Embed Size (px)
Citation preview

PDGF and TGF-a Act Synergistically to Improve Wound Healingin the Geneotically Diabetic Mouse
REBECCAHL. BROWN, M.D., MA1vrHEwP. BREEDEN, B.S., AND DAVID G. GREENHALGH, M.D., FACS1
Shriners Burns lnstitute and Department af Surgery, University af Cincinnati Callege af Medicine, Cincinnati, Ohia 45229
Presentedat the Annual Meeting oc the Association Cor Academic Surgery, Hershey, Pennsylvania, November 10-13, 1993
witb tbe combination of PDGF-BB and EGF. @ 1994Academic Preaa, Inc.Impaired wound healing results in significant morbid-
ity for the surgical patient. The genetically diabetic(C57BL/KsJ-db/db) mouse is obese, hyperglycemic, in-sulin-resistant, and exhibits markedly impaired woundhealing. Previous studies have demonstrated that thefibroblast mitogens, BB homodimer of platelet-derivedgrowth factor (PDGF-BB) or basic fibroblast growthfactor, plus insulin-like growth factor, act synergisti-caIly to enhance wound closure in the geneticaIly dia-betic mouse. The purpose of this study was to determinewhether the keratinocyte mitogens, epidermal growthfactor (EGF) or transforming growth factor-a (TGF-a),in combination with the fibroblast mitogen, PDGF-BB,would produce a similar synergistic enhancement intissuc rcpair. FuIl-thickness skin wounds created onthe backs of diabetic mice received topical applicationsof vehicle (5% polyethylene glycol), PDGF-BB (10 JLg),EGF (1 JLg), TGF-a (1 JLg), or the combination of PDGF(10 JLg) and EG F (1 JLg) or TG F -a (1 JLg) for 5 consecuti vedays starting at wounding. Application of PDG F -BB orTGF-a alone to wounds in diabetic animals improvedwound closure when compared to vehicle treatment.EGF did not affect healing and did not have any addi-tive effects when combined with PDGF-BB. Signifi-can'.; improvements in wound closure were observedwith the combination of PDGF-BB and TGF-a whencompared to treatment with the individual growth fac-torso The PDGF-BB/TGF-a combination acceleratedhealing in the diabetic animals to arate that was closerto that seen in nondiabetic mice. By histologic analysisat Day 15, aIl criteria for healing were more advancedin the PDGF-BB/TGF-a combination wounds whencompared to the other treatment groups. As aIl woundsapproached complete healing by Day 21, these differ-ences were lost. In summary, PDGF-BB and TGF-aacted synergisticaIly in geneticaIly diabetic mice topromote early wound healing beyond that ofthe individ-ual growth factors. Similar synergy was not observed
"INTRODUCTION
Impaired wound healing is a significan t source of mor-bidity for the surgical patient and may result in suchcomplications as wound dehiscence, anastomotic break-clown, and chronic nonhealing wounds. 1'he cost asso-ciated with such complications may be extreme due toprolonged hospitalization and increased time away fromwork. In the normal host, wound healing is usually un-complicated and proceeds at a rapid rateo In contrast,most healing failures are associated with so me form ofhost impairment, including diabetes, infection, immuno-suppression, obesity, or malnutrition [1-4]. For greaterclinical relevance, wound healing studies should focuson models of impaired healing.
Wound healing is a complex biologic process whichmay be divided into three phases-inflammatory, prolif-erative, and maturational. Growth factors appear to playan important role in all phases ofthis process by orches-trating complex cell-to-cell interactions which are es-sential for successful wound repair. Growth factors,which are released into the wound site at the time ofinjury, have been shown to regulate cellular migration[5-8] and proliferation [9-12] as well as extracellularmatrix deposition and remodeling [13-17]. Multiplegrowth factors or their transcripts have been identifiedin healing wounds, including platelet-derived growthfactor (PDGF) [18-23], basic fibroblast growth factor(bFGF) [20], epidermal growth factor (EGF) [20, 24],transforming growth factor-a (TGF-a) [18, 25, 26],transforming growth factor-{3 (TGF-{3) [18,26,27], insu-lin-like growth factor-I (IGF-I) [18,28], and insulin-likegrowth factor-II (IGF-II) [28]. The specific interactionsof these growth factors, however, are not well under-stood.
It has been hypothesized that impaired wound healingmay result from lack of adequate stimulation by growthfactors. Schultz et al. [29] report that fluid obtained from
lTo whom correspondence and reprint requests should be ad-dressed at Shriners Burns Institute, 3229 Burnet Avenue, Cincinnati,OH 45229. FAX: (513) 872-6999.
562
¡.fr:r T :ri.',,"f'"0022-4804/94 $5.00Copyright @ 1994 by Academic Press, Inc.Al! rights of reproduction in any form reserved.
.sI
t. p,¡:- + rCrl(~ ""~F + ~ 61"' f_~~
563BROWN, BREEDEN, AND GREENHALGH: PDGF AND TGF-a IMPROVE WOUND HEALING
versity of Cincinnati Institutional Animal Care Utiliza-tion Committee.
Tissue repair in the genetically diabetic (C57BL/KsJ-db/db) mouse has been proven to be a clinically relevantmodel of impaired wound healing. The animals exhibitseveral characteristics of human adult-onset diabetesincluding obesity, insulin-resistant hyperglycemia, andmarkedly delayed wound closure. These abnormalitiesarise as a result of a single autosomal recessive mutationon chromosome 4 [60]. In our laboratory, serum glucoselevels in the diabetic mice averaged greater than 900 mg/dI with insulin levels more than doubling levels found inthe nondiabetic littermates [34]. The diabetic animalswere not treated with insulin because of their markedresistance and because the goal was to examine healingin diabetes. Only the homozygous carriers of the reces-sive gene develop signs of diabetes. Heterozygotes areclinically unaffected, and wound healing proceeds at anormal rateo Because previous studies from this labora-.tory have documented that growth factors have no effecton enhancement of wound closure in the heterozygousnondiabetic littermate, this study was performed in ho-mozygous diabetic animals. A representative healingcurve of nondiabetic heterozygotes has been included forcomparison purposes.
Wounding
The animals were anesthetized using methoxyfluraneinhalation (Metofane; Pitman-Moore, Inc., Mundelein,IL). After clipping the hair on the back, the skin wasprepped with povidone-iodine solution and wiped with30% isopropyl alcohol. Using a sterile template, a full-thickness wound measuring 1.5 X 1.5 cm was created byexcising the skin on the mid-back, including the pannicu-lus carnosus. Tincture of benzoin (Compound BenzoinTincture U.S.P.; Cumberland-Swan, Inc., Smyrna, TN)was applied to the perimeter of the wound and allowed todry. The wound was then covered with a transparent,semipermeable polyurethane dressing (OpSite; Smithand Nephew Medical Limited, Hull, England) andsealed at the edges by the benzoin. The transparent Op-Site dressing allowed for easy visualization of thewound.
chest drains of healing mastectomy wounds containedhigh levels of growth factors and stimulated high levelsof DNA synthesis by fibroblast cultures. In contrast,fluids collected from chronic, nonhealing wounds hadlow levels of growth factors and failed to stimulate DNAsynthesis. Indeed, growth factors have been shown toimprove wound repair in animals with diabetes [30-36],infection [37], malnutrition [38], or in those impaired asa result of steroids [39-41], chemotherapeutic agents[42, 43], or radiation [44]. Clinical trials investigatingthe use of growth factors to improve wound closure inpatients with chronic, nonhealing wounds [45-51] orpartial-thickness donar sites [52,53] have al so been per-formed.
Although significant enhancement of wound closuremay be obtained with single growth factors, several stud-ies have demonstrated a more pronounced effect usingcombinations of growth factors, suggesting synergy [54-58]. It is logical that combinations of growth factorswould be more effective than individual growth factorssince, in the wound, multiple growth factors are presentand presumably active.
