Embed Size (px)
Citation preview

Review ArticlePediatric Adrenal Insufficiency: Diagnosis, Management,and New Therapies
Sasigarn A. Bowden and Rohan Henry
Division of Endocrinology, Department of Pediatrics, Nationwide Children’s Hospital/The Ohio State University College of Medicine,Columbus, Ohio, USA
Correspondence should be addressed to Sasigarn A. Bowden; [email protected]
Received 31 May 2018; Accepted 27 September 2018; Published 1 November 2018
Academic Editor: Alessandro Mussa
Copyright © 2018 Sasigarn A. Bowden and Rohan Henry. This is an open access article distributed under the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
Adrenal insufficiency may result from a wide variety of congenital or acquired disorders of hypothalamus, pituitary, or adrenalcortex. Destruction or dysfunction of the adrenal cortex is the cause of primary adrenal insufficiency, while secondary adrenalinsufficiency is a result of pituitary or hypothalamic disease. Timely diagnosis and clinical management of adrenal insufficiencyare critical to prevent morbidity and mortality. This review summarizes the etiologies, presentation, and diagnosis of adrenalinsufficiency utilizing different dynamic hormone testing and describes current treatment recommendations and new therapies.
1. Introduction
Adrenal Insufficiency (AI) may be caused by destructionor dysfunction of the adrenal gland (primary AI, Addison’sdisease), deficient pituitary adrenocorticotrophic hormone(ACTH) secretion (secondary AI), or deficient hypothalamicsecretion of corticotropic releasing hormone (CRH) (tertiaryAI). The secondary and tertiary AI can also be called centralAI. Primary AI is rare with a prevalence of approximately 93-140 per 1,000,000 [1–3]. The most common cause of primaryAI in children is congenital adrenal hyperplasia (CAH)which accounts for 70% of pediatric patients with primaryAI, whereas autoimmune adrenalitis (Addison’s disease)accounts for up to 15% of cases [4]. The most common causeof CAH is 21-hydroxylase deficiency, accounting for ∼ 90%of all CAH cases, with an incidence of 1 in 14,000 live births[5]. Secondary AI secondary to intracranial pathology is alsorare and may be isolated deficiency of ACTH or CRH, or itmay be part of other pituitary hormonal deficiencies, calledhypopituitarism. Iatrogenic tertiary AI caused by suppressionof the hypothalamic-pituitary adrenal (HPA) axis secondaryto glucocorticoid administration is the most common causeof central AI, with an estimated prevalence of 150- 280 per1,000,000 [6]. AI is associated with considerable morbidity
and mortality [7], frequently associated with lack of aware-ness or education regarding AI management, especially attime of physical stress that requires increased GC dose. Thisreview summarizes the etiologies, presentation, diagnosis,and treatment of AI and highlights new therapies.
2. Etiology and Presentation ofAdrenal Insufficiency
2.1. Primary AI. The most common cause of primary AIin children is CAH, which is due to a deficiency of one ofseveral enzymes required for adrenal synthesis of cortisol.CAH may be associated with aldosterone deficiency orexcess, depending on the type of enzyme deficiency. Morecommonly, CAH can also be associated with androgen excessbut can also be in combination with androgen deficiency.For all other causes of primary AI, all 3 zones of the adrenalcortex are usually involved by a disease process. The processcan be local or a manifestation of systemic disorders, such asautoimmune disease (either isolated or as part of the polyg-landular autoimmune syndrome), granulomatous diseasessuch as tuberculosis and histoplasmosis, and hemorrhageassociated with meningococcemia. Primary AI can also bedue to rare genetic diseases, which include disorders of
HindawiInternational Journal of PediatricsVolume 2018, Article ID 1739831, 8 pageshttps://doi.org/10.1155/2018/1739831

2 International Journal of Pediatrics
Table 1: Causes of adrenal insufficiency.
PRIMARY(i) Congenital adrenal hyperplasia(ii) Congenital adrenal hypoplasia due to gene mutations (e.g. DAX-1, SF1 mutations)(iii) Peroxisome defects (adrenoleukodystrophy [childhood or neonatal], Zellweger syndrome)(iv) Bilateral adrenal hemorrhage of the newborn(v) Adrenal hemorrhage of acute infection (Waterhouse-Friderichsen syndrome)(vi) Autoimmune adrenalitis (isolated or part of autoimmune polyglandular syndrome type 1 and 2)(vii) Infection (e.g. tuberculosis, fungal infection, human immunodeficiency virus, cytomegalovirus)(viii) Triple A syndrome or Allgrove syndrome (alacrimia, achalasia, adrenal insufficiency)(ix) Adrenal unresponsiveness to ACTH due to gene mutations(x) Familial glucocorticoid deficiency(xi) Drug effects (mitotane, ketoconazole, aminoglutethimide, metyrapone, megestrol, rifampin)
SECONDARY (CENTRAL)(i) Congenital
(a) Septo-optic dysplasia(b) Pituitary aplasia/hypoplasia(c) Agenesis of corticotrophs(d) POMC
(ii) Acquired(a) Trauma(b) Brain tumor (craniopharyngioma)(c) Lymphocytic hypophysitis(d) Surgery(e) Cranial irradiation(f) Infiltrative disease (hemochromatosis, sarcoidosis, Langerhans cell histiocytosis)(g) Steroid withdrawal after prolonged administration
steroidogenesis, peroxisomal defects, and abnormal adrenalgland development due to mutations (Table 1). The result isinadequate secretion of glucocorticoids, mineralocorticoids,and androgens.
