Embed Size (px)
Citation preview

Clinical Imaging xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Clinical Imaging
j ourna l homepage: ht tp : / /www.c l in i ca l imag ing.org
Pearls and pitfalls in first-trimester obstetric sonography
Fernanda S. Mazzariol⁎, Jeffrey Roberts, Sarah K Oh, Zina Ricci, Mordecai Koenigsberg, Marjorie W. SteinDepartment of Radiology, Montefiore Medical Center, Albert Einstein College of Medicine
a b s t r a c ta r t i c l e i n f o
⁎ Corresponding author. Department of Radiology, Mon210 Street, Bronx, NY 10467. Tel.: +1 718 9204396; fax:
E-mail address: [email protected] (F.S. Mazzariol).
http://dx.doi.org/10.1016/j.clinimag.2014.10.0090899-7071/© 2014 Elsevier Inc. All rights reserved.
Please cite this article as: Mazzariol FS, et al10.1016/j.clinimag.2014.10.009
Article history:Received 19 April 2014Received in revised form 13 October 2014Accepted 16 October 2014Available online xxxx
Keywords:UltrasoundEctopicPregnancyBleedingEmbryo
Ultrasound is the primary imaging modality used in the evaluation of first-trimester vaginal bleeding and pelvicpain. This article will summarize the ultrasound findings in normal first-trimester pregnancy, failed pregnancy,ectopic pregnancy, subchorionic hemorrhage, retained products of conception, and gestational trophoblastic dis-ease. Mastery of the spectrum of sonographic findings in the normal and abnormal first-trimester pregnancy al-lows the radiologist to make accurate diagnoses and helps to appropriately guide patient management.
tefioreMedical Center, 111 East+1 718 798 7983.
, Pearls and pitfalls in first-trimester obstetric
© 2014 Elsevier Inc. All rights reserved.
1. Introduction
Vaginal bleeding and pelvic pain are common presenting complaintsduring first-trimester pregnancies. It is estimated that up to 15% to 20%of all pregnancies are complicated by vaginal bleeding [1]. The work-upincludes serum B-HCG sampling as well as transabdominal andtransvaginal sonography (TVS) to determine the gestational sac (GS)location and its shape, size, and internal contents. If present, the yolksac(s), embryo(s), and heart rate(s) [HR(s)] are evaluated, and the pres-ence of perigestational hemorrhage should be noted. The patient’s lastmenstrual period (LMP) and serum B-HCG levels are correlated withthe ultrasoundfindings to formulate a diagnosis and guide patientman-agement. It is incumbent on the radiologist to be familiar with the nor-mal and abnormal ultrasound findings of first-trimester pregnancy toavoid misdiagnosis.
2. Normal and abnormal features of first-trimester intrauterinepregnancy
2.1. The Gestational Sac
TheGS implants in the uterine fundus at approximately day 23 of themenstrual cycle. The earliest imaging sign of an intrauterine pregnancy(IUP) seen on TVS is an eccentric, extraluminal, rounded GS locatedwithin the endometrium, termed the intradecidual sign [2,3] (Fig. 1).This sign can be observed as early as 4 ½weeks of menstrual age. Thedouble decidual sac sign, representing the hyperechogenic peripheral
decidua vera and the inner decidua capsularis with intervening an-echoic endometrial lumen, is seen on TVS at about 5 menstrualweeks [2] (Fig. 2).0
Teaching Points• While the intradecidual sac sign and double decidual sac signs arereassuring and useful signs prior to the appearance of the yolk sac(YS), they will not be seen in 50% of intrauterine pregnancies [3–5].
• A nonspecific intrauterine fluid collection, which is not clearly dem-onstrated within the decidua, has a greater than 99% chance ofbeing an early IUP than a pseudo-GS of ectopic pregnancy becausethe incidence of ectopics is low (approximately 2%) and pseudo-GSsare only seen in up to 10% of ectopics [6]. Thus, a stable patient witha small nonspecific intrauterine fluid collection presenting with vagi-nal bleeding and/or pelvic pain should be followedwith ultrasound in2 to 3 days to help differentiate an early IUP from a pseudo-GS of ec-topic pregnancy.
The GS is composed of anechoic amniotic fluid and chorionic extra-embryonic coelom, which may contain low-level echoes. By TVS, theYS is usually visualized within the extraembryonic coelom at approxi-mately 5½ weeks or 8-mmmean GS diameter (MSD), and the embryois usually seen at 6 weeks or 16 mmMSD. The embryonic heart motionis usually detected at an embryonic crown-rump length (CRL) of 5 mm[5]. More recently, the recommendation for the diagnosis of embryonicdemise has been redefined as absent heart motion at a CRL of 7 mm inorder to avoid false positives [7]. The amniotic cavity expands to obliter-ate the chorionic cavity by 14 to 16 weeks.
