Embed Size (px)
Citation preview
15th European AIDS Conference; October 21-24, 2015; Barcelona, Spain
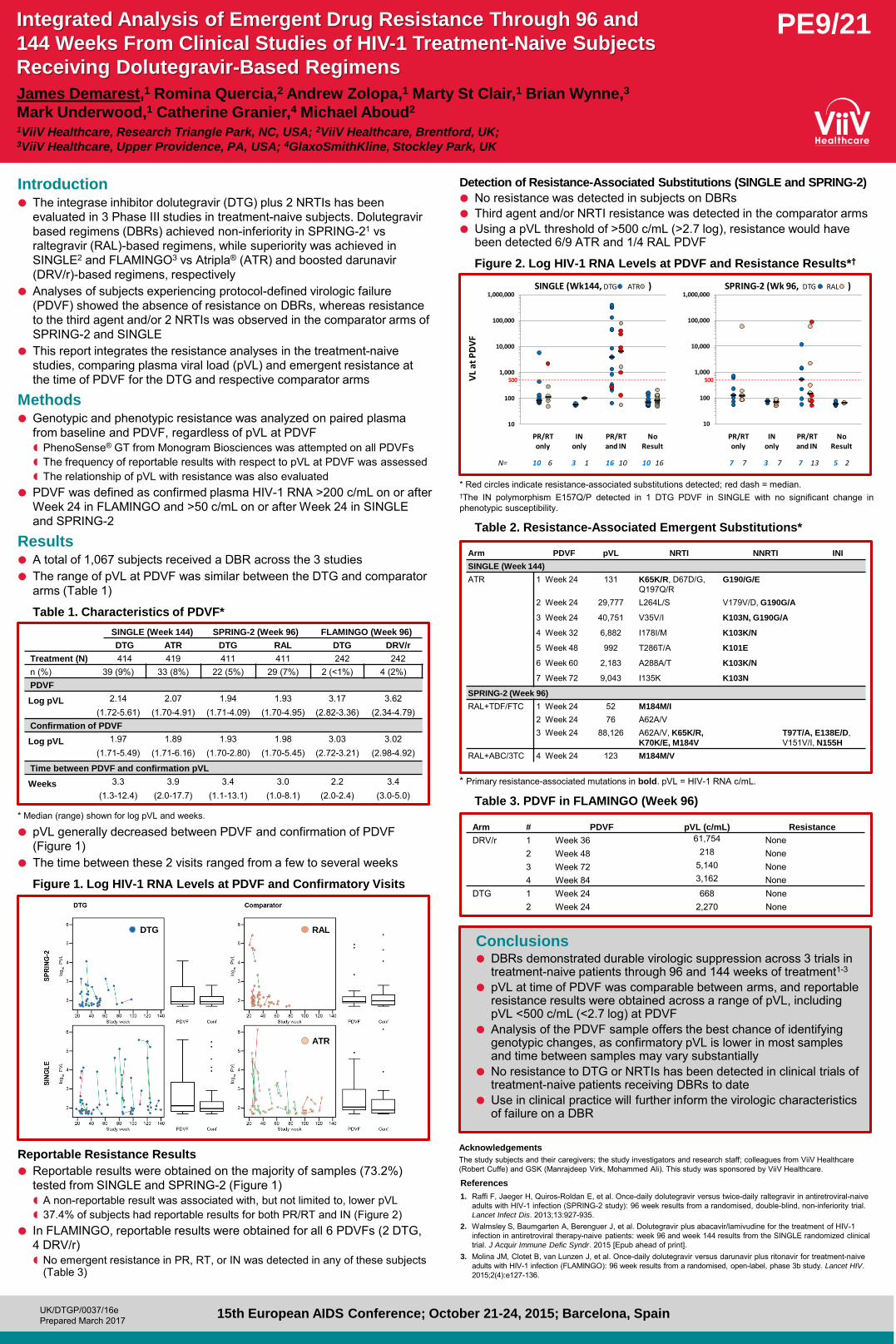
Detection of Resistance-Associated Substitutions (SINGLE and SPRING-2)
No resistance was detected in subjects on DBRs Third agent and/or NRTI resistance was detected in the comparator arms Using a pVL threshold of >500 c/mL (>2.7 log), resistance would have
been detected 6/9 ATR and 1/4 RAL PDVF
Figure 2. Log HIV-1 RNA Levels at PDVF and Resistance Results*†
* Red circles indicate resistance-associated substitutions detected; red dash = median. †The IN polymorphism E157Q/P detected in 1 DTG PDVF in SINGLE with no significant change in phenotypic susceptibility.