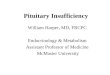
The clinical presentation of AI can be gradual andnonspecific to hypotension or shock, so-called adrenal crisis,depending on the degree of insufficiency and precipitatingstress events. Symptoms include fatigue, nausea, muscleweakness, and headache. Infants with salt wasting CAHoften present in the second week of life with signs ofacute primary AI which include dehydration, weight loss,lethargy, hyponatremia, hyperkalemia, and hypoglycemia.In older children and adolescents, symptoms may includefatigue, nausea, vomiting, diarrhea, abdominal pain, weightloss, slow growth, and salt craving. The lack of cortisolnegative feedback increases hypothalamic CRH, leading toincreased pituitary ACTH and melanocyte-stimulating hor-mone (MSH), both of which are derived from a precursor,proopiomelanocortin (POMC). When CRH is cleaved fromPOMC, MSH is concurrently released. Elevated ACTH andMSH cause hyperpigmentation of the skin (Figure 1) andmucous membranes, involving skin creases, axillae, groin,gingival, and scars.
Aldosterone deficiency causes sodium loss, which leadsto electrolyte abnormalities including hyponatremia, hyper-kalemia, and metabolic acidosis. Symptoms of aldosterone
deficiency include salt craving, anorexia, dizziness, hypoten-sion, dehydration, and weight loss.
2.2. Secondary AI. Secondary AI or central AI is causedby deficiency of pituitary ACTH or hypothalamic CRHsecretion and consequent insufficient adrenal cortisol secre-tion (Table 1). Clinical presentation of central AI is similarto that of primary AI but without salt wasting, becausealdosterone secretion is normal in central AI, being regulatedby the renin-aldosterone pathway. Therefore, dehydration,hypotension, hyponatremia, and hyperkalemia are usuallynot present. With the absence of an increased production ofACTH, patients with secondary AI do not have hyperpig-mentation. In isolated ACTH deficiency or in combinationwith growth hormone deficiency as part of hypopituitarism,hypoglycemia can occur which can lead to seizures and comaif severe [8].
3. Diagnosis of AI
Because the signs and symptoms of AI are nonspecific,clinicians must have high index of suspicion. Serum elec-trolytes often provide a clue to diagnosis, as hyponatremiawith or without hyperkalemia is common in patients withprimary AI. Hyponatremia with absence of hyperkalemiain primary AI can be explained by protracted vomiting,

International Journal of Pediatrics 3
(a) (b)
Figure 1: (a) Hyperpigmentation at nipples and axillar in a 10-day-old male infant with salt-wasting congenital adrenal hyperplasia due to21-hydroxylase deficiency. (b) Hyperpigmentation in a 9-year-old boy with Addison's disease.
a common symptom at presentation [9]. Hyponatremia isvery common in primary AI due to aldosterone deficiency.However, hyponatremia can also be seen in patients withcentral AI. The explanation for this is vasopressin hyper-secretion with resultant water retention [10]. The lack ofcortisol negative feedback not only increases hypothalamicCRH but also increases vasopressin synthesis and secretion.Hypoglycemia can be seen in both primary and secondary AIand can bemore pronounced in secondaryAI in combinationwith growth hormone deficiency. Hypoglycemia may be apresenting symptom; therefore, laboratory investigation forhypoglycemia should include serum cortisol, drawn at thetime of hypoglycemia. Patients with AI have impaired gluco-neogenesis andhepatic glycogenesis; therefore, hypoglycemiamay be associated with ketosis.
In primary AI with salt losing crisis, plasma reninactivity is elevated,while aldosterone secretion is low.Urinaryexcretion of sodium and chloride is increased and that ofpotassium decreased.
Themost definitive test is measurement of serum cortisollevels. A morning cortisol of < 3 ug/dL is indicative ofadrenal insufficiency, while cortisol level >18 mcg/dL rulesout adrenal insufficiency. A diagnosis of primary AI isconfirmed if the serum cortisol level is < 18 mcg/dL, inthe presence of markedly elevated ACTH and plasma reninactivity. It is important to note that the cortisol level cutoffmay differ among different laboratories, depending on theassays bywhich cortisol ismeasured [11]. Conditions affectingcortisol-binding globulin (estrogen hormone, as in preg-nancy or the use of oral contraceptives or hypoproteinemiasuch as nephrotic syndrome) may also affect cortisol values[12].
Positive adrenal autoantibodies establish autoimmuneadrenal insufficiency or Addison’s disease. All males diag-nosed with primary adrenal insufficiency without evidenceof autoimmunity should have plasma very long chain fattyacids obtained to rule out X-linked adrenoleukodystro-phy.
When CAH is being considered in newborns presentingwith ambiguous genitalia or salt-losing crisis, random corti-sol and androgen hormone studies, particularly 17-hydroxyprogesterone, are obtained to confirm or exclude diagnosis.Patients with mild or early stage of AI or central AI oftenrequire additional dynamic testing.
