatric disorders. Parental training withCBT protocols and the treatment of mood and anxietydisorders in clinically-ill parents are suggested by someauthors.188 Although scarce, there is promising evidencethat treatments based on existing therapies (CBT,parental training, and pharmacotherapy), adapted to at-risk populations, i.e., highly symptomatic children, but stillnot meeting criteria for the diagnosis of anxiety disorders,or children with first-degree relatives diagnosed withanxiety disorders, result in preventing and reducing theseverity of these disorders.189
This is a general overview about pediatric anxietydisorders. More specific and comprehensive reviewsabout the following topics can be found in the literature:prevalence,15,18-20 behavioral inhibition,190-192 behavioralgenetics,48,52 genetics,55,56,193,194 gene vs. environmentinterplay,52,70 pathophysiology,31,71 neural substrates,71
normal development of fears,195 psychopharmacologicaltreatment,196-198 and CBT.164,199-201
Conclusions
Anxiety disorders are prevalent, associated with anumber of negative life outcomes, and currently under-recognized and under-treated. The etiology involves bothgenes and environmental factors in a complex interplay.
Pathophysiology is still in its infancy, but some brainregions such as the amygdala and the prefrontal cortexpotentially play a key role to explain individual differencesrelated to fear and anxiety. The diagnosis is clinical andinvolves clinical interviews with the child, parents, andteachers. Treatment is effective using medication, CBT,or a combination of strategies.
Disclosure
Giovanni Abrahao Salum receives a post-doctoral fellow-ship from Coordenacao de Aperfeicoamento de Pessoalde Nıvel Superior (CAPES) and Fundacao de Amparo aPesquisa do Estado do Rio Grande do Sul (FAPERGS).Diogo Araujo DeSouza receives a doctoral fellowshipfrom Conselho Nacional de Desenvolvimento Cientıfico eTecnologico (CNPq). Maria Conceicao do Rosarioreceives research support from Brazilian governmentinstitutions (CNPq) and has worked in the last 5 years asa speaker for the companies Novartis and Shire. DanielPine declares no potential conflicts of interest. Gisele GusManfro receives research support from Brazilian govern-ment institutions (CNPq, FAPERGS and Fundo deIncentivo a Pesquisa - Hospital de Clınicas de PortoAlegre - FIPE-HCPA).
References
1 Woodward LJ, Fergusson DM. Life course outcomes of youngpeople with anxiety disorders in adolescence. J Am Acad ChildAdolesc Psychiatry. 2001;40:1086-93.
2 Essau CA, Conradt J, Petermann F. Frequency, comorbidity, andpsychosocial impairment of anxiety disorders in German adoles-cents. J Anxiety Disord. 2000;14:263-79.
3 Ezpeleta L, Keeler G, Erkanli A, Costello EJ, Angold A.Epidemiology of psychiatric disability in childhood and adolescence.J Child Psychol Psychiatry. 2001;42:901-14.
4 Balazs J, Miklosi M, Kereszteny A, Hoven CW, Carli V, WassermanC, et al. Adolescent subthreshold-depression and anxiety: psycho-pathology, functional impairment and increased suicide risk. J ChildPsychol Psychiatry. 2013;54:670-7.
5 Last CG, Hansen C, Franco N. Anxious children in adulthood: aprospective study of adjustment. J Am Acad Child AdolescPsychiatry. 1997;36:645-52.
6 Olatunji BO, Cisler JM, Tolin DF. Quality of life in the anxietydisorders: a meta-analytic review. Clin Psychol Rev. 2007;27:572-81.
7 Nock MK, Hwang I, Sampson NA, Kessler RC. Mental disorders,comorbidity and suicidal behavior: results from the NationalComorbidity Survey Replication. Mol Psychiatry. 2010;15:868-76.
8 Roest AM, Martens EJ, de Jonge P, Denollet J. Anxiety and risk ofincident coronary heart disease: a meta-analysis. J Am Coll Cardiol.2010;56:38-46.
9 Baldwin DS, Pallanti S, Zwanzger P. Developing a Europeanresearch network to address unmet needs in anxiety disorders.Neurosci Biobehav Rev. 2013 Jan 10. [Epub ahead of print]
10 Ranta K, Kaltiala-Heino R, Rantanen P, Marttunen M. Social phobiain Finnish general adolescent population: prevalence, comorbidity,individual and family correlates, and service use. Depress Anxiety.2009;26:528-36.
11 Merikangas KR, He JP, Brody D, Fisher PW, Bourdon K, KoretzDS. Prevalence and treatment of mental disorders among USchildren in the 2001-2004 NHANES. Pediatrics. 2010;125:75-81.
12 Chavira DA, Stein MB, Bailey K, Stein MT. Child anxiety in primarycare: prevalent but untreated. Depress Anxiety. 2004;20:155-64.
13 Wren FJ, Scholle SH, Heo J, Comer DM. Pediatric mood andanxiety syndromes in primary care: who gets identified? Int JPsychiatry Med. 2003;33:1-16.
GA Salum et al.S16
Rev Bras Psiquiatr. 2013;35(Suppl 1)

14 Rutter M. Research review: child psychiatric diagnosis andclassification: concepts, findings, challenges and potential. J ChildPsychol Psychiatry. 2011;52:647-60.
15 Beesdo-Baum K, Knappe S. Developmental epidemiology ofanxiety disorders. Child Adolesc Psychiatr Clin N Am.2012;21:457-78.
16 Merikangas KR, He JP, Burstein M, Swanson SA, Avenevoli S, CuiL, et al. Lifetime prevalence of mental disorders in U.S. adoles-cents: results from the National Comorbidity Survey Replication--Adolescent Supplement (NCS-A). J Am Acad Child AdolescPsychiatry. 2010;49:980-9.
17 Rapee RM, Schniering CA, Hudson JL. Anxiety disorders duringchildhood and adolescence: origins and treatment. Annu Rev ClinPsychol. 2009;5:311-41.
18 Costello EJ, Egger HL, Angold A. The developmental epidemiologyof anxiety disorders: phenomenology, prevalence, and comorbidity.Child Adolesc Psychiatr Clin N Am. 2005;14:631-48.
19 Beesdo K, Knappe S, Pine DS. Anxiety and anxiety disorders inchildren and adolescents: developmental issues and implicationsfor DSM-V. Psychiatr Clin North Am. 2009;32:483-524.
20 Baxter AJ, Scott KM, Vos T, Whiteford HA. Global prevalence ofanxiety disorders: a systematic review and meta-regression.Psychol Med. 2013;43:897-910.
21 Somers JM, Goldner EM, Waraich P, Hsu L. Prevalence andincidence studies of anxiety disorders: a systematic review of theliterature. Can J Psychiatry. 2006;51:100-13.
22 Adornetto C, Suppiger A, In-Albon T, Neuschwander M, SchneiderS. Concordances and discrepancies between ICD-10 and DSM-IVcriteria for anxiety disorders in childhood and adolescence. ChildAdolesc Psychiatry Ment Health. 2012;6:40.
23 Salum GA, Isolan LR, Bosa VL, Tocchetto AG, Teche SP, Schuch I,et al. The multidimensional evaluation and treatment of anxiety inchildren and adolescents: rationale, design, methods and prelimin-ary findings. Rev Bras Psiquiatr. 2011;33:181-95.
24 Baxter AJ, Charlson FJ, Somerville AJ, Whiteford HA. Mentaldisorders as risk factors: assessing the evidence for the GlobalBurden of Disease Study. BMC Med. 2011;9:134.
25 Anselmi L, Fleitlich-Bilyk B, Menezes AM, Araujo CL, Rohde LA.Prevalence of psychiatric disorders in a Brazilian birth cohort of 11-year-olds. Soc Psychiatry Psychiatr Epidemiol. 2010;45:135-42.
26 Fleitlich-Bilyk B, Goodman R. Prevalence of child and adolescentpsychiatric disorders in southeast Brazil. J Am Acad Child AdolescPsychiatry. 2004;43:727-34.
27 Craske MG. Origins of phobias and anxiety disorders: why morewomen than men? Amsterdam: Elsevier; 2003.
28 American Psychiatric Association. Diagnostic and statistical manualof mental disorders - DSM-IV-TRH. 4th ed. Arlington: AmericanPsychiatric Publishing; 1994.
29 Gregory AM, Caspi A, Moffitt TE, Koenen K, Eley TC, Poulton R.Juvenile mental health histories of adults with anxiety disorders. AmJ Psychiatry. 2007;164:301-8.
30 Pine DS, Klein RG. Anxiety disorders. In: Rutter M, Bishop DVM,Pine DS, Scott S, Stevenson J, Taylor E, Thapar A , editors.Rutter’s child and adolescent psychiatry. 5th ed. Oxford: BlackwellPublishing Ltd; 2009. p. 628-647.
31 Pine DS. Research review: a neuroscience framework for pediatricanxiety disorders. J Child Psychol Psychiatry. 2007;48:631-48.
32 Wittchen HU, Lieb R, Pfister H, Schuster P. The waxing and waningof mental disorders: evaluating the stability of syndromes of mentaldisorders in the population. Compr Psychiatry. 2000;41:122-32.
33 Kessler RC, Avenevoli S, Costello EJ, Georgiades K, Green JG,Gruber MJ, et al. Prevalence, persistence, and sociodemographiccorrelates of DSM-IV disorders in the National Comorbidity SurveyReplication Adolescent Supplement. Arch Gen Psychiatry.2012;69:372-80.
34 Pine DS, Cohen P, Gurley D, Brook J, Ma Y. The risk for early-adulthood anxiety and depressive disorders in adolescents withanxiety and depressive disorders. Arch Gen Psychiatry.1998;55:56-64.
35 Copeland WE, Shanahan L, Costello EJ, Angold A. Childhood andadolescent psychiatric disorders as predictors of young adultdisorders. Arch Gen Psychiatry. 2009;66:764-72.
36 Bittner A, Egger HL, Erkanli A, Jane Costello E, Foley DL, Angold A.What do childhood anxiety disorders predict? J Child PsycholPsychiatry. 2007;48:1174-83.
37 Angst J, Vollrath M. The natural history of anxiety disorders. ActaPsychiatr Scand. 1991;84:446-52.
38 Beesdo K, Pine DS, Lieb R, Wittchen HU. Incidence and riskpatterns of anxiety and depressive disorders and categorization ofgeneralized anxiety disorder. Arch Gen Psychiatry. 2010;67:47-57.
39 Last CG, Perrin S, Hersen M, Kazdin AE. A prospective study ofchildhood anxiety disorders. J Am Acad Child Adolesc Psychiatry.1996;35:1502-10.
40 Pine DS, Cohen P, Brook J. Adolescent fears as predictors ofdepression. Biol Psychiatry. 2001;50:721-4.
41 Kim-Cohen J, Caspi A, Moffitt TE, Harrington H, Milne BJ, PoultonR. Prior juvenile diagnoses in adults with mental disorder:developmental follow-back of a prospective-longitudinal cohort.Arch Gen Psychiatry. 2003;60:709-17.
42 Colman I, Wadsworth ME, Croudace TJ, Jones PB. Forty-yearpsychiatric outcomes following assessment for internalizing dis-order in adolescence. Am J Psychiatry. 2007;164:126-33.
43 Scholten WD, Batelaan NM, van Balkom AJ, Wjh Penninx B, SmitJH, van Oppen P. Recurrence of anxiety disorders and itspredictors. J Affect Disord. 2013;147:180-5.
44 Insel TR. Disruptive insights in psychiatry: transforming a clinicaldiscipline. J Clin Invest. 2009;119:700-5.
45 Insel TR, Quirion R. Psychiatry as a clinical neuroscience discipline.JAMA. 2005;294:2221-4.
46 Levitt P, March J. NIMH Council Workgroup on Neurodevelopment:Update on Activities and Workgroup Recommendations. Bethesda,MD: 2008.
47 Skre I, Onstad S, Edvardsen J, Torgersen S, Kringlen E. A familystudy of anxiety disorders: familial transmission and relationship tomood disorder and psychoactive substance use disorder. ActaPsychiatr Scand. 1994;90:366-74.
48 Gregory AM, Eley TC. Genetic influences on anxiety in children:what we’ve learned and where we’re heading. Clin Child FamilyPsychol Rev. 2007;10:199-212.
49 Hettema JM, Neale MC, Kendler KS. A review and meta-analysis ofthe genetic epidemiology of anxiety disorders. American JPsychiatry. 2001;158:1568-78.
50 Topolski TD, Hewitt JK, Eaves L, Meyer JM, Silberg JL, Simonoff E,et al. Genetic and environmental influences on ratings of manifestanxiety by parents and children. J Anxiety Disord. 1999;13:371-97.
51 Hettema JM, Prescott CA, Myers JM, Neale MC, Kendler KS. Thestructure of genetic and environmental risk factors for anxietydisorders in men and women. Arch Gen Psychiatry. 2005;62:182-9.
52 Franic S, Middeldorp CM, Dolan CV, Ligthart L, Boomsma DI.Childhood and adolescent anxiety and depression: beyond herit-ability. J Am Acad Child Adolesc Psychiatry. 2010;49:820-9.
53 Rommelse NN, Franke B, Geurts HM, Hartman CA, Buitelaar JK.Shared heritability of attention-deficit/hyperactivity disorder andautism spectrum disorder. Eur Child Adolesc Psychiatry.2010;19:281-95.
54 Lahey BB, Van Hulle CA, Singh AL, Waldman ID, Rathouz PJ.Higher-order genetic and environmental structure of prevalentforms of child and adolescent psychopathology. Arch GenPsychiatry. 2011;68:181-9.
55 Sakolsky DJ, McCracken JT, Nurmi EL. Genetics of pediatric anxietydisorders. Child Adolesc Psychiatr Clin N Am. 2012;21:479-500.
56 McGrath LM, Weill S, Robinson EB, Macrae R, Smoller JW.Bringing a developmental perspective to anxiety genetics. DevPsychopathol. 2012;24:1179-93.
57 Erhardt A, Czibere L, Roeske D, Lucae S, Unschuld PG, Ripke S,et al. TMEM132D, a new candidate for anxiety phenotypes:evidence from human and mouse studies. Mol Psychiatry.2011;16:647-63.
58 Otowa T, Tanii H, Sugaya N, Yoshida E, Inoue K, Yasuda S, et al.Replication of a genome-wide association study of panic disorder ina Japanese population. J Hum Genet. 2010;55:91-6.
59 Otowa T, Yoshida E, Sugaya N, Yasuda S, Nishimura Y, Inoue K,et al. Genome-wide association study of panic disorder in theJapanese population. J Hum Genet. 2009;54:122-6.
Pediatric anxiety disorders S17
Rev Bras Psiquiatr. 2013;35(Suppl 1)

60 Stewart SE, Yu D, Scharf JM, Neale BM, Fagerness JA, MathewsCA, et al. Genome-wide association study of obsessive-compulsivedisorder. Mol Psychiatry. 2012 Aug 14. [Epub ahead of print]
61 Logue MW, Baldwin C, Guffanti G, Melista E, Wolf EJ, Reardon AF,et al. A genome-wide association study of post-traumatic stressdisorder identifies the retinoid-related orphan receptor alpha(RORA) gene as a significant risk locus. Mol Psychiatry. 2012Aug 7. [Epub ahead of print]
62 Gregersen N, Dahl HA, Buttenschon HN, Nyegaard M, HedemandA, Als TD, et al. A genome-wide study of panic disorder suggeststhe amiloride-sensitive cation channel 1 as a candidate gene. Eur JHum Genet. 2012;20:84-90.
63 Otowa T, Kawamura Y, Nishida N, Sugaya N, Koike A, Yoshida E,et al. Meta-analysis of genome-wide association studies for panicdisorder in the Japanese population. Transl Psychiatry.2012;2:e186.
64 Kawamura Y, Otowa T, Koike A, Sugaya N, Yoshida E, Yasuda S,et al. A genome-wide CNV association study on panic disorder in aJapanese population. J Hum Genet. 2011;56:852-6.
65 Lau JY, Gregory AM, Goldwin MA, Pine DS, Eley TC. Assessinggene-environment interactions on anxiety symptom subtypesacross childhood and adolescence. Dev Psychopathol.2007;19:1129-46.
66 Hicks BM, DiRago AC, Iacono WG, McGue M. Gene-environmentinterplay in internalizing disorders: consistent findings across sixenvironmental risk factors. J Child Psychol Psychiatry.2009;50:1309-17.
67 Narusyte J, Neiderhiser JM, D’Onofrio BM, Reiss D, Spotts EL,Ganiban J, et al. Testing different types of genotype-environmentcorrelation: an extended children-of-twins model. Dev Psychol.2008;44:1591-603.
68 Kendler KS, Baker JH. Genetic influences on measures of theenvironment: a systematic review. Psychol Med. 2007;37:615-26.
69 Kendler KS. Parenting: a genetic-epidemiologic perspective. Am JPsychiatry. 1996;153:11-20.
70 Rutter M, Moffitt TE, Caspi A. Gene-environment interplay andpsychopathology: multiple varieties but real effects. J Child PsycholPsychiatry. 2006;47:226-61.
71 Blackford JU, Pine DS. Neural substrates of childhood anxietydisorders: a review of neuroimaging findings. Child AdolescPsychiatr Clin N Am. 2012;21:501-25.
72 Shechner T, Britton JC, Perez-Edgar K, Bar-Haim Y, Ernst M, FoxNA, et al. Attention biases, anxiety, and development: toward oraway from threats or rewards? Depress Anxiety. 2012;29:282-94.
73 Britton JC, Lissek S, Grillon C, Norcross MA, Pine DS.Development of anxiety: the role of threat appraisal and fearlearning. Depress Anxiety. 2011;28:5-17.
74 Lissek S. Toward an account of clinical anxiety predicated on basic,neurally mapped mechanisms of Pavlovian fear-learning: the casefor conditioned overgeneralization. Depress Anxiety. 2012;29:257-63.
75 Kheirbek MA, Klemenhagen KC, Sahay A, Hen R. Neurogenesisand generalization: a new approach to stratify and treat anxietydisorders. Nat Neurosci. 2012;15:1613-20.
76 Guyer AE, Lau JY, McClure-Tone EB, Parrish J, Shiffrin ND,Reynolds RC, et al. Amygdala and ventrolateral prefrontal cortexfunction during anticipated peer evaluation in pediatric socialanxiety. Arch Gen Psychiatry. 2008;65:1303-12.
77 Guyer AE, Choate VR, Detloff A, Benson B, Nelson EE, Perez-Edgar K, et al. Striatal functional alteration during incentiveanticipation in pediatric anxiety disorders. Am J Psychiatry.2012;169:205-12.
78 Guyer AE, Nelson EE, Perez-Edgar K, Hardin MG, Roberson-NayR, Monk CS, et al. Striatal functional alteration in adolescentscharacterized by early childhood behavioral inhibition. J Neurosci.2006;26:6399-405.
79 Mana S, Paillere Martinot ML, Martinot JL. Brain imaging findings inchildren and adolescents with mental disorders: a cross-sectionalreview. Eur Psychiatry. 2010;25:345-54.
80 Milad MR, Rauch SL. Obsessive-compulsive disorder: beyondsegregated cortico-striatal pathways. Trends Cogn Sci. 2012;16:43-51.
81 Rapee RM. Potential role of childrearing practices in the develop-ment of anxiety and depression. Clin Psychol Rev. 1997;17:47-67.
82 McLeod BD, Wood JJ, Weisz JR. Examining the associationbetween parenting and childhood anxiety: a meta-analysis. ClinPsychol Rev. 2007;27:155-72.
83 Allen JL, Rapee RM, Sandberg S. Severe life events and chronicadversities as antecedents to anxiety in children: a matched controlstudy. J Abnorm Child Psychol. 2008;36:1047-56.
84 Eley TC, Stevenson J. Specific life events and chronic experiencesdifferentially associated with depression and anxiety in young twins.J Abnorm Child Psychol. 2000;28:383-94.
85 Murray L, Creswell C, Cooper PJ. The development of anxietydisorders in childhood: an integrative review. Psychol Med.2009;39:1413-23.
86 Otowa T, Gardner CO, Kendler KS, Hettema JM. Parenting and riskfor mood, anxiety and substance use disorders: a study inpopulation-based male twins. Soc Psychiatry Psychiatr Epidemiol.2013 Jan 24. [Epub ahead of print]
87 de Rosnay M, Cooper PJ, Tsigaras N, Murray L. Transmission ofsocial anxiety from mother to infant: an experimental study using asocial referencing paradigm. Behav Res Ther. 2006;44:1165-75.
88 Gerull FC, Rapee RM. Mother knows best: effects of maternalmodelling on the acquisition of fear and avoidance behaviour intoddlers. Behav Res Ther. 2002;40:279-87.
89 Murray L, de Rosnay M, Pearson J, Bergeron C, Schofield E,Royal-Lawson M, et al. Intergenerational transmission of socialanxiety: the role of social referencing processes in infancy. ChildDev. 2008;79:1049-64.
90 Field AP. Is conditioning a useful framework for understanding thedevelopment and treatment of phobias? Clin Psychol Rev.2006;26:857-75.
91 Field AP, Lawson J. Fear information and the development of fearsduring childhood: effects on implicit fear responses and behaviouralavoidance. Behav Res Ther. 2003;41:1277-93.
92 Kraemer HC, Kazdin AE, Offord DR, Kessler RC, Jensen PS,Kupfer DJ. Coming to terms with the terms of risk. Arch GenPsychiatry. 1997;54:337-43.
93 Kraemer HC, Stice E, Kazdin A, Offord D, Kupfer D. How do riskfactors work together? Mediators, moderators, and independent,overlapping, and proxy risk factors. Am J Psychiatry. 2001;158:848-56.
94 Kendler KS. ‘‘A gene for...’’: the nature of gene action in psychiatricdisorders. Am J Psychiatry. 2005;162:1243-52.
95 Kendler KS. Preparing for gene discovery: a further agenda forpsychiatry. Arch Gen Psychiatry. 1999;56:554-5.
96 Kendler KS. Explanatory models for psychiatric illness. Am JPsychiatry. 2008;165:695-702.
97 Insel T, Cuthbert B, Garvey M, Heinssen R, Pine DS, Quinn K, et al.Research Domain Criteria (RDoC): toward a new classificationframework for research on mental disorders. Am J Psychiatry.2010;167:748-51.
98 Sanislow CA, Pine DS, Quinn KJ, Kozak MJ, Garvey MA, HeinssenRK, et al. Developing constructs for psychopathology research:research domain criteria. J Abnorm Psychol. 2010;119:631-9.
99 Coghill D, Sonuga-Barke EJ. Annual research review: categoriesversus dimensions in the classification and conceptualisation ofchild and adolescent mental disorders--implications of recentempirical study. J Child Psychol Psychiatry. 2012;53:469-89.
100 Skarin K. Cognitive and contextual determinants of stranger fear insix- and eleven-month-old infants. Child Dev. 1977;48:537-44.
101 Thompson RA, Limber SP. ‘‘Social anxiety’’ in infancy: stranger andseparation reactions. In: Leitenberg H, editor. Handbook of socialand evaluation anxiety. New York: Plenum Press; 1990. p. 85-137.
102 Kagan J, Snidman N, Zentner M, Peterson E. Infant temperamentand anxious symptoms in school age children. Dev Psychopathol.1999;11:209-24.
103 Clauss JA, Blackford JU. Behavioral inhibition and risk fordeveloping social anxiety disorder: a meta-analytic study. J AmAcad Child Adolesc Psychiatry. 2012;51:1066-75.
104 Degnan KA, Almas AN, Fox NA. Temperament and the environ-ment in the etiology of childhood anxiety. J Child PsycholPsychiatry. 2010;51:497-517.
105 Noel VA, Francis SE. A meta-analytic review of the role of childanxiety sensitivity in child anxiety. J Abnorm Child Psychol.2011;39:721-33.
GA Salum et al.S18
Rev Bras Psiquiatr. 2013;35(Suppl 1)

106 Olatunji BO, Wolitzky-Taylor KB. Anxiety sensitivity and the anxietydisorders: a meta-analytic review and synthesis. Psychol Bull.2009;135:974-99.
107 Salum GA, Alvarenga PG, Manfro GG. Transtornos de ansiedade etranstorno obsessivo-compulsivo. In: Polanczyk GV, LamberteMTMR, editors. Psiquiatria da infancia e adolescencia. SaoPaulo: Manole; 2012.
108 Walkup JT, Albano AM, Piacentini J, Birmaher B, Compton SN,Sherrill JT, et al. Cognitive behavioral therapy, sertraline, or acombination in childhood anxiety. N Engl J Med. 2008;359:2753-66.
109 Angold A, Costello EJ, Erkanli A. Comorbidity. J Child PsycholPsychiatry. 1999;40:57-87.
110 Wolitzky-Taylor K, Bobova L, Zinbarg RE, Mineka S, Craske MG.Longitudinal investigation of the impact of anxiety and mooddisorders in adolescence on subsequent substance use disorderonset and vice versa. Addict Behav. 2012;37:982-5.
111 Moffitt TE, Harrington H, Caspi A, Kim-Cohen J, Goldberg D,Gregory AM, et al. Depression and generalized anxiety disorder:cumulative and sequential comorbidity in a birth cohort followedprospectively to age 32 years. Arch Gen Psychiatry. 2007;64:651-60.
112 Gandhi B, Cheek S, Campo JV. Anxiety in the pediatric medicalsetting. Child Adolesc Psychiatr Clin N Am. 2012;21:643-53.
113 Brasil HHA. Development of the Brazilian version of K-SADS-PL(Schedule for Affective Disorders and Schizophrenia for SchoolAged Children Present and Lifetime Version) and study ofpsychometric properties [dissertation]. Sao Paulo: UniversidadeFederal de Sao Paulo; 2003.
114 Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, et al.Schedule for Affective Disorders and Schizophrenia for School-AgeChildren-Present and Lifetime Version (K-SADS-PL): initial relia-bility and validity data. J Am Acad Child Adolesc Psychiatry.1997;36:980-8.
115 Polanczyk GV, Eizirik M, Aranovich V, Denardin D, da Silva TL,da Conceicao TV, et al. Interrater agreement for the schedulefor affective disorders and schizophrenia epidemiological versionfor school-age children (K-SADS-E). Rev Bras Psiquiatr. 2003;25:87-90.
116 Angold A, Erkanli A, Copeland W, Goodman R, Fisher PW, CostelloEJ. Psychiatric diagnostic interviews for children and adolescents: acomparative study. J Am Acad Child Adolesc Psychiatry.2012;51:506-17.
117 Goodman R, Ford T, Richards H, Gatward R, Meltzer H. TheDevelopment and Well-Being Assessment: description and initialvalidation of an integrated assessment of child and adolescentpsychopathology. J Child Psychol Psychiatry. 2000;41:645-55.
118 Souza IGS, Serra-Pinheiro MA, Mousinho R, Mattos PA. ABrazilian version of the ‘‘Children’s Interview for PsychiatricSyndromes’’ (ChIPS). J Bras Psiquiatr. 2009;58:115-8.
119 Weller EB, Weller RA, Fristad MA, Rooney MT, Schecter J.Children’s Interview for Psychiatric Syndromes (ChIPS). J Am AcadChild Adolesc Psychiatry. 2000;39:76-84.
120 Shaffer D, Fisher P, Lucas CP, Dulcan MK, Schwab-Stone ME.NIMH Diagnostic Interview Schedule for Children Version IV (NIMHDISC-IV): description, differences from previous versions, andreliability of some common diagnoses. J Am Acad Child AdolescPsychiatry. 2000;39:28-38.
121 Reich W. Diagnostic interview for children and adolescents (DICA).J Am Acad Child Adolesc Psychiatry. 2000;39:59-66.
122 Welner Z, Reich W, Herjanic B, Jung KG, Amado H. Reliability,validity, and parent-child agreement studies of the DiagnosticInterview for Children and Adolescents (DICA). J Am Acad ChildAdolesc Psychiatry. 1987;26:649-53.
123 Sherrill JT, Kovacs M. Interview schedule for children andadolescents (ISCA). J Am Acad Child Adolesc Psychiatry.2000;39:67-75.