Previous studies from this laboratory have demon-strated that the fibroblast mitogens, PDGF-BB orbFGF, act synergistically with IGF-II to improve woundhealing in the genetically diabetic mouse [36, 59]. Themost profound improvement in healing was achievedwith the combination of PDGF-BB and IGF-II [36].Lynch el al. reported similar findings with the combina-tion of PDGF-BB and IGF-I in partial-thickness por-cine skin wounds [54, 55J and canine bone regenerationmodels [56, 57J.
Although functions may averiar, fibroblast mitogensact primarily to stimulate fibroblast replication, extra-cellular matrix deposition, and remodeling, while kera-tinocyte mitogens predominantly affect epithelial prolif-eration and migration. The purpose of this study was todetermine whether the combination of a keratinocytemitogen, EGF or TGF-a, and a fibroblast mitogen,PDGF-BB, would produce a synergistic effect similar tothat previously seen with the fibroblast mitogens in thegenetically diabetic mouse.
METHOOS ANO MA TERIALS Growth Factors
Human recombinant PDGF-BB was generously pro-vided by Zymogenetics, Inc. (Seattle, W A). Recombi-nant human TG F -a was purchased from R & D Systems,Inc. (Minneapolis, MN). Recombinant human EGF waspurchased from Upstate Biotechnology, Inc. (LakePlacid, NY). Growth factors were mixed in a vehicle ofsterilely filtered 5% polyethylene glycol (average mw8000; Aldrich Chemical Company, Inc., Milwaukee, WI).
Animals were randomly assigned to treatment groups,and investigators were blinded until completi9n of allobservations. The dose for each mouse was prepared
Animals
Female genetically diabetic (C57BL/KsJ-db/db)mice, ages 8-12 weeks and weighing 35-45 g, were ob-tained from Jackson Laboratories (Bar Harbor, ME).During experiments, animals were housed in individualcages in a central animal care facility, maintained on a12-h light-dark cycle, and given free access to standardrodent chow and water. The animal care facilities weremaintained by professionals in accordance with federalguidelines, and all procedures were approved by the Uni-
564 JOURNAL OF SURGICAL RESEARCH: VOL. 56, NO. 6, JUNE 1994
T ABLE 1
Histology Scoring System
Score Criteria
1-3
4-6
7-9
None to rninirnal cell accurnulation. Nogranulation tissue or epithelial travel.
Thin, irnrnature granulation that is dorninated byinflarnrnatory cells but has few fibroblasts,capillaries, or collagen deposition. Minirnalepithelial migration.
Moderately thick granulation tissue, can rangefrom being dominated by inflammatory cellsto more fibroblasts and collagen deposition.Extensive neovascularization. Epithelium canrange from minimal to moderate migration.
Thick, vascular granulation tissue dominated byfibroblasts and extensive collagen deposition.Epithelium partially to completely covering thewound.
10-12
Note. From Ref. 34 with permission ofth~ publisher.
sure were made with one-between, one-within, repeatedmeasures analysis of variance (RM-ANOV A), withDuncan's multiple range test being used for individualcomparisons. Statistical analysis of the histologic scoreswas performed using the Wilcoxon rank-sum test. Val-ues with P < 0.05 were considered significant. Data anal-ysis was performed with SAS software (version 6.04;SAS Institute, Inc., Cary, NC).
prior to wounding and sto red in individual syringes at4 °C. Approximately 0.6 mI of treatment solution wasprepared for each mouse, and 0.1 mI of the solution wasapplied once daily for 5 consecutive days starting atwounding by injecting it beneath the OpSite dressingand allowing it to spread ayer the wound. Wounds re-ceived topical application of vehicle (5% polyethyleneglycol) , PDGF-BB (10 p.g/dose) , TGF-a (1 p.g/dose),EGF (1 p.g/dose), or the combination of PDGF-BB (10p.g/dose) and TGF-a (1 p.g/dose) or EGF (1 p.g/dose).Treatment groups consisted of 8 to 10 animals per group,and experimente were repeated two to three times todocument consistency of resulte. Because of the variabil-ity of healing for each group of animals, each experimentincluded its own vehicle control.
Wound Analysis
Diabetic animals heal their wounds by granulationtissue formation and reepithelialization rather than bycontraction [34, 36]. The edge of migrating epithelium iseasily discernible from the moist granulation tissue. His-tology confirme the presence of the epithelial holder asthe edge of the healing wound.
The edges of epithelial migration were serially tracedanta glass slides on days 0,3,7, 11, 15, 18, and 21. Theafeas ofthe traced wounds were measured by planimetryusing an image analysis system (Image-1; UniversalImaging Corporation, Media, PA), and percentagewound closure was determined. Wound closure is ex-pressed as percentage closure of the original wound andis calculated as
RESULTS% wound closure
= [(Day o afea -Day N area)/Day O afea] X 100. Genetically diabetic animals tolerated the woundingprocedures well. An occasional wound (approximately3%) developed frank purulence and was eliminated fromthe data analysis beca use ofprobable infection. The restof the animals tended to gain weight and showed noovert signs of illness.
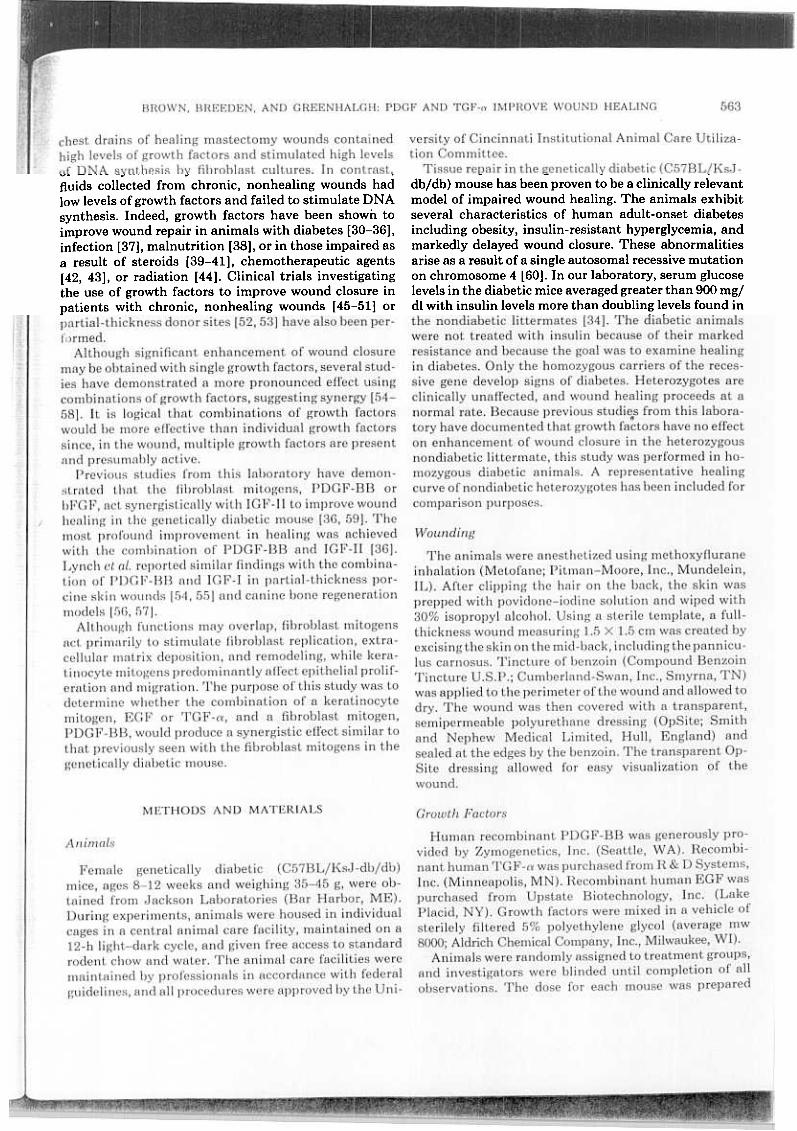
In the first experiment, the effects of combining ofPDGF-BB (10 Ilg) and EGF (lllg) were studied (Fig. 1,N = 8/group). As previously documented, healing in thevehicle-treated diabetic animals was significantly de-layed when compared with the typical healing ofnondia-betic mice. Since the purpose was to compare the effectsof growth factors in diabetic animals, nondiabetics werenot included in the experiments. A representative heal-ing curve of a group of untreated nondiabetic animals (N= 12) is included for comparison but was not included inthe statistical analysis. Treatment of wounds in diabeticanimals with PDGF-BB enhanced wound closure whencompared to vehicle treatment. The keratinocyte mito-gen EGF did not have any effect on healing. Further-more, EGF was unable to further enhance the beneficialeffects of PDGF-BB. Histologic analysis of Day 21wounds support these findings. The highest histologicscore was seen with PDGF-BB (10.25 ::!: 0.63), followed
After the final wound tracing on either Day 15 or Day21, the animals were given a lethal intraperitoneal injec-tion of pentobarbital, and the entire wound, including a5-mm margin of unwounded skin, was excised clown tothe fascia. The wound was divided in half through theleast healed porlion. One-half of the wound was placedin 10% formalin (Forma-Scent Fixative; Baxter Health-care Corporation, McGraw Park, IL) for histologic anal-ysis, and the other half was placed in liquid nitrogen andstored at -70°C for future molecular studies. Woundsections were stained with hematoxylin and eosin, andMasson's trichrome. Each wound section was evaluatedby two blinded investigators and assigned a histologicscore ranging from 1 (no healing) to 12 (complete heal-ing) based on degree of cellular infiltration, granulationtissue formation, vascularity, and reepithelialization(Table 1). The complete histologic scoring system hasbeen previously published [34].