Table 2. Resistance-Associated Emergent Substitutions*
* Primary resistance-associated mutations in bold. pVL = HIV-1 RNA c/mL.
Table 3. PDVF in FLAMINGO (Week 96)
Introduction The integrase inhibitor dolutegravir (DTG) plus 2 NRTIs has been
evaluated in 3 Phase III studies in treatment-naive subjects. Dolutegravir based regimens (DBRs) achieved non-inferiority in SPRING-21 vs raltegravir (RAL)-based regimens, while superiority was achieved in SINGLE2 and FLAMINGO3 vs Atripla® (ATR) and boosted darunavir (DRV/r)-based regimens, respectively
Analyses of subjects experiencing protocol-defined virologic failure (PDVF) showed the absence of resistance on DBRs, whereas resistance to the third agent and/or 2 NRTIs was observed in the comparator arms of SPRING-2 and SINGLE
This report integrates the resistance analyses in the treatment-naive studies, comparing plasma viral load (pVL) and emergent resistance at the time of PDVF for the DTG and respective comparator arms
Methods Genotypic and phenotypic resistance was analyzed on paired plasma
from baseline and PDVF, regardless of pVL at PDVF PhenoSense® GT from Monogram Biosciences was attempted on all PDVFs The frequency of reportable results with respect to pVL at PDVF was assessed The relationship of pVL with resistance was also evaluated
PDVF was defined as confirmed plasma HIV-1 RNA >200 c/mL on or after Week 24 in FLAMINGO and >50 c/mL on or after Week 24 in SINGLE and SPRING-2
Results A total of 1,067 subjects received a DBR across the 3 studies The range of pVL at PDVF was similar between the DTG and comparator
arms (Table 1)
Table 1. Characteristics of PDVF*
* Median (range) shown for log pVL and weeks.
pVL generally decreased between PDVF and confirmation of PDVF (Figure 1)
The time between these 2 visits ranged from a few to several weeks
Figure 1. Log HIV-1 RNA Levels at PDVF and Confirmatory Visits
Reportable Resistance Results
Reportable results were obtained on the majority of samples (73.2%) tested from SINGLE and SPRING-2 (Figure 1) A non-reportable result was associated with, but not limited to, lower pVL 37.4% of subjects had reportable results for both PR/RT and IN (Figure 2)
In FLAMINGO, reportable results were obtained for all 6 PDVFs (2 DTG, 4 DRV/r) No emergent resistance in PR, RT, or IN was detected in any of these subjects
(Table 3)
Conclusions DBRs demonstrated durable virologic suppression across 3 trials in
treatment-naive patients through 96 and 144 weeks of treatment1-3 pVL at time of PDVF was comparable between arms, and reportable
resistance results were obtained across a range of pVL, including pVL <500 c/mL (<2.7 log) at PDVF
Analysis of the PDVF sample offers the best chance of identifying genotypic changes, as confirmatory pVL is lower in most samples and time between samples may vary substantially
No resistance to DTG or NRTIs has been detected in clinical trials of treatment-naive patients receiving DBRs to date
Use in clinical practice will further inform the virologic characteristics of failure on a DBR
PE9/21
James Demarest,1 Romina Quercia,2 Andrew Zolopa,1 Marty St Clair,1 Brian Wynne,3
Mark Underwood,1 Catherine Granier,4 Michael Aboud2 1ViiV Healthcare, Research Triangle Park, NC, USA; 2ViiV Healthcare, Brentford, UK; 3ViiV Healthcare, Upper Providence, PA, USA; 4GlaxoSmithKline, Stockley Park, UK
Integrated Analysis of Emergent Drug Resistance Through 96 and
144 Weeks From Clinical Studies of HIV-1 Treatment-Naive Subjects
Receiving Dolutegravir-Based Regimens
Acknowledgements
The study subjects and their caregivers; the study investigators and research staff; colleagues from ViiV Healthcare (Robert Cuffe) and GSK (Manrajdeep Virk, Mohammed Ali). This study was sponsored by ViiV Healthcare.
