Embed Size (px)
Citation preview

CLINICAL POLICY
Critical Issues in the Evaluation and Management of AdultPatients Presenting to the Emergency Department With
Suspected Pulmonary Embolism
From the American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Critical Issuesin the Evaluation and Management of Adult Patients Presenting to the Emergency Department With SuspectedPulmonary Embolism
Francis M Fesmire MD (Subcommittee ChairCommittee Co-Chair
Michael D Brown MD MScJames A Espinosa MDRichard D Shih MDScott M Silvers MDStephen J Wolf MDWyatt W Decker MD (Committee Co-Chair)
Members of the American College of Emergency Physicians Clinical Policies Committee (Oversight Committee)
EDA
SRSESDRR
A
S
Wyatt W Decker MD (Co-Chair 2006-2007 Chair 2007-2010 Co-Chair 2010-2011)
Francis M Fesmire MD (Co-Chair 2010-2011)Michael D Brown MD MScDeborah B Diercks MD MScBarry M Diner MD MPH (Methodologist)Jonathan A Edlow MDSteven A Godwin MDSigrid A Hahn MDBenjamin W Hatten MD (EMRA Representative 2008-
2010)John E Houghland MD (EMRA Representative 2010-
2011)J Stephen Huff MDEric J Lavonas MDGail Lenehan EdD RN FAEN FAAN (ENA
Representative 2010-2011)
Sharon E Mace MD
doi101016jannemergmed201101020
[Ann Emerg Med 201157628-652]
628 Annals of Emergency Medicine
dward Melnick MDevorah J Nazarian MDnnMarie Papa RN MSN CEN FAEN (ENA
Representative 2007-2010)usan B Promes MDichard D Shih MDcott M Silvers MDdward P Sloan MD MPHtephen J Wolf MDavid C Seaberg MD CPE (Board Liaison 2006-2010)obert E OrsquoConnor MD MPH (Board Liaison 2010-2011)honda R Whitson RHIA Staff Liaison Clinical PoliciesCommittee and Subcommittees
pproved by the ACEP Board of Directors January 132011
uppported by the Emergency Nurses Association
March 17 2011
Policy statements and clinical policies are the official policies of the American College of EmergencyPhysicians and as such are not subject to the same peer review process as articles appearing in the printjournal Policy statements and clinical policies of ACEP do not necessarily reflect the policies and beliefsof Annals of Emergency Medicine and its editors
0196-0644$-see front matterCopyright copy 2011 by the American College of Emergency Physicians
Volume June
owEpDCiit
oVPirapeu
M
aaAsuasa
medeeraPUCeefwA
gecdra
Clinical Policy
ABSTRACTThis clinical policy from the American College of Emergency
Physicians is the revision of a 2003 clinical policy on theevaluation and management of adult patients presenting withsuspected pulmonary embolism (PE)1 A writing subcommitteereviewed the literature to derive evidence-basedrecommendations to help clinicians answer the following criticalquestions (1) Do objective criteria provide improved riskstratification over gestalt clinical assessment in the evaluation ofpatients with possible PE (2) What is the utility of thePulmonary Embolism Rule-out Criteria (PERC) in theevaluation of patients with suspected PE (3)What is the role ofquantitative D-dimer testing in the exclusion of PE (4) What isthe role of computed tomography pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE (5) Whatis the role of venous imaging in the evaluation of patients withsuspected PE (6) What are the indications for thrombolytictherapy in patients with PE Evidence was graded andrecommendations were given based on the strength of theavailable data in the medical literature
INTRODUCTIONIt is estimated that 650000 to 900000 individuals each year
have fatal or nonfatal acute pulmonary embolism (PE)2 and thatas many as 200000 people in the United States die each yearfrom PE3 Untreated PE can be rapidly fatal with the majorityof deaths occurring in the first hour34 Furthermore survivorsof undiagnosed PE can experience disabling morbidity frompulmonary hypertension5 andor postthrombotic syndrome6-8
Because there is a strong association between deep venousthrombosis (DVT) and PE it is difficult to discuss thediagnostic evaluation of one entity without discussing theother7 Approximately 50 of patients with documented DVThave perfusion defects on nuclear lung scanning andasymptomatic venous thrombosis is found in approximately40 of patients with confirmed PE6910
During the past decade there has been an explosion ofpublished research and development of new diagnosticmodalities and therapies relating to patients with suspected PEand DVT with greater than 1000 publications appearing inthe medical literature per year This current policy represents arevision of the 2003 American College of Emergency Physicians(ACEP) clinical policy on critical issues in the evaluation andmanagement of adult patients with suspected PE1 The 2003policy focused on 4 major areas of interest andor controversythat existed when the policy was formulated (1) Can a negativeD-dimer result exclude PE (2) When can ventilation-perfusion(VQ) scan alone or in combination with venousultrasonography andor D-dimer assay exclude PE (3) Canspiral computed tomography (CT) replace VQ scanning in thediagnostic evaluation of PE and (4) What are the indicationsfor thrombolytic therapy in patients with PE This currentpolicy focuses on 6 areas of interest andor controversy that have
developed or still exist since the 2003 policy was formulated A
Volume June
(1) Do objective criteria provide improved risk stratificationver general clinical assessment in the evaluation of patientsith possible PE (2) What is the utility of the Pulmonarymbolism Rule-out Criteria (PERC) in the evaluation ofatients with suspected PE (3)What is the role of quantitative-dimer testing in the exclusion of PE (4) What is the role ofT pulmonary angiogram of the chest as the sole diagnostic test
n the exclusion of PE (5) What is the role of venous imagingn the exclusion of PE and (6) What are the indications forhrombolytic therapy in patients with PE
This policy does not discuss VQ scanning in the evaluationf patients with suspected PE The authors do recognize thatQ scanning is used in the evaluation of patients with suspectedE in whom CT scan may be contraindicated11-13 Also with
ncreasing awareness of potential long-term effects of ionizingadiation exposure from repetitive CT scans there may bedditional subgroups of patients for whom a VQ scan may bereferred as the initial imaging modality because of decreasedxposure to radiation compared with CT scan13-17 Futurepdates of this policy may directly address these issues
ETHODOLOGYThis clinical policy was created after careful review and critical
nalysis of the medical literature Multiple searches of MEDLINEnd the Cochrane Library were performed To update the 2003CEP clinical policy all searches were limited to English-language
ources and human studies Specific key wordsphrases and yearssed in the searches are identified under each critical question Inddition relevant articles from the bibliographies of includedtudies and more recent articles identified by committee membersnd peer reviewers are included
The reasons for developing clinical policies in emergencyedicine and the approaches used in their development have been
numerated18 This policy is a product of the ACEP clinical policyevelopment process including expert review and is based on thexisting literature when literature was not available consensus ofmergency physicians was used Expert review comments wereeceived from individual emergency physicians and cardiologistsnd from individual members of the American College of Chesthysicians American College of Radiology ACEPrsquos Emergencyltrasound Section and ACEPrsquos Quality and Performanceommittee Their responses were used to further refine and
nhance this policy however their responses do not implyndorsement of this clinical policy Clinical policies are scheduledor revision every 3 years however interim reviews are conductedhen technology or the practice environment changes significantlyCEP is the funding source for this clinical policy
All articles used in the formulation of this clinical policy wereraded by at least 2 subcommittee members for strength ofvidence and classified by the subcommittee members into 3lasses of evidence on the basis of the design of the study withesign 1 representing the strongest evidence and design 3epresenting the weakest evidence for therapeutic diagnosticnd prognostic clinical reports respectively (Appendix A)
rticles were then graded on 6 dimensions thought to be most
Annals of Emergency Medicine 629
oi
rettmc
p(
p
aas
C1ow
gwp
pdGaD
Eaeltswccpoa
O
i
Clinical Policy
relevant to the development of a clinical guideline blindedversus nonblinded outcome assessment blinded or randomizedallocation direct or indirect outcome measures (reliability andvalidity) biases (eg selection detection transfer) externalvalidity (ie generalizability) and sufficient sample size Articlesreceived a final grade (Class I II III) on the basis of apredetermined formula taking into account design and qualityof study (Appendix B) Articles with fatal flaws were given anldquoXrdquo grade and not used in formulating recommendations in thispolicy Evidence grading was done with respect to the specificdata being extracted and the specific critical question beingreviewed Thus the level of evidence for any one study may varyaccording to the question and it is possible for a single article toreceive different levels of grading as different critical questionsare answered Question-specific level of evidence grading may befound in the Evidentiary Table included online (available athttpwwwannemergmedcom)
Clinical findings and strength of recommendations regardingpatient management were then made according to the followingcriteria
Level A recommendations Generally accepted principles forpatient management that reflect a high degree of clinicalcertainty (ie based on strength of evidence Class I oroverwhelming evidence from strength of evidence Class IIstudies that directly address all of the issues)
Level B recommendations Recommendations for patientmanagement that may identify a particular strategy or range ofmanagement strategies that reflect moderate clinical certainty (iebased on strength of evidence Class II studies that directly addressthe issue decision analysis that directly addresses the issue or strongconsensus of strength of evidence Class III studies)
Level C recommendations Other strategies for patientmanagement that are based on Class III studies or in the absence ofany adequate published literature based on panel consensus
There are certain circumstances in which the recommendationsstemming from a body of evidence should not be rated as highly asthe individual studies on which they are based Factors such asheterogeneity of results uncertainty about effect magnitude andconsequences and publication bias among others might lead tosuch a downgrading of recommendations
When possible clinically oriented statistics (eg likelihoodratios [LRs] number needed to treat) will be presented to helpthe reader better understand how the results can be applied tothe individual patient For a definition of these statisticalconcepts see Appendix C
This policy is not intended to be a complete manual on theevaluation and management of patients with suspected PE butrather a focused examination of critical issues that have particularrelevance to the current practice of emergency medicine
It is the goal of the Clinical Policies Committee to providean evidence-based recommendation when the medical literatureprovides enough quality information to answer a criticalquestion When the medical literature does not contain enough
quality information to answer a critical question the members p
630 Annals of Emergency Medicine
f the Clinical Policies Committee believe that it is equallymportant to alert emergency physicians to this fact
Recommendations offered in this policy are not intended toepresent the only diagnostic and management options that themergency physician should consider ACEP clearly recognizeshe importance of the individual physicianrsquos judgment Ratherhis guideline defines for the physician those strategies for whichedical literature exists to provide support for answers to the
rucial questions addressed in this policyScope of Application This guideline is intended for
hysicians working in hospital-based emergency departmentsEDs) or ED-based observation centers
Inclusion Criteria This guideline is intended for adultatients presenting to the ED with suspected PE
Exclusion Criteria This guideline is not intended toddress the care of patients with PE in the presence of cardiacrrest or pregnancy patients with absence of symptomsuggestive of PE or pediatric patients
RITICAL QUESTIONS Do objective criteria provide improved risk stratificationver gestalt clinical assessment in the evaluation of patientsith possible PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Either objective criteria or
estalt clinical assessment can be used to risk stratify patientsith suspected PE There is insufficient evidence to support thereferential use of one method over another
Level C recommendations None specified
Key wordsphrases for literature searches risk stratificationulmonary embolism ED emergency service risk assessmentiagnostic strategies Wells criteria Wicki criteria Kline criteriaeneva score revised Geneva score PISA model and variations
nd combinations of the key wordsphrases years 2000 throughecember 2009This critical question focuses on pretest probability assessment
stimation of pretest probability is imperative for the properpplication of any diagnostic test This general principle becomesven more important for PE because it is a common but potentiallyethal disease when left undiagnosed and untreated Unfortunatelyhe classic presentation of PE is rare and physicians must makeome sort of assessment about whether to evaluate patients for PEhen they present with symptoms such as unexplained dyspnea
hest pain hemoptysis palpitations syncope back pain and otherommonplace symptoms that have been associated with PE Pretestrobability assessment in PE can be estimated in 2 general waysbjective criteria (clinical decision rules) or gestalt clinicalssessment (implicit approach)
bjective Criteria (Clinical Decision Rules)Clinical decision rules are a form of objective criteria that are
ntended to provide more accurate and reproducible measure of
retest probability assessment than the overall gestalt clinical
Volume June
W
omesaP
TaewPprCrtp
V
RAPRASUHCH
P
S
R041S
025
03
tnaacv
Clinical Policy
impression that depends on the physicianrsquos expertise and clinicalexperience Such rules can be derived and validated They alsocan be compared to each other and refined over time Severalclinical decision rules have been developed for use in patientswith suspected PE The most commonly used methods are (1)Geneva score19-21 (2) Wells (Canadian) score22 (3) Kline(Charlotte) criteria23 and (4) Pisa model2425
Geneva ScoreThe original Geneva score as described by Wicki et al19 in
2001 is a Class II study that was performed at a single hospitalin Switzerland and consists of a clinical score ranging from 0 to16 points derived from 8 parameters relating to risk factorsclinical signs blood gas analysis and chest radiographProbability of PE in patients defined as low- (0 to 4 points)intermediate- (5 to 8 points) and high- (9 points) risk was10 38 and 81 respectively Multiple Class III studieshave since validated the usefulness of the Geneva score in riskstratification of patients with suspected PE26-31
Because of the reliance of the original Geneva score on roomair blood gas analysis and chest radiograph interpretation LeGal et al20 in a Class II study retrospectively analyzed datafrom 2 previous multicenter clinical investigations to develop ascore independent of diagnostic testing The subsequent revisedGeneva score ranged from 0 to 25 points and was derived from8 parameters relating to risk factors symptoms and clinicalsigns (Table 1) In the validations set probability of PE in low-(score 0 to 3) intermediate- (score 4 to 10) and high-risk (score11) patients was 8 29 and 74 respectively To dateonly one Class II investigation has validated the revised Genevascore32
One of the difficulties of the revised Geneva score is thatdifferent elements have different weights making it potentiallymore difficult to apply in the clinical setting (Table 1) As a resultKlok et al21 in a Class II study reanalyzed the same populationand developed the simplified revised Geneva score that uses theidentical 8 parameters of the revised Geneva score (Table 1) Onepoint is assigned to each parameter except for pulse rate greaterthan or equal to 95 beatsmin which results in an additional pointProbability of PE in patients defined as low- (0 to 1 point)intermediate- (2 to 4 points) and high- (5 to 7 points) risk was 829 and 64 respectively The investigators also divided thepatients into the dichotomous group of PE unlikely (0 to 2 pointsprobability of PE 115) and PE likely (3 to 7 points probabilityof PE 351) to select a patient population safe for use of D-dimertesting for exclusion of PE Of the 330 patients with a PE unlikelyscore and a negative D-dimer result no patient was diagnosed ashaving venous thromboembolic disease on presentation or on 3-month follow-up Receiver operating characteristic (ROC) curveanalysis revealed no differences in diagnostic performance of therevised Geneva score (area under ROC curve 075 95 confidenceinterval [CI] 071 to 078) compared with the simplified revised
Geneva score (area under ROC curve 074 95 CI 070 to 077) a
Volume June
ells ScoreThe original Wells study was a Class III investigation in use
f a clinical model to risk stratify 1239 patients in low-oderate- and high-risk groups33 The investigators used
vidence from the published literature to establish a risk-tratification model by consensus The risk model initiallyssessed patients based on signs and symptoms as ldquotypicalrdquo forE ldquoatypicalrdquo for PE or ldquosevererdquo Physicians then made an
able 1 Revised Geneva score as described by Le Gal et al20
nd the simplified revised Geneva score as described by Klokt al21 for assessment of pretest probability of PE Reprintedith permission Copyright copy American College of Physiciansublisher Le Gal G Righini M Roy P-M et al Prediction ofulmonary embolism in the emergency department theevised Geneva score Ann Intern Med 2006144165-171opyright copy 2008 American Medical Association All rightseserved Klok FA Mos IC Nijkeuter M et al Simplification ofhe revised Geneva score for assessing clinical probability ofulmonary embolism Arch Intern Med 20081682131-2136
ariable
Points
RevisedGeneva
Simplified RevisedGeneva
isk factorsge 65 y 1 1revious DVTPE 3 1ecent surgeryfracture (4 wk) 2 1ctive malignancy 2 1ymptomsnilateral lower-limb pain 3 1emoptysis 2 1linical signseart rate75ndash94 beatsmin 3 195 beatsmin 5 2
ain on lower-limb deep venouspalpation and unilateral edema
4 1
core RangeProbability of PE
(95 CI)Patients WithThis Score
Interpretationof Risk
evised Geneva Score20
ndash3 79 (50ndash121) 370 Lowndash10 285 (246ndash328) 574 Moderate1ndash25 737 (610ndash834) 55 Highimplified Revised Geneva Score21
Traditional interpretationndash1 77 (52ndash108) 360 Lowndash4 294 (259ndash331) 60 Moderatendash7 643 (480ndash785) 40 HighAlternative interpretation
ndash2 129 (105ndash157) 649 PE unlikelyndash7 416 (365ndash468) 351 PE likely
The original table from Klok et al21 lists 1 point for heart rate 95 beatsmin buthe assessment of score states ldquo[b]ecause of the weight of heart rate in the origi-al score we attributed 1 point to a heart rate between 75 and 94 beatsmin andn additional point for a heart rate of 95 beatsmin or morerdquo Thus a patient withheart rate of 100 beatsmin would receive a total of 2 points (personal communi-
ation F A Klok MD PhD Department of General Internal Medicine Leiden Uni-ersity Medical CenterBronovo Hospital Den Haag May 2010)
ssessment about whether an ldquoalternative diagnosis that was as
Annals of Emergency Medicine 631
11pw1v9ts
vopphedP(
vHaarcp
K
csephsrwwaut(thps9Cet1IL
Clinical Policy
likely as or more likely than PErdquo to further subdivide thepatients into 10 possible outcomes These outcomes were thendivided into low- moderate- and high-risk groups Rates of PEin patients with low moderate and high risk were 34278 and 784 respectively Although this modelperformed well the algorithmic approach was not suitable to beused as an objective risk-stratification tool
Wells et al22 subsequently performed a retrospective analysisof the data used in the original study to develop a simple scoringsystem that could be used in conjunction with D-dimer for theevaluation of patients with suspected PE (Table 2) Usingregression techniques a risk-stratification model consisting of 7variables was created that classified patients as having lowmoderate and high probability of PE In addition analternative interpretation system was developed in which thepatients were classified into the dichotomist groups ldquoPEunlikelyrdquo and ldquoPE likelyrdquo to identify a group of patients forwhom a negative D-dimer test would result in a PE rate of 2If the D-dimer result was negative the rate of PE in patientsdesignated PE unlikely (score 0 to 4) was 22 in the derivationset and 17 in the validation set
This model was subsequently prospectively validated in aClass II investigation in a cohort of 4 EDs at tertiary carehospitals in Canada34 The initial pretest probabilities weredetermined by the clinical model to be low in 57 of patientsmoderate in 36 of patients and high in 7 of patientsIncluding follow-up events PE was diagnosed in 13 of
Table 2 Wells Canadian Score for assessment of pretestprobability for PE22 Reprinted with permission Copyright copySchattauer Publisher Wells PS Anderson DR Rodger M etal Derivation of a simple clinical model to categorize patientsprobability of pulmonary embolism increasing the modelsutility with the SimpliRED D-dimer Thromb Haemost 200083416-420
Criteria Points
Suspected DVT 30An alternative diagnosis is less likely than PE 30Heart rate 100 beatsminute 15Immobilization or surgery in the previous 4 weeks 15Previous DVTPE 15Hemoptysis 10Malignancy (on treatment treated in the last 6
months or palliative)10
Score RangePoints Probability of PE ()
With ThisScore
Interpretationof Risk
Traditionalinterpretation
0ndash1 36 (20ndash59) 403 Low2ndash6 205 (170ndash241) 526 Moderate6 667 (543ndash776) 71 HighAlternate
interpretation0ndash4 78 (59ndash101) 715 PE unlikely4 407 (349ndash465) 285 PE likely
patients with low pretest probability (95 CI 05 to 27) d
632 Annals of Emergency Medicine
62 of patients with moderate pretest probability (95 CI25 to 206) and in 406 of patients with high pretestrobability (95 CI 287 to 537) Of the 437 patientsith a negative D-dimer result and low clinical probability onlydeveloped PE during follow-up giving a negative predictive
alue for the use of the clinical model with D-dimer testing of95 (95 CI 991 to 100) No information is given inhis investigation about performance of the alternative scoringystem of ldquoPE unlikelyrdquo and ldquoPE likelyrdquo
A Class II investigation by the Christopher Study Investigatorsalidated the utility of the dichotomized alternative scoring systemf ldquoPE unlikelyrdquo versus ldquoPE likelyrdquo35 This study was a multicenterrospective cohort of 3306 patients A total of 2206 (667)atients were classified as PE unlikely Of these 1057 patients alsoad a negative D-dimer result and PE was considered to have beenxcluded On 3-month follow-up 5 (05) patients received aiagnosis of venous thromboembolic disease with no deaths In theE likely subgroup PE was diagnosed on CT scan in 674 patients204)
Multiple Class II3637and Class III studies28-3138-43 havealidated the usefulness of the Wells score in risk stratificationowever a major criticism of the Wells score is that it is not truly
n objective criterion because it contains the subjective variable ldquoanlternative diagnosis is less likely than PErdquo This variable in essenceepresents physician judgment override of the objectiveomponents of the score because it is worth 3 points and thuslaces the patient in the intermediate-risk group19324445
line RuleKline et al23 in a Class II study derived a decision rule to
reate a binary partition of ED patients with suspected PE toelect patients for whom a negative D-dimer result reliablyxcluded the presence of PE (Figure) Nine-hundred thirty-fouratients were studied at 7 urban EDs in the United States Theistory and physical process occurred prospectively beforetandard imaging to look for recognized symptoms signs andisk factors associated with PE Selected variables were analyzedith multivariate logistic analysis to determine factors associatedith PE A decision rule was then constructed to categorize
pproximately 80 of ED patients as being able to safelyndergo D-dimer testing Six variables were used to constructhe decision rule Unsafe patients had either a shock indexpulse ratesystolic blood pressure more than 10) or age greaterhan 50 years together with any of the following unexplainedypoxemia (arterial blood oxygen saturation [SaO2] 95 norevious lung disease) unilateral leg swelling recent majorurgery or hemoptysis These criteria were met by 197 (21) of34 patients Of these 197 patients 83 had PE (421 95I 355 to 496) When these 197 ldquounsaferdquo patients were
xcluded the probability of PE was significantly decreased inhe remaining 737 (79) ldquosaferdquo patients to 133 (95 CI09 to 159) Assuming use of an Enzyme-Linkedmmunosorbent Assay (ELISA) D-dimer assay with a negativeR of 007 the use of the Kline rule in conjunction with D-
imer testing would decrease the posttest probability of PE to
Volume June
eurgmdpmpiovoirpeh(a
wa3osPrsw2(
C
hcnCp
Pspwalps
cWaP
Clinical Policy
approximately 1 The authors concluded that these criteriacan permit safe D-dimer testing in the majority of ED patientswith suspected PE
There are no prospective outcome studies validating the useof the Kline rule in conjunction with D-dimer but 1 Class IIIstudy demonstrated a 21 decrease in CT scanning when theyinstituted this protocol46
Pisa ModelThe original Pisa investigation is a Class II study consisting
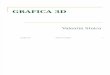
Figure Kline decision rule for excluding PE23 Reprintedfrom Annals of Emergency Medicine 39 Kline JA NelsonRD Jackson RE et al Criteria for the safe use of D-dimertesting in emergency department patients with suspectedpulmonary embolism a multicenter US study 144-1522002 Copyright from the American College of EmergencyPhysicians [2002]
Flow diagram demonstrating the Kline decision rule inselecting patients in whom D-dimer assay less than 500 ngml can reliably rule out PE This decision rule splits thepatients into 2 groups four fifths of whom are eligible for D-dimer testing (ldquosaferdquo patients with pretest probability of PE of133) and one fifth of whom are ineligible for D-dimertesting (ldquounsaferdquo patients with pretest probability of 421)
of 1100 consecutive patients with suspected PE who were W
Volume June
valuated at a single hospital in Pisa Italy24 All patientsnderwent a detailed clinical history physical examinationigorous interpretation of ECG and chest radiograph and bloodas measurements Using logistic regression techniques aathematical model for predicting probability of PE was
eveloped Probability was categorized as low (10robability of PE) intermediate (10 to 50 probability)oderately high (50 to 90 probability) and high (90
robability) Ten characteristics were associated with anncreased risk of PE male sex older age history of DVT acutenset dyspnea chest pain hemoptysis ECG signs of rightentricular overload radiographic signs of oligemia amputationf the hilar artery and pulmonary consolidations suggestive ofnfarction Five characteristics were associated with a decreasedisk previous cardiovascular or pulmonary disease feverulmonary consolidation other than infarction and pulmonarydema With this model 432 patients (39) were rated asaving low probability (4 PE) 283 (26) as intermediate22 PE) 72 (7) as moderately high probability (74 PE)nd 313 (28) as high probability (98 PE)
In the original Pisa model the highest regression coefficientsere for the chest radiograph findings (oligemia 386
mputation of hilar artery 392 and pulmonary infarction55) Because of the heavy reliance of the original Pisa modeln advanced chest radiograph interpretation skills beyond thekill level of the average physician Miniati et al25 refined theisa model in the same patient population after excluding chestadiograph from the final equation (Table 3) In the validationet of this Class II investigation the prevalence of PE was 2hen the predicted clinical probability was low (0 to 10)8 when moderate (11 to 50) 67 when substantial51 to 80) and 94 when high (81 to 100)
omparative Studies of Objective CriteriaThere are two Class II3247 and 3 Class III283031 studies that
ave evaluated performance of the various objective criteria Inomparing the Geneva score to the Wells score 3 studies foundo significant differences in performance though the study byhagnon et al28 suggested that the Geneva score overridden byhysician judgment may be more accurate283132
Miniati et al30 compared the Geneva score Wells score andisa model in 215 patients with suspected PE and foundtatistically significant differences in performance of the 3retest probability assessment tools Areas under the ROC curveere 054 075 and 094 for the Geneva score Wells score
nd Pisa model respectively However findings in this study areimited because of small sample size and the PE rate in thisatient population was extremely high (43) indicatingignificant patient selection bias
Runyon et al47 compared the Wells score with the Klineriteria in 2603 patients with a PE prevalence of 58 The
ells score identified 73 of patients as low risk (score 2)nd the Kline criteria identified 88 of patients as low risk TheE rates in these low-risk patients were 30 and 42 for the
ells and Kline criteria respectively
Annals of Emergency Medicine 633
wadt16gIp
oipgaoiRr(3s
ppap1ssi3ldquotrlcbp
pIgsi
L
r
ypP
Clinical Policy
Gestalt Clinical AssessmentGestalt clinical assessment is an unstructured (nonruled based)
estimate of the pretest probability of disease It is based on theclinicianrsquos training clinical experience and judgment Thisapproach has also been described as implicit in nature Theclinician using this approach surmises an overall impression of thepretest probability of PE and applies that impression to the decisionabout whether to pursue the diagnosis through objective testing
The Prospective Investigation of Pulmonary EmbolismDiagnosis (PIOPED) study was a prospective multi-institutioninvestigation designed to evaluate various conventional methodsfor diagnosing PE48 The PIOPED study is the first major studyreporting gestalt assessment As one element of the study the
Table 3 Regression coefficients and odds ratio for the Pisamodel as described by Miniati et al25 for estimatingprobability of pulmonary embolism according to clinical andECG findings Calculation of the clinical probability ofpulmonary embolism is performed as follows (1) Add all thecoefficients that apply to a given patient and the constantndash343 to obtain a sum score (2) the probability of pulmonaryembolism equals [1exp(ndashsum)]ndash1 Reprinted with permissionof the American Thoracic Society Copyright copy AmericanThoracic Society Miniati M Bottal M Monti S et al Simpleand accurate prediction of the clinical probability of pulmonaryembolism American Journal of Respiratory and Critical CareMedicine 2008178290-294 Official journal of the AmericanThoracic Society Diane Gern Publisher
Predictor Coefficient Odds Ratio 95 CI
Age y57ndash67 080 223 137ndash36368ndash74 087 238 141ndash40175 114 311 182ndash532Male sex 060 182 127ndash261Risk factorsImmobilization 042 153 108ndash215Deep venous thrombosis (ever) 064 190 123ndash295Preexisting diseasesCardiovascular ndash051 060 041ndash088Pulmonary ndash089 041 024ndash072SymptomsDyspnea (sudden onset) 200 738 518ndash1051Orthopnea ndash151 022 005ndash093Chest pain 101 274 193ndash388Fainting or syncope 066 193 125ndash298Hemoptysis 093 252 119ndash535SignsLeg swelling (unilateral) 080 223 135ndash370Fever 38degC (1004degF) ndash147 023 013ndash040Wheezes ndash120 030 014ndash066Crackles ndash061 054 035ndash083ElectrocardiogramAcute cor pulmonale 196 711 466ndash1087Constant ndash343
One or more of the following ECG abnormalities S1Q3T3 S1S2S3 negativeT waves in right precordial leads transient right bundle branch blockpseudoinfarction
clinicianrsquos assessment of the likelihood of PE from 0 to 100 t
634 Annals of Emergency Medicine
as recorded for 887 patients and was compared with PE statuss determined by angiogram and follow-up information Forata analysis low risk was considered pretest probability of 0o 19 intermediate risk 20 to 79 and high risk 80 to00 PE subsequently was diagnosed in 92 299 and78 of patients in the low- intermediate- and high-riskroups respectively Since the PIOPED study multiple ClassII studies have validated the usefulness of gestalt assessment ofretest probability in evaluating patients with suspected PE49-53
There have been several comparative studies of gestalt versusbjective criteria In a Class II study investigating potentialmpact of adjusting the D-dimer threshold Kabrhel et al37
rospectively performed pretest probability assessment usingestalt versus the Wells score in 7940 patients from 10cademic centers By gestalt pretest probability assessment 68f patients were low risk (15 pretest probability PE) 26ntermediate risk (15 to 40) and 6 high risk (40)ates of PE in these 3 subgroups were 3 10 and 33
espectively By the Wells score 69 of patients were low riskWells score 2) 28 intermediate (Wells score 2 to 6) and high risk (Wells score 6) Rates of PE in these 3ubgroups were 3 13 and 36 respectively
Sanson et al41 in a Class III study investigated pretestrobability assessment of gestalt versus the Wells score in 517atients with a 31 PE rate By gestalt pretest probabilityssessment 14 of patients were low risk (20 pretestrobability PE) 67 intermediate risk (20 to 80) and9 high risk (80 to 100) Rates of PE in these 3ubgroups were 19 29 and 46 respectively By the Wellscore 36 of patients were low risk (Wells score 2) 63ntermediate (Wells score 2 to 6) and 2 high risk (Wells score
6) Rates of PE in these 3 subgroups were 28 30 and8 respectively The authors conclude that both methodsalthough comparable perform disappointingly in categorizinghe pretest probability in patients with suspected PErdquo The highate of patients categorized as having intermediate risk and theow rate of patients categorized as having low risk in this studyompared with other studies suggest significant patient selectionias that may account for the poor performance in pretestrobability assessment by these 2 methods
Runyon et al47 in a Class II study compared gestalt pretestrobability assessment with the Wells criteria and the Kline rulen the low-risk group rate of PE was 26 30 and 42 forestalt Wells and Kline rule respectively Gestalt and Wellscore also were equivalent in pretest probability assessment forntermediate- and high-risk patients
imitationsSeveral issues concerning performance of clinical decision
ules and gestalt assessment have been raised in the literature(1) Interrater reliability Nordenholtz et al54 compared third-
ear emergency medicine resident and attending emergencyhysician interrater reliability for 271 patients with suspectedE Specific elements of the Wells and Kline risk-stratification
ools were studied Interrater agreement was concluded to be
Volume June
ea2
sdm2cditaupAatapsmawbsPkc
cpoby
P8wTeao3plnc3sr
Clinical Policy
moderate for DVT symptoms (054) immobilization(041) unexplained hypoxia (058) and PE more likelythan alternative diagnosis (05) good for hemoptysis(076) and very good for previous DVT (090)malignancy (087) and tachycardia (094) Runyon et al47
in a large single hospital study involving a subset of 154 patientsfound only moderate interrater agreement for gestalt clinicalassessment of low probability (06) and Wells score less than 2(047) and very good for Kline rule ldquosaferdquo (085)
(2) Clinical experience as a factor in the determination ofpretest probability of PE Accurate determination of the pretestprobability of PE appeared to trend with clinical experienceHowever the authors concluded that difference in accuracybetween the inexperienced and experienced physicians is notsufficiently large to distinguish between the 2 when determiningwhether clinical gestalt or a clinical prediction rule should beused to determine the pretest probability of PE55
Iles et al44 performed a survey to investigate whether numberof years since graduation from medical school affected pretestprobability score for the Geneva Wells and gestalt pretestprobability assessment The Geneva score was found to be themost consistent method of determining pretest probabilityGestalt assessment was inversely proportional to clinicalexperience suggesting that as physicians gain experience theyrecognize the difficulties in ruling out PE and are reluctant toexclude it on clinical grounds
(3) Knowledge and use of the rules Runyon et al56 surveyedemergency medicine clinicians and found that only half of allclinicians reporting familiarity with the rules use them in morethan 50 of applicable cases Spontaneous recall of the ruleswas low to moderate
ConclusionBoth objective criteria and gestalt assessment appear to
perform equally well for patients with suspected PE With theadvent of electronic charting future studies need to beperformed investigating the use of computer support aids infacilitating pretest probability assessment Studies also need tobe performed investigating use of pretest probability assessmentto guide subsequent diagnostic testing Finally studies need tobe performed to clarify the definitions of low- intermediate-and high-risk groups especially for gestalt assessment in whichstudies have used pretest probabilities ranging from 20 to80 as definition for intermediate probability
2 What is the utility of the PERC in the evaluation ofpatients with suspected PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations In patients with a low pretest
probability for suspected PE consider using the PERC toexclude the diagnosis based on historical and physical
examination data alone a
Volume June
Level C recommendations None specified
Key wordsphrases for literature searches PERC pulmonarymbolism rule-out criteria block rule pulmonary embolismnd variations and combinations of the key wordsphrases years000 through December 2009In 2004 Kline et al57 published a Class II prospective
tudy deriving clinical criteria to prevent unnecessaryiagnostic testing in ED patients with suspected PE In thisulticenter study with 3148 patients in a derivation cohort
1 descriptive variables relevant to the diagnosis of PE wereollected The primary outcome variable was the EDiagnosis of PE using a composite criterion standard
ncluding 90-day follow-up The overall prevalence of venoushromboembolism (VTE) was 11 Logistic regressionnalysis with stepwise backwards elimination of variables wassed to identify criteria that could predict a patientopulation estimated to have a prevalence of disease of 18t or below this low pretest probability of disease theuthors proposed that no further laboratory or radiographicesting would be needed to exclude the diagnosis of PElthough this threshold which was based on a previouslyublished method for calculating testing thresholds58 hasubsequently been more accurately estimated to be 14 by aore recent decision analytic model balancing the benefits
nd costs of using the PERC59 After their analysis 8 variablesere identified age younger than 50 years pulse rate less than 100eatsmin SaO2 greater than 94 (at sea level) no unilateral legwelling no hemoptysis no recent trauma or surgery no previousE or DVT and no hormone use These criteria have since becomenown as the PERC When all criteria are met a patient isonsidered to be PERC negative
In this same study the authors went on to internally validate theriteria in a separate patient cohort57 When applied to 1427atients considered to be low risk for PE by gestalt assessment 25f patients were PERC negative The criteria when considered toe a diagnostic test had 96 sensitivity and 27 specificityielding a LR- of 015 and a 14 false-negative rate
In 2008 Kline et al60 published a Class II validation study of theERC (Table 4) This multicenter prospective study enrolled138 patients Although limited by the number of eligible patientsho were not enrolled the authors made attempts to address thishe outcome measures were similar to those of the original study
xcept for follow-up occurring at 45 days as opposed to 90 daysnd the overall prevalence of VTE being 69 Sixty-seven percentf patients were classified as low risk by clinical gestalt and of these07 were PERC negative This equated to 204 of enrolledatients The sensitivity specificity and LR- for the PERC in the
ow-risk cohort were 947 219 and 012 respectively Ofote 35 of enrolled patients were PERC negative but notonsidered to be low risk by clinical gestalt This subgroup had a1 prevalence of VTE Although outcomes on this specificubgroup were not reported not all PERC negative patients are lowisk and the rulersquos applicability in these patients is unknown The
uthors concluded that the PERC could be used in combination
Annals of Emergency Medicine 635
pa
edk
DlSqbsrs(tapeii(oidhat
qdoCtpdpoCc9pos
tPrzi
Clinical Policy
with a low pretest probability to identify very low-risk patients forwhom the diagnosis of PE can be reliably excluded based onhistorical and physical examination data alone
In 2008 Wolf et al61 published a small Class III externalvalidation of the PERC This study was a post hoc analysis ofprospectively collected data on 120 consecutive ED patientswith a suspicion of PE The original database contained allPERC variables Outcome measures used were similar to thoseof the original study yielding a 12 prevalence of PE Whentheir entire patient population is considered regardless ofpretest probability the sensitivity and specificity were 100 and16 respectively When only the patients with low pretestprobability as defined by Wells Criteria are considered thespecificity increased to 22 The authors concluded that thePERC may identify a cohort of patients with suspected PE forwhom diagnostic testing beyond history and physicalexamination is not indicated
In each of the above 3 clinical studies even though patient datawere collected prospectively the application of the PERC rule wasperformed retrospectively As such there is no prospective outcomestudy of the use of the PERC rule for clinical decisionmaking Thislimits the strength of recommendations that can be made based onthe available evidence Future research should focus on the clinicalapplication of the PERC rule with measurement of acceptedoutcomes
3 What is the role of quantitative D-dimer testing in theexclusion of PE
Patient Management RecommendationsLevel A recommendations In patients with a low pretest
probability for PE a negative quantitative D-dimer assay resultcan be used to exclude PE
Table 4 The Pulmonary Embolism Rule Out Criteria (PERC)
The PERC criteria negative (PERCndash) require the clinician to answer noto the 8 questions below60 If a patient is low risk by gestaltimpression and PERCndash the posttest probability of venousthromboembolism is 2 Reprinted with permission Copyright copyJohn Wiley amp Sons Ltd Publisher Kline JA Courtney DM KabrhelC et al Prospective multicenter evaluation of the pulmonaryembolism rule-out criteria J Thromb Haemost 20086772-780
1 Is the patient older than 49 years of age2 Is the pulse rate greater than 99 beatsminndash13 Is the pulse oximetry reading 95 while the patient breathes
room air4 Is there a present history of hemoptysis5 Is the patient receiving exogenous estrogen6 Does the patient have a prior diagnosis of venous
thromboembolism (VTE)7 Has the patient had recent surgery or trauma (requiring
endotracheal intubation or hospitalization in the previous 4weeks)
8 Does the patient have unilateral leg swelling (visual observation ofasymmetry of the calves)
CHigh sensitivity (eg turbidimetric ELISA)
636 Annals of Emergency Medicine
Level B recommendations None specifiedLevel C recommendations In patients with an intermediate
retest probability for PE a negative quantitative D-dimerssay result may be used to exclude PE
Key wordsphrases for literature searches pulmonarymbolism fibrin fragment D sensitivity specificity D-dimerifferential diagnosis and variations and combinations of theey wordsphrases years 2001 through December 2009
This revision to the 2003 clinical policy1 focuses on quantitative-dimer tests that have become available to most hospital
aboratories across the United States The Clinical Policiesubcommittee on PE elected not to assess the evidence forualitative D-dimer tests (often used in point-of-care panels)ecause of problems with variability in interpretation and lowerensitivity reported in multiple studies62-65 However the onlyandomized clinical trial directly assessing the impact of a D-dimertrategy used a qualitative whole-blood agglutination testSimpliRED Agen Biomedical Ltd Brisbane Australia)66 In thisrial potential subjects suspected of having PE were first stratifiedccording to the Wells criteria and those with a low clinicalrobability and negative D-dimer test result were randomized toither no additional testing or VQ scanning Althoughnterpretation of results is limited due to early study closure thencidence of VTE during 6 months was similar among the 2 groups0182 versus 1185) Given that we were unable to identify anyther randomized controlled trials specifically designed to test thempact of a D-dimer strategy our recommendations are based onata from cohort studies and high-quality systematic reviews thatave been published since the original ACEP clinical policy1 Tovoid duplication cohort studies that were included in at least 1 ofhe systematic reviews are not reported in the Evidentiary Table
Class I systematic reviews assessing the test characteristics ofuantitative D-dimer tests in outpatient settings conclude that D-imer has excellent sensitivity (pooled sensitivity093 to 096) butnly moderate specificity (pooled specificity039 to 051)656768
lass I3542 and II 3769-75cohort studies that were not included inhese systematic reviews report similar results In patients with a lowretest probability (10) a negative ELISA or turbidimetric D-imer (LR-01) test result would be expected to decrease therobability of PE to approximately 1 These assumptions basedn the application of Bayesrsquo Theorem are supported by Class I35
lass II6973-75 and Class III38394676-79 studies that haveonsistently reported negative predictive values of approximately9 when D-dimer testing is applied to low-risk or ldquoPE unlikelyrdquoatient populations The American College of Physicians guidelinesn PE also support using D-dimer testing among low-risk patientsuspected of having PE8081
Despite consensus guidelines that recommend using D-dimeresting on patients with an intermediate pretest probability forE82 strong evidence supporting this approach is lacking Aetrospective analysis of 2 studies by Righini et al83 reportedero VTE events at 3-month follow-up for both low- andntermediate-risk groups however the upper limit for the 95
I was 1 for the low-probability group but extended up to
Volume June
hme
ipscea
na(td
caV
teponv2
tdad
hbfTgmstmIb
rrfidcma
Clinical Policy
5 for the intermediate-probability group Subsequent studiesthat have included intermediate pretest probability patientswithin their D-dimer strategy have either not reported resultsseparately737584 or have had too few patients in this subgroupto draw any firm conclusions777885
Given the relatively poor specificity of D-dimer testingvarious strategies have been suggested to limit the number offalse-positive tests that may lead to further unnecessarydiagnostic testing Retrospective subgroup analyses suggest thatD-dimer sensitivity remains fairly constant among varioussubpopulations but specificity decreases with certain comorbidconditions and advanced age678687 Two prospective studiesassessing the performance of D-dimer testing among cancerpatients suspected of having PE reported very low specificities(specificity018 to 021)8889 Pregnancy is also associated withincreasing concentrations of D-dimer particularly in womenbeyond the first trimester90 A restrictive approach to D-dimertesting whereby the elderly are excluded improves testspecificity8691 however this approach is unlikely to decreaseresource utilization since these patients would be expected to godirectly to some form of advanced imaging Adjusting the D-dimer test threshold based on the patientrsquos pretest probability orother variables (eg age) has been suggested as an alternativeapproach to improve the performance of D-dimertesting378792-94 Although raising the D-dimer test thresholdwould be expected to increase test specificity the associateddecrease in sensitivity may be unacceptable to most cliniciansand has not been prospectively studied95
Potential benefits of using a highly sensitive D-dimer as ascreening test include decreased cost and radiation exposurehowever if the test is ordered indiscriminately on patients withvery little or no risk for PE false-positive D-dimer results mayincrease the harms associated with unnecessary advancedimaging A formal decision analysis concluded that using D-dimer was not cost-effective if CT is readily available96
Although the authorsrsquo assumptions about the sensitivity andspecificity of quantitative D-dimer tests were consistent with thestudies included in the Evidentiary Table the authors state thattheir analysis was based on a patient suspected of having PEwithout other competing diagnoses96 It is rare in the EDsetting to have such a straightforward clinical presentation inwhich only 1 diagnosis is considered
Future research is needed for patients with an intermediatepretest probability of PE and to assess whether changing theD-dimer cutoff for different patient subgroups could improvespecificity without a clinically significant decrease in sensitivity
4 What is the role of the CT pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations For patients with a low or PE
unlikely (Wells score 4) pretest probability for PE who require
additional diagnostic testing (eg positive D-dimer result or p
Volume June
ighly sensitive D-dimer test not available) a negativeultidetector CT pulmonary angiogram alone can be used to
xclude PELevel C recommendations (1) For patients with an
ntermediate pretest probability for PE and a negative CTulmonary angiogram result in whom a clinical concern for PEtill exists and CT venogram has not already been performedonsider additional diagnostic testing (eg D-dimer lowerxtremity imaging VQ scanning traditional pulmonaryrteriography) prior to exclusion of VTE disease
(2) For patients with a high pretest probability for PE and aegative CT angiogram result and CT venogram has notlready been performed perform additional diagnostic testingeg D-dimer lower extremity imaging VQ scanningraditional pulmonary arteriography) prior to exclusion of VTEiseaseA negative highly sensitive quantitative D-dimer result in
ombination with a negative multidetector CT pulmonaryngiogram result theoretically provides a posttest probability ofTE less than 1
Key wordsphrases for literature searches x-ray computedomography CT spiral computed tomography pulmonarymbolism sensitivity specificity probability likelihoodulmonary angiogram angiography thromboembolismutcome follow-up recurrent morbidity mortality falseegative false positive prognosis treatment outcome andariations and combinations of the key wordsphrases years001 through December 2009The use of the spiral CT angiogram for the visualization of
he pulmonary vasculature and the evaluation of PE was firstescribed in 199297 A single detector rotated in a spiral fashiont fixed intervals collecting data to generate vascular imagesuring a single breath holdSince that time the technology of this diagnostic modality
as advanced dramatically Multidetector CT scanners now useetween 4 64 or more channels (detectors) and rotate at muchaster gantry speeds (04 seconds versus 1 second per rotation)hus an older-generation single-detector CT with a 1-secondantry speed captures 1 slice per second whereas a 16-channelultidetector CT scanner rotating at a gantry speed of 04
econds captures 40 slices per second98 This in addition tohinner collimation allows for faster image acquisition lessotion artifact and ultimately higher-resolution images
mproved image acquisition protocols and resolution areelieved to result in improved diagnostic performanceIn 1992 Remy-Jardin et al97 in a Class III investigation
eported sensitivities and specificities of 100 and 96espectively for a single-detector CT for detection of PE Thisnding led to eager acceptance of the spiral CT angiogram intoiagnostic algorithms in the hope of simplifying theomplicated diagnostic workup of PE Since this initial studyultiple accuracy and outcomes studies in addition to meta-
nalyses and systematic reviews have been published on the
erformance of the CT pulmonary angiogram Unfortunately
Annals of Emergency Medicine 637
ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