Data AnalysisValues are expressed as means :j: standard error oí the
mean (SEM), Comparisons of the extent of wound clo-
BROWN, BREEOEN, ANO GREENHALGH: POGF ANO TGF-a IMPROVE WOUNO HEALING 565
100
90
w 80~~'" 70 -o-'u 80 -
cz 50 -~o~ 40 -
..30 -
20 -
10 -
O -
.10 -
-O-VEHICLE--PDGF.BB (10 ug)--TGF.ALPHA (1 ug)-PDGF (10 ug)/TGF.ALPHA (1 ug)
tNON.DIABETIC
¡..r
1/t//
~
.I
15o 3 6 9 12
100 ""J
90 -180
70
...80
50-'u 40cZ 30~~ 20..10 -O-VEHICLE
-PDGF-BB (10 ug)O -EGF (1 ug)
-lO ~PDGF-BB (10 ug){EGF (1 ug)-t NON-DIABETIC
-20
O 3 8 9 12 15 18 21DAY
FIG.1. Percentage wound closure (means:!: SEM) in geneticallydiabetic (C57BL/KsJ-db/db) mice (N = 8/group) treated with vehicle(5% polyethylene glycol) , PDGF-BB (10 /lg), EGF (1 /lg), or the combi-nation of PDGF-BB (10 /lg) and EGF (1 /lg). There are no significantdifferences between groups by RM-ANOV A. A representative nondia-betic healing curve is included for comparison purposes but was notincluded in the statistical analysis.
DAY
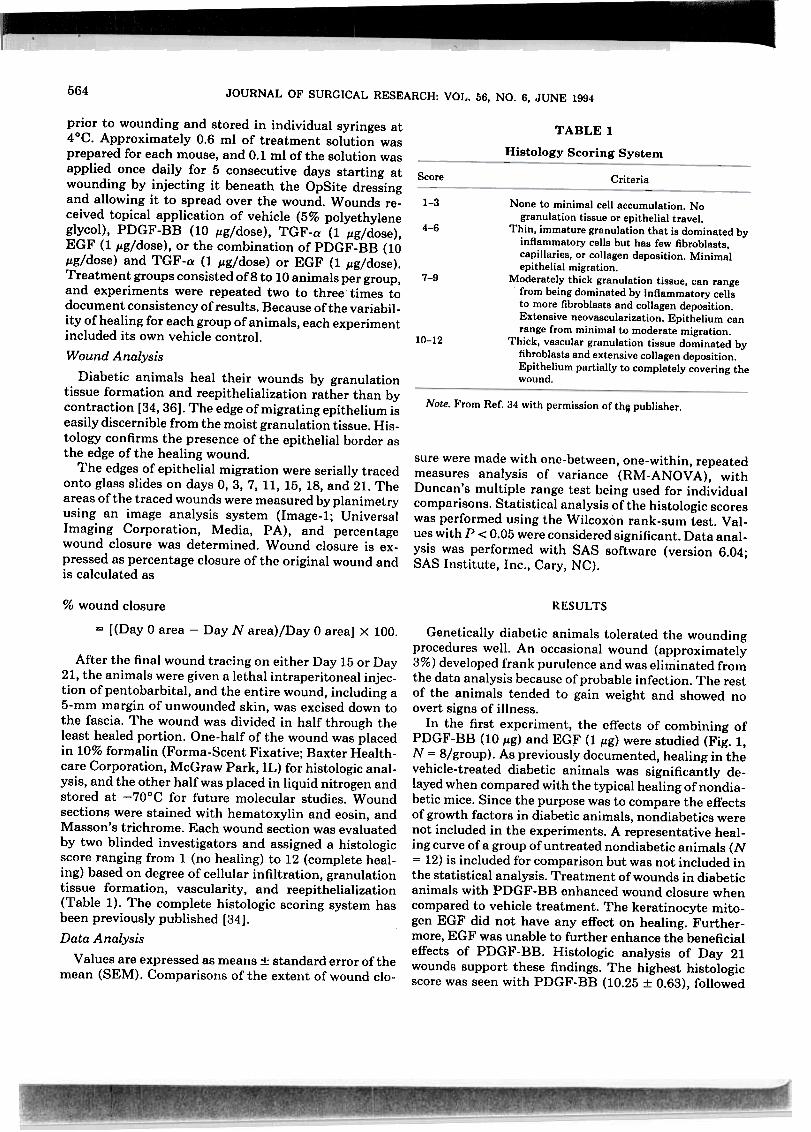
FIG. 3. Percentage wound closure (means :1: SEM) in geneticallydiabetic (C57BL/KsJ-db/db) micetreated with vehicle (5% polyethyl-ene glycol), PDGF-BB (10 ¡tg), TGF-a (1 ¡tg), or the combination ofPDGF-BB (10 ¡tg) and TGF-a (1 ¡tg). Cumulative data from four ex-periments (N = 36/group) reveals that the combination of PDGF-BBand TGF -a consistently enhances healing beyond that seen withPDGF-BB or TGF-a alone. (A) P < 0.05 fo~ PDGF-BB, TGF-a, orPDGF-BB/TGF-a vs vehicle; (B) all groups are significantly (P <0.05) different from each other; and (C) P < 0.05 for PDGF-BB, TGF-a, or PDGF-BB/TGF-a vs vehicle and PDGF-BB/TGF-a vs TGF-a.
by the combination ofPDGF-BB and EGF (9.38:t 0.81),vehicle (8.88 :t 1.10), and EGF (7.75 :t 0.85).