4. Dynamic Testing to Assess the HPA Axis
4.1. ACTH Stimulation Test. Administration of cosyntropin(1-24 ACTH; Cortrosyn) to directly stimulate adrenal cortisolrelease is the most commonly used diagnostic test to evaluateadrenal function. Baseline ACTH and cortisol samples areobtained (with additional tests such as plasma renin activity,aldosterone, or androgen hormones as indicated), and then250 𝜇g of cosyntropin is administered intravenously, followedby cortisol samples drawn at 30 and 60 minutes later. Plasmacortisol level ≥ 18 𝜇g/dL, along with a normal baselineACTH level rules out primary adrenal insufficiency. Thistest may not be sensitive in identifying patients with mildAI or recent onset secondary adrenal insufficiency [13] asadrenal reserve may still be adequate with a normal cortisolresponse to exogenous ACTH. Therefore, a low dose ACTHstimulation test using 1 𝜇g cosyntropin should be used inpatients suspected of secondary AI as 1 𝜇g dose is moresensitive to detect AI, thereby preventing false positive results[14, 15]. Technical difficulties in performing the low doseACTH stimulation test exist. These include dilution error ofACTH, afternoon testing, or loss of ACTH due to adherenceto long plastic tubing through which ACTH is administered[16]. Hence, the clinician should be cognizant of these issueswhen interpreting test results.
In patients with central AI, ACTH level can be low or lownormal. When the diagnosis of ACTH deficiency is made, itis important to rule out other pituitary hormone deficienciesbecause isolated ACTH deficiency is rare.
In neonates with congenital hypopituitarism, adrenalfunction test using 1 𝜇g ACTH stimulation test, performed

4 International Journal of Pediatrics
during postnatal period to diagnose ACTH deficiency, maybe falsely normal [17]. Newborns with ACTH deficiencyhave a normal upregulation of fetal steroidogenic enzymesand normal fetal adrenal maturation and steroidogenesisunder the placental CRH stimulation [18], therefore, stillhave adequate adrenal reserve that allows temporary normalcortisol response to synthetic ACTH injection after birth.Clinicians must maintain a high degree of suspicion for falsenegative testing and repeat ACTH stimulation test within 3-4weeks after initial testing, for timely diagnosis of central AIin these infants [17].
4.2. Glucagon Stimulation Test. Glucagon stimulation test isa sensitive test for evaluating adrenal function and is notassociated with hypoglycemia and, therefore, provides analternative to insulin-induced hypoglycemia in evaluatingcentral hypoadrenalism. In this test, glucagon at 0.03 mg/kg(maximum 1 mg) is given subcutaneously. Blood samplesfor serum glucose and cortisol are obtained at 60, 90, 120,and 150 minutes after glucagon administration. Glucagonadministration causes an increase in blood glucose whichthen evokes an endogenous insulin response, resulting in afall in blood glucose which stimulates a counter-regulatoryhormone response including cortisol [19]. Glucagon stim-ulation test was found to have a high false-positive rate of23.7% in children (thosewho failed the test had a normal peakcortisol on the ACTH stimulation test) [20]. Moreover, peakglucagon-stimulated cortisol level was inversely related to age[20, 21] and gender [20] in children.Therefore, interpretationof glucagon stimulation test can be problematic. Lowerpeak cortisol cutoff for glucagon stimulation test has beensuggested in adults [22, 23]. Glucagon-stimulated cortisolcutoff has not been established in pediatrics.
4.3. Insulin-Induced Hypoglycemia. Hypoglycemia provokescounter-regulatory hormone response and is used to assessthe integrity of the HPA axis. This test was once consideredthe gold standard for the diagnosis of AI but is no longer usedin children because of the risk of hypoglycemic seizures andsevere hypokalemia after treatment with glucose infusion [7,24].
4.4. Metyrapone Test. Metyrapone inhibits the activity of11𝛽-hydroxylase enzyme that converts precursor to cortisol,resulting in decreased cortisol secretion and a compensatoryincrease in ACTH levels, as well as 11-deoxy-cortisol (theprecursor of cortisol) and its urinary metabolites. For theconvenient single dose test, 30 mg/kg to a maximum of 3grams is given at midnight with a snack to decrease thenausea associated with metyrapone ingestion. Cortisol, 11-deoxycortisol, and ACTH are measured at 8 AM followingthe dose. A normal response is the increase in plasma 11-deoxycortisol to > 7 𝜇g/dL [25]. Lack of increase in ACTHand 11-deoxycortisol levels after metyrapone administrationis diagnostic of ACTH deficiency. The metyrapone test is anexcellent test to evaluate the integrity of adrenal functionbut is rarely performed because of the difficulty in obtainingmetyrapone and the risk of precipitating an adrenal crisis[7].
5. Treatment of AI
5.1. Maintenance Therapy. In primary adrenal insufficiency,maintenance therapy requires both glucocorticoids and min-eralocorticoid replacement. In secondary or central adrenalinsufficiency, only cortisol replacement is required withoutthe need of salt-retaining aldosterone replacement.
5.1.1. Hydrocortisone. Thedaily basal cortisol production ratein children is approximately 6-8 mg/m2/day, lower thanpreviously estimated [26]. When administering orally, therecommended physiologic replacement dose of hydrocorti-sone in pediatric patients is approximately 10-12.5mg/m2/daydivided into two or three doses, compensating for theincomplete intestinal absorption and hepatic metabolism [7].In children with AI secondary to CAH, a supraphysiologicdose of 12-20 mg/m2/day is required to suppress adrenalandrogens. Goal of therapy is to control the symptoms ofAI with the lowest dose possible, without compromisinggrowth that is seen in overtreatment. Hydrocortisone ispreferred in children over other types of glucocorticoidbecause it is easy to titrate and has a short half-life with lessadverse effects, compared with themore potent longer-actingglucocorticoids.
