Embed Size (px)
Citation preview

PEBB: 1/18/05Prepared by Aon Consulting 1
Chronic Disease Management 2003 Annual Report -Highlights
PEBB Board Meeting1/18/05
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 2
2003 Highlights - Outline
• Purpose of Annual CDM Report• Review Methodology• Prevalence Updates• Aon Reported Statistical Findings (Cost &
Utilization for Level I & Level II Analysis)• Carrier Program Design• Participation• Carrier Reported Clinical Measures• Summary and Next Steps
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 3
2003 Highlights - Outline
• Purpose of Annual CDM Report• Review Methodology• Prevalence Updates• Aon Reported Statistical Findings (Cost &
Utilization for Level I & Level II Analysis)• Carrier Program Design• Participation• Carrier Reported Clinical Measures• Summary and Next Steps
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 4
Purpose
To coordinate and measure theeffectiveness of component chronic diseasemanagement programs developed andadministered by PEBB’s medical insuranceCarriers (Kaiser and Regence).
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 5
2003 Highlights - Outline
• Purpose of Annual CDM Report• Review Methodology• Prevalence Updates• Aon Reported Statistical Findings (Cost &
Utilization for Level I & Level II Analysis)• Carrier Program Design• Participation• Carrier Reported Clinical Measures• Summary and Next Steps
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 6
Methodology
Aon Statistical Report• Examines 4 different chronic diseases: Asthma, Diabetes,
Coronary Artery Disease (CAD), Congestive Heart Failure (CHF)
• Measures changes in disease prevalence, participation, utilization, & cost for PEBB members based on incurred claims data
• Prevalence based on agreed-upon definitions of each chronic disease (ICD, CPT, & NDC Codes)
• Participation based on member list provided by carriers
• Three types of utilization & cost analysisLevel I – with & without diseaseLevel II – participant vs. non-participantsClinical Measures – provided by carriers
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 7
Methodology
Carrier Reported Clinical Measures• Additional clinical measures reported separately by carriers
from non-claims sources (e.g. chart notes).
• Data reported uses the criteria mutually agreed upon by both carriers as outlined in the 2003 CDM Report
• HEDIS* measures have been added as a benchmark where available
• Regence relies on claims system for reporting on clinical measures from administrative data and does not have access to lab results
* The carrier reported values should not be compared to HEDIS values as the carriers do not have the HEDIS continuous enrollment requirement. This difference in methodology was agreed to by both carriers at the beginning of the reporting process.
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 8
Methodology
Illustration of Different Criteria Used for the Three Types of Analysis
Level I AnalysisAll Diagnosis
Level IIAnalysis
Disease andRelated
Diagnosis Only
ClinicalMeasures
DiseaseDiagnosis
Only
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 9
2003 Highlights - Outline
• Purpose of Annual CDM Report• Review Methodology• Prevalence Updates• Aon Reported Statistical Findings (Cost &
Utilization for Level I & Level II Analysis)• Carrier Program Design• Participation• Carrier Reported Clinical Measures• Summary and Next Steps
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 10
Prevalence
• 11,835 (9.5%) PEBB members were identified with one or more of theses four chronic diseases as of 12/31/03, including:– 5.0% with Asthma– 3.6% with Diabetes– 1.75% with CAD– 0.50% with CHF
• 1,179 (0.94%) have more than one chronic disease
• Prevalence rates are generally consistent with industry benchmarks
• Prevalence rates are similar for both carriers for CAD and CHF. Kaiser has a much higher prevalence of Asthma and Diabetes than Regence
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 11
2003 Highlights - Outline
• Purpose of Annual CDM Report• Review Methodology• Prevalence Updates• Aon Reported Statistical Findings (Cost &
Utilization for Level I & Level II Analysis)• Carrier Program Design• Participation• Carrier Reported Clinical Measures• Summary and Next Steps
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 12
Aon Statistical Findings
Cost Findings• 28% of total 2003 PEBB claims were for members with at
least one of the four chronic disease (includes claims for non-disease related illness/injury)
• Average monthly claims for members (PMPM) with chronic disease was $570 – 4x higher than for those without chronic disease
• PMPM ranged from $493 for asthma to $2,039 for CHF
• Rate of increase in PMPM costs from 2002 to 2003 was 19% for members with chronic disease compared to a 5% increase for members without chronic disease
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 13
Aon Statistical Findings
Utilization Findings• Overall utilization continues to be higher for members with
chronic disease verses members without chronic disease
• Changes in utilization rates for members with chronic disease are mixed; additional analysis will be conducted to explain the reasons. Increases in utilization may be the result of members receiving appropriate preventive procedures which is positive.