Adverse outcomes are frequently seen with very irregular or low-lying GSs, MSD N8 mmwithout a YS, or MSD N25 mm without an em-bryo [7]. An abnormally small GS size is a poor prognostic sign; anMSD b5 mm larger than the embryonic CRL is associated with a 94%
sonography, Clin Imaging (2014), http://dx.doi.org/

Fig. 1. Intradecidual sign. Transverse view of the uterus—eccentric GSwithin the endome-trium (arrow).
Fig. 3. Anembryonic pregnancy. Transverse view of the uterus showing a 2.5-cm empty GS.
2 F.S. Mazzariol et al. / Clinical Imaging xxx (2014) xxx–xxx
rate of first-trimester spontaneous abortion [8,9]. In a suspected case ofpregnancy failure, follow-up sonography in 2 to 3days is recommendedbecause lack of MSD or CRL growth during this interval is diagnostic. Ananembryonic intrauterine pregnancy, or blighted ovum, is likely presentif an embryo is absent at 16 to 24mmMSD and is definitively diagnosedwhen the embryo is absent at anMSD N25mm on TVS [10] (Fig. 3). TheGS may have an irregular, abnormal shape in a blighted ovum.
Comparison with prior sonograms is also helpful in evaluating forpregnancy failure. Suspicion of pregnancy failure increases when a liveembryo is not demonstrated on TVS 7–10 days after an exam demon-strating a YS or 7–13 days after an exam demonstrating an empty GS.Absence of a live embryo N11 days after seeing a YS or N14 days afterseeing an empty GS is diagnostic of pregnancy failure [10].
Teaching Points• If a GS is low lying, look for a fundal fibroid, whichmay be displacing anormal IUP inferiorly.
Fig. 2. Double decidual sign. Long view of the uterus–hyperechogenic peripheral deciduavera (arrowhead) and inner decidua capsularis (long arrow)with intervening hypoechoicendometrial lumen (short arrow).
Please cite this article as: Mazzariol FS, et al, Pearls and pitfalls in first-tri10.1016/j.clinimag.2014.10.009
Normally, if an amniotic cavity is detected on TVS, an embryo withlength similar to the MSD should be present. The empty amnion signrefers to visualization of an amniotic sac without a discernible embryoand is strongly associated with pregnancy failure [11] (Fig. 4). Theexpanded amnion sign refers to an embryo that lacks heart motionbut is surrounded by visible amnion and is indicative of embryonic de-mise even when the CRL is less than 5 mm [8,12] (Fig. 5).
2.2. The Yolk Sac
A normal YS measures less than 5.6 mm internal diameter between5 and 10 weeks and starts to regress by 11weeks. Abnormal prognosticfactors include absence of the YS in the presence of an embryo, and alarge, calcified, or persistently deformed YS [8] (Fig. 6). The YS is nolonger seen after the amniotic cavity expands to obliterate the chorioniccavity by 14 to 16 weeks [8,13].
Fig. 4. Empty amnion sign. Empty amniotic sac (arrowhead). Mildly deformed YS (shortwhite arrow). Note presence of echoes in the extraembryonic coelom (long whitearrow). Small subchorionic hemorrhage (black arrow).
mester obstetric sonography, Clin Imaging (2014), http://dx.doi.org/

Fig. 5. Expanded amnion sign. (a) Less than 5-mm embryo (short arrow) andmuch largeramniotic sac (long arrow). YS (arrowhead). (b) No embryonic heart motion.
Fig. 6. Abnormal pregnancy that resulted in embryonic demise. (a) Large YS (arrow).(b) Low embryonic HR.
3F.S. Mazzariol et al. / Clinical Imaging xxx (2014) xxx–xxx
Teaching Points• A hyperechogenic, nonshadowing YS can be a normal finding and mayconvert to a typical appearance on follow-up scan. It should not bemis-taken for a calcified YS, which is only seenwith embryonic demise [13].
2.3. Embryonic HR
The embryonic HR is generally≥120 beats perminute (bpm) in em-bryos larger than 5 mm. An HR b110 bpm is associated with a poorerprognosis. In embryos smaller than 5 mm, the HR can be as low as100 bpm. However, an HR b100 bpm is associated with an increasedrate of embryonic loss, proportional to the degree of bradycardia[14,15] (Fig. 6).
2.4. B-HCG discriminatory level
Obstetric sonograms should be interpreted jointly with serum B-HCG assay levels. The B-HCG discriminatory level, defined as the levelabove which an IUP is expected to be seen on TVS, is usually quoted as1500 to 2000 mIU/ml using the third international standard or
Please cite this article as: Mazzariol FS, et al, Pearls and pitfalls in first-tri10.1016/j.clinimag.2014.10.009
international reference preparation. However, B-HCG assay levels varywidely in early pregnancy, depending on the laboratory, and a normalIUPmay not be seen on TVS evenwhen the B-HCG is above the discrim-inatory level [16] (Table 1). Adherence to a set B-HCG discriminatoryvalue may be misleading. It is important to remember that, in a normalearly IUP, the B-HCG level doubles approximately every 48 h. In an ec-topic or failed pregnancy, the B-HCG level rises at a slower rate, pla-teaus, or drops [5].