5.1.2. Hydrocortisone Dosing Consideration. When hydrocor-tisone is given twice a day in children and adolescents withhypopituitarism, a nonphysiological nadir of cortisol levelsis observed 2-4 hours prior to the next dose [27]. Therefore,children with central AI (secondary to hypopituitarism)who are more prone to hypoglycemia or children withCAH who have additional risk of hyperandrogenism whenhydrocortisone is inadequate should receive hydrocortisone 3times a day. It is recommended that glucocorticoid should beadministered with food to prolong the half-life of hydrocorti-sone and to facilitate the production of a more physiologicalcortisol profile [28].
In patients with both TSH and ACTH deficiency orpatients with autoimmune polyendocrine syndrome type II(primary hypothyroidism and Addison’s disease), treatmentwith levothyroxine may precipitate an acute adrenal crisisbecause thyroxine increases cortisol metabolism [29, 30].Therefore, cortisol replacement should precede thyroid hor-mone replacement.
Although commercial liquid preparations of hydrocorti-sone are not recommended due to the uneven distributionof the drug in the liquid, hydrocortisone oral compoundedsuspension prepared extemporaneously from hydrocortisonetablets can be used safely and effectively in young children[31, 32]
Hydrocortisone dose needs to be increased to ensureadequate cortisol replacement when taken with medicationsthat induce hepatic cortisol metabolism by enzyme inductionof cytochrome P450 3A4. These medications that acceler-ate hepatic glucocorticoid metabolism include rifampicin,mitotane, anticonvulsants such as phenytoin, carbamazepine,oxcarbazepine, phenobarbital, and topiramate. Conversely,patient treated with drugs that inhibit CYP3A4 such asantiretroviral medicationmay require reduction of hydrocor-tisone dose [33].

International Journal of Pediatrics 5
5.1.3. Other Glucocorticoids (Dexamethasone and Prednisone).Dexamethasone can be used to treat patients with suspectedAI while undergoing a diagnostic ACTH stimulation test,because the cortisol tests can be performed without theinterference of dexamethasone. However, the use of dex-amethasone for this purpose may suppress the HPA axisthat may influence adrenal function testing. For long-termmaintenance therapy in growing children, dexamethasoneand prednisone are not recommended due to concerns ofgrowth suppression and significant weight gain. In somecircumstances when adherence to hydrocortisone is prob-lematic, one can use oral prednisolone or prednisone that canbe dosed every 12 hours. The conversion of hydrocortisoneto prednisone is a 5:1 ratio (prednisone or prednisolone is 5times more potent than hydrocortisone).
5.1.4. Fludrocortisone. In children with primary AI andconfirmed aldosterone deficiency, treatment with fludrocor-tisone at 0.05-0.2 mg per day in two divided doses is recom-mended. It has been suggested that fludrocortisone has notonly mineralocorticoid but also potent glucocorticoid activ-ity [9].This is of particular relevance in newborns and infantsto avoid glucocorticoid overexposure. The dose adjustmentof fludrocortisone for body size is rarely required since thealdosterone secretion rate does not increase from infancyto adulthood. Excessive fludrocortisone can cause hyper-volemia, hypertension, and edema. Monitoring of growth,weight gain, symptoms of salt craving, blood pressure, serumelectrolytes, and plasma renin activity provides guidance foradjusting doses of fludrocortisone.
5.1.5. Salt Supplementation. Because of low salt contentin breast milk and infant formulas and mineralocorticoidresistance in the immature infant kidney, sodium chloridesupplements at 1–2 gm/day (17–34 mEq per day) distributedin several feedings are given in the newborn period and up tothe age of 8-12 months when salt intake from diet is sufficient[5, 34].
5.2. Acute Management of AI or Adrenal Crisis. Adrenalcrisis is a life-threatening emergency that requires promptdiagnosis and treatment. Acute AI must be treated urgentlywith sufficient parenteral hydrocortisone, 100-150 mg or 100mg per m2 intravenously, saline with dextrose to restoreintravascular volume, and normalized serum sodium andblood glucose concentrations. Treatment of underlying con-ditions such as infection or trauma must also be undertaken.An intravenous isotonic saline with dextrose infusion atmaintenance rate should be continued for the following 24-48hours until patient is hemodynamically stable. Intravenoushydrocortisone at stress dose (100 mg per m2/day) given ascontinuous infusion or intravenous boluses every 6 hoursshould be continued in the first 24 hours and tapered over 2-3days (if clinically stable) to oral glucocorticoid maintenancedose. Mineralocorticoid replacement with fludrocortisoneshould be started in patients with primary AI when they areable to have oral intake.
