Embed Size (px)
Citation preview

PDSA
NewcastleExperience
Level1Hospitals11th January2016
DrAngusVincentRegionalCLODNorthern

Plan-Do-Study-Act• Achievingchangeandgettingthingsdoneoncriticalcareunits
ishard.
“…delivering improvement inhealthcarerequiresthealterationofprocesseswithincomplexsocialsystemsthatchangeovertimeinpredictableandunpredictableways.”
• Hugeinfluenceoflocalcontext onsuccessofanintervention
Level1Meeting, January2016

Level1Meeting, January2016

Plan-Do-Study-Act
• Aqualityimprovementtool(toeffectchange ornewprocess)
• EndorsedbyNHSInstituteforInnovationandImprovement
• Longhistory,originatedinthebusinessworld
Level1Meeting, January2016

PDSA- Essence• Startsmallandsimple– e.g.1patient
• Iterative
• Effectiveinterventionsareusuallycomplexandmulti-facetedandadapttolocalcontextandallowforunforseencircumstance
Level1Meeting, January2016

Level1Meeting, January2016

EUwideproject– multipleworkstreams
Thus– pickaprojectandimplementbyPDSAmethodology
Level1Meeting, January2016

Phase1– IdentifyingtheProblem
DBDConsent
62%
DCDConsent
45%Level1Meeting, January2016

Phase1– IdentificationoftheProblem
SignificantdropinconsentratesMarch– August2013
CombinedDBD/DCD 55%ConsentWithSNOD 72% WithoutSNOD20%SNODUsed 54%
Despiteafullytrainedconsultantbody
ConcernsfromournursingstaffregardingtheSNODrolewereidentified
Level1Meeting, January2016

ModelforImprovement
Whatwerewetryingtoachieve?
IncreasedconsentratesbyincreasingSN-ODinvolvement
Howwouldweknowthechangewasanimprovement?
MeasureconsentratesandSN-ODinvolvementratesinPhase2datacollectionofACCORD,alongsideUKPDA
Level1Meeting, January2016

Plan- Do
1.Targetnursingstaff- specifictraininginterventionontheconsentprocess– valueaddedbySNOD
2.PeerReviewConsultantPerformance – ‘public’feedbackontheirconsentpracticeatmonthlyM+M
3.ClarifyourUnitExpectationandPractice – explicitstepbystepconsentpracticeoutlinedinourunitdonationdocumentation
Level1Meeting, January2016

Do– NurseMandatoryTraining
Time Subject Speaker
09:00-09:15 Introduction, NICE guidelines, Organ Donation as part of good end of life care.
Kate Dreyer (Specialist Nurse –Organ Donation)
09:15-09:45 Donation after Circulatory Death (DCD) Linda Wilson (Specialist Nurse –Organ Donation)
09:45-10:15 Donation after Brain Stem Death (DBD) Dr Phil Laws/Sue Lee (SN-OD)
10:15-10:30 Donor family experience of organ donation Lesley Kremer (Donor Family Member)
10:30-11:00 TEA/COFFEE & CAKES
11:00-11:30 Planning a collaborative approach & the role of the SNOD in the donation process.
Specialist Nurses –Organ Donation
11:30-12:30 Role play – approaching families about organ & tissue donation.
All
12:30-13:00 Discussion & debriefing – chance for the staff to discuss any issues, questions, previous experiences.
All
Level1Meeting, January2016

Do - M&MReportingTotal Deaths
Uncontrolled Deaths
BSD/WLST with contraindications
to donation
No. of Potential Donors
Referral Rate
No Families approached
SNOD involvement
rate
Consent Rate
8 2 1 5 100% 4 75% 50%
Initials Age Gender
Diagnosis BSD/WLST On ODR? SNOD used in approach
Consent?
Organs donated/Reason for refusal
JI 43 M TBI BSD Y Referred but coroner refused permission for donation due to circumstances surrounding death.
XS 48 F HBI following OOHCA
BSD N Y N Husband was not accepting of death, organ donation was brought up with SNOD present, husband didn’t realy answer the question but due to circumstances was not reapproached.
SB 17 F TBI BSD Y Y Y DBD donor – donated heart, liver to be split, kidneys, pancreas & small bowel. Lungs unsuitable due to consolidation.
KG 30 F ICH WLST Y Y Y DCD donor – donated liver, kidneys & pancreas. Lungs placed but unsuitable at retrieval. Family brought up donation when SNOD was present.
DH 70 F CVA WLST N N N Kidneys suitable for donation. Referred, on call SNOD was at Freeman & offered to come but consultant approached alone due to time pressures.
Level1Meeting, January2016