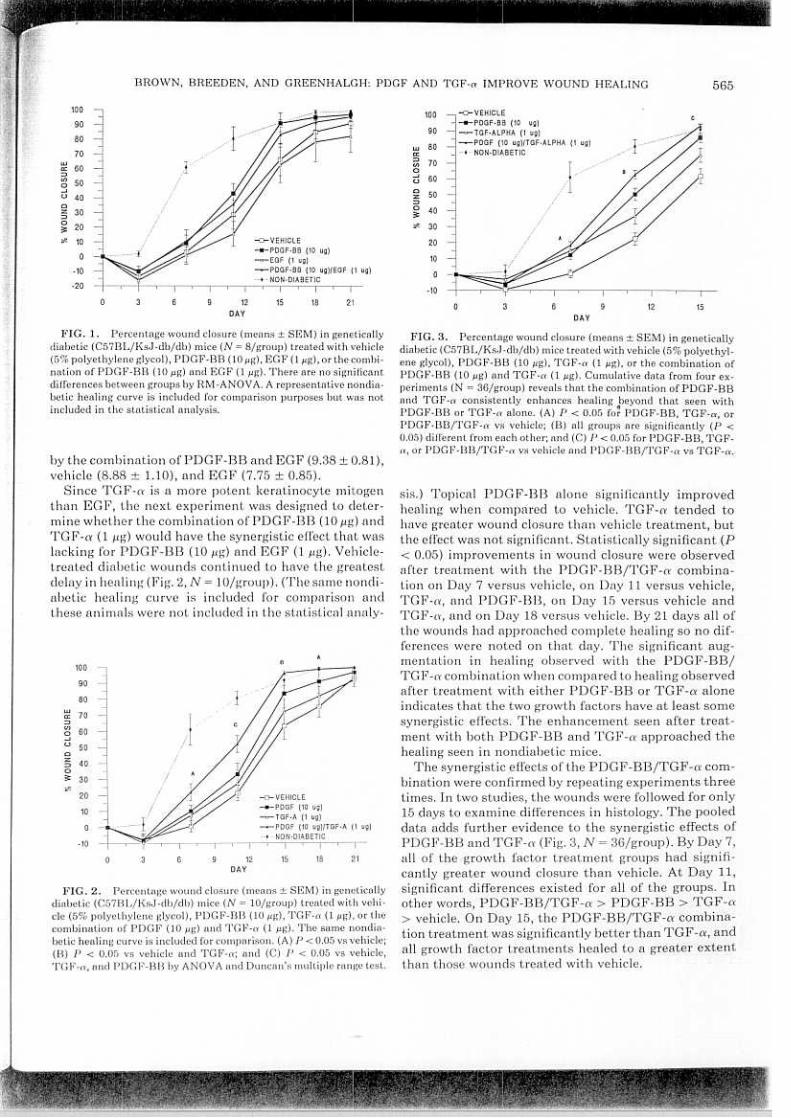
Since TGF-a is a more potent keratinocyte mitogenthan EGF, the next experiment was designed to deter-mine whether the combination ofPDGF-BB (10 Jlg) andTGF-a (1 Jlg) would have the synergistic effect that waslacking for PDGF-BB (10 Jlg) and EGF (1 Jlg). Vehicle-treated diabetic wounds continued to ha ve the greatestdelay in healing (Fig. 2, N = 10/group). (The same nondi-abetic healing curve is included for comparison andthese animals were not included in the statistical analy-
WIC::>C/Io-'U
QZ::>o~""
B A~~
/
sis.) Topical PDGF-BB alone significantly improvedhealing when compared to vehicle. TGF-a tended tohave greater wound closure than vehicle treatment, butthe eft'ect was not significant. Statistically significant (P< 0.05) improvements in wound closure were observedafter treatment with the PDGF-BBjTGF-a combina-tion on Day 7 versus vehicle, on Day 11 versus vehicle,TGF-a, and PDGF-BB, on Day 15 versus vehicle andTGF-a, and on Day 18 versus vehicle. By 21 days all ofthe wounds had approached complete healing so no dif-ferences were noted on that day. The significant aug-mentation in healing observed with the PDGF-BBjTG F -a combination when compared to healing observedafter treatment with either PDGF-BB or TGF-a aloneindicates that the two growth factors have at least somesynergistic effects. The enhancement seen after treat-ment with both PDGF-BB and TGF-a approached thehealing seen in nondiabetic mice.
The synergistic effects ofthe PDGF-BBjTGF-a com-bination were confirmed by repeating experiments threetimes. In two studies, the wounds were followed for only15 days to examine dift'erences in histology. The pooleddata adds further evidence to the synergistic effects ofPDGF-BB and TGF-a (Fig. 3, N = 36jgroup). By Day 7,all of the growth factor treatment groups had signifi-cantly greater wound closure than vehicle. At Day 11,significant differences existed for all of the groups. Inother words, PDGF-BBjTGF-a > PDGF-BB > TGF-a> vehicle. On Day 15, the PDGF-BBjTGF-a combina-tion treatment was significantlybetter than TG F -a, andall growth factor treatments healed to a greater extentthan those wounds treated with vehicle.
/1 -o-VEHICLE---PDGF (10 ug)--TGF-A (1 ug)-PDGF (10 ug)/TGF-A (1 ug)-t-NON-DIABETIC
, I ' I ' I
O 3 9 12 15 18 21DAY
FIG.2. Percentage wound closure (means:t SEM) in geneticallydiabetic (C57BL/KsJ-db/db) mice (N = 10/group) treated with vehi-cle (5% polyethylene glycol), PDGF-BB (10 ¡tg), TGF-a (1 ¡tg), or thecombination of PDGF (10 ¡tg) and TGF-a (1 ¡tg). The same nondia-betic healing curve is included for comparison. (A) P < 0_05 vs vehicle;(B) P < 0.05 vs vehicle and TGF-a; and (C) P < 0.05 vs vehicle,TGF-a, and PDGF-BB by ANOV A and Duncan's multiple range test.
/'
~
--,--,-6
100
90
60
70
60
50
40
30
20
10
O
-10
~
~';'1
566 JOURNAL OF SURGICAL RESEARCH: VOL. 56, NO. 6, JUNE 1994
T~-
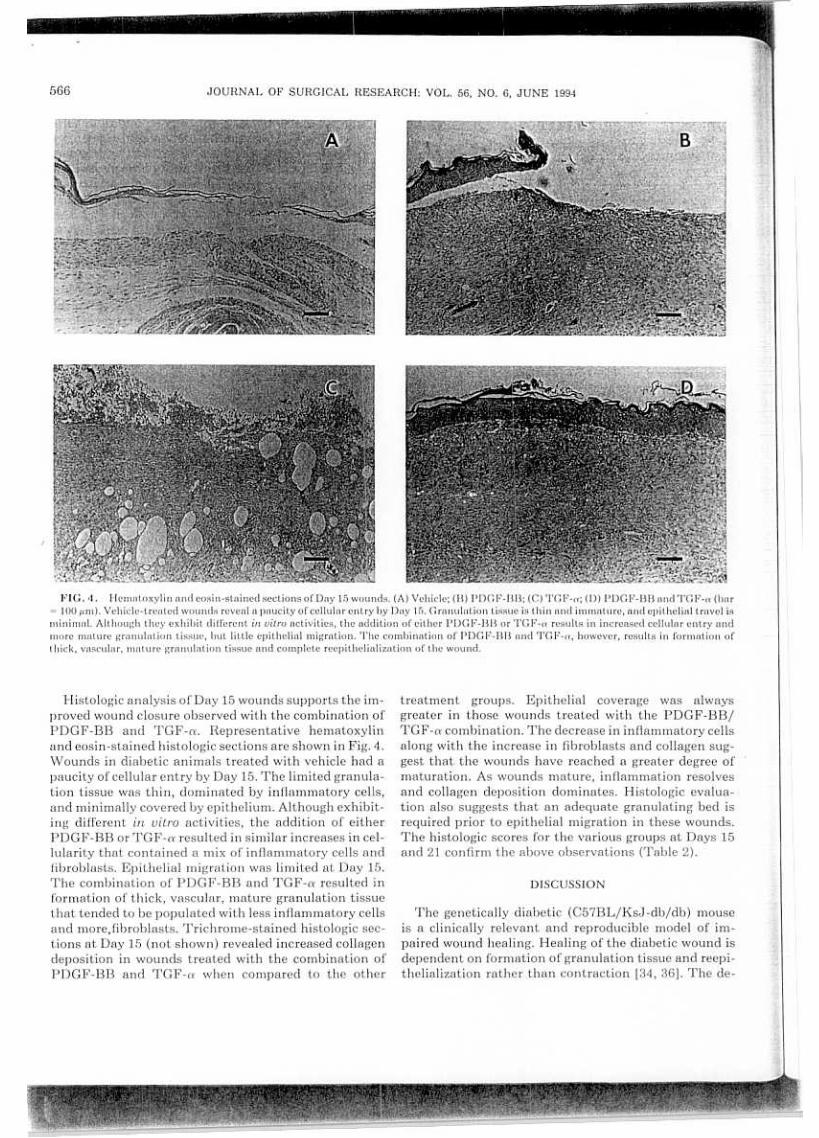
FIG.4. Hcmntoxylin nnd cosin-stnined sections ofDny 15 wounds. (A) Vchiclc; (B) PDGF-BB; (C) 'l'GF-CY; (O) PDGF-BB nnd TGF-cy (bnr= 100 ¡lm). Vehiclc-trcntcd wounds rcvenl n pnucity of cel\ulnr entry by Dny 15. Grnnulntion tissue is thin nnd immnturc, nnd epithclinl trnvel isminimnl. Although they exhibit dill'crcnt in vitro activities, thc addition of eithcr PDGF-BB or 'l'GF-cy results in increnscd ccl\ular entry andmore mnturc granulntion tissuc, but little epithelial migration. The combination of PDGF-BB and TGF-cy, however, resulta in formntion ofthick, vasculnr, maturc granulntion tissue and complete reepithelialization of the wound.
Histologic analysis ofDay 15 wounds supports the im-proved wound closure observed with the combination ofPDGF-BB and TGF-a. Representative hematoxylinand eosin-stained histologic sections are shown in Fig. 4.Wounds in diabetic animals treated with vehicle had apaucity of cellular entry by Day 15. The limited granula-tion tissue was thin, dominated by inflammatory cells,and minimally covered by epithelium. Although exhibit-ing different in vitro activities, the addition of eitherPDGF-BB or TGF-a resulted in similar increases in cel-lularity that contained a mix of inflammatory cells andfibroblasts. Epithelial migration was limited at Day 15.The combination of PDGF-BB and TGF-a resulted information of thick, vascular, mature granulation tissuethat tended to be populated with less inflammatory cellsand more,fibroblasts. Trichrome-stained histologic sec-tions at Day 15 (not shown) revealed increased collagendeposition in wounds treated with the combination ofPDGF-BB and TGF-a when compared to the other
treatment groups. Epithelial coverage was alwaysgreater in those wounds treated with the PDGF-BB/TGF -(1 combination. The decrease in inflammatory cellsalong with the increase in fibroblasts and collagen sug-gest that the wounds have reached a greater degree ofmaturation. As wounds mature, inflammation resolvesand collagen deposition dominates. Histologic evalua-tion algo suggests that an adequate granulating bed isrequired prior to epithelial migration in these wounds.The histologic scores for the various groups at Days 15and 21 confirm the above observations (Table 2).
DISCUSSION
The genetically diabetic (C57BL/KsJ-db/db) mouseis a clinically relevant and reproducible model of im-paired wound healing. Healing of the diabetic wound isdependent on formation of granulation tissue and reepi-thelialization rather than contraction [34, 36]. The de-

BROWN, BREEDEN, AND GREENHALGH: PDGF AND TGF-a IMPROVE WOUND HEALING 567
TABLE2
Histologic Scores (Values Expressed as Means :t SEM)
Day 15 Day 21Treatment
7.38 :t8.25 :t6.88 :t
8.73 :t 0.45 (13)9.85 :t 0.52 (13)9.46 :t 0.62 (12)
VehiclePDGF-BB (10 /lg)TGF-a (1 /lg)PDGF-BB (10 /lg)
and TGF-a (1 /lg) 9.54 :t 0.55 (12)* 10.15 :t 0.49 (13)
* P < 0.05 vs vehicle and TGF-a; P = 0.06 vs PDGF-BB by Wilcoxon
rank-sum test.
and resulted in more mature granulation tissue with in-creased collagen deposition.
Keratinocyte mitogens al so play an important role inthe wound healing process. The most thoroughly studiedkeratinocyte mitogens are EGF and TGF-a, which be-long to the same family and have similar mechanisms ofaction [29]. Both EGF and TGF-a are approximately6000 MW single-chain polypeptides which share about40% amino acid homology. The biologic activities ofboth EGF and TGF-a are mediated through the EGFreceptor. Both are potent keratinocyte mitogens whichstimulate both epithelial proliferation and migration.Additionally, both growth factors are mitogenic forfibroblasts and endothelial cells. Studies suggest thatTGF-a is more potent than EGF in vivo both as an an-giogenic factor [61] and as a promoter of epidermal re-generation [70].
EGF has been shown to enhance wound healing inseveral animal models [32,68,71-74] and has producedequivocal results in clinical trials in ~atients with par-tial-thickness donor sites [45] and chronic wounds [48].Lynch et al. [55] reported no significant improvement inhealing with the application of TGF-a to partial-thick-ness porcine skin wounds, but did find a significant syn-ergistic effect with the combination of PDG F and TGF-a. In our study, topical application of EGF to full-thick-ness diabetic mouse wounds resulted in no significantimprovement in wound healing above that of vehicle.Histologic analysis ofEG F -treated wounds revealed rela-tively immature granulation tissue and minimal to noepithelial travel. On the other hand, treatment withTG F -a resulted in improved wound closure above that ofvehicle, characterized histologically by thicker, moremature granulation tissue, but still with little epithelialtravel. Increased vascularity was al so observed inwounds treated with TGF-a. These results suggest thatTGF -a is a more potent fibroblast mitogen and angio-genic factor than EGF. Although not tested, higherclases of EGF may have produced an enhancement ofwound closure in the diabetic animals. PDGF, however,appears to the most active of the three. These findingslend further support to the hypothesis that formation ofa thick, vascular granulation tissue base is required forreepithelialization to proceed. One explanation for thestimulatory effects of TGF -a and not EGF could be thatthe Corroer had more pronounced effects on fibroblastsand angiogenesis than EGF. The stimulation ofkeratin-ocyte migration and proliferation, a dominant effect ofEGF, might be ineffective in the lack of an adequatewound bed.
Several studies have documented the synergistic ef-fects of growth factor combinations in vitro [75-78].Stiles et al. [75] demonstrated the requirement for both a"competence" factor (i.e., PDGF or FGF) and a "progres-sion" factor (i.e., IGF-I or IGF-II) for progression ofBALB/c 3T3 cells into the S phase ofthe cell cycle.lnvivo studies in this laboratory have documented the syn-
fect in tissue repair has been related to a delay in cellularentry which makes this an attractive model for study ofgrowth factor effects. Once inflammatory cells arrive inthe wound, healing appears to proceed relatively nor-mally. Exogenous application of growth factors appearsto draw inflammatory cells into the wound and acceler-ate granulation tissue formation. It appears that epithe-lial migration depends on the deposition of an adequategranulation bed. The dependence on granulation tissueis supported by the findings that EGF has no effect inaccelerating healing in these animals. TGF-a has beenshown to enhance fibroblast proliferation and have anangiogenic effect, in addition to its ability to enhanceepithelial migration and proliferation [61]. The moder-ate ability of TGF-a to enhance granulation tissue for-mation in the diabetic animals could result from theseeffects.
l:)DGF is an approximately 30,000 MW polypeptidegrowth factor which is a disulfide-linked dimer consist-ing of two chains-A and B. lt exists in three isomericforms-PDGF-AB, PDGF-AA, and PDGF-BB. ThePDGF-BB isomer was utilized in all of our experiments,but similar enhancement has been found following ap-plication of PDGF-AA [62]. PDGF is released from a-granules of platelets at the time of injury and by acti-vated macrophages later in the wound healing process.PDGF may al so be released from smooth muscle cellsand endothelial cells. lt is a potent mitogen for cells ofmesenchymal origin, including fibroblasts and smoothmuscle cells. Likewise, PDGF is a potent chemotacticagent for fibroblasts, smooth muscle cells, monocytes,and neutrophils. It serves an important role in modifica-tion of the extracellular matrix by stimulating collagen,collagenase, and glycosaminoglycan synthesis [63].PDGF may alBo playa role in angiogenesis, which maybe either indirect by stimulating macrophages to pro-duce angiogenic factors or a direct action on vascularendothelial cells [64].
In vivo, PDGF has been shown to significantly en-hance tissue repair in several wounding models [30, 34,40, 44, 65-69]. In our study, the application of PDGF-BB to full-thickness diabetic mouse wounds improvedwound closure beyond that of vehicle, EGF, or TGF-a
0.58 (13)0.41 (12)0.66 (12)
568 JOURNAL OF SURGICAL RESEARCH: VOL. 56, NO. 6, JUNE 1994
Iergistic effects of the combination of PDGF-BB orbFGF (competence factors) with IGF-II (progressionfactor) on enhancing wound repair in the genetically dia-betic mouse. Lynch et al. likewise demonstrated syner-gism with PDGF and IGF-I in partial-thickness porcineskin wounds [54,55] and canine bone regeneration mod-els [56, 56].
The purpose of the present study was to determinewhether the combination of a potent fibroblast mitogen,PDGF-BB, with a keratinocyte mitogen, EGF or TGF-a, would act synergistically to improve wound healing inthe genetically diabetic mouse. The results demon-strated that no synergistic effect was obtained with thecombination of PDGF-BB and EGF. In contrast,PDGF-BB and TGF-a appear to act synergistically topromote wound healing beyond that of the individualgrowth factors. As previously discussed, Lynch et al. [55]reported similar synergy with the combination of PDGFand TGF-a for treatment of partial-thickness porcineskin wounds.
Further studies should investigate the effects of thecombination of PDGF-BB (fibroblast competence fac-tor), IGF-II (fibroblast progression factor), and TGF-a(keratinocyte mitogen) to determine if a more pro-nounced synergistic eft'ect could be achieved. Likewise,the effects of a diff'erent fibroblast mitogen (i,e., bFGF)in combination with TGF-a should be studied,
Although these in vivo studies provide insight into pos-sible mechanisms of wound repair in the impaired host,many questions will remain unanswered and will remainuntil the complex interactions of growth factors at themolecular level are unraveled. It does appear, however,that growth factor combinations may eventually becomea valuable adjuvant for the clinical management ofchronic wounds, including diabetic ulcers, venous stasisulcers, and majar burns.
ACKNOWLEDGMENTS
We thank Laura James, M.S., for her assistance with statisticalanalysis. This work was supported by the Shriners of North America.
REFERENCES
4
Cruse, P. J., and Foord, R. A five-year prospective study of23,649 surgical wounds. Arch. Burgo 107: 206, 1973.Schrock, T. R., Deveney, C. W., and Dunphy, J. E. Factors con-tributing to leakage of colonic anastomoses. Ann. Burgo 177:513, 1973.Poole, G. U., Jr. Mechanical factors of abdominal closure: Thepreyention of fascial dehiscence. Surgery 97: 631, 1985.Irvin, G. L., Robinson, D. S., and Hubbard, S. Operative risks inpatients with colorectal cancer. Am. Burgo 51: 418, 1985.
Seppa, H., Grotendorst, G., Seppa, S., Schiffman, E., and Mar-tin, G. R. Platelet-derived growth factor is chemotactic for fibro-blasts. J. Cell. Biol. 92: 584, 1982.Deuel, T. F., Senior, R. M., Huang, J. S., and Griflin, G. L. Che-
motaxis of monocytes and neutrophils to platelet-derived growthfactor. J. Clin. Invest. 69: 1046, 1982.
7. Wahl, S. M., Hunt, D. A., Wakefield, L. M., McCartney-Francis,N., Wahl, L. M., Roberts, A. B., and Sporn, M. B. Transforminggrowth factor beta induces monocyte chemotaxis and growth fac-tor production. Proc. Notl. Acod. Sci. USA 84: 5788, 1987.
8. Adelmann.Grill, B. C., Wach, F., Cully, Z., Hein, R., and Krieg,T. Chemotactic migration of normal dermal fibroblasts towardsepidermal growth factor and its modulation by platelet-derivedgrowth factor and transforming growth factor-beta. Eur. J. CellBiol. 51: 322, 1990.
9. Carpenter, G., and Caben, S. Human epidermal growth factorand the proliferation of human fibroblasts. J. Cell. Physiol. 88:227, 1975.
10. Gospodarowicz, D., Moran, J. S., and Braun, D. L. Control ofproliferation ofbovine vascular endothelial cells. J. Cell. Physiol.91: 377,1977.
11. Bowen-Pope, D. F., and Ross, R. Platelet.derived growth factor.11. Specific binding to cultured cells. J. Cell. Biol. 257: 5161.
12. Roberts, A. B., Anzano, M. A., Wakefield, L. M., Roche, N. S.,Stern, D. F., and Sporn, M. B. Type fJ trlnsforming growth fac-tor: A bifunctional regulator of cellular growth. Proc. Notl. Acod.Sci. USA 82: 119, 1985.
13. Chua, C. C., Geiman, D. E., Keller, G. H., and Ladda, R. L. In-duction of collagenase secretion in human fibroblasts by growthpromoting factors. J. Hiol. Chem. 260: 5213, 1985.
14. Rohcrts, A. B., Sporn, M. B., Assoian, R. K., Smith, J. M., Rochc,N. S., Wakcficld, I~. M., Hcinc, U. l., Liotta, L. A., Falanl(a, V.,Kehrl, J. H., nnd Fnuci, A. S. Trunsforming growth factor type fJ:Rnpid induction of fihrosis and angúIgcncsis in vivo nnd stimultl-tion of collagcn formntion in vitru. ['ruco Natl. Acad. Sci. U."A83: 4167,1986.
15. Saval(c, K., Siehcrt, E., nlld Swalln, O. Thc ctfcct of platclct-dc-rivcd I(rowth factor on ccll divisiolllllld glycoslIminoglycnn syn-thcsis hy skin IInd sclIr tihrohlusts. J. [nve.~t. [Jermatul. 89: 93,1987.
16. Picrcc, G. F., Brown, O., 11 lid Mustoc, T. A. Quantitativc allalysisof inflammatory cell influx, procollagcn typc 1 synthesis, andcollagen cross-linking in incisional woullds: Influence of PDGF-BB and TGF-fJ1 thcrapy. J. Lab. Clin. Mcd. 117: 373,1991.
17. Pierce, G. F., Berg, J. V., Ralldolph, R., Tarpley, J., and Mustoe,T. A. Platelet-derived growth factor-BB and transforminggrowth factor beta-1 selectively modulate glycosaminoglycans,collagen, and myofibroblasts in excisional wounds. Am. J.Pothol. 138: 629, 1991.