• Still too early to confirm trends due to anomalies during the reporting period– 2002 consolidation of carriers and plan designs– Small numbers for PEBB’s chronic disease populations– Many members have co-morbidities that confound
analysis
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 14
2003 Highlights - Outline
• Purpose of Annual CDM Report• Review Methodology• Prevalence Updates• Aon Reported Statistical Findings (Cost &
Utilization for Level I & Level II Analysis)• Carrier Program Design• Participation• Carrier Reported Clinical Measures• Summary and Next Steps
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 15
Carrier Program Design
Kaiser• Members are automatically
registered in DM programs – ‘opt-out’ program
• Members are automatically considered participating once entered in the Disease Registry
• DM programs tightly integrated with physicians and case management
• Kaiser data collected through EMR which includes lab results
Regence• DM programs rely on
voluntary member participation – ‘opt-in’ program
• Member must receive 2 interventions to be considered a participant
• DM programs target the member and do not have direct contact with physicians
• Regence data relies on claims system for reporting from administrative data
A detailed description of the disease management programs for each carrier by disease is found in the ‘Carrier Interventions’ section
beginning on page 13 of the 2003 Report .
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 16
2003 Highlights - Outline
• Purpose of Annual CDM Report• Review Methodology• Prevalence Updates• Aon Reported Statistical Findings (Cost &
Utilization for Level I & Level II Analysis)• Carrier Program Design• Participation• Carrier Reported Clinical Measures• Summary and Next Steps
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 17
Participation
• Kaiser participation is 100% for all diseases
• Regence participation rates vary by disease:– Asthma: 56%– Diabetes: 74%– CAD: 27%– CHF: 34%
• Regence participation increased significantly for CAD and CHF as a result of substantial changes in the administration of its disease management programs. Participation in 2002 was 5% for each disease prior to the changes.
Note: Regence only contacts members considered ‘suitable’ for enrollment in disease
management. For participation based on Regence suitability refer to page 20 of the
2003 Report.
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 18
2003 Highlights - Outline
• Purpose of Annual CDM Report• Review Methodology• Prevalence Updates• Aon Reported Statistical Findings (Cost &
Utilization for Level I & Level II Analysis)• Carrier Program Design• Participation• Carrier Reported Clinical Measures• Summary and Next Steps
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 19
72.0%
71.2%
Carrier Reported Clinical Measures: Asthma
79.3%
79.0%Use of Appropriate Medications for Patients with Persistent Asthma
Kaiser Regence HEDIS 75th
•Good care for asthmatics includes preventing flares of wheezing and shortness of breath which interfere with the patient’s functioning.
•Two types of medication are used to treat patients with asthma; one to prevent acute flares, and one to treat acute flares when they occur
•Clinical Goal: increase in the percentage of patients regularly using medications to prevent acute flares
Note: HEDIS percentiles have been included for benchmarking only and should not be used as a comparator with the carrier reported values as the carriers do not have a continuous enrollment requirement.
Compliance with Appropriate Labs & Exams
2002
2003
Data for Regence is Not Available
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 20
47.7
52.1
Carrier Reported Clinical Measures: Asthma
59.5
60.6ER Visits per 1,000
Kaiser Regence HEDIS 75th
•Preventive treatment should reduce acute flares which cause the patient to seek emergency care
•Clinical Goal: a decrease in the number of ER visits by patients with asthma
Utilization Results
2002
2003
There is no HEDIS Equivalent
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 21
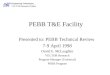
Carrier Reported Clinical Measures: Diabetes
50.9%
73.7%
49.8%
88.0%
51.7%
44.3%
52.9%
87.2%Mbrs (18-75 yrs old) who had HbA1c Test
Mbrs who had Eye Exam
Mbrs (18-75 yrs old) who had LDL-C Screening
Mbrs Monitored for Diabetic Nephropathy
Kaiser Regence HEDIS 75th
•Excellent care of diabetes includes good control of the blood sugar levels and of cardiac risk factors (coronary artery disease is the leading killer of diabetics)
•Early detection of eye or kidney disease can lead to interventions to prevent or delay the onset of blindness or kidney failure
•Clinical Goal: increase in percentage of members receiving appropriate screenings
49.2%
86.9%
40.7%
88.1%
35.0%
78.4%
33.2%
81.4%
58.7%
89.8%
60.4%
88.3%
52.8%
85.9%
61.3%
86.9%
Note: HEDIS percentiles have been included for benchmarking only and should not be used as a comparator with the carrier reported values as the carriers do not have a continuous enrollment
requirement.
Compliance with Appropriate Labs & Exams
2002
2003
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 22
61.0%
39.6%
55.5%
42.3%
Carrier Reported Clinical Measures: Diabetes
60.0%
23.9%
55.1%
26.0%Of the Mbrs Tested for HbA1c, the % of those tested with Poor HbA1c Control
Of the Mbrs Screened for LDL-C, the % of those screened with LDL-C Controlled
Kaiser Regence HEDIS 75th
•Proper care should result in controlled blood sugar level and controlled cardiac risk factors
•Clinical Goal:-Decrease in the percent of members with poor HbA1c control-Increase in the percent of members with LDL-C controlled
Note: HEDIS percentiles have been included for benchmarking only and should not be used as a comparator with the carrier reported values as the carriers do not have a continuous enrollment
requirement.
Clinical Results
2002
2003
Regence does not have Access to Lab Results
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 23
Carrier Reported Clinical Measures: Diabetes
154.5
137.3
35.8
90.9
25.1
8.4
ER visits per 1,000
Hospitalization for Diabetes or Comorbidity as Any Diagnosis
Kaiser Regence HEDIS 75th
•Proper care should result in a reduction in the number of hospital admissions and ER visits for members with diabetes
•Clinical Goal: decrease in the number of hospitalizations per 1,000 and ER visits per 1,000 for diabetics
130.9
136.4
34.9
67.6
11.0
9.1
Utilization Results
2002
2003
Hospitalization for Diabetes or Comorbidity as Primary Diagnosis
There are no HEDIS Equivalents
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 24
83.5%
97.9%
82.2%
97.0%
69.4%
86.2%
72.8%
79.6%
Carrier Reported Clinical Measures: CAD
57.6%
84.9%
87.0%
57.1%
81.0%
75.8%Mbrs Receiving Beta Blocker following a Heart Attack (AMI)
Mbrs who had LDL-C Screening following an Acute Coronary Event (AMI, CABG, PTCA)Mbrs Using Aspirin following an Acute Coronary Event (AMI, CABG, PTCA)
Kaiser Regence HEDIS 75th
•The goal of managing CAD is to prevent further events (angina/chest pain or repeat heart attacks) by controlling all risk factors (high blood pressure, cholesterol, inactivity, tobacco use)
•Beta Blocker medications are the best drug treatment for preventing recurrent heart attacks
•Aspirin has the ability to reduce clot formation in the narrowed coronary arteries
•Clinical Goal: increase in percentage of members receiving beta blocker treatment, cholesterol screening, and aspirin use
Note: HEDIS percentiles have been included for benchmarking only and should not be used as a comparator with the carrier reported values as the carriers do not have a continuous enrollment
requirement.
Compliance with Appropriate Labs & Exams
2002
2003 There is no HEDIS Equivalent
Regence does not have Access to Chart Notes
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 25
68.6%
67.2%
Carrier Reported Clinical Measures: CAD
89.3%
Of the Mbrs Screened for LDL-C, the % of those screened with LDL-C Controlled
Kaiser Regence HEDIS 75th
•LDL cholesterol is the form of cholesterol circulating in the blood that can attach to the blood vessel wall and cause further damage/narrowing
•Good care will result in management of all cardiac risk factors including cholesterol levels
•Clinical Goal: an increase in the percent of members with LDL-C controlled
Note: HEDIS percentiles have been included for benchmarking only and should not be used as a comparator with the carrier reported values as the carriers do not have a continuous enrollment
requirement.
Clinical Results
2002
2003
Regence does not have Access to Lab Results
Kaiser Data not Available in 2002
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 26
226.0
91.8
Carrier Reported Clinical Measures: CAD
153.9
127.0Hospital Admits for Members Having a Coronary Event (AMI, CABG, PTCA)
Kaiser Regence HEDIS 75th
•Preventive treatment should reduce the number of hospital admissions for members with CAD
•Clinical Goal: a decrease in the number of hospital admits per 1,000 for members with CAD
Utilization Results
2002
2003
There is no HEDIS Equivalent
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 27
65.8
1,315.8
18.2
1,389.1
Carrier Reported Clinical Measures: CHF
0.0
423.4
68.5
14.6
Hospital Days for CHF (per 1,000)
Re-admissions within 90 days (per 1,000)
Kaiser Regence HEDIS 75th
•There are two goals of treatment for CHF-Minimize patient care-After hospitalization, discharge in a stable condition so that patient is able to self-manage
•Appropriate diagnosis and care during hospitalization and appropriate management as an outpatient will reduce both the number of hospital admissions as well as the number of re-admissions
•Clinical Goal: decrease in both the number of hospital days and the number of re-admissions
Utilization Results
2002
2003
There are no HEDIS Equivalents
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 28
Carrier Reported Measures
Clinical Measures - Findings• Performance on appropriate screenings and exams
generally improved in 2003
• Utilization results are mixed; additional analysis will be conducted to explain the causes. For example, the increase in CAD hospitalizations may be due to increased use of PCTA’s which is positive.
• Both carriers scored below HEDIS 75th percentile on some measures, however, comparisons with HEDIS are difficult to interpret given the small size of PEBB’s chronic disease populations and differences in methodology
*HEDIS benchmark measures not directly comparable due to HEDIS continuous enrollment requirement
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 29
2003 Highlights - Outline
• Purpose of Annual CDM Report• Review Methodology• Prevalence Updates• Aon Reported Statistical Findings (Cost &
Utilization for Level I & Level II Analysis)• Carrier Program Design• Participation• Carrier Reported Clinical Measures• Summary and Next Steps
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 30
Summary
• There is clear evidence members with chronic disease experience higher cost and utilization than the population without chronic disease
• Performance on clinical measures generally improved in 2003
• Still too early to evaluate the effectiveness of PEBB’s Chronic Disease Management Program on controlling costs - consistent with current industry knowledge as outlined in the recent Congressional Budget Office findings
• In the early stages of evaluation, performance on clinical measures is a better short-term indicator of the overall effectiveness
• Additional experience is needed to isolate the long-term effect of chronic disease management due to:– Anomalies in 2002 reporting year (consolidation of carriers/plan
design)– Random variations possibly due to the small population being
measured
BD attach. 5

PEBB: 1/18/05Prepared by Aon Consulting 31
Recommendations for Future Program Direction
• Continue to track prevalence, utilization, cost, and clinical measures over time
• Encourage carriers to demonstrate continuous improvement in program design, participation, and outcomes
• Align current programs with 2007 Vision
• Develop intervention strategies for other conditions prevalent in the PEBB population e.g., obesity and smoking cessation
• Develop metrics and opportunities for collaboration to address depression
BD attach. 5