Study
• Phase2(Dec13– May14)
• Overallconsentrate- 76%
• UseofSNOD– 96%(27/28)
0
5
10
15
20
25
30
FamiliesApproached(N) SNODInvolved(N) Consents(N)
Phase1Phase2
Level1Meeting, January2016

Act Sustainability(April14– March15)
DBD Familiesapproached 27SNODused 27 =100%Consent 17/27 =63%
DCD Familiesapproached 25SNODused 24 =96%Consent 20/25 =80%
Level1Meeting, January2016

WasthistruePDSA?
• Inpart– Plannedafterdiscussion– Deliberateandmonitoredintervention– Impactassessedandpresented
• But,– Didn’tstartsmall– Didn’tanalyseandrepeatwithmodification
Level1Meeting, January2016

11th January 2016 Programme
Time Topic Speaker/s
1000-1030 RegistrationandCoffee
1030-1050 Level1nationalupdate DrDaleGardinerDeputyNationalCLOD
1050-1130 Sharingbestpracticesession Various
1130-1200 Results, neurological deathtestingaudit DrPaulMurphyNational CLOD
1200-1220 PDSA,howweusedthemethodology DrAngus VincentRegionalCLOD,Northern
1220-1250 PDSAExercise1 DrPaulMurphy (chair)
1250-1330 Lunch
1330-1400 PDSAExercise2 DrMalcolmWatters(chair)RegionalCLOD,SouthCentral
1400-1440 Group1Ante-morteminterventionworkshop andGroup2EDstrategyworkshop
1440-1500 Coffee
1500-1540 Group1EDstrategyworkshopandGroup2Ante-morteminterventionworkshop
1540-1600 Level1s andtheirimportancetoNHSBT Mr IanTrenholmChief Executive, NHSBT
The Wesley, 81 – 103 Euston Street, London NW1 2EZ.
Level 1 Meeting, January 2016

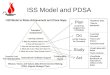
Improvement Model and PDSA Cycles

Overview
Understand the problem and its causes
Define aim and measures
Collect change ideas
Test change idea with PDSA cycles
Implement changes that are improvements
Work with colleagues and value different perspectivesLink frontline changes with strategic objectivesWork towards sustainability as part of implementation

Root cause analysis using the Ishikawa fishbone
example brain death testing
Brain Death (BD) tests are not always carried out when patient meets pre-conditions
Family have declinedResources
BD tests not a standard part of care
Donation will not happen
Lack of knowledge
Doubts/ concerns regarding the validity of testingNo clinical
interpretation of current BD testing policy
Can not/ will not test
Other patients considered to be higher priority for beds
Judicial/ Police refusal
Medical contra-indications
Patient choice not understood by family
Previous poor experience of care whilst in hospital
Approached prematurely Family refused
before a formal approach made
Biased due to adverse press/ TV
Poor approach from staff
Ancillary testing not available/ supported
Lack of suitable medical staff to perform tests
No transplant surgeon available
Lack of availability of expert opinion
Lack of available equipment for testing
Prevented by clinical condition (e.g. hypothermia)
Paediatric case
Doubts about time needed to wait
Lack of confidence / experience in performing tests

What are we trying to achieve?
How will we know that change is an
improvement?
What changes can we make that will result in
improvement?
dostudy
planact
dostudy
planact
The aim should be clear, focussed and based upon real and important problems. It should measurable and, where relevant, in line with national targets.
Any intervention should be designed in such a way that its impact can be accurately measured. Monitoring arrangements need to be agreed before the change idea is introduced.
Change ideas may come from many sources, and are most likely when they concentrate on the patient rather than the various teams involved in the pathway.
The PDSA cycle is a controlled test of a change idea that should provide a quick assessment of whether the idea will be effective or not.
The Model for Improvement