18. Rappolee, D. A., Mark, D., Banda, M. J., and Werb, Z. Woundmacrophages express TGF.ff and other growth factors in vivo:Analysis by mRNA phenotyping. Science 241: 709,1988.
19. Antioniades, H., Galanopoulos, T., Neville-Golden, J., Kiritsy,C. P., and Lynch, S. E. Injury induces in vivo expression ofplate.let-derived growth factor (PDGF) and PDGF receptor mRNAsin ski n epithelial cells and PDGF mRNA in connective tissuefibroblasts. Proc. Natl. Acod. Sci. USA 88: 565, 1991.
20. Whitby, D. J., and Ferguson, W. J. Immunohistochemicallocal-ization of growth factors in fetal wound healing. Dev. Biol. 147:207, 1991.
21. Golden, M. A., Au, Y. P. T., Kirkman, T. R., Wilcox,. J. N.,Raines, E. R., Ross, R., and Clowes, A. W. Platelet-derivedgrowth factor activity and mRNA expression in healing vasculargrafts in baboons. J. Clin. Invest. 87: 406, 1991.
22. Dvonch, V. M., Murphey, R. J., Matsuoka, J., and Grotendorst,G. R. Changes in growth factor levels in human wound fluidoSurgery 112: 18, 1992.
23. Soma, Y., Dvonch, V., and Grotendorst, G. R. Platelet-derivedgrowth factor AA homodimer is the predominant isoform in hu.

BROWN, BREEDEN, AND GREENHALGH: PDGF AND TGF-a IMPROVE WOUND HEALING 569
man platelets and acute human wound fluido FASEB J. 6: 2996,1992.
24. Gartner, M. H., Benson, J. D., and Caldwell, M. D. Time courseof epidermal growth factor mRNA expression in healing woundsusing polymerase chain reaction. Surco Forum 42: 643, 1991.
25. Todd, R., Donoff, B. R., Chiang, T., Chou, M. Y., Elovic, A.,GaIlagher, G. T., and Wong, D. T. W. The eosinophil as a ceIlularsource of transforming growth factor alpha in healing c~taneouswounds. Am. J. Patho/. 138: 1307, 1991.
26. Wong, D. T. W., Donoff, R. B., Yang, J., Song, B., Matossian, K.,Nagura, N., Elovic, A., McBride, J., GaIlagher, G., Todd, R.,Chiang, T., Chou, L. S., Yung, C. M., Galli, S. J.., and WeIler,P. F. Sequential expression of transforming growth factors a andfJl by eosinophils during cutaneous wound healing in the ham-ster. Am. J. Patho/. 143: 130, 1993.
27. Cromack, D. T., Spom, M. B., Roberts, A. B., Merino, M. J.,Dart, L. L., and Norton, J. A. Transforming growth factor fJ lev-els in rat wound chambers. J. Surco Res. 42: 622, 1987.
28. Gartner, M. H., Benson, J. D., and CaldweIl, M. D. Insulin-likegrowth factors 1 and 11 expression in the healing wound. J. SurcoRes. 52: 389, 1992.
29. Schultz, G., Rotatori, D. S., and Clark, W. EGF and TGF-a inwound healing and repair. J. Ce/l. Biochem. 45: 346, 1991.
30. Grotendorst, G. R., Martin, G. R., Pencev, D., Sodek, J., andHarvey, A. K. Stimulation of granulation tissue formation byplatelet-derived growth factor in normal and diabetic rats. J.Glin. lnue.~t. 76: 2:32:1, 1985.
31. Broadley, K. N., Aquino, A. M., Hicks, B., Dietsheim, J. A.,McGee, G. S., Demetriou, A. A., Woodwllrd, S. C., and Dllvidson,J. M. The dinbetic rllt 11M nn impnired wound healinl{ model: Stim-ulntory e/rectA of trnns/(Jrminl{ Rrowth fllctor-betn nnd bnsic 11-broblllst Rrowth factor. Hiot/'chno/. Ther. 1: 55,1990.
32. Hennessey, P. .1., I3ll1Ck, C. T., IInd Andrllssy, R. .1. EGF in-creases short-term type 1 coIllIl{en nccumulntion durinR woundhealinR in dialJetic rllts. J. Pediatr. Surg. 25: 893,1990.
33. Tsuboi, R., IInd Ri/kin, D. B. Recombinllnt basic I1broblllstgrowth fllctor stimullltes wound healing in hellling-impllired db/db mice. J. Exp. Med. 172: 245, 1990.
34. Greenhalgh, D. G., Sprugel, K. H., Murrny, M. J., IInd Ross, R.PDGF nnd FGF stimulnte hellling in the genetically dillbcticmousc. Am. J. Patho/. 136: 1235, 1990.
35. Klingbeil, C. K., Cesllr, L. B., nnd Fiddes, J. C. Bnsic I1broblastgrowth factor accelerates tissue repair in rnodels of implliredwound healing. Prog. G/in. Bio/. Res. 365: 443, 1991.
36. Greenhalgh, D. G., Hummel, R. P., 111, Albertson, S., and Bree-den, M. P. Synergistic actions of platelet-derived growth factorand the insulin-like growth factors in vivo. Wound Rep. Reg. 1:69, 1993.
37. Hllyward, P., Hokanson, J., Heggars, J., Fiddes, J., Klingbeil, C.,Goeger, M., and Robson.. M. Fibroblast growth factor reversesthe bacterial retardation of wound contraction. Am. J. Surco163: 288, 1992.
38. Albertson, S., Hurnrnel, R. P., 111, Breeden, M. P., and Green-halgh, D. G. PDGF and FGF reverse the healing impairment inprotein-rnalnourished diabetic mice. Surgery 114: 368, 1993.
39. Laato, M., Heino, J., Kajari, V. M., Niinikoski, J., and Gerdin, B.Epiderrnal growth factor (EGF) prevents rnethylprednisolone-induced inhibition ofwound healing. J. Surco Res. 47: 354,1989.
40. Pierce, G. F., Mustoe, T. A., Lingelbach, J., Masakowski, V. R.,Gramates, P., and Deuel, T. F. Transforming growth factor fJreverses the glucocorticoid-induced wound-healing deficit inrats: Possible regulation in rnacrophages by platelet-derivedgrowth factor. Proc. Nat/. Acad. Sci. USA 86: 2229, 1989.
41. Beck, L. S., DeGuzman, L., Lee, W. P., Xu, Y., McFatridge, L. A.,and Amento, E. P. TGF-fJl accelerates wound healing: Reversal
of steroid-impaired healing in rats and rabbits. Growth Factors 5:295, 1991.
42. Lawrence, W. T., Sporn, M. B., Gorschboth, C., Norton, J. A.,and Grotendorst, G. R. The reversal of an Adriamycin inducedhealing impairment with chemoattractants and growth factors.Ann. Surg. 203: 142, 1986.
43. DeCunzo, L. P., MacKenzie, J. W., Marafino, B. J., Jr., and Dev-ereux, D. F. The effect ofinterleukin-2 administration on woundhealing in adriamycin-treated rats. J. Surg. Res. 49: 419, 1991.
44. Mustoe, T. A., Purdy, J., Gramates, P., Deuel, T. F., Thomason,A., and Pierce, G. F. Reversal of impaired wound healing in irra-diated rats by platelet-derived growth factor-BB. Am. J. Surg.158: 345, 1989.
45. Brown, G. L., Nanney, L. B., Griffen, J., Cramer, A. B., Yancey,J. M., Curtsinger, L. J., 111, Holtzin, L., Schultz, G. S., Jurkie-wicz, and Lynch, J. B. Enhancement ofwound healing by topicaltreatment with epidermal growth factor. N. Engl. J. Med. 321:76, 1989.