5.3. Treatment during Illness, Injury, or Surgery. Cortisol isan important stress hormone that is essential for human sur-vival, particularly during stress. Surgery, anesthesia, trauma,and illnesses result in increased plasma ACTH and corti-sol levels. Many studies have demonstrated increased dailycortisol secretion proportionate to the degree of stress inhealthy adults undergoing surgery or in acutely ill individuals[35, 36]. According to the recommendations published bythe Pediatric Endocrine Society Drug andTherapeutic Com-mittee, the stress hydrocortisone doses are 30-50 mg/m2/dayfor mild to moderate stress and 100 mg/m2/day for the mostsevere stresses, such as major surgery or critical illness [7].The initial dose is followed by the same dose at a constant rateover a 24-hour period.The stress doses of hydrocortisone aretapered back to physiologic dose based on the pace of clinicalimprovement usually within 2-3 days. Patients with diarrheaand vomiting, who are unable to take oral medication bymouth, require intramuscular hydrocortisone (100 mg/m2per dose). In an emergency event when patient’s weight orheight may not be available, a quick, simple age-based dosingcan be used: 25 mg IV/IM for 0-3 years, 50 mg for 3-12 years,and 100 mg for ≥12 years.
5.4. NovelTherapies. Thecurrent oral glucocorticoid replace-ment therapy for patients with AI does not truly mimic thenormal physiologic cortisol rhythm, a nadir at bedtime andgradually rising levels to the early morning peak between3 am and 6 am before waking. Many patients continue tohave fatigue, nausea, and headaches on current conventionaltherapy [37] and some have nocturnal hypoglycemia due tovery low cortisol levels during the night and early morning[38]. Moreover, a higher prevalence of obesity, impairedglucose tolerance, and dyslipidemia has been demonstratedin patients with Addison’s disease [39], with increased useof antihypertensive drugs and lipid-lowering agents, as wellas an increased risk for cardiovascular morbidity comparedto general population [40]. Children with CAH, on sup-raphysiological glucocorticoid doses that cause an altereddiurnal cortisol profile, have high rate of obesity, hyper-tension, growth suppression, and low bone density [41–43].Increased evening cortisol levels have been shown to reduceglucose tolerance, insulin secretion, and insulin sensitivity inhealthy young adults [44]. Because of all these concerns andunfavorable treatment outcomes, novel therapies have beendeveloped in recent years.
5.4.1. Continuous Subcutaneous Hydrocortisone Infusion.Continuous subcutaneous hydrocortisone infusion therapyadministered via an insulin pump has been utilized to deliverhydrocortisone. Several studies have demonstrated that thismode of drug delivery restores a circadian cortisol rhythmand normalizes the ACTH levels compared to conventionaltherapy [45] and improves quality of life [46]. However, dueto high cost and other risks associated with the use of pump(such as site and pump failures), continuous subcutaneoushydrocortisone infusion has not been used routinely inclinical practice but can be considered a treatment optionin classic CAH poorly controlled on conventional therapy[47].

6 International Journal of Pediatrics
5.4.2. Sustained Release Hydrocortisone Preparations. Threemodified release hydrocortisone formulations have beendeveloped in Europe to mimic a normal circadian rhythmof cortisol. Chronocort is a hydrocortisone preparation withdelayed-release given twice a day, with a larger dose given atnight before sleep and a smaller dose given in the morning.The large dose given at night is to suppress the overnightACTH surge which drives excess androgen production inCAH and to provide a high peak cortisol early in themorning at wakening. Studies in adults with CAH resultedin more physiologic cortisol profile similar to that seen inhealthy individuals. Moreover, patients on modified releasehydrocortisone preparation had a better control of androgenlevels throughout the day [48, 49].
A dual-release hydrocortisone preparation is given oncedaily in the morning, with immediate release coating thatis rapidly absorbed, followed by a slow release from thecore of tablet. Studies of this hydrocortisone formulationin adults with Addison’s disease have shown to achievephysiologic cortisol profile, reduce central adiposity, andimprove metabolic parameters, as well as quality of life[50, 51]. Once-daily, modified–release hydrocortisone treat-ment in patients with AI restores a more physiologic cir-cadian cortisol rhythm, normalizes the immune cell pro-file, and reduces recurrent infections, compared to treat-ment with conventional glucocorticoid replacement therapy[52].
Infacort is an immediate-release, oral formulation ofhydrocortisone which has been designed specifically forinfants and children. Infacort is provided in capsules contain-ing taste-masked granules or sprinkle, which allows flexiblelow dosing to children in units of 0.5 mg, 1 mg, 2 mg, and5 mg of hydrocortisone [53]. Infacort has been shown to beeasy to administer to neonates, infants, and children withgood absorption, achieving cortisol levels at 60 minutes afteradministration similar to physiologic cortisol levels in healthychildren [53].
6. Patient Education andEmergency Precautions
Education of the patient and family is the key to successfultherapy of AI and prevention of morbidity and mortalityassociated with AI. The patient and their caretakers mustbe instructed about the rationale for replacement therapy,the maintenance medications, and stress dosing for illnesses.They need to be taught on how to administer injectableglucocorticoid when the patient is vomiting or unable totake oral stress doses, and when to consult a physician orgo to the emergency department. All patients should at alltimes wear a medical alert identification and carry a medicalemergency information card that indicate the diagnosis of“adrenal insufficiency” and daily medications.
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article.
References
[1] M.-F. Kong and W. Jeffcoate, “Eighty-six cases of Addison’sdisease,” Clinical Endocrinology, vol. 41, no. 6, pp. 757–761, 1994.
[2] A. C. Willis, “The prevalence of Addison’s disease in Coventry,UK,” PostgraduateMedical Journal, vol. 73, no. 859, pp. 286–288,1997.