PDSA
Plan: we will do this, in this location, with this expectation
Do: we did this, we made these measurements and observed these unexpected occurrences
Study: our data from the pilot compare with baseline data in this way. We also had the
following problems
Act: as a result of our observations we will now extend the trial, adjust the change idea, trial more widely, implement into practice etc
What are we trying to achieve?
How will we know that change is an improvement?
What changes can we make that will result in improvement?
act plan
study do

What are we trying to achieve?
How will we know that change is an
improvement?
What changes can we make that will result in
improvement?
dostudy
planact
dostudy
planact
The aim should be clear, focussed and based upon real and important problems. It should measurable and, where relevant, in line with national targets.
Any intervention should be designed in such a way that its impact can be accurately measured. Monitoring arrangements need to be agreed before the change idea is introduced.
Change ideas may come from many sources, and are most likely when they concentrate on the patient rather than the various teams involved in the pathway.
The PDSA cycle is a controlled test of a change idea that should provide a quick assessment of whether the idea will be effective or not.
What are we trying to achieve?
How will we know that change is an
improvement?
What changes can we make that will result in
improvement?
dostudy
planact
dostudy
planact
The aim should be clear, focussed and based upon real and important problems. It should measurable and, where relevant, in line with national targets.
Any intervention should be designed in such a way that its impact can be accurately measured. Monitoring arrangements need to be agreed before the change idea is introduced.
Change ideas may come from many sources, and are most likely when they concentrate on the patient rather than the various teams involved in the pathway.
The PDSA cycle is a controlled test of a change idea that should provide a quick assessment of whether the idea will be effective or not.
Level 1 Meeting PDSA Exercise 1
Increase FICM/ICS form use (and thereforeapnoea compliance) in your hospital/s.How will you measure form use and apnoeacompliance?
PDSA Plan
Plan (anything else you need to do):
Do (when will you start):
Study (when will you assess):
Act:

11th January 2016 Programme
Time Topic Speaker/s
1000-1030 RegistrationandCoffee
1030-1050 Level1nationalupdate DrDaleGardinerDeputyNationalCLOD
1050-1130 Sharingbestpracticesession Various
1130-1200 Results, neurological deathtestingaudit DrPaulMurphyNational CLOD
1200-1220 PDSA,howweusedthemethodology DrAngus VincentRegionalCLOD,Northern
1220-1250 PDSAExercise1 DrPaulMurphy (chair)
1250-1330 Lunch
1330-1400 PDSAExercise2 DrMalcolmWatters(chair)RegionalCLOD,SouthCentral
1400-1440 Group1Ante-morteminterventionworkshop andGroup2EDstrategyworkshop
1440-1500 Coffee
1500-1540 Group1EDstrategyworkshopandGroup2Ante-morteminterventionworkshop
1540-1600 Level1s andtheirimportancetoNHSBT Mr IanTrenholmChief Executive, NHSBT
The Wesley, 81 – 103 Euston Street, London NW1 2EZ.
Level 1 Meeting, January 2016

What are we trying to achieve?
How will we know that change is an
improvement?
What changes can we make that will result in
improvement?
dostudy
planact
dostudy
planact
The aim should be clear, focussed and based upon real and important problems. It should measurable and, where relevant, in line with national targets.
Any intervention should be designed in such a way that its impact can be accurately measured. Monitoring arrangements need to be agreed before the change idea is introduced.
Change ideas may come from many sources, and are most likely when they concentrate on the patient rather than the various teams involved in the pathway.
The PDSA cycle is a controlled test of a change idea that should provide a quick assessment of whether the idea will be effective or not.
What are we trying to achieve?
How will we know that change is an
improvement?
What changes can we make that will result in
improvement?
dostudy
planact
dostudy
planact
The aim should be clear, focussed and based upon real and important problems. It should measurable and, where relevant, in line with national targets.
Any intervention should be designed in such a way that its impact can be accurately measured. Monitoring arrangements need to be agreed before the change idea is introduced.
Change ideas may come from many sources, and are most likely when they concentrate on the patient rather than the various teams involved in the pathway.
The PDSA cycle is a controlled test of a change idea that should provide a quick assessment of whether the idea will be effective or not.
Level 1 Meeting PDSA Exercise 2 Takeaperformanceratefromyour
hospital/sthatimpactsonconsent.Howwillyouimproveit?
PDSA Plan
Plan (anything else you need to do):
Do (when will you start):
Study (when will you assess):
Act: