Embed Size (px)
Citation preview

-, x
.-,,^",.^.1^". . - t ^ ;;^^.-.""-.-..' ^ . ^ ^^I..,..: ,-; . , - ;'-, .. ,..
...I.'
,^;:''^ -, .. . -, - .-,I .. .,;. - ^ - - ;^ -^ — -^ w ',. . I — .1 1,. .
.I-.." -, ..I-^,,., - , .- , "^-' ^ I ", . I ^'i%^-^^-',.'-';'—..'.. "..—;.
.^' : ^'
.....1 "' ^ I ".:' ^ .. ..'' '.I - : , k , "- , " ^ , ' -'.; ^ ' Aj" - - -- ^ ,,^ ^^.l - , , ' -, ."- : ,. ! —
-
:
Peat M iwi5k '' -..,. - ,. ,'-"-"^':*.^ .W;'^^.. -j? - I -';;--:;;-.'i^ ^ ".1 ,'.,;...". ^' ^ --- ^;+,,41,_ Management Consultants , - "
- - -;. t .,..11
or, I S -
F,
:
--- r-- -
S - 4.
S- - --4
14 52 (
L -
- - .- -' S-S
& S
2 -ç-
Sf r1.
- 5-
5-'- - t -
--5 4' -
,ç-_,,4_.
`*i-
-
;_S-
'-
r--.'- 5,
)c:4.A - :
1992,_ _A
-i-"- r't,"45 -.
-t -j, 41_, -. s,,,
.5 ,-t--

thAfPeat Marwick
Department of Health
National Cervical Screening Programme- Option Review -
April 1992
Inormatiofl Centre.y of Health
w

kaA4Peat Marwick
Department of Health
National Cervical Screening Programme- Option Review -
- .Contents -
1. Executive Summary
1.1Terms of Reference1.2Findings1.3 Key Recommendations1.4 Other Recommendations
2. Existing Situation
2.1Introduction2.2 Systems Configuration2.3Existing Procedures2.4 Communications
3. Costs 6
3.1 Methodology3.2 AHB Survey3.3Statistics and Total Expenditure for AHB NCSP3.4 DOH Expenditure3.5Relevant Statistics3.6 Summary of Costs
4. Computer Options
4.1 Overview4.2Provisional Results4.3Further Rankings4.4Staffing Cost Differential of Option 4 versus Current Situation
Page
1
1123
4
4455
67889
10
12
13151717

kA4 iPeat Marwick
Page
5.NCSP Issues
Data SharingUse of NMPI NumberOpt on or Opt off RegisterNational Forms/Education PamphletsDOH Chart of Accounts and Management ReportReports to DOHDefinition of TermsHistology LinkDatabase DesignRHA/CHE StructureHelp DeskPre-EnrolmentsCommunity ClinicsAHB ApproachesHardware Ownership
Glossary
Appendices
Existing AHB NCSP ProceduresSurvey of Establishment and On-going CostsSurvey of all AHBsDOH Cervical Screening Costs to Date1990/91 DOH Costs1990-1992 $ Funding per Enrolment1990-1992 $ Funding Per FemaleAverage Number of Monthly Enrolments per FTEAverage Number of Enrolments per FFERegister Structure OptionsData Input OptionsSuggested Chart of Accounts/Monthly Management ReportPossible Report Information for DOH CollationDOH-NCSP Call Desk Statistics
5.15.25.35.45.55.65.75.85.95.105.115.125.135.145.15
1234567891011121314
19
191920202121212222222223232324

kAciPeat Marwick
1.Executive Summary
1.1Terms of Reference
KPMG Peat Marwick was requested by the National Cervical ScreeningProgramme ("NCSP") Manager to:
(i) examine and analyse the costs of the NCSP;
(ii) comment on the costs/benefits of converting the 14 Area HealthBoard ('AHB") databases into one national database.
1.2Findings
While we have carried out the terms of reference in as much detail as theinformation available allows, we have also highlighted some importantissues for resolution.
These issues are:
(i)
(ii)rat1 ii1d -0-3O%totaLfundmg toAHëãlfliRö?d,actualcotThaveexceeded-funding-byapproximately 90/o;
(iii) little in the way of regular, formal, detailed reporting on progress hasbeen provided to enable a clear relationship between expenditure andperformance to be established;
(iv) monitoring of performance and action on non-performance has notoccurred in a structured manner,
BE

ka6A4iPeat Marwick
(v) information on numbers of enrolments and numbers of smears takenfor enrolled women is inconsistent between Area Health Boards and
- requires further auditing;
(vi) the future control and funding of the programme; whether:
•directed by each Regional Health Authority;•directed by the Public Health bodies;•centrally directed
are the key issues to the future organisation of the database;
(vii) the additional costs of the most favourable option (option 4- onenational register on one machine) are less than the possibleoperational savings with centralised and automated input;
(viii) average costs to date are considered relatively high, namely:
$150 per enrolment over the three years to date;$44 per annum per enrolment to AHBs;
and require further attention.
1.3Key Recommendations
Our key recommendations include:
(i) instigate formal reporting structures;(ii) act on poor performance;(iii) institute an aggressive campaign to increase enrolment numbers;(iv) consider any decision on the restructuring of the databases and
computer facilities when a decision is made as to the structure andcontrol of the NCSP.
-2-

kAlb l Peat Marwick
1.4 Other Recommendations
In addition we make the following recommendations:
1.4.1 Reporting
A prescribed summary reporting should be required from eachregister which includes:
•summary number of enrolments;•summary number of smears•percentage change from previous period;•summary of operating costs;•number of abnormal smears;•number of education sessions.
This type of report will enable central monitoring regardless of thecomputer system operating.
1.4.2 Funding
Funding of the NCSP should include provision of base leveloperating costs for current enrolment levels and a fee for eachenrolment above the monthly enrolment level to enhanceperformance.
1.4.3 Publicity and Legislation
Aggressive publicity and 'opt off legislation is required to increasethe success of the NCSP. This is an area which should be handledcentrally to effect a consistent and economical approach.
SIE

2A4i'Peat Marwick
2.Existing Situation
2.1Introduction
The NCSP is currently divided into 14 separate registers with one located ateach AHB. All activities for the operation of the register are performed at anAHB level, with the exception of software development and support whichis performed at a national level at the Department of Health ("DOW).
At present there is no interaction between the systems at each AHB, nor anycombination of the registers at a national level, except as described in thecommunications section of this document
Pre-enrolment, enrolment, smear result recording, and reporting of resultsand recalls are all performed at an individual A}IB level.
2.2Systems Confiration
Fifteen separate Hewlett Packard PC 386 machines are used to run theregisters. One is at each of the AHBs and one at the DOH. The registerapplication software running on each of these machines is written in theIngres fourth generation language, and runs on the Unix operating systemCare has been taken to ensure that the software on each machine is identicaland that where enhancements or modifications are made to the applicationsystems, these changes are reflected on each of the 15 separate machines.
The software has been developed at the DOH by software consultants. Theconsulting firm has been retained by the department to maintain the softwareas required, and to run a national help desk located at the DOH.
-4-

kaA4 i Peat Marwick
- Most of the AHB machines are configured with 310 megabytes of diskstorage space and 4 megabytes of main memory. The exceptions to this are
- the machines at Auckland, Waikato, Wellington, Canterbury, and the DOH.where 8 megabytes of memory and 620 megabytes of disk space has beenprovided. All systems have two terminals attached excepting Waikato,
• - Wellington, Canterbury and Otago which have three terminals, and Aucklandwhich has five. In addition, each site has one Hewlett Packard Laser Jet IIIprinter and a Dot Matrix printer.
2.3Existing Procedures
Existing procedures for operation at the Area Health Board level are detailedin Appendix 1.
2.4Communications
At present there is no electronic communication between any machine withinthe system, with the exception of a link between the Paxus NMPI systemand the register at most AliBs. Transmission of data and software betweenAHBs, and between an A}IB and the DOH is by floppy diskette or tape.Similarly transmission of data between the private laboratories and theAHBs is by floppy diskette.
WIE

k'A4 ] Peat Marwick
3.Costs
3.1Methodology
This section deals with the costs of the NCSP covering both the DOH andthe A}iB costs. All costs exclude the actual costs of processing the smear asthese are paid directly to each laboratory from the DOlL Currently thereimbursement is $13.96 excluding GST for each smear.
Our approach was firstly to analyse the costs of a sample of AHBs. Sevenwere selected as representative by both size and geographical spread, andwere assessed from our experience as having relatively good financial datathat could be provided quickly.
Our selection was:
Auckland;•Northland;
•Taranaki;•Nelson-Marlborough;•West Coast;•Canterbury;•Otago.
A survey was prepared in conjunction with yourselves, Auckland AHB staffand Dr Terri Green, Health Fellow for Health Research Council. A copy ofthis survey is attached in Appendix 2. The survey asked for basicinformation that was expected to be available on statistics and costs ofestablishing the register and the ongoing annual operating costs.

044iPeat Marwick
3.2 AHB Survey
The AI{B survey provided us with cost information of AHB NCSP currentannual operating costs and establishment costs (where these were known).
In our sample of AHBs there was a mismatching of funding to actualexpenditure. Smaller AHBs in the sample are under-funded with the balanceprovided from the AHB's normal operating grants. Larger AHBs in thesample are overfunded, for example Otago currently subsidise some costs ofa smaller AHB. However some costs such as rent, telephones andmaintenance have not been budgeted for in the NCSP budgets within eachAHB, but have been provided from the AHB operating grant. These costsare considered to be under 10% of the total operating costs for NCSP at theAHBs.
Based on our sample, establishment costs to set up the programme averaged$0.95 for each female aged 15 to 64. These establishment costs excluded
I pilot site costs as pilot establishment costs were not available for analysis.The establishment costs were based on Canterbury, Northland, Otago,Taranaki and West Coast AHBs, as the most reasonable data available in thesample. The costs included setup of clinics, training of smeartakers, initialeducation and publicity projects. The major components were for computerrelated costs and capital items such as furniture and equipment.
Based on our sample of AHBs, on-going costs were $24.44 for eachenrolment on the NCSP (including pre-enrolment). The main costs in thiscategory are for staffing. These costs vary considerably between each AHBin the sample. Some AHBs use coordinators and community clinics, otherAHBs do not. Community clinic costs were analysed, but no detail obtainedof the percentage of enrolments or smears taken at these venues. Furtheranalysis would show the relative benefits of these clinics if good statisticswere available. We note that the survey results were not audited and thatAuckland did not return cost data for its district clinics. This skewed theaverage costs to a lower level than expected.
-7-

kaA.q4ipeat Marwick
3.3
Statistics and Total Expenditure for AHB NCSP
As no recent information was available for total enrolments and staffnumbers, we contacted all other AHBs by phone and fax. These replies are
- summarised in Appendix 3.
The appendix details, for each AHB and the total of all AHBs:
•staff numbers by type;•
number of enrolments (including pre-enrolments as these are notalways known separately);
•number of smear results processed;•number of pre-enrolments (where known);•
female population by AHB (based on 1990 estimates fromDepartment of Statistics, aged 15-64 years);
•funding from DOH each year.
This information has been collated and various statistics provided. Many ofthese statistics would be appropriate monitoring tools for the DOH.
3.4 DOH Exrenditure
The DOH costs to date were also analysed to determine the areas ofexpenditure involved. A summary of this by year is in Appendix 4, showingthe total DOH expenditure of $15,474,000 for the three years to 30 June1992.
The 1990/91 DOH costs of $1,713,000 for the NCSP are estimated at:
Establishment costs $845,000Annual ongoing costs $543,000Other sundry projects $325,000
$1,713,000
-8-

k.A4b]Peat Marwick
These are further detailed in Appendix 5.
Establishment costs were considered to be one-off setup costs and includedcomputer implementation and developments, policy statement preparation,initial printing of forms and leaflets, the initial publicity campaign and legal
costs.
Annual ongoing costs for the DOH includes the NCSP specific staff(currently 6), committee meeting costs, computer maintenance contracts, andequipment rental.
You expect that these costs should reduce substantially in future years, as theNCSP computer system is now stable and initial policy formulation time washigh. However, if major changes to policy are being considered, such as theHistology link and 'opt off legislation, these costs could remain at this level.Any software changes necessary would also involve some one-off setupcosts for this development.
3.5Relevant Statistics
Total funding to DOH and AHBs over the three years to 30 June1992 calculates at an average of $149.97 per enrolment
Funding over the two years to 30 June 1992 to AHBs calculates at anaverage of $44 per annum for each enrolment (refer Appendix 6),and ranges from $15 to $140 for each enrolment.
Funding in the two years to 30 June 1992 to AHBs calculates at anaverage of $4 per annum for every woman aged 15 to 64 in NewZealand (refer Appendix 7), and ranges from $3.67 to $7.05 for
every woman.
An average of 8,400 women are enrolled each month.
S

kAi lpeat Marwick
•8 women out of 1,000 are enrolled each month.
•On average, 150 women are enrolled each month for each staffmember (Appendix 8).
•On average, 1,845 enrolments have been recorded for each staffmember (refer Appendix 9).
•9.38% of women aged 15 to 64 are enrolled.
•103,000 women are enrolled.
3.6 Summary of Costs
The details of DOH costs and AHB NCSP grants for the three years to 30June 1992 are set out in Appendix 4.
In summary these are:
DOH Costs $NCSP Policy Output 3,351,855CS Benefits Paid 5,291AHB Register Hardware 1,500,000POBOC: Register, Advisory Education 1.497.000
6,354,146AHB NCSP Grants 9,119,503
Total Paid Out 15,473,649
-10-

0A4 1 Peat Marwick
Actual costs 1991/92 excluding Option 3 compared with funding for the sixAHBs surveyed who supplied full data were as follows:
CostsFundingDifference($)($)
($)
NorthlandTaranakiNelson MarlboroughWest CoastCanterburyOtago
Totals
226,355170,000
198,558196,000
201,859144,000
106,37644,000
559,068607,000
253,283245,000
1,545,4991,406,000
(56,355)(2,558)
(57,859)(62,376)
47,932(8,283)
(139,499)
Note: That these figures have been obtained by survey of the Boardsconcerned and the information has not been audited.
- 11 -

k)'A4& peat Marwick
4.Computer Options
We have examined a number of options for the restructuring of the database systemsto improve both the cost effectiveness of operating the NCSP register and theamount of information available from the NCSP. We have looked at four majoroptions as follows
Option 1
One database at each AHB as at present, with a link to provide relevantinformation to the DOH at a national level;
Option 2
Combination of the 14 existing AHB databases into four regional healthauthority (RI-IA) registers, running on a machine located at each RHA;
Option 3
Combination of the 14 existing AHB databases into four RHA registerswhich would be operated on a single computer,
•Option 4
One single national database computer operated from a central location.
In addition we have investigated the possible data input methods within each of theabove options. These methods are:
•input from private and public laboratories;•input by AHB staff (similar to existing system);•input by centralised data entry staff.
Data input options are detailed more fully in Appendix 11.
-12-

kA4bi Peat Marwick
4.1Overview
The four options for database structure which are examined in greater detailin Appendix 10, all provide for a greater level of summary informationretrieval at a national level than is achieved at present.
During the course of our investigation into the NCSP we have determinedthat one of the greatest perceived deficiencies of the current databasestructure is the lack of information available at a national leveL Thisdeficiency is conceptually one of the easiest problems to fix. All fouroptions discussed in Appendix 10 make some summary data available at anational level.
Attached is a cost summary schedule for available costs of computersystems.
-13-

Cost Summary
Option 1Option 2Option 3Option 4
14 AHBs4 RHAs4 RHAs 1 rn/c1 Central
Additional hardware n/a324,000190,000-.190,000
Ingres licences n/a120,00090,000 )t90,000;
Communications charges: AHB - DOH not available n/a n/a n/a
Communications charges: RHA - DOH n/anot available n/a n/a
Software to extract summary data from (AHB,not availablenot availablenot available n/aRHA) register
Transmission of summary data to DOH not availablenot available n/a n/a
Combination and reporting on summary data atnot availablenot availablenot available n/aDOH
Hardware maintenance: new (pa) 87,00060,00033,800 33,800lessexisting (pa) (-8000r8-7,00)---- —7OOO--- —81tRD0J
Total 0417,000226,800226,800
Note: n/a is not applicablecosts marked not available indicate further research is needed to determine this cost.
SO
oQ
çC) C)-Y '- S pC(

Ranking Model
In this model, the four options as detailed in section 4 and Appendix 10 are ranked by category, and are compared with the existingsituation.
A score of "5" in a particular category indicates the best result for that particular category.
Category No changeOption 1Opton 2Option 3Option 414 AHBs4 RHAs 4 RHAs 1 rn/c1 central
Hardware and software costs 5 5 1 2 2
Fit to RHA environment 1 1 5 5 3
Fit to PH Agency environment 2 2 3 3 5
Ease of support and operation of database 1 1 3 5 5
Ease of summary reporting 1 2 3 4 5
Confidentiality of data 5 4 3 2 1
TOTAL 15 15 18 21 21

ka5A4 1 Peat Marwick
4.3Further Ranldngs
Each of the categories was then weighted by Gillian Grew as to itsimportance.
Marginally, the most favourable option is Option 4(1 central data base).Further cost analysis on this option was then considered.
Weighted Table
NoOption 1 Option 2 Option 3 Option 4CategoryWeightChange14 AHBs 4 RHAs 4 RHAs I Central
1 M/CHardware andsoftware costs105050102020
Fit to RHAEnvironment 999454527
Fit to PH AgencyEnvironment 91818272745
Ease of Support &Operation of 888244040Database
Ease of SummaryReporting 8816243240
Confidentiality 7352821147
TOTAL 128129151178179
4.4Staffing Cost Differential of Option 4 versus Current Situation
A data input staff of three would initially be required in a central location.Current distributed data input staff in AHBs total 12. A saving of $189,000(9 data input staff at $21,000 each) would result.
In addition, systems administrator numbers and clerical staff would reducewhen batching and administration of computer systems move to a centrallocation. Up to 13 staff could be redeployed at approximately $260,000 forthe 10 systems administrator and $72,000 for the three clerical positions.
-17-

kA4i peat Marwick
This is an estimate of staff savings assuming that results are automaticallyupdated by laboratories. Further savings would be made if a reduction ofnumber of enrolments by a central location occurred and increasing numberswere made through the laboratories using the future National Health Index.
There will be a transitional period when NMPI registration is still used andlaboratories do not have access to a National Index and double entry will stilloccur.
Laboratories may well require a small amount of extra clerical staff toadminister this transfer of information.
Total staff savings of Option 4 over the current situation are approximately$521,000. Costs of supplementary hardware and software areapproximately $227,000. Communications and data transfer costs fromlaboratories to the register have not been included at this stage.
-18-

kAthiPeat Marwick
S.NCSP Issues
We have identified a number of issues as a result of our involvement with thisproject. While not necessarily quantifiable or affecting the costs of the NCSP, webelieve they are worthy of mention.
5.1Data Sharing
There is a general unease about the sharing of data at a national level,particularly by certain groups such as Maori women. These groups mayprefer that data was not combined at a national level. We believe that it isimportant for the programme to be able to monitor its progress andeffectiveness by the collection and analysis of at least summary data at anational level.
One of the objectives of the NCSP is the enrolment of and recording ofsmears for as many women as possible on the register. Summary datasufficient to be able to monitor progress and to assist with the targeting ofspecific priority groups should be available to assist with this objective.
5.2 Use of NMPI Number
We are aware of discussion concerning the suitability of continuing to usethe NMPI number as the key identifier of records on the NCSP register. Wehave encountered criticism that the Paxus NMPI database is not accurate andthese inaccuracies will be transferred to the NCSP system.
We recommend that a national code number is used as the record identifier.The development of a completely independent index for NCSP purposeswould seem contrary to the recent suggestions by the Government topromote some commonality of record identifiers for various nationaldatabases.
-19-

kA4iPeat Marwick
The experience of the Victoria, Australia register which does not use awoman record index system, is that many women's records are duplicated,i.e. one woman may have several records on the system and these are notrelated to each other. In the opinion of the register controller for Victoria,this has been caused by their failure to use a national indexing system.
5.3 Opt on or Opt off Register
In discussion with yourself and some register controllers and pathologistsaround the country, we noted that most believe the NCSP would be moreeffective and successful if the register were run as an opt off scheme. Interms of achieving the objective of the programme, any change which seesmore women enrolled on the register will be beneficial.
5.4National Forms/Education Pamphlets
During the initial establishment, publicity material and enrolment forms etc.were provided from the DOH. Currently AHBs print or photocopy theirown forms and materials. This includes:
•enrolment and pre-enrolment forms;
•change of status;
•change of detail;
•batch input headers;
•register information leaflets for women.
Benefits and overall cost savings due to economies of scale could resultfrom use of standard NZ wide forms and leaflets, which could use anidentifiable logo as used in other national advertisements.
-20-

kAqiPeat Marwick
5.5 DOH Chart of Accounts and Management Report
From our analysis of your DOH costs, it is apparent that there are too manyaccount codes used with small balances, and monthly variance reports oflimited value are produced. We enclose in Appendix 12 a sample Chart ofAccounts with a small number of accounts that could easily fit within theDOH coding structure. A sample Monthly Variance Report using theseaccounts is also attached. These would give you regular summarisedinformation on the DOH costs of the NCSP.
5.6 Reports to DOH
The DOH need to establish their direction on reports from each register. Webelieve that a reporting requirement should be established to enable progressto be monitored regularly as the register grows. We have included a set ofpossible reports and performance measures which we consider would help tomonitor progress as Appendix 13. Regardless of the operating environmentthese could be faxed each month to the DOH for collation on a PC andreporting back to all registers.
5.7Definition of Terms
From discussion with A}{B register controllers, there appears to be someconfusion as to the definition of terms used when the DOH requestsinformation from each register. This issue needs to be addressed ifmeaningful monitoring information is to flow from the registers, usingmanually extracted and collated information.
-21-

Ik'Peat Marwick
5.8Histology Link
We believe that a link to the histology records maintained by the nationalPaxus NMPI system for a particular woman, would be advantageous to theNCSP register. If input to the register were to be performed by thelaboratories, such histology information would also be available whenanalysing a woman's smear results. This could be of benefit to assist withtargeting specific "at risk" groups.
5.9Database Design
We have not analysed the NCSP software controlling the registers andcannot comment as to its efficiency. The removal of the previouslydownloaded Paxus NMPI data from the Wellington and Auckland machinesdue to the excessive database search times now requires these two AHBs tolink to Paxus to search for NMPI codes, at a cost to the programme. Weanticipate that any combination of the registers into 4 or 1 database couldcompound the database search problem. We suggest that the DOH considera review of the NCSP database software with a view to optimising the searchalgorithms.
5.10 RHA/CHE Structure
The restructuring of the current AHBs environment into RHAs may meanthat the existing AHB registers have no logical place in the new structure. Adecision to retain 14 separate registers, may bear little relationship to thenew RHA/CHE structure.
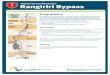
5.11 Help Desk
An analysis of the help desk statistics reveals that 106 calls were received bythe desk during the month of February 1992. Appendix 14 indicates (basedon this sample) that there is a reduction in calls to the desk as the length oftime the system has been installed increases.
-22-

kAf 1 Peat Marwick
An average of 5.3 calls per day were received in this period by the helpdesk. This is a low rate and possibly indicates the stability of the currentsoftware. The DOH may wish to review the need for a fuiltime help desk,given the low call rates being experienced.
5.12 Pre-Enrolments
The value of continuing with the processing of pre-enrolments needs to bediscussed with all AHB registers. Currently the national total appears verysmall, but the value cannot be easily quantified. It may be preferable in theshort term to concentrate on increasing the percentage of enrolments with asmear taken. Six AHBs do not currently bother to collect any pre-enrolments.
5.13 Community Clinics
From the sample of seven AHBs, it is clear that not all AHBs use theirfunding for operating community clinics. Numbers of enrolments andsmears taken at these clinics were not separately recorded to allow acomparison of enrolments between clinics and other facilities.
5.14 AHB Approaches
It is apparent that many of the AHBs are following procedures whichdemonstrate minor differences from those at other AHBs. While this is notnecessarily a problem it can lead to inefficiencies in operating the systems.These differences are usually caused by either.
(a)unclear directions, or a lack of control from the central controller,e.g. central requests for ad hoc information not always clearlydefined and with differing requirements and definitions; or
-23-

kA4 1 Peat Marwick
(b)specific changes introduced to procedures at the AHB level withoutauthority from the central controller, e.g:
(1)removal of initial downloaded NMPI data from the registers;(ii) redesign of the enrolment forms and publicity leaflets;(iii) decision not to pre-enrol in some AHBs;(iv) procedures for notification of abnormal results differs in each
AHB.
We suggest that if the registers are to continue to operate at an AHB level,that more control is exerted by the DOH over the running of the register toboth:
(a) maintain a consistent nationwide approach, and
(b) be able to take advantage of improvements in efficiency across thewhole country.
Written procedures covering all areas of policy and operation for use atregister level are necessary to assist new and existing staff.
5.15 Hardware Ownership
We note that the Hewlett Packard PCs which run the NCSP registers atpresent were gifted to the AHBs by the DOH. Any scheme which sees theregisters moved off the PCs onto one or four centralised machines will makethis equipment redundant. While it could be traded in against the purchase ofnew hardware, we believe that it is more cost effective to utilise thisequipment for other purposes at the AHBs or DOH. The 15% discountapplied by Hewlett Packard on costings for centralised equipment does notdepend on trading the existing PCs back.
-24-

k)A41 peat Marwick
Glossary
The following abbreviations have been used in this document
AHB:Area Health Board
DOH:Department of Health
NCSP:National Cervical Screening Programme
NMPI:National Master Patient Index
RHA:Regional Health Authority

k.A4b 1peat Marwick
Appendices

kfiPeat Marwick
Appendix 1
Existing AHB NCSP Procedures
The initial database setup at each of the 14 AHBs involved the download of relevantinformation for women from the National Master Patient Index ("NMPF') system. This datawas extracted from the NMPI system based on both domicile code and age and loaded ontoeach AHB register. The information downloaded used the NMPI number as the uniqueidentifier for each woman record.
Women in the AHBs have been encouraged to pre-enrol for the NCSP. This process showsa woman's active interest in participating in the programme even though a smear has notbeen taken. Such women are described as registered but not active. When the results of asmear test are available for a specific woman, data is entered to the Al-TB registers for thatwoman and her status becomes registered and active.
Where a smear result is received for a woman who has not pre-enrolled, enrolment detailsfrom the enrolment form are entered and matched with the woman's first smear result on theregister.
On receipt of a pre-enrolment form or an enrolment form, the NCSP operator at the AHBsearches for the woman's NMPI number based on name, address, and age information, assupplied on the forms. The operator first searches the register's database for the appropriaterecord, if pre-enrolled, or a previous smear result on the register. If unable to locate theappropriate record the operator then searches through the previously downloadedinformation from Paxus which is held on the AHB NCSP machine. If the search of thedownloaded information is unsuccessful the operator then logs on to the Paxus systemthrough the NCSP terminal and attempts to locate the woman on the national Paxus NMPIsystem. If still unable to locate the woman, the NCSP operator will add a record to thePaxus NMPI database and use this same number to create a record on the NCSP register.In some AHBs this process using the Paxus NMPI may be completed by medical recordsstaff.

kA4-1 Peat Marwick
This is a somewhat lengthy procedure for those women who do not have a NMPI numberincluded with their laboratory results and forms. At both the Wellington and AucklandAHBs, the records initially downloaded to the registers from the Paxus system have beendeleted due to excessive search times on the local databases when attempting to locate theappropriate NMPI records.
On completion of a smear analysis by the laboratory, result data is transferred to floppydiskette by each laboratory and given to the NCSP operator on a regular (e.g. daily, weekly)basis for uploading to the local register. Upon uploading of the data to the AHB register,some data validation procedures are completed by the software, and the smear result isentered to the register. Data rejected by the validation programme is returned to theappropriate laboratory for checking and correction. This is then reloaded Onto the registerfor completion of the batches of enrolments.
Information on a woman's change of address is provided to each AHB by the NMPIsystem. This prompts the operator at each AHB to output history data for women who havetransferred to another AHB to floppy diskette. This is subsequently posted to theappropriate AHB in which the woman now resides. On receipt at the appropriate AHB, thishistory information is uploaded to their local database.
Manual forms for change of address and other details, or a change in status (active/non-active) are also received direct from women or smear takers. These are input into the localregister to update the woman's record. Change of status forms make recall reports inactivefor women if receiving follow-up treatment such as colposcopy.
Reports are provided on a periodic basis from each AHB to the DOH. These are generalstatistical reports and to date have been on an as required basis.
Any software modifications which are required to the registers are performed by thesoftware consultants and each AHB register is updated by distribution of back up tapes.

Appendix 2Page 1
Department of Health - Cervical Screening Programme
Survey of Establishment and Ongoing Costs
Purpose: KPMG Peat Marwick have been asked by theDepartment of Health to compile the overall costs ofthe Cervical Screening Programme for use in futurerationalisatjon
Name of AHB Programme:
Contact phone number.(
Date Established:
Number of Registrations to Date:
Smears;
Enrolment;
•Pre-enrolments;
Total.
(A sample of Area Health Boards are being surveyed only and yours was chosen as beingrepresentative)
Please note that this survey is additional to that provided recently by Dr Terri Green butcomplementary to it.Replies are required by 5 p.m. Thursday 19 March 1992 and you will be contacted todiscuss your replies.
Mark as not applicable (N/A) if not relevant to your AHB

AppendixPage 2
Full entTime EstablishmAnnualEquivalentCostsOperatingStaff (IF Costs
Staff Costs
•Programme Manager•Systems Administrator•Data Entry•Clerical•Other co-ordinators (such as health
educators, Maori & Pacific Island)
Other Staff Costs
Computer Costs
•Paxus processing (NMPIregistration)
•Depreciation of equipment•Disks for Laboratories•Disks for backups
Postage/Franking and courier costs
Rental of equipment (fax machine,photocopier)
Stationery and Printing
Telephone & Tolls
Rental of building
Electricity
Mileage or Vehicle Expenses

Appendix 2Page 3
T
Fu1H1Time Establishment AnnuajvalentCostsOperatingFTE's) Costs____ $ S
Community clinic costs:•Staffing•Rental of site•Rental of Equipment•Smearraking Items(slides, spatulas)•Training of smear takers•Other costs
Education/Publicity costs
Priority Groups including Maori/Pacific Island (If separate from theabove caxegories,please detail)
Other Costs (please detail if over$5000)
Capital Costs:
•Cars•Furniture & Fittings•Equipment Purchased
(note date purchased and cost price)

Appendix 2Page 4
Notes
1. Establishment costs arc the one off costs to set up the register including publicity.
2. Annual operating costs are the ongoing costs for the register based on actual orbudget costs.
3. Community clinic costs relate to alternative venues set up and paid for by theprogramme. Note if not applicable to you.
4. If there are no costs in your budget relating to any item please note this and if knownwho pays state this as well (e.g. items paid by AHB).
5. If cost are recorded by various activities such as administradon,sreening;egister,education,etc please detail these under each item.
6. Other staff costs include recruitment, training, conferences and meetings.
7. Education and publicity costs include promotion packs, seminars and publicmeetings.
8. Stationery and printing costs include computer paper, envelopes, photocopying,forms.
I

Survey of all Area Health Boards NCSP Area Health Board
* Full cost survey provided * Northland * AucklandWaikatoBOPTairawhiti
Programme Manager 1.001.001.001.001.00Systems Administrator i .001.001.001.001.00Data Entry 3.00 0.40Clerical 0.200.401.00Other Co-ordinators 1.454.002.00 1.00
Total Staff FTE 3.659.405.002.403.00
Number of enrolments(incl. Pre-enrolments) 5,80912,7593,4164,5002,477Number of smear results(if not available from AHB = enrolments 4,27310,5003,4844,5001,919Number of pre-enrolments 1,626 small
1990 Female Estimated Population(15-64 years) 40,000314,440104,90065,23013,720Source:Dept of Stats based on 1986 census estimated to 31/3/90 by AHB
Funding 1991/92 $170,000$1,265,000$419,000$279,000$62,000Funding 1990/91 $183,000$1,043,000$432,000$277,000$100,000
$1990-1992 AHB Funding/Enrolments $60.77$180.89$249.12$123.56$65.40$1990-1992 AHB Funding/Female population(15-64) $8.83$7.34$8.11$8.52$11.81
Number of months operating 21 7 6 12Average number of enrolments/month 2771,823569900206Average number of enrolments per month/1000 Female population (15-64 7 6 5 14 15Average number of smears/month 2031,500581900160
Average number of enrolments/FTE 1,5921,3576831,875826Average monthly enrolments/FTE 76194114375 69
% Enrolments/ Female population(15-64) 14.52%4.06%3.26%6.90%18.05%No. Smears/1000 Female population(15-64) 10713 3 133 691140 tjj

J --
Survey of all Area Health Boards NCSP IArea Health Board
* Full cost survey provided * TaranakiHawkes BayM-WangWellingtonNel-Marl
Programme Manager 1.001.001.000.501.00Systems Administrator i .001.001.001.00Data Entry 0.601.001.16ClericalOther Co-ordinators 1.002.50 0.75
Total Staff FTE 2.003.005.102.502.91
Number of enrolments(incl. Pre-enrolments) 8,4413,04314,7353,60010,927Number of smear results(if not available from AHB = enrolments 5,27212,20114,7353,6004,226Number of pre-enrolments 338 33
1990 Female Estimated Population (15-64 years) 45,19034,74070,760132,28033,560Source:Dept of Stats based on 1986 census estimated to 31/3/90 by AHB
Funding 1991/92 $196,000$149,000$312,000$502,000$144,000Funding 1990/91 $201,000$171,000$295,000$504,000$193,000
$1990-1992 AHB Funding/Enrolments $47.03$105.16$41.19$279.44$30.84$1990-1992 AHB Funding/Female population(15-64) $8.79$9.21$8.58$7.61$10.04
Number of months operating ii 7 27 2 20Average number of enrolments/month 7674355461,800546Average number of enrolments per month/1000 Female population (15-64 17 13 8 14 16Average number of smears/month 4791,7435461,800211
Average number of enrolments/FTE 4,2211,0142,8891,4403,755Average monthly enrolments/FTE 384145107720188
% Enrolments/ Female population(15-64) 18.68%18.76%120.82%12.72%132.56%No. Smears/boo Female population(15-64) 117135112081271126

Ij
Survey of all Area Health Boards NCSP I IArea Health Board
* Full cost survey provided West Coast * Canterbury *
OtagoSouthland fotal/Averag
Programme Manager 1.001.001.001.0013.50Systems Administrator 0.501.001.001.0012.50Data Entry 1.001.000.508.66Clerical 2.00 3.6 0Other Co-ordinators 0.103.50 1.3817.68
Total Staff FTE 1.608.503.003.8855.94
Number of enrolments(incl. Pre-enrolments) 2,79013,9669,5037,228103,194Number of smear results(if not available from AHB = enrolments 2,20411,8836,8544,23189,882Number of pre-enrolments 1,344 202,7552,9979,113
1990 Female Estimated Population(15-64 years) 10,210143,53057,39034,5201,100,470Source:Dept of Stats based on 1986 census estimated to 31/3/90 by AHB
Funding 1991/92 $44,000$607,000$245,000$136,000$4,530,000Funding 1990/91 $100,000$549,000$312,000$171,000$4,531,000
$1990-1992 AHB Funding/Enrolments $51.61$82.77$58.61$42.47$87.81$1990-1992 AHB Funding/Female population (15-64) $14.10$8.05$9.71$8.89$823
Number of months operating 14 20 9 1112.29Average number of enrolments/month 1996981,0566578,400Average number of enrolments per month/1000 Female population (15-64 20 5 18 19 8Average number of smears/month 1575947623857,316
Average number of enrolments/FTE 1,7441,6433,1681,8651,845Average monthly enrolments/FTE 125 82352170150
% Enrolments/ Female population(15-64) 27.33%9.73%16.56%20.94%9.38%No. Smears/1000 Female population(15-64) 2161 831119 1123 82

Appendix 4Department of Health Cervical Screening Total Costs to Date
NCSP : Policy Output
Smear Benefits Paid
A%HB Register Hardware
POBOC CS (Register, advisory education)
3ub-Total
POBOC : AHB
1otal Paid Out
1989/901990/911991/92TotalActualActualBudget
$ $ $ $
1,065,8551,713,000573,0003,351,855
5,291 0 05,291
01,500,000 01,500,000
0 01,497,0001,497,000
1,071,1463,213,0002,070,0006,354,146
119,5034,500,0004,500,0009,119,503
$1,190,649$7,713,000$6,570,000$15,473,649
Department of Health Cervical Screening Total Allocated to Date
1989/901990/911991/92TotalAllocatedAllocatedAllocatedAllocated
$ $ $ $YCSP : Policy Output 3,651,7501,739,000573,0005,963,750rnear Benefits Paid 5,080,5005,010,000 010,090,500
AHB Register Hardware 01,500,000 01,500,000D OBOC : CS (Register, advisory ,education) 0 01,497,0001,497,000ub-Total 8,732,2508,249,0002,070,00019,051,250
POBOC:AHB 5,674,0005,484,0004,500,00015,658,000lotal Allocated $14,406,250$13,733,000$6,570,000$34,709,250

1990-1991 DOH Costs Appendix 5
Establishment EstablishmentOngoingOngoingCostsCostsCostsCosts$000s$000's$000's$000's
Y/E 6/91Y/E 6/91Y/E 6/91Y/E 6/91
Staff CostsSalaries and WagesOther StaffOther Staff CostsTotal Staff Costs
Professional servicesLegalPolicy Statement-NaullsBusiness analysis/programmingImplementation/DevelopmentImplementation/Project Management
Total Professional Services
Committee/Meetings and Travel Expenses
Publicity/Promotions
Printing and Stationery
Computer CostsRentalProcessing Charges - PaxusCustomer Service Contracts
'OtherTotal Computer Costs
Other ( Small items not clearly identified)
TOTAL EXPENDITURE
18615
5206
5597
132121
93498
76
250 71
97
113420
873
117
$845 $543

Average
Southland
Otago
Canterbury
West Coast
Nel-Marl
Wellington
Area Health Board
M-Wang
Hawkes Bay
Taranaki
Tairawhiti
BOP
Waikato
Auckland
Northland
-.--ij• '4 (T 'i) T ( 31 LT 41
Appendix 6
190-1992 $ Funding Per Enrolment
$0.00$50.00$100.00$150.00$200.00$250.00$300.00$ AHB Funding

, i_'.T •L•:-c:T
$0.00$2.00$4.00$6.00$8.00$10.00$12.00$14.0()Dollars
$16.00
Appendix 7
1990-1992 $ Funding Per Female Population (15-64)
Average
Southland
Otago
Canterbury
West Coast
Nei-Marl
Wellington
M-Wang
Hawkes Bay
Taranaki
Tairawhiti
BOP
Waikato
Auckland
Northland
Area HealthBoard

I(
[Ave-rage Number of Monthly Enrolments Per FTE
0100200300400500600700800Number of Enrolments
Appendix 8
Average
Southland
Otago
Canterbury
West Coast
Nel-Marl
Wellington
M-Wang
Hawkes Bay
Taranaki
Ta Ira whit i
BOP
Waikato
Auckland
Northland
Area HealthBoard

05001,0001,5002,0002,5003,000Number of Enrolments
35004,0004,500
Appendix 9
LAverage Number of Enrolments Per FTE
Average
Southland
Otago
Canterbury
West Coast
Nel-Marl
Wellington
M-Wang
Hawkes Bay
Taranaki
Tairawhiti
BOP
Waikato
Auckland
Northland
Area HealthBoard

04iPeat Marwick.
Appendix 10
Register Structure Options
A large number of potential options exist for the database register structure and wehave examined those which we consider to be the most suitable options.
Option 1: 14 Registers Located One at Each AHB
This option retains many features of the existing register structure, but establishes acommunications link between each AHB machine and a central database at the DOH.
Under this option, the individual registers would continue to operate at the AHBlevel, but previously defined summary data would be transmitted at, say, month endfrom each AHB register to the DOH database. Data arriving at the DOH databasecould be combined and analysed to provide summary information at a national level.
SummaryDatabase
electronictransmission ofsummary data
14AHBDatabases
The advantages of this option are:
security and confidentiality of the detailed woman data is retained at the localA}I]3 level. No detailed information is stored or available at a national level;

Jrb"Ir' Marwick
the existing computer hardware is retained and will continue to operate theregisters. The modems which are now used at each AHB site tocommunicate with Paxus could be utilised to transmit data to the DOHdatabase at month end.. The existing DOH machine could be used to collectand analyse summary data from the AHBs;
•summary data will be available at a national level, and DOH staff couldaccess their own summary database as often as required without needing torequest information from the AHB systems. Provided the summary datatransmitted from the AHB machines was suitably defined, it is possible thatsignificant flexibility for adhoc reporting would be available on the DOHmachine;
the register retains a local presence at each AHB for liaison with women,smear takers and laboratories. This allows follow-up on results and any datavalidation to be handled locally.
The disadvantages of this option are:
additional software would need to be developed for
- -preparation of summary data on the AHB databases;-transmission of summary data from AHB to DOH;-collation of received data on the DOH machine;
•communication costs would be incurred in the transmission of summary datato the DOH machine at month end.
Input Options
The input options are:
•input to the distributed Al-TB registers directly from the laboratories;
•input to the distributed AHB registers at the Al{Bs.

kA,i lpeat Marwick
- These options are discussed further under Data Input Options.
- Additional Costs
Additional costs from those currently incurred associated with this approach are:
providing communication links between each AHB and the central register.Further research is required to determine these costs;
costs to develop additional software are required, and cannot be determinedwithout further research.
Option 2: Four Registers on Four Separate Machines
This option calls for the combination of the 14 existing AHB registers in one registerfor each of the four RHA. Each RHA database could be linked to a nationalsummary database at the DOR
As in Option 1, summary data could be extracted off each RHA machine andtransmitted on a monthly basis to the central DOH summary database. Data storedon the summary database at the DOH could be interrogated as required on an adhocbasis to provide national reports without need to request the information at RHAlevel.

kA4Peat Marwick
4 RHADatabases
The advantages of this option are as follows:
•detailed data is retained at the RHA level, and not available at a national level.This retains a certain level of confidentiality as detailed woman data wouldnot leave the RHA area;
summary data would be available at a national level as in Option 1;
•fewer data entry staff should be required if input is performed at an RHAlevel, as input processing would be more streamlined;
•increased volumes being processed at one site should result in cost savingsthrough economies of scale.
The disadvantages of this option are as follows:
•additional computer equipment is required to run the registers at an RHAlevel;

kü&Ipeat Marwick
additional software would need to be written to:
-prepare summary data on RHA machines;-transmit summary data from RHAs to DOH;-collate and analyse data received at DOH;
communication costs will be incurred at month end in transmitting summarydata from the RHAs to the DOH;
there will be additional costs involved in communicating with laboratories,smear takers, and women who are within the RHA but outside the local areain terms of toll calls, faxes and travelling costs to educate and promote thescheme.
Input Options
The input options are:
•input to the four RHA registers from the laboratories;•input to the four RHA registers from the 14 AHB sites;•input to the four RHA registers from central data entry staff located at each
RHA.
These options are discussed further under Data Input Options.
Additional Costs
The additional costs associated with this option are as follows:
•Four machines of equivalent power to the Hewlett Packard 9000/817 wouldbe required at each RHA with approximately 500 mB of disk space and 24mB of memory.

Peat Marwick
The cost of each such machine is approximately: $81,000
•An Ingres software licence will be required for each site atapproximately: $30,000
(Note that these costs are after discount of 15% offered to the DOH byHewlett Packard.)
•Communication costs to transmit summary data monthly from the RHA tothe DOH. Further research is required to determine these costs.
•Additional software is required, the costs of which cannot be determinedwithout further research.
Benefits
•Maintenance of the four HP9000/817 machines will be $15,000 p.a. permachine, compared with $5,800 p.a. per existing AHB machine.
Total maintenance $60,000Less existing maintenance $87,000
(Note that existing hardware is still on warranty.)
•Staff savings by reducing the number of data entry personnel are possible.Further research is required to determine this benefit. Note that this potentialsaving is dependent on the input option which will be adopted, and which isoutlined under Data Input Options.
Option 3: Four RHA Registers on One Machine
This option calls for the combination of the 14 existing AHB registers which wouldrun on one central machine. The data could be effectively partitioned into fourdatabases.

k'A41i Peat Marwick
Detailed data would be available at a national and at an RHA level.
Single machine:RHA1 dataRHA2 dataRHA3 dataRHA4 data
DOH DetailedDatabase
-- The advantages of this approach are:
only one machine would exist which reduces the complexity of both supportand operations involved in 14 separate databases and machines. In additionequipment maintenance costs will be lower than for 14 machines;
detailed data and summary is available at a national level, and anyinformation required nationally could be extracted;
•data input from one central location becomes possible and fewer data entrystaff should be required, as the input process would be more streamlined;
increased volumes being processed at one site should result in cost savingsthrough economies of scale.
= The disadvantages are:
existing confidentiality of data which is restricted at the AHB level could belost. Detailed data would be held outside the AHB or RHA, and securitycontrols would need to be established to ensure confidentiality wasmaintained;
• higher costs and difficulties are involved with communicating with smeaitakers, laboratories and women. Local knowledge and liaisons currentlyestablished could be lost

kaA4-l Peat Marwick
- •AHB staff would have very reduced access to data relevant to their districtand would be reliant on reports back to them from the DOH;
•some software would be required to produce summary reports which wouldspan the four databases;
•
the register is exposed to machine failure more than if 4 or 14 separatemachines are used.
Input Options
As in Option 2, data could be input from:
•laboratories;•AHB staff;•centralised data entry staff.
These options are discussed further under Data Input Options.
Costs
Additional costs are involved with:
•Purchase of a centralised machine. The Hewlett Packard 9000/847 would be- suitable, configured with 2gB of disk and 48mB of memory.
Such a machine would cost approximately: $190,000
•An Ingres software licence upgrade would berequired at: $90,000
(These costs are after discount of 15% offered to the DOH by HewlettPackard.)

011'Peat Marwick
•Additional software would be required to enable the four databaseenviront\çients to be combined for reporting purposes. This cost cannot bedetermind without further research, but should be less than the softwarecosts assciated with either Options 1 or 2.
Benefits
•Maintenance of th'HP 9000/847 machine will be $33,800 p.a., comparedwith $5,800 p.a. perxisting AHB machine.
Total maintenance $33,800Less existing maintenance $87,000
(Note that existing hardware is still under warranty.)
• Centralised input should reduce data entry staff number from those currentlyemployed at the AHB level. This will depend on the input option preferredfrom among those outlined under Data Input Options.
Option 4: One National Register on One Machine
This option completely centralises the 14 A}IB registers into one national registerrunning on a single machine.
11 NationalDatabase
Tne advantages of this option are:
•all data is available at a national level;
•no software modifications are required to combine databases;

0A4 i Peat Marwick
•support and enhancement of a single database is cheaper than for distributeddatabases;
any further health sector restructuring would be unlikely to adversely affectthe NCSP operations.
potential staff savings of A}{B staff dedicated to running the distributeddatabases can be made as the input process would be more streamlined;
changes of reporting requirements at a national level are easily achieved;
increased volume being processed at one location should result in costsavings through economies of scale;
change of a woman's geographic location no longer requires transfer ofrecords between AHB databases as at present;
complete woman history (using NMPI or other national index) is possibledespite location or name changes.
The disadvantages are:
additional computer equipment is required
•extra security controls would be required to ensure that data confidentiality(currently restricted to an AHB level) is not lost;
•exposure of the register to machine failure is higher with a single machine;
•higher costs associated with communicating with smear takers, laboratories,and women than under the current AHB structure. Local knowledge andliaisons would be lost;
- •AHB staff would have reduced access to data relevant to their district.

küZlpeat Marwick.
Input Options
As in Options 2 and 3, data could be input from:
•laboratories;•A}IB staff;•centralised data entry staff.
These options are discussed further under Data Input Options.
Costs
Additional costs are involved with:
•Purchase of an additional machine for the centralised database.A Hewlett Packard 9000/847 could be used with 2.0 gB of diskand 4.8 mB of memory at a cost of approximately $190,000
An Ingres software licence upgrade would be required at$90,000
(These costs are after discount of 15% offered to DOH by Hewlett Packard.)
Benefits
Maintenance of the HP 9000/847 machine will be $33,800 p.a., comparedwith $5,800 p.a. per existing AHB machine.
Total machine $33,800Less existing maintenance $87,000
(Note that existing hardware is still under warranty.)
Centralised input should reduce data entry staff numbers from thosecurrently employed at the AFIB level. This will depend on the input optionpreferred from among those outlined under Data Input Options.

kaIlPeat Marwick
Appendix 11
Data Input Options
As outlined in Register Structure Options (Appendix 10), there are a number ofpossible sources from which data could be entered to the register. These options fallinto two broad categories:
(a) input by terminals remote from the register's location;(b) input by operators at the register site.
In general, input by terminals remote from the register's location will allow for moretimely entry of data than where the data is physically sent to another location forinput. It may also allow a local register presence to be justifiably maintained tofollow up with smear takers, laboratories, and women from a local base ofoperations.
Input under option (b) will, in general, avoid the incurring of datatransmission/telecommunications costs, and may be able to create efficiencies in staffnumbers by providing a more centralised data entry service.
Input From Laboratories
Data could be input to the register, whether held at an AHB level or at national level,directly from the laboratories. This would involve the setting up of PCs at eachlaboratory with a modem which could be used to transmit the new enrolments andsmear results directly to the register. Data would be uploaded to a holding areawithin the register, verified as to validity of data and used to automatically update theregister.
Laboratories could be responsible for input of enrolment and result data. Pre-enrolment data could continue to be entered at a register operations level.

2;,4 l Peat Marwick
Laboratories
We envisage data being uploaded to the register in batch mode. A daily or weeklybatch of smear results and new enrolments would be transmitted by the laboratoryand be held in a "temporary holding file" at the register awaiting data validationprocessing by register staff.
The advantages are:
Most laboratories are already generating smear result data for the AHBregisters using PC based software. The results are output to floppy disketteand sent to the register for uploading to the database. Virtually no changewould be required to the hardware or software to enable laboratory input viaelectronic transmission.
Double keying of data is eliminated.
There are occasions when a smear result is not entered on the registerbecause the enrolment form is misplaced by the laboratory or smear taker,and the laboratory are under the impression that the result relates to an opt-off woman. Allowing the laboratories to enter the enrolment details wouldhelp to avoid this situation, and more accurately match smears andenrolments.
As an option for future consideration, this method would allow laboratoriesto have logon access to the register database if desired, to access smearhistory, and potential histology data (refer Issues section).

kA4 J Peat Marwick
The disadvantages are:
Additional workload would fall to the laboratories, particularly indetermining NMPI numbers and entering enrolment details.
Modems would need to be purchased, and costs would be incurred intransmitting data to the register. Note that transmission costs will depend onthe location of the register relative to the laboratory.
The quality of the data entry would not be under the direct control of theregister personnel. Note however that at present most of the data is suppliedby the laboratories on diskette and is not under direct register control.
A link between the laboratory and the NMPI system would need to beestablished to search for a woman's NMPI number. We note that there isalso a search cost charged by Paxus to perform this activity.
Some form of recompense could be expected by the laboratories forperforming this additional service. (Note that the only real additional effortis the entering of enrolment data by the laboratory staff). This additional costwould be offset by the reduction in data entry staff at the register, and by theelimination of the double keying of data which occurs at present.
Some functions would still need to be performed by NCSP personnel. Databatches uploaded from the laboratories will still need to go through the dataverification and upload process under NCSP control.
Input From Area Health Board Staff
Whether the registers are centralised or not, input could continue, as at present, to beperformed by staff at the AHBs.

thA,4 1 Peat Marwick
(a) Centralised Register
We do not see many advantages in having data entry performed at an AHBlevel if the register is centralised at national or RI-IA level. Using remote dataentry personnel has all the cost disadvantages discussed for laboratory input,without any of the benefits. Data is still double keyed, once at the laboratoryand once at the ABB. Delays in the data being available on the register areincurred and no staff savings are made in data entry operators.
We suggest that input at the AHB should only be considered if the register isto remain at the ABB.
(b) AHB Registers As At Present
We see certain advantages in maintaining an NCSP presence at the Al-lBlevel. Should such a presence be maintained, input by data entry staff at theAHB may be optimal. If the register is retained at the AHB level, input canbe sensibly performed either by laboratory personnel (described in InputOption from Laboratories) or by AHB level personnel.
W
L9J1 AHBregister
localterminals
The advantages of using AHB personnel are:
non dedicated data entry staff are available to the NCSP for other activities,e.g. checking on invalid data, generating and forwarding reminders, liaisonwith smear takers and laboratories, and promotion of the programme;

kA41i Peat Marwick
data input and verification is largely under the direct control and supervisionof the register controllers. Input direct from the laboratories loses certain ofthis control.
The disadvantages of using AHB personnel for input are that:
data entry staff levels will not be reduced;
data is still double keyed, once at the laboratory and once at the register.
Input From Centralised Data Entry Staff
Under this option, primary result data would be generated by the laboratories andforwarded to the central register on floppy diskette as at present. Centralised dataentry personnel would receive the data, pass it through the data validation processand upload to the central register.
0CentralRegister
CentralTerminals
The advantages of this option are:
data input remains largely under the control of the NCSP, especially where awoman's NMPI number is not readily available but must be searched for onthe Paxus database;
no telecommunications lines need to be set up between the database andremote input locations;

Peat Marwick
inefficiencies and rationalisation in use of data entry staff is possible. Wewould expect less data entry staff to be necessary than if laboratories wereresponsible for input and therefore less training will be necessary, and staffcosts can be minimised.
The disadvantages are:
data will be couriered or mailed by diskette and may be more vulnerable todamage, less than if it were transmitted;
time will be wasted in the mailing of data.
Summary
In summary we believe that the valid data entry options are:
(a) Laboratory input to:•AHB register;•RHA register;
central register.
(b) AHB input to:AHB register.
(c) Centralised input to:central register.
We believe that the following factors are of critical importance in this decision:
•who is to be responsible for the NCSP, (RHAs or Public Health Agencies)and their requirements
•the need to eliminate inefficient double keying which occurs at present;•obvious savings in the elimination of AHB NCSP data entry staff.

Appendix 12Chart of AccountSuggested Format
Income:
Sale of AssetsOther
Expenses:
Staff Costs:Salaries
PolicyAdvisory CommitteesAHB/Overseas LiaisonEducation/PromotionRegister -
Programme Managers and CoordinatorsSystem ManagersOther
•Wages -Data entryClerical
•Other (include Help Desk Consultant)•Other Staff Costs (Training, ACC Levy, Superannuation)
Operating Costs:•Professional Services:
•Computer Development•Computer Support•Legal•Other
•Committees/Meetings and Travel Expenses:•Advisory•AHBs/Liaison•Other
Publicity/Promotions
Printing and Stationery
Computer Costs•Rental•Maintenance•Processing (such as NMPI)•Other
•Other Costs (Postage, Telephone and Tolls, Motor Vehicles and Mileage)(Detail if over $5,000-$10,000 budget)
•Depreciation
•DOH Overheads (detail if possible)

Appendix 12A
ro YTD '(TOAct Bud Var
Monthly Management ReportSuggested Format
Income
Sale of AssetsOther
Total Income
MTD MTD MIDAct Bud Var
Operating Costs
Staff Costs (Note 1)
Other Staff Costs
Total Staff Costs
Other Operating Costs
Professional Services
•Computer•Other
Committees/Meetings and Travel Expenses
•Advisory•AHB5/Ljaison•Other
Publicity/Promotions
Printing and Stationery
Computer Costs
•Rental•Maintenance•Processing•Other
Depreciation
Other Costs
Total Operating Costs
Net Expenditure
Note 1 . Detail as per Chart of Accounts if required.

Possible Report Information For DOH Collation Appendix 13
Each Area Health Board Total
Total number of enrolments on the register
New enrolments this month (with a smear taken)New pre-enrolments this month
Smear results processed on the register this monthTotal smears processed by registered laboratories this month (private and public)
Abnormal smear results processed this month
Enrolments from commuity clinics this monthSmears taken from commuity clinics this month
Priority groups:
Enrolments this monthSmear results processed this month
Ages Groups:
Enrolments this monthSmear results processed this month
Outstanding recall numbers this monthOutstanding recall over 2 monthsOutstanding recall over 3 months
<A

Appendix 13Possible Report Information For DOH Collation
Each Area Health Board Total
Staff Numbers:
Programme ManagerSystems Administrator
Data EntryClericalOther Co-ordinators
Total Staff Numbers
Female population by age groups
Priority groups female population by age groups
Funding $
Number of smears taken using register
Total number of smears taken in register area

25
20
15
Number
10
5
Calls
Months Live
I
Appendix 14
rDOH-NCSP Call Desk Statistics
WellBOP Waik Auck HBay Otago Tara South Taira WestC N-Marl Canty NorthArea Health Board
A

nforrnatic •'-Mistry Of Lc1h
We1irgLCfl