References
1. Raffi F, Jaeger H, Quiros-Roldan E, et al. Once-daily dolutegravir versus twice-daily raltegravir in antiretroviral-naive adults with HIV-1 infection (SPRING-2 study): 96 week results from a randomised, double-blind, non-inferiority trial. Lancet Infect Dis. 2013;13:927-935.
2. Walmsley S, Baumgarten A, Berenguer J, et al. Dolutegravir plus abacavir/lamivudine for the treatment of HIV-1 infection in antiretroviral therapy-naive patients: week 96 and week 144 results from the SINGLE randomized clinical trial. J Acquir Immune Defic Syndr. 2015 [Epub ahead of print].
3. Molina JM, Clotet B, van Lunzen J, et al. Once-daily dolutegravir versus darunavir plus ritonavir for treatment-naive adults with HIV-1 infection (FLAMINGO): 96 week results from a randomised, open-label, phase 3b study. Lancet HIV. 2015;2(4):e127-136.
SINGLE (Week 144) SPRING-2 (Week 96) FLAMINGO (Week 96) DTG ATR DTG RAL DTG DRV/r
Treatment (N) 414 419 411 411 242 242 n (%) 39 (9%) 33 (8%) 22 (5%) 29 (7%) 2 (<1%) 4 (2%) PDVF
Log pVL 2.14 (1.72-5.61)
2.07 (1.70-4.91)
1.94 (1.71-4.09)
1.93 (1.70-4.95)
3.17 (2.82-3.36)
3.62 (2.34-4.79)
Confirmation of PDVF
Log pVL 1.97 (1.71-5.49)
1.89 (1.71-6.16)
1.93 (1.70-2.80)
1.98 (1.70-5.45)
3.03 (2.72-3.21)
3.02 (2.98-4.92)
Time between PDVF and confirmation pVL
Weeks 3.3 (1.3-12.4)
3.9 (2.0-17.7)
3.4 (1.1-13.1)
3.0 (1.0-8.1)
2.2 (2.0-2.4)
3.4 (3.0-5.0)
DTG RAL
ATR
10
100
1,000
10,000
100,000
1,000,000
10
100
1,000
10,000
100,000
1,000,000
500 500VL
at P
DV
F
PR/RTonly
PR/RTand IN
7 7 3 7 7 13 5 2
INonly
NoResult
PR/RTonly
PR/RTand IN
10 6N= 3 1 16 10 10 16
INonly
NoResult
SINGLE (Wk144, DTG ATR ) SPRING-2 (Wk 96, DTG RAL )
Arm PDVF pVL NRTI NNRTI INI
SINGLE (Week 144)
ATR 1 Week 24 131 K65K/R, D67D/G, Q197Q/R
G190/G/E
2 Week 24 29,777 L264L/S V179V/D, G190G/A
3 Week 24 40,751 V35V/I K103N, G190G/A
4 Week 32 6,882 I178I/M K103K/N
5 Week 48 992 T286T/A K101E
6 Week 60 2,183 A288A/T K103K/N
7 Week 72 9,043 I135K K103N
SPRING-2 (Week 96)
RAL+TDF/FTC 1 Week 24 52 M184M/I
2 Week 24 76 A62A/V 3 Week 24 88,126 A62A/V, K65K/R,
K70K/E, M184V
T97T/A, E138E/D, V151V/I, N155H
RAL+ABC/3TC 4 Week 24 123 M184M/V
Arm # PDVF pVL (c/mL) Resistance
DRV/r 1 Week 36 61,754 None 2 Week 48 218 None 3 Week 72 5,140 None 4 Week 84 3,162 None
DTG 1 Week 24 668 None 2 Week 24 2,270 None
UK/DTGP/0037/16e Prepared March 2017
Prescribing Information Triumeq® ▼ dolutegravir 50mg/abacavir 600mg/lamivudine 300mg tablets See Summary of Product Characteristics before prescribing. Indication: HIV in over 12 years and > 40kg. Screen for HLA-B*5701 prior to use. Do not use if HLA-B*5701 positive. Dose: one tablet once daily with or without food. Elderly: Limited data in 65+ yrs. Creatinine clearance <50ml/min or moderate/severe hepatic impairment: Not recommended. Monitor closely in mild hepatic impairment. Contraindications: Hypersensitivity to any ingredient. Co-administration with dofetilide. Warnings/precautions: Both abacavir and dolutegravir are associated with risk of hypersensitivity reactions (HSR). Do not initiate in HLA-B*5701+ or previous suspected abacavir HSR. Stop Triumeq without delay if HSR suspected. Never reintroduce any dolutegravir- or abacavir-containing product after suspected HSR. Risks of immune reactivation syndrome, osteonecrosis, increased weight, lipids, glucose. Monitor LFTs in Hepatitis B/C co-infection. Inconclusive data on relationship between abacavir and MI; minimise all modifiable CV risk factors (e.g. smoking, hypertension, hyperlipidaemia). Not recommended if dolutegravir required b.d.
(with etravirine [without boosted PI], efavirenz, nevirapine, rifampicin, boosted tipranavir, carbamazepine, oxcarbazepine, phenytoin, phenobarbital and St John’s Wort). Use with cladribine not recommended. Use with Mg/Al-containing antacids, calcium, multivitamins or iron requires dosage separation. Caution with metformin: monitor renal function and consider metformin dose adjustment. Pregnancy/lactation: Not recommended. Avoid breast-feeding. Side effects: See SPC for details. Headache, insomnia, sleep/dream disorders, GI disturbance, fatigue, hypersensitivity, anorexia, depression, dizziness, somnolence, lethargy, malaise, cough, nasal symptoms, rash, pruritus, alopecia, arthralgia, myalgia, asthenia, fever, elevations of ALT, AST and CPK, blood dyscrasias, suicidal ideation or suicide attempt, rhabdomyolysis, lactic acidosis, erythema multiforme, Stevens-Johnson syndrome, toxic epidermal necrolysis. Basic NHS costs: 30 tablets: £798.16 EU/1/14/940/001. MA holder: ViiV Healthcare UK Ltd, 980 Great West Road, Brentford, Middlesex TW8 9GS. Further information is available from Customer Contact Centre, GlaxoSmithKline UK Ltd, Stockley Park West, Uxbridge, Middlesex UB11 1BT.
POM S1A Triumeq is a registered trademark of the ViiV Healthcare Group of Companies Date of approval: January 2017 Zinc code: UK/TRIM/0037/14(7) Adverse events should be reported. For the UK, reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to GlaxoSmithKline on 0800 221 441. Adverse events should be reported. For Ireland, adverse events should be reported directly to the HPRA; Freepost, Pharmacovigilance Section, Health Products Regulatory Authority, Earlsfort Terrace, Dublin 2, Tel: +353 1 676 4971, [email protected]. Adverse events should also be reported to GlaxoSmithKline on 1800 244 255.

Tivicay® ▼ dolutegravir 50mg tablets Prescribing Information See Summary of Product Characteristics before prescribing Indication: HIV in >12 years and >40kg as part of combination therapy. Dosing: 50mg once daily with or without food if no proven/ suspected integrase resistance. 50mg twice daily with efavirenz, nevirapine, tipranavir/ritonavir, etravirine (without boosted PI), carbamazepine, oxcarbazepine, phenytoin, phenobarbital, St John’s Wort or rifampicin. Adults with proven/ suspected integrase resistance: 50mg twice daily preferably with food. Elderly: Limited data in 65+ yrs. Caution in severe hepatic impairment. Contraindications: Hypersensitivity to any ingredient. Co-administration with dofetilide. Warnings/precautions: Risk of hypersensitivity reactions. Discontinue dolutegravir and other suspect agents immediately if suspected. Risks of osteonecrosis, immune reactivation syndrome. Monitor LFTs in Hepatitis B/C co-infection and
ensure effective Hepatitis B therapy. Caution with metformin: monitor renal function and consider metformin dose adjustment. Use with etravirine requires boosted PI or increased dose of dolutegravir. Use with Mg/Al-containing antacids, calcium, multivitamins or iron requires dosage separation. Pregnancy/ lactation: Not recommended. Avoid breast-feeding. Side effects: See SPC for full details. Headache, GI disturbance, insomnia, abnormal dreams, depression, dizziness, rash, pruritus, fatigue, elevations of ALT, AST and CPK, arthralgia, myalgia, hypersensitivity, suicidal ideation or suicide attempt. Basic NHS costs: 30 tablets £498.75 EU/1/13/892/001. MA holder: ViiV Healthcare UK Ltd, 980 Great West Road, Brentford, Middlesex TW8 9GS. Further information available from Customer Contact Centre, GlaxoSmithKline UK Ltd, Stockley Park West, Uxbridge, Middlesex UB11 1BT. POM S1A
Tivicay is a registered trademark of the ViiV Healthcare Group of Companies Date of approval: January 2017 Zinc code: UK/DLG/0055/13(9)
Adverse events should be reported. For the UK, reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to GlaxoSmithKline on 0800 221 441.
Adverse events should be reported. For Ireland, adverse events should be reported directly to the HPRA; Freepost, Pharmacovigilance Section, Health Products Regulatory Authority, Earlsfort Terrace, Dublin 2, Tel: +353 1 676 4971, [email protected]. Adverse events should also be reported to GlaxoSmithKline on 1800 244 255.

Kivexa® abacavir 600mg/lamivudine 300mg tablets Prescribing Information See Summary of Product Characteristics before prescribing Indications: HIV in adults, adolescents and children weighing at least 25 kg as part of combination therapy. Screen for HLA-B*5701 prior to use. Dose: one tablet daily with or without food. Elderly: No pharmacokinetic data in 65+ yrs. Renal impairment: Creatinine clearance <50ml/min: not recommended. Hepatic impairment: not recommended in moderate or severe hepatic impairment. Monitor closely in mild hepatic impairment. Contraindications: Hypersensitivity to any ingredient. Warnings/precautions: Risk of hypersensitivity reactions (HSR). Do not initiate in HLA-B*5701+ or previous suspected abacavir HSR. Stop Kivexa without delay if HSR suspected. Never re-introduce any abacavir-containing product after suspected HSR. Risks of virological failure, immune reactivation syndrome, osteonecrosis, increased
weight, lipids, glucose. Monitor LFTs in Hepatitis B/C co-infection. Inconclusive data on relationship between abacavir and MI; minimise modifiable CV risk factors (e.g. smoking, hypertension, hyperlipidaemia). Use with cladribine, emtricitabine or high doses of co-trimoxazole not recommended. Pregnancy/lactation: Not recommended. Avoid breast-feeding. Side effects: See SmPC for full details. Hypersensitivity, GI disturbance, headache, anorexia, insomnia, rash, fever, lethargy, fatigue, malaise, arthralgia, muscle disorders, nasal symptoms, cough, alopecia, blood dyscrasias, rhabdomyolysis, lactic acidosis, erythema multiforme, Stevens-Johnson syndrome and toxic epidermal necrolysis. Basic NHS costs: 30 tablets: £299.41 EU/1/04/298/002. MA holder: ViiV Healthcare UK Ltd, 980 Great West Road, Brentford, Middlesex TW8 9GS. Further information is available from Customer Contact Centre, GlaxoSmithKline UK Ltd, Stockley Park West, Uxbridge, Middlesex UB11 1BT.
POM S1A Kivexa is a registered trademark of the ViiV Healthcare Group of Companies Date of approval: October 2016 UK/ABC3TC/0008/13(9)
Adverse events should be reported. For the UK, reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to GlaxoSmithKline on 0800 221 441. Adverse events should be reported. For Ireland, adverse events should be reported directly to the HPRA; Freepost, Pharmacovigilance Section, Health Products Regulatory Authority, Earlsfort Terrace, Dublin 2, Tel: +353 1 676 4971, [email protected]. Adverse events should also be reported to GlaxoSmithKline on 1800 244 255.





