Teaching Points• Overreliance on the B-HCG discriminatory level to “assume” ectop-ic pregnancy in the presence of an empty endometrium can resultin improper methotrexate administration to a woman with a nor-mal early pregnancy.
• A stable pregnant patientwith a B-HCG above the discriminatory leveland without IUP on TVS should be followed with short-term TVS andB-HCG to determine the status and site of the pregnancy.
mester obstetric sonography, Clin Imaging (2014), http://dx.doi.org/

Table 1β-HCG levels in weeks from LMPa
Weeks from LMP B-HCG assay level (mIU/ml)
3 5–504 5–4265 18–73406 1080–56,5007–8 7650–229,0009–12 25,700–288,000
a The American Pregnancy Association (http://americanpregnancy.org/duringpregnancy/hcglevels.html).
4 F.S. Mazzariol et al. / Clinical Imaging xxx (2014) xxx–xxx
2.5. The Chorionic Bump
The chorionic bump is a focal solid or complex protuberance fromthe choriodecidual region bulging into the GS (Figs. 7 and 8). Harriset al. identified this sign in 0.7% of 2178 early obstetrical sonogramsand noted that 50% of these pregnancies aborted, a pregnancy failurerate four times that of the general population control group [17].Based on the sonographic evolution of the “chorionic bump” onfollow-up studies and pathologic investigation of abortuses, the chori-onic bump likely represents a small subchorionic bleed [18,19].
2.6. Subchorionic Hemorrhage
Intrauterine hematomas, a common ultrasound finding associatedwith first-trimester bleeding, have a reported incidence between 4%and 22% [19]. Subchorionic hemorrhage is themost common type of in-trauterine chorionic bleed and is thought to result from partial detach-ment of the trophoblast from the uterine wall with blood dissectingbetween the chorion and the decidual layer of endometrium [20].When the hematoma dissects into the endometrial cavity, the patientcan present with vaginal bleeding.
Subchorionic bleeds are graded into small, medium, and large ac-cording to their sizes relative to GS circumference. One large retrospec-tive review reported a rate of pregnancy loss of 7.7% for smallhematomas (less than one third the circumference of the GS), 9.2% formedium hematomas (encompassing one third to one half the circum-ference of the GS), and 18.8% for large hematomas (encompassing at
Fig. 7. The chorionic bump. A solid protuberance from the choriodecidual reaction bulginginto the GS (arrow).
Fig. 8. The chorionic bump. (a) Complex cystic/solid appearance of the chorionic bump(white arrow) and the YS (arrowhead). (b) Another view of the same gestation showingthe chorionic bump (arrow), the embryo (between calipers), and the YS (arrowhead).
Please cite this article as: Mazzariol FS, et al, Pearls and pitfalls in first-tri10.1016/j.clinimag.2014.10.009
least two thirds the circumference of the GS) [1]. Subchorionic hemor-rhage has a worse prognosis when associated with advanced maternalage or early gestational age [19,1]. A subchorionic hemorrhage mayprogress into an abruption when the bleed extends behind the placenta.
Subchorionic hemorrhage can be crescentic, ovoid, linear, or curvi-linear, and its echogenicity is dependent on the stage of the hemor-rhage. It is echo poor in the hyperacute setting, transitioning tohyperechogenic as the hematoma organizes and subsequently decreas-ing in echogenicity as the hematomaundergoes hemolysis and liquefac-tion [21] (Fig. 9). Due to its variable appearance, a first-trimestersubchorionic hematoma can be confusedwith normalfirst-trimester in-complete chorioamniotic fusion, an intrauterinemass, a vanishing twin,or slow flow within perigestational veins. The latter condition may berecognized by detection of slow-moving particles on gray scale orcolor Doppler imaging.
Teaching Points• The majority of subchorionic hematomas are small, regress spontane-ously, and do not result in pregnancy loss.
• Larger or persistent hemorrhages tend to have worse prognoses.
mester obstetric sonography, Clin Imaging (2014), http://dx.doi.org/

Fig. 9. Subchorionic hemorrhage. (a) Small, hypoechoic subchorionic bleed (less than onethird of circumference of GS; arrow). (b) Large subchorionic bleed with heterogeneousechogenicity (between calipers) surrounding the GS (arrow).
Fig. 10. Vanishing twin. Live gestation (long arrow) with a vanishing twin (short arrow).