owEpDCiit
oVPirapeu
M
aaAsuasa
medeeraPUCeefwA
gecdra
Clinical Policy
ABSTRACTThis clinical policy from the American College of Emergency
Physicians is the revision of a 2003 clinical policy on theevaluation and management of adult patients presenting withsuspected pulmonary embolism (PE)1 A writing subcommitteereviewed the literature to derive evidence-basedrecommendations to help clinicians answer the following criticalquestions (1) Do objective criteria provide improved riskstratification over gestalt clinical assessment in the evaluation ofpatients with possible PE (2) What is the utility of thePulmonary Embolism Rule-out Criteria (PERC) in theevaluation of patients with suspected PE (3)What is the role ofquantitative D-dimer testing in the exclusion of PE (4) What isthe role of computed tomography pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE (5) Whatis the role of venous imaging in the evaluation of patients withsuspected PE (6) What are the indications for thrombolytictherapy in patients with PE Evidence was graded andrecommendations were given based on the strength of theavailable data in the medical literature
INTRODUCTIONIt is estimated that 650000 to 900000 individuals each year
have fatal or nonfatal acute pulmonary embolism (PE)2 and thatas many as 200000 people in the United States die each yearfrom PE3 Untreated PE can be rapidly fatal with the majorityof deaths occurring in the first hour34 Furthermore survivorsof undiagnosed PE can experience disabling morbidity frompulmonary hypertension5 andor postthrombotic syndrome6-8
Because there is a strong association between deep venousthrombosis (DVT) and PE it is difficult to discuss thediagnostic evaluation of one entity without discussing theother7 Approximately 50 of patients with documented DVThave perfusion defects on nuclear lung scanning andasymptomatic venous thrombosis is found in approximately40 of patients with confirmed PE6910
During the past decade there has been an explosion ofpublished research and development of new diagnosticmodalities and therapies relating to patients with suspected PEand DVT with greater than 1000 publications appearing inthe medical literature per year This current policy represents arevision of the 2003 American College of Emergency Physicians(ACEP) clinical policy on critical issues in the evaluation andmanagement of adult patients with suspected PE1 The 2003policy focused on 4 major areas of interest andor controversythat existed when the policy was formulated (1) Can a negativeD-dimer result exclude PE (2) When can ventilation-perfusion(VQ) scan alone or in combination with venousultrasonography andor D-dimer assay exclude PE (3) Canspiral computed tomography (CT) replace VQ scanning in thediagnostic evaluation of PE and (4) What are the indicationsfor thrombolytic therapy in patients with PE This currentpolicy focuses on 6 areas of interest andor controversy that have
developed or still exist since the 2003 policy was formulated A
Volume June
(1) Do objective criteria provide improved risk stratificationver general clinical assessment in the evaluation of patientsith possible PE (2) What is the utility of the Pulmonarymbolism Rule-out Criteria (PERC) in the evaluation ofatients with suspected PE (3)What is the role of quantitative-dimer testing in the exclusion of PE (4) What is the role ofT pulmonary angiogram of the chest as the sole diagnostic test
n the exclusion of PE (5) What is the role of venous imagingn the exclusion of PE and (6) What are the indications forhrombolytic therapy in patients with PE
This policy does not discuss VQ scanning in the evaluationf patients with suspected PE The authors do recognize thatQ scanning is used in the evaluation of patients with suspectedE in whom CT scan may be contraindicated11-13 Also with
ncreasing awareness of potential long-term effects of ionizingadiation exposure from repetitive CT scans there may bedditional subgroups of patients for whom a VQ scan may bereferred as the initial imaging modality because of decreasedxposure to radiation compared with CT scan13-17 Futurepdates of this policy may directly address these issues
ETHODOLOGYThis clinical policy was created after careful review and critical
nalysis of the medical literature Multiple searches of MEDLINEnd the Cochrane Library were performed To update the 2003CEP clinical policy all searches were limited to English-language
ources and human studies Specific key wordsphrases and yearssed in the searches are identified under each critical question Inddition relevant articles from the bibliographies of includedtudies and more recent articles identified by committee membersnd peer reviewers are included
The reasons for developing clinical policies in emergencyedicine and the approaches used in their development have been
numerated18 This policy is a product of the ACEP clinical policyevelopment process including expert review and is based on thexisting literature when literature was not available consensus ofmergency physicians was used Expert review comments wereeceived from individual emergency physicians and cardiologistsnd from individual members of the American College of Chesthysicians American College of Radiology ACEPrsquos Emergencyltrasound Section and ACEPrsquos Quality and Performanceommittee Their responses were used to further refine and
nhance this policy however their responses do not implyndorsement of this clinical policy Clinical policies are scheduledor revision every 3 years however interim reviews are conductedhen technology or the practice environment changes significantlyCEP is the funding source for this clinical policy
All articles used in the formulation of this clinical policy wereraded by at least 2 subcommittee members for strength ofvidence and classified by the subcommittee members into 3lasses of evidence on the basis of the design of the study withesign 1 representing the strongest evidence and design 3epresenting the weakest evidence for therapeutic diagnosticnd prognostic clinical reports respectively (Appendix A)
rticles were then graded on 6 dimensions thought to be most
Annals of Emergency Medicine 629
oi
rettmc
p(
p
aas
C1ow
gwp
pdGaD
Eaeltswccpoa
O
i
Clinical Policy
relevant to the development of a clinical guideline blindedversus nonblinded outcome assessment blinded or randomizedallocation direct or indirect outcome measures (reliability andvalidity) biases (eg selection detection transfer) externalvalidity (ie generalizability) and sufficient sample size Articlesreceived a final grade (Class I II III) on the basis of apredetermined formula taking into account design and qualityof study (Appendix B) Articles with fatal flaws were given anldquoXrdquo grade and not used in formulating recommendations in thispolicy Evidence grading was done with respect to the specificdata being extracted and the specific critical question beingreviewed Thus the level of evidence for any one study may varyaccording to the question and it is possible for a single article toreceive different levels of grading as different critical questionsare answered Question-specific level of evidence grading may befound in the Evidentiary Table included online (available athttpwwwannemergmedcom)
Clinical findings and strength of recommendations regardingpatient management were then made according to the followingcriteria
Level A recommendations Generally accepted principles forpatient management that reflect a high degree of clinicalcertainty (ie based on strength of evidence Class I oroverwhelming evidence from strength of evidence Class IIstudies that directly address all of the issues)
Level B recommendations Recommendations for patientmanagement that may identify a particular strategy or range ofmanagement strategies that reflect moderate clinical certainty (iebased on strength of evidence Class II studies that directly addressthe issue decision analysis that directly addresses the issue or strongconsensus of strength of evidence Class III studies)
Level C recommendations Other strategies for patientmanagement that are based on Class III studies or in the absence ofany adequate published literature based on panel consensus
There are certain circumstances in which the recommendationsstemming from a body of evidence should not be rated as highly asthe individual studies on which they are based Factors such asheterogeneity of results uncertainty about effect magnitude andconsequences and publication bias among others might lead tosuch a downgrading of recommendations
When possible clinically oriented statistics (eg likelihoodratios [LRs] number needed to treat) will be presented to helpthe reader better understand how the results can be applied tothe individual patient For a definition of these statisticalconcepts see Appendix C
This policy is not intended to be a complete manual on theevaluation and management of patients with suspected PE butrather a focused examination of critical issues that have particularrelevance to the current practice of emergency medicine
It is the goal of the Clinical Policies Committee to providean evidence-based recommendation when the medical literatureprovides enough quality information to answer a criticalquestion When the medical literature does not contain enough
quality information to answer a critical question the members p
630 Annals of Emergency Medicine
f the Clinical Policies Committee believe that it is equallymportant to alert emergency physicians to this fact
Recommendations offered in this policy are not intended toepresent the only diagnostic and management options that themergency physician should consider ACEP clearly recognizeshe importance of the individual physicianrsquos judgment Ratherhis guideline defines for the physician those strategies for whichedical literature exists to provide support for answers to the
rucial questions addressed in this policyScope of Application This guideline is intended for
hysicians working in hospital-based emergency departmentsEDs) or ED-based observation centers
Inclusion Criteria This guideline is intended for adultatients presenting to the ED with suspected PE
Exclusion Criteria This guideline is not intended toddress the care of patients with PE in the presence of cardiacrrest or pregnancy patients with absence of symptomsuggestive of PE or pediatric patients
RITICAL QUESTIONS Do objective criteria provide improved risk stratificationver gestalt clinical assessment in the evaluation of patientsith possible PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Either objective criteria or
estalt clinical assessment can be used to risk stratify patientsith suspected PE There is insufficient evidence to support thereferential use of one method over another
Level C recommendations None specified
Key wordsphrases for literature searches risk stratificationulmonary embolism ED emergency service risk assessmentiagnostic strategies Wells criteria Wicki criteria Kline criteriaeneva score revised Geneva score PISA model and variations
nd combinations of the key wordsphrases years 2000 throughecember 2009This critical question focuses on pretest probability assessment
stimation of pretest probability is imperative for the properpplication of any diagnostic test This general principle becomesven more important for PE because it is a common but potentiallyethal disease when left undiagnosed and untreated Unfortunatelyhe classic presentation of PE is rare and physicians must makeome sort of assessment about whether to evaluate patients for PEhen they present with symptoms such as unexplained dyspnea
hest pain hemoptysis palpitations syncope back pain and otherommonplace symptoms that have been associated with PE Pretestrobability assessment in PE can be estimated in 2 general waysbjective criteria (clinical decision rules) or gestalt clinicalssessment (implicit approach)
bjective Criteria (Clinical Decision Rules)Clinical decision rules are a form of objective criteria that are
ntended to provide more accurate and reproducible measure of
retest probability assessment than the overall gestalt clinical
Volume June
W
omesaP
TaewPprCrtp
V
RAPRASUHCH
P
S
R041S
025
03
tnaacv
Clinical Policy
impression that depends on the physicianrsquos expertise and clinicalexperience Such rules can be derived and validated They alsocan be compared to each other and refined over time Severalclinical decision rules have been developed for use in patientswith suspected PE The most commonly used methods are (1)Geneva score19-21 (2) Wells (Canadian) score22 (3) Kline(Charlotte) criteria23 and (4) Pisa model2425
Geneva ScoreThe original Geneva score as described by Wicki et al19 in
2001 is a Class II study that was performed at a single hospitalin Switzerland and consists of a clinical score ranging from 0 to16 points derived from 8 parameters relating to risk factorsclinical signs blood gas analysis and chest radiographProbability of PE in patients defined as low- (0 to 4 points)intermediate- (5 to 8 points) and high- (9 points) risk was10 38 and 81 respectively Multiple Class III studieshave since validated the usefulness of the Geneva score in riskstratification of patients with suspected PE26-31
Because of the reliance of the original Geneva score on roomair blood gas analysis and chest radiograph interpretation LeGal et al20 in a Class II study retrospectively analyzed datafrom 2 previous multicenter clinical investigations to develop ascore independent of diagnostic testing The subsequent revisedGeneva score ranged from 0 to 25 points and was derived from8 parameters relating to risk factors symptoms and clinicalsigns (Table 1) In the validations set probability of PE in low-(score 0 to 3) intermediate- (score 4 to 10) and high-risk (score11) patients was 8 29 and 74 respectively To dateonly one Class II investigation has validated the revised Genevascore32
One of the difficulties of the revised Geneva score is thatdifferent elements have different weights making it potentiallymore difficult to apply in the clinical setting (Table 1) As a resultKlok et al21 in a Class II study reanalyzed the same populationand developed the simplified revised Geneva score that uses theidentical 8 parameters of the revised Geneva score (Table 1) Onepoint is assigned to each parameter except for pulse rate greaterthan or equal to 95 beatsmin which results in an additional pointProbability of PE in patients defined as low- (0 to 1 point)intermediate- (2 to 4 points) and high- (5 to 7 points) risk was 829 and 64 respectively The investigators also divided thepatients into the dichotomous group of PE unlikely (0 to 2 pointsprobability of PE 115) and PE likely (3 to 7 points probabilityof PE 351) to select a patient population safe for use of D-dimertesting for exclusion of PE Of the 330 patients with a PE unlikelyscore and a negative D-dimer result no patient was diagnosed ashaving venous thromboembolic disease on presentation or on 3-month follow-up Receiver operating characteristic (ROC) curveanalysis revealed no differences in diagnostic performance of therevised Geneva score (area under ROC curve 075 95 confidenceinterval [CI] 071 to 078) compared with the simplified revised
Geneva score (area under ROC curve 074 95 CI 070 to 077) a
Volume June
ells ScoreThe original Wells study was a Class III investigation in use
f a clinical model to risk stratify 1239 patients in low-oderate- and high-risk groups33 The investigators used
vidence from the published literature to establish a risk-tratification model by consensus The risk model initiallyssessed patients based on signs and symptoms as ldquotypicalrdquo forE ldquoatypicalrdquo for PE or ldquosevererdquo Physicians then made an
able 1 Revised Geneva score as described by Le Gal et al20
nd the simplified revised Geneva score as described by Klokt al21 for assessment of pretest probability of PE Reprintedith permission Copyright copy American College of Physiciansublisher Le Gal G Righini M Roy P-M et al Prediction ofulmonary embolism in the emergency department theevised Geneva score Ann Intern Med 2006144165-171opyright copy 2008 American Medical Association All rightseserved Klok FA Mos IC Nijkeuter M et al Simplification ofhe revised Geneva score for assessing clinical probability ofulmonary embolism Arch Intern Med 20081682131-2136
ariable
Points
RevisedGeneva
Simplified RevisedGeneva
isk factorsge 65 y 1 1revious DVTPE 3 1ecent surgeryfracture (4 wk) 2 1ctive malignancy 2 1ymptomsnilateral lower-limb pain 3 1emoptysis 2 1linical signseart rate75ndash94 beatsmin 3 195 beatsmin 5 2
ain on lower-limb deep venouspalpation and unilateral edema
4 1
core RangeProbability of PE
(95 CI)Patients WithThis Score
Interpretationof Risk
evised Geneva Score20
ndash3 79 (50ndash121) 370 Lowndash10 285 (246ndash328) 574 Moderate1ndash25 737 (610ndash834) 55 Highimplified Revised Geneva Score21
Traditional interpretationndash1 77 (52ndash108) 360 Lowndash4 294 (259ndash331) 60 Moderatendash7 643 (480ndash785) 40 HighAlternative interpretation
ndash2 129 (105ndash157) 649 PE unlikelyndash7 416 (365ndash468) 351 PE likely
The original table from Klok et al21 lists 1 point for heart rate 95 beatsmin buthe assessment of score states ldquo[b]ecause of the weight of heart rate in the origi-al score we attributed 1 point to a heart rate between 75 and 94 beatsmin andn additional point for a heart rate of 95 beatsmin or morerdquo Thus a patient withheart rate of 100 beatsmin would receive a total of 2 points (personal communi-
ation F A Klok MD PhD Department of General Internal Medicine Leiden Uni-ersity Medical CenterBronovo Hospital Den Haag May 2010)
ssessment about whether an ldquoalternative diagnosis that was as
Annals of Emergency Medicine 631
11pw1v9ts
vopphedP(
vHaarcp
K
csephsrwwaut(thps9Cet1IL
Clinical Policy
likely as or more likely than PErdquo to further subdivide thepatients into 10 possible outcomes These outcomes were thendivided into low- moderate- and high-risk groups Rates of PEin patients with low moderate and high risk were 34278 and 784 respectively Although this modelperformed well the algorithmic approach was not suitable to beused as an objective risk-stratification tool
Wells et al22 subsequently performed a retrospective analysisof the data used in the original study to develop a simple scoringsystem that could be used in conjunction with D-dimer for theevaluation of patients with suspected PE (Table 2) Usingregression techniques a risk-stratification model consisting of 7variables was created that classified patients as having lowmoderate and high probability of PE In addition analternative interpretation system was developed in which thepatients were classified into the dichotomist groups ldquoPEunlikelyrdquo and ldquoPE likelyrdquo to identify a group of patients forwhom a negative D-dimer test would result in a PE rate of 2If the D-dimer result was negative the rate of PE in patientsdesignated PE unlikely (score 0 to 4) was 22 in the derivationset and 17 in the validation set
This model was subsequently prospectively validated in aClass II investigation in a cohort of 4 EDs at tertiary carehospitals in Canada34 The initial pretest probabilities weredetermined by the clinical model to be low in 57 of patientsmoderate in 36 of patients and high in 7 of patientsIncluding follow-up events PE was diagnosed in 13 of
Table 2 Wells Canadian Score for assessment of pretestprobability for PE22 Reprinted with permission Copyright copySchattauer Publisher Wells PS Anderson DR Rodger M etal Derivation of a simple clinical model to categorize patientsprobability of pulmonary embolism increasing the modelsutility with the SimpliRED D-dimer Thromb Haemost 200083416-420
Criteria Points
Suspected DVT 30An alternative diagnosis is less likely than PE 30Heart rate 100 beatsminute 15Immobilization or surgery in the previous 4 weeks 15Previous DVTPE 15Hemoptysis 10Malignancy (on treatment treated in the last 6
months or palliative)10
Score RangePoints Probability of PE ()
With ThisScore
Interpretationof Risk
Traditionalinterpretation
0ndash1 36 (20ndash59) 403 Low2ndash6 205 (170ndash241) 526 Moderate6 667 (543ndash776) 71 HighAlternate
interpretation0ndash4 78 (59ndash101) 715 PE unlikely4 407 (349ndash465) 285 PE likely
patients with low pretest probability (95 CI 05 to 27) d
632 Annals of Emergency Medicine
62 of patients with moderate pretest probability (95 CI25 to 206) and in 406 of patients with high pretestrobability (95 CI 287 to 537) Of the 437 patientsith a negative D-dimer result and low clinical probability onlydeveloped PE during follow-up giving a negative predictive
alue for the use of the clinical model with D-dimer testing of95 (95 CI 991 to 100) No information is given inhis investigation about performance of the alternative scoringystem of ldquoPE unlikelyrdquo and ldquoPE likelyrdquo
A Class II investigation by the Christopher Study Investigatorsalidated the utility of the dichotomized alternative scoring systemf ldquoPE unlikelyrdquo versus ldquoPE likelyrdquo35 This study was a multicenterrospective cohort of 3306 patients A total of 2206 (667)atients were classified as PE unlikely Of these 1057 patients alsoad a negative D-dimer result and PE was considered to have beenxcluded On 3-month follow-up 5 (05) patients received aiagnosis of venous thromboembolic disease with no deaths In theE likely subgroup PE was diagnosed on CT scan in 674 patients204)
Multiple Class II3637and Class III studies28-3138-43 havealidated the usefulness of the Wells score in risk stratificationowever a major criticism of the Wells score is that it is not truly
n objective criterion because it contains the subjective variable ldquoanlternative diagnosis is less likely than PErdquo This variable in essenceepresents physician judgment override of the objectiveomponents of the score because it is worth 3 points and thuslaces the patient in the intermediate-risk group19324445
line RuleKline et al23 in a Class II study derived a decision rule to
reate a binary partition of ED patients with suspected PE toelect patients for whom a negative D-dimer result reliablyxcluded the presence of PE (Figure) Nine-hundred thirty-fouratients were studied at 7 urban EDs in the United States Theistory and physical process occurred prospectively beforetandard imaging to look for recognized symptoms signs andisk factors associated with PE Selected variables were analyzedith multivariate logistic analysis to determine factors associatedith PE A decision rule was then constructed to categorize
pproximately 80 of ED patients as being able to safelyndergo D-dimer testing Six variables were used to constructhe decision rule Unsafe patients had either a shock indexpulse ratesystolic blood pressure more than 10) or age greaterhan 50 years together with any of the following unexplainedypoxemia (arterial blood oxygen saturation [SaO2] 95 norevious lung disease) unilateral leg swelling recent majorurgery or hemoptysis These criteria were met by 197 (21) of34 patients Of these 197 patients 83 had PE (421 95I 355 to 496) When these 197 ldquounsaferdquo patients were
xcluded the probability of PE was significantly decreased inhe remaining 737 (79) ldquosaferdquo patients to 133 (95 CI09 to 159) Assuming use of an Enzyme-Linkedmmunosorbent Assay (ELISA) D-dimer assay with a negativeR of 007 the use of the Kline rule in conjunction with D-
imer testing would decrease the posttest probability of PE to
Volume June
eurgmdpmpiovoirpeh(a
wa3osPrsw2(
C
hcnCp
Pspwalps
cWaP
Clinical Policy
approximately 1 The authors concluded that these criteriacan permit safe D-dimer testing in the majority of ED patientswith suspected PE
There are no prospective outcome studies validating the useof the Kline rule in conjunction with D-dimer but 1 Class IIIstudy demonstrated a 21 decrease in CT scanning when theyinstituted this protocol46
Pisa ModelThe original Pisa investigation is a Class II study consisting
Figure Kline decision rule for excluding PE23 Reprintedfrom Annals of Emergency Medicine 39 Kline JA NelsonRD Jackson RE et al Criteria for the safe use of D-dimertesting in emergency department patients with suspectedpulmonary embolism a multicenter US study 144-1522002 Copyright from the American College of EmergencyPhysicians [2002]
Flow diagram demonstrating the Kline decision rule inselecting patients in whom D-dimer assay less than 500 ngml can reliably rule out PE This decision rule splits thepatients into 2 groups four fifths of whom are eligible for D-dimer testing (ldquosaferdquo patients with pretest probability of PE of133) and one fifth of whom are ineligible for D-dimertesting (ldquounsaferdquo patients with pretest probability of 421)
of 1100 consecutive patients with suspected PE who were W
Volume June
valuated at a single hospital in Pisa Italy24 All patientsnderwent a detailed clinical history physical examinationigorous interpretation of ECG and chest radiograph and bloodas measurements Using logistic regression techniques aathematical model for predicting probability of PE was
eveloped Probability was categorized as low (10robability of PE) intermediate (10 to 50 probability)oderately high (50 to 90 probability) and high (90
robability) Ten characteristics were associated with anncreased risk of PE male sex older age history of DVT acutenset dyspnea chest pain hemoptysis ECG signs of rightentricular overload radiographic signs of oligemia amputationf the hilar artery and pulmonary consolidations suggestive ofnfarction Five characteristics were associated with a decreasedisk previous cardiovascular or pulmonary disease feverulmonary consolidation other than infarction and pulmonarydema With this model 432 patients (39) were rated asaving low probability (4 PE) 283 (26) as intermediate22 PE) 72 (7) as moderately high probability (74 PE)nd 313 (28) as high probability (98 PE)
In the original Pisa model the highest regression coefficientsere for the chest radiograph findings (oligemia 386
mputation of hilar artery 392 and pulmonary infarction55) Because of the heavy reliance of the original Pisa modeln advanced chest radiograph interpretation skills beyond thekill level of the average physician Miniati et al25 refined theisa model in the same patient population after excluding chestadiograph from the final equation (Table 3) In the validationet of this Class II investigation the prevalence of PE was 2hen the predicted clinical probability was low (0 to 10)8 when moderate (11 to 50) 67 when substantial51 to 80) and 94 when high (81 to 100)
omparative Studies of Objective CriteriaThere are two Class II3247 and 3 Class III283031 studies that
ave evaluated performance of the various objective criteria Inomparing the Geneva score to the Wells score 3 studies foundo significant differences in performance though the study byhagnon et al28 suggested that the Geneva score overridden byhysician judgment may be more accurate283132
Miniati et al30 compared the Geneva score Wells score andisa model in 215 patients with suspected PE and foundtatistically significant differences in performance of the 3retest probability assessment tools Areas under the ROC curveere 054 075 and 094 for the Geneva score Wells score
nd Pisa model respectively However findings in this study areimited because of small sample size and the PE rate in thisatient population was extremely high (43) indicatingignificant patient selection bias
Runyon et al47 compared the Wells score with the Klineriteria in 2603 patients with a PE prevalence of 58 The
ells score identified 73 of patients as low risk (score 2)nd the Kline criteria identified 88 of patients as low risk TheE rates in these low-risk patients were 30 and 42 for the
ells and Kline criteria respectively
Annals of Emergency Medicine 633
wadt16gIp
oipgaoiRr(3s
ppap1ssi3ldquotrlcbp
pIgsi
L
r
ypP
Clinical Policy
Gestalt Clinical AssessmentGestalt clinical assessment is an unstructured (nonruled based)
estimate of the pretest probability of disease It is based on theclinicianrsquos training clinical experience and judgment Thisapproach has also been described as implicit in nature Theclinician using this approach surmises an overall impression of thepretest probability of PE and applies that impression to the decisionabout whether to pursue the diagnosis through objective testing
The Prospective Investigation of Pulmonary EmbolismDiagnosis (PIOPED) study was a prospective multi-institutioninvestigation designed to evaluate various conventional methodsfor diagnosing PE48 The PIOPED study is the first major studyreporting gestalt assessment As one element of the study the
Table 3 Regression coefficients and odds ratio for the Pisamodel as described by Miniati et al25 for estimatingprobability of pulmonary embolism according to clinical andECG findings Calculation of the clinical probability ofpulmonary embolism is performed as follows (1) Add all thecoefficients that apply to a given patient and the constantndash343 to obtain a sum score (2) the probability of pulmonaryembolism equals [1exp(ndashsum)]ndash1 Reprinted with permissionof the American Thoracic Society Copyright copy AmericanThoracic Society Miniati M Bottal M Monti S et al Simpleand accurate prediction of the clinical probability of pulmonaryembolism American Journal of Respiratory and Critical CareMedicine 2008178290-294 Official journal of the AmericanThoracic Society Diane Gern Publisher
Predictor Coefficient Odds Ratio 95 CI
Age y57ndash67 080 223 137ndash36368ndash74 087 238 141ndash40175 114 311 182ndash532Male sex 060 182 127ndash261Risk factorsImmobilization 042 153 108ndash215Deep venous thrombosis (ever) 064 190 123ndash295Preexisting diseasesCardiovascular ndash051 060 041ndash088Pulmonary ndash089 041 024ndash072SymptomsDyspnea (sudden onset) 200 738 518ndash1051Orthopnea ndash151 022 005ndash093Chest pain 101 274 193ndash388Fainting or syncope 066 193 125ndash298Hemoptysis 093 252 119ndash535SignsLeg swelling (unilateral) 080 223 135ndash370Fever 38degC (1004degF) ndash147 023 013ndash040Wheezes ndash120 030 014ndash066Crackles ndash061 054 035ndash083ElectrocardiogramAcute cor pulmonale 196 711 466ndash1087Constant ndash343
One or more of the following ECG abnormalities S1Q3T3 S1S2S3 negativeT waves in right precordial leads transient right bundle branch blockpseudoinfarction
clinicianrsquos assessment of the likelihood of PE from 0 to 100 t
634 Annals of Emergency Medicine
as recorded for 887 patients and was compared with PE statuss determined by angiogram and follow-up information Forata analysis low risk was considered pretest probability of 0o 19 intermediate risk 20 to 79 and high risk 80 to00 PE subsequently was diagnosed in 92 299 and78 of patients in the low- intermediate- and high-riskroups respectively Since the PIOPED study multiple ClassII studies have validated the usefulness of gestalt assessment ofretest probability in evaluating patients with suspected PE49-53
There have been several comparative studies of gestalt versusbjective criteria In a Class II study investigating potentialmpact of adjusting the D-dimer threshold Kabrhel et al37
rospectively performed pretest probability assessment usingestalt versus the Wells score in 7940 patients from 10cademic centers By gestalt pretest probability assessment 68f patients were low risk (15 pretest probability PE) 26ntermediate risk (15 to 40) and 6 high risk (40)ates of PE in these 3 subgroups were 3 10 and 33
espectively By the Wells score 69 of patients were low riskWells score 2) 28 intermediate (Wells score 2 to 6) and high risk (Wells score 6) Rates of PE in these 3ubgroups were 3 13 and 36 respectively
Sanson et al41 in a Class III study investigated pretestrobability assessment of gestalt versus the Wells score in 517atients with a 31 PE rate By gestalt pretest probabilityssessment 14 of patients were low risk (20 pretestrobability PE) 67 intermediate risk (20 to 80) and9 high risk (80 to 100) Rates of PE in these 3ubgroups were 19 29 and 46 respectively By the Wellscore 36 of patients were low risk (Wells score 2) 63ntermediate (Wells score 2 to 6) and 2 high risk (Wells score
6) Rates of PE in these 3 subgroups were 28 30 and8 respectively The authors conclude that both methodsalthough comparable perform disappointingly in categorizinghe pretest probability in patients with suspected PErdquo The highate of patients categorized as having intermediate risk and theow rate of patients categorized as having low risk in this studyompared with other studies suggest significant patient selectionias that may account for the poor performance in pretestrobability assessment by these 2 methods
Runyon et al47 in a Class II study compared gestalt pretestrobability assessment with the Wells criteria and the Kline rulen the low-risk group rate of PE was 26 30 and 42 forestalt Wells and Kline rule respectively Gestalt and Wellscore also were equivalent in pretest probability assessment forntermediate- and high-risk patients
imitationsSeveral issues concerning performance of clinical decision
ules and gestalt assessment have been raised in the literature(1) Interrater reliability Nordenholtz et al54 compared third-
ear emergency medicine resident and attending emergencyhysician interrater reliability for 271 patients with suspectedE Specific elements of the Wells and Kline risk-stratification
ools were studied Interrater agreement was concluded to be
Volume June
ea2
sdm2cditaupAatapsmawbsPkc
cpoby
P8wTeao3plnc3sr
Clinical Policy
moderate for DVT symptoms (054) immobilization(041) unexplained hypoxia (058) and PE more likelythan alternative diagnosis (05) good for hemoptysis(076) and very good for previous DVT (090)malignancy (087) and tachycardia (094) Runyon et al47
in a large single hospital study involving a subset of 154 patientsfound only moderate interrater agreement for gestalt clinicalassessment of low probability (06) and Wells score less than 2(047) and very good for Kline rule ldquosaferdquo (085)
(2) Clinical experience as a factor in the determination ofpretest probability of PE Accurate determination of the pretestprobability of PE appeared to trend with clinical experienceHowever the authors concluded that difference in accuracybetween the inexperienced and experienced physicians is notsufficiently large to distinguish between the 2 when determiningwhether clinical gestalt or a clinical prediction rule should beused to determine the pretest probability of PE55
Iles et al44 performed a survey to investigate whether numberof years since graduation from medical school affected pretestprobability score for the Geneva Wells and gestalt pretestprobability assessment The Geneva score was found to be themost consistent method of determining pretest probabilityGestalt assessment was inversely proportional to clinicalexperience suggesting that as physicians gain experience theyrecognize the difficulties in ruling out PE and are reluctant toexclude it on clinical grounds
(3) Knowledge and use of the rules Runyon et al56 surveyedemergency medicine clinicians and found that only half of allclinicians reporting familiarity with the rules use them in morethan 50 of applicable cases Spontaneous recall of the ruleswas low to moderate
ConclusionBoth objective criteria and gestalt assessment appear to
perform equally well for patients with suspected PE With theadvent of electronic charting future studies need to beperformed investigating the use of computer support aids infacilitating pretest probability assessment Studies also need tobe performed investigating use of pretest probability assessmentto guide subsequent diagnostic testing Finally studies need tobe performed to clarify the definitions of low- intermediate-and high-risk groups especially for gestalt assessment in whichstudies have used pretest probabilities ranging from 20 to80 as definition for intermediate probability
2 What is the utility of the PERC in the evaluation ofpatients with suspected PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations In patients with a low pretest
probability for suspected PE consider using the PERC toexclude the diagnosis based on historical and physical
examination data alone a
Volume June
Level C recommendations None specified
Key wordsphrases for literature searches PERC pulmonarymbolism rule-out criteria block rule pulmonary embolismnd variations and combinations of the key wordsphrases years000 through December 2009In 2004 Kline et al57 published a Class II prospective
tudy deriving clinical criteria to prevent unnecessaryiagnostic testing in ED patients with suspected PE In thisulticenter study with 3148 patients in a derivation cohort
1 descriptive variables relevant to the diagnosis of PE wereollected The primary outcome variable was the EDiagnosis of PE using a composite criterion standard
ncluding 90-day follow-up The overall prevalence of venoushromboembolism (VTE) was 11 Logistic regressionnalysis with stepwise backwards elimination of variables wassed to identify criteria that could predict a patientopulation estimated to have a prevalence of disease of 18t or below this low pretest probability of disease theuthors proposed that no further laboratory or radiographicesting would be needed to exclude the diagnosis of PElthough this threshold which was based on a previouslyublished method for calculating testing thresholds58 hasubsequently been more accurately estimated to be 14 by aore recent decision analytic model balancing the benefits
nd costs of using the PERC59 After their analysis 8 variablesere identified age younger than 50 years pulse rate less than 100eatsmin SaO2 greater than 94 (at sea level) no unilateral legwelling no hemoptysis no recent trauma or surgery no previousE or DVT and no hormone use These criteria have since becomenown as the PERC When all criteria are met a patient isonsidered to be PERC negative
In this same study the authors went on to internally validate theriteria in a separate patient cohort57 When applied to 1427atients considered to be low risk for PE by gestalt assessment 25f patients were PERC negative The criteria when considered toe a diagnostic test had 96 sensitivity and 27 specificityielding a LR- of 015 and a 14 false-negative rate
In 2008 Kline et al60 published a Class II validation study of theERC (Table 4) This multicenter prospective study enrolled138 patients Although limited by the number of eligible patientsho were not enrolled the authors made attempts to address thishe outcome measures were similar to those of the original study
xcept for follow-up occurring at 45 days as opposed to 90 daysnd the overall prevalence of VTE being 69 Sixty-seven percentf patients were classified as low risk by clinical gestalt and of these07 were PERC negative This equated to 204 of enrolledatients The sensitivity specificity and LR- for the PERC in the
ow-risk cohort were 947 219 and 012 respectively Ofote 35 of enrolled patients were PERC negative but notonsidered to be low risk by clinical gestalt This subgroup had a1 prevalence of VTE Although outcomes on this specificubgroup were not reported not all PERC negative patients are lowisk and the rulersquos applicability in these patients is unknown The
uthors concluded that the PERC could be used in combination
Annals of Emergency Medicine 635
pa
edk
DlSqbsrs(tapeii(oidhat
qdoCtpdpoCc9pos
tPrzi
Clinical Policy
with a low pretest probability to identify very low-risk patients forwhom the diagnosis of PE can be reliably excluded based onhistorical and physical examination data alone
In 2008 Wolf et al61 published a small Class III externalvalidation of the PERC This study was a post hoc analysis ofprospectively collected data on 120 consecutive ED patientswith a suspicion of PE The original database contained allPERC variables Outcome measures used were similar to thoseof the original study yielding a 12 prevalence of PE Whentheir entire patient population is considered regardless ofpretest probability the sensitivity and specificity were 100 and16 respectively When only the patients with low pretestprobability as defined by Wells Criteria are considered thespecificity increased to 22 The authors concluded that thePERC may identify a cohort of patients with suspected PE forwhom diagnostic testing beyond history and physicalexamination is not indicated
In each of the above 3 clinical studies even though patient datawere collected prospectively the application of the PERC rule wasperformed retrospectively As such there is no prospective outcomestudy of the use of the PERC rule for clinical decisionmaking Thislimits the strength of recommendations that can be made based onthe available evidence Future research should focus on the clinicalapplication of the PERC rule with measurement of acceptedoutcomes
3 What is the role of quantitative D-dimer testing in theexclusion of PE
Patient Management RecommendationsLevel A recommendations In patients with a low pretest
probability for PE a negative quantitative D-dimer assay resultcan be used to exclude PE
Table 4 The Pulmonary Embolism Rule Out Criteria (PERC)
The PERC criteria negative (PERCndash) require the clinician to answer noto the 8 questions below60 If a patient is low risk by gestaltimpression and PERCndash the posttest probability of venousthromboembolism is 2 Reprinted with permission Copyright copyJohn Wiley amp Sons Ltd Publisher Kline JA Courtney DM KabrhelC et al Prospective multicenter evaluation of the pulmonaryembolism rule-out criteria J Thromb Haemost 20086772-780
1 Is the patient older than 49 years of age2 Is the pulse rate greater than 99 beatsminndash13 Is the pulse oximetry reading 95 while the patient breathes
room air4 Is there a present history of hemoptysis5 Is the patient receiving exogenous estrogen6 Does the patient have a prior diagnosis of venous
thromboembolism (VTE)7 Has the patient had recent surgery or trauma (requiring
endotracheal intubation or hospitalization in the previous 4weeks)
8 Does the patient have unilateral leg swelling (visual observation ofasymmetry of the calves)
CHigh sensitivity (eg turbidimetric ELISA)
636 Annals of Emergency Medicine
Level B recommendations None specifiedLevel C recommendations In patients with an intermediate
retest probability for PE a negative quantitative D-dimerssay result may be used to exclude PE
Key wordsphrases for literature searches pulmonarymbolism fibrin fragment D sensitivity specificity D-dimerifferential diagnosis and variations and combinations of theey wordsphrases years 2001 through December 2009
This revision to the 2003 clinical policy1 focuses on quantitative-dimer tests that have become available to most hospital
aboratories across the United States The Clinical Policiesubcommittee on PE elected not to assess the evidence forualitative D-dimer tests (often used in point-of-care panels)ecause of problems with variability in interpretation and lowerensitivity reported in multiple studies62-65 However the onlyandomized clinical trial directly assessing the impact of a D-dimertrategy used a qualitative whole-blood agglutination testSimpliRED Agen Biomedical Ltd Brisbane Australia)66 In thisrial potential subjects suspected of having PE were first stratifiedccording to the Wells criteria and those with a low clinicalrobability and negative D-dimer test result were randomized toither no additional testing or VQ scanning Althoughnterpretation of results is limited due to early study closure thencidence of VTE during 6 months was similar among the 2 groups0182 versus 1185) Given that we were unable to identify anyther randomized controlled trials specifically designed to test thempact of a D-dimer strategy our recommendations are based onata from cohort studies and high-quality systematic reviews thatave been published since the original ACEP clinical policy1 Tovoid duplication cohort studies that were included in at least 1 ofhe systematic reviews are not reported in the Evidentiary Table
Class I systematic reviews assessing the test characteristics ofuantitative D-dimer tests in outpatient settings conclude that D-imer has excellent sensitivity (pooled sensitivity093 to 096) butnly moderate specificity (pooled specificity039 to 051)656768
lass I3542 and II 3769-75cohort studies that were not included inhese systematic reviews report similar results In patients with a lowretest probability (10) a negative ELISA or turbidimetric D-imer (LR-01) test result would be expected to decrease therobability of PE to approximately 1 These assumptions basedn the application of Bayesrsquo Theorem are supported by Class I35
lass II6973-75 and Class III38394676-79 studies that haveonsistently reported negative predictive values of approximately9 when D-dimer testing is applied to low-risk or ldquoPE unlikelyrdquoatient populations The American College of Physicians guidelinesn PE also support using D-dimer testing among low-risk patientsuspected of having PE8081
Despite consensus guidelines that recommend using D-dimeresting on patients with an intermediate pretest probability forE82 strong evidence supporting this approach is lacking Aetrospective analysis of 2 studies by Righini et al83 reportedero VTE events at 3-month follow-up for both low- andntermediate-risk groups however the upper limit for the 95
I was 1 for the low-probability group but extended up to
Volume June
hme
ipscea
na(td
caV
teponv2
tdad
hbfTgmstmIb
rrfidcma
Clinical Policy
5 for the intermediate-probability group Subsequent studiesthat have included intermediate pretest probability patientswithin their D-dimer strategy have either not reported resultsseparately737584 or have had too few patients in this subgroupto draw any firm conclusions777885
Given the relatively poor specificity of D-dimer testingvarious strategies have been suggested to limit the number offalse-positive tests that may lead to further unnecessarydiagnostic testing Retrospective subgroup analyses suggest thatD-dimer sensitivity remains fairly constant among varioussubpopulations but specificity decreases with certain comorbidconditions and advanced age678687 Two prospective studiesassessing the performance of D-dimer testing among cancerpatients suspected of having PE reported very low specificities(specificity018 to 021)8889 Pregnancy is also associated withincreasing concentrations of D-dimer particularly in womenbeyond the first trimester90 A restrictive approach to D-dimertesting whereby the elderly are excluded improves testspecificity8691 however this approach is unlikely to decreaseresource utilization since these patients would be expected to godirectly to some form of advanced imaging Adjusting the D-dimer test threshold based on the patientrsquos pretest probability orother variables (eg age) has been suggested as an alternativeapproach to improve the performance of D-dimertesting378792-94 Although raising the D-dimer test thresholdwould be expected to increase test specificity the associateddecrease in sensitivity may be unacceptable to most cliniciansand has not been prospectively studied95
Potential benefits of using a highly sensitive D-dimer as ascreening test include decreased cost and radiation exposurehowever if the test is ordered indiscriminately on patients withvery little or no risk for PE false-positive D-dimer results mayincrease the harms associated with unnecessary advancedimaging A formal decision analysis concluded that using D-dimer was not cost-effective if CT is readily available96
Although the authorsrsquo assumptions about the sensitivity andspecificity of quantitative D-dimer tests were consistent with thestudies included in the Evidentiary Table the authors state thattheir analysis was based on a patient suspected of having PEwithout other competing diagnoses96 It is rare in the EDsetting to have such a straightforward clinical presentation inwhich only 1 diagnosis is considered
Future research is needed for patients with an intermediatepretest probability of PE and to assess whether changing theD-dimer cutoff for different patient subgroups could improvespecificity without a clinically significant decrease in sensitivity
4 What is the role of the CT pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations For patients with a low or PE
unlikely (Wells score 4) pretest probability for PE who require
additional diagnostic testing (eg positive D-dimer result or p
Volume June
ighly sensitive D-dimer test not available) a negativeultidetector CT pulmonary angiogram alone can be used to
xclude PELevel C recommendations (1) For patients with an
ntermediate pretest probability for PE and a negative CTulmonary angiogram result in whom a clinical concern for PEtill exists and CT venogram has not already been performedonsider additional diagnostic testing (eg D-dimer lowerxtremity imaging VQ scanning traditional pulmonaryrteriography) prior to exclusion of VTE disease
(2) For patients with a high pretest probability for PE and aegative CT angiogram result and CT venogram has notlready been performed perform additional diagnostic testingeg D-dimer lower extremity imaging VQ scanningraditional pulmonary arteriography) prior to exclusion of VTEiseaseA negative highly sensitive quantitative D-dimer result in
ombination with a negative multidetector CT pulmonaryngiogram result theoretically provides a posttest probability ofTE less than 1
Key wordsphrases for literature searches x-ray computedomography CT spiral computed tomography pulmonarymbolism sensitivity specificity probability likelihoodulmonary angiogram angiography thromboembolismutcome follow-up recurrent morbidity mortality falseegative false positive prognosis treatment outcome andariations and combinations of the key wordsphrases years001 through December 2009The use of the spiral CT angiogram for the visualization of
he pulmonary vasculature and the evaluation of PE was firstescribed in 199297 A single detector rotated in a spiral fashiont fixed intervals collecting data to generate vascular imagesuring a single breath holdSince that time the technology of this diagnostic modality
as advanced dramatically Multidetector CT scanners now useetween 4 64 or more channels (detectors) and rotate at muchaster gantry speeds (04 seconds versus 1 second per rotation)hus an older-generation single-detector CT with a 1-secondantry speed captures 1 slice per second whereas a 16-channelultidetector CT scanner rotating at a gantry speed of 04
econds captures 40 slices per second98 This in addition tohinner collimation allows for faster image acquisition lessotion artifact and ultimately higher-resolution images
mproved image acquisition protocols and resolution areelieved to result in improved diagnostic performanceIn 1992 Remy-Jardin et al97 in a Class III investigation
eported sensitivities and specificities of 100 and 96espectively for a single-detector CT for detection of PE Thisnding led to eager acceptance of the spiral CT angiogram intoiagnostic algorithms in the hope of simplifying theomplicated diagnostic workup of PE Since this initial studyultiple accuracy and outcomes studies in addition to meta-
nalyses and systematic reviews have been published on the
erformance of the CT pulmonary angiogram Unfortunately
Annals of Emergency Medicine 637
ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