[3] K. Løvas and E. S. Husebye, “High prevalence and increasingincidence of Addison’s disease in western Norway,” ClinicalEndocrinology, vol. 56, no. 6, pp. 787–791, 2002.
[4] R. Perry, O. Kecha, J. Paquette, C. Huot, G. van Vliet, and C.Deal, “Primary adrenal insufficiency in children: twenty yearsexperience at the Sainte-JustineHospital,Montreal,”TheJournalof Clinical Endocrinology &Metabolism, vol. 90, no. 6, pp. 3243–3250, 2005.
[5] P. W. Speiser, R. Azziz, L. S. Baskin et al., “Congenitaladrenal hyperplasia due to steroid 21-hydroxylase deficiency:an endocrine society clinical practice guideline,”The Journal ofClinical Endocrinology & Metabolism, vol. 95, no. 9, pp. 4133–4160, 2010.
[6] W. Arlt and B. Allolio, “Adrenal insufficiency,” The Lancet, vol.361, no. 9372, pp. 1881–1893, 2003.
[7] D. I. Shulman, M. R. Palmert, and S. F. Kemp, “Adrenalinsufficiency: Still a cause ofmorbidity and death in childhood,”Pediatrics, vol. 119, no. 2, pp. e484–e494, 2007.
[8] S. Vallette-Kasic, T. Brue, A.-M. Pulichino et al., “Congenitalisolated adrenocorticotropin deficiency: An underestimatedcause of neonatal death, explained by TPIT gene mutations,”The Journal of Clinical Endocrinology &Metabolism, vol. 90, no.3, pp. 1323–1331, 2005.
[9] M.D.Thompson, E. Kalmar, and S.A. Bowden, “Severe hypona-traemia with absence of hyperkalaemia in rapidly progressiveAddison’s disease,” BMJ Case Reports, vol. 2015, 2015.
[10] K. Kamoi, T. Tamura, K. Tanaka, M. Ishibashi, and T. Yamaji,“Hyponatremia and osmoregulation of thirst and vasopressinsecretion in patients with adrenal insufficiency,” The Journal ofClinical Endocrinology & Metabolism, vol. 77, no. 6, pp. 1584–1588, 1993.
[11] N. El-Farhan, A. Pickett, D. Ducroq et al., “Method-specificserum cortisol responses to the adrenocorticotrophin test:Comparison of gas chromatography-mass spectrometry andfive automated immunoassays,” Clinical Endocrinology, vol. 78,no. 5, pp. 673–680, 2013.
[12] M.C.Klose,M. Lange,A.K. Rasmussen et al., “Factors influenc-ing the adrenocorticotropin test: Role of contemporary cortisolassays, body composition, and oral contraceptive agents,” TheJournal of Clinical Endocrinology & Metabolism, vol. 92, no. 4,pp. 1326–1333, 2007.
[13] R. Kazlauskaite, A. T. Evans, C. V. Villabona et al., “Corti-cotropin tests for hypothalamic-pituitary-adrenal insufficiency:A metaanalysis,” The Journal of Clinical Endocrinology &Metabolism, vol. 93, no. 11, pp. 4245–4253, 2008.
[14] S. R. Rose, R. H. Lustig, S. Burstein, P. Pitukcheewanont, D. C.Broome, and G. A. Burghen, “Diagnosis of ACTH deficiency.Comparison of overnight metyrapone test to either low-dose orhigh-dose ACTH test,”Hormone Research, vol. 52, no. 2, pp. 73–79, 1999.
[15] G. Dickstein and W. Oelkers, “Commentary to the article:Comparison of low and high dose corticotropin stimulationtests in patients with pituitary disease [4] (multiple letters),”TheJournal of Clinical Endocrinology & Metabolism, vol. 83, no. 12,pp. 4531–4533, 1998.

International Journal of Pediatrics 7
[16] M. Wade, S. Baid, K. Calis, H. Raff, N. Sinaii, and L. Nieman,“Technical details influence the diagnostic accuracy of the 1 𝜇gACTH stimulation test,”European Journal of Endocrinology, vol.162, no. 1, pp. 109–113, 2010.
[17] L. K. Coshway, J. A. Indyk, and S. A. Bowden, “RepeatingACTHStimulation Test Is Necessary to Diagnose ACTHDeficiency inNeonatal Hypopituitarism With Initial False Negative Result,”Global Pediatric Health, vol. 1, p. 2333794X1456338, 2014.
[18] R. Sirianni, K. S. Rehman, B. R. Carr, C. R. Parker Jr., andW. E. Rainey, “Corticotropin-releasing hormone directly stim-ulates cortisol and the cortisol biosynthetic pathway in humanfetal adrenal cells,” The Journal of Clinical Endocrinology &Metabolism, vol. 90, no. 1, pp. 279–285, 2005.
[19] R. H. Rao and G. S. Spathis, “Intramuscular glucagon as aprovocative stimulus for the assessment of pituitary function:Growth hormone and cortisol responses,” Metabolism, vol. 36,no. 7, pp. 658–663, 1987.
[20] A. Tenenbaum, M. Phillip, and L. De Vries, “The intramuscularglucagon stimulation test does not provide good discriminationbetween normal and inadequate ACTH reserve when used inthe investigation of short healthy children,” Hormone Researchin Paediatrics, vol. 82, no. 3, pp. 194–200, 2014.
[21] H. C. Johnstone and T. D. Cheetham, “GH and cortisolresponse to glucagon administration in short children,” Hor-mone Research, vol. 62, no. 1, pp. 27–32, 2004.
[22] Y. Simsek, Z. Karaca, F. Tanriverdi, K. Unluhizarci, A. Selcuklu,and F. Kelestimur, “A comparison of low-dose ACTH, glucagonstimulation and insulin tolerance test in patients with pituitarydisorders,”Clinical Endocrinology, vol. 82, no. 1, pp. 45–52, 2015.
[23] A. H. Hamrahian, K. C. J. Yuen, M. B. Gordon, K. J. Pulaski-Liebert, J. Bena, and B. M. K. Biller, “Revised GH and cortisolcut-points for the glucagon stimulation test in the evaluationof GH and hypothalamic–pituitary–adrenal axes in adults:results from a prospective randomized multicenter study,” ThePituitary Society, vol. 19, no. 3, pp. 332–341, 2016.
[24] G. Binder, A. Bosk,M.Gass,M. B. Ranke, and P.H.Heidemann,“Insulin tolerance test causes hypokalaemia and can provokecardiac arrhythmias,” Hormone Research, vol. 62, no. 2, pp. 84–87, 2004.
[25] T. M. Flad, J. M. Kirby, S. K. Cunningham, and T. J. McKenna,“The overnight single-dosemetyrapone test is a simple and reli-able index of the hypothalamic-pituitary-adrenal axis,” ClinicalEndocrinology, vol. 40, no. 5, pp. 603–609, 1994.
[26] B. L. Linder, N. V. Esteban, A. L. Yergey, J. C. Winterer, D. L.Loriaux, and F. Cassorla, “Cortisol production rate in childhoodand adolescence,” Journal of Pediatrics, vol. 117, no. 6, pp. 892–896, 1990.
[27] C. J. DeVile and R. Stanhope, “Hydrocortisone replacementtherapy in children and adolescents with hypopituitarism,”Clinical Endocrinology, vol. 47, no. 1, pp. 37–41, 1997.
[28] P. M. Mah, R. C. Jenkins, A. Rostami-Hodjegan et al., “Weight-related dosing, timing and monitoring hydrocortisone replace-ment therapy in patients with adrenal insufficiency,” ClinicalEndocrinology, vol. 61, no. 3, pp. 367–375, 2004.
[29] O. Lakhani, S. Tripathi, K. Indu, and M. Desai, “Levothyrox-ine replacement before glucocorticoid replacement leading toadrenal crisis in a case of autoimmune polyendocrine syndrometype II (Schmidt syndrome),”Thyroid Research and Practice, vol.12, no. 3, p. 116, 2015.
[30] V. Fonseca, R. Brown, D. Hochhauser, J. Ginsburg, and C.W. H.Havard, “Acute adrenal crisis precipitated by thyroxine,” British
Medical Journal (Clinical Research ed.), vol. 292, no. 6529, pp.1185-1186, 1986.
[31] J. P. Fawcett, D.W. Boulton, R. Jiang, and D. J. Woods, “Stabilityof hydrocortisone oral suspensions prepared from tablets andpowder,” Annals of Pharmacotherapy, vol. 29, no. 10, pp. 987–990, 1995.
[32] K. Sarafoglou, M. T. Gonzalez-Bolanos, C. L. Zimmerman,T. Boonstra, O. Yaw Addo, and R. Brundage, “Compar-ison of cortisol exposures and pharmacodynamic adrenalsteroid responses to hydrocortisone suspension VS. Commer-cial tablets,”Clinical Pharmacology andTherapeutics, vol. 55, no.4, pp. 452–457, 2015.
[33] E. A. Webb and N. Krone, “Current and novel approaches tochildren and young people with congenital adrenal hyperplasiaand adrenal insufficiency,” Best Practice & Research ClinicalEndocrinology & Metabolism, vol. 29, no. 3, pp. 449–468, 2015.
[34] Group JLECW, “Consensus statement on 21-hydroxylase defi-ciency from the Lawson Wilkins pediatric endocrine societyand the European Society for Paediatric Endocrinology,” TheJournal of Clinical Endocrinology & Metabolism, 2013.
[35] D. M. Hume, C. C. Bell, and F. Bartter, “Direct measurement ofadrenal secretion during operative trauma and convalescence,”Surgery, vol. 52, no. 1, pp. 174–187, 1962.
[36] S. W. J. Lamberts, H. A. Bruining, and F. H. De Jong, “Corti-costeroid therapy in severe illness,”The New England Journal ofMedicine, vol. 337, no. 18, pp. 1285–1292, 1997.
[37] M. M. Erichsen, K. Løvas, B. Skinningsrud et al., “Clinical,immunological, and genetic features of autoimmune primaryadrenal insufficiency: observations from a Norwegian registry,”The Journal of Clinical Endocrinology &Metabolism, vol. 94, no.12, pp. 4882–4890, 2009.
[38] G. Meyer, A. Hackemann, J. Reusch, and K. Badenhoop,“Nocturnal hypoglycemia identified by a continuous glucosemonitoring system in patients with primary adrenal insuffi-ciency (Addison’s disease),”Diabetes Technology&Therapeutics,vol. 14, no. 5, pp. 386–388, 2012.
[39] R. Giordano, S.Marzotti,M. Balbo et al., “Metabolic and cardio-vascular profile in patients with Addison’s disease under con-ventional glucocorticoid replacement,” Journal of Endocrinolog-ical Investigation, vol. 32, no. 11, pp. 917–923, 2009.
[40] S. Bjornsdottir, A. Sundstrom, J. F. Ludvigsson, P. Blomqvist, O.Kampe, and S. Bensing, “Drug prescription patterns in patientswith Addison’s disease: A Swedish population-based cohortstudy,”The Journal of Clinical Endocrinology &Metabolism, vol.98, no. 5, pp. 2009–2018, 2013.
[41] A. Halper, B. Sanchez, J. S. Hodges et al., “Bone mineral densityand body composition in children with congenital adrenalhyperplasia,” Clinical Endocrinology, 2018.
[42] C. F.Mooij, E. A.Webb, H. L. ClaahsenVanDerGrinten, andN.Krone, “Cardiovascular health, growth and gonadal function inchildren and adolescents with congenital adrenal hyperplasia,”Archives of Disease in Childhood, vol. 102, no. 6, pp. 578–584,2017.
[43] A. Subbarayan, M. T. Dattani, C. J. Peters, and P. C. Hindmarsh,“Cardiovascular risk factors in children and adolescents withcongenital adrenal hyperplasia due to 21-hydroxylase defi-ciency,” Clinical Endocrinology, vol. 80, no. 4, pp. 471–477, 2014.
[44] L. Plat, R. Leproult, M. L’Hermite-Baleriaux et al., “Metaboliceffects of short-term elevations of plasma cortisol are morepronounced in the evening than in the morning,”The Journal ofClinical Endocrinology & Metabolism, vol. 84, no. 9, pp. 3082–3092, 1999.

8 International Journal of Pediatrics
[45] S. Bjornsdottir, M. Øksnes, M. Isaksson et al., “Circadian hor-mone profiles and insulin sensitivity in patients with Addison’sdisease: A comparison of continuous subcutaneous hydrocor-tisone infusion with conventional glucocorticoid replacementtherapy,” Clinical Endocrinology, vol. 83, no. 1, pp. 28–35, 2015.
[46] A. A. Nella, A. Mallappa, A. F. Perritt et al., “A phase 2 studyof continuous subcutaneous hydrocortisone infusion in adultswith congenital adrenal hyperplasia,” The Journal of ClinicalEndocrinology & Metabolism, vol. 101, no. 12, pp. 4690–4698,2016.
[47] P. C. Hindmarsh, “The child with difficult to control CongenitalAdrenal Hyperplasia: Is there a place for continuous subcuta-neous hydrocortisone therapy,” Clinical Endocrinology, vol. 81,no. 1, pp. 15–18, 2014.
[48] A. Mallappa, N. Sinaii, P. Kumar et al., “A phase 2 study ofChronocort, a modified-release formulation of hydrocortisone,in the treatment of adults with classic congenital adrenal hyper-plasia,”The Journal of Clinical Endocrinology &Metabolism, vol.100, no. 3, pp. 1137–1145, 2015.
[49] CM. Jones, A. Mallappa, N. Reisch, N. Nikolaou, N. Krone,and BA. Hughes, “Modified release and conventional glu-cocorticoids and diurnal androgen excretion in congenitaladrenal hyperplasia,” The Journal of Clinical Endocrinology &Metabolism, pp. 2016–2855, 2016.
[50] R. Giordano, F. Guaraldi, E. Marinazzo et al., “Improvementof anthropometric and metabolic parameters, and quality oflife following treatment with dual-release hydrocortisone inpatients with Addison’s disease,” Endocrine Journal, vol. 51, no.2, pp. 360–368, 2016.
[51] G. Johannsson, H. Lennernas, C. Marelli, K. Rockich, and S.Skrtic, “Achieving a physiological cortisol profile with once-daily dual-release hydrocortisone: A pharmacokinetic study,”European Journal of Endocrinology, vol. 175, no. 1, pp. 85–93,2016.
[52] A. M. Isidori, M. A. Venneri, C. Graziadio et al., “Effect ofonce-daily, modified-release hydrocortisone versus standardglucocorticoid therapy on metabolism and innate immunityin patients with adrenal insufficiency (DREAM): a single-blind, randomised controlled trial,” The Lancet Diabetes &Endocrinology, vol. 6, no. 3, pp. 173–185, 2018.
[53] U. Neumann, M. J. Whitaker, S. Wiegand et al., “Absorptionand tolerability of taste-masked hydrocortisone granules inneonates, infants and children under 6 years of age with adrenalinsufficiency,” Clinical Endocrinology, vol. 88, no. 1, pp. 21–29,2018.

Stem Cells International
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Disease Markers
Hindawiwww.hindawi.com Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwww.hindawi.com Volume 2013
Hindawiwww.hindawi.com Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwww.hindawi.com Volume 2018
PPAR Research
Hindawi Publishing Corporation http://www.hindawi.com Volume 2013Hindawiwww.hindawi.com
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwww.hindawi.com Volume 2018
Journal of
ObesityJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwww.hindawi.com Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwww.hindawi.com Volume 2018
Diabetes ResearchJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Research and TreatmentAIDS
Hindawiwww.hindawi.com Volume 2018
Gastroenterology Research and Practice
Hindawiwww.hindawi.com Volume 2018
Parkinson’s Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwww.hindawi.com
Submit your manuscripts atwww.hindawi.com