5F.S. Mazzariol et al. / Clinical Imaging xxx (2014) xxx–xxx
2.7. Pregnancy Number
The vanishing twin syndrome is due to involution of one embryo of atwin or othermultiple gestations. It is a common eventwhen amultiplegestation is diagnosed early in pregnancy. The prognosis for the surviv-ing fetus is generally excellent in the first trimester, andmanagement isconservative. A hypoechoic subchorionic hemorrhage can mimic amni-otic fluid and be mistaken for a “vanishing twin” [21] (Fig. 10).
Teaching Points• Reporting the number of embryos in a multiple gestation before 6weeks may lead to over- or underestimation.
Table 2Clinical terminology for the spectrum of findings related to abortion
Spontaneous abortion Pregnancy loss without medical intervention
Threatened abortion Up to 20 weeks pregnant with vaginal bleedingand a closed cervix
Inevitable abortion Progressive cervical dilatation with products ofconception not yet expelled
Abortion in progress Open cervix with products of conception in theprocess of being expelled
Incomplete abortion Some products of conception expelled, but someremain in the uterus
Complete abortion Products of conception completely expelled in thepresence of a closed cervix
Missed abortion Embryonic demise in uterus with a closed cervix
3. Abortion
The clinical terminology for the spectrum of findings related to abor-tion is summarized on Table 2 [22].
4. Ectopic Pregnancy
Ectopic pregnancies, which account for 1.4% to 2% of all pregnanciesand 4.5% of all in vitro pregnancies, are responsible for 15% of maternaldeaths [8]. Risk factors include prior pelvic inflammatory disease, priorectopic pregnancy, endometriosis, tubal surgery, infertility, in vitro
Please cite this article as: Mazzariol FS, et al, Pearls and pitfalls in first-tri10.1016/j.clinimag.2014.10.009
fertilization, ovulation induction, presence of an intrauterine device,prior diethylstilbestrol exposure, and salpingitis isthmica nodosum [5].
Ninety-five percent of all ectopic pregnancies occur in the fallopiantubes, and 75% to 80% of these are located in the ampullary portion[5]. Less common sites of ectopic pregnancies include interstitial portionof the fallopian tube, cesarean (C)-section scar, and cervix. Ovarian andabdominal ectopic pregnancies are very rare [5].
Teaching Points• The sonographic examination should start with transabdominal tech-nique because, occasionally, a tubal ectopic pregnancymay be locatedhigh in the pelvis, outside the field of view of the transvaginal scan.
A sonogram showing an empty uterus and an extrauterine GS withembryonic heart motion is definitive for a tubal ectopic pregnancy,but these findings are observed only in 17% to 28% of ectopic pregnan-cies [5,8] (Fig. 11).
A very common sonographic sign of a tubal ectopic pregnancy isthe tubal ring, an extraovarian cystic structure with a thickened,hyperechogenic wall of trophoblast [23–25] (Fig. 12). The tubal ringmay be empty or contain an embryo or YS. It typically exhibits a “ringof fire” on color Doppler imaging, with high-velocity, low-resistanceflow on spectral tracing. Useful hints to differentiate an ectopic preg-nancy from a corpus luteum (CL) are eccentric position of the CLwithinthe ovarian tissue and hyperechogenicity of the trophoblast in the tubalring compared with the echogenicity of the CL [23,24]. However, thesedistinguishing features are not always obvious, and the CLmay demon-strate greater peripheral echogenicity and/or a more pronounced “ringof fire” than the ectopic pregnancy [25].
mester obstetric sonography, Clin Imaging (2014), http://dx.doi.org/

Fig. 11. Live tubal ectopic pregnancy. (a) Tubal ring containing an embryo (between cali-pers) of CRL 0.77, corresponding to gestation of 6 weeks and 5 days. (b) Color Dopplershowing heart motion.
Fig. 12. Tubal ring. (a) Extraovarian cystic structure with a thickened wall due to the tro-phoblastic change (white arrow). Ovary containing a large CL (black arrow). (b) Ring offire on color Doppler.
6 F.S. Mazzariol et al. / Clinical Imaging xxx (2014) xxx–xxx
Teaching Points• Ovarian ectopic pregnancies are exceedingly rare, and a cystic struc-ture within the ovary is almost always a CL. There are cases in whichit is difficult to determine whether the tubal ring-like structure is aCL extending off the ovary or an adjacent ectopic.
• Gentle probingwith the endovaginal transducer allows the radiologistto identify the point of tenderness andmay help localize the site of pa-thology. A complex adnexal mass that is demonstrated to separatefrom or slide over the ovary when transducer pressure is directed atthe interface between the mass and the ovary is a strong indicationof an ectopic pregnancy. However, this maneuver may not differenti-ate an ectopic from a CL in up to 10% of ectopics [26].