oi
rettmc
p(
p
aas
C1ow
gwp
pdGaD
Eaeltswccpoa
O
i
Clinical Policy
relevant to the development of a clinical guideline blindedversus nonblinded outcome assessment blinded or randomizedallocation direct or indirect outcome measures (reliability andvalidity) biases (eg selection detection transfer) externalvalidity (ie generalizability) and sufficient sample size Articlesreceived a final grade (Class I II III) on the basis of apredetermined formula taking into account design and qualityof study (Appendix B) Articles with fatal flaws were given anldquoXrdquo grade and not used in formulating recommendations in thispolicy Evidence grading was done with respect to the specificdata being extracted and the specific critical question beingreviewed Thus the level of evidence for any one study may varyaccording to the question and it is possible for a single article toreceive different levels of grading as different critical questionsare answered Question-specific level of evidence grading may befound in the Evidentiary Table included online (available athttpwwwannemergmedcom)
Clinical findings and strength of recommendations regardingpatient management were then made according to the followingcriteria
Level A recommendations Generally accepted principles forpatient management that reflect a high degree of clinicalcertainty (ie based on strength of evidence Class I oroverwhelming evidence from strength of evidence Class IIstudies that directly address all of the issues)
Level B recommendations Recommendations for patientmanagement that may identify a particular strategy or range ofmanagement strategies that reflect moderate clinical certainty (iebased on strength of evidence Class II studies that directly addressthe issue decision analysis that directly addresses the issue or strongconsensus of strength of evidence Class III studies)
Level C recommendations Other strategies for patientmanagement that are based on Class III studies or in the absence ofany adequate published literature based on panel consensus
There are certain circumstances in which the recommendationsstemming from a body of evidence should not be rated as highly asthe individual studies on which they are based Factors such asheterogeneity of results uncertainty about effect magnitude andconsequences and publication bias among others might lead tosuch a downgrading of recommendations
When possible clinically oriented statistics (eg likelihoodratios [LRs] number needed to treat) will be presented to helpthe reader better understand how the results can be applied tothe individual patient For a definition of these statisticalconcepts see Appendix C
This policy is not intended to be a complete manual on theevaluation and management of patients with suspected PE butrather a focused examination of critical issues that have particularrelevance to the current practice of emergency medicine
It is the goal of the Clinical Policies Committee to providean evidence-based recommendation when the medical literatureprovides enough quality information to answer a criticalquestion When the medical literature does not contain enough
quality information to answer a critical question the members p
630 Annals of Emergency Medicine
f the Clinical Policies Committee believe that it is equallymportant to alert emergency physicians to this fact
Recommendations offered in this policy are not intended toepresent the only diagnostic and management options that themergency physician should consider ACEP clearly recognizeshe importance of the individual physicianrsquos judgment Ratherhis guideline defines for the physician those strategies for whichedical literature exists to provide support for answers to the
rucial questions addressed in this policyScope of Application This guideline is intended for
hysicians working in hospital-based emergency departmentsEDs) or ED-based observation centers
Inclusion Criteria This guideline is intended for adultatients presenting to the ED with suspected PE
Exclusion Criteria This guideline is not intended toddress the care of patients with PE in the presence of cardiacrrest or pregnancy patients with absence of symptomsuggestive of PE or pediatric patients
RITICAL QUESTIONS Do objective criteria provide improved risk stratificationver gestalt clinical assessment in the evaluation of patientsith possible PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Either objective criteria or
estalt clinical assessment can be used to risk stratify patientsith suspected PE There is insufficient evidence to support thereferential use of one method over another
Level C recommendations None specified
Key wordsphrases for literature searches risk stratificationulmonary embolism ED emergency service risk assessmentiagnostic strategies Wells criteria Wicki criteria Kline criteriaeneva score revised Geneva score PISA model and variations
nd combinations of the key wordsphrases years 2000 throughecember 2009This critical question focuses on pretest probability assessment
stimation of pretest probability is imperative for the properpplication of any diagnostic test This general principle becomesven more important for PE because it is a common but potentiallyethal disease when left undiagnosed and untreated Unfortunatelyhe classic presentation of PE is rare and physicians must makeome sort of assessment about whether to evaluate patients for PEhen they present with symptoms such as unexplained dyspnea
hest pain hemoptysis palpitations syncope back pain and otherommonplace symptoms that have been associated with PE Pretestrobability assessment in PE can be estimated in 2 general waysbjective criteria (clinical decision rules) or gestalt clinicalssessment (implicit approach)
bjective Criteria (Clinical Decision Rules)Clinical decision rules are a form of objective criteria that are
ntended to provide more accurate and reproducible measure of
retest probability assessment than the overall gestalt clinical
Volume June
W
omesaP
TaewPprCrtp
V
RAPRASUHCH
P
S
R041S
025
03
tnaacv
Clinical Policy
impression that depends on the physicianrsquos expertise and clinicalexperience Such rules can be derived and validated They alsocan be compared to each other and refined over time Severalclinical decision rules have been developed for use in patientswith suspected PE The most commonly used methods are (1)Geneva score19-21 (2) Wells (Canadian) score22 (3) Kline(Charlotte) criteria23 and (4) Pisa model2425
Geneva ScoreThe original Geneva score as described by Wicki et al19 in
2001 is a Class II study that was performed at a single hospitalin Switzerland and consists of a clinical score ranging from 0 to16 points derived from 8 parameters relating to risk factorsclinical signs blood gas analysis and chest radiographProbability of PE in patients defined as low- (0 to 4 points)intermediate- (5 to 8 points) and high- (9 points) risk was10 38 and 81 respectively Multiple Class III studieshave since validated the usefulness of the Geneva score in riskstratification of patients with suspected PE26-31
Because of the reliance of the original Geneva score on roomair blood gas analysis and chest radiograph interpretation LeGal et al20 in a Class II study retrospectively analyzed datafrom 2 previous multicenter clinical investigations to develop ascore independent of diagnostic testing The subsequent revisedGeneva score ranged from 0 to 25 points and was derived from8 parameters relating to risk factors symptoms and clinicalsigns (Table 1) In the validations set probability of PE in low-(score 0 to 3) intermediate- (score 4 to 10) and high-risk (score11) patients was 8 29 and 74 respectively To dateonly one Class II investigation has validated the revised Genevascore32
One of the difficulties of the revised Geneva score is thatdifferent elements have different weights making it potentiallymore difficult to apply in the clinical setting (Table 1) As a resultKlok et al21 in a Class II study reanalyzed the same populationand developed the simplified revised Geneva score that uses theidentical 8 parameters of the revised Geneva score (Table 1) Onepoint is assigned to each parameter except for pulse rate greaterthan or equal to 95 beatsmin which results in an additional pointProbability of PE in patients defined as low- (0 to 1 point)intermediate- (2 to 4 points) and high- (5 to 7 points) risk was 829 and 64 respectively The investigators also divided thepatients into the dichotomous group of PE unlikely (0 to 2 pointsprobability of PE 115) and PE likely (3 to 7 points probabilityof PE 351) to select a patient population safe for use of D-dimertesting for exclusion of PE Of the 330 patients with a PE unlikelyscore and a negative D-dimer result no patient was diagnosed ashaving venous thromboembolic disease on presentation or on 3-month follow-up Receiver operating characteristic (ROC) curveanalysis revealed no differences in diagnostic performance of therevised Geneva score (area under ROC curve 075 95 confidenceinterval [CI] 071 to 078) compared with the simplified revised
Geneva score (area under ROC curve 074 95 CI 070 to 077) a
Volume June
ells ScoreThe original Wells study was a Class III investigation in use
f a clinical model to risk stratify 1239 patients in low-oderate- and high-risk groups33 The investigators used
vidence from the published literature to establish a risk-tratification model by consensus The risk model initiallyssessed patients based on signs and symptoms as ldquotypicalrdquo forE ldquoatypicalrdquo for PE or ldquosevererdquo Physicians then made an
able 1 Revised Geneva score as described by Le Gal et al20
nd the simplified revised Geneva score as described by Klokt al21 for assessment of pretest probability of PE Reprintedith permission Copyright copy American College of Physiciansublisher Le Gal G Righini M Roy P-M et al Prediction ofulmonary embolism in the emergency department theevised Geneva score Ann Intern Med 2006144165-171opyright copy 2008 American Medical Association All rightseserved Klok FA Mos IC Nijkeuter M et al Simplification ofhe revised Geneva score for assessing clinical probability ofulmonary embolism Arch Intern Med 20081682131-2136
ariable
Points
RevisedGeneva
Simplified RevisedGeneva
isk factorsge 65 y 1 1revious DVTPE 3 1ecent surgeryfracture (4 wk) 2 1ctive malignancy 2 1ymptomsnilateral lower-limb pain 3 1emoptysis 2 1linical signseart rate75ndash94 beatsmin 3 195 beatsmin 5 2
ain on lower-limb deep venouspalpation and unilateral edema
4 1
core RangeProbability of PE
(95 CI)Patients WithThis Score
Interpretationof Risk
evised Geneva Score20
ndash3 79 (50ndash121) 370 Lowndash10 285 (246ndash328) 574 Moderate1ndash25 737 (610ndash834) 55 Highimplified Revised Geneva Score21
Traditional interpretationndash1 77 (52ndash108) 360 Lowndash4 294 (259ndash331) 60 Moderatendash7 643 (480ndash785) 40 HighAlternative interpretation
ndash2 129 (105ndash157) 649 PE unlikelyndash7 416 (365ndash468) 351 PE likely
The original table from Klok et al21 lists 1 point for heart rate 95 beatsmin buthe assessment of score states ldquo[b]ecause of the weight of heart rate in the origi-al score we attributed 1 point to a heart rate between 75 and 94 beatsmin andn additional point for a heart rate of 95 beatsmin or morerdquo Thus a patient withheart rate of 100 beatsmin would receive a total of 2 points (personal communi-
ation F A Klok MD PhD Department of General Internal Medicine Leiden Uni-ersity Medical CenterBronovo Hospital Den Haag May 2010)
ssessment about whether an ldquoalternative diagnosis that was as
Annals of Emergency Medicine 631
11pw1v9ts
vopphedP(
vHaarcp
K
csephsrwwaut(thps9Cet1IL
Clinical Policy
likely as or more likely than PErdquo to further subdivide thepatients into 10 possible outcomes These outcomes were thendivided into low- moderate- and high-risk groups Rates of PEin patients with low moderate and high risk were 34278 and 784 respectively Although this modelperformed well the algorithmic approach was not suitable to beused as an objective risk-stratification tool
Wells et al22 subsequently performed a retrospective analysisof the data used in the original study to develop a simple scoringsystem that could be used in conjunction with D-dimer for theevaluation of patients with suspected PE (Table 2) Usingregression techniques a risk-stratification model consisting of 7variables was created that classified patients as having lowmoderate and high probability of PE In addition analternative interpretation system was developed in which thepatients were classified into the dichotomist groups ldquoPEunlikelyrdquo and ldquoPE likelyrdquo to identify a group of patients forwhom a negative D-dimer test would result in a PE rate of 2If the D-dimer result was negative the rate of PE in patientsdesignated PE unlikely (score 0 to 4) was 22 in the derivationset and 17 in the validation set
This model was subsequently prospectively validated in aClass II investigation in a cohort of 4 EDs at tertiary carehospitals in Canada34 The initial pretest probabilities weredetermined by the clinical model to be low in 57 of patientsmoderate in 36 of patients and high in 7 of patientsIncluding follow-up events PE was diagnosed in 13 of
Table 2 Wells Canadian Score for assessment of pretestprobability for PE22 Reprinted with permission Copyright copySchattauer Publisher Wells PS Anderson DR Rodger M etal Derivation of a simple clinical model to categorize patientsprobability of pulmonary embolism increasing the modelsutility with the SimpliRED D-dimer Thromb Haemost 200083416-420
Criteria Points
Suspected DVT 30An alternative diagnosis is less likely than PE 30Heart rate 100 beatsminute 15Immobilization or surgery in the previous 4 weeks 15Previous DVTPE 15Hemoptysis 10Malignancy (on treatment treated in the last 6
months or palliative)10
Score RangePoints Probability of PE ()
With ThisScore
Interpretationof Risk
Traditionalinterpretation
0ndash1 36 (20ndash59) 403 Low2ndash6 205 (170ndash241) 526 Moderate6 667 (543ndash776) 71 HighAlternate
interpretation0ndash4 78 (59ndash101) 715 PE unlikely4 407 (349ndash465) 285 PE likely
patients with low pretest probability (95 CI 05 to 27) d
632 Annals of Emergency Medicine
62 of patients with moderate pretest probability (95 CI25 to 206) and in 406 of patients with high pretestrobability (95 CI 287 to 537) Of the 437 patientsith a negative D-dimer result and low clinical probability onlydeveloped PE during follow-up giving a negative predictive
alue for the use of the clinical model with D-dimer testing of95 (95 CI 991 to 100) No information is given inhis investigation about performance of the alternative scoringystem of ldquoPE unlikelyrdquo and ldquoPE likelyrdquo
A Class II investigation by the Christopher Study Investigatorsalidated the utility of the dichotomized alternative scoring systemf ldquoPE unlikelyrdquo versus ldquoPE likelyrdquo35 This study was a multicenterrospective cohort of 3306 patients A total of 2206 (667)atients were classified as PE unlikely Of these 1057 patients alsoad a negative D-dimer result and PE was considered to have beenxcluded On 3-month follow-up 5 (05) patients received aiagnosis of venous thromboembolic disease with no deaths In theE likely subgroup PE was diagnosed on CT scan in 674 patients204)
Multiple Class II3637and Class III studies28-3138-43 havealidated the usefulness of the Wells score in risk stratificationowever a major criticism of the Wells score is that it is not truly
n objective criterion because it contains the subjective variable ldquoanlternative diagnosis is less likely than PErdquo This variable in essenceepresents physician judgment override of the objectiveomponents of the score because it is worth 3 points and thuslaces the patient in the intermediate-risk group19324445
line RuleKline et al23 in a Class II study derived a decision rule to
reate a binary partition of ED patients with suspected PE toelect patients for whom a negative D-dimer result reliablyxcluded the presence of PE (Figure) Nine-hundred thirty-fouratients were studied at 7 urban EDs in the United States Theistory and physical process occurred prospectively beforetandard imaging to look for recognized symptoms signs andisk factors associated with PE Selected variables were analyzedith multivariate logistic analysis to determine factors associatedith PE A decision rule was then constructed to categorize
pproximately 80 of ED patients as being able to safelyndergo D-dimer testing Six variables were used to constructhe decision rule Unsafe patients had either a shock indexpulse ratesystolic blood pressure more than 10) or age greaterhan 50 years together with any of the following unexplainedypoxemia (arterial blood oxygen saturation [SaO2] 95 norevious lung disease) unilateral leg swelling recent majorurgery or hemoptysis These criteria were met by 197 (21) of34 patients Of these 197 patients 83 had PE (421 95I 355 to 496) When these 197 ldquounsaferdquo patients were
xcluded the probability of PE was significantly decreased inhe remaining 737 (79) ldquosaferdquo patients to 133 (95 CI09 to 159) Assuming use of an Enzyme-Linkedmmunosorbent Assay (ELISA) D-dimer assay with a negativeR of 007 the use of the Kline rule in conjunction with D-
imer testing would decrease the posttest probability of PE to
Volume June
eurgmdpmpiovoirpeh(a
wa3osPrsw2(
C
hcnCp
Pspwalps
cWaP
Clinical Policy
approximately 1 The authors concluded that these criteriacan permit safe D-dimer testing in the majority of ED patientswith suspected PE
There are no prospective outcome studies validating the useof the Kline rule in conjunction with D-dimer but 1 Class IIIstudy demonstrated a 21 decrease in CT scanning when theyinstituted this protocol46
Pisa ModelThe original Pisa investigation is a Class II study consisting
Figure Kline decision rule for excluding PE23 Reprintedfrom Annals of Emergency Medicine 39 Kline JA NelsonRD Jackson RE et al Criteria for the safe use of D-dimertesting in emergency department patients with suspectedpulmonary embolism a multicenter US study 144-1522002 Copyright from the American College of EmergencyPhysicians [2002]
Flow diagram demonstrating the Kline decision rule inselecting patients in whom D-dimer assay less than 500 ngml can reliably rule out PE This decision rule splits thepatients into 2 groups four fifths of whom are eligible for D-dimer testing (ldquosaferdquo patients with pretest probability of PE of133) and one fifth of whom are ineligible for D-dimertesting (ldquounsaferdquo patients with pretest probability of 421)
of 1100 consecutive patients with suspected PE who were W
Volume June
valuated at a single hospital in Pisa Italy24 All patientsnderwent a detailed clinical history physical examinationigorous interpretation of ECG and chest radiograph and bloodas measurements Using logistic regression techniques aathematical model for predicting probability of PE was
eveloped Probability was categorized as low (10robability of PE) intermediate (10 to 50 probability)oderately high (50 to 90 probability) and high (90
robability) Ten characteristics were associated with anncreased risk of PE male sex older age history of DVT acutenset dyspnea chest pain hemoptysis ECG signs of rightentricular overload radiographic signs of oligemia amputationf the hilar artery and pulmonary consolidations suggestive ofnfarction Five characteristics were associated with a decreasedisk previous cardiovascular or pulmonary disease feverulmonary consolidation other than infarction and pulmonarydema With this model 432 patients (39) were rated asaving low probability (4 PE) 283 (26) as intermediate22 PE) 72 (7) as moderately high probability (74 PE)nd 313 (28) as high probability (98 PE)
In the original Pisa model the highest regression coefficientsere for the chest radiograph findings (oligemia 386
mputation of hilar artery 392 and pulmonary infarction55) Because of the heavy reliance of the original Pisa modeln advanced chest radiograph interpretation skills beyond thekill level of the average physician Miniati et al25 refined theisa model in the same patient population after excluding chestadiograph from the final equation (Table 3) In the validationet of this Class II investigation the prevalence of PE was 2hen the predicted clinical probability was low (0 to 10)8 when moderate (11 to 50) 67 when substantial51 to 80) and 94 when high (81 to 100)
omparative Studies of Objective CriteriaThere are two Class II3247 and 3 Class III283031 studies that
ave evaluated performance of the various objective criteria Inomparing the Geneva score to the Wells score 3 studies foundo significant differences in performance though the study byhagnon et al28 suggested that the Geneva score overridden byhysician judgment may be more accurate283132
Miniati et al30 compared the Geneva score Wells score andisa model in 215 patients with suspected PE and foundtatistically significant differences in performance of the 3retest probability assessment tools Areas under the ROC curveere 054 075 and 094 for the Geneva score Wells score
nd Pisa model respectively However findings in this study areimited because of small sample size and the PE rate in thisatient population was extremely high (43) indicatingignificant patient selection bias
Runyon et al47 compared the Wells score with the Klineriteria in 2603 patients with a PE prevalence of 58 The
ells score identified 73 of patients as low risk (score 2)nd the Kline criteria identified 88 of patients as low risk TheE rates in these low-risk patients were 30 and 42 for the
ells and Kline criteria respectively
Annals of Emergency Medicine 633
wadt16gIp
oipgaoiRr(3s
ppap1ssi3ldquotrlcbp
pIgsi
L
r
ypP
Clinical Policy
Gestalt Clinical AssessmentGestalt clinical assessment is an unstructured (nonruled based)
estimate of the pretest probability of disease It is based on theclinicianrsquos training clinical experience and judgment Thisapproach has also been described as implicit in nature Theclinician using this approach surmises an overall impression of thepretest probability of PE and applies that impression to the decisionabout whether to pursue the diagnosis through objective testing
The Prospective Investigation of Pulmonary EmbolismDiagnosis (PIOPED) study was a prospective multi-institutioninvestigation designed to evaluate various conventional methodsfor diagnosing PE48 The PIOPED study is the first major studyreporting gestalt assessment As one element of the study the
Table 3 Regression coefficients and odds ratio for the Pisamodel as described by Miniati et al25 for estimatingprobability of pulmonary embolism according to clinical andECG findings Calculation of the clinical probability ofpulmonary embolism is performed as follows (1) Add all thecoefficients that apply to a given patient and the constantndash343 to obtain a sum score (2) the probability of pulmonaryembolism equals [1exp(ndashsum)]ndash1 Reprinted with permissionof the American Thoracic Society Copyright copy AmericanThoracic Society Miniati M Bottal M Monti S et al Simpleand accurate prediction of the clinical probability of pulmonaryembolism American Journal of Respiratory and Critical CareMedicine 2008178290-294 Official journal of the AmericanThoracic Society Diane Gern Publisher
Predictor Coefficient Odds Ratio 95 CI
Age y57ndash67 080 223 137ndash36368ndash74 087 238 141ndash40175 114 311 182ndash532Male sex 060 182 127ndash261Risk factorsImmobilization 042 153 108ndash215Deep venous thrombosis (ever) 064 190 123ndash295Preexisting diseasesCardiovascular ndash051 060 041ndash088Pulmonary ndash089 041 024ndash072SymptomsDyspnea (sudden onset) 200 738 518ndash1051Orthopnea ndash151 022 005ndash093Chest pain 101 274 193ndash388Fainting or syncope 066 193 125ndash298Hemoptysis 093 252 119ndash535SignsLeg swelling (unilateral) 080 223 135ndash370Fever 38degC (1004degF) ndash147 023 013ndash040Wheezes ndash120 030 014ndash066Crackles ndash061 054 035ndash083ElectrocardiogramAcute cor pulmonale 196 711 466ndash1087Constant ndash343
One or more of the following ECG abnormalities S1Q3T3 S1S2S3 negativeT waves in right precordial leads transient right bundle branch blockpseudoinfarction
clinicianrsquos assessment of the likelihood of PE from 0 to 100 t
634 Annals of Emergency Medicine
as recorded for 887 patients and was compared with PE statuss determined by angiogram and follow-up information Forata analysis low risk was considered pretest probability of 0o 19 intermediate risk 20 to 79 and high risk 80 to00 PE subsequently was diagnosed in 92 299 and78 of patients in the low- intermediate- and high-riskroups respectively Since the PIOPED study multiple ClassII studies have validated the usefulness of gestalt assessment ofretest probability in evaluating patients with suspected PE49-53
There have been several comparative studies of gestalt versusbjective criteria In a Class II study investigating potentialmpact of adjusting the D-dimer threshold Kabrhel et al37
rospectively performed pretest probability assessment usingestalt versus the Wells score in 7940 patients from 10cademic centers By gestalt pretest probability assessment 68f patients were low risk (15 pretest probability PE) 26ntermediate risk (15 to 40) and 6 high risk (40)ates of PE in these 3 subgroups were 3 10 and 33
espectively By the Wells score 69 of patients were low riskWells score 2) 28 intermediate (Wells score 2 to 6) and high risk (Wells score 6) Rates of PE in these 3ubgroups were 3 13 and 36 respectively
Sanson et al41 in a Class III study investigated pretestrobability assessment of gestalt versus the Wells score in 517atients with a 31 PE rate By gestalt pretest probabilityssessment 14 of patients were low risk (20 pretestrobability PE) 67 intermediate risk (20 to 80) and9 high risk (80 to 100) Rates of PE in these 3ubgroups were 19 29 and 46 respectively By the Wellscore 36 of patients were low risk (Wells score 2) 63ntermediate (Wells score 2 to 6) and 2 high risk (Wells score
6) Rates of PE in these 3 subgroups were 28 30 and8 respectively The authors conclude that both methodsalthough comparable perform disappointingly in categorizinghe pretest probability in patients with suspected PErdquo The highate of patients categorized as having intermediate risk and theow rate of patients categorized as having low risk in this studyompared with other studies suggest significant patient selectionias that may account for the poor performance in pretestrobability assessment by these 2 methods
Runyon et al47 in a Class II study compared gestalt pretestrobability assessment with the Wells criteria and the Kline rulen the low-risk group rate of PE was 26 30 and 42 forestalt Wells and Kline rule respectively Gestalt and Wellscore also were equivalent in pretest probability assessment forntermediate- and high-risk patients
imitationsSeveral issues concerning performance of clinical decision
ules and gestalt assessment have been raised in the literature(1) Interrater reliability Nordenholtz et al54 compared third-
ear emergency medicine resident and attending emergencyhysician interrater reliability for 271 patients with suspectedE Specific elements of the Wells and Kline risk-stratification
ools were studied Interrater agreement was concluded to be
Volume June
ea2
sdm2cditaupAatapsmawbsPkc
cpoby
P8wTeao3plnc3sr
Clinical Policy
moderate for DVT symptoms (054) immobilization(041) unexplained hypoxia (058) and PE more likelythan alternative diagnosis (05) good for hemoptysis(076) and very good for previous DVT (090)malignancy (087) and tachycardia (094) Runyon et al47
in a large single hospital study involving a subset of 154 patientsfound only moderate interrater agreement for gestalt clinicalassessment of low probability (06) and Wells score less than 2(047) and very good for Kline rule ldquosaferdquo (085)
(2) Clinical experience as a factor in the determination ofpretest probability of PE Accurate determination of the pretestprobability of PE appeared to trend with clinical experienceHowever the authors concluded that difference in accuracybetween the inexperienced and experienced physicians is notsufficiently large to distinguish between the 2 when determiningwhether clinical gestalt or a clinical prediction rule should beused to determine the pretest probability of PE55
Iles et al44 performed a survey to investigate whether numberof years since graduation from medical school affected pretestprobability score for the Geneva Wells and gestalt pretestprobability assessment The Geneva score was found to be themost consistent method of determining pretest probabilityGestalt assessment was inversely proportional to clinicalexperience suggesting that as physicians gain experience theyrecognize the difficulties in ruling out PE and are reluctant toexclude it on clinical grounds
(3) Knowledge and use of the rules Runyon et al56 surveyedemergency medicine clinicians and found that only half of allclinicians reporting familiarity with the rules use them in morethan 50 of applicable cases Spontaneous recall of the ruleswas low to moderate
ConclusionBoth objective criteria and gestalt assessment appear to
perform equally well for patients with suspected PE With theadvent of electronic charting future studies need to beperformed investigating the use of computer support aids infacilitating pretest probability assessment Studies also need tobe performed investigating use of pretest probability assessmentto guide subsequent diagnostic testing Finally studies need tobe performed to clarify the definitions of low- intermediate-and high-risk groups especially for gestalt assessment in whichstudies have used pretest probabilities ranging from 20 to80 as definition for intermediate probability
2 What is the utility of the PERC in the evaluation ofpatients with suspected PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations In patients with a low pretest
probability for suspected PE consider using the PERC toexclude the diagnosis based on historical and physical
examination data alone a
Volume June
Level C recommendations None specified
Key wordsphrases for literature searches PERC pulmonarymbolism rule-out criteria block rule pulmonary embolismnd variations and combinations of the key wordsphrases years000 through December 2009In 2004 Kline et al57 published a Class II prospective
tudy deriving clinical criteria to prevent unnecessaryiagnostic testing in ED patients with suspected PE In thisulticenter study with 3148 patients in a derivation cohort
1 descriptive variables relevant to the diagnosis of PE wereollected The primary outcome variable was the EDiagnosis of PE using a composite criterion standard
ncluding 90-day follow-up The overall prevalence of venoushromboembolism (VTE) was 11 Logistic regressionnalysis with stepwise backwards elimination of variables wassed to identify criteria that could predict a patientopulation estimated to have a prevalence of disease of 18t or below this low pretest probability of disease theuthors proposed that no further laboratory or radiographicesting would be needed to exclude the diagnosis of PElthough this threshold which was based on a previouslyublished method for calculating testing thresholds58 hasubsequently been more accurately estimated to be 14 by aore recent decision analytic model balancing the benefits
nd costs of using the PERC59 After their analysis 8 variablesere identified age younger than 50 years pulse rate less than 100eatsmin SaO2 greater than 94 (at sea level) no unilateral legwelling no hemoptysis no recent trauma or surgery no previousE or DVT and no hormone use These criteria have since becomenown as the PERC When all criteria are met a patient isonsidered to be PERC negative
In this same study the authors went on to internally validate theriteria in a separate patient cohort57 When applied to 1427atients considered to be low risk for PE by gestalt assessment 25f patients were PERC negative The criteria when considered toe a diagnostic test had 96 sensitivity and 27 specificityielding a LR- of 015 and a 14 false-negative rate
In 2008 Kline et al60 published a Class II validation study of theERC (Table 4) This multicenter prospective study enrolled138 patients Although limited by the number of eligible patientsho were not enrolled the authors made attempts to address thishe outcome measures were similar to those of the original study
xcept for follow-up occurring at 45 days as opposed to 90 daysnd the overall prevalence of VTE being 69 Sixty-seven percentf patients were classified as low risk by clinical gestalt and of these07 were PERC negative This equated to 204 of enrolledatients The sensitivity specificity and LR- for the PERC in the
ow-risk cohort were 947 219 and 012 respectively Ofote 35 of enrolled patients were PERC negative but notonsidered to be low risk by clinical gestalt This subgroup had a1 prevalence of VTE Although outcomes on this specificubgroup were not reported not all PERC negative patients are lowisk and the rulersquos applicability in these patients is unknown The
uthors concluded that the PERC could be used in combination
Annals of Emergency Medicine 635
pa
edk
DlSqbsrs(tapeii(oidhat
qdoCtpdpoCc9pos
tPrzi
Clinical Policy
with a low pretest probability to identify very low-risk patients forwhom the diagnosis of PE can be reliably excluded based onhistorical and physical examination data alone
In 2008 Wolf et al61 published a small Class III externalvalidation of the PERC This study was a post hoc analysis ofprospectively collected data on 120 consecutive ED patientswith a suspicion of PE The original database contained allPERC variables Outcome measures used were similar to thoseof the original study yielding a 12 prevalence of PE Whentheir entire patient population is considered regardless ofpretest probability the sensitivity and specificity were 100 and16 respectively When only the patients with low pretestprobability as defined by Wells Criteria are considered thespecificity increased to 22 The authors concluded that thePERC may identify a cohort of patients with suspected PE forwhom diagnostic testing beyond history and physicalexamination is not indicated
In each of the above 3 clinical studies even though patient datawere collected prospectively the application of the PERC rule wasperformed retrospectively As such there is no prospective outcomestudy of the use of the PERC rule for clinical decisionmaking Thislimits the strength of recommendations that can be made based onthe available evidence Future research should focus on the clinicalapplication of the PERC rule with measurement of acceptedoutcomes
3 What is the role of quantitative D-dimer testing in theexclusion of PE
Patient Management RecommendationsLevel A recommendations In patients with a low pretest
probability for PE a negative quantitative D-dimer assay resultcan be used to exclude PE
Table 4 The Pulmonary Embolism Rule Out Criteria (PERC)
The PERC criteria negative (PERCndash) require the clinician to answer noto the 8 questions below60 If a patient is low risk by gestaltimpression and PERCndash the posttest probability of venousthromboembolism is 2 Reprinted with permission Copyright copyJohn Wiley amp Sons Ltd Publisher Kline JA Courtney DM KabrhelC et al Prospective multicenter evaluation of the pulmonaryembolism rule-out criteria J Thromb Haemost 20086772-780
1 Is the patient older than 49 years of age2 Is the pulse rate greater than 99 beatsminndash13 Is the pulse oximetry reading 95 while the patient breathes
room air4 Is there a present history of hemoptysis5 Is the patient receiving exogenous estrogen6 Does the patient have a prior diagnosis of venous
thromboembolism (VTE)7 Has the patient had recent surgery or trauma (requiring
endotracheal intubation or hospitalization in the previous 4weeks)
8 Does the patient have unilateral leg swelling (visual observation ofasymmetry of the calves)
CHigh sensitivity (eg turbidimetric ELISA)
636 Annals of Emergency Medicine
Level B recommendations None specifiedLevel C recommendations In patients with an intermediate
retest probability for PE a negative quantitative D-dimerssay result may be used to exclude PE
Key wordsphrases for literature searches pulmonarymbolism fibrin fragment D sensitivity specificity D-dimerifferential diagnosis and variations and combinations of theey wordsphrases years 2001 through December 2009
This revision to the 2003 clinical policy1 focuses on quantitative-dimer tests that have become available to most hospital
aboratories across the United States The Clinical Policiesubcommittee on PE elected not to assess the evidence forualitative D-dimer tests (often used in point-of-care panels)ecause of problems with variability in interpretation and lowerensitivity reported in multiple studies62-65 However the onlyandomized clinical trial directly assessing the impact of a D-dimertrategy used a qualitative whole-blood agglutination testSimpliRED Agen Biomedical Ltd Brisbane Australia)66 In thisrial potential subjects suspected of having PE were first stratifiedccording to the Wells criteria and those with a low clinicalrobability and negative D-dimer test result were randomized toither no additional testing or VQ scanning Althoughnterpretation of results is limited due to early study closure thencidence of VTE during 6 months was similar among the 2 groups0182 versus 1185) Given that we were unable to identify anyther randomized controlled trials specifically designed to test thempact of a D-dimer strategy our recommendations are based onata from cohort studies and high-quality systematic reviews thatave been published since the original ACEP clinical policy1 Tovoid duplication cohort studies that were included in at least 1 ofhe systematic reviews are not reported in the Evidentiary Table
Class I systematic reviews assessing the test characteristics ofuantitative D-dimer tests in outpatient settings conclude that D-imer has excellent sensitivity (pooled sensitivity093 to 096) butnly moderate specificity (pooled specificity039 to 051)656768
lass I3542 and II 3769-75cohort studies that were not included inhese systematic reviews report similar results In patients with a lowretest probability (10) a negative ELISA or turbidimetric D-imer (LR-01) test result would be expected to decrease therobability of PE to approximately 1 These assumptions basedn the application of Bayesrsquo Theorem are supported by Class I35
lass II6973-75 and Class III38394676-79 studies that haveonsistently reported negative predictive values of approximately9 when D-dimer testing is applied to low-risk or ldquoPE unlikelyrdquoatient populations The American College of Physicians guidelinesn PE also support using D-dimer testing among low-risk patientsuspected of having PE8081
Despite consensus guidelines that recommend using D-dimeresting on patients with an intermediate pretest probability forE82 strong evidence supporting this approach is lacking Aetrospective analysis of 2 studies by Righini et al83 reportedero VTE events at 3-month follow-up for both low- andntermediate-risk groups however the upper limit for the 95
I was 1 for the low-probability group but extended up to
Volume June
hme
ipscea
na(td
caV
teponv2
tdad
hbfTgmstmIb
rrfidcma
Clinical Policy
5 for the intermediate-probability group Subsequent studiesthat have included intermediate pretest probability patientswithin their D-dimer strategy have either not reported resultsseparately737584 or have had too few patients in this subgroupto draw any firm conclusions777885
Given the relatively poor specificity of D-dimer testingvarious strategies have been suggested to limit the number offalse-positive tests that may lead to further unnecessarydiagnostic testing Retrospective subgroup analyses suggest thatD-dimer sensitivity remains fairly constant among varioussubpopulations but specificity decreases with certain comorbidconditions and advanced age678687 Two prospective studiesassessing the performance of D-dimer testing among cancerpatients suspected of having PE reported very low specificities(specificity018 to 021)8889 Pregnancy is also associated withincreasing concentrations of D-dimer particularly in womenbeyond the first trimester90 A restrictive approach to D-dimertesting whereby the elderly are excluded improves testspecificity8691 however this approach is unlikely to decreaseresource utilization since these patients would be expected to godirectly to some form of advanced imaging Adjusting the D-dimer test threshold based on the patientrsquos pretest probability orother variables (eg age) has been suggested as an alternativeapproach to improve the performance of D-dimertesting378792-94 Although raising the D-dimer test thresholdwould be expected to increase test specificity the associateddecrease in sensitivity may be unacceptable to most cliniciansand has not been prospectively studied95
Potential benefits of using a highly sensitive D-dimer as ascreening test include decreased cost and radiation exposurehowever if the test is ordered indiscriminately on patients withvery little or no risk for PE false-positive D-dimer results mayincrease the harms associated with unnecessary advancedimaging A formal decision analysis concluded that using D-dimer was not cost-effective if CT is readily available96
Although the authorsrsquo assumptions about the sensitivity andspecificity of quantitative D-dimer tests were consistent with thestudies included in the Evidentiary Table the authors state thattheir analysis was based on a patient suspected of having PEwithout other competing diagnoses96 It is rare in the EDsetting to have such a straightforward clinical presentation inwhich only 1 diagnosis is considered
Future research is needed for patients with an intermediatepretest probability of PE and to assess whether changing theD-dimer cutoff for different patient subgroups could improvespecificity without a clinically significant decrease in sensitivity
4 What is the role of the CT pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations For patients with a low or PE
unlikely (Wells score 4) pretest probability for PE who require
additional diagnostic testing (eg positive D-dimer result or p
Volume June
ighly sensitive D-dimer test not available) a negativeultidetector CT pulmonary angiogram alone can be used to
xclude PELevel C recommendations (1) For patients with an
ntermediate pretest probability for PE and a negative CTulmonary angiogram result in whom a clinical concern for PEtill exists and CT venogram has not already been performedonsider additional diagnostic testing (eg D-dimer lowerxtremity imaging VQ scanning traditional pulmonaryrteriography) prior to exclusion of VTE disease
(2) For patients with a high pretest probability for PE and aegative CT angiogram result and CT venogram has notlready been performed perform additional diagnostic testingeg D-dimer lower extremity imaging VQ scanningraditional pulmonary arteriography) prior to exclusion of VTEiseaseA negative highly sensitive quantitative D-dimer result in
ombination with a negative multidetector CT pulmonaryngiogram result theoretically provides a posttest probability ofTE less than 1
Key wordsphrases for literature searches x-ray computedomography CT spiral computed tomography pulmonarymbolism sensitivity specificity probability likelihoodulmonary angiogram angiography thromboembolismutcome follow-up recurrent morbidity mortality falseegative false positive prognosis treatment outcome andariations and combinations of the key wordsphrases years001 through December 2009The use of the spiral CT angiogram for the visualization of
he pulmonary vasculature and the evaluation of PE was firstescribed in 199297 A single detector rotated in a spiral fashiont fixed intervals collecting data to generate vascular imagesuring a single breath holdSince that time the technology of this diagnostic modality
as advanced dramatically Multidetector CT scanners now useetween 4 64 or more channels (detectors) and rotate at muchaster gantry speeds (04 seconds versus 1 second per rotation)hus an older-generation single-detector CT with a 1-secondantry speed captures 1 slice per second whereas a 16-channelultidetector CT scanner rotating at a gantry speed of 04
econds captures 40 slices per second98 This in addition tohinner collimation allows for faster image acquisition lessotion artifact and ultimately higher-resolution images
mproved image acquisition protocols and resolution areelieved to result in improved diagnostic performanceIn 1992 Remy-Jardin et al97 in a Class III investigation
eported sensitivities and specificities of 100 and 96espectively for a single-detector CT for detection of PE Thisnding led to eager acceptance of the spiral CT angiogram intoiagnostic algorithms in the hope of simplifying theomplicated diagnostic workup of PE Since this initial studyultiple accuracy and outcomes studies in addition to meta-
nalyses and systematic reviews have been published on the
erformance of the CT pulmonary angiogram Unfortunately
Annals of Emergency Medicine 637
ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

W
omesaP
TaewPprCrtp
V
RAPRASUHCH
P
S
R041S
025
03
tnaacv
Clinical Policy
impression that depends on the physicianrsquos expertise and clinicalexperience Such rules can be derived and validated They alsocan be compared to each other and refined over time Severalclinical decision rules have been developed for use in patientswith suspected PE The most commonly used methods are (1)Geneva score19-21 (2) Wells (Canadian) score22 (3) Kline(Charlotte) criteria23 and (4) Pisa model2425
Geneva ScoreThe original Geneva score as described by Wicki et al19 in
2001 is a Class II study that was performed at a single hospitalin Switzerland and consists of a clinical score ranging from 0 to16 points derived from 8 parameters relating to risk factorsclinical signs blood gas analysis and chest radiographProbability of PE in patients defined as low- (0 to 4 points)intermediate- (5 to 8 points) and high- (9 points) risk was10 38 and 81 respectively Multiple Class III studieshave since validated the usefulness of the Geneva score in riskstratification of patients with suspected PE26-31
Because of the reliance of the original Geneva score on roomair blood gas analysis and chest radiograph interpretation LeGal et al20 in a Class II study retrospectively analyzed datafrom 2 previous multicenter clinical investigations to develop ascore independent of diagnostic testing The subsequent revisedGeneva score ranged from 0 to 25 points and was derived from8 parameters relating to risk factors symptoms and clinicalsigns (Table 1) In the validations set probability of PE in low-(score 0 to 3) intermediate- (score 4 to 10) and high-risk (score11) patients was 8 29 and 74 respectively To dateonly one Class II investigation has validated the revised Genevascore32
One of the difficulties of the revised Geneva score is thatdifferent elements have different weights making it potentiallymore difficult to apply in the clinical setting (Table 1) As a resultKlok et al21 in a Class II study reanalyzed the same populationand developed the simplified revised Geneva score that uses theidentical 8 parameters of the revised Geneva score (Table 1) Onepoint is assigned to each parameter except for pulse rate greaterthan or equal to 95 beatsmin which results in an additional pointProbability of PE in patients defined as low- (0 to 1 point)intermediate- (2 to 4 points) and high- (5 to 7 points) risk was 829 and 64 respectively The investigators also divided thepatients into the dichotomous group of PE unlikely (0 to 2 pointsprobability of PE 115) and PE likely (3 to 7 points probabilityof PE 351) to select a patient population safe for use of D-dimertesting for exclusion of PE Of the 330 patients with a PE unlikelyscore and a negative D-dimer result no patient was diagnosed ashaving venous thromboembolic disease on presentation or on 3-month follow-up Receiver operating characteristic (ROC) curveanalysis revealed no differences in diagnostic performance of therevised Geneva score (area under ROC curve 075 95 confidenceinterval [CI] 071 to 078) compared with the simplified revised
Geneva score (area under ROC curve 074 95 CI 070 to 077) a
Volume June
ells ScoreThe original Wells study was a Class III investigation in use
f a clinical model to risk stratify 1239 patients in low-oderate- and high-risk groups33 The investigators used
vidence from the published literature to establish a risk-tratification model by consensus The risk model initiallyssessed patients based on signs and symptoms as ldquotypicalrdquo forE ldquoatypicalrdquo for PE or ldquosevererdquo Physicians then made an
able 1 Revised Geneva score as described by Le Gal et al20
nd the simplified revised Geneva score as described by Klokt al21 for assessment of pretest probability of PE Reprintedith permission Copyright copy American College of Physiciansublisher Le Gal G Righini M Roy P-M et al Prediction ofulmonary embolism in the emergency department theevised Geneva score Ann Intern Med 2006144165-171opyright copy 2008 American Medical Association All rightseserved Klok FA Mos IC Nijkeuter M et al Simplification ofhe revised Geneva score for assessing clinical probability ofulmonary embolism Arch Intern Med 20081682131-2136
ariable
Points
RevisedGeneva
Simplified RevisedGeneva
isk factorsge 65 y 1 1revious DVTPE 3 1ecent surgeryfracture (4 wk) 2 1ctive malignancy 2 1ymptomsnilateral lower-limb pain 3 1emoptysis 2 1linical signseart rate75ndash94 beatsmin 3 195 beatsmin 5 2
ain on lower-limb deep venouspalpation and unilateral edema
4 1
core RangeProbability of PE
(95 CI)Patients WithThis Score
Interpretationof Risk
evised Geneva Score20
ndash3 79 (50ndash121) 370 Lowndash10 285 (246ndash328) 574 Moderate1ndash25 737 (610ndash834) 55 Highimplified Revised Geneva Score21
Traditional interpretationndash1 77 (52ndash108) 360 Lowndash4 294 (259ndash331) 60 Moderatendash7 643 (480ndash785) 40 HighAlternative interpretation
ndash2 129 (105ndash157) 649 PE unlikelyndash7 416 (365ndash468) 351 PE likely
The original table from Klok et al21 lists 1 point for heart rate 95 beatsmin buthe assessment of score states ldquo[b]ecause of the weight of heart rate in the origi-al score we attributed 1 point to a heart rate between 75 and 94 beatsmin andn additional point for a heart rate of 95 beatsmin or morerdquo Thus a patient withheart rate of 100 beatsmin would receive a total of 2 points (personal communi-
ation F A Klok MD PhD Department of General Internal Medicine Leiden Uni-ersity Medical CenterBronovo Hospital Den Haag May 2010)
ssessment about whether an ldquoalternative diagnosis that was as
Annals of Emergency Medicine 631
11pw1v9ts
vopphedP(
vHaarcp
K
csephsrwwaut(thps9Cet1IL
Clinical Policy
likely as or more likely than PErdquo to further subdivide thepatients into 10 possible outcomes These outcomes were thendivided into low- moderate- and high-risk groups Rates of PEin patients with low moderate and high risk were 34278 and 784 respectively Although this modelperformed well the algorithmic approach was not suitable to beused as an objective risk-stratification tool
Wells et al22 subsequently performed a retrospective analysisof the data used in the original study to develop a simple scoringsystem that could be used in conjunction with D-dimer for theevaluation of patients with suspected PE (Table 2) Usingregression techniques a risk-stratification model consisting of 7variables was created that classified patients as having lowmoderate and high probability of PE In addition analternative interpretation system was developed in which thepatients were classified into the dichotomist groups ldquoPEunlikelyrdquo and ldquoPE likelyrdquo to identify a group of patients forwhom a negative D-dimer test would result in a PE rate of 2If the D-dimer result was negative the rate of PE in patientsdesignated PE unlikely (score 0 to 4) was 22 in the derivationset and 17 in the validation set
This model was subsequently prospectively validated in aClass II investigation in a cohort of 4 EDs at tertiary carehospitals in Canada34 The initial pretest probabilities weredetermined by the clinical model to be low in 57 of patientsmoderate in 36 of patients and high in 7 of patientsIncluding follow-up events PE was diagnosed in 13 of
Table 2 Wells Canadian Score for assessment of pretestprobability for PE22 Reprinted with permission Copyright copySchattauer Publisher Wells PS Anderson DR Rodger M etal Derivation of a simple clinical model to categorize patientsprobability of pulmonary embolism increasing the modelsutility with the SimpliRED D-dimer Thromb Haemost 200083416-420
Criteria Points
Suspected DVT 30An alternative diagnosis is less likely than PE 30Heart rate 100 beatsminute 15Immobilization or surgery in the previous 4 weeks 15Previous DVTPE 15Hemoptysis 10Malignancy (on treatment treated in the last 6
months or palliative)10
Score RangePoints Probability of PE ()
With ThisScore
Interpretationof Risk
Traditionalinterpretation
0ndash1 36 (20ndash59) 403 Low2ndash6 205 (170ndash241) 526 Moderate6 667 (543ndash776) 71 HighAlternate
interpretation0ndash4 78 (59ndash101) 715 PE unlikely4 407 (349ndash465) 285 PE likely
patients with low pretest probability (95 CI 05 to 27) d
632 Annals of Emergency Medicine
62 of patients with moderate pretest probability (95 CI25 to 206) and in 406 of patients with high pretestrobability (95 CI 287 to 537) Of the 437 patientsith a negative D-dimer result and low clinical probability onlydeveloped PE during follow-up giving a negative predictive
alue for the use of the clinical model with D-dimer testing of95 (95 CI 991 to 100) No information is given inhis investigation about performance of the alternative scoringystem of ldquoPE unlikelyrdquo and ldquoPE likelyrdquo
A Class II investigation by the Christopher Study Investigatorsalidated the utility of the dichotomized alternative scoring systemf ldquoPE unlikelyrdquo versus ldquoPE likelyrdquo35 This study was a multicenterrospective cohort of 3306 patients A total of 2206 (667)atients were classified as PE unlikely Of these 1057 patients alsoad a negative D-dimer result and PE was considered to have beenxcluded On 3-month follow-up 5 (05) patients received aiagnosis of venous thromboembolic disease with no deaths In theE likely subgroup PE was diagnosed on CT scan in 674 patients204)
Multiple Class II3637and Class III studies28-3138-43 havealidated the usefulness of the Wells score in risk stratificationowever a major criticism of the Wells score is that it is not truly
n objective criterion because it contains the subjective variable ldquoanlternative diagnosis is less likely than PErdquo This variable in essenceepresents physician judgment override of the objectiveomponents of the score because it is worth 3 points and thuslaces the patient in the intermediate-risk group19324445
line RuleKline et al23 in a Class II study derived a decision rule to
reate a binary partition of ED patients with suspected PE toelect patients for whom a negative D-dimer result reliablyxcluded the presence of PE (Figure) Nine-hundred thirty-fouratients were studied at 7 urban EDs in the United States Theistory and physical process occurred prospectively beforetandard imaging to look for recognized symptoms signs andisk factors associated with PE Selected variables were analyzedith multivariate logistic analysis to determine factors associatedith PE A decision rule was then constructed to categorize
pproximately 80 of ED patients as being able to safelyndergo D-dimer testing Six variables were used to constructhe decision rule Unsafe patients had either a shock indexpulse ratesystolic blood pressure more than 10) or age greaterhan 50 years together with any of the following unexplainedypoxemia (arterial blood oxygen saturation [SaO2] 95 norevious lung disease) unilateral leg swelling recent majorurgery or hemoptysis These criteria were met by 197 (21) of34 patients Of these 197 patients 83 had PE (421 95I 355 to 496) When these 197 ldquounsaferdquo patients were
xcluded the probability of PE was significantly decreased inhe remaining 737 (79) ldquosaferdquo patients to 133 (95 CI09 to 159) Assuming use of an Enzyme-Linkedmmunosorbent Assay (ELISA) D-dimer assay with a negativeR of 007 the use of the Kline rule in conjunction with D-
imer testing would decrease the posttest probability of PE to
Volume June
eurgmdpmpiovoirpeh(a
wa3osPrsw2(
C
hcnCp
Pspwalps
cWaP
Clinical Policy
approximately 1 The authors concluded that these criteriacan permit safe D-dimer testing in the majority of ED patientswith suspected PE
There are no prospective outcome studies validating the useof the Kline rule in conjunction with D-dimer but 1 Class IIIstudy demonstrated a 21 decrease in CT scanning when theyinstituted this protocol46
Pisa ModelThe original Pisa investigation is a Class II study consisting
Figure Kline decision rule for excluding PE23 Reprintedfrom Annals of Emergency Medicine 39 Kline JA NelsonRD Jackson RE et al Criteria for the safe use of D-dimertesting in emergency department patients with suspectedpulmonary embolism a multicenter US study 144-1522002 Copyright from the American College of EmergencyPhysicians [2002]
Flow diagram demonstrating the Kline decision rule inselecting patients in whom D-dimer assay less than 500 ngml can reliably rule out PE This decision rule splits thepatients into 2 groups four fifths of whom are eligible for D-dimer testing (ldquosaferdquo patients with pretest probability of PE of133) and one fifth of whom are ineligible for D-dimertesting (ldquounsaferdquo patients with pretest probability of 421)
of 1100 consecutive patients with suspected PE who were W
Volume June
valuated at a single hospital in Pisa Italy24 All patientsnderwent a detailed clinical history physical examinationigorous interpretation of ECG and chest radiograph and bloodas measurements Using logistic regression techniques aathematical model for predicting probability of PE was
eveloped Probability was categorized as low (10robability of PE) intermediate (10 to 50 probability)oderately high (50 to 90 probability) and high (90
robability) Ten characteristics were associated with anncreased risk of PE male sex older age history of DVT acutenset dyspnea chest pain hemoptysis ECG signs of rightentricular overload radiographic signs of oligemia amputationf the hilar artery and pulmonary consolidations suggestive ofnfarction Five characteristics were associated with a decreasedisk previous cardiovascular or pulmonary disease feverulmonary consolidation other than infarction and pulmonarydema With this model 432 patients (39) were rated asaving low probability (4 PE) 283 (26) as intermediate22 PE) 72 (7) as moderately high probability (74 PE)nd 313 (28) as high probability (98 PE)
In the original Pisa model the highest regression coefficientsere for the chest radiograph findings (oligemia 386
mputation of hilar artery 392 and pulmonary infarction55) Because of the heavy reliance of the original Pisa modeln advanced chest radiograph interpretation skills beyond thekill level of the average physician Miniati et al25 refined theisa model in the same patient population after excluding chestadiograph from the final equation (Table 3) In the validationet of this Class II investigation the prevalence of PE was 2hen the predicted clinical probability was low (0 to 10)8 when moderate (11 to 50) 67 when substantial51 to 80) and 94 when high (81 to 100)
omparative Studies of Objective CriteriaThere are two Class II3247 and 3 Class III283031 studies that
ave evaluated performance of the various objective criteria Inomparing the Geneva score to the Wells score 3 studies foundo significant differences in performance though the study byhagnon et al28 suggested that the Geneva score overridden byhysician judgment may be more accurate283132
Miniati et al30 compared the Geneva score Wells score andisa model in 215 patients with suspected PE and foundtatistically significant differences in performance of the 3retest probability assessment tools Areas under the ROC curveere 054 075 and 094 for the Geneva score Wells score
nd Pisa model respectively However findings in this study areimited because of small sample size and the PE rate in thisatient population was extremely high (43) indicatingignificant patient selection bias
Runyon et al47 compared the Wells score with the Klineriteria in 2603 patients with a PE prevalence of 58 The
ells score identified 73 of patients as low risk (score 2)nd the Kline criteria identified 88 of patients as low risk TheE rates in these low-risk patients were 30 and 42 for the
ells and Kline criteria respectively
Annals of Emergency Medicine 633
wadt16gIp
oipgaoiRr(3s
ppap1ssi3ldquotrlcbp
pIgsi
L
r
ypP
Clinical Policy
Gestalt Clinical AssessmentGestalt clinical assessment is an unstructured (nonruled based)
estimate of the pretest probability of disease It is based on theclinicianrsquos training clinical experience and judgment Thisapproach has also been described as implicit in nature Theclinician using this approach surmises an overall impression of thepretest probability of PE and applies that impression to the decisionabout whether to pursue the diagnosis through objective testing
The Prospective Investigation of Pulmonary EmbolismDiagnosis (PIOPED) study was a prospective multi-institutioninvestigation designed to evaluate various conventional methodsfor diagnosing PE48 The PIOPED study is the first major studyreporting gestalt assessment As one element of the study the
Table 3 Regression coefficients and odds ratio for the Pisamodel as described by Miniati et al25 for estimatingprobability of pulmonary embolism according to clinical andECG findings Calculation of the clinical probability ofpulmonary embolism is performed as follows (1) Add all thecoefficients that apply to a given patient and the constantndash343 to obtain a sum score (2) the probability of pulmonaryembolism equals [1exp(ndashsum)]ndash1 Reprinted with permissionof the American Thoracic Society Copyright copy AmericanThoracic Society Miniati M Bottal M Monti S et al Simpleand accurate prediction of the clinical probability of pulmonaryembolism American Journal of Respiratory and Critical CareMedicine 2008178290-294 Official journal of the AmericanThoracic Society Diane Gern Publisher
Predictor Coefficient Odds Ratio 95 CI
Age y57ndash67 080 223 137ndash36368ndash74 087 238 141ndash40175 114 311 182ndash532Male sex 060 182 127ndash261Risk factorsImmobilization 042 153 108ndash215Deep venous thrombosis (ever) 064 190 123ndash295Preexisting diseasesCardiovascular ndash051 060 041ndash088Pulmonary ndash089 041 024ndash072SymptomsDyspnea (sudden onset) 200 738 518ndash1051Orthopnea ndash151 022 005ndash093Chest pain 101 274 193ndash388Fainting or syncope 066 193 125ndash298Hemoptysis 093 252 119ndash535SignsLeg swelling (unilateral) 080 223 135ndash370Fever 38degC (1004degF) ndash147 023 013ndash040Wheezes ndash120 030 014ndash066Crackles ndash061 054 035ndash083ElectrocardiogramAcute cor pulmonale 196 711 466ndash1087Constant ndash343
One or more of the following ECG abnormalities S1Q3T3 S1S2S3 negativeT waves in right precordial leads transient right bundle branch blockpseudoinfarction
clinicianrsquos assessment of the likelihood of PE from 0 to 100 t
634 Annals of Emergency Medicine
as recorded for 887 patients and was compared with PE statuss determined by angiogram and follow-up information Forata analysis low risk was considered pretest probability of 0o 19 intermediate risk 20 to 79 and high risk 80 to00 PE subsequently was diagnosed in 92 299 and78 of patients in the low- intermediate- and high-riskroups respectively Since the PIOPED study multiple ClassII studies have validated the usefulness of gestalt assessment ofretest probability in evaluating patients with suspected PE49-53
There have been several comparative studies of gestalt versusbjective criteria In a Class II study investigating potentialmpact of adjusting the D-dimer threshold Kabrhel et al37
rospectively performed pretest probability assessment usingestalt versus the Wells score in 7940 patients from 10cademic centers By gestalt pretest probability assessment 68f patients were low risk (15 pretest probability PE) 26ntermediate risk (15 to 40) and 6 high risk (40)ates of PE in these 3 subgroups were 3 10 and 33
espectively By the Wells score 69 of patients were low riskWells score 2) 28 intermediate (Wells score 2 to 6) and high risk (Wells score 6) Rates of PE in these 3ubgroups were 3 13 and 36 respectively
Sanson et al41 in a Class III study investigated pretestrobability assessment of gestalt versus the Wells score in 517atients with a 31 PE rate By gestalt pretest probabilityssessment 14 of patients were low risk (20 pretestrobability PE) 67 intermediate risk (20 to 80) and9 high risk (80 to 100) Rates of PE in these 3ubgroups were 19 29 and 46 respectively By the Wellscore 36 of patients were low risk (Wells score 2) 63ntermediate (Wells score 2 to 6) and 2 high risk (Wells score
6) Rates of PE in these 3 subgroups were 28 30 and8 respectively The authors conclude that both methodsalthough comparable perform disappointingly in categorizinghe pretest probability in patients with suspected PErdquo The highate of patients categorized as having intermediate risk and theow rate of patients categorized as having low risk in this studyompared with other studies suggest significant patient selectionias that may account for the poor performance in pretestrobability assessment by these 2 methods
Runyon et al47 in a Class II study compared gestalt pretestrobability assessment with the Wells criteria and the Kline rulen the low-risk group rate of PE was 26 30 and 42 forestalt Wells and Kline rule respectively Gestalt and Wellscore also were equivalent in pretest probability assessment forntermediate- and high-risk patients
imitationsSeveral issues concerning performance of clinical decision
ules and gestalt assessment have been raised in the literature(1) Interrater reliability Nordenholtz et al54 compared third-
ear emergency medicine resident and attending emergencyhysician interrater reliability for 271 patients with suspectedE Specific elements of the Wells and Kline risk-stratification
ools were studied Interrater agreement was concluded to be
Volume June
ea2
sdm2cditaupAatapsmawbsPkc
cpoby
P8wTeao3plnc3sr
Clinical Policy
moderate for DVT symptoms (054) immobilization(041) unexplained hypoxia (058) and PE more likelythan alternative diagnosis (05) good for hemoptysis(076) and very good for previous DVT (090)malignancy (087) and tachycardia (094) Runyon et al47
in a large single hospital study involving a subset of 154 patientsfound only moderate interrater agreement for gestalt clinicalassessment of low probability (06) and Wells score less than 2(047) and very good for Kline rule ldquosaferdquo (085)
(2) Clinical experience as a factor in the determination ofpretest probability of PE Accurate determination of the pretestprobability of PE appeared to trend with clinical experienceHowever the authors concluded that difference in accuracybetween the inexperienced and experienced physicians is notsufficiently large to distinguish between the 2 when determiningwhether clinical gestalt or a clinical prediction rule should beused to determine the pretest probability of PE55
Iles et al44 performed a survey to investigate whether numberof years since graduation from medical school affected pretestprobability score for the Geneva Wells and gestalt pretestprobability assessment The Geneva score was found to be themost consistent method of determining pretest probabilityGestalt assessment was inversely proportional to clinicalexperience suggesting that as physicians gain experience theyrecognize the difficulties in ruling out PE and are reluctant toexclude it on clinical grounds
(3) Knowledge and use of the rules Runyon et al56 surveyedemergency medicine clinicians and found that only half of allclinicians reporting familiarity with the rules use them in morethan 50 of applicable cases Spontaneous recall of the ruleswas low to moderate
ConclusionBoth objective criteria and gestalt assessment appear to
perform equally well for patients with suspected PE With theadvent of electronic charting future studies need to beperformed investigating the use of computer support aids infacilitating pretest probability assessment Studies also need tobe performed investigating use of pretest probability assessmentto guide subsequent diagnostic testing Finally studies need tobe performed to clarify the definitions of low- intermediate-and high-risk groups especially for gestalt assessment in whichstudies have used pretest probabilities ranging from 20 to80 as definition for intermediate probability
2 What is the utility of the PERC in the evaluation ofpatients with suspected PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations In patients with a low pretest
probability for suspected PE consider using the PERC toexclude the diagnosis based on historical and physical
examination data alone a
Volume June
Level C recommendations None specified
Key wordsphrases for literature searches PERC pulmonarymbolism rule-out criteria block rule pulmonary embolismnd variations and combinations of the key wordsphrases years000 through December 2009In 2004 Kline et al57 published a Class II prospective
tudy deriving clinical criteria to prevent unnecessaryiagnostic testing in ED patients with suspected PE In thisulticenter study with 3148 patients in a derivation cohort
1 descriptive variables relevant to the diagnosis of PE wereollected The primary outcome variable was the EDiagnosis of PE using a composite criterion standard
ncluding 90-day follow-up The overall prevalence of venoushromboembolism (VTE) was 11 Logistic regressionnalysis with stepwise backwards elimination of variables wassed to identify criteria that could predict a patientopulation estimated to have a prevalence of disease of 18t or below this low pretest probability of disease theuthors proposed that no further laboratory or radiographicesting would be needed to exclude the diagnosis of PElthough this threshold which was based on a previouslyublished method for calculating testing thresholds58 hasubsequently been more accurately estimated to be 14 by aore recent decision analytic model balancing the benefits
nd costs of using the PERC59 After their analysis 8 variablesere identified age younger than 50 years pulse rate less than 100eatsmin SaO2 greater than 94 (at sea level) no unilateral legwelling no hemoptysis no recent trauma or surgery no previousE or DVT and no hormone use These criteria have since becomenown as the PERC When all criteria are met a patient isonsidered to be PERC negative
In this same study the authors went on to internally validate theriteria in a separate patient cohort57 When applied to 1427atients considered to be low risk for PE by gestalt assessment 25f patients were PERC negative The criteria when considered toe a diagnostic test had 96 sensitivity and 27 specificityielding a LR- of 015 and a 14 false-negative rate
In 2008 Kline et al60 published a Class II validation study of theERC (Table 4) This multicenter prospective study enrolled138 patients Although limited by the number of eligible patientsho were not enrolled the authors made attempts to address thishe outcome measures were similar to those of the original study
xcept for follow-up occurring at 45 days as opposed to 90 daysnd the overall prevalence of VTE being 69 Sixty-seven percentf patients were classified as low risk by clinical gestalt and of these07 were PERC negative This equated to 204 of enrolledatients The sensitivity specificity and LR- for the PERC in the
ow-risk cohort were 947 219 and 012 respectively Ofote 35 of enrolled patients were PERC negative but notonsidered to be low risk by clinical gestalt This subgroup had a1 prevalence of VTE Although outcomes on this specificubgroup were not reported not all PERC negative patients are lowisk and the rulersquos applicability in these patients is unknown The
uthors concluded that the PERC could be used in combination
Annals of Emergency Medicine 635
pa
edk
DlSqbsrs(tapeii(oidhat
qdoCtpdpoCc9pos
tPrzi
Clinical Policy
with a low pretest probability to identify very low-risk patients forwhom the diagnosis of PE can be reliably excluded based onhistorical and physical examination data alone
In 2008 Wolf et al61 published a small Class III externalvalidation of the PERC This study was a post hoc analysis ofprospectively collected data on 120 consecutive ED patientswith a suspicion of PE The original database contained allPERC variables Outcome measures used were similar to thoseof the original study yielding a 12 prevalence of PE Whentheir entire patient population is considered regardless ofpretest probability the sensitivity and specificity were 100 and16 respectively When only the patients with low pretestprobability as defined by Wells Criteria are considered thespecificity increased to 22 The authors concluded that thePERC may identify a cohort of patients with suspected PE forwhom diagnostic testing beyond history and physicalexamination is not indicated
In each of the above 3 clinical studies even though patient datawere collected prospectively the application of the PERC rule wasperformed retrospectively As such there is no prospective outcomestudy of the use of the PERC rule for clinical decisionmaking Thislimits the strength of recommendations that can be made based onthe available evidence Future research should focus on the clinicalapplication of the PERC rule with measurement of acceptedoutcomes
3 What is the role of quantitative D-dimer testing in theexclusion of PE
Patient Management RecommendationsLevel A recommendations In patients with a low pretest
probability for PE a negative quantitative D-dimer assay resultcan be used to exclude PE
Table 4 The Pulmonary Embolism Rule Out Criteria (PERC)
The PERC criteria negative (PERCndash) require the clinician to answer noto the 8 questions below60 If a patient is low risk by gestaltimpression and PERCndash the posttest probability of venousthromboembolism is 2 Reprinted with permission Copyright copyJohn Wiley amp Sons Ltd Publisher Kline JA Courtney DM KabrhelC et al Prospective multicenter evaluation of the pulmonaryembolism rule-out criteria J Thromb Haemost 20086772-780
1 Is the patient older than 49 years of age2 Is the pulse rate greater than 99 beatsminndash13 Is the pulse oximetry reading 95 while the patient breathes
room air4 Is there a present history of hemoptysis5 Is the patient receiving exogenous estrogen6 Does the patient have a prior diagnosis of venous
thromboembolism (VTE)7 Has the patient had recent surgery or trauma (requiring
endotracheal intubation or hospitalization in the previous 4weeks)
8 Does the patient have unilateral leg swelling (visual observation ofasymmetry of the calves)
CHigh sensitivity (eg turbidimetric ELISA)
636 Annals of Emergency Medicine
Level B recommendations None specifiedLevel C recommendations In patients with an intermediate
retest probability for PE a negative quantitative D-dimerssay result may be used to exclude PE
Key wordsphrases for literature searches pulmonarymbolism fibrin fragment D sensitivity specificity D-dimerifferential diagnosis and variations and combinations of theey wordsphrases years 2001 through December 2009
This revision to the 2003 clinical policy1 focuses on quantitative-dimer tests that have become available to most hospital
aboratories across the United States The Clinical Policiesubcommittee on PE elected not to assess the evidence forualitative D-dimer tests (often used in point-of-care panels)ecause of problems with variability in interpretation and lowerensitivity reported in multiple studies62-65 However the onlyandomized clinical trial directly assessing the impact of a D-dimertrategy used a qualitative whole-blood agglutination testSimpliRED Agen Biomedical Ltd Brisbane Australia)66 In thisrial potential subjects suspected of having PE were first stratifiedccording to the Wells criteria and those with a low clinicalrobability and negative D-dimer test result were randomized toither no additional testing or VQ scanning Althoughnterpretation of results is limited due to early study closure thencidence of VTE during 6 months was similar among the 2 groups0182 versus 1185) Given that we were unable to identify anyther randomized controlled trials specifically designed to test thempact of a D-dimer strategy our recommendations are based onata from cohort studies and high-quality systematic reviews thatave been published since the original ACEP clinical policy1 Tovoid duplication cohort studies that were included in at least 1 ofhe systematic reviews are not reported in the Evidentiary Table
Class I systematic reviews assessing the test characteristics ofuantitative D-dimer tests in outpatient settings conclude that D-imer has excellent sensitivity (pooled sensitivity093 to 096) butnly moderate specificity (pooled specificity039 to 051)656768
lass I3542 and II 3769-75cohort studies that were not included inhese systematic reviews report similar results In patients with a lowretest probability (10) a negative ELISA or turbidimetric D-imer (LR-01) test result would be expected to decrease therobability of PE to approximately 1 These assumptions basedn the application of Bayesrsquo Theorem are supported by Class I35
lass II6973-75 and Class III38394676-79 studies that haveonsistently reported negative predictive values of approximately9 when D-dimer testing is applied to low-risk or ldquoPE unlikelyrdquoatient populations The American College of Physicians guidelinesn PE also support using D-dimer testing among low-risk patientsuspected of having PE8081
Despite consensus guidelines that recommend using D-dimeresting on patients with an intermediate pretest probability forE82 strong evidence supporting this approach is lacking Aetrospective analysis of 2 studies by Righini et al83 reportedero VTE events at 3-month follow-up for both low- andntermediate-risk groups however the upper limit for the 95
I was 1 for the low-probability group but extended up to
Volume June
hme
ipscea
na(td
caV
teponv2
tdad
hbfTgmstmIb
rrfidcma
Clinical Policy
5 for the intermediate-probability group Subsequent studiesthat have included intermediate pretest probability patientswithin their D-dimer strategy have either not reported resultsseparately737584 or have had too few patients in this subgroupto draw any firm conclusions777885
Given the relatively poor specificity of D-dimer testingvarious strategies have been suggested to limit the number offalse-positive tests that may lead to further unnecessarydiagnostic testing Retrospective subgroup analyses suggest thatD-dimer sensitivity remains fairly constant among varioussubpopulations but specificity decreases with certain comorbidconditions and advanced age678687 Two prospective studiesassessing the performance of D-dimer testing among cancerpatients suspected of having PE reported very low specificities(specificity018 to 021)8889 Pregnancy is also associated withincreasing concentrations of D-dimer particularly in womenbeyond the first trimester90 A restrictive approach to D-dimertesting whereby the elderly are excluded improves testspecificity8691 however this approach is unlikely to decreaseresource utilization since these patients would be expected to godirectly to some form of advanced imaging Adjusting the D-dimer test threshold based on the patientrsquos pretest probability orother variables (eg age) has been suggested as an alternativeapproach to improve the performance of D-dimertesting378792-94 Although raising the D-dimer test thresholdwould be expected to increase test specificity the associateddecrease in sensitivity may be unacceptable to most cliniciansand has not been prospectively studied95
Potential benefits of using a highly sensitive D-dimer as ascreening test include decreased cost and radiation exposurehowever if the test is ordered indiscriminately on patients withvery little or no risk for PE false-positive D-dimer results mayincrease the harms associated with unnecessary advancedimaging A formal decision analysis concluded that using D-dimer was not cost-effective if CT is readily available96
Although the authorsrsquo assumptions about the sensitivity andspecificity of quantitative D-dimer tests were consistent with thestudies included in the Evidentiary Table the authors state thattheir analysis was based on a patient suspected of having PEwithout other competing diagnoses96 It is rare in the EDsetting to have such a straightforward clinical presentation inwhich only 1 diagnosis is considered
Future research is needed for patients with an intermediatepretest probability of PE and to assess whether changing theD-dimer cutoff for different patient subgroups could improvespecificity without a clinically significant decrease in sensitivity
4 What is the role of the CT pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations For patients with a low or PE
unlikely (Wells score 4) pretest probability for PE who require
additional diagnostic testing (eg positive D-dimer result or p
Volume June
ighly sensitive D-dimer test not available) a negativeultidetector CT pulmonary angiogram alone can be used to
xclude PELevel C recommendations (1) For patients with an
ntermediate pretest probability for PE and a negative CTulmonary angiogram result in whom a clinical concern for PEtill exists and CT venogram has not already been performedonsider additional diagnostic testing (eg D-dimer lowerxtremity imaging VQ scanning traditional pulmonaryrteriography) prior to exclusion of VTE disease
(2) For patients with a high pretest probability for PE and aegative CT angiogram result and CT venogram has notlready been performed perform additional diagnostic testingeg D-dimer lower extremity imaging VQ scanningraditional pulmonary arteriography) prior to exclusion of VTEiseaseA negative highly sensitive quantitative D-dimer result in
ombination with a negative multidetector CT pulmonaryngiogram result theoretically provides a posttest probability ofTE less than 1
Key wordsphrases for literature searches x-ray computedomography CT spiral computed tomography pulmonarymbolism sensitivity specificity probability likelihoodulmonary angiogram angiography thromboembolismutcome follow-up recurrent morbidity mortality falseegative false positive prognosis treatment outcome andariations and combinations of the key wordsphrases years001 through December 2009The use of the spiral CT angiogram for the visualization of
he pulmonary vasculature and the evaluation of PE was firstescribed in 199297 A single detector rotated in a spiral fashiont fixed intervals collecting data to generate vascular imagesuring a single breath holdSince that time the technology of this diagnostic modality
as advanced dramatically Multidetector CT scanners now useetween 4 64 or more channels (detectors) and rotate at muchaster gantry speeds (04 seconds versus 1 second per rotation)hus an older-generation single-detector CT with a 1-secondantry speed captures 1 slice per second whereas a 16-channelultidetector CT scanner rotating at a gantry speed of 04
econds captures 40 slices per second98 This in addition tohinner collimation allows for faster image acquisition lessotion artifact and ultimately higher-resolution images
mproved image acquisition protocols and resolution areelieved to result in improved diagnostic performanceIn 1992 Remy-Jardin et al97 in a Class III investigation
eported sensitivities and specificities of 100 and 96espectively for a single-detector CT for detection of PE Thisnding led to eager acceptance of the spiral CT angiogram intoiagnostic algorithms in the hope of simplifying theomplicated diagnostic workup of PE Since this initial studyultiple accuracy and outcomes studies in addition to meta-
nalyses and systematic reviews have been published on the
erformance of the CT pulmonary angiogram Unfortunately
Annals of Emergency Medicine 637
ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

11pw1v9ts
vopphedP(
vHaarcp
K
csephsrwwaut(thps9Cet1IL
Clinical Policy
likely as or more likely than PErdquo to further subdivide thepatients into 10 possible outcomes These outcomes were thendivided into low- moderate- and high-risk groups Rates of PEin patients with low moderate and high risk were 34278 and 784 respectively Although this modelperformed well the algorithmic approach was not suitable to beused as an objective risk-stratification tool
Wells et al22 subsequently performed a retrospective analysisof the data used in the original study to develop a simple scoringsystem that could be used in conjunction with D-dimer for theevaluation of patients with suspected PE (Table 2) Usingregression techniques a risk-stratification model consisting of 7variables was created that classified patients as having lowmoderate and high probability of PE In addition analternative interpretation system was developed in which thepatients were classified into the dichotomist groups ldquoPEunlikelyrdquo and ldquoPE likelyrdquo to identify a group of patients forwhom a negative D-dimer test would result in a PE rate of 2If the D-dimer result was negative the rate of PE in patientsdesignated PE unlikely (score 0 to 4) was 22 in the derivationset and 17 in the validation set
This model was subsequently prospectively validated in aClass II investigation in a cohort of 4 EDs at tertiary carehospitals in Canada34 The initial pretest probabilities weredetermined by the clinical model to be low in 57 of patientsmoderate in 36 of patients and high in 7 of patientsIncluding follow-up events PE was diagnosed in 13 of
Table 2 Wells Canadian Score for assessment of pretestprobability for PE22 Reprinted with permission Copyright copySchattauer Publisher Wells PS Anderson DR Rodger M etal Derivation of a simple clinical model to categorize patientsprobability of pulmonary embolism increasing the modelsutility with the SimpliRED D-dimer Thromb Haemost 200083416-420
Criteria Points
Suspected DVT 30An alternative diagnosis is less likely than PE 30Heart rate 100 beatsminute 15Immobilization or surgery in the previous 4 weeks 15Previous DVTPE 15Hemoptysis 10Malignancy (on treatment treated in the last 6
months or palliative)10
Score RangePoints Probability of PE ()
With ThisScore
Interpretationof Risk
Traditionalinterpretation
0ndash1 36 (20ndash59) 403 Low2ndash6 205 (170ndash241) 526 Moderate6 667 (543ndash776) 71 HighAlternate
interpretation0ndash4 78 (59ndash101) 715 PE unlikely4 407 (349ndash465) 285 PE likely
patients with low pretest probability (95 CI 05 to 27) d
632 Annals of Emergency Medicine
62 of patients with moderate pretest probability (95 CI25 to 206) and in 406 of patients with high pretestrobability (95 CI 287 to 537) Of the 437 patientsith a negative D-dimer result and low clinical probability onlydeveloped PE during follow-up giving a negative predictive
alue for the use of the clinical model with D-dimer testing of95 (95 CI 991 to 100) No information is given inhis investigation about performance of the alternative scoringystem of ldquoPE unlikelyrdquo and ldquoPE likelyrdquo
A Class II investigation by the Christopher Study Investigatorsalidated the utility of the dichotomized alternative scoring systemf ldquoPE unlikelyrdquo versus ldquoPE likelyrdquo35 This study was a multicenterrospective cohort of 3306 patients A total of 2206 (667)atients were classified as PE unlikely Of these 1057 patients alsoad a negative D-dimer result and PE was considered to have beenxcluded On 3-month follow-up 5 (05) patients received aiagnosis of venous thromboembolic disease with no deaths In theE likely subgroup PE was diagnosed on CT scan in 674 patients204)
Multiple Class II3637and Class III studies28-3138-43 havealidated the usefulness of the Wells score in risk stratificationowever a major criticism of the Wells score is that it is not truly
n objective criterion because it contains the subjective variable ldquoanlternative diagnosis is less likely than PErdquo This variable in essenceepresents physician judgment override of the objectiveomponents of the score because it is worth 3 points and thuslaces the patient in the intermediate-risk group19324445
line RuleKline et al23 in a Class II study derived a decision rule to
reate a binary partition of ED patients with suspected PE toelect patients for whom a negative D-dimer result reliablyxcluded the presence of PE (Figure) Nine-hundred thirty-fouratients were studied at 7 urban EDs in the United States Theistory and physical process occurred prospectively beforetandard imaging to look for recognized symptoms signs andisk factors associated with PE Selected variables were analyzedith multivariate logistic analysis to determine factors associatedith PE A decision rule was then constructed to categorize
pproximately 80 of ED patients as being able to safelyndergo D-dimer testing Six variables were used to constructhe decision rule Unsafe patients had either a shock indexpulse ratesystolic blood pressure more than 10) or age greaterhan 50 years together with any of the following unexplainedypoxemia (arterial blood oxygen saturation [SaO2] 95 norevious lung disease) unilateral leg swelling recent majorurgery or hemoptysis These criteria were met by 197 (21) of34 patients Of these 197 patients 83 had PE (421 95I 355 to 496) When these 197 ldquounsaferdquo patients were
xcluded the probability of PE was significantly decreased inhe remaining 737 (79) ldquosaferdquo patients to 133 (95 CI09 to 159) Assuming use of an Enzyme-Linkedmmunosorbent Assay (ELISA) D-dimer assay with a negativeR of 007 the use of the Kline rule in conjunction with D-
imer testing would decrease the posttest probability of PE to
Volume June
eurgmdpmpiovoirpeh(a
wa3osPrsw2(
C
hcnCp
Pspwalps
cWaP
Clinical Policy
approximately 1 The authors concluded that these criteriacan permit safe D-dimer testing in the majority of ED patientswith suspected PE
There are no prospective outcome studies validating the useof the Kline rule in conjunction with D-dimer but 1 Class IIIstudy demonstrated a 21 decrease in CT scanning when theyinstituted this protocol46
Pisa ModelThe original Pisa investigation is a Class II study consisting
Figure Kline decision rule for excluding PE23 Reprintedfrom Annals of Emergency Medicine 39 Kline JA NelsonRD Jackson RE et al Criteria for the safe use of D-dimertesting in emergency department patients with suspectedpulmonary embolism a multicenter US study 144-1522002 Copyright from the American College of EmergencyPhysicians [2002]
Flow diagram demonstrating the Kline decision rule inselecting patients in whom D-dimer assay less than 500 ngml can reliably rule out PE This decision rule splits thepatients into 2 groups four fifths of whom are eligible for D-dimer testing (ldquosaferdquo patients with pretest probability of PE of133) and one fifth of whom are ineligible for D-dimertesting (ldquounsaferdquo patients with pretest probability of 421)
of 1100 consecutive patients with suspected PE who were W
Volume June
valuated at a single hospital in Pisa Italy24 All patientsnderwent a detailed clinical history physical examinationigorous interpretation of ECG and chest radiograph and bloodas measurements Using logistic regression techniques aathematical model for predicting probability of PE was
eveloped Probability was categorized as low (10robability of PE) intermediate (10 to 50 probability)oderately high (50 to 90 probability) and high (90
robability) Ten characteristics were associated with anncreased risk of PE male sex older age history of DVT acutenset dyspnea chest pain hemoptysis ECG signs of rightentricular overload radiographic signs of oligemia amputationf the hilar artery and pulmonary consolidations suggestive ofnfarction Five characteristics were associated with a decreasedisk previous cardiovascular or pulmonary disease feverulmonary consolidation other than infarction and pulmonarydema With this model 432 patients (39) were rated asaving low probability (4 PE) 283 (26) as intermediate22 PE) 72 (7) as moderately high probability (74 PE)nd 313 (28) as high probability (98 PE)
In the original Pisa model the highest regression coefficientsere for the chest radiograph findings (oligemia 386
mputation of hilar artery 392 and pulmonary infarction55) Because of the heavy reliance of the original Pisa modeln advanced chest radiograph interpretation skills beyond thekill level of the average physician Miniati et al25 refined theisa model in the same patient population after excluding chestadiograph from the final equation (Table 3) In the validationet of this Class II investigation the prevalence of PE was 2hen the predicted clinical probability was low (0 to 10)8 when moderate (11 to 50) 67 when substantial51 to 80) and 94 when high (81 to 100)
omparative Studies of Objective CriteriaThere are two Class II3247 and 3 Class III283031 studies that
ave evaluated performance of the various objective criteria Inomparing the Geneva score to the Wells score 3 studies foundo significant differences in performance though the study byhagnon et al28 suggested that the Geneva score overridden byhysician judgment may be more accurate283132
Miniati et al30 compared the Geneva score Wells score andisa model in 215 patients with suspected PE and foundtatistically significant differences in performance of the 3retest probability assessment tools Areas under the ROC curveere 054 075 and 094 for the Geneva score Wells score
nd Pisa model respectively However findings in this study areimited because of small sample size and the PE rate in thisatient population was extremely high (43) indicatingignificant patient selection bias
Runyon et al47 compared the Wells score with the Klineriteria in 2603 patients with a PE prevalence of 58 The
ells score identified 73 of patients as low risk (score 2)nd the Kline criteria identified 88 of patients as low risk TheE rates in these low-risk patients were 30 and 42 for the
ells and Kline criteria respectively
Annals of Emergency Medicine 633
wadt16gIp
oipgaoiRr(3s
ppap1ssi3ldquotrlcbp
pIgsi
L
r
ypP
Clinical Policy
Gestalt Clinical AssessmentGestalt clinical assessment is an unstructured (nonruled based)
estimate of the pretest probability of disease It is based on theclinicianrsquos training clinical experience and judgment Thisapproach has also been described as implicit in nature Theclinician using this approach surmises an overall impression of thepretest probability of PE and applies that impression to the decisionabout whether to pursue the diagnosis through objective testing
The Prospective Investigation of Pulmonary EmbolismDiagnosis (PIOPED) study was a prospective multi-institutioninvestigation designed to evaluate various conventional methodsfor diagnosing PE48 The PIOPED study is the first major studyreporting gestalt assessment As one element of the study the
Table 3 Regression coefficients and odds ratio for the Pisamodel as described by Miniati et al25 for estimatingprobability of pulmonary embolism according to clinical andECG findings Calculation of the clinical probability ofpulmonary embolism is performed as follows (1) Add all thecoefficients that apply to a given patient and the constantndash343 to obtain a sum score (2) the probability of pulmonaryembolism equals [1exp(ndashsum)]ndash1 Reprinted with permissionof the American Thoracic Society Copyright copy AmericanThoracic Society Miniati M Bottal M Monti S et al Simpleand accurate prediction of the clinical probability of pulmonaryembolism American Journal of Respiratory and Critical CareMedicine 2008178290-294 Official journal of the AmericanThoracic Society Diane Gern Publisher
Predictor Coefficient Odds Ratio 95 CI
Age y57ndash67 080 223 137ndash36368ndash74 087 238 141ndash40175 114 311 182ndash532Male sex 060 182 127ndash261Risk factorsImmobilization 042 153 108ndash215Deep venous thrombosis (ever) 064 190 123ndash295Preexisting diseasesCardiovascular ndash051 060 041ndash088Pulmonary ndash089 041 024ndash072SymptomsDyspnea (sudden onset) 200 738 518ndash1051Orthopnea ndash151 022 005ndash093Chest pain 101 274 193ndash388Fainting or syncope 066 193 125ndash298Hemoptysis 093 252 119ndash535SignsLeg swelling (unilateral) 080 223 135ndash370Fever 38degC (1004degF) ndash147 023 013ndash040Wheezes ndash120 030 014ndash066Crackles ndash061 054 035ndash083ElectrocardiogramAcute cor pulmonale 196 711 466ndash1087Constant ndash343
One or more of the following ECG abnormalities S1Q3T3 S1S2S3 negativeT waves in right precordial leads transient right bundle branch blockpseudoinfarction
clinicianrsquos assessment of the likelihood of PE from 0 to 100 t
634 Annals of Emergency Medicine
as recorded for 887 patients and was compared with PE statuss determined by angiogram and follow-up information Forata analysis low risk was considered pretest probability of 0o 19 intermediate risk 20 to 79 and high risk 80 to00 PE subsequently was diagnosed in 92 299 and78 of patients in the low- intermediate- and high-riskroups respectively Since the PIOPED study multiple ClassII studies have validated the usefulness of gestalt assessment ofretest probability in evaluating patients with suspected PE49-53
There have been several comparative studies of gestalt versusbjective criteria In a Class II study investigating potentialmpact of adjusting the D-dimer threshold Kabrhel et al37
rospectively performed pretest probability assessment usingestalt versus the Wells score in 7940 patients from 10cademic centers By gestalt pretest probability assessment 68f patients were low risk (15 pretest probability PE) 26ntermediate risk (15 to 40) and 6 high risk (40)ates of PE in these 3 subgroups were 3 10 and 33
espectively By the Wells score 69 of patients were low riskWells score 2) 28 intermediate (Wells score 2 to 6) and high risk (Wells score 6) Rates of PE in these 3ubgroups were 3 13 and 36 respectively
Sanson et al41 in a Class III study investigated pretestrobability assessment of gestalt versus the Wells score in 517atients with a 31 PE rate By gestalt pretest probabilityssessment 14 of patients were low risk (20 pretestrobability PE) 67 intermediate risk (20 to 80) and9 high risk (80 to 100) Rates of PE in these 3ubgroups were 19 29 and 46 respectively By the Wellscore 36 of patients were low risk (Wells score 2) 63ntermediate (Wells score 2 to 6) and 2 high risk (Wells score
6) Rates of PE in these 3 subgroups were 28 30 and8 respectively The authors conclude that both methodsalthough comparable perform disappointingly in categorizinghe pretest probability in patients with suspected PErdquo The highate of patients categorized as having intermediate risk and theow rate of patients categorized as having low risk in this studyompared with other studies suggest significant patient selectionias that may account for the poor performance in pretestrobability assessment by these 2 methods
Runyon et al47 in a Class II study compared gestalt pretestrobability assessment with the Wells criteria and the Kline rulen the low-risk group rate of PE was 26 30 and 42 forestalt Wells and Kline rule respectively Gestalt and Wellscore also were equivalent in pretest probability assessment forntermediate- and high-risk patients
imitationsSeveral issues concerning performance of clinical decision
ules and gestalt assessment have been raised in the literature(1) Interrater reliability Nordenholtz et al54 compared third-
ear emergency medicine resident and attending emergencyhysician interrater reliability for 271 patients with suspectedE Specific elements of the Wells and Kline risk-stratification
ools were studied Interrater agreement was concluded to be
Volume June
ea2
sdm2cditaupAatapsmawbsPkc
cpoby
P8wTeao3plnc3sr
Clinical Policy
moderate for DVT symptoms (054) immobilization(041) unexplained hypoxia (058) and PE more likelythan alternative diagnosis (05) good for hemoptysis(076) and very good for previous DVT (090)malignancy (087) and tachycardia (094) Runyon et al47
in a large single hospital study involving a subset of 154 patientsfound only moderate interrater agreement for gestalt clinicalassessment of low probability (06) and Wells score less than 2(047) and very good for Kline rule ldquosaferdquo (085)
(2) Clinical experience as a factor in the determination ofpretest probability of PE Accurate determination of the pretestprobability of PE appeared to trend with clinical experienceHowever the authors concluded that difference in accuracybetween the inexperienced and experienced physicians is notsufficiently large to distinguish between the 2 when determiningwhether clinical gestalt or a clinical prediction rule should beused to determine the pretest probability of PE55
Iles et al44 performed a survey to investigate whether numberof years since graduation from medical school affected pretestprobability score for the Geneva Wells and gestalt pretestprobability assessment The Geneva score was found to be themost consistent method of determining pretest probabilityGestalt assessment was inversely proportional to clinicalexperience suggesting that as physicians gain experience theyrecognize the difficulties in ruling out PE and are reluctant toexclude it on clinical grounds
(3) Knowledge and use of the rules Runyon et al56 surveyedemergency medicine clinicians and found that only half of allclinicians reporting familiarity with the rules use them in morethan 50 of applicable cases Spontaneous recall of the ruleswas low to moderate
ConclusionBoth objective criteria and gestalt assessment appear to
perform equally well for patients with suspected PE With theadvent of electronic charting future studies need to beperformed investigating the use of computer support aids infacilitating pretest probability assessment Studies also need tobe performed investigating use of pretest probability assessmentto guide subsequent diagnostic testing Finally studies need tobe performed to clarify the definitions of low- intermediate-and high-risk groups especially for gestalt assessment in whichstudies have used pretest probabilities ranging from 20 to80 as definition for intermediate probability
2 What is the utility of the PERC in the evaluation ofpatients with suspected PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations In patients with a low pretest
probability for suspected PE consider using the PERC toexclude the diagnosis based on historical and physical
examination data alone a
Volume June
Level C recommendations None specified
Key wordsphrases for literature searches PERC pulmonarymbolism rule-out criteria block rule pulmonary embolismnd variations and combinations of the key wordsphrases years000 through December 2009In 2004 Kline et al57 published a Class II prospective
tudy deriving clinical criteria to prevent unnecessaryiagnostic testing in ED patients with suspected PE In thisulticenter study with 3148 patients in a derivation cohort
1 descriptive variables relevant to the diagnosis of PE wereollected The primary outcome variable was the EDiagnosis of PE using a composite criterion standard
ncluding 90-day follow-up The overall prevalence of venoushromboembolism (VTE) was 11 Logistic regressionnalysis with stepwise backwards elimination of variables wassed to identify criteria that could predict a patientopulation estimated to have a prevalence of disease of 18t or below this low pretest probability of disease theuthors proposed that no further laboratory or radiographicesting would be needed to exclude the diagnosis of PElthough this threshold which was based on a previouslyublished method for calculating testing thresholds58 hasubsequently been more accurately estimated to be 14 by aore recent decision analytic model balancing the benefits
nd costs of using the PERC59 After their analysis 8 variablesere identified age younger than 50 years pulse rate less than 100eatsmin SaO2 greater than 94 (at sea level) no unilateral legwelling no hemoptysis no recent trauma or surgery no previousE or DVT and no hormone use These criteria have since becomenown as the PERC When all criteria are met a patient isonsidered to be PERC negative
In this same study the authors went on to internally validate theriteria in a separate patient cohort57 When applied to 1427atients considered to be low risk for PE by gestalt assessment 25f patients were PERC negative The criteria when considered toe a diagnostic test had 96 sensitivity and 27 specificityielding a LR- of 015 and a 14 false-negative rate
In 2008 Kline et al60 published a Class II validation study of theERC (Table 4) This multicenter prospective study enrolled138 patients Although limited by the number of eligible patientsho were not enrolled the authors made attempts to address thishe outcome measures were similar to those of the original study
xcept for follow-up occurring at 45 days as opposed to 90 daysnd the overall prevalence of VTE being 69 Sixty-seven percentf patients were classified as low risk by clinical gestalt and of these07 were PERC negative This equated to 204 of enrolledatients The sensitivity specificity and LR- for the PERC in the
ow-risk cohort were 947 219 and 012 respectively Ofote 35 of enrolled patients were PERC negative but notonsidered to be low risk by clinical gestalt This subgroup had a1 prevalence of VTE Although outcomes on this specificubgroup were not reported not all PERC negative patients are lowisk and the rulersquos applicability in these patients is unknown The
uthors concluded that the PERC could be used in combination
Annals of Emergency Medicine 635
pa
edk
DlSqbsrs(tapeii(oidhat
qdoCtpdpoCc9pos
tPrzi
Clinical Policy
with a low pretest probability to identify very low-risk patients forwhom the diagnosis of PE can be reliably excluded based onhistorical and physical examination data alone
In 2008 Wolf et al61 published a small Class III externalvalidation of the PERC This study was a post hoc analysis ofprospectively collected data on 120 consecutive ED patientswith a suspicion of PE The original database contained allPERC variables Outcome measures used were similar to thoseof the original study yielding a 12 prevalence of PE Whentheir entire patient population is considered regardless ofpretest probability the sensitivity and specificity were 100 and16 respectively When only the patients with low pretestprobability as defined by Wells Criteria are considered thespecificity increased to 22 The authors concluded that thePERC may identify a cohort of patients with suspected PE forwhom diagnostic testing beyond history and physicalexamination is not indicated
In each of the above 3 clinical studies even though patient datawere collected prospectively the application of the PERC rule wasperformed retrospectively As such there is no prospective outcomestudy of the use of the PERC rule for clinical decisionmaking Thislimits the strength of recommendations that can be made based onthe available evidence Future research should focus on the clinicalapplication of the PERC rule with measurement of acceptedoutcomes
3 What is the role of quantitative D-dimer testing in theexclusion of PE
Patient Management RecommendationsLevel A recommendations In patients with a low pretest
probability for PE a negative quantitative D-dimer assay resultcan be used to exclude PE
Table 4 The Pulmonary Embolism Rule Out Criteria (PERC)
The PERC criteria negative (PERCndash) require the clinician to answer noto the 8 questions below60 If a patient is low risk by gestaltimpression and PERCndash the posttest probability of venousthromboembolism is 2 Reprinted with permission Copyright copyJohn Wiley amp Sons Ltd Publisher Kline JA Courtney DM KabrhelC et al Prospective multicenter evaluation of the pulmonaryembolism rule-out criteria J Thromb Haemost 20086772-780
1 Is the patient older than 49 years of age2 Is the pulse rate greater than 99 beatsminndash13 Is the pulse oximetry reading 95 while the patient breathes
room air4 Is there a present history of hemoptysis5 Is the patient receiving exogenous estrogen6 Does the patient have a prior diagnosis of venous
thromboembolism (VTE)7 Has the patient had recent surgery or trauma (requiring
endotracheal intubation or hospitalization in the previous 4weeks)
8 Does the patient have unilateral leg swelling (visual observation ofasymmetry of the calves)
CHigh sensitivity (eg turbidimetric ELISA)
636 Annals of Emergency Medicine
Level B recommendations None specifiedLevel C recommendations In patients with an intermediate
retest probability for PE a negative quantitative D-dimerssay result may be used to exclude PE
Key wordsphrases for literature searches pulmonarymbolism fibrin fragment D sensitivity specificity D-dimerifferential diagnosis and variations and combinations of theey wordsphrases years 2001 through December 2009
This revision to the 2003 clinical policy1 focuses on quantitative-dimer tests that have become available to most hospital
aboratories across the United States The Clinical Policiesubcommittee on PE elected not to assess the evidence forualitative D-dimer tests (often used in point-of-care panels)ecause of problems with variability in interpretation and lowerensitivity reported in multiple studies62-65 However the onlyandomized clinical trial directly assessing the impact of a D-dimertrategy used a qualitative whole-blood agglutination testSimpliRED Agen Biomedical Ltd Brisbane Australia)66 In thisrial potential subjects suspected of having PE were first stratifiedccording to the Wells criteria and those with a low clinicalrobability and negative D-dimer test result were randomized toither no additional testing or VQ scanning Althoughnterpretation of results is limited due to early study closure thencidence of VTE during 6 months was similar among the 2 groups0182 versus 1185) Given that we were unable to identify anyther randomized controlled trials specifically designed to test thempact of a D-dimer strategy our recommendations are based onata from cohort studies and high-quality systematic reviews thatave been published since the original ACEP clinical policy1 Tovoid duplication cohort studies that were included in at least 1 ofhe systematic reviews are not reported in the Evidentiary Table
Class I systematic reviews assessing the test characteristics ofuantitative D-dimer tests in outpatient settings conclude that D-imer has excellent sensitivity (pooled sensitivity093 to 096) butnly moderate specificity (pooled specificity039 to 051)656768
lass I3542 and II 3769-75cohort studies that were not included inhese systematic reviews report similar results In patients with a lowretest probability (10) a negative ELISA or turbidimetric D-imer (LR-01) test result would be expected to decrease therobability of PE to approximately 1 These assumptions basedn the application of Bayesrsquo Theorem are supported by Class I35
lass II6973-75 and Class III38394676-79 studies that haveonsistently reported negative predictive values of approximately9 when D-dimer testing is applied to low-risk or ldquoPE unlikelyrdquoatient populations The American College of Physicians guidelinesn PE also support using D-dimer testing among low-risk patientsuspected of having PE8081
Despite consensus guidelines that recommend using D-dimeresting on patients with an intermediate pretest probability forE82 strong evidence supporting this approach is lacking Aetrospective analysis of 2 studies by Righini et al83 reportedero VTE events at 3-month follow-up for both low- andntermediate-risk groups however the upper limit for the 95
I was 1 for the low-probability group but extended up to
Volume June
hme
ipscea
na(td
caV
teponv2
tdad
hbfTgmstmIb
rrfidcma
Clinical Policy
5 for the intermediate-probability group Subsequent studiesthat have included intermediate pretest probability patientswithin their D-dimer strategy have either not reported resultsseparately737584 or have had too few patients in this subgroupto draw any firm conclusions777885
Given the relatively poor specificity of D-dimer testingvarious strategies have been suggested to limit the number offalse-positive tests that may lead to further unnecessarydiagnostic testing Retrospective subgroup analyses suggest thatD-dimer sensitivity remains fairly constant among varioussubpopulations but specificity decreases with certain comorbidconditions and advanced age678687 Two prospective studiesassessing the performance of D-dimer testing among cancerpatients suspected of having PE reported very low specificities(specificity018 to 021)8889 Pregnancy is also associated withincreasing concentrations of D-dimer particularly in womenbeyond the first trimester90 A restrictive approach to D-dimertesting whereby the elderly are excluded improves testspecificity8691 however this approach is unlikely to decreaseresource utilization since these patients would be expected to godirectly to some form of advanced imaging Adjusting the D-dimer test threshold based on the patientrsquos pretest probability orother variables (eg age) has been suggested as an alternativeapproach to improve the performance of D-dimertesting378792-94 Although raising the D-dimer test thresholdwould be expected to increase test specificity the associateddecrease in sensitivity may be unacceptable to most cliniciansand has not been prospectively studied95
Potential benefits of using a highly sensitive D-dimer as ascreening test include decreased cost and radiation exposurehowever if the test is ordered indiscriminately on patients withvery little or no risk for PE false-positive D-dimer results mayincrease the harms associated with unnecessary advancedimaging A formal decision analysis concluded that using D-dimer was not cost-effective if CT is readily available96
Although the authorsrsquo assumptions about the sensitivity andspecificity of quantitative D-dimer tests were consistent with thestudies included in the Evidentiary Table the authors state thattheir analysis was based on a patient suspected of having PEwithout other competing diagnoses96 It is rare in the EDsetting to have such a straightforward clinical presentation inwhich only 1 diagnosis is considered
Future research is needed for patients with an intermediatepretest probability of PE and to assess whether changing theD-dimer cutoff for different patient subgroups could improvespecificity without a clinically significant decrease in sensitivity
4 What is the role of the CT pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations For patients with a low or PE
unlikely (Wells score 4) pretest probability for PE who require
additional diagnostic testing (eg positive D-dimer result or p
Volume June
ighly sensitive D-dimer test not available) a negativeultidetector CT pulmonary angiogram alone can be used to
xclude PELevel C recommendations (1) For patients with an
ntermediate pretest probability for PE and a negative CTulmonary angiogram result in whom a clinical concern for PEtill exists and CT venogram has not already been performedonsider additional diagnostic testing (eg D-dimer lowerxtremity imaging VQ scanning traditional pulmonaryrteriography) prior to exclusion of VTE disease
(2) For patients with a high pretest probability for PE and aegative CT angiogram result and CT venogram has notlready been performed perform additional diagnostic testingeg D-dimer lower extremity imaging VQ scanningraditional pulmonary arteriography) prior to exclusion of VTEiseaseA negative highly sensitive quantitative D-dimer result in
ombination with a negative multidetector CT pulmonaryngiogram result theoretically provides a posttest probability ofTE less than 1
Key wordsphrases for literature searches x-ray computedomography CT spiral computed tomography pulmonarymbolism sensitivity specificity probability likelihoodulmonary angiogram angiography thromboembolismutcome follow-up recurrent morbidity mortality falseegative false positive prognosis treatment outcome andariations and combinations of the key wordsphrases years001 through December 2009The use of the spiral CT angiogram for the visualization of
he pulmonary vasculature and the evaluation of PE was firstescribed in 199297 A single detector rotated in a spiral fashiont fixed intervals collecting data to generate vascular imagesuring a single breath holdSince that time the technology of this diagnostic modality
as advanced dramatically Multidetector CT scanners now useetween 4 64 or more channels (detectors) and rotate at muchaster gantry speeds (04 seconds versus 1 second per rotation)hus an older-generation single-detector CT with a 1-secondantry speed captures 1 slice per second whereas a 16-channelultidetector CT scanner rotating at a gantry speed of 04
econds captures 40 slices per second98 This in addition tohinner collimation allows for faster image acquisition lessotion artifact and ultimately higher-resolution images
mproved image acquisition protocols and resolution areelieved to result in improved diagnostic performanceIn 1992 Remy-Jardin et al97 in a Class III investigation
eported sensitivities and specificities of 100 and 96espectively for a single-detector CT for detection of PE Thisnding led to eager acceptance of the spiral CT angiogram intoiagnostic algorithms in the hope of simplifying theomplicated diagnostic workup of PE Since this initial studyultiple accuracy and outcomes studies in addition to meta-
nalyses and systematic reviews have been published on the
erformance of the CT pulmonary angiogram Unfortunately
Annals of Emergency Medicine 637
ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

eurgmdpmpiovoirpeh(a
wa3osPrsw2(
C
hcnCp
Pspwalps
cWaP
Clinical Policy
approximately 1 The authors concluded that these criteriacan permit safe D-dimer testing in the majority of ED patientswith suspected PE
There are no prospective outcome studies validating the useof the Kline rule in conjunction with D-dimer but 1 Class IIIstudy demonstrated a 21 decrease in CT scanning when theyinstituted this protocol46
Pisa ModelThe original Pisa investigation is a Class II study consisting
Figure Kline decision rule for excluding PE23 Reprintedfrom Annals of Emergency Medicine 39 Kline JA NelsonRD Jackson RE et al Criteria for the safe use of D-dimertesting in emergency department patients with suspectedpulmonary embolism a multicenter US study 144-1522002 Copyright from the American College of EmergencyPhysicians [2002]
Flow diagram demonstrating the Kline decision rule inselecting patients in whom D-dimer assay less than 500 ngml can reliably rule out PE This decision rule splits thepatients into 2 groups four fifths of whom are eligible for D-dimer testing (ldquosaferdquo patients with pretest probability of PE of133) and one fifth of whom are ineligible for D-dimertesting (ldquounsaferdquo patients with pretest probability of 421)
of 1100 consecutive patients with suspected PE who were W
Volume June
valuated at a single hospital in Pisa Italy24 All patientsnderwent a detailed clinical history physical examinationigorous interpretation of ECG and chest radiograph and bloodas measurements Using logistic regression techniques aathematical model for predicting probability of PE was
eveloped Probability was categorized as low (10robability of PE) intermediate (10 to 50 probability)oderately high (50 to 90 probability) and high (90
robability) Ten characteristics were associated with anncreased risk of PE male sex older age history of DVT acutenset dyspnea chest pain hemoptysis ECG signs of rightentricular overload radiographic signs of oligemia amputationf the hilar artery and pulmonary consolidations suggestive ofnfarction Five characteristics were associated with a decreasedisk previous cardiovascular or pulmonary disease feverulmonary consolidation other than infarction and pulmonarydema With this model 432 patients (39) were rated asaving low probability (4 PE) 283 (26) as intermediate22 PE) 72 (7) as moderately high probability (74 PE)nd 313 (28) as high probability (98 PE)
In the original Pisa model the highest regression coefficientsere for the chest radiograph findings (oligemia 386
mputation of hilar artery 392 and pulmonary infarction55) Because of the heavy reliance of the original Pisa modeln advanced chest radiograph interpretation skills beyond thekill level of the average physician Miniati et al25 refined theisa model in the same patient population after excluding chestadiograph from the final equation (Table 3) In the validationet of this Class II investigation the prevalence of PE was 2hen the predicted clinical probability was low (0 to 10)8 when moderate (11 to 50) 67 when substantial51 to 80) and 94 when high (81 to 100)
omparative Studies of Objective CriteriaThere are two Class II3247 and 3 Class III283031 studies that
ave evaluated performance of the various objective criteria Inomparing the Geneva score to the Wells score 3 studies foundo significant differences in performance though the study byhagnon et al28 suggested that the Geneva score overridden byhysician judgment may be more accurate283132
Miniati et al30 compared the Geneva score Wells score andisa model in 215 patients with suspected PE and foundtatistically significant differences in performance of the 3retest probability assessment tools Areas under the ROC curveere 054 075 and 094 for the Geneva score Wells score
nd Pisa model respectively However findings in this study areimited because of small sample size and the PE rate in thisatient population was extremely high (43) indicatingignificant patient selection bias
Runyon et al47 compared the Wells score with the Klineriteria in 2603 patients with a PE prevalence of 58 The
ells score identified 73 of patients as low risk (score 2)nd the Kline criteria identified 88 of patients as low risk TheE rates in these low-risk patients were 30 and 42 for the
ells and Kline criteria respectively
Annals of Emergency Medicine 633
wadt16gIp
oipgaoiRr(3s
ppap1ssi3ldquotrlcbp
pIgsi
L
r
ypP
Clinical Policy
Gestalt Clinical AssessmentGestalt clinical assessment is an unstructured (nonruled based)
estimate of the pretest probability of disease It is based on theclinicianrsquos training clinical experience and judgment Thisapproach has also been described as implicit in nature Theclinician using this approach surmises an overall impression of thepretest probability of PE and applies that impression to the decisionabout whether to pursue the diagnosis through objective testing
The Prospective Investigation of Pulmonary EmbolismDiagnosis (PIOPED) study was a prospective multi-institutioninvestigation designed to evaluate various conventional methodsfor diagnosing PE48 The PIOPED study is the first major studyreporting gestalt assessment As one element of the study the
Table 3 Regression coefficients and odds ratio for the Pisamodel as described by Miniati et al25 for estimatingprobability of pulmonary embolism according to clinical andECG findings Calculation of the clinical probability ofpulmonary embolism is performed as follows (1) Add all thecoefficients that apply to a given patient and the constantndash343 to obtain a sum score (2) the probability of pulmonaryembolism equals [1exp(ndashsum)]ndash1 Reprinted with permissionof the American Thoracic Society Copyright copy AmericanThoracic Society Miniati M Bottal M Monti S et al Simpleand accurate prediction of the clinical probability of pulmonaryembolism American Journal of Respiratory and Critical CareMedicine 2008178290-294 Official journal of the AmericanThoracic Society Diane Gern Publisher
Predictor Coefficient Odds Ratio 95 CI
Age y57ndash67 080 223 137ndash36368ndash74 087 238 141ndash40175 114 311 182ndash532Male sex 060 182 127ndash261Risk factorsImmobilization 042 153 108ndash215Deep venous thrombosis (ever) 064 190 123ndash295Preexisting diseasesCardiovascular ndash051 060 041ndash088Pulmonary ndash089 041 024ndash072SymptomsDyspnea (sudden onset) 200 738 518ndash1051Orthopnea ndash151 022 005ndash093Chest pain 101 274 193ndash388Fainting or syncope 066 193 125ndash298Hemoptysis 093 252 119ndash535SignsLeg swelling (unilateral) 080 223 135ndash370Fever 38degC (1004degF) ndash147 023 013ndash040Wheezes ndash120 030 014ndash066Crackles ndash061 054 035ndash083ElectrocardiogramAcute cor pulmonale 196 711 466ndash1087Constant ndash343
One or more of the following ECG abnormalities S1Q3T3 S1S2S3 negativeT waves in right precordial leads transient right bundle branch blockpseudoinfarction
clinicianrsquos assessment of the likelihood of PE from 0 to 100 t
634 Annals of Emergency Medicine
as recorded for 887 patients and was compared with PE statuss determined by angiogram and follow-up information Forata analysis low risk was considered pretest probability of 0o 19 intermediate risk 20 to 79 and high risk 80 to00 PE subsequently was diagnosed in 92 299 and78 of patients in the low- intermediate- and high-riskroups respectively Since the PIOPED study multiple ClassII studies have validated the usefulness of gestalt assessment ofretest probability in evaluating patients with suspected PE49-53
There have been several comparative studies of gestalt versusbjective criteria In a Class II study investigating potentialmpact of adjusting the D-dimer threshold Kabrhel et al37
rospectively performed pretest probability assessment usingestalt versus the Wells score in 7940 patients from 10cademic centers By gestalt pretest probability assessment 68f patients were low risk (15 pretest probability PE) 26ntermediate risk (15 to 40) and 6 high risk (40)ates of PE in these 3 subgroups were 3 10 and 33
espectively By the Wells score 69 of patients were low riskWells score 2) 28 intermediate (Wells score 2 to 6) and high risk (Wells score 6) Rates of PE in these 3ubgroups were 3 13 and 36 respectively
Sanson et al41 in a Class III study investigated pretestrobability assessment of gestalt versus the Wells score in 517atients with a 31 PE rate By gestalt pretest probabilityssessment 14 of patients were low risk (20 pretestrobability PE) 67 intermediate risk (20 to 80) and9 high risk (80 to 100) Rates of PE in these 3ubgroups were 19 29 and 46 respectively By the Wellscore 36 of patients were low risk (Wells score 2) 63ntermediate (Wells score 2 to 6) and 2 high risk (Wells score
6) Rates of PE in these 3 subgroups were 28 30 and8 respectively The authors conclude that both methodsalthough comparable perform disappointingly in categorizinghe pretest probability in patients with suspected PErdquo The highate of patients categorized as having intermediate risk and theow rate of patients categorized as having low risk in this studyompared with other studies suggest significant patient selectionias that may account for the poor performance in pretestrobability assessment by these 2 methods
Runyon et al47 in a Class II study compared gestalt pretestrobability assessment with the Wells criteria and the Kline rulen the low-risk group rate of PE was 26 30 and 42 forestalt Wells and Kline rule respectively Gestalt and Wellscore also were equivalent in pretest probability assessment forntermediate- and high-risk patients
imitationsSeveral issues concerning performance of clinical decision
ules and gestalt assessment have been raised in the literature(1) Interrater reliability Nordenholtz et al54 compared third-
ear emergency medicine resident and attending emergencyhysician interrater reliability for 271 patients with suspectedE Specific elements of the Wells and Kline risk-stratification
ools were studied Interrater agreement was concluded to be
Volume June
ea2
sdm2cditaupAatapsmawbsPkc
cpoby
P8wTeao3plnc3sr
Clinical Policy
moderate for DVT symptoms (054) immobilization(041) unexplained hypoxia (058) and PE more likelythan alternative diagnosis (05) good for hemoptysis(076) and very good for previous DVT (090)malignancy (087) and tachycardia (094) Runyon et al47
in a large single hospital study involving a subset of 154 patientsfound only moderate interrater agreement for gestalt clinicalassessment of low probability (06) and Wells score less than 2(047) and very good for Kline rule ldquosaferdquo (085)
(2) Clinical experience as a factor in the determination ofpretest probability of PE Accurate determination of the pretestprobability of PE appeared to trend with clinical experienceHowever the authors concluded that difference in accuracybetween the inexperienced and experienced physicians is notsufficiently large to distinguish between the 2 when determiningwhether clinical gestalt or a clinical prediction rule should beused to determine the pretest probability of PE55
Iles et al44 performed a survey to investigate whether numberof years since graduation from medical school affected pretestprobability score for the Geneva Wells and gestalt pretestprobability assessment The Geneva score was found to be themost consistent method of determining pretest probabilityGestalt assessment was inversely proportional to clinicalexperience suggesting that as physicians gain experience theyrecognize the difficulties in ruling out PE and are reluctant toexclude it on clinical grounds
(3) Knowledge and use of the rules Runyon et al56 surveyedemergency medicine clinicians and found that only half of allclinicians reporting familiarity with the rules use them in morethan 50 of applicable cases Spontaneous recall of the ruleswas low to moderate
ConclusionBoth objective criteria and gestalt assessment appear to
perform equally well for patients with suspected PE With theadvent of electronic charting future studies need to beperformed investigating the use of computer support aids infacilitating pretest probability assessment Studies also need tobe performed investigating use of pretest probability assessmentto guide subsequent diagnostic testing Finally studies need tobe performed to clarify the definitions of low- intermediate-and high-risk groups especially for gestalt assessment in whichstudies have used pretest probabilities ranging from 20 to80 as definition for intermediate probability
2 What is the utility of the PERC in the evaluation ofpatients with suspected PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations In patients with a low pretest
probability for suspected PE consider using the PERC toexclude the diagnosis based on historical and physical
examination data alone a
Volume June
Level C recommendations None specified
Key wordsphrases for literature searches PERC pulmonarymbolism rule-out criteria block rule pulmonary embolismnd variations and combinations of the key wordsphrases years000 through December 2009In 2004 Kline et al57 published a Class II prospective
tudy deriving clinical criteria to prevent unnecessaryiagnostic testing in ED patients with suspected PE In thisulticenter study with 3148 patients in a derivation cohort
1 descriptive variables relevant to the diagnosis of PE wereollected The primary outcome variable was the EDiagnosis of PE using a composite criterion standard
ncluding 90-day follow-up The overall prevalence of venoushromboembolism (VTE) was 11 Logistic regressionnalysis with stepwise backwards elimination of variables wassed to identify criteria that could predict a patientopulation estimated to have a prevalence of disease of 18t or below this low pretest probability of disease theuthors proposed that no further laboratory or radiographicesting would be needed to exclude the diagnosis of PElthough this threshold which was based on a previouslyublished method for calculating testing thresholds58 hasubsequently been more accurately estimated to be 14 by aore recent decision analytic model balancing the benefits
nd costs of using the PERC59 After their analysis 8 variablesere identified age younger than 50 years pulse rate less than 100eatsmin SaO2 greater than 94 (at sea level) no unilateral legwelling no hemoptysis no recent trauma or surgery no previousE or DVT and no hormone use These criteria have since becomenown as the PERC When all criteria are met a patient isonsidered to be PERC negative
In this same study the authors went on to internally validate theriteria in a separate patient cohort57 When applied to 1427atients considered to be low risk for PE by gestalt assessment 25f patients were PERC negative The criteria when considered toe a diagnostic test had 96 sensitivity and 27 specificityielding a LR- of 015 and a 14 false-negative rate
In 2008 Kline et al60 published a Class II validation study of theERC (Table 4) This multicenter prospective study enrolled138 patients Although limited by the number of eligible patientsho were not enrolled the authors made attempts to address thishe outcome measures were similar to those of the original study
xcept for follow-up occurring at 45 days as opposed to 90 daysnd the overall prevalence of VTE being 69 Sixty-seven percentf patients were classified as low risk by clinical gestalt and of these07 were PERC negative This equated to 204 of enrolledatients The sensitivity specificity and LR- for the PERC in the
ow-risk cohort were 947 219 and 012 respectively Ofote 35 of enrolled patients were PERC negative but notonsidered to be low risk by clinical gestalt This subgroup had a1 prevalence of VTE Although outcomes on this specificubgroup were not reported not all PERC negative patients are lowisk and the rulersquos applicability in these patients is unknown The
uthors concluded that the PERC could be used in combination
Annals of Emergency Medicine 635
pa
edk
DlSqbsrs(tapeii(oidhat
qdoCtpdpoCc9pos
tPrzi
Clinical Policy
with a low pretest probability to identify very low-risk patients forwhom the diagnosis of PE can be reliably excluded based onhistorical and physical examination data alone
In 2008 Wolf et al61 published a small Class III externalvalidation of the PERC This study was a post hoc analysis ofprospectively collected data on 120 consecutive ED patientswith a suspicion of PE The original database contained allPERC variables Outcome measures used were similar to thoseof the original study yielding a 12 prevalence of PE Whentheir entire patient population is considered regardless ofpretest probability the sensitivity and specificity were 100 and16 respectively When only the patients with low pretestprobability as defined by Wells Criteria are considered thespecificity increased to 22 The authors concluded that thePERC may identify a cohort of patients with suspected PE forwhom diagnostic testing beyond history and physicalexamination is not indicated
In each of the above 3 clinical studies even though patient datawere collected prospectively the application of the PERC rule wasperformed retrospectively As such there is no prospective outcomestudy of the use of the PERC rule for clinical decisionmaking Thislimits the strength of recommendations that can be made based onthe available evidence Future research should focus on the clinicalapplication of the PERC rule with measurement of acceptedoutcomes
3 What is the role of quantitative D-dimer testing in theexclusion of PE
Patient Management RecommendationsLevel A recommendations In patients with a low pretest
probability for PE a negative quantitative D-dimer assay resultcan be used to exclude PE
Table 4 The Pulmonary Embolism Rule Out Criteria (PERC)
The PERC criteria negative (PERCndash) require the clinician to answer noto the 8 questions below60 If a patient is low risk by gestaltimpression and PERCndash the posttest probability of venousthromboembolism is 2 Reprinted with permission Copyright copyJohn Wiley amp Sons Ltd Publisher Kline JA Courtney DM KabrhelC et al Prospective multicenter evaluation of the pulmonaryembolism rule-out criteria J Thromb Haemost 20086772-780
1 Is the patient older than 49 years of age2 Is the pulse rate greater than 99 beatsminndash13 Is the pulse oximetry reading 95 while the patient breathes
room air4 Is there a present history of hemoptysis5 Is the patient receiving exogenous estrogen6 Does the patient have a prior diagnosis of venous
thromboembolism (VTE)7 Has the patient had recent surgery or trauma (requiring
endotracheal intubation or hospitalization in the previous 4weeks)
8 Does the patient have unilateral leg swelling (visual observation ofasymmetry of the calves)
CHigh sensitivity (eg turbidimetric ELISA)
636 Annals of Emergency Medicine
Level B recommendations None specifiedLevel C recommendations In patients with an intermediate
retest probability for PE a negative quantitative D-dimerssay result may be used to exclude PE
Key wordsphrases for literature searches pulmonarymbolism fibrin fragment D sensitivity specificity D-dimerifferential diagnosis and variations and combinations of theey wordsphrases years 2001 through December 2009
This revision to the 2003 clinical policy1 focuses on quantitative-dimer tests that have become available to most hospital
aboratories across the United States The Clinical Policiesubcommittee on PE elected not to assess the evidence forualitative D-dimer tests (often used in point-of-care panels)ecause of problems with variability in interpretation and lowerensitivity reported in multiple studies62-65 However the onlyandomized clinical trial directly assessing the impact of a D-dimertrategy used a qualitative whole-blood agglutination testSimpliRED Agen Biomedical Ltd Brisbane Australia)66 In thisrial potential subjects suspected of having PE were first stratifiedccording to the Wells criteria and those with a low clinicalrobability and negative D-dimer test result were randomized toither no additional testing or VQ scanning Althoughnterpretation of results is limited due to early study closure thencidence of VTE during 6 months was similar among the 2 groups0182 versus 1185) Given that we were unable to identify anyther randomized controlled trials specifically designed to test thempact of a D-dimer strategy our recommendations are based onata from cohort studies and high-quality systematic reviews thatave been published since the original ACEP clinical policy1 Tovoid duplication cohort studies that were included in at least 1 ofhe systematic reviews are not reported in the Evidentiary Table
Class I systematic reviews assessing the test characteristics ofuantitative D-dimer tests in outpatient settings conclude that D-imer has excellent sensitivity (pooled sensitivity093 to 096) butnly moderate specificity (pooled specificity039 to 051)656768
lass I3542 and II 3769-75cohort studies that were not included inhese systematic reviews report similar results In patients with a lowretest probability (10) a negative ELISA or turbidimetric D-imer (LR-01) test result would be expected to decrease therobability of PE to approximately 1 These assumptions basedn the application of Bayesrsquo Theorem are supported by Class I35
lass II6973-75 and Class III38394676-79 studies that haveonsistently reported negative predictive values of approximately9 when D-dimer testing is applied to low-risk or ldquoPE unlikelyrdquoatient populations The American College of Physicians guidelinesn PE also support using D-dimer testing among low-risk patientsuspected of having PE8081
Despite consensus guidelines that recommend using D-dimeresting on patients with an intermediate pretest probability forE82 strong evidence supporting this approach is lacking Aetrospective analysis of 2 studies by Righini et al83 reportedero VTE events at 3-month follow-up for both low- andntermediate-risk groups however the upper limit for the 95
I was 1 for the low-probability group but extended up to
Volume June
hme
ipscea
na(td
caV
teponv2
tdad
hbfTgmstmIb
rrfidcma
Clinical Policy
5 for the intermediate-probability group Subsequent studiesthat have included intermediate pretest probability patientswithin their D-dimer strategy have either not reported resultsseparately737584 or have had too few patients in this subgroupto draw any firm conclusions777885
Given the relatively poor specificity of D-dimer testingvarious strategies have been suggested to limit the number offalse-positive tests that may lead to further unnecessarydiagnostic testing Retrospective subgroup analyses suggest thatD-dimer sensitivity remains fairly constant among varioussubpopulations but specificity decreases with certain comorbidconditions and advanced age678687 Two prospective studiesassessing the performance of D-dimer testing among cancerpatients suspected of having PE reported very low specificities(specificity018 to 021)8889 Pregnancy is also associated withincreasing concentrations of D-dimer particularly in womenbeyond the first trimester90 A restrictive approach to D-dimertesting whereby the elderly are excluded improves testspecificity8691 however this approach is unlikely to decreaseresource utilization since these patients would be expected to godirectly to some form of advanced imaging Adjusting the D-dimer test threshold based on the patientrsquos pretest probability orother variables (eg age) has been suggested as an alternativeapproach to improve the performance of D-dimertesting378792-94 Although raising the D-dimer test thresholdwould be expected to increase test specificity the associateddecrease in sensitivity may be unacceptable to most cliniciansand has not been prospectively studied95
Potential benefits of using a highly sensitive D-dimer as ascreening test include decreased cost and radiation exposurehowever if the test is ordered indiscriminately on patients withvery little or no risk for PE false-positive D-dimer results mayincrease the harms associated with unnecessary advancedimaging A formal decision analysis concluded that using D-dimer was not cost-effective if CT is readily available96
Although the authorsrsquo assumptions about the sensitivity andspecificity of quantitative D-dimer tests were consistent with thestudies included in the Evidentiary Table the authors state thattheir analysis was based on a patient suspected of having PEwithout other competing diagnoses96 It is rare in the EDsetting to have such a straightforward clinical presentation inwhich only 1 diagnosis is considered
Future research is needed for patients with an intermediatepretest probability of PE and to assess whether changing theD-dimer cutoff for different patient subgroups could improvespecificity without a clinically significant decrease in sensitivity
4 What is the role of the CT pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations For patients with a low or PE
unlikely (Wells score 4) pretest probability for PE who require
additional diagnostic testing (eg positive D-dimer result or p
Volume June
ighly sensitive D-dimer test not available) a negativeultidetector CT pulmonary angiogram alone can be used to
xclude PELevel C recommendations (1) For patients with an
ntermediate pretest probability for PE and a negative CTulmonary angiogram result in whom a clinical concern for PEtill exists and CT venogram has not already been performedonsider additional diagnostic testing (eg D-dimer lowerxtremity imaging VQ scanning traditional pulmonaryrteriography) prior to exclusion of VTE disease
(2) For patients with a high pretest probability for PE and aegative CT angiogram result and CT venogram has notlready been performed perform additional diagnostic testingeg D-dimer lower extremity imaging VQ scanningraditional pulmonary arteriography) prior to exclusion of VTEiseaseA negative highly sensitive quantitative D-dimer result in
ombination with a negative multidetector CT pulmonaryngiogram result theoretically provides a posttest probability ofTE less than 1
Key wordsphrases for literature searches x-ray computedomography CT spiral computed tomography pulmonarymbolism sensitivity specificity probability likelihoodulmonary angiogram angiography thromboembolismutcome follow-up recurrent morbidity mortality falseegative false positive prognosis treatment outcome andariations and combinations of the key wordsphrases years001 through December 2009The use of the spiral CT angiogram for the visualization of
he pulmonary vasculature and the evaluation of PE was firstescribed in 199297 A single detector rotated in a spiral fashiont fixed intervals collecting data to generate vascular imagesuring a single breath holdSince that time the technology of this diagnostic modality
as advanced dramatically Multidetector CT scanners now useetween 4 64 or more channels (detectors) and rotate at muchaster gantry speeds (04 seconds versus 1 second per rotation)hus an older-generation single-detector CT with a 1-secondantry speed captures 1 slice per second whereas a 16-channelultidetector CT scanner rotating at a gantry speed of 04
econds captures 40 slices per second98 This in addition tohinner collimation allows for faster image acquisition lessotion artifact and ultimately higher-resolution images
mproved image acquisition protocols and resolution areelieved to result in improved diagnostic performanceIn 1992 Remy-Jardin et al97 in a Class III investigation
eported sensitivities and specificities of 100 and 96espectively for a single-detector CT for detection of PE Thisnding led to eager acceptance of the spiral CT angiogram intoiagnostic algorithms in the hope of simplifying theomplicated diagnostic workup of PE Since this initial studyultiple accuracy and outcomes studies in addition to meta-
nalyses and systematic reviews have been published on the
erformance of the CT pulmonary angiogram Unfortunately
Annals of Emergency Medicine 637
ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

wadt16gIp
oipgaoiRr(3s
ppap1ssi3ldquotrlcbp
pIgsi
L
r
ypP
Clinical Policy
Gestalt Clinical AssessmentGestalt clinical assessment is an unstructured (nonruled based)
estimate of the pretest probability of disease It is based on theclinicianrsquos training clinical experience and judgment Thisapproach has also been described as implicit in nature Theclinician using this approach surmises an overall impression of thepretest probability of PE and applies that impression to the decisionabout whether to pursue the diagnosis through objective testing
The Prospective Investigation of Pulmonary EmbolismDiagnosis (PIOPED) study was a prospective multi-institutioninvestigation designed to evaluate various conventional methodsfor diagnosing PE48 The PIOPED study is the first major studyreporting gestalt assessment As one element of the study the
Table 3 Regression coefficients and odds ratio for the Pisamodel as described by Miniati et al25 for estimatingprobability of pulmonary embolism according to clinical andECG findings Calculation of the clinical probability ofpulmonary embolism is performed as follows (1) Add all thecoefficients that apply to a given patient and the constantndash343 to obtain a sum score (2) the probability of pulmonaryembolism equals [1exp(ndashsum)]ndash1 Reprinted with permissionof the American Thoracic Society Copyright copy AmericanThoracic Society Miniati M Bottal M Monti S et al Simpleand accurate prediction of the clinical probability of pulmonaryembolism American Journal of Respiratory and Critical CareMedicine 2008178290-294 Official journal of the AmericanThoracic Society Diane Gern Publisher
Predictor Coefficient Odds Ratio 95 CI
Age y57ndash67 080 223 137ndash36368ndash74 087 238 141ndash40175 114 311 182ndash532Male sex 060 182 127ndash261Risk factorsImmobilization 042 153 108ndash215Deep venous thrombosis (ever) 064 190 123ndash295Preexisting diseasesCardiovascular ndash051 060 041ndash088Pulmonary ndash089 041 024ndash072SymptomsDyspnea (sudden onset) 200 738 518ndash1051Orthopnea ndash151 022 005ndash093Chest pain 101 274 193ndash388Fainting or syncope 066 193 125ndash298Hemoptysis 093 252 119ndash535SignsLeg swelling (unilateral) 080 223 135ndash370Fever 38degC (1004degF) ndash147 023 013ndash040Wheezes ndash120 030 014ndash066Crackles ndash061 054 035ndash083ElectrocardiogramAcute cor pulmonale 196 711 466ndash1087Constant ndash343
One or more of the following ECG abnormalities S1Q3T3 S1S2S3 negativeT waves in right precordial leads transient right bundle branch blockpseudoinfarction
clinicianrsquos assessment of the likelihood of PE from 0 to 100 t
634 Annals of Emergency Medicine
as recorded for 887 patients and was compared with PE statuss determined by angiogram and follow-up information Forata analysis low risk was considered pretest probability of 0o 19 intermediate risk 20 to 79 and high risk 80 to00 PE subsequently was diagnosed in 92 299 and78 of patients in the low- intermediate- and high-riskroups respectively Since the PIOPED study multiple ClassII studies have validated the usefulness of gestalt assessment ofretest probability in evaluating patients with suspected PE49-53
There have been several comparative studies of gestalt versusbjective criteria In a Class II study investigating potentialmpact of adjusting the D-dimer threshold Kabrhel et al37
rospectively performed pretest probability assessment usingestalt versus the Wells score in 7940 patients from 10cademic centers By gestalt pretest probability assessment 68f patients were low risk (15 pretest probability PE) 26ntermediate risk (15 to 40) and 6 high risk (40)ates of PE in these 3 subgroups were 3 10 and 33
espectively By the Wells score 69 of patients were low riskWells score 2) 28 intermediate (Wells score 2 to 6) and high risk (Wells score 6) Rates of PE in these 3ubgroups were 3 13 and 36 respectively
Sanson et al41 in a Class III study investigated pretestrobability assessment of gestalt versus the Wells score in 517atients with a 31 PE rate By gestalt pretest probabilityssessment 14 of patients were low risk (20 pretestrobability PE) 67 intermediate risk (20 to 80) and9 high risk (80 to 100) Rates of PE in these 3ubgroups were 19 29 and 46 respectively By the Wellscore 36 of patients were low risk (Wells score 2) 63ntermediate (Wells score 2 to 6) and 2 high risk (Wells score
6) Rates of PE in these 3 subgroups were 28 30 and8 respectively The authors conclude that both methodsalthough comparable perform disappointingly in categorizinghe pretest probability in patients with suspected PErdquo The highate of patients categorized as having intermediate risk and theow rate of patients categorized as having low risk in this studyompared with other studies suggest significant patient selectionias that may account for the poor performance in pretestrobability assessment by these 2 methods
Runyon et al47 in a Class II study compared gestalt pretestrobability assessment with the Wells criteria and the Kline rulen the low-risk group rate of PE was 26 30 and 42 forestalt Wells and Kline rule respectively Gestalt and Wellscore also were equivalent in pretest probability assessment forntermediate- and high-risk patients
imitationsSeveral issues concerning performance of clinical decision
ules and gestalt assessment have been raised in the literature(1) Interrater reliability Nordenholtz et al54 compared third-
ear emergency medicine resident and attending emergencyhysician interrater reliability for 271 patients with suspectedE Specific elements of the Wells and Kline risk-stratification
ools were studied Interrater agreement was concluded to be
Volume June
ea2
sdm2cditaupAatapsmawbsPkc
cpoby
P8wTeao3plnc3sr
Clinical Policy
moderate for DVT symptoms (054) immobilization(041) unexplained hypoxia (058) and PE more likelythan alternative diagnosis (05) good for hemoptysis(076) and very good for previous DVT (090)malignancy (087) and tachycardia (094) Runyon et al47
in a large single hospital study involving a subset of 154 patientsfound only moderate interrater agreement for gestalt clinicalassessment of low probability (06) and Wells score less than 2(047) and very good for Kline rule ldquosaferdquo (085)
(2) Clinical experience as a factor in the determination ofpretest probability of PE Accurate determination of the pretestprobability of PE appeared to trend with clinical experienceHowever the authors concluded that difference in accuracybetween the inexperienced and experienced physicians is notsufficiently large to distinguish between the 2 when determiningwhether clinical gestalt or a clinical prediction rule should beused to determine the pretest probability of PE55
Iles et al44 performed a survey to investigate whether numberof years since graduation from medical school affected pretestprobability score for the Geneva Wells and gestalt pretestprobability assessment The Geneva score was found to be themost consistent method of determining pretest probabilityGestalt assessment was inversely proportional to clinicalexperience suggesting that as physicians gain experience theyrecognize the difficulties in ruling out PE and are reluctant toexclude it on clinical grounds
(3) Knowledge and use of the rules Runyon et al56 surveyedemergency medicine clinicians and found that only half of allclinicians reporting familiarity with the rules use them in morethan 50 of applicable cases Spontaneous recall of the ruleswas low to moderate
ConclusionBoth objective criteria and gestalt assessment appear to
perform equally well for patients with suspected PE With theadvent of electronic charting future studies need to beperformed investigating the use of computer support aids infacilitating pretest probability assessment Studies also need tobe performed investigating use of pretest probability assessmentto guide subsequent diagnostic testing Finally studies need tobe performed to clarify the definitions of low- intermediate-and high-risk groups especially for gestalt assessment in whichstudies have used pretest probabilities ranging from 20 to80 as definition for intermediate probability
2 What is the utility of the PERC in the evaluation ofpatients with suspected PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations In patients with a low pretest
probability for suspected PE consider using the PERC toexclude the diagnosis based on historical and physical
examination data alone a
Volume June
Level C recommendations None specified
Key wordsphrases for literature searches PERC pulmonarymbolism rule-out criteria block rule pulmonary embolismnd variations and combinations of the key wordsphrases years000 through December 2009In 2004 Kline et al57 published a Class II prospective
tudy deriving clinical criteria to prevent unnecessaryiagnostic testing in ED patients with suspected PE In thisulticenter study with 3148 patients in a derivation cohort
1 descriptive variables relevant to the diagnosis of PE wereollected The primary outcome variable was the EDiagnosis of PE using a composite criterion standard
ncluding 90-day follow-up The overall prevalence of venoushromboembolism (VTE) was 11 Logistic regressionnalysis with stepwise backwards elimination of variables wassed to identify criteria that could predict a patientopulation estimated to have a prevalence of disease of 18t or below this low pretest probability of disease theuthors proposed that no further laboratory or radiographicesting would be needed to exclude the diagnosis of PElthough this threshold which was based on a previouslyublished method for calculating testing thresholds58 hasubsequently been more accurately estimated to be 14 by aore recent decision analytic model balancing the benefits
nd costs of using the PERC59 After their analysis 8 variablesere identified age younger than 50 years pulse rate less than 100eatsmin SaO2 greater than 94 (at sea level) no unilateral legwelling no hemoptysis no recent trauma or surgery no previousE or DVT and no hormone use These criteria have since becomenown as the PERC When all criteria are met a patient isonsidered to be PERC negative
In this same study the authors went on to internally validate theriteria in a separate patient cohort57 When applied to 1427atients considered to be low risk for PE by gestalt assessment 25f patients were PERC negative The criteria when considered toe a diagnostic test had 96 sensitivity and 27 specificityielding a LR- of 015 and a 14 false-negative rate
In 2008 Kline et al60 published a Class II validation study of theERC (Table 4) This multicenter prospective study enrolled138 patients Although limited by the number of eligible patientsho were not enrolled the authors made attempts to address thishe outcome measures were similar to those of the original study
xcept for follow-up occurring at 45 days as opposed to 90 daysnd the overall prevalence of VTE being 69 Sixty-seven percentf patients were classified as low risk by clinical gestalt and of these07 were PERC negative This equated to 204 of enrolledatients The sensitivity specificity and LR- for the PERC in the
ow-risk cohort were 947 219 and 012 respectively Ofote 35 of enrolled patients were PERC negative but notonsidered to be low risk by clinical gestalt This subgroup had a1 prevalence of VTE Although outcomes on this specificubgroup were not reported not all PERC negative patients are lowisk and the rulersquos applicability in these patients is unknown The
uthors concluded that the PERC could be used in combination
Annals of Emergency Medicine 635
pa
edk
DlSqbsrs(tapeii(oidhat
qdoCtpdpoCc9pos
tPrzi
Clinical Policy
with a low pretest probability to identify very low-risk patients forwhom the diagnosis of PE can be reliably excluded based onhistorical and physical examination data alone
In 2008 Wolf et al61 published a small Class III externalvalidation of the PERC This study was a post hoc analysis ofprospectively collected data on 120 consecutive ED patientswith a suspicion of PE The original database contained allPERC variables Outcome measures used were similar to thoseof the original study yielding a 12 prevalence of PE Whentheir entire patient population is considered regardless ofpretest probability the sensitivity and specificity were 100 and16 respectively When only the patients with low pretestprobability as defined by Wells Criteria are considered thespecificity increased to 22 The authors concluded that thePERC may identify a cohort of patients with suspected PE forwhom diagnostic testing beyond history and physicalexamination is not indicated
In each of the above 3 clinical studies even though patient datawere collected prospectively the application of the PERC rule wasperformed retrospectively As such there is no prospective outcomestudy of the use of the PERC rule for clinical decisionmaking Thislimits the strength of recommendations that can be made based onthe available evidence Future research should focus on the clinicalapplication of the PERC rule with measurement of acceptedoutcomes
3 What is the role of quantitative D-dimer testing in theexclusion of PE
Patient Management RecommendationsLevel A recommendations In patients with a low pretest
probability for PE a negative quantitative D-dimer assay resultcan be used to exclude PE
Table 4 The Pulmonary Embolism Rule Out Criteria (PERC)
The PERC criteria negative (PERCndash) require the clinician to answer noto the 8 questions below60 If a patient is low risk by gestaltimpression and PERCndash the posttest probability of venousthromboembolism is 2 Reprinted with permission Copyright copyJohn Wiley amp Sons Ltd Publisher Kline JA Courtney DM KabrhelC et al Prospective multicenter evaluation of the pulmonaryembolism rule-out criteria J Thromb Haemost 20086772-780
1 Is the patient older than 49 years of age2 Is the pulse rate greater than 99 beatsminndash13 Is the pulse oximetry reading 95 while the patient breathes
room air4 Is there a present history of hemoptysis5 Is the patient receiving exogenous estrogen6 Does the patient have a prior diagnosis of venous
thromboembolism (VTE)7 Has the patient had recent surgery or trauma (requiring
endotracheal intubation or hospitalization in the previous 4weeks)
8 Does the patient have unilateral leg swelling (visual observation ofasymmetry of the calves)
CHigh sensitivity (eg turbidimetric ELISA)
636 Annals of Emergency Medicine
Level B recommendations None specifiedLevel C recommendations In patients with an intermediate
retest probability for PE a negative quantitative D-dimerssay result may be used to exclude PE
Key wordsphrases for literature searches pulmonarymbolism fibrin fragment D sensitivity specificity D-dimerifferential diagnosis and variations and combinations of theey wordsphrases years 2001 through December 2009
This revision to the 2003 clinical policy1 focuses on quantitative-dimer tests that have become available to most hospital
aboratories across the United States The Clinical Policiesubcommittee on PE elected not to assess the evidence forualitative D-dimer tests (often used in point-of-care panels)ecause of problems with variability in interpretation and lowerensitivity reported in multiple studies62-65 However the onlyandomized clinical trial directly assessing the impact of a D-dimertrategy used a qualitative whole-blood agglutination testSimpliRED Agen Biomedical Ltd Brisbane Australia)66 In thisrial potential subjects suspected of having PE were first stratifiedccording to the Wells criteria and those with a low clinicalrobability and negative D-dimer test result were randomized toither no additional testing or VQ scanning Althoughnterpretation of results is limited due to early study closure thencidence of VTE during 6 months was similar among the 2 groups0182 versus 1185) Given that we were unable to identify anyther randomized controlled trials specifically designed to test thempact of a D-dimer strategy our recommendations are based onata from cohort studies and high-quality systematic reviews thatave been published since the original ACEP clinical policy1 Tovoid duplication cohort studies that were included in at least 1 ofhe systematic reviews are not reported in the Evidentiary Table
Class I systematic reviews assessing the test characteristics ofuantitative D-dimer tests in outpatient settings conclude that D-imer has excellent sensitivity (pooled sensitivity093 to 096) butnly moderate specificity (pooled specificity039 to 051)656768
lass I3542 and II 3769-75cohort studies that were not included inhese systematic reviews report similar results In patients with a lowretest probability (10) a negative ELISA or turbidimetric D-imer (LR-01) test result would be expected to decrease therobability of PE to approximately 1 These assumptions basedn the application of Bayesrsquo Theorem are supported by Class I35
lass II6973-75 and Class III38394676-79 studies that haveonsistently reported negative predictive values of approximately9 when D-dimer testing is applied to low-risk or ldquoPE unlikelyrdquoatient populations The American College of Physicians guidelinesn PE also support using D-dimer testing among low-risk patientsuspected of having PE8081
Despite consensus guidelines that recommend using D-dimeresting on patients with an intermediate pretest probability forE82 strong evidence supporting this approach is lacking Aetrospective analysis of 2 studies by Righini et al83 reportedero VTE events at 3-month follow-up for both low- andntermediate-risk groups however the upper limit for the 95
I was 1 for the low-probability group but extended up to
Volume June
hme
ipscea
na(td
caV
teponv2
tdad
hbfTgmstmIb
rrfidcma
Clinical Policy
5 for the intermediate-probability group Subsequent studiesthat have included intermediate pretest probability patientswithin their D-dimer strategy have either not reported resultsseparately737584 or have had too few patients in this subgroupto draw any firm conclusions777885
Given the relatively poor specificity of D-dimer testingvarious strategies have been suggested to limit the number offalse-positive tests that may lead to further unnecessarydiagnostic testing Retrospective subgroup analyses suggest thatD-dimer sensitivity remains fairly constant among varioussubpopulations but specificity decreases with certain comorbidconditions and advanced age678687 Two prospective studiesassessing the performance of D-dimer testing among cancerpatients suspected of having PE reported very low specificities(specificity018 to 021)8889 Pregnancy is also associated withincreasing concentrations of D-dimer particularly in womenbeyond the first trimester90 A restrictive approach to D-dimertesting whereby the elderly are excluded improves testspecificity8691 however this approach is unlikely to decreaseresource utilization since these patients would be expected to godirectly to some form of advanced imaging Adjusting the D-dimer test threshold based on the patientrsquos pretest probability orother variables (eg age) has been suggested as an alternativeapproach to improve the performance of D-dimertesting378792-94 Although raising the D-dimer test thresholdwould be expected to increase test specificity the associateddecrease in sensitivity may be unacceptable to most cliniciansand has not been prospectively studied95
Potential benefits of using a highly sensitive D-dimer as ascreening test include decreased cost and radiation exposurehowever if the test is ordered indiscriminately on patients withvery little or no risk for PE false-positive D-dimer results mayincrease the harms associated with unnecessary advancedimaging A formal decision analysis concluded that using D-dimer was not cost-effective if CT is readily available96
Although the authorsrsquo assumptions about the sensitivity andspecificity of quantitative D-dimer tests were consistent with thestudies included in the Evidentiary Table the authors state thattheir analysis was based on a patient suspected of having PEwithout other competing diagnoses96 It is rare in the EDsetting to have such a straightforward clinical presentation inwhich only 1 diagnosis is considered
Future research is needed for patients with an intermediatepretest probability of PE and to assess whether changing theD-dimer cutoff for different patient subgroups could improvespecificity without a clinically significant decrease in sensitivity
4 What is the role of the CT pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations For patients with a low or PE
unlikely (Wells score 4) pretest probability for PE who require
additional diagnostic testing (eg positive D-dimer result or p
Volume June
ighly sensitive D-dimer test not available) a negativeultidetector CT pulmonary angiogram alone can be used to
xclude PELevel C recommendations (1) For patients with an
ntermediate pretest probability for PE and a negative CTulmonary angiogram result in whom a clinical concern for PEtill exists and CT venogram has not already been performedonsider additional diagnostic testing (eg D-dimer lowerxtremity imaging VQ scanning traditional pulmonaryrteriography) prior to exclusion of VTE disease
(2) For patients with a high pretest probability for PE and aegative CT angiogram result and CT venogram has notlready been performed perform additional diagnostic testingeg D-dimer lower extremity imaging VQ scanningraditional pulmonary arteriography) prior to exclusion of VTEiseaseA negative highly sensitive quantitative D-dimer result in
ombination with a negative multidetector CT pulmonaryngiogram result theoretically provides a posttest probability ofTE less than 1
Key wordsphrases for literature searches x-ray computedomography CT spiral computed tomography pulmonarymbolism sensitivity specificity probability likelihoodulmonary angiogram angiography thromboembolismutcome follow-up recurrent morbidity mortality falseegative false positive prognosis treatment outcome andariations and combinations of the key wordsphrases years001 through December 2009The use of the spiral CT angiogram for the visualization of
he pulmonary vasculature and the evaluation of PE was firstescribed in 199297 A single detector rotated in a spiral fashiont fixed intervals collecting data to generate vascular imagesuring a single breath holdSince that time the technology of this diagnostic modality
as advanced dramatically Multidetector CT scanners now useetween 4 64 or more channels (detectors) and rotate at muchaster gantry speeds (04 seconds versus 1 second per rotation)hus an older-generation single-detector CT with a 1-secondantry speed captures 1 slice per second whereas a 16-channelultidetector CT scanner rotating at a gantry speed of 04
econds captures 40 slices per second98 This in addition tohinner collimation allows for faster image acquisition lessotion artifact and ultimately higher-resolution images
mproved image acquisition protocols and resolution areelieved to result in improved diagnostic performanceIn 1992 Remy-Jardin et al97 in a Class III investigation
eported sensitivities and specificities of 100 and 96espectively for a single-detector CT for detection of PE Thisnding led to eager acceptance of the spiral CT angiogram intoiagnostic algorithms in the hope of simplifying theomplicated diagnostic workup of PE Since this initial studyultiple accuracy and outcomes studies in addition to meta-
nalyses and systematic reviews have been published on the
erformance of the CT pulmonary angiogram Unfortunately
Annals of Emergency Medicine 637
ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

ea2
sdm2cditaupAatapsmawbsPkc
cpoby
P8wTeao3plnc3sr
Clinical Policy
moderate for DVT symptoms (054) immobilization(041) unexplained hypoxia (058) and PE more likelythan alternative diagnosis (05) good for hemoptysis(076) and very good for previous DVT (090)malignancy (087) and tachycardia (094) Runyon et al47
in a large single hospital study involving a subset of 154 patientsfound only moderate interrater agreement for gestalt clinicalassessment of low probability (06) and Wells score less than 2(047) and very good for Kline rule ldquosaferdquo (085)
(2) Clinical experience as a factor in the determination ofpretest probability of PE Accurate determination of the pretestprobability of PE appeared to trend with clinical experienceHowever the authors concluded that difference in accuracybetween the inexperienced and experienced physicians is notsufficiently large to distinguish between the 2 when determiningwhether clinical gestalt or a clinical prediction rule should beused to determine the pretest probability of PE55
Iles et al44 performed a survey to investigate whether numberof years since graduation from medical school affected pretestprobability score for the Geneva Wells and gestalt pretestprobability assessment The Geneva score was found to be themost consistent method of determining pretest probabilityGestalt assessment was inversely proportional to clinicalexperience suggesting that as physicians gain experience theyrecognize the difficulties in ruling out PE and are reluctant toexclude it on clinical grounds
(3) Knowledge and use of the rules Runyon et al56 surveyedemergency medicine clinicians and found that only half of allclinicians reporting familiarity with the rules use them in morethan 50 of applicable cases Spontaneous recall of the ruleswas low to moderate
ConclusionBoth objective criteria and gestalt assessment appear to
perform equally well for patients with suspected PE With theadvent of electronic charting future studies need to beperformed investigating the use of computer support aids infacilitating pretest probability assessment Studies also need tobe performed investigating use of pretest probability assessmentto guide subsequent diagnostic testing Finally studies need tobe performed to clarify the definitions of low- intermediate-and high-risk groups especially for gestalt assessment in whichstudies have used pretest probabilities ranging from 20 to80 as definition for intermediate probability
2 What is the utility of the PERC in the evaluation ofpatients with suspected PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations In patients with a low pretest
probability for suspected PE consider using the PERC toexclude the diagnosis based on historical and physical
examination data alone a
Volume June
Level C recommendations None specified
Key wordsphrases for literature searches PERC pulmonarymbolism rule-out criteria block rule pulmonary embolismnd variations and combinations of the key wordsphrases years000 through December 2009In 2004 Kline et al57 published a Class II prospective
tudy deriving clinical criteria to prevent unnecessaryiagnostic testing in ED patients with suspected PE In thisulticenter study with 3148 patients in a derivation cohort
1 descriptive variables relevant to the diagnosis of PE wereollected The primary outcome variable was the EDiagnosis of PE using a composite criterion standard
ncluding 90-day follow-up The overall prevalence of venoushromboembolism (VTE) was 11 Logistic regressionnalysis with stepwise backwards elimination of variables wassed to identify criteria that could predict a patientopulation estimated to have a prevalence of disease of 18t or below this low pretest probability of disease theuthors proposed that no further laboratory or radiographicesting would be needed to exclude the diagnosis of PElthough this threshold which was based on a previouslyublished method for calculating testing thresholds58 hasubsequently been more accurately estimated to be 14 by aore recent decision analytic model balancing the benefits
nd costs of using the PERC59 After their analysis 8 variablesere identified age younger than 50 years pulse rate less than 100eatsmin SaO2 greater than 94 (at sea level) no unilateral legwelling no hemoptysis no recent trauma or surgery no previousE or DVT and no hormone use These criteria have since becomenown as the PERC When all criteria are met a patient isonsidered to be PERC negative
In this same study the authors went on to internally validate theriteria in a separate patient cohort57 When applied to 1427atients considered to be low risk for PE by gestalt assessment 25f patients were PERC negative The criteria when considered toe a diagnostic test had 96 sensitivity and 27 specificityielding a LR- of 015 and a 14 false-negative rate
In 2008 Kline et al60 published a Class II validation study of theERC (Table 4) This multicenter prospective study enrolled138 patients Although limited by the number of eligible patientsho were not enrolled the authors made attempts to address thishe outcome measures were similar to those of the original study
xcept for follow-up occurring at 45 days as opposed to 90 daysnd the overall prevalence of VTE being 69 Sixty-seven percentf patients were classified as low risk by clinical gestalt and of these07 were PERC negative This equated to 204 of enrolledatients The sensitivity specificity and LR- for the PERC in the
ow-risk cohort were 947 219 and 012 respectively Ofote 35 of enrolled patients were PERC negative but notonsidered to be low risk by clinical gestalt This subgroup had a1 prevalence of VTE Although outcomes on this specificubgroup were not reported not all PERC negative patients are lowisk and the rulersquos applicability in these patients is unknown The
uthors concluded that the PERC could be used in combination
Annals of Emergency Medicine 635
pa
edk
DlSqbsrs(tapeii(oidhat
qdoCtpdpoCc9pos
tPrzi
Clinical Policy
with a low pretest probability to identify very low-risk patients forwhom the diagnosis of PE can be reliably excluded based onhistorical and physical examination data alone
In 2008 Wolf et al61 published a small Class III externalvalidation of the PERC This study was a post hoc analysis ofprospectively collected data on 120 consecutive ED patientswith a suspicion of PE The original database contained allPERC variables Outcome measures used were similar to thoseof the original study yielding a 12 prevalence of PE Whentheir entire patient population is considered regardless ofpretest probability the sensitivity and specificity were 100 and16 respectively When only the patients with low pretestprobability as defined by Wells Criteria are considered thespecificity increased to 22 The authors concluded that thePERC may identify a cohort of patients with suspected PE forwhom diagnostic testing beyond history and physicalexamination is not indicated
In each of the above 3 clinical studies even though patient datawere collected prospectively the application of the PERC rule wasperformed retrospectively As such there is no prospective outcomestudy of the use of the PERC rule for clinical decisionmaking Thislimits the strength of recommendations that can be made based onthe available evidence Future research should focus on the clinicalapplication of the PERC rule with measurement of acceptedoutcomes
3 What is the role of quantitative D-dimer testing in theexclusion of PE
Patient Management RecommendationsLevel A recommendations In patients with a low pretest
probability for PE a negative quantitative D-dimer assay resultcan be used to exclude PE
Table 4 The Pulmonary Embolism Rule Out Criteria (PERC)
The PERC criteria negative (PERCndash) require the clinician to answer noto the 8 questions below60 If a patient is low risk by gestaltimpression and PERCndash the posttest probability of venousthromboembolism is 2 Reprinted with permission Copyright copyJohn Wiley amp Sons Ltd Publisher Kline JA Courtney DM KabrhelC et al Prospective multicenter evaluation of the pulmonaryembolism rule-out criteria J Thromb Haemost 20086772-780
1 Is the patient older than 49 years of age2 Is the pulse rate greater than 99 beatsminndash13 Is the pulse oximetry reading 95 while the patient breathes
room air4 Is there a present history of hemoptysis5 Is the patient receiving exogenous estrogen6 Does the patient have a prior diagnosis of venous
thromboembolism (VTE)7 Has the patient had recent surgery or trauma (requiring
endotracheal intubation or hospitalization in the previous 4weeks)
8 Does the patient have unilateral leg swelling (visual observation ofasymmetry of the calves)
CHigh sensitivity (eg turbidimetric ELISA)
636 Annals of Emergency Medicine
Level B recommendations None specifiedLevel C recommendations In patients with an intermediate
retest probability for PE a negative quantitative D-dimerssay result may be used to exclude PE
Key wordsphrases for literature searches pulmonarymbolism fibrin fragment D sensitivity specificity D-dimerifferential diagnosis and variations and combinations of theey wordsphrases years 2001 through December 2009
This revision to the 2003 clinical policy1 focuses on quantitative-dimer tests that have become available to most hospital
aboratories across the United States The Clinical Policiesubcommittee on PE elected not to assess the evidence forualitative D-dimer tests (often used in point-of-care panels)ecause of problems with variability in interpretation and lowerensitivity reported in multiple studies62-65 However the onlyandomized clinical trial directly assessing the impact of a D-dimertrategy used a qualitative whole-blood agglutination testSimpliRED Agen Biomedical Ltd Brisbane Australia)66 In thisrial potential subjects suspected of having PE were first stratifiedccording to the Wells criteria and those with a low clinicalrobability and negative D-dimer test result were randomized toither no additional testing or VQ scanning Althoughnterpretation of results is limited due to early study closure thencidence of VTE during 6 months was similar among the 2 groups0182 versus 1185) Given that we were unable to identify anyther randomized controlled trials specifically designed to test thempact of a D-dimer strategy our recommendations are based onata from cohort studies and high-quality systematic reviews thatave been published since the original ACEP clinical policy1 Tovoid duplication cohort studies that were included in at least 1 ofhe systematic reviews are not reported in the Evidentiary Table
Class I systematic reviews assessing the test characteristics ofuantitative D-dimer tests in outpatient settings conclude that D-imer has excellent sensitivity (pooled sensitivity093 to 096) butnly moderate specificity (pooled specificity039 to 051)656768
lass I3542 and II 3769-75cohort studies that were not included inhese systematic reviews report similar results In patients with a lowretest probability (10) a negative ELISA or turbidimetric D-imer (LR-01) test result would be expected to decrease therobability of PE to approximately 1 These assumptions basedn the application of Bayesrsquo Theorem are supported by Class I35
lass II6973-75 and Class III38394676-79 studies that haveonsistently reported negative predictive values of approximately9 when D-dimer testing is applied to low-risk or ldquoPE unlikelyrdquoatient populations The American College of Physicians guidelinesn PE also support using D-dimer testing among low-risk patientsuspected of having PE8081
Despite consensus guidelines that recommend using D-dimeresting on patients with an intermediate pretest probability forE82 strong evidence supporting this approach is lacking Aetrospective analysis of 2 studies by Righini et al83 reportedero VTE events at 3-month follow-up for both low- andntermediate-risk groups however the upper limit for the 95
I was 1 for the low-probability group but extended up to
Volume June
hme
ipscea
na(td
caV
teponv2
tdad
hbfTgmstmIb
rrfidcma
Clinical Policy
5 for the intermediate-probability group Subsequent studiesthat have included intermediate pretest probability patientswithin their D-dimer strategy have either not reported resultsseparately737584 or have had too few patients in this subgroupto draw any firm conclusions777885
Given the relatively poor specificity of D-dimer testingvarious strategies have been suggested to limit the number offalse-positive tests that may lead to further unnecessarydiagnostic testing Retrospective subgroup analyses suggest thatD-dimer sensitivity remains fairly constant among varioussubpopulations but specificity decreases with certain comorbidconditions and advanced age678687 Two prospective studiesassessing the performance of D-dimer testing among cancerpatients suspected of having PE reported very low specificities(specificity018 to 021)8889 Pregnancy is also associated withincreasing concentrations of D-dimer particularly in womenbeyond the first trimester90 A restrictive approach to D-dimertesting whereby the elderly are excluded improves testspecificity8691 however this approach is unlikely to decreaseresource utilization since these patients would be expected to godirectly to some form of advanced imaging Adjusting the D-dimer test threshold based on the patientrsquos pretest probability orother variables (eg age) has been suggested as an alternativeapproach to improve the performance of D-dimertesting378792-94 Although raising the D-dimer test thresholdwould be expected to increase test specificity the associateddecrease in sensitivity may be unacceptable to most cliniciansand has not been prospectively studied95
Potential benefits of using a highly sensitive D-dimer as ascreening test include decreased cost and radiation exposurehowever if the test is ordered indiscriminately on patients withvery little or no risk for PE false-positive D-dimer results mayincrease the harms associated with unnecessary advancedimaging A formal decision analysis concluded that using D-dimer was not cost-effective if CT is readily available96
Although the authorsrsquo assumptions about the sensitivity andspecificity of quantitative D-dimer tests were consistent with thestudies included in the Evidentiary Table the authors state thattheir analysis was based on a patient suspected of having PEwithout other competing diagnoses96 It is rare in the EDsetting to have such a straightforward clinical presentation inwhich only 1 diagnosis is considered
Future research is needed for patients with an intermediatepretest probability of PE and to assess whether changing theD-dimer cutoff for different patient subgroups could improvespecificity without a clinically significant decrease in sensitivity
4 What is the role of the CT pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations For patients with a low or PE
unlikely (Wells score 4) pretest probability for PE who require
additional diagnostic testing (eg positive D-dimer result or p
Volume June
ighly sensitive D-dimer test not available) a negativeultidetector CT pulmonary angiogram alone can be used to
xclude PELevel C recommendations (1) For patients with an
ntermediate pretest probability for PE and a negative CTulmonary angiogram result in whom a clinical concern for PEtill exists and CT venogram has not already been performedonsider additional diagnostic testing (eg D-dimer lowerxtremity imaging VQ scanning traditional pulmonaryrteriography) prior to exclusion of VTE disease
(2) For patients with a high pretest probability for PE and aegative CT angiogram result and CT venogram has notlready been performed perform additional diagnostic testingeg D-dimer lower extremity imaging VQ scanningraditional pulmonary arteriography) prior to exclusion of VTEiseaseA negative highly sensitive quantitative D-dimer result in
ombination with a negative multidetector CT pulmonaryngiogram result theoretically provides a posttest probability ofTE less than 1
Key wordsphrases for literature searches x-ray computedomography CT spiral computed tomography pulmonarymbolism sensitivity specificity probability likelihoodulmonary angiogram angiography thromboembolismutcome follow-up recurrent morbidity mortality falseegative false positive prognosis treatment outcome andariations and combinations of the key wordsphrases years001 through December 2009The use of the spiral CT angiogram for the visualization of
he pulmonary vasculature and the evaluation of PE was firstescribed in 199297 A single detector rotated in a spiral fashiont fixed intervals collecting data to generate vascular imagesuring a single breath holdSince that time the technology of this diagnostic modality
as advanced dramatically Multidetector CT scanners now useetween 4 64 or more channels (detectors) and rotate at muchaster gantry speeds (04 seconds versus 1 second per rotation)hus an older-generation single-detector CT with a 1-secondantry speed captures 1 slice per second whereas a 16-channelultidetector CT scanner rotating at a gantry speed of 04
econds captures 40 slices per second98 This in addition tohinner collimation allows for faster image acquisition lessotion artifact and ultimately higher-resolution images
mproved image acquisition protocols and resolution areelieved to result in improved diagnostic performanceIn 1992 Remy-Jardin et al97 in a Class III investigation
eported sensitivities and specificities of 100 and 96espectively for a single-detector CT for detection of PE Thisnding led to eager acceptance of the spiral CT angiogram intoiagnostic algorithms in the hope of simplifying theomplicated diagnostic workup of PE Since this initial studyultiple accuracy and outcomes studies in addition to meta-
nalyses and systematic reviews have been published on the
erformance of the CT pulmonary angiogram Unfortunately
Annals of Emergency Medicine 637
ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

pa
edk
DlSqbsrs(tapeii(oidhat
qdoCtpdpoCc9pos
tPrzi
Clinical Policy
with a low pretest probability to identify very low-risk patients forwhom the diagnosis of PE can be reliably excluded based onhistorical and physical examination data alone
In 2008 Wolf et al61 published a small Class III externalvalidation of the PERC This study was a post hoc analysis ofprospectively collected data on 120 consecutive ED patientswith a suspicion of PE The original database contained allPERC variables Outcome measures used were similar to thoseof the original study yielding a 12 prevalence of PE Whentheir entire patient population is considered regardless ofpretest probability the sensitivity and specificity were 100 and16 respectively When only the patients with low pretestprobability as defined by Wells Criteria are considered thespecificity increased to 22 The authors concluded that thePERC may identify a cohort of patients with suspected PE forwhom diagnostic testing beyond history and physicalexamination is not indicated
In each of the above 3 clinical studies even though patient datawere collected prospectively the application of the PERC rule wasperformed retrospectively As such there is no prospective outcomestudy of the use of the PERC rule for clinical decisionmaking Thislimits the strength of recommendations that can be made based onthe available evidence Future research should focus on the clinicalapplication of the PERC rule with measurement of acceptedoutcomes
3 What is the role of quantitative D-dimer testing in theexclusion of PE
Patient Management RecommendationsLevel A recommendations In patients with a low pretest
probability for PE a negative quantitative D-dimer assay resultcan be used to exclude PE
Table 4 The Pulmonary Embolism Rule Out Criteria (PERC)
The PERC criteria negative (PERCndash) require the clinician to answer noto the 8 questions below60 If a patient is low risk by gestaltimpression and PERCndash the posttest probability of venousthromboembolism is 2 Reprinted with permission Copyright copyJohn Wiley amp Sons Ltd Publisher Kline JA Courtney DM KabrhelC et al Prospective multicenter evaluation of the pulmonaryembolism rule-out criteria J Thromb Haemost 20086772-780
1 Is the patient older than 49 years of age2 Is the pulse rate greater than 99 beatsminndash13 Is the pulse oximetry reading 95 while the patient breathes
room air4 Is there a present history of hemoptysis5 Is the patient receiving exogenous estrogen6 Does the patient have a prior diagnosis of venous
thromboembolism (VTE)7 Has the patient had recent surgery or trauma (requiring
endotracheal intubation or hospitalization in the previous 4weeks)
8 Does the patient have unilateral leg swelling (visual observation ofasymmetry of the calves)
CHigh sensitivity (eg turbidimetric ELISA)
636 Annals of Emergency Medicine
Level B recommendations None specifiedLevel C recommendations In patients with an intermediate
retest probability for PE a negative quantitative D-dimerssay result may be used to exclude PE
Key wordsphrases for literature searches pulmonarymbolism fibrin fragment D sensitivity specificity D-dimerifferential diagnosis and variations and combinations of theey wordsphrases years 2001 through December 2009
This revision to the 2003 clinical policy1 focuses on quantitative-dimer tests that have become available to most hospital
aboratories across the United States The Clinical Policiesubcommittee on PE elected not to assess the evidence forualitative D-dimer tests (often used in point-of-care panels)ecause of problems with variability in interpretation and lowerensitivity reported in multiple studies62-65 However the onlyandomized clinical trial directly assessing the impact of a D-dimertrategy used a qualitative whole-blood agglutination testSimpliRED Agen Biomedical Ltd Brisbane Australia)66 In thisrial potential subjects suspected of having PE were first stratifiedccording to the Wells criteria and those with a low clinicalrobability and negative D-dimer test result were randomized toither no additional testing or VQ scanning Althoughnterpretation of results is limited due to early study closure thencidence of VTE during 6 months was similar among the 2 groups0182 versus 1185) Given that we were unable to identify anyther randomized controlled trials specifically designed to test thempact of a D-dimer strategy our recommendations are based onata from cohort studies and high-quality systematic reviews thatave been published since the original ACEP clinical policy1 Tovoid duplication cohort studies that were included in at least 1 ofhe systematic reviews are not reported in the Evidentiary Table
Class I systematic reviews assessing the test characteristics ofuantitative D-dimer tests in outpatient settings conclude that D-imer has excellent sensitivity (pooled sensitivity093 to 096) butnly moderate specificity (pooled specificity039 to 051)656768
lass I3542 and II 3769-75cohort studies that were not included inhese systematic reviews report similar results In patients with a lowretest probability (10) a negative ELISA or turbidimetric D-imer (LR-01) test result would be expected to decrease therobability of PE to approximately 1 These assumptions basedn the application of Bayesrsquo Theorem are supported by Class I35
lass II6973-75 and Class III38394676-79 studies that haveonsistently reported negative predictive values of approximately9 when D-dimer testing is applied to low-risk or ldquoPE unlikelyrdquoatient populations The American College of Physicians guidelinesn PE also support using D-dimer testing among low-risk patientsuspected of having PE8081
Despite consensus guidelines that recommend using D-dimeresting on patients with an intermediate pretest probability forE82 strong evidence supporting this approach is lacking Aetrospective analysis of 2 studies by Righini et al83 reportedero VTE events at 3-month follow-up for both low- andntermediate-risk groups however the upper limit for the 95
I was 1 for the low-probability group but extended up to
Volume June
hme
ipscea
na(td
caV
teponv2
tdad
hbfTgmstmIb
rrfidcma
Clinical Policy
5 for the intermediate-probability group Subsequent studiesthat have included intermediate pretest probability patientswithin their D-dimer strategy have either not reported resultsseparately737584 or have had too few patients in this subgroupto draw any firm conclusions777885
Given the relatively poor specificity of D-dimer testingvarious strategies have been suggested to limit the number offalse-positive tests that may lead to further unnecessarydiagnostic testing Retrospective subgroup analyses suggest thatD-dimer sensitivity remains fairly constant among varioussubpopulations but specificity decreases with certain comorbidconditions and advanced age678687 Two prospective studiesassessing the performance of D-dimer testing among cancerpatients suspected of having PE reported very low specificities(specificity018 to 021)8889 Pregnancy is also associated withincreasing concentrations of D-dimer particularly in womenbeyond the first trimester90 A restrictive approach to D-dimertesting whereby the elderly are excluded improves testspecificity8691 however this approach is unlikely to decreaseresource utilization since these patients would be expected to godirectly to some form of advanced imaging Adjusting the D-dimer test threshold based on the patientrsquos pretest probability orother variables (eg age) has been suggested as an alternativeapproach to improve the performance of D-dimertesting378792-94 Although raising the D-dimer test thresholdwould be expected to increase test specificity the associateddecrease in sensitivity may be unacceptable to most cliniciansand has not been prospectively studied95
Potential benefits of using a highly sensitive D-dimer as ascreening test include decreased cost and radiation exposurehowever if the test is ordered indiscriminately on patients withvery little or no risk for PE false-positive D-dimer results mayincrease the harms associated with unnecessary advancedimaging A formal decision analysis concluded that using D-dimer was not cost-effective if CT is readily available96
Although the authorsrsquo assumptions about the sensitivity andspecificity of quantitative D-dimer tests were consistent with thestudies included in the Evidentiary Table the authors state thattheir analysis was based on a patient suspected of having PEwithout other competing diagnoses96 It is rare in the EDsetting to have such a straightforward clinical presentation inwhich only 1 diagnosis is considered
Future research is needed for patients with an intermediatepretest probability of PE and to assess whether changing theD-dimer cutoff for different patient subgroups could improvespecificity without a clinically significant decrease in sensitivity
4 What is the role of the CT pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations For patients with a low or PE
unlikely (Wells score 4) pretest probability for PE who require
additional diagnostic testing (eg positive D-dimer result or p
Volume June
ighly sensitive D-dimer test not available) a negativeultidetector CT pulmonary angiogram alone can be used to
xclude PELevel C recommendations (1) For patients with an
ntermediate pretest probability for PE and a negative CTulmonary angiogram result in whom a clinical concern for PEtill exists and CT venogram has not already been performedonsider additional diagnostic testing (eg D-dimer lowerxtremity imaging VQ scanning traditional pulmonaryrteriography) prior to exclusion of VTE disease
(2) For patients with a high pretest probability for PE and aegative CT angiogram result and CT venogram has notlready been performed perform additional diagnostic testingeg D-dimer lower extremity imaging VQ scanningraditional pulmonary arteriography) prior to exclusion of VTEiseaseA negative highly sensitive quantitative D-dimer result in
ombination with a negative multidetector CT pulmonaryngiogram result theoretically provides a posttest probability ofTE less than 1
Key wordsphrases for literature searches x-ray computedomography CT spiral computed tomography pulmonarymbolism sensitivity specificity probability likelihoodulmonary angiogram angiography thromboembolismutcome follow-up recurrent morbidity mortality falseegative false positive prognosis treatment outcome andariations and combinations of the key wordsphrases years001 through December 2009The use of the spiral CT angiogram for the visualization of
he pulmonary vasculature and the evaluation of PE was firstescribed in 199297 A single detector rotated in a spiral fashiont fixed intervals collecting data to generate vascular imagesuring a single breath holdSince that time the technology of this diagnostic modality
as advanced dramatically Multidetector CT scanners now useetween 4 64 or more channels (detectors) and rotate at muchaster gantry speeds (04 seconds versus 1 second per rotation)hus an older-generation single-detector CT with a 1-secondantry speed captures 1 slice per second whereas a 16-channelultidetector CT scanner rotating at a gantry speed of 04
econds captures 40 slices per second98 This in addition tohinner collimation allows for faster image acquisition lessotion artifact and ultimately higher-resolution images
mproved image acquisition protocols and resolution areelieved to result in improved diagnostic performanceIn 1992 Remy-Jardin et al97 in a Class III investigation
eported sensitivities and specificities of 100 and 96espectively for a single-detector CT for detection of PE Thisnding led to eager acceptance of the spiral CT angiogram intoiagnostic algorithms in the hope of simplifying theomplicated diagnostic workup of PE Since this initial studyultiple accuracy and outcomes studies in addition to meta-
nalyses and systematic reviews have been published on the
erformance of the CT pulmonary angiogram Unfortunately
Annals of Emergency Medicine 637
ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

hme
ipscea
na(td
caV
teponv2
tdad
hbfTgmstmIb
rrfidcma
Clinical Policy
5 for the intermediate-probability group Subsequent studiesthat have included intermediate pretest probability patientswithin their D-dimer strategy have either not reported resultsseparately737584 or have had too few patients in this subgroupto draw any firm conclusions777885
Given the relatively poor specificity of D-dimer testingvarious strategies have been suggested to limit the number offalse-positive tests that may lead to further unnecessarydiagnostic testing Retrospective subgroup analyses suggest thatD-dimer sensitivity remains fairly constant among varioussubpopulations but specificity decreases with certain comorbidconditions and advanced age678687 Two prospective studiesassessing the performance of D-dimer testing among cancerpatients suspected of having PE reported very low specificities(specificity018 to 021)8889 Pregnancy is also associated withincreasing concentrations of D-dimer particularly in womenbeyond the first trimester90 A restrictive approach to D-dimertesting whereby the elderly are excluded improves testspecificity8691 however this approach is unlikely to decreaseresource utilization since these patients would be expected to godirectly to some form of advanced imaging Adjusting the D-dimer test threshold based on the patientrsquos pretest probability orother variables (eg age) has been suggested as an alternativeapproach to improve the performance of D-dimertesting378792-94 Although raising the D-dimer test thresholdwould be expected to increase test specificity the associateddecrease in sensitivity may be unacceptable to most cliniciansand has not been prospectively studied95
Potential benefits of using a highly sensitive D-dimer as ascreening test include decreased cost and radiation exposurehowever if the test is ordered indiscriminately on patients withvery little or no risk for PE false-positive D-dimer results mayincrease the harms associated with unnecessary advancedimaging A formal decision analysis concluded that using D-dimer was not cost-effective if CT is readily available96
Although the authorsrsquo assumptions about the sensitivity andspecificity of quantitative D-dimer tests were consistent with thestudies included in the Evidentiary Table the authors state thattheir analysis was based on a patient suspected of having PEwithout other competing diagnoses96 It is rare in the EDsetting to have such a straightforward clinical presentation inwhich only 1 diagnosis is considered
Future research is needed for patients with an intermediatepretest probability of PE and to assess whether changing theD-dimer cutoff for different patient subgroups could improvespecificity without a clinically significant decrease in sensitivity
4 What is the role of the CT pulmonary angiogram of thechest as the sole diagnostic test in the exclusion of PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations For patients with a low or PE
unlikely (Wells score 4) pretest probability for PE who require
additional diagnostic testing (eg positive D-dimer result or p
Volume June
ighly sensitive D-dimer test not available) a negativeultidetector CT pulmonary angiogram alone can be used to
xclude PELevel C recommendations (1) For patients with an
ntermediate pretest probability for PE and a negative CTulmonary angiogram result in whom a clinical concern for PEtill exists and CT venogram has not already been performedonsider additional diagnostic testing (eg D-dimer lowerxtremity imaging VQ scanning traditional pulmonaryrteriography) prior to exclusion of VTE disease
(2) For patients with a high pretest probability for PE and aegative CT angiogram result and CT venogram has notlready been performed perform additional diagnostic testingeg D-dimer lower extremity imaging VQ scanningraditional pulmonary arteriography) prior to exclusion of VTEiseaseA negative highly sensitive quantitative D-dimer result in
ombination with a negative multidetector CT pulmonaryngiogram result theoretically provides a posttest probability ofTE less than 1
Key wordsphrases for literature searches x-ray computedomography CT spiral computed tomography pulmonarymbolism sensitivity specificity probability likelihoodulmonary angiogram angiography thromboembolismutcome follow-up recurrent morbidity mortality falseegative false positive prognosis treatment outcome andariations and combinations of the key wordsphrases years001 through December 2009The use of the spiral CT angiogram for the visualization of
he pulmonary vasculature and the evaluation of PE was firstescribed in 199297 A single detector rotated in a spiral fashiont fixed intervals collecting data to generate vascular imagesuring a single breath holdSince that time the technology of this diagnostic modality
as advanced dramatically Multidetector CT scanners now useetween 4 64 or more channels (detectors) and rotate at muchaster gantry speeds (04 seconds versus 1 second per rotation)hus an older-generation single-detector CT with a 1-secondantry speed captures 1 slice per second whereas a 16-channelultidetector CT scanner rotating at a gantry speed of 04
econds captures 40 slices per second98 This in addition tohinner collimation allows for faster image acquisition lessotion artifact and ultimately higher-resolution images
mproved image acquisition protocols and resolution areelieved to result in improved diagnostic performanceIn 1992 Remy-Jardin et al97 in a Class III investigation
eported sensitivities and specificities of 100 and 96espectively for a single-detector CT for detection of PE Thisnding led to eager acceptance of the spiral CT angiogram intoiagnostic algorithms in the hope of simplifying theomplicated diagnostic workup of PE Since this initial studyultiple accuracy and outcomes studies in addition to meta-
nalyses and systematic reviews have been published on the
erformance of the CT pulmonary angiogram Unfortunately
Annals of Emergency Medicine 637
ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

ioip
powpaw
(
(
(
Cntwpwaop
weleC
sp
Clinical Policy
data are lacking about the performance of the most current CTpulmonary angiogram technology (eg 128-channelmultidetector CTs)
Since 2001 2 Class II99100 and 4 Class III101-104 accuracystudies on the prospective diagnostic performance of singledetector CT have shown variable results with sensitivitiesranging from 57 to 91 and specificities ranging from 84to 100 Likewise 4 Class III systematic reviews solelyevaluating single-detector CT technology demonstratedsensitivities between 37 and 100 and specificities between78 and 10098105-107 The sensitivity for the detection ofemboli to the subsegmental level (37 to 93) was lower thanthat for the segmental and lobar level (53 to 100) Becausethese findings demonstrate suboptimal LR- (009 to 046) mostof the authors recommend caution when using single detectorCT as the sole diagnostic test in the exclusion of PE
One Class II study108 and 2 Class III109110 prospectiveaccuracy studies on multidetector CT have also been publishedsince 2001 These studies show better performance comparedwith single-detector CT with sensitivities ranging from 83 to100 and specificities between 89 and 98 A Class IIImeta-analysis98 and one Class III systematic review106
evaluating multidetector CT performance found the sensitivitiesand specificities were reported as 83 to 90 and 94 to100 respectively These data are consistent with those frommultiple other reviews evaluating multidetector CT incombination with single-detector CT111-114 As such given thecontinued potential for false-negative CT results due to LRs-between 002 and 041 many of these authors still recommendcaution when using multidetector CT as the sole diagnostic testin the exclusion of PE
Negative CT Pulmonary Angiogram Outcome StudiesAlthough CT pulmonary angiogram alone detects the
majority of pulmonary emboli it seems that it may be falselynegative in approximately 15 of cases108 It has beenhypothesized that the pulmonary emboli currently missed byCT pulmonary angiogram alone may be small and clinicallyinsignificant115 which may justify the discharging home of EDpatients without anticoagulation Studies reporting theoutcome of patients with clinically suspected PE for whomanticoagulation was withheld following a negative CTpulmonary angiogram alone were reviewed to evaluate thishypothesis In general these studies enrolled patients who wereclinically suspected of having a PE The patients then receivedCT pulmonary angiogram imaging for the evaluation of PEWhen PE was identified on imaging they were treated withanticoagulation If CT imaging was negative they weredischarged with no anticoagulation and followed clinically forevidence of subsequent VTE
Some studies incorporated the pretest risk stratification ofpatients prior to CT in their evaluation algorithms Patientsmay have had additional negative testing results (eg D-dimervenous imaging VQ scanning pulmonary arteriography) prior
to discharge off anticoagulation As general consensus in the r
638 Annals of Emergency Medicine
nternational medical community patients clinically suspectedf experiencing a PE are presumed to have PE if lower extremitymaging reveals DVT even if the patient has a negative CTulmonary angiogram result
A total of 16 articles were identified ranging in year ofublication from 2000 to 2008 that investigatedutcome after a negative CT scan result (Table 5) Two studiesere retrospective116117 13 studies wererospective1126355084108115118-123 and there was 1 meta-nalysis111 In these studies the evaluation of the conclusionsas often confounded by one or more of the following(1) variability in the types of CTs and CT imaging protocols
between studies(2) variability in the definition of recurrent PE between
studies(3) failure to separate ED patients from inpatients and other
outpatients(4) lack of standardized PE screening protocols or protocols
that were poorly adhered to(5) failure to differentiate patients by their pretest probability
of disease (eg low risk intermediate risk or high risk)(6) differing inclusion or exclusion criteria between studies(7) excluding of patients who received testing other than CT
pulmonary angiogram that was positive(8) including of patients who received testing other than CT
pulmonary angiogram that was negative(9) variability in training of the interpreting radiologists
between studies (eg radiologists subspecialized in thoracicradiology versus general radiologists)
10) differing durations of follow-up after discharge betweenstudies
11) loss of a significant proportion of the study sample tofollow-up
12) low rates of autopsy among patients who diedThe two Class III retrospective studies used a single-detector
T scan and reported rates of subsequent PE in patients with aegative CT pulmonary angiogram result of approximately 0o 2116117 In addition to being retrospective these studiesere also limited by smaller sample sizes the loss of a significantroportion of patients to follow-up the exclusion of patientsho received anticoagulation before or after CT pulmonary
ngiogram due to a higher perceived pretest probability of PEr the exclusion of patients who received testing other than CTulmonary angiogram that was positive
Of the 13 prospective studies between 2000 and 2008 3ere Class I level of evidence355084 4 were Class II level of
vidence1126108118 and the remaining 6 studies were Class IIIevel of evidence115119-123 Of the 7 Class I and II level ofvidence studies 5 studies incorporated data from multidetectorTs11263584108 and 2 did not50118
One of the Class I studies35 found a low incidence ofubsequent VTE during follow-up after a negative CTulmonary angiogram result similar to that found in the
etrospective studies In this 2006 study35 the Christopher
Volume June
9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

9oaCbspwaui9thotileaifbrs
a
Clinical Policy
Study Investigators reported 3-month follow-up of aprospective consecutive sample of 1436 patients who hadanticoagulation withheld following a negative CT pulmonaryangiogram for the workup of clinically suspected PE Patientswere initially risk stratified as either PE ldquounlikelyrdquo (ie Wellsscore 4) or PE ldquolikelyrdquo (Wells score 4) Patients for whomthe diagnosis of PE was judged ldquounlikelyrdquo received highlysensitive D-dimer testing PE unlikely patients with a positiveD-dimer result and patients with a likely clinical probability ofPE received further testing with CT pulmonary angiogramalone Of the 1436 patients with a negative CT pulmonaryangiogram result who did not receive anticoagulation 18(13 95 CI 07 to 2) were found to develop VTEduring the 3-month follow-up Seven (39) of the patientsfound to have VTE in follow-up died This mortality rateamong patients with missed PE is similar to that reported inother studies84116 Only 1 patient had incomplete follow-upThe results of this study were very similar to those of anotherdichotomously risk-stratified Class II study by Anderson et al11
that reported the incidence of subsequent VTE after acombined negative CT pulmonary angiogram result andbilateral ultrasound of 17 In another prospective Class IIstudy van Strijen et al118 found a 2 incidence of subsequentVTE among patients with a negative single-detector CT resultwho were followed for 3 months In contrast to these studiesother prospective studies have raised concerns that CTpulmonary angiogram may not reliably exclude subsequentVTE especially among patients risk stratified as having higher
Table 5 Negative CT pulmonary angiogram outcome study table
Author Year Design Detector TypeColl
Goodman et al115 2000 Prospective SingleMusset et al50 2002 Prospective SingleSwensen et al116 2002 Retrospective SingleDonato et al117 2003 Retrospective Multiplevan Strijen et al118 2003 Prospective SinglePerrier et al26 2004 Prospective SinglemultipleFriera et al119 2004 Prospective SingleKavanagh et al120 2004 Prospective MultipleMoores et al111 2004 Meta-analysis
prospectiveretrospective
Singlemultiple 1
Prologo et al121 2005 Prospective Singlemultiplevan Belle et al35 2006 Prospective Singlemultiple 1Stein et al108 2006 Prospective Multiple (4ndash16) NotVigo et al122 2006 Prospective Multiple
Anderson et al11 2007 Prospective Singlemultiple
Subramaniamet al123
2007 Prospective Single
Righini et al84 2008 Prospective Multiple
CT Computed tomography ED emergency department mo month
clinical pretest probability for PE5084108122 C
Volume June
In a 2002 Class I prospective single-detector CT study with88 follow-up at 3 months Musset et al50 reported on theutcome of consecutive risk-stratified patients who hadnticoagulation withheld following a negative single-detectorT pulmonary angiogram result that was combined withilateral lower extremity ultrasound The incidence ofubsequent VTE in this study during a 3-month follow-uperiod was 18 (95 CI 08 to 33) among 507 patientsith a low and intermediate pretest probability of PE Ten low
nd intermediate pretest probability patients were lost to follow-p Among the low- and intermediate-risk patient group
npatients had a higher incidence of disease in follow-up (485 CI 18 to 101) than outpatients (08 95 CI 02o 23) Seventy-five of 76 high pretest probability patientsad VQ imaging traditional arteriography or both at the timef their initial evaluation Four of the 75 (53 95 CI 15o 131) high-risk patients proved to have PE on subsequentmaging after a negative CT pulmonary angiogram and bilateralower extremity ultrasound This study combined lowerxtremity ultrasound imaging with CT in the evaluation processnd still found a modest proportion of patients especiallynpatients and those assessed as high risk who developed PE inollow-up This study shows the importance of risk stratificationefore CT pulmonary angiogram and calls into question theeports of lower incidences of subsequent VTE among nonrisk-tratified patients
Results from additional studies have also raised questionsbout the previously reported low rate of VTE after a negative
on Sample Size(CT Negative) Patient Type
Duration ofFollow-up
mo
285 InpatientoutpatientED 1 and 3601 InpatientoutpatientED 1 2 and 3993 InpatientoutpatientED 3243 Inpatientoutpatient 3248 InpatientoutpatientED 3458 ED 3132 Not specified 385 Not specified 4 to 13
4657 InpatientoutpatientED 3 or more
221 Not specified 3 and 61436 InpatientoutpatientED 3
fied 773 InpatientoutpatientED 6257 negative D-dimer
279 positive D-dimer
Inpatientoutpatient 6
694 positive D-dimeror at higher risk
InpatientoutpatientED 3
483 InpatientED 3
673 ED 3
imatimm
32ndash33353312525ndash5
325ndash3speci25
1
3
125
T pulmonary angiogram alone result for patients with
Annals of Emergency Medicine 639
dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

dagDCr
mseaap(r
pfasearp
Ppaasaiu
5p
ing or
Clinical Policy
clinically suspected PE In 2006 the PIOPED II investigatorsin a Class II prospective study of 1090 risk-stratified inpatientsand outpatients with suspected PE reported patient outcomesof the use of CT pulmonary angiogram in conjunction withdelayed CT venogram108 Of these 1090 patients 28 wereexcluded for not undergoing CT 238 were excluded for nothaving a reference test diagnosis and 51 were excluded forhaving a noninterpretable CT scan There were 592 patientswith an interpretable CT for whom PE was ruled out on initialpresentation The overall incidence of subsequent VTE on 6-month follow-up in this subgroup was 17 (95 CI 8 to24) after a negative CT pulmonary angiogram alone resultand 10 (95 CI 7 to 16) after a negative CT pulmonaryangiogram with CT venogram The rate of false-negative CTstudies was higher among the subjects risk stratified as ldquohighclinical probabilityrdquo and lower among the ldquolow clinicalprobabilityrdquo group (Table 6)
Conversely the false positive rate was highest among the lowclinical probability patients and lowest among those riskstratified as high clinical probability This study was limited bythe high exclusion rate (29) and by the fact that patientsuniformly received additional testing after their negative CTpulmonary angiogram with or without CT venogram prior todischarge therefore the study did not directly assess theprognostic value of a negative CT pulmonary angiogram aloneresult to predict outcome among patients not receivinganticoagulation
In a 2006 Class III study with 6-month follow-up thatcombined the result of a highly sensitive quantitative D-dimerafter a negative multidetector CT pulmonary angiogram resultamong 279 consecutive patients with clinically suspected PEVigo et al122 found that the incidence of PE after a negative CTpulmonary angiogram and positive D-dimer result was 197(55279) The incidence of PE after a negative CT pulmonaryangiogram and negative D-dimer result was 117 (325795 CI 024 to 338) This study was limited by the factthat patients with a positive D-dimer result had immediate
Table 6 Positive and negative predictive values of CTA comparpermission Copyright copy Massachusetts Medical Society PublisInvestigators Multidetector computed tomography for acute pul
Variable
High Clinical Proba
NoTotal No Value (
Positive predictive value of CTA 2223 96 (7Positive predictive value of CTA or CTV 2728 96 (8Negative predictive value of CTA 915 60 (3Negative predictive value of both CTA and CTV 911 82 (4
CI confidence interval CTA computed tomography angiogram CTV computed toThe clinical probability of pulmonary embolism was based on the Wells score lehigh probabilitydaggerTo avoid bias for the calculation of the negative predictive value in patients deemment only patients with a reference test diagnosis by ventilation perfusion scann
evaluation with VQ scanning prior to discharge home and the
640 Annals of Emergency Medicine
ecision to prescribe anticoagulation Additionally there was noutopsy rate reported among the 15 patients who died in theroup that had both a negative CT pulmonary angiogram and-dimer test result This study adds concern to the ability ofT pulmonary angiogram to reliably exclude PE among higher-
isk patientsIn a 2008 Class I study Righini et al84 investigated the 3-
onth outcome of 1819 consecutive risk-stratified patientsuspected of having PE randomized into 2 diagnosticvaluation strategies D-dimer combined with CT pulmonaryngiogram versus D-dimer combined with venous ultrasoundnd CT pulmonary angiogram The 3-month VTE risk inatients with a negative workup in these 2 subgroups was 0395 CI 01 to 12) and 03 (95 CI 01 to 11)espectively
The false-negative rate of CT pulmonary angiogram alone inatients clinically deemed high risk for PE ranges in studiesrom 53 to 405084108 Although data are more limitedbout those specific high-risk patients for PE outcome studiesupport the use of additional testing (eg D-dimer lowerxtremity venous imaging VQ scanning traditionalrteriography) after a negative CT pulmonary angiogram aloneesult before definitively ruling out VTE in this subset ofatients
Until more perfect diagnostic testing evolves for diagnosingE future studies of CT should include the reproducibleretest clinical risk stratification of patients in addition to well-dhered-to standardized PE screening protocols Additionallys screening and confirmatory tests for PE become increasinglyensitive it will be crucial to better define the incidence costnd risk associated with false-positive testing These risks maynclude unnecessary long-term anticoagulation as well asninsurability for medical financial coverage
What is the role of venous imaging in the evaluation ofatients with suspected PE
Patient Management Recommendations
ith previous clinical assessment108 Reprinted withStein PD Fowler SE Goodman LR et al for the PIOPED II
ary embolism N Engl J Med 20063542317-2327
Intermediate ClinicalProbability Low Clinical Probability
CI) NoTotal No Value (95 CI) NoTotal No Value (95 CI)
) 93101 92 (84ndash96) 2238 58 (40ndash73)) 100111 90 (82ndash94) 2442 57 (40ndash72)) 121136 89 (82ndash93) 158164
dagger96 (92ndash98)
) 114124 92 (85ndash96) 146151dagger
97 (92ndash98)
phy venogramn 20 low probability 20 to 60 moderate probability and more than 60
have a low probability of pulmonary embolism on previous clinical assess-conventional pulmonary digital subtraction angiogram were included
ed whermon
bility
95
8ndash991ndash992ndash838ndash97
mograss tha
ed to
Level A recommendations None specified
Volume June
acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

acf
psntpipbpiOtbspaeastTshaaa
iisnv
mpaauaewpnutPpai
Clinical Policy
Level B recommendations When a decision is made toperform venous ultrasound as the initial imaging modality apositive finding in a patient with symptoms consistent withPE can be considered evidence for diagnosis of VTE diseaseand may preclude the need for additional diagnostic imagingin the ED
Examples of situations in which a venous ultrasound may beconsidered as initial imaging may include patients with obvioussigns of DVT for whom venous ultrasound is readily availablepatients with relative contraindications for CT scan (egborderline renal insufficiency CT contrast agent allergy) andpregnant patients
Level C recommendations (1) For patients with anintermediate pretest probability for PE and a negative CTangiogram result for whom a clinical concern for PE still existsand CT venogram has not already been performed considerlower extremity venous ultrasound as an additional test toexclude VTE disease (see question 4)
(2) In patients with a high pretest probability for PE and anegative CT angiogram result and CT venogram has notalready been performed perform additional testing to excludeVTE disease (see question 4) As one of these additional testsconsider lower extremity venous ultrasound to exclude VTEdisease (see question 4)
Key wordsphrases for literature searches pulmonaryembolism venous ultrasonography sensitivity specificityprobability likelihood and variations and combinations of thekey wordsphrases years 2002 through December 2009
Various strategies are currently used in the ED evaluation ofpatients with suspected PE Most involve a combination ofpretest probability assessment D-dimer measurement VQscanning CT angiogram and pulmonary arterial angiogramVenous imaging CT venous imaging (obtained in conjunctionwith CT pulmonary angiogram) and venous ultrasound mayplay useful roles in the management of these patients
The use of venous imaging for PE assessment has beenreported in 3 Class I365084 3 Class II108124125 and 5 Class IIIstudies126-130 CT venous imaging is performed in sequencedirectly after CT angiogram This technique uses theopacification of the venous system that follows rapid infusion ofcontrast medium that is involved with the performance of CTangiogram but also results in additional radiation exposureImages are obtained of the veins of the legs pelvis andabdomen When CT angiogram is used in the assessment ofpatients with suspected PE the time to acquire these additionalimages is minimal Although venous ultrasound of bilaterallower extremities does not involve additional radiation exposurethis test does not allow for evaluation of the abdominal andpelvic venous systems and typically requires more time becausedifferent technicians and departments are involved
Previous reports of the use of venous imaging typically
involve either the performance of venous ultrasound before or p
Volume June
fter CT angiogram or the use of CT venous imaging inonjunction with CT angiogram to increase the diagnostic yieldor the diagnosis of thromboembolic disease
In the assessment of ED patients with suspected PE theerformance of venous ultrasound with the finding of aignificant DVT is diagnostic of VTE and may preclude theeed for further diagnostic testing84108131132 In these patientshe use of venous ultrasound before CT angiogram is for theurposes of limiting radiation exposure and in some situationsn which venous ultrasound is more available or more rapidlyerformed decreasing time for evaluation This strategy shoulde considered for patients with obvious signs of DVT foratients with relative contraindications for CT scan (eg renalnsufficiency CT contrast agent allergy) and pregnant patients
nly 1 Class I study84 evaluated outcomes with this strategy forhe use of venous ultrasound for ED patients with suspected PEefore CT angiogram This study randomized 2 differenttrategies for the ED workup of these patients pretestrobability assessment D-dimer measurement and CTngiogram with 3-month follow-up versus the same regimenxcept the addition of venous ultrasound testing before CTngiogram if indicated If the venous ultrasound revealed aignificant DVT no further testing was performed andreatment for venous thromboembolic disease was initiatedhis study found that both treatment algorithms were equally
afe at 3-month follow-up and about 10 of the patients whoad venous ultrasound were diagnosed with a significant DVTnd did not need CT angiogram to be performed However theddition of venous ultrasound required 11 patients to have thisdditional test to identify 1 patient with DVT
The remaining clinical trials involved the use of venousmaging after the performance of CT angiogram in order tomprove the sensitivity for the diagnosis of PE Most of thesetudies report on venous ultrasound after CT angiogram witho Class I studies available for CT angiogram followed by CTenous imaging
Anderson et al36 in a Class I study performed a prospectiveulticenter study assessing a treatment algorithm for ED
atients with suspected PE that incorporated venous ultrasoundfter CT angiogram This protocol involved pretest probabilityssessment D-dimer measurement CT angiogram and venousltrasound with 3-month follow-up All patients who had CTngiogram testing also had venous ultrasound This studynrolled 858 patients of whom 96 (95 CI 77 to 118)ere diagnosed with PE Of these patients 369 had low pretestrobability with a negative D-dimer result These patients didot undergo further testing The remaining 489 patientsnderwent CT angiogram and venous ultrasound testing Ofhese 489 patients 67 (137 95 CI 108 to 171) hadE diagnosed by CT angiogram Of the remaining 422 13atients had a DVT diagnosed by venous ultrasound Theddition of venous ultrasound to CT angiogram in this studydentified an additional 31 (95 CI 17 to 52) of
atients who were treated for venous thrombotic disease A
Annals of Emergency Medicine 641
rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

rvrV(PDov2ciauap
dutppDdrHnou0
tTgangwtiwi
6p
tPl
t
Clinical Policy
Class I study by Musset et al50 used a similar protocol andfound that the addition of venous ultrasound after CTangiogram identified 60 (95 CI 45 to 77) of patientswith significant DVTs Of the remaining studies involvingvenous ultrasound testing after CT angiogram there were 1Class II and 2 Class III studies that revealed similar findings LeGal et al125 finding 09 (95 CI 02 to 26) Au et al126
finding 26 (95 CI 01 to 138) and Coche et al127
finding 23 (95 CI 01 to 123) of additional patientsidentified with venous ultrasound testing after CT angiogram
One Class II108 and 5 Class III126-130 studies assessed the utilityof CT venous imaging after CT angiogram Five of the 6 studiesenrolled both inpatients and outpatients with 4 of these studiesincluding predominantly inpatients referred to radiology for CTangiogram for suspected PE Additionally none of these studiesassessed 3-month follow-up in patients with negative CTangiogram results The PIOPED II trial108 was a Class IImulticenter prospective study that enrolled adults (18 years) withclinically suspected PE from the inpatient or outpatient setting Allpatients who met inclusionexclusion criteria underwent pretestprobability assessment and then CT angiogram followed by CTvenous imaging CT was conducted in 824 patients with 51patients having inconclusive testing due to poor CT image qualityPE was diagnosed in 192 (23 95 CI 204 to 263)patients with 21 (95 CI 11 to 35) being identified withthe addition of CT venogram The 5 Class III studies reportedsimilar findings126-130 The addition of CT venous imaging to CTangiogram identified an additional 79 (95 CI 17 to 214)of patients in the Au et al126 study 47 (95 CI 06 to 158)in the Coche et al127 study 0 (95 CI 0 to 161) in theBegemann et al128 study 03 (95 CI 001 to 14) in theJohnson et al129 study and 55 (95 CI 38 to 77) in theLoud et al130 study
Based on these studies it appears that venous ultrasound andCT venous imaging after negative CT angiogram result areequally useful There are 1 Class II and 2 Class III studies inwhich CT venous imaging and venous ultrasound wereperformed after CT angiograms in patients with suspectedPE126127133 Goodman et al133 in a Class II study performeda substudy analysis of the PIOPED II108 data There were 711patients who underwent CT angiogram and had both CTvenogram and venous ultrasound performed Both CTvenogram and venous ultrasound were positive in 81 of 711(11) patients CT venogram was positive and venousultrasound negative in 17 (2) patients and CT venogram wasnegative and venous ultrasound was positive in 15 (2)patients Coche et al127 performed CT angiogram CT venousimaging and venous ultrasound in a prospective study ofinpatients and outpatients with suspected PE (only 7 of 65patients were from the ED) Venous ultrasound was performedwithin 24 hours of CT scanning PE was diagnosed by CTangiogram alone DVT was diagnosed if a patient hadconcordant DVT on CT venous imaging and venous
ultrasound For 5 patients for whom there were discordant a
642 Annals of Emergency Medicine
esults for CT venous imaging and venous ultrasound standardenogram was performed in 2 patients and 3 patients hadepeated focalized venous ultrasound to arrive at final diagnosisTE was diagnosed in 38 (585) patients and consisted of 22
338) patients with isolated PE 13 (20) with co-existentE and DVT and 3 (46) with DVT In the 16 patients withVT CT venous imaging had a sensitivityspecificity for DVT
f 93898 respectively compared with 87598 forenous ultrasound CT venous imaging identified an additionalpatients with VTE (53 of total patients with VTE)
ompared with CT angiogram whereas venous ultrasounddentified an additional 1 (26) patient The study by Au etl126 reported similar results Given the available data venousltrasound and CT venous imaging after CT angiogram bothppear to be equally effective in the evaluation of VTE inatients with suspected PE84126127130
In summary venous imaging may be a useful adjunct in theiagnostic algorithm of ED patients suspected of having PE These of venous ultrasound as the initial diagnostic test may establishhe diagnosis of VTE in approximately 10 of patients andreclude the need for CT angiogram This strategy may bearticularly useful in patients who have obvious clinical signs ofVT contraindications for contrast dye administration (eg renal
ysfunction CT contrast agent allergy) or when limitation ofadiation exposure is extremely important (eg pregnancy)owever for most patients (90) this strategy will involve a
egative venous ultrasound test and the increased time and expensef this additional test The use of venous imaging (venousltrasound or CT venous imaging) identifies DVT in approximately to 6 of patients with a negative CT angiogram
A limitation of the presently available studies is that most ofhe data come from research using older single-detector CTsheoretically higher-resolution multidetector CTs will havereater sensitivity for detecting PE and future studies need toddress whether venous imaging is warranted for patients with aegative CT angiogram result when obtained with the newesteneration of CT scanners Future studies also need to identifyhich patients would most benefit from adding venous imaging
o CT angiogram An additional area of future research isdentification of subgroups of patients with suspected PE whoould most benefit from a protocol of venous ultrasound as the
nitial diagnostic test before CT angiogram
What are the indications for thrombolytic therapy inatients with PE
Patient Management RecommendationsLevel A recommendations None specifiedLevel B recommendations Administer thrombolytic
herapy in hemodynamically unstable patients with confirmedE for whom the benefits of treatment outweigh the risks of
ife-threatening bleeding complicationsIn centers with the capability for surgical or mechanical
hrombectomy procedural intervention may be used as an
lternative therapy
Volume June
uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

uei7si
tmshelai
GPKsphsvdPPisaas
pomptsPaP
mtoc(ro(n
Clinical Policy
Level C recommendations (1) Consider thrombolytictherapy in hemodynamically unstable patients with a highclinical suspicion for PE for whom the diagnosis of PE cannotbe confirmed in a timely manner
(2) At this time there is insufficient evidence to make anyrecommendations regarding use of thrombolytics in anysubgroup of hemodynamically stable patients Thrombolyticshave been demonstrated to result in faster improvements inright ventricular function and pulmonary perfusion but thesebenefits have not translated to improvements in mortality
Key wordsphrases for literature searches pulmonaryembolism thrombolytic therapy massive pulmonary embolismand variations and combinations of the key wordsphrases years2000 through December 2009
Despite proven benefit of thrombolytic therapy in patientswith ST-segment elevation acute myocardial infarction(STEMI)134 and select patients with acute cerebral vascularaccidents135136 indications for use of thrombolytic therapy inpatients with PE remain controversial despite more than 40years of experience182137-142 It is well established thattreatment of PE with thrombolytic therapydagger results in morerapid resolution of arterial emboli decreased pulmonary arterypressure and improvements in cardiac output and pulmonarycirculation143-151 However none of these clinical benefits havebeen demonstrated to result in improvement in mortality orrecurrent PE in unselected patients with PE
Treatment benefit for acute myocardial infarction andcerebral vascular accident is directly related to time fromsymptom onset until administration of thrombolytic therapy(ie door-to-needle time) For acute myocardial infarctionbenefit has been demonstrated during the first 12 hours ofsymptom onset134 For cerebral vascular accident the NationalInstitute of Neurologic Disorders and Stroke (NINDS) StudyGroup135 demonstrated benefit of treatment with alteplaseduring the first 3 hours and Hacke et al136 subsequentlydemonstrated a benefit in the 3- to 45-hour time windowTheoretically similar time-dependent treatment benefits shouldexist for thrombolytic therapy in PE To date no randomizedtrial has investigated potential time-dependent benefits duringthe initial hours of symptom onset
Clinical Investigations of Thrombolytics in PEThere are 11 randomized studies investigating utility of
thrombolytics in PE that have appeared in subsequent meta-analyses146-156 Four of these 7 articles were given a grade of Xby this subcommittee153-156 Table 7 summarizes some of theimportant features of these 11 randomized studies (seeEvidentiary Table for more detailed information)
daggerThe 2 thrombolytic drugs available in the United States that areapproved for use by the Food and Drug Administration arestreptokinase (250000-unit bolus followed by 100000 unitshourfor 24 hours) and recombinant tissue plasminogen activator (rt-PA)
e(100 mg infused over 2 hours)
Volume June
The shortest inclusion criterion from time of symptom onsetntil presentation was 96 hours in the study by Konstantinidest al152 Two studies did not provide time eligibilitynformation153156 and the remaining studies used 5 days149151
days150155 10 days146 and 14 days147148154 None of thesetudies reported time-dependent treatment benefits and thus its impossible to perform any valid meta-analysis on this topic
A significant limitation of the 11 studies investigating PE ishat only 2 studies had mortality as a primary outcomeeasure152154 The primary endpoint of the remaining 9
tudies related to pulmonary perfusion parameters oremodynamic parameters146-151153155156 Seven studiesxcluded hypotensive patients146-150152155 Other significantimitations relate to the multitude of differing thrombolyticgents differing doses and routes of administration differingnclusionexclusion criteria and differing clinical endpoints
The 3 largest studies to date are the Class II study byoldhaber et al147 and the Class III studies by the Urokinaseulmonary Embolism Trial (UPET) Study Group151 and byonstantinides et al152 The Goldhaber et al147 study was a
ingle-center nonblinded randomized controlled trial in 101atients whose primary outcomes were right ventricularemodynamics and pulmonary perfusion by nuclear lungcanning The study demonstrated improvements in rightentricular wall motion (39 versus 17 P005) and inegree of 24-hour pulmonary perfusion (146 versus 15005) in patients treated with thrombolytics No recurrentE was observed in the alteplase group as opposed to 5 patients
n the heparin group (P006) A significant limitation of thistudy was the inclusion of late presenters as these patients hadlready survived the initial phase of their disease and thus weret extremely low risk of adverse outcome (approximately 30 oftudy patients presented 5 days after symptom onset)
The UPET Class III study was a multicenter randomizedlacebo-controlled trial in 160 patients whose primaryutcomes were pulmonary angiogram scores hemodynamiceasurements via right heart catheterization and pulmonary
erfusion scanning151 Significant improvements in thehrombolytic group were observed in pulmonary angiogramcores (53 versus 9 with moderate or greater improvementvalues and CI not provided) mean hemodynamic
bnormalities and 24-hour lung scanning (221 versus 81values and CI not provided)The Class III study by Konstantinides et al152 was a
ulticenter double-blinded randomized placebo-controlledrial in 256 patients presenting within 96 hours of symptomnset The primary endpoint was defined as inhospital death orlinical deterioration that required an escalation of treatmentsecondary thrombolysis catecholamines cardiopulmonaryesuscitation and surgical embolectomy) The primary endpointccurred in 110 of alteplase versus 246 of heparin patientsP005) However analysis of the data reveals that there wereo differences in the individual outcomes of the composite
ndpoint among those patients who received alteplase versus
Annals of Emergency Medicine 643
owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

owi
M
cwsOCCi
rWnsrprs
Clinical Policy
heparin for death (34 versus 22 P071) catecholamineinfusion (25 versus 58 P033) intubation (25 versus22 P085) cardiopulmonary resuscitation (0 versus 1P1) and embolectomy (0 versus 1 P1)The onlyoutcome that had a statistically significant difference wassecondary thrombolysis (76 versus 232) however thestudy had a serious flaw in that the study protocol allowedbreaking of the randomization code if consideration was beinggiven for escalation of treatment Given this unblinding ofgroup allocation it is likely that patients who had already failedthrombolytic therapy were less likely to undergo secondarythrombolysis In conclusion the findings of this study provideevidence that thrombolytics do not decrease mortality inhemodynamically stable patients with PE
A recent Class III study by Becattini et al157 that is notincluded in the meta-analyses was a multicenter double-blinded randomized controlled trial comparing tenecteplase toplacebo in patients presenting within 10 days of symptom onsetPrimary outcome was right ventricular dysfunction as assessedby echocardiography at 24 hours The study was prematurelyterminated after enrollment of 58 patients because of startup ofthe Pulmonary Embolism Thrombolysis Study (PEITHO)158
Table 7 Important features of the 11 randomized clinical trials of thr
Study Class Thrombolytic Regimen
Dalla-Volta et al146 III Alteplase 10-mg bolus plus 90 mgduring 100 min plus heparin
Goldhaber et al147 II Alteplase 100 mg during 2 h plusheparin
Levine et al148 III Alteplase 06 mgkg during 2 minplus heparin
Ly et al149 III Streptokinase 250000 IU loadthen 100000h during 72 h
PIOPED Investigators150 III Alteplase 40 to 80 mg infused at1 mgmin plus heparin
UPET Study Group151 III Urokinase 2000 IUpoundh loadthen 2000 IUpound during12 h followed by heparin
Konstantinides et al152 III Alteplase 10-mg bolus plus 90 mgduring 120 min plus heparin
Dotter et al153 X Streptokinase 250000 load during20 to 30 min then 100000IUh for 18 to 72 h followed byheparin
Jerjes-Sanches et al154 X Streptokinase 1500000 IU during1 h followed by heparin
Marini et al155 X Urokinase 2400000 IU during3 days (10 patients) urokinase330000 IU during 12 h(10 patients)
Tibbutt et al156 X Streptokinase 600000 IU loadthen 100000h during 72 h bypulmonary artery catheter
h Hour IU unit kg kilogram mg milligram min minuteEighty percent of patients presented within 96 h of symptom onset
Although this study demonstrated improvements in the primary t
644 Annals of Emergency Medicine
utcome of right ventricular dysfunction in patients treatedith tenecteplase it was underpowered to detect any differences
n secondary efficacy or safety outcomes
eta-analyses of Thrombolytics in PEThere have been 4 meta-analyses of randomized studies
omparing thrombolytic therapy versus heparin therapy in patientsith PE159-162 The study by Agnelli et al159 was given an X for
erious flaws in methodology discussed in the Evidentiary Tablef the remaining 3 meta-analyses the study by Dong et al162 was alass II study and those by Thabut et al160 and Wan et al161 werelass III studies Table 8 is a summary of the individual studies
ncluded in each meta-analysisAll 3 meta-analyses found no decrease in either mortality or
ecurrent PE in unselected patients treated with thrombolyticsan et al161 performed subgroup analysis of studies that did
ot exclude patients with hemodynamic instability Thisubgroup analysis consisting of 5 trials revealed a significanteduction in the combined endpoint of death or recurrent PE inatients treated with thrombolytics (94 versus 19 oddsatio [OR] 045 CI 022 to 092) The findings of thisubgroup analysis are highly suspect because 3 of the 5 studies
olytic therapy in PE that were used in subsequent meta-analyses
Primary EndpointsSymptom OnsetInclusion Criteria
Excluded HypotensivePatients
giogram score 10 days Yes
ght ventricular functionpulmonary perfusionmortality
14 days Yes
lmonary perfusion 14 days Yes
giogram score 5 days No
giogram scorepulmonary perfusion
7 days Yes
giogram scorehemodynamics
5 days No
ortality escalation oftreatment
96 h Yes
giogram score Not stated No
ortality 14 days No
lmonary perfusion 7 days Yes
giogram score Not stated No
omb
An
Ri
Pu
An
An
An
M
An
M
Pu
An
hat did not exclude hemodynamically unstable patients were
Volume June
mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

mtshRrte2adsd
R
tiPpfFichsflh
tmiwow
Clinical Policy
given an X by this subcommittee for serious methodologic flawsAfter exclusion of data from these 3 studies mortality occurredin 7 of 96 (73) patients treated with thrombolytics comparedwith 9 of 89 (101) patients in the heparin group
Thrombolytic Administration in Select Subgroupsof Patients
A controversial issue is whether or not hemodynamicallystable patients with right ventricular dysfunction asdemonstrated on echocardiography (often referred to assubmassive PE) should be considered a criterion forthrombolytic therapy1142163-166 Although it is well establishedthat patients with right ventricular dysfunction onechocardiography have more rapid return of right ventricularfunction and restoration of pulmonary perfusion when treatedwith thrombolytics these improvements have not translated todecreases in mortality143144146-151
In an unstable patient with strong clinical suspicion of PE ithas been advocated that one should consider thrombolytictherapy in a patient in whom the diagnosis of PE is unable to beconfirmed (eg patient instability unavailability of testingcontraindications for testing)1137138142167 In this subgroup ofpatients the finding of right ventricular dysfunction on bedsideechocardiography may be used as indirect evidence for presenceof PE although this technology or skill level is unavailable inmost EDs1142163164166168
Another subgroup of patients who theoretically may benefitfrom thrombolytics are patients with PE and right heartthrombus on echocardiography because these patients are athigher risk for recurrent PE and death169170 Torbicki et al170
analyzed data from the International Cooperative PulmonaryEmbolism Registry (ICOPER) Of the 2454 patients in theICOPER registry 1113 had baseline echocardiography as partof the evaluation In this subgroup 42 patients were identifiedas having right heart thrombus The mortality rate was 21 inpatients with right heart thrombus as compared to 11 without
Table 8 Summary of randomized trials of thrombolytic therapyand Dong et al162
ClassTh
Dalla-Volta et al146 (N36) IIIGoldhaber et al147 (N101) IILevine et al148 (N58) IIILy et al149 (N25) IIIPIOPED Investigators150 (N13) IIIUPET Study Group151 (N160) IIIKonstantinides et al152 (N256) IIIDotter et al153 (N31) XJerjes-Sanches et al154 (N8) XMarini et al155 (N30) XTibbutt et al156 (N30) X
NA Study not available for inclusion in the meta-analysisStudies graded as an X that were included in the meta-analysis
right heart thrombus (P005) There were no differences in i
Volume June
ortality between patients treated with and withouthrombolytics (208 versus 235) However patientselected for treatment with thrombolytics had more significantemodynamic compromise that may have biased these findingsose et al171 retrospectively analyzed 177 patients with PE and
ight heart thrombus The authors looked at patients with noreatment heparin alone thrombolytic therapy andmbolectomy The mortality in these 4 subgroups was 10086 238 and 113 respectively On multivariatenalysis only thrombolytic therapy was associated with aecreased mortality The findings of this article are limited byignificant selection bias because the patient population iserived from 95 case reports or case series
isk Benefit Assessment of Patients With PEWhen one considers thrombolytic therapy in PE just as in
he treatment of patients with STEMI or acute cerebralschemia one must conduct a risk-benefit assessmentresumably patients at higher risk of death from PE have greaterotential for benefit from thrombolytic therapy The ICOPERound overall 3-month mortality from PE to be 174172
actors that have been associated with higher mortality from PEnclude age greater than 70 years congestive heart failurehronic obstructive lung disease presence of one lung cancerypotension tachypnea hypoxia tachycardia altered mentaltatus right ventricular hypokinesis syncope chronic renalailure previous cerebral vascular accident elevated troponinevel elevated brain-type natriuretic peptide level and righteart thrombus170172-180
The Pulmonary Embolism Severity Index (PESI) is a scorehat may assist the physician in determining the risk ofortality in a patient with PE (Table 9)181-183 The score was
nitially developed using logistic regression in 15531 inpatientsith a discharge diagnosis of PE181 The prediction rule is basedn 11 patient characteristics that were independently associatedith mortality and stratifies patients into 5 severity classes with
used in the meta-analysis by Thabut et al160 Wan et al161
2002160
n461)Wan 2004161
(III) (N748)Dong 2006162
(II) (n679)
es Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes Yeses Yes YesA Yes Yeso Yes Noes Yes Noes Yes Noes Yes Yes
in PE
abut(III) (
YYYYYYNNYYY
ncreasing risk181 The score is easily calculated and has been
Annals of Emergency Medicine 645
C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

C
pOauttoauahoomicpthpss
ic
wsi
R
Clinical Policy
validated in subsequent clinical investigations182183 Althoughthe PESI score was originally developed as a decision aid toidentify patients suitable for outpatient treatment it appears toreliably predict mortality and thus has the potential to assistphysicians in making risk-benefit decisions when consideringadministration of thrombolytics
Risk-benefit assessment must also take into account the risk ofserious bleeding complications with thrombolytic therapy A meta-analysis of 5 studies on thrombolytic therapy in PE found anintracranial hemorrhage rate of 2 with a mortality rate of05184 Diastolic hypertension was the principal risk factor inpredicting development of intracranial hemorrhage The meta-analysis by Dong et al162 found no differences on pooled analysis inrisk of major hemorrhagic events (OR 16 95 CI 091 to 286)or in minor hemorrhagic events (OR 198 95 CI 068 to 575)in the thrombolytic group compared with the heparin group
Data from the ICOPER registry found that intracranialbleeding in thrombolytic-treated patients occurred in 30 andmajor bleeding occurred in 217 versus 03 (P005) and88 (P005) respectively in patients not receivingthrombolytics172 Factors that are associated with increasedbleeding complications are increasing age uncontrolled
Table 9 The Pulmonary Embolism Severity Index (PESI) andmortality by total point score181 Reprinted with permission ofthe American Thoracic Society Copyright copy American ThoracicSociety Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolismAmerican Journal of Respiratory and Critical Care Medicine20051721041-1046 Official journal of the American ThoracicSociety Diane Gern Publisher
Prognostic Variables Points Assigned
DemographicsAge Age in yMale sex 10Comorbid conditionsCancer 30Heart failure 10Chronic lung disease 10Clinical findingsPulse 110 beatsmin 20Systolic blood pressure 100 mm Hg 30Respiratory rate 30 breathsmin 20Temperature 36degC (968degF) 20Altered mental status 60Arterial oxygen saturation 90 20
Risk Class 30-Day Mortality (95 CI) Total Point Scoredagger
I 16 (09ndash26) 65II 35 (25ndash47) 66ndash85III 71 (57ndash87) 86ndash105IV 114 (93ndash138) 106ndash125V 239 (214ndash265) 125
Mortality by class reported for the 5177-patient internal validation sampledaggerA total point score for a given patient is obtained by summing the patientrsquos agein years and the points for each applicable prognostic variable
hypertension recent stroke or surgery and bleeding diathesis185
646 Annals of Emergency Medicine
onclusionIn conclusion there is little evidence to guide the emergency
hysician in the administration of thrombolytic therapyverwhelming consensus opinion based on Class III reports
nd published clinical guidelines is to treat hemodynamicallynstable patients with confirmed PE when the benefits ofreatment outweigh the risks Also based on available evidencehrombolytic therapy does not reduce mortality in the majorityf hemodynamically stable patients Because it is doubtful thatny randomized study in the treatment of the hemodynamicallynstable patients will ever receive Institutional Review Boardpproval future studies need to focus on the treatment ofemodynamically stable patients at higher risk for adverseutcomes who present during the initial hours of symptomnset as well as determining whether outcomes other thanortality and recurrent PE should be used The PEITHO trial
s in progress and is a multicenter double-blinded randomizedontrolled trial comparing tenecteplase with placebo in PEatients with right ventricular dysfunction and an elevatedroponin level158 Primary outcome is 7-day mortality oremodynamic collapse with an enrollment goal of 1000atients It is hoped that this study will provide evidence toupport recommendations for thrombolytic therapy in thisubgroup of patients at higher risk for adverse outcome
Relevant industry relationships There were no relevantndustry relationships disclosed by the subcommittee orommittee members
Relevant industry relationships are those relationshipsith companies associated with products or services that
ignificantly impact the specific aspect of disease addressedn the critical question
EFERENCES1 American College of Emergency Physicians Clinical policy
critical issues in the evaluation and management of patientspresenting with suspected pulmonary embolism Ann EmergMed 200341257-270
2 Sutherland SF Pulmonary embolism Emedicine 2009 May 8Available at httpwwwmedscatecomviewarticle552618Accessed October 20 2009
3 Wood KE Major pulmonary embolism review of a pathophysiologicapproach to the golden hour of hemodynamically significantpulmonary embolism Chest 2002121877-905
4 Moser KM Fatal pulmonary embolism old pitfalls newchallenges Mayo Clin Proc 199570501-502
5 Menzel T Wagner S Kramm T et al Pathophysiology ofimpaired right and left ventricular function in chronic embolicpulmonary hypertension changes after pulmonarythromboendarterectomy Chest 2000118897-903
6 Hirsh J Hoak J Council on Thrombosis (in consultation with theCouncil on Cardiovascular Radiology) American HeartAssociation Management of deep vein thrombosis andpulmonary embolism A statement for healthcare professionalsCirculation 1996932212-2245
7 Bell WR Simon TL Current status of pulmonary thromboembolicdisease pathophysiology diagnosis prevention and treatment
Am Heart J 1982103239-262
Volume June
Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Clinical Policy
8 Schulman S Lindmarker P Holmstrom M et al Post-thromboticsyndrome recurrence and death 10 years after the first episodeof venous thromboembolism treated with warfarin for 6 weeks or6 months J Thromb Haemost 20064734-742
9 Moser KM Fedullo PF LitteJohn JK et al Frequentasymptomatic pulmonary embolism in patients with deep venousthrombosis JAMA 1994271223-225
10 van Rossum AB van Houwelingen HC Kieft GJ et al Prevalenceof deep vein thrombosis in suspected and proven pulmonaryembolism a meta-analysis Br J Radiol 1998711260-1265
11 Anderson DR Kahn SR Rodger MA et al Computedtomographic pulmonary angiography vs ventilation-perfusion lungscanning in patients with suspected pulmonary embolism Arandomized controlled trial JAMA 20072982743-2753
12 Sostman HD Stein PD Gottschalk A et al Acute pulmonaryembolism sensitivity and specificity of ventilation-perfusionscintigraphy in PIOPED II study Radiology 2008246941-946
13 Anderson DR Barnes DC Computerized tomographic pulmonaryangiography versus ventilation perfusion lung scanning for thediagnosis of pulmonary embolism Curr Opin Pulm Med 200915425-429
14 Brenner DJ Hall EJ Phil D Computed tomographymdashanincreasing source of radiation exposure N Engl J Med 20073572277-2284
15 Fazel R Krumholz HM Wang Y et al Exposure to low-doseionizing radiation from medical imaging procedures N EnglJ Med 2009361849-857
16 Stein EG Haramati LB Bellin E et al Radiation exposure frommedical imaging in patients with chronic and recurrentconditions J Am Coll Radiol 20107351-359
17 Stein EG Haramati LB Chamarthy M et al Success of a safeand simple algorithm to reduce use of CT pulmonaryangiography in the emergency department AJR Am JRoentgenol 2010194392-397
18 Schriger DL Cantrill SV Greene CS The origins benefitsharms and implications of emergency medicine clinical policiesAnn Emerg Med 199322597-602
19 Wicki J Perneger TV Junod AF et al Assessing clinicalprobability of pulmonary embolism in the emergency ward ArchIntern Med 200116192-97
20 Le Gal G Righini M Roy P-M et al Prediction of pulmonaryembolism in the emergency department the revised Genevascore Ann Intern Med 2006144165-171
21 Klok FA Mos IC Nijkeuter M et al Simplification of the revisedGeneva score for assessing clinical probability of pulmonaryembolism Arch Intern Med 20081682131-2136
22 Wells PS Anderson DR Rodger M et al Derivation of a simpleclinical model to categorize patients probability of pulmonaryembolism increasing the models utility with the SimpliREDD-dimer Thromb Haemost 200083416-420
23 Kline JA Nelson RD Jackson RE et al Criteria for the safe useof D-dimer testing in emergency department patients withsuspected pulmonary embolism a multicenter US study AnnEmerg Med 200239144-152
24 Miniati M Monti S Bottai M A structured clinical model forpredicting the probability of pulmonary embolism Am J Med2003114173-179
25 Miniati M Bottal M Monti S et al Simple and accurateprediction of the clinical probability of pulmonary embolismAm J Respir Crit Care Med 2008178290-294
26 Perrier A Roy P-M Aujesky D et al Diagnosing pulmonaryembolism in outpatients with clinical assessment D-dimermeasurement venous ultrasound and helical computedtomography a multicenter management study Am J Med
2004116291-299
Volume June
27 Tillie-Leblond I Marquette C-H Perez T et al Pulmonaryembolism in patients with unexplained exacerbation of chronicobstructive pulmonary disease prevalence and risk factors AnnIntern Med 2006144390-396
28 Chagnon I Bounameaux H Aujesky D et al Comparison of twoclinical prediction rules and implicit assessment among patientswith suspected pulmonary embolism Am J Med 2002113269-275
29 Moores LK Collen JF Woods KM et al Practical utility of clinicalprediction rules for suspected acute pulmonary embolism in a largeacademic institution Thromb Res 20041131-6
30 Miniati M Bottai M Monti S Comparison of 3 clinical modelsfor predicting the probability of pulmonary embolism Medicine200584107-114
31 Ollenberger GP Worsley DF Effect of patient location on theperformance of clinical models to predict pulmonary embolismThromb Res 2006118685-690
32 Klok FA Kruisman E Spaan J et al Comparison of the revisedGeneva score with the Wells rule for assessing clinical probabilityof pulmonary embolism J Thromb Haemost 2008640-44
33 Wells PS Ginsberg JS Anderson DR et al Use of a clinicalmodel for safe management of patients with suspectedpulmonary embolism Ann Intern Med 1998129997-1005
34 Wells PS Anderson DR Rodger M et al Excluding pulmonaryembolism at the bedside without diagnostic imagingmanagement of patients with suspected pulmonary embolismpresenting to the emergency department by using a simpleclinical model and D-dimer Ann Intern Med 200113598-107
35 van Belle A Buller HR Huisman MV et al Writing Group for theChristopher Study Investigators Effectiveness of managingsuspected pulmonary embolism using an algorithm combiningclinical probability D-dimer testing and computed tomographyJAMA 2006295172-179
36 Anderson DR Kovacs MJ Dennie C et al Use of spiralcomputed tomography contrast angiography and ultrasonographyto exclude the diagnosis of pulmonary embolism in theemergency department J Emerg Med 200529399-404
37 Kabrhel C Courtney DM Camargo CA Jr et al Potential impactof adjusting the threshold of the quantitative D-dimer based onpretest probability of acute pulmonary embolism Acad EmergMed 200916325-332
38 Goekoop RJ Steeghs N Niessen RW et al Simple and safeexclusion of pulmonary embolism in outpatients usingquantitative D-dimer and Wellsrsquo simplified decision rule ThrombHaemost 200797146-150
39 Hogg K Dawson D Mackway-Jones K Outpatient diagnosis ofpulmonary embolism the MIOPED (Manchester Investigation ofPulmonary Embolism Diagnosis) study Emerg Med J 200623123-127
40 Kruip MJ Slob MJ Schijen JH et al Use of a clinical decisionrule in combination with D-dimer concentration in diagnosticworkup of patients with suspected pulmonary embolism aprospective management study Arch Intern Med 20021621631-1635
41 Sanson B-J Lijmer JG Mac Gillavry MR et al ANTELOPE-StudyGroup Comparison of a clinical probability estimate and twoclinical models in patients with suspected pulmonary embolismThromb Haemost 200083199-203
42 Wolf SJ McCubbin TR Feldhaus KM et al Prospective validationof Wells criteria in the evaluation of patients with suspectedpulmonary embolism Ann Emerg Med 200444503-510
43 Yap KS Kalff V Turlakow A et al A prospective reassessmentof the utility of the Wells score in identifying pulmonary
embolism Med J Aust 2007187333-336
Annals of Emergency Medicine 647
Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Clinical Policy
44 Iles S Hodges AM Darley JR et al Clinical experience and pre-test probability scores in the diagnosis of pulmonary embolismQ J Med 200396211-215
45 Testuz A Le Gal G Righini M et al Influence of specificalternative diagnoses on the probability of pulmonary embolismThromb Haemost 200695958-962
46 Goergen SK Chan T de Campo JF et al Reducing the use ofdiagnostic imaging in patients with suspected pulmonaryembolism validation of a risk assessment strategy Emerg MedAustralas 20051716-23
47 Runyon MS Webb WB Jones AE et al Comparison of theunstructured clinician estimate of pretest probability forpulmonary embolism to the Canadian score and the Charlotterule a prospective observational study Acad Emerg Med 200512587-593
48 PIOPED Investigators Value of the ventilationperfusion scan inacute pulmonary embolism diagnosis Results of the ProspectiveInvestigation of Pulmonary Embolism Diagnosis (PIOPED) JAMA19902632753-2759
49 Barghouth G Yersin B Boubaker A et al Combination ofclinical and VQ scan assessment for the diagnosis ofpulmonary embolism a 2-year outcome prospective study EurJ Nucl Med 2000271280-1285
50 Musset D Parent F Meyer G et al Diagnostic strategy forpatients with suspected pulmonary embolism a prospectivemulticentre outcome study Lancet 20023601914-1920
51 Nilsson T Mare K Carlsson A Value of structured clinical andscintigraphic protocols in acute pulmonary embolism J InternMed 2001250213-218
52 Perrier A Bounameaux H Morabia A et al Diagnosis ofpulmonary embolism by a decision analysis-based strategyincluding clinical probability D-dimer levels andultrasonography a management study Arch Intern Med 1996156531-536
53 Perrier A Miron M-J Desmarais S et al Using clinicalevaluation and lung scan to rule out suspected pulmonaryembolism Is it a valid option in patients with normal results oflower-limb venous compression ultrasonography Arch InternMed 2000160512-516
54 Nordenholz KE Naviaux NW Stegelmeier K et al Pulmonaryembolism risk assessment screening tools the interraterreliability of their criteria Am J Emerg Med 200725285-290
55 Kabrhel C Camargo CA Jr Goldhaber SZ Clinical gestalt andthe diagnosis of pulmonary embolism Does experience matterChest 20051271627-1630
56 Runyon MS Richman PB Kline JA Pulmonary EmbolismResearch Consortium Study Group Emergency medicinepractitioner knowledge and use of decision rules for theevaluation of patients with suspected pulmonary embolismvariations by practice setting and training level Acad EmergMed 20071453-57
57 Kline JA Mitchell AM Kabrhel C et al Clinical criteria toprevent unnecessary diagnostic testing in emergencydepartment patients with suspected pulmonary embolism JThromb Haemost 200421247-1255
58 Pauker SG Kassirer JP The threshold approach to clinicaldecision making N Engl J Med 19803021109-1117
59 Lessler AL Isserman JA Agarwal R et al Testing low-riskpatients for suspected pulmonary embolism a decisionanalysis Ann Emerg Med 201055316-326
60 Kline JA Courtney DM Kabrhel C et al Prospective multicenterevaluation of the pulmonary embolism rule-out criteria J ThrombHaemost 20086772-780
61 Wolf SJ McCubbin TR Nordenholz KE et al Assessment of the
pulmonary embolism rule-out criteria rule for evaluation of
648 Annals of Emergency Medicine
suspected pulmonary embolism in the emergency departmentAm J Emerg Med 200826181-185
62 Geersing GJ Janssen KJM Oudega R et al Excluding venousthromboembolism using point of care D-dimer tests inoutpatients a diagnostic meta-analysis BMJ 2009339b2990
63 Kline JA Runyon MS Webb WB et al Prospective study of thediagnostic accuracy of the simplify D-dimer assay for pulmonaryembolism in emergency department patients Chest 20061291417-1423
64 Stein PD Hull RD Patel KC et al D-dimer for the exclusion ofacute venous thrombosis and pulmonary embolism Asystematic review Ann Intern Med 2004140589-602
65 Di Nisio M Squizzato A Rutjes AW et al Diagnostic accuracy ofD-dimer test for exclusion of venous thromboembolism asystematic review J Thromb Haemost 20075296-304
66 Kearon C Ginsberg JS Douketis J et al An evaluation ofD-dimer in the diagnosis of pulmonary embolism A randomizedtrial Ann Intern Med 2006144812-821
67 Brown MD Rowe BH Reeves MJ et al The accuracy of theenzyme-linked immunosorbent assay D-dimer test in thediagnosis of pulmonary embolism a meta-analysis Ann EmergMed 200240133-144
68 Brown MD Lau J Nelson RD et al Turbidimetric D-dimer test inthe diagnosis of pulmonary embolism a metaanalysis ClinChem 2003491846-1853
69 Courtney DM Steinberg JM McCormick JC Prospectivediagnostic accuracy assessment of the HemosIL HS D-dimer toexclude pulmonary embolism in emergency department patientsThromb Res 201012579-83
70 Ghanima W Almaas V Aballi S et al Management ofsuspected pulmonary embolism (PE) by D-dimer and multi-slicecomputed tomography in outpatients an outcome study JThromb Haemost 200531926-1932
71 Mitchell AM Nordenholz KE Kline JA Tandem measurement ofD-dimer and myeloperoxidase or C-reactive protein to effectivelyscreen for pulmonary embolism in the emergency departmentAcad Emerg Med 200815800-805
72 Parent F Maitre S Meyer G et al Diagnostic value of D-dimerin patients with suspected pulmonary embolism results from amulticentre outcome study Thromb Res 2007120195-200
73 Perrier A Roy P-M Sanchez O et al Multidetector-row computedtomography in suspected pulmonary embolism N Engl J Med20053521760-1768
74 Steeghs N Goekoop RJ Niessen RW et al C-reactive proteinand D-dimer with clinical probability score in the exclusion ofpulmonary embolism Br J Haematol 2005130614-619
75 Than MP Helm J Calder K et al Comparison of high specificitywith standard versions of a quantitative latex D-dimer test in theassessment of community pulmonary embolism HaemosILD-dimer and pulmonary embolism Thromb Res 2009124230-235
76 Carrier M Righini M Djurabi RK et al VIDAS D-dimer incombination with clinical pre-test probability to rule outpulmonary embolism A systematic review of managementoutcome studies Thromb Haemost 2009101886-892
77 Legnani C Cini M Scarvelis D et al Multicenter evaluation of anew quantitative highly sensitive D-dimer assay the HemosilregD-dimer HS 500 in patients with clinically suspected venousthromboembolism Thromb Res 2010125398-401
78 Runyon MS Beam DM King MC et al Comparison of theSimplify D-dimer assay performed at the bedside with alaboratory-based quantitative D-dimer assay for the diagnosis ofpulmonary embolism in a low prevalence emergency department
population Emerg Med J 20082570-75
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
79 Ten Wolde M Hagen PJ Macgillavry MR et al Non-invasivediagnostic work-up of patients with clinically suspectedpulmonary embolism results of a management study J ThrombHaemost 200421110-1117
80 Qaseem A Snow V Barry P et al Current diagnosis of venousthromboembolism in primary care a clinical practice guidelinefrom the American Academy of Family Physicians and theAmerican College of Physicians Ann Fam Med 2007557-62
81 Segal JB Eng J Tamariz LJ et al Review of the evidence ondiagnosis of deep venous thrombosis and pulmonary embolismAnn Fam Med 2007563-73
82 Torbicki A Perrier A Konstantinides S et al The Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism ofthe European Society of Cardiology (ESC) Guidelines on thediagnosis and management of acute pulmonary embolism EurHeart J 2008292276-2315
83 Righini M Aujesky D Roy P-M et al Clinical usefulness ofD-dimer depending on clinical probability and cutoff value inoutpatients with suspected pulmonary embolism Arch InternMed 20041642483-2487
84 Righini M Le Gal G Aujesky D et al Diagnosis of pulmonaryembolism by multidetector CT alone or combined with venousultrasonography of the leg a randomized non-inferiority trialLancet 20083711343-1352
85 Kabrhel C Outcomes of high pretest probability patientsundergoing D-dimer testing for pulmonary embolism a pilotstudy J Emerg Med 200835373-377
86 Sohne M Kamphuisen PW van Mierlo PJ et al Diagnosticstrategy using a modified clinical decision rule and D-dimer testto rule out pulmonary embolism in elderly in- and outpatientsThromb Haemost 200594206-210
87 Righini M Le Gal G De Lucia S et al Clinical usefulness ofD-dimer testing in cancer patients with suspected pulmonaryembolism Thromb Haemost 200695715-719
88 Di Nisio M Sohne M Kamphuisen PW et al D-dimer test incancer patients with suspected acute pulmonary embolismJ Thromb Haemost 200531239-1242
89 King V Vaze AA Moskowitz CS et al D-dimer assay to excludepulmonary embolism in high-risk oncologic populationcorrelation with CT pulmonary angiography in an urgent caresetting Radiology 2008247854-861
90 Kline JA Williams GW Hernandez-Nino J D-dimer concentrationsin normal pregnancy new diagnostic thresholds are needed ClinChem 200551825-829
91 Brown MA Vance SJ Kline JA An emergency departmentguideline for the diagnosis of pulmonary embolism an outcomestudy Acad Emerg Med 20051220-25
92 Linkins L-A Bates SM Ginsberg JS et al Use of differentD-dimer levels to exclude venous thromboembolism depending onclinical pretest probability J Thromb Haemost 200421256-1260
93 Douma RA le Gal G Sohne M et al Potential of an ageadjusted D-dimer cut-off value to improve the exclusion ofpulmonary embolism in older patients a retrospective analysisof three large cohorts BMJ 2010340c1475
94 Duriseti RS Brandeau ML Cost-effectiveness of strategies fordiagnosing pulmonary embolism among emergency departmentpatients presenting with undifferentiated symptoms Ann EmergMed 201056321-332
95 Le Gal G Righini M Roy P-M et al Value of D-dimer testing forthe exclusion of pulmonary embolism in patients with previousvenous thromboembolism Arch Intern Med 2006166176-180
96 Duriseti RS Shachter RD Brandeau ML Value of quantitativeD-dimer assays in identifying pulmonary embolism implicationfrom a sequential decision model Acad Emerg Med 200613
755-766
Volume June
97 Remy-Jardin M Remy J Wattinne L et al Central pulmonarythromboembolism diagnosis with spiral volumetric CT with thesingle-breath-hold techniquemdashcomparison with pulmonaryangiography Radiology 1992185381-387
98 Russo V Piva T Lovato L et al Multidetector CT a new goldstandard in the diagnosis of pulmonary embolism State of theart and diagnostic algorithms Radiol Med 200510949-63
99 Perrier A Howarth N Didier D et al Performance of helicalcomputed tomography in unselected outpatients with suspectedpulmonary embolism Ann Intern Med 200113588-97
00 Ost D Rozenshtein A Saffran L et al The negative predictivevalue of spiral computed tomography for the diagnosis ofpulmonary embolism in patients with nondiagnostic ventilation-perfusion scans Am J Med 200111016-21
01 Nilsson T Soderberg M Lundqvist G et al A comparison of spiralcomputed tomography and latex agglutination D-dimer assay inacute pulmonary embolism using pulmonary arteriography as goldstandard Scand Cardiovasc J 200236373-377
02 Ruiz Y Caballero P Caniego JL et al Prospective comparisonof helical CT with angiography in pulmonary embolism globaland selective vascular territory analysis Interobserveragreement Eur Radiol 200313823-829
03 Stone E Roach P Bernard E et al Use of computedtomography pulmonary angiography in the diagnosis ofpulmonary embolism in patients with an intermediate probabilityventilationperfusion scan Intern Med J 20033374-78
04 van Strijen MJ De Monye W Kieft GJ et al Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism aprospective multicenter cohort study of consecutive patientswith abnormal perfusion scintigraphy J Thromb Haemost 2005317-25
05 Eng J Krishnan JA Segal JB et al Accuracy of CT in thediagnosis of pulmonary embolism a systematic literaturereview AJR Am J Roentgenol 20041831819-1827
06 Stein PD Kayali F Hull RD Spiral computed tomography for thediagnosis of acute pulmonary embolism Thromb Haemost200798713-720
07 Cueto SM Cavanaugh SH Benenson RS et al Computedtomography scan versus ventilation-perfusion lung scan in thedetection of pulmonary embolism J Emerg Med 200121155-164
08 Stein PD Fowler SE Goodman LR et al for the PIOPED IIInvestigators Multidetector computed tomography for acutepulmonary embolism N Engl J Med 20063542317-2327
09 Winer-Muram HT Rydberg J Johnson MS et al Suspectedacute pulmonary embolism evaluation with multidetector row CTversus digital subtraction pulmonary arteriography Radiology2004233806-815
10 Coche E Verschuren F Keyeux A et al Diagnosis of acutepulmonary embolism in outpatients comparison of thin-collimation multidetector row spiral CT and planar ventilation-perfusion scintigraphy Radiology 2003229757-765
11 Moores LK Jackson WL Jr Shorr AF et al Meta-analysisoutcomes in patients with suspected pulmonary embolismmanaged with computed tomographic pulmonary angiographyAnn Intern Med 2004141866-874
12 Hayashino Y Goto M Noguchi Y et al Ventilation-perfusionscanning and helical CT in suspected pulmonary embolismmeta-analysis of diagnostic performance Radiology 2005234740-748
13 Hogg K Brown G Dunning J et al Diagnosis of pulmonaryembolism with CT pulmonary angiography a systematic review
Emerg Med J 200623172-178
Annals of Emergency Medicine 649
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
114 Roy PM Colombet I Durieux P et al Systematic review andmeta-analysis of strategies for the diagnosis of suspectedpulmonary embolism BMJ 2005331259
115 Goodman LR Lipchik RJ Kuzo RS et al Subsequent pulmonaryembolism risk after a negative helical CT pulmonaryangiogrammdashprospective comparison with scintigraphyRadiology 2000215535-542
116 Swensen SJ Sheedy PF II Ryu JH et al Outcomes afterwithholding anticoagulation from patients with suspected acutepulmonary embolism and negative computed tomographicfindings a cohort study Mayo Clin Proc 200277130-138
117 Donato AA Scheirer JJ Atwell MS et al Clinical outcomes inpatients with suspected acute pulmonary embolism andnegative helical computed tomographic results in whomanticoagulation was withheld Arch Intern Med 20031632033-2038
118 van Strijen MJ de Monye W Schiereck J et al Single-detectorhelical computed tomography as the primary diagnostic test insuspected pulmonary embolism a multicenter clinicalmanagement study of 510 patients Ann Intern Med 2003138307-314
119 Friera A Olivera MJ Suarez C et al Clinical validity of negativehelical computed tomography for clinical suspicion of pulmonaryembolism Respiration 20047130-36
120 Kavanagh EC OrsquoHare A Hargaden G et al Risk of pulmonaryembolism after negative MDCT pulmonary angiography findingsAJR Am J Roentgenol 2004182499-504
121 Prologo JD Gilkeson RC Diaz M et al The effect of single-detector CT versus MDCT on clinical outcomes in patients withsuspected acute pulmonary embolism and negative results onCT pulmonary angiography AJR Am J Roentgenol 20051841231-1235
122 Vigo M Pesavento R Bova C et al The value of four-detectorrow spiral computed tomography for the diagnosis of pulmonaryembolism Semin Thromb Hemost 200632831-837
123 Subramaniam RM Blair D Gilbert K et al Withholdinganticoagulation after a negative computed tomographypulmonary angiogram as a stand-alone imaging investigation aprospective management study Int Med J 200737624-630
124 Elias A Colombier D Victor G et al Diagnostic performance ofcomplete lower limb venous ultrasound in patients with clinicallysuspected acute pulmonary embolism Thromb Haemost 200491187-195
125 Le Gal G Righini M Sanchez O et al A positive compressionultrasonography of the lower limb veins is highly predictive ofpulmonary embolism on computed tomography in suspectedpatients Thromb Haemost 200695963-966
126 Au VW Walsh G Fon G Computed tomography pulmonaryangiography with pelvic venography in the evaluation of thrombo-embolic disease Australas Radiol 200145141-145
127 Coche EE Hamoir XL Hammer FD et al Using dual-detectorhelical CT angiography to detect deep venous thrombosis inpatients with suspicion of pulmonary embolism diagnostic valueand additional findings AJR Am J Roentgenol 20011761035-1039
128 Begemann PG Bonacker M Kemper J et al Evaluation of thedeep venous system in patients with suspected pulmonaryembolism with multi-detector CT a prospective study incomparison to Doppler sonography J Comput Assist Tomogr200327399-409
129 Johnson JC Brown MD McCullough N et al CT lower extremityvenography in suspected pulmonary embolism in the ED EmergRadiol 200612160-163
130 Loud PA Katz DS Bruce DA et al Deep venous thrombosis
with suspected pulmonary embolism detection with combined
650 Annals of Emergency Medicine
CT venography and pulmonary angiography Radiology 2001219498-502
31 Perrier A Bounameaux H Accuracy or outcome in suspectedpulmonary embolism N Engl J Med 200635422
32 Tapson VF Acute pulmonary embolism N Engl J Med 20083581037-1052
33 Goodman LR Stein PD Matta F et al CT venography andcompression sonography are diagnostically equivalent datafrom PIOPED II AJR Am J Roentgenol 20071891071-1076
34 FibrinolyticTherapyTrialists (FTT) Collaborative Group Indicationsfor fibrinolytic therapy in suspected acute myocardial infarctioncollaborative overview of early mortality and major morbidityresults from all randomised trials of more than 1000 patientsLancet 1994343311-322
35 The National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group Tissue plasminogen activator for acuteischemic stroke N Engl J Med 19953331581-1587
36 Hacke W Kaste M Bluhmki E et al Thrombolysis withalteplase 3 to 45 hours after acute ischemic stroke N EnglJ Med 20083591317-1329
37 British Thoracic Society Standards of Care CommitteePulmonary Embolism Guideline Development Group BritishThoracic Society guidelines for the management of suspectedacute pulmonary embolism Thorax 200358470-483
38 Buller HR Agnelli G Hull RD et al Antithrombotic therapy forvenous thromboembolic disease the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy Chest 2004126401S-428S
39 Dalen JE Alpert JS Hirsh J Thrombolytic therapy for pulmonaryembolism Is it effective Is it safe When is it indicated ArchIntern Med 19971572550-2556
40 Dalen JE Thrombolysis in submassive PE No J ThrombHaemost 200311130-1132
41 Konstantinides S Thrombolysis in submassive pulmonaryembolism Yes J Thromb Haemost 200311127-1129
42 Harris T Meek S When should we thrombolyse patients withpulmonary embolism A systematic review of literature EmergMed J 200522766-771
43 Anderson DR Levine MN Thrombolytic therapy for the treatmentof acute pulmonary embolism CMAJ 19921461317-1324
44 Konstantinides S Tiede N Geibel A et al Comparison ofalteplase versus heparin for resolution of major pulmonaryembolism Am J Cardiol 199882966-970
45 Nass N McConnell MV Goldhaber SZ et al Recovery ofregional right ventricular function after thrombolysis forpulmonary embolism Am J Cardiol 199983804-806
46 Dalla-Volta S Palla A Santolicandro A et al PAIMS2 alteplasecombined with heparin versus heparin in the treatment of acutepulmonary embolism Plasminogen Activator Italian MulticenterStudy 2 J Am Coll Cardiol 199220520-526
47 Goldhaber SZ Haire WD Feldstein ML et al Alteplase versusheparin in acute pulmonary embolism randomised trialassessing right-ventricular function and pulmonary perfusionLancet 1993341507-511
48 Levine M Hirsh J Weitz J et al A randomized trial of a singlebolus dosage regimen of recombinant tissue plasminogenactivator in patients with acute pulmonary embolism Chest1990981473-1479
49 Ly B Arnesen H Eie H et al A controlled clinical trial ofstreptokinase and heparin in the treatment of major pulmonaryembolism Acta Med Scand 1978203465-470
50 PIOPED Investigators Tissue plasminogen activator for thetreatment of acute pulmonary embolism A collaborative study
by the PIOPED Investigators Chest 199097528-533
Volume June
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Clinical Policy
151 Urokinase Pulmonary Embolism Trial (UPET) Study GroupUrokinase pulmonary embolism trial Phase 1 results Acooperative study JAMA 19702142163-2172
152 Konstantinides S Geibel A Heusel G et al for theManagement Strategies and Prognosis of Pulmonary Embolism-3Trial Investigators Heparin plus alteplase compared withheparin alone in patients with submassive pulmonary embolismN Engl J Med 20023471143-1150
153 Dotter CT Seaman AJ Rosch J et al Streptokinase andheparin in the treatment of major pulmonary embolism arandomized comparison Vasc Surg 19791342-52
154 Jerjes-Sanchez C Ramirez-Rivera A de Lourdes Garcia M et alStreptokinase and heparin versus heparin alone in massivepulmonary embolism a randomized controlled trial J ThrombThrombolysis 19952227-229
155 Marini C Di Ricco G Rossi G et al Fibrinolytic effects ofurokinase and heparin in acute pulmonary embolism arandomized clinical trial Respiration 198854162-173
156 Tibbutt DA Davies JA Anderson JA et al Comparison bycontrolled clinical trial of streptokinase and heparin in treatmentof life-threatening pulmonary embolism Br Med J 19741343-347
157 Becattini C Agnelli G Salvi A et al TIPES Study Group Bolustenecteplase for right ventricle dysfunction in hemodynamicallystable patients with pulmonary embolism Thromb Res 2010125e82-e86
158 Meyer G PEITHO Pulmonary Embolism Thrombolysis StudyClinical Trialsgov [Web site] Bethesda MD National Library ofMedicine 2000 Available at httpclinicaltrialsgovct2showNCT00639743temnct00639743 NLMIdentifierNCT00639743 Accessed May 11 2010
159 Agnelli G Becattini C Kirschstein T Thrombolysis vs heparin inthe treatment of pulmonary embolism A clinical outcome-basedmeta-analysis Arch Intern Med 20021622537-2541
160 Thabut G Thabut D Myers RP et al Thrombolytic therapy ofpulmonary embolism A meta-analysis J Am Coll Cardiol 2002401660-1667
161 Wan S Quinlan DJ Agnelli G et al Thrombolysis compared withheparin for the initial treatment of pulmonary embolism A meta-analysis of the randomized controlled trials Circulation 2004110744-749
162 Dong B Jirong Y Liu G et al Thrombolytic therapy forpulmonary embolism Cochrane Database Syst Rev 2006(2)CD004437 DOI 10100214651858CD004437pub2
163 Goldhaber SZ Echocardiography in the management ofpulmonary embolism Ann Intern Med 2002136691-700
164 Nakamura M Nakanishi N Yamada N et al Effectiveness andsafety of the thrombolytic therapy for acute pulmonarythromboembolism results of a multicenter registry in theJapanese Society of Pulmonary Embolism Research IntJ Cardiol 20059983-89
165 Wolfe MW Lee RT Feldstein ML et al Prognosticsignificance of right ventricular hypokinesis and perfusionlung scan defects in pulmonary embolism Am Heart J 19941271371-1375
166 Wood KE Major pulmonary embolism Review of apathophysiologic approach to the golden hour ofhemodynamically significant pulmonary embolism Chest2002121877-905
167 Kasper W Konstantinides S Geibel A et al Managementstrategies and determinants of outcome in acute majorpulmonary embolism results of a multicenter registry J Am Coll
Cardiol 1997301165-1171
Volume June
68 American Thoracic Society The diagnostic approach to acutevenous thromboembolism Clinical practice guideline Am JRespir Crit Care Med 19991601043-1066
69 Kasper W Konstantinides S Geibel A et al Prognosticsignificance of right ventricular afterload stress detected byechocardiography in patients with clinically suspected pulmonaryembolism Heart 199777346-349
70 Torbicki A Gali N Covezzoli A et al Right heart thrombi inpulmonary embolism Results from the International CooperativePulmonary Embolism Registry J Am Coll Cardiol 2003412245-2251
71 Rose PS Punjabi NM Pearse DB Treatment of right heartthromboemboli Chest 2002121806-814
72 Goldhaber SZ Visani L De Rosa M Acute pulmonaryembolism clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER) Lancet 19993531386-1389
73 Konstantinides S Geibel A Olschewski M et al Associationbetween thrombolytic treatment and the prognosis ofhemodynamically stable patients with major pulmonaryembolism Results of a multicenter registry Circulation 199796882-888
74 Becattini C Vedovati MC Agnelli G Prognostic value oftroponins in acute pulmonary embolism A meta-analysisCirculation 2007116427-433
75 Kucher N Wallmann D Carone A et al Incrementalprognostic value of troponin I and echocardiography inpatients with acute pulmonary embolism Eur Heart J 2003241651-1656
76 Aujesky D Obrosky S Stone RA et al A prediction rule toidentify low-risk patients with pulmonary embolism Arch InternMed 2006166169-175
77 Jimenez D Uresandi F Otero R et al Troponin-based riskstratification of patients with acute nonmassive pulmonaryembolism Systematic review and metaanalysis Chest 2009136974-982
78 Kreit JW The impact of right ventricular dysfunction on theprognosis and therapy of normotensive patients with pulmonaryembolism Chest 20041251539-1545
79 Klok FA Mos IC Huisman MV Brain-type natriuretic peptidelevels in the prediction of adverse outcome in patients withpulmonary embolism A systematic review and meta-analysisAm J Respir Crit Care Med 2008178425-430
80 Stein PD Matta F Janjua M et al Outcome in stable patientswith acute pulmonary embolism who had right ventricularenlargement andor elevated levels of troponin I Am J Cardiol2010106558-563
81 Aujesky D Obrosky DS Stone RA et al Derivation andvalidation of a prognostic model for pulmonary embolism Am JRespir Crit Care Med 20051721041-1046
82 Aujesky D Roy P-M Le Manach CP et al Validation of a modelto predict adverse outcomes in patients with pulmonaryembolism Eur Heart J 200627476-481
83 Donze J Le Gal G Fine MJ et al Prospective validation ofthe Pulmonary Embolism Severity Index A clinical prognosticmodel for pulmonary embolism Thromb Haemost 2008100943-948
84 Kanter DS Mikkola KM Patel SR et al Thrombolytic therapyfor pulmonary embolism Frequency of intracranialhemorrhage and associated risk factors Chest 19971111241-1245
85 River-Bou WL Cabanas JG Villanueva SE et al Thrombolytictherapy eMedicine 2008 Available at httpemedicinemedscapecomarticle811234-overview Accessed December
16 2009
Annals of Emergency Medicine 651
sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

sectObjective is to predict outcome including mortality and morbidity
Fatally flawed X X X
experimental and control groups)
Clinical Policy
652 Annals of Emergency Medicine
DiagnosisDagger
Prognosissect
ve cohort using a criterionrd or meta-analysis ofctive studies
Population prospective cohort ormeta-analysis of prospectivestudies
ctive observational Retrospective cohortCase control
iesort consensus review)
Case seriesCase reportOther (eg consensus review)
lly
Appendix A Literature classification schema
DesignClass Therapydagger
1 Randomized controlled trial ormeta-analyses ofrandomized trials
Prospectistandaprospe
2 Nonrandomized trial Retrospe
3 Case seriesCase reportOther (eg consensus review)
Case serCase repOther (eg
Some designs (eg surveys) will not fit this schema and should be assessed individuadaggerObjective is to measure therapeutic efficacy comparing interventionsDaggerObjective is to determine the sensitivity and specificity of diagnostic tests
Appendix B Approach to downgrading strength of evidence
Downgrading
DesignClass
1 2 3
None I II III1 level II III X2 levels III X X
Appendix C Likelihood ratios and number needed to treat
LR () LR ()
10 10 Useless1ndash5 05ndash1 Rarely of value only minimally changes
pretest probability10 01 Worthwhile test may be diagnostic if
the result is concordant with pretestprobability
20 005 Strong test usually diagnostic100 001 Very accurate test almost always
diagnostic even in the setting of lowor high pretest probability
Number needed to treat (NNT) number of patients who need to be treated toachieve 1 additional good outcome NNT1absolute risk reduction100where absolute risk reduction is the risk difference between 2 event rates (ie
Volume June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e1
652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e2A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e3
652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e4A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e5
652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e6A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e7
652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e8A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e9
652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e10A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e11
652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e12A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e13
652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e14A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e15
652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e16A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e17
652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e18A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e19
652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e20A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e21
652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e22A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e23
652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e24A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e25
652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e26A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e27
652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e28A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e29
652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e30A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e31
652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e32A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e33
652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e34A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e35
652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e36A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e37
652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e38A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e39
652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e40A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e41
652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e42A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e43
652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e44A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e45
652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e46A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e47
652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e48A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e49
652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e50A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e51
652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e52A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e53
652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e54A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e55
652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e56A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e57
652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e58A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e59
652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e60A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e61
652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e62A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e63
652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e64A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e65
652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e66A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e67
652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e68A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e69
652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e70A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e71
652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e72A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e73
652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

652
ClinicalPolicy
e74A
nnalsof
Em
ergencyM
edicineV
olume
June
Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75

Volum
ClinicalPolicy
e
June
Annals
ofE
mergency
Medicine
652e75