124 Lyneham HJ, Abbott MJ, Rapee RM. Interrater reliability of theAnxiety Disorders Interview Schedule for DSM-IV: child and parentversion. J Am Acad Child Adolesc Psychiatry. 2007;46:731-6.
125 Silverman WK, Saavedra LM, Pina AA. Test-retest reliability ofanxiety symptoms and diagnoses with the Anxiety DisordersInterview Schedule for DSM-IV: child and parent versions. J AmAcad Child Adolesc Psychiatry. 2001;40:937-44.
126 Angold A, Costello EJ. The Child and Adolescent PsychiatricAssessment (CAPA). J Am Acad Child Adolesc Psychiatry.2000;39:39-48.
127 Angold A, Prendergast M, Cox A, Harrington R, Simonoff E, RutterM. The Child and Adolescent Psychiatric Assessment (CAPA).Psychol Med. 1995;25:739-53.
128 Egger HL, Erkanli A, Keeler G, Potts E, Walter BK, Angold A. Test-retest reliability of the Preschool Age Psychiatric Assessment(PAPA). J Am Acad Child Adolesc Psychiatry. 2006;45:538-49.
129 Merikangas K, Avenevoli S, Costello J, Koretz D, Kessler RC.National comorbidity survey replication adolescent supplement(NCS-A): I. background and measures. J Am Acad Child AdolescPsychiatry. 2009;48:367-9.
130 Biaggio AMB, Spielberger CD. [Manual of the Portuguese form ofthe STAI]. Rio de Janeiro: CEPA; 1983.
131 Spielberger CD. Manual for the State-Trait Anxiety Inventory forChildren. Palo Alto: Consulting Psychologist Press; 1973.
132 Gorayeb MAM, Gorayeb R. [Revised Children’s Manifest AnxietyScale (RCMAS) adapt to Portuguese in Brazil]. Temas Psicol.2008;16:35-45.
133 Reynolds CR, Richmond BO. What I think and feel: a revisedmeasure of children’s manifest anxiety. J Abnorm Child Psychol.1997;25:15-20.
134 Beck JS, Beck AT, Jolly JB, Steer RA. Beck Youth Inventories forchildren and adolescents: manual. 2nd ed. San Antonio: HarcourtAssessment, Inc; 2005.
135 The Pediatric Anxiety Rating Scale (PARS): development andpsychometric properties. J Am Acad Child Adolesc Psychiatry.2002;41:1061-9.
136 Caporino NE, Brodman DM, Kendall PC, Albano AM, Sherrill J,Piacentini J, et al. Defining treatment response and remission inchild anxiety: signal detection analysis using the pediatric anxietyrating scale. J Am Acad Child Adolesc Psychiatry. 2013;52:57-67.
137 Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, BaugherM. Psychometric properties of the Screen for Child Anxiety RelatedEmotional Disorders (SCARED): a replication study. J Am AcadChild Adolesc Psychiatry. 1999;38:1230-6.
138 Birmaher B, Khetarpal S, Brent D, Cully M, Balach L, Kaufman J,et al. The Screen for Child Anxiety Related Emotional Disorders(SCARED): scale construction and psychometric characteristics. JAm Acad Child Adolesc Psychiatry. 1997;36:545-53.
139 Desousa DA, Salum GA, Isolan LR, Manfro GG. Sensitivity andspecificity of the screen for Child Anxiety Related EmotionalDisorders (SCARED): a community-based study. Child PsychiatryHum Dev. 2013;44:391-9.
140 Isolan L, Salum GA, Osowski AT, Amaro E, Manfro GG.Psychometric properties of the Screen for Child Anxiety RelatedEmotional Disorders (SCARED) in Brazilian children and adoles-cents. J Anxiety Disord. 2011;25:741-8.
141 DeSousa DA, Petersen CS, Behs R, Manfro GG, Koller SH.Brazilian Portuguese version of the Spence Children’s AnxietyScale (SCAS-Brasil). Trends Psychiatry Psychother. 2012;34:147-53.
142 Spence SH. A measure of anxiety symptoms among children.Behav Res Ther. 1998;36:545-66.
143 Spence SH. Structure of anxiety symptoms among children: aconfirmatory factor-analytic study. J Abnorm Psychol.1997;106:280-97.
144 March JS, Parker JD, Sullivan K, Stallings P, Conners CK. TheMultidimensional Anxiety Scale for Children (MASC): factorstructure, reliability, and validity. J Am Acad Child AdolescPsychiatry. 1997;36:554-65.
145 Masia-Warner C, Storch EA, Pincus DB, Klein RG, Heimberg RG,Liebowitz MR. The Liebowitz social anxiety scale for children andadolescents: an initial psychometric investigation. J Am Acad ChildAdolesc Psychiatry. 2003;42:1076-84.
146 Gauer GC, Picon P, Davoglio TR, Silva LM, Beidel DC.Psychometric characteristics of the Brazilian Portuguese versionof Social Phobia and Anxiety Inventory for Children (SPAI-C).Psico. 2009;40:354-8.
147 Gauer GJ, Picon P, Vasconcellos SJ, Turner SM, Beidel DC.Validation of the Social Phobia and Anxiety Inventory for Children(SPAI-C) in a sample of Brazilian children. Braz J Med Biol Res.2005;38:795-800.
Pediatric anxiety disorders S19
Rev Bras Psiquiatr. 2013;35(Suppl 1)

148 Scaini S, Battaglia M, Beidel DC, Ogliari A. A meta-analysis of thecross-cultural psychometric properties of the Social Phobia andAnxiety Inventory for Children (SPAI-C). J Anxiety Disord.2012:182-8.
149 Beidel DC, Turner SM, Morris TL. A new inventory to assesschildhood social anxiety and phobia: The Social Phobia and AnxietyInventory for Children. Psychol Assess. 1995;7:73-9.
150 Freeman J, Flessner CA, Garcia A. The Children’s Yale-BrownObsessive Compulsive Scale: reliability and validity for use among5 to 8 year olds with obsessive-compulsive disorder. J AbnormChild Psychol. 2011;39:877-83.
151 Scahill L, Riddle MA, McSwiggin-Hardin M, Ort SI, King RA,Goodman WK, et al. Children’s Yale-Brown Obsessive CompulsiveScale: reliability and validity. J Am Acad Child Adolesc Psychiatry.1997;36:844-52.
152 Storch EA, Murphy TK, Adkins JW, Lewin AB, Geffken GR, JohnsNB, et al. The children’s Yale-Brown obsessive-compulsive scale:psychometric properties of child- and parent-report formats. JAnxiety Disord. 2006;20:1055-70.
153 Rosario-Campos MC, Miguel EC, Quatrano S, Chacon P, Ferrao Y,Findley D, et al. The Dimensional Yale-Brown Obsessive-Compulsive Scale (DY-BOCS): an instrument for assessingobsessive-compulsive symptom dimensions. Mol Psychiatry.2006;11:495-504.
154 Ollendick TH. Reliability and validity of the Revised Fear SurgerySchedule for Children (FSSC-R). Behav Res Ther. 1983;21:685-92.
155 Masi G, Pari C, Millepiedi S. Pharmacological treatment options forpanic disorder in children and adolescents. Expert OpinPharmacother. 2006;7:545-54.
156 Pine DS, Cohen JA. Trauma in children and adolescents: risk andtreatment of psychiatric sequelae. Biol Psychiatry. 2002;51:519-31.
157 Cohen JA, Bukstein O, Walter H, Benson SR, Chrisman A,Farchione TR, et al. Practice parameter for the assessment andtreatment of children and adolescents with posttraumatic stressdisorder. J Am Acad Child Adolesc Psychiatry. 2010;49:414-30.
158 Ipser JC, Stein DJ, Hawkridge S, Hoppe L. Pharmacotherapy foranxiety disorders in children and adolescents. Cochrane DatabaseSyst Rev. 2009:CD005170.
159 DeVeaugh-Geiss J, Moroz G, Biederman J, Cantwell D, FontaineR, Greist JH, et al. Clomipramine hydrochloride in childhood andadolescent obsessive-compulsive disorder--a multicenter trial. JAm Acad Child Adolesc Psychiatry. 1992;31:45-9.
160 Uthman OA, Abdulmalik J. Comparative efficacy and acceptabilityof pharmacotherapeutic agents for anxiety disorders in children andadolescents: a mixed treatment comparison meta-analysis. CurrMed Res Opin. 2010;26:53-9.
161 Connolly SD, Suarez L, Sylvester C. Assessment and treatment ofanxiety disorders in children and adolescents. Curr Psychiatry Rep.2011;13:99-110.
162 Graae F, Milner J, Rizzotto L, Klein RG. Clonazepam in childhoodanxiety disorders. J Am Acad Child Adolesc Psychiatry.1994;33:372-6.
163 O’Kearney RT, Anstey KJ, von Sanden C. Behavioural andcognitive behavioural therapy for obsessive compulsive disorderin children and adolescents. Cochrane Database Syst Rev.2006:CD004856.
164 Reynolds S, Wilson C, Austin J, Hooper L. Effects of psychotherapyfor anxiety in children and adolescents: a meta-analytic review. ClinPsychol Rev. 2012;32:251-62.
165 Davis TE, 3rd, May A, Whiting SE. Evidence-based treatment ofanxiety and phobia in children and adolescents: current status andeffects on the emotional response. Clin Psychol Rev. 2011;31:592-602.
166 James A, Soler A, Weatherall R. Cognitive behavioural therapy foranxiety disorders in children and adolescents. Cochrane DatabaseSyst Rev. 2005:CD004690.
167 Alvarenga PG, Mastrorosa RS, Rosario MC. Obsessive compulsivedisorder in children and adolescents. In Rey JM, editor. IACAPAPe-Textbook of Child and Adolescent Mental Health. Geneva:International Association for Child and Adolescent Psychiatry andAllied Professions; 2012. p. 1-17.
168 Pediatric OCD Treatment Study (POTS) Team. Cognitive-behaviortherapy, sertraline, and their combination for children and adoles-cents with obsessive-compulsive disorder: the Pediatric OCD
Treatment Study (POTS) randomized controlled trial. JAMA.2004;292:1969-76.
169 Garcia AM, Sapyta JJ, Moore PS, Freeman JB, Franklin ME, MarchJS, et al. Predictors and moderators of treatment outcome in thePediatric Obsessive Compulsive Treatment Study (POTS I). J AmAcad Child Adolesc Psychiatry. 2011;49:1024-33.
170 March JS, Franklin ME, Leonard H, Garcia A, Moore P, Freeman J,et al. Tics moderate treatment outcome with sertraline but notcognitive-behavior therapy in pediatric obsessive-compulsive dis-order. Biol Psychiatry. 2007;61:344-7.
171 Rosario M, Alvarenga P, Mathis M, Leckman J. Obsessive-compulsive disorder in childhood. In: Banaschewski T, Rohde L,editors. Biological child psychiatry - recent trends and develop-ments. Basel: Karger; 2008. p. 82-94.
172 Norberg MM, Krystal JH, Tolin DF. A meta-analysis of D-cycloserine and the facilitation of fear extinction and exposuretherapy. Biol Psychiatry. 2008;63:1118-26.
173 Hakamata Y, Lissek S, Bar-Haim Y, Britton JC, Fox NA, LeibenluftE, et al. Attention bias modification treatment: a meta-analysistoward the establishment of novel treatment for anxiety. BiolPsychiatry. 2010;68:982-90.
174 Eldar S, Apter A, Lotan D, Edgar KP, Naim R, Fox NA, et al.Attention bias modification treatment for pediatric anxiety disorders:a randomized controlled trial. Am J Psychiatry. 2012;169:213-20.
175 Pittenger C, Kelmendi B, Wasylink S, Bloch MH, Coric V. Riluzoleaugmentation in treatment-refractory obsessive-compulsive disor-der: a series of 13 cases, with long-term follow-up. J ClinPsychopharmacol. 2008;28:363-7.
176 Grant JE, Kim SW, Odlaug BL. N-acetyl cysteine, a glutamate-modulating agent, in the treatment of pathological gambling: a pilotstudy. Biol Psychiatry. 2007;62:652-7.
177 Jayakody K, Gunadasa S, Hosker C. Exercise for anxiety disorders:systematic review. Br J Sports Med. 2013 Jan 7. [Epub ahead ofprint]
178 Asmundson GJ, Fetzner MG, Deboer LB, Powers MB, Otto MW,Smits JA. Let’s get physical: a contemporary review of the anxiolyticeffects of exercise for anxiety and its disorders. Depress Anxiety.2013;30:362-73.
179 Larun L, Nordheim LV, Ekeland E, Hagen KB, Heian F. Exercise inprevention and treatment of anxiety and depression among childrenand young people. Cochrane Database Syst Rev. 2006:CD004691.
180 Pittler MH, Ernst E. Kava extract for treating anxiety. CochraneDatabase Syst Rev. 2003:CD003383.
181 Miyasaka LS, Atallah AN, Soares BG. Valerian for anxietydisorders. Cochrane Database Syst Rev. 2006:CD004515.
182 Miyasaka LS, Atallah AN, Soares BG. Passiflora for anxietydisorder. Cochrane Database Syst Rev. 2007:CD004518.
183 Krisanaprakornkit T, Krisanaprakornkit W, Piyavhatkul N,Laopaiboon M. Meditation therapy for anxiety disorders.Cochrane Database Syst Rev. 2006:CD004998.
184 Robinson J, Biley FC, Dolk H. Therapeutic touch for anxietydisorders. Cochrane Database Syst Rev. 2007:CD006240.
185 Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D,Ritz L, et al. Evaluation of outcomes with citalopram for depressionusing measurement-based care in STAR*D: implications for clinicalpractice. Am J Psychiatry. 2006;163:28-40.
186 Bridge JA, Iyengar S, Salary CB, Barbe RP, Birmaher B, PincusHA, et al. Clinical response and risk for reported suicidalideation and suicide attempts in pediatric antidepressant treatment:a meta-analysis of randomized controlled trials. JAMA. 2007;297:1683-96.
187 Stein DJ, Baldwin DS, Bandelow B, Blanco C, Fontenelle LF, LeeS, et al. A 2010 evidence-based algorithm for the pharmacotherapyof social anxiety disorder. Curr Psychiatry Rep. 2010;12:471-7.
188 Gleason MM, Egger HL, Emslie GJ, Greenhill LL, Kowatch RA,Lieberman AF, et al. Psychopharmacological treatment for veryyoung children: contexts and guidelines. J Am Acad Child AdolescPsychiatry. 2007;46:1532-72.
189 Rapee RM, Kennedy SJ, Ingram M, Edwards SL, Sweeney L.Altering the trajectory of anxiety in at-risk young children. Am JPsychiatry. 2010;167:1518-25.
190 Degnan KA, Fox NA. Behavioral inhibition and anxiety disorders:multiple levels of a resilience process. Dev Psychopathol. 2007;19:729-46.
GA Salum et al.S20
Rev Bras Psiquiatr. 2013;35(Suppl 1)

191 Fox NA, Henderson HA, Marshall PJ, Nichols KE, Ghera MM.Behavioral inhibition: linking biology and behavior within a devel-opmental framework. Annu Rev Psychol. 2005;56:235-62.
192 Hirshfeld-Becker DR, Micco J, Henin A, Bloomfield A, Biederman J,Rosenbaum J. Behavioral inhibition. Depress Anxiety. 2008;25:357-67.
193 Smoller JW, Block SR, Young MM. Genetics of anxiety disorders: thecomplex road from DSM to DNA. Depress Anxiety. 2009;26:965-75.
194 Domschke K, Deckert J. Genetics of anxiety disorders - status quoand quo vadis. Curr Pharm Des. 2012;18:5691-8.
195 Gullone E. The development of normal fear: a century of research.Clin Psychol Rev. 2000;20:429-51.
196 Strawn JR, Sakolsky DJ, Rynn MA. Psychopharmacologic treat-ment of children and adolescents with anxiety disorders. ChildAdolesc Psychiatr Clin N Am. 2012;21:527-39.
197 Rynn M, Puliafico A, Heleniak C, Rikhi P, Ghalib K, Vidair H.Advances in pharmacotherapy for pediatric anxiety disorders.Depress Anxiety. 2011;28:76-87.
198 Peters TE, Connolly S. Psychopharmacologic treatment forpediatric anxiety disorders. Child Adolesc Psychiatr Clin N Am.2012;21:789-806.
199 Kar N. Cognitive behavioral therapy for the treatment of post-traumatic stress disorder: a review. Neuropsychiatr Dis Treat.2011;7:167-81.
200 Kircanski K, Peris TS, Piacentini JC. Cognitive-behavioral therapyfor obsessive-compulsive disorder in children and adolescents.Child Adolesc Psychiatr Clin N Am. 2011;20:239-54.
201 Seligman LD, Ollendick TH. Cognitive-behavioral therapy foranxiety disorders in youth. Child Adolesc Psychiatr Clin N Am.2011;20:217-38.
Pediatric anxiety disorders S21
Rev Bras Psiquiatr. 2013;35(Suppl 1)