Any complex adnexal mass distinct from the ovary in a pregnantwoman without an IUP on TVS is highly suspicious for an ectopic preg-nancy. A complex tubular mass may represent a hematosalpinx or he-matoma in the setting of a tubal ectopic pregnancy (Fig. 13). A distinctcomplex cystic mass with a vascular rim may be seen within thehematosalpinx, representing the GS. Inmany ectopic pregnancies, how-ever, it is not possible to detect the small ectopic sac.Moreover, we havenoted that ectopic pregnancies that have been treated with methotrex-ate may appear as a solid mass on follow-up exam.
A small amount of fluid in the cul-de-sac is usually physiologic. Fluidin Morison’s pouch is abnormal and requires careful evaluation for ec-topic pregnancy. The pelvis and Morison’s pouch must be meticulously
Please cite this article as: Mazzariol FS, et al, Pearls and pitfalls in first-tri10.1016/j.clinimag.2014.10.009
evaluated for fluid containing low-level echoes with or withouthyperechogenic clot, representing hemoperitoneum. Hemoperitoneumdoes not necessarily imply rupture of an ectopic pregnancy, as bloodmay exit from the fimbriated end of an intact tube or may result froma ruptured ovarian cyst [8]. Conversely, an intact tubal ring does not ex-clude the presence of rupture [27].
Teaching Points• A normal pelvic sonogram, without evidence of an intrauterine preg-nancy, does not exclude the possibility of an ectopic pregnancy.
Uterine findings in the setting of an ectopic pregnancy include anempty uterus, a nonspecific decidual cyst, or a pseudo-GS (e.g., decidualcast) containing fluid, blood, or mobile debris (Fig. 14). The pseudosac,when present, is centrally located in the endometrial complexand surrounded by a single, often irregular decidual layer [5]. Itmay demonstrate acutely angulated margins along the axis of theuterine lumen.
The sonographic features of an interstitial ectopic pregnancy are asfollows: eccentric high location in the uterine fundus, bulge of the uter-ine contour,≤5mmofmyometrial thickness between the decidual reac-tion and the uterine serosa, and the interstitial line sign [5,28]. Theinterstitial line sign is described as a thin, straight hyperechogenic lineextending from the endometrial cavity to the medial aspect of the GS(Fig. 15). An interstitial ectopic pregnancy can grow larger before the
mester obstetric sonography, Clin Imaging (2014), http://dx.doi.org/

Fig. 13. Hematosalpinx. (a) Cross-sectional view of the ovary with a CL (shortarrow) and adjacent hematosalpinx (long arrow). Complex fluid representshemoperitoneum (black arrow). (b) Long view of the hematosalpinx (arrow)surrounded by hemoperitoneum (arrowheads).
Fig. 14. Pseudo-GS. (a) Tubal ectopic pregnancy with YS (long arrow) and adjacent ovarywith CL (short arrow). (b) The pseudo-GS is a fluid-filled structure in the center of the en-dometrial cavity (arrow).
Fig. 15. Interstitial line sign of cornual ectopic pregnancy. On transverse viewof the uterus,a thin, straight hyperechogenic line (arrow) extending from the endometrial cavity to themedial aspect of the GS.
7F.S. Mazzariol et al. / Clinical Imaging xxx (2014) xxx–xxx
patient becomes symptomatic as it is partially surrounded bymyometrium. Interstitial ectopic pregnancy rupture is associated withgreatermorbidity andmortality due tomassive hemorrhage from the di-lated arcuate uterine vessels [5,28].
It is important to differentiate an interstitial pregnancy fromamildlyeccentric IUP, an IUP in a septate or bicornuate uterus, or an eccentricIUP position due to a fibroid displacing the GS. In the septate uterus, acurved endometrium is seen extending to the sac [28]. An eccentricIUP will not bulge the uterine contour, will lie within the endometrialcomplex with ≥5 mm myometrial mantle, and will not demonstratean interstitial line sign. A 3-dimensional ultrasound may be valuablein establishing the diagnosis of interstitial pregnancy.
A C-section scar ectopic pregnancy is located in the anterior loweruterine segment. There is absence or paucity of myometrium betweenthe decidual reaction and the anterior uterine serosa or the bladderwall [29] (Fig. 16). Frequently, the uterine lumen can be shown to puck-er anteriorly in the region of this ectopic.
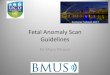
Distinction should be made between a cervical ectopic and an abor-tion in progress. With an abortion in progress, the sac is located central-ly in the canal and usually appears flattened, with an absent ornonvascular hyperechogenic rim. In the vast majority of cases, if an em-bryo is detected, the heartmotion is absent (Fig. 17). In contrast, embry-onic cardiac activity inferior to the internal os is highly suggestive of acervical ectopic. A cervical ectopic has a surrounding hyperechogenicdecidual reaction that is lacking in an abortion in progress (Fig. 18). Ifdifferentiation between a cervical ectopic and the much more frequent
Please cite this article as: Mazzariol FS, et al, Pearls and pitfalls in first-tri10.1016/j.clinimag.2014.10.009
abortion in progress is not possible on the initial exam, follow-up ultra-sound, sometimes within hours, may show dramatic change in appear-ance of abortion in progress [5,29]. A cervical ectopic pregnancy is
mester obstetric sonography, Clin Imaging (2014), http://dx.doi.org/

Fig. 17. Abortion in progress. Flattened GS (long arrow) without surrounding decidu-al reaction located centrally in the upper cervix. An embryo (short arrow) and YS (ar-rowhead) present.
8 F.S. Mazzariol et al. / Clinical Imaging xxx (2014) xxx–xxx
situatedmore eccentrically in the cervix, and the anteriormyometrium isof normal thickness [29], a distinguishing feature from C-section scar ec-topic. A cervical Nabothian cyst is nonvascular, lacks a hyperechogenicrim, and should not be confused with ectopic pregnancy.
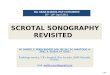
The incidence of heterotopic pregnancies is very low. However,women undergoing ovulation induction or in vitro fertilization are at in-creased risk, with an incidence of 1%–3% [30] (Fig. 19). Therefore, partic-ularly in these populations, the adnexa must be carefully examined forthe presence of a concomitant ectopic pregnancy.
Abdominal pregnancy is exceedingly rare and usually located in theovarian ligaments. A potential pitfall is tomistake the empty uterus for a“myoma” in the lower uterine segment, inferior to an abdominal preg-nancy. In order to obviate this pitfall, careful evaluation of the sagittalmidline view of the uterusmust be performed to ensure that the vaginalstripe is continuous with the cervical lumen and that it leads to the GSwithin the uterus.
5. Retained Products of Conception
In first-trimester pregnancy failure, abnormal prolonged vaginalbleeding and absent or abnormal decline of B-HCG levels raise suspicionof retained products of conception (RPOCs). RPOC is a risk factor for en-dometritis, and its treatment almost always includes curettage [31].
Distinction of RPOC from intrauterine clot can be difficult as both canpresent as an endometrialmass of variable echogenicity, complex endo-metrial fluid, and endometrial thickening greater than 10 mm [31]. Adynamic real-time clip of the endometrium will aid in differentiatingthickened decidua and mobile blood and debris within the lumen.
A study by Durfee et al. [31] found that an endometrial mass was themost sensitive (79%) and specific (89%) finding for RPOC, while anotherstudy by Kamaya et al. [32] found only a moderate positive predictivevalue (80%) for the diagnosis of RPOC. Atri et al. observed that increasedcolor Doppler flow, with or without amass, is the best sonographic pre-dictor of RPOC, but the sensitivity of this finding is reduced [33].
Kamaya et al. [30] graded the vascularity of the endometrium rela-tive to the myometrium on color Doppler in patients with positiveRPOC. Four categories are described: type 0—no flow; type 1—minimalflow, less than that of the myometrium; type 2—moderate flow, equalto that of the myometrium; and type 3—marked flow, greater thanthat of the myometrium. Type 0 vascularity can be seen with intrauter-ine clot and RPOC. Type 1 vascularity is seenmore frequently with RPOCthan clot. Types 2 and 3 vascularities are only seen with RPOC (Fig. 20).
Teaching Points• Type 3 vascularity pattern can be confused with a uterine AVMwhichalso demonstrates high-velocity flow. Identification of a type 3
Fig. 16. C-section scar ectopic pregnancy. Longitudinal view of the uterus. GS in the loweruterine segment, at the site of a C-section scar, with paucity of myometrium between thedecidual reaction and the anterior serosa of the uterus (arrow).
Please cite this article as: Mazzariol FS, et al, Pearls and pitfalls in first-tri10.1016/j.clinimag.2014.10.009
vascularity pattern can potentially alter management, including con-siderations for longer course of uterotonics, more cautious dilatationand curettage, and possible embolization [34].
Fig. 18. Live cervical ectopic pregnancy. (a) GS in the cervix with fetus (between calipers).External cervical os (short arrow) and placenta (long arrow). (b) Normal fetal heart motion.
mester obstetric sonography, Clin Imaging (2014), http://dx.doi.org/

Fig. 19. Heterotopic pregnancy. (a) Longitudinal view of the uterus showing a normallysituated pregnancy (long arrow) and a GS in the cervix (short arrow). (b) Eccentrically lo-cated GS in the cervix with decidual reaction (arrow) and an embryo (between calipers).
Fig. 20. Retained products of conception (type 3 vascularity). (a) Longitudinal view of theuterus. Endometrial thickening and low echogenicity material in the fundus (long arrow)and hyperechoic clot in the body (short arrow). (b) Increased vascular flow on RPOC rel-ative to myometrium on color Doppler (arrow) and low-resistance arterial flow on spec-tral Doppler.
9F.S. Mazzariol et al. / Clinical Imaging xxx (2014) xxx–xxx
6. Gestational Trophoblastic Disease
Gestational trophoblastic disease (GTD) is an uncommon cause offirst-trimester bleeding. Conversely, vaginal bleeding during early preg-nancy is the most common clinical presentation of patients with GTD[35]. The classic clinical signs such as hyperemesis, hypertension, andexcessive uterine growthmay not be present until the second trimester.In addition, these patientsmay demonstrate normal-range B-HCG assaylevels during the first trimester [35].
TVS is often performed before GTD is clinically suspected, and thefirst-trimester sonographic findings are frequently nonspecific. At9–12 weeks of menstrual age, a complete hydatiformmole may appearas a complex heterogeneous intrauterine mass with multiple tiny vesi-cles, termed the "snowstorm" appearance (Fig. 21), with increased vas-cularity and arteriovenous shunting. An embryo may be seen in acomplete mole with a twin pregnancy or in a partial mole. In cases ofpartial hydatiform mole, an enlarged placenta with scattered “cysts”may produce a "Swiss cheese" appearance. The fetus in a partial molehas triploid aneuploidy, with symmetric intrauterine growth retarda-tion and fetal malformations [36].
The finding of a small multicystic mass in the endometrial regionmaybe mistakenly interpreted as a hydropically degenerating anembryonicgestation or mixture of blood/clot with RPOCs [35]. An abnormally highB-HCG level aids the diagnosis of a mole. With high B-HCG levels, en-larged ovaries demonstrating theca lutein cysts are seen in up to half ofthese patients [37].
Please cite this article as: Mazzariol FS, et al, Pearls and pitfalls in first-tri10.1016/j.clinimag.2014.10.009
7. Conclusion
Sonographic evaluation of patients presenting with first-trimestervaginal bleeding and pelvic pain should begin with a thorough under-standing of the normal appearance and evolution of the early gestation.The radiologist must also recognize conditions that may result in preg-nancy failure and increased maternal morbidity and mortality. Whenimaging is not definitive, the radiologist must correlate the ultrasoundfindings with the clinical history and B-HCG levels to render an accuratediagnosis and guide patient management.
References
[1] Bennett G, Bromley B, Lieberman E, Benacerraf. Subchorionic hemorrhage in first-trimester pregnancies: prediction of pregnancy outcome with sonography. Radiolo-gy 1996;200:803–6.
[2] Yeh HC, Goodman JD, Carr L, Rabinowitz JG. Intradecidual sign: a US criterion ofearly intrauterine pregnancy. Radiology 1986;161:463–7.
[3] Chiang G, Levine D, Swire M, McNamara A, Mehta T. The intradecidual sign: is it re-liable for diagnosis of early intrauterine pregnancy? AJR Am J Roentgenol 2004;183:725–31.
[4] Laing FC, Brown DL, Price JF, Teeger S, Wong ML. Intradecidual sign: is it effective indiagnosis of an early intrauterine pregnancy? Radiology 1997;204:655–60.
[5] Levine D. Ectopic pregnancy. Radiology 2007;245:385–96.
mester obstetric sonography, Clin Imaging (2014), http://dx.doi.org/

Fig. 21. Complete hydatiformmole. (a) Longitudinal view of retroverted uterus. Small en-dometrial mass containing tiny vesicles (between calipers). (b) Increased vascular flow.
10 F.S. Mazzariol et al. / Clinical Imaging xxx (2014) xxx–xxx
[6] Doubilet P, Benson C. First, do no harm… to early pregnancies. J Ultrasound Med2010;29:685–9.
[7] Abdallah Y, Daemen A, Kirk E, Pexsters A, Naji O, Stalder C, Gould D, Ahmed S, Guha S,Syed S, Bottomley C, TimmermanD, Bourne T. Limitations of current definitions of mis-carriage using mean gestational sac diameter and crown-rump length measurements:a multicenter observational study. Ultrasound Obstet Gynecol 2011;38:497–502.
[8] Lyons EA, Levi CS. The first trimester. In: Rumack CM,Wilson SR, Charboneau JW, JohnsonJM, editors. Diagnostic ultrasound. 3rd ed. St. Louis: Elsevier Mosby; 2005. p. 1069–125.
[9] Bromley B, Harlow B, Laboda L, Benacerraf. Small sac size in the first trimester: a pre-dictor of poor fetal outcome. Radiology 1991;178:375–7.
Please cite this article as: Mazzariol FS, et al, Pearls and pitfalls in first-tri10.1016/j.clinimag.2014.10.009
[10] Doubilet P, Benson C, Bourne T, Blaivas M. Diagnostic criteria for nonviable pregnan-cy early in the first trimester. N Engl J Med 2013;369:1443–51.
[11] McKenna KM, Feldstein VA, Goldstein RB, Filly RA. The "empty amnion": a sign ofearly pregnancy failure. J Ultrasound Med 1995;14:117–21.
[12] Yegul NT, Filly RA. The expanded amnion sign: evidence of early embryonicdeath. J Ultrasound Med 2009;28:1331–5.
[13] Tan S, Pektas, Arslan H. Sonographic evaluation of the yolk sac. J Ultrasound Med2012;31:87–95.
[14] Arleo E, Troiano R. Outcome of early first-trimester pregnancies (b6.1 weeks) withslow embryonic heart rate. AJR 2011;197:252–5.
[15] Doubilet P, Benson C. Outcome of first-trimester pregnancies with slow embryonicheart rate at 6–7 weeks gestation and normal heart rate by 8 weeks at US. Radiology2005;236:643–6.
[16] Doubilet P, Benson C. Further evidence against the reliability of the human chorionicgonadotropin discriminatory level. J Ultrasound Med 2011;30:1637–42.
[17] Harris RD, Couto C, Karpovsky C, Porter MM, Ouhilal S. The chorionic bump: a first-trimester pregnancy sonographic finding associated with a guarded prognosis. J Ul-trasound Med 2006;25:757–63.
[18] Tan S, Ipek A, Sivaslioglu AA, Sungu N, Sarici OU, Karaoglanoglu M. The chorionicbump: radiologic and pathologic correlation. J Clin Ultrasound 2011;39:35–7.
[19] Leite J, Ross P, Rossi AC, Jeanty P. Prognosis of very large first-trimester hema-tomas. J Ultrasound Med 2006;25:1441–5.
[20] Maso G, D’Ottavio G, De Seta F, Sartore A, Piccoli M, Mandruzzato G. First-trimesterintrauterine hematoma and outcome of pregnancy. Obstet Gynecol 2005;105:339–44.
[21] Abu-Yosef MM, Bleicher JJ, Williamson RA, Wiener CP. Subchorionic hemorrhage:sonographic diagnosis and clinical significance. AJR 1987;149:737–40.
[22] Griebel C, Halvorsen J, Golemon T, Day A. Management of spontaneous abortion. AmFam Physician 2005;72:1243–50.
[23] Frates MC, Visweswaran A, Laing FC. Comparison of tubal ring and corpus luteumechogenicites: a useful differentiating characteristic. J Ultrasound Med 2001;20:27–31.
[24] Stein M, Ricci Z, Novak L, Roberts J, Koenigsberg M. Sonographic comparison of thetubal ring of ectopic pregnancy with the corpus luteum. J Ultrasound Med 2004;23:57–62.
[25] Atri M. Ectopic pregnancy versus corpus luteum cyst revisited: best Doppler predic-tors. J Ultrasound Med 2003;22:1181–4.
[26] Blaivas M, LyonM. Reliability of adnexal mass mobility in distinguishing possible ec-topic pregnancy from corpus luteum cysts. J Ultrasound Med 2005;24:599–603.
[27] Frates MC, Brown DL, Doubilet PM, Hornstein MD. Tubal rupture in patients with ec-topic pregnancy: diagnosis with transvaginal US. Radiology 1994;191:769–72.
[28] Frates MC, Laing FC. Sonographic evaluation of ectopic pregnancy: an update. AJR1995;165:251–9.
[29] Osborn D, Williams T, Craig B. Cesarean scar pregnancy—sonographic and magneticresonance imaging findings, complications, and treatment. J Ultrasound Med 2012;31:1449–56.
[30] Kirsch JD, Scoutt LM. Imaging of ectopic pregnancy. Appl Radiol 2010;39:10–25.[31] Durfee SM, Frates MC, Luong A, Benson CB. The sonographic and color Doppler fea-
tures of retained products of conception. J Ultrasound Med 2005;24:1181–6.[32] Kamaya A, Petrovitch I, Chen B, Frederick CE, Jeffrey RB. Retained products of con-
ception: spectrum of color Doppler findings. J Ultrasound Med 2009;28:1031–41.[33] Atri M, Rao A, Boylan C, Rasty G, Gerber D. Best predictors of grayscale ultrasound
combined with color Doppler in the diagnosis of retained products of conception.J Clin Ultrasound 2011;39:122–7.
[34] Jain K, Fogata M. Retained products of conception mimicking a large endometrialAVM: complete resolution following spontaneous abortion. J Clin Ultrasound2007;35:42–7.
[35] Lazarus E, Hulka C, Siewert B, Levine D. Sonographic appearance of early completemolar pregnancy. J Ultrasound Med 1999;18:589–94.
[36] Fraser-Hill M, Wilson S. Gestational trophoblastic neoplasia. In: Rumack CM, WilsonSR, Charboneau JW, Johnson JM, editors. Diagnostic ultrasound. 3rd ed. St. Louis:Elsevier Mosby; 2005. p. 589–92.
[37] Callen PW. Ultrasonography in obstetric and gynecology. 4th ed. Philadelphia:Saunders; 2000 848.
mester obstetric sonography, Clin Imaging (2014), http://dx.doi.org/