46. Knighton, D. R., Ciresi, K., Fiegel, V. D., Schumerth, S., andButler, E. L. Stimulation of repair of chronic, nonhealing, cutane-ous ulcers using platelet-derived wound healing formula. Surg.Gynecol. Obstet. 170: 56, 1990. '
47. Atri, S. C., Misra, J., Bisht, D., and Misra, K. Use ofhomologousplatelet factors in achieving total healing of recalcitrant skinulcers. Surgery 108: 508, 1990.
48. Brown, G. L., Curtsinger, L., Jurkiewicz, M. J., Nahai, F., andSchultz, G. Stimulation of healing of chronic wounds by epider-milI growth factor. Pla.o;t. Ilecon.o;tr. Surg. 88: 189, 1991.
49. Robson, M. C., Phillips, L. G., Thomllson, A., Robson, L. E., andPicrce, G. F. Platclct-dcrivcd growth factor BB for thc treatmcntof chronic pressurc ulcers. Lancet 339: 23, 1992.
50. Robson, M. C., Phillips, L. G., Lawrcncc, W. T., Bishop, J. B.,Youngcrman, J. S., Hayward, 1'. G., Broemcling, L. D., and Heg-gcrs, J. P. The safety and effcct oftopically applied recombinantbagic fibroblast growth factor on thc hcaling of chronic pressurcgOles. AIIII. Surg. 216: 410.
51. Stecd, D. L., C;oslcn, J. B., Holloway, G. A., Malone, J. M., Bunt,T. J., and W ebster, M. W. Randomized prospective double-blindtrilll in hcl1ling chronic dillbetic foot ulcers: CT-102 activlltedplatelet supernatant, topical versus placebo. Diabetes Cure 15:1599, 1992.
52. Caben, l. K., Kormos, A., Garrett, A., Crossland, M. C., Geerlof,J. S., Battikha, J., and Diegelmann, R. F. Topical application ofcpidermal growth factor does not enhance re-epithelialization ofpartial thickness wounds in human volunteers. Proc. WoundHealing Soco 1: 37, 1991.
53. Greenhalgh, D. G., and Rieman, M. The effects of basic fibro-blast growth factor on the healing of partial thickness donarsites: A prospective, randomized, double blinded trial. WoundRep. Regell., in press.
54. Lynch, S. E., Nixo"n, J. C., Colvin, R. B., and Antoniades, H. N.Role of platelet-derived growth factor in wound healing: Syner-gistic eft'ects with other growth factors. Proc. Natl. Acad. Sci.USA 84: 7696, 1987.
55. Lynch, S. E., Colvin, R. B., and Antoniades, H. N. Growth fac-tors in wound healing: Single and synergistic effects on partialthickness porcine skin wounds. J. Clin. Invest. 84: 640, 1989.
56. Lynch, S. E., Buser, D., Hernandez, R. A., Weber, H. P., Stich,H., Fox, C. H., and Williams, R. C. Effects of the platelet-derivedgrowth factor/insulin-like growth factor-1 combination on boneregeneration around titanium dental implants: Results of a pilotstudy in beagle dogs. J. Periodontol. 62: 710, 1991.
57. Lynch, S. E., de Castilla, G. R.,Williams, R. C., Kiritsy, C. P.,Howell, T. H., Reddy, M. S., and Antoniades, H. N. The effectsof short-term application of a combination of platelet-derived
570 JOURNAL OF SURGICAL RESEARCH: VOL. 56, NO. 6, JUNE 1994
and insulin-like growth factors on periodontal wound healing. J.Periodontol. 62: 458, 1991.
58. Hennessey, P. J., Black, C. T., and Andrassey, R. J. Epidermalgrowth factor and insulin act synergistically during diabetic heal-ing. Arch. Surco 125: 926, 1990.
59. Albertson, S., Hummel, R. P., 111, Breeden, M. P., and Green-halgh, D. G. Insulin-like growth factor, incombination with fibro-blast growth factor, improve wound healing in diabetic mice.Surco Forum XLIII: 680, 1992.
60. Coleman, D. L. Obese and diabetes: Two mutant genes causingdiabetes-obesity syndromes in mice. Diabetologia 14: 141, 1978.
61. Schreiber, A., Winkler, M. E., and Derynck, R. Transforminggrowth factor a is a more potent angiogenic mediator than epi-dermal growth factor. Science 232: 1250, 1986.
62. Sprugel, K. H., Greenhalgh, D. G., Murray, M. J., and Ross, R.Platelet-derived growth factor and impaired wound healing.Prog. Clin. Biol. Res. 365: 327, 1991.
63. Ross, R., Raines, E., and Bowen-Pope, D. The biology of plate-let-derived growth factor. Cell46: 155, 1986.
64. Hom, D. B., and Maisel, R. H. Angiogenic growth factors: Theireffects and potential in soft tissue wound healing. Ann. Otol.Rhino. Laryngol. 101: 349,1992.
65. Pierce, G. F., Mustoe, T. A., Senior, R. M., Reed, J., Griffin,G. L., Thomason, A., and Deuel, T. F. In vivo incisional woundhealing augmented by platelet-derived growth factor and recom-binant c-sis gene homodimeric proteins. J. Exp. Med. 167: 974,1988.
66. Pierce, G. F., Mustoe, T. A., Lingelbach, J., Masakowski, V. R.,Griffin, G. L., Senior, R. M., and Deuel, T. F. Platelet-derivedgrowth factor and transforming growth factor-1J enhance ti!l!luerepair activities by unique mechanisms. J. Cell Biol. 109: 429,1989.
67. Hill, E., Turner-Beatty, M., Grotewiel, M., Fosha-Thomas, S.,Cox, C., Turman, C., Drees, D., Baird, L., Maratea, D., Tucker,R., and Counts, D. The effect of PDGF on the healinK of fullthickness wounds in hairless guinea pig!l. Campo Biochem. Phys-iol. 100A: 365, 1991.
68. Mustoe, T. A., Pierce, G. F., Morishima, C., and Deuel, T. F.Growth factor-induced acceleration of tissue repair through di-
rect and inductive activities in a rabbit dermal ulcer modelo J.Clin. Invest. 87: 694, 1991.
69. Lepisto, J., Laato, M., Niinikoski, J., Lundberg, C., Gerdin, B.,and Heldin, C. Effects of homodimeric isoforms of platelet-de-rived growth factor (PDGF-AA and PDGF-BB) on wound heal-ing in rato J. Surg. Res. 53: 596, 1992.
70. Schultz, G. S., White, M., Mitchell, R., Brown, G., Lynch, J.,Twardzik, D. R., and Todaro, G. J. Epithelial wound healingenhanced by transforming growth factor-a and vaccinia growthfactor. Science 235: 350, 1987.
71. Niall, M., Ryan, G., and O'Brien, B. M. The effect of epidermalgrowth factor on wound healing in mice. J. Surg. Res. 33: 164,1982.
72. Laato, M. The effect of epidermal growth factor on granulationtissue formation in the rato ACTA Chir. Scand. Suppl. 546: 6,1988.
73. Kitazawa, T., Kinoshita, S., Fujita, K., Araki, K., Watanabe, H.,Ohashi, Y., and Manabe, R. The mechanism of accelerated cor-neal epithelial healing by human epidermal growth factor. In-vest. Ophthalmol. Vis. Sci. 31: 1773, 1990.
74. Noguchi, S., Ohba, Y., and Oka, T. Effect of epidermal growthfactor on wound healing of tongue tn mice. Am. J. Physiol.23(260): E620, 1991.
75. Stiles, C. D., Capone, G. T., Scher, C. D., Antoniades, H. N., vanWyk, J. J., and Pledger, W. J. Dual roleofcell growth by somato-medins and platelet-derived growth factor. Proc. Natl. Acad. Sci.USA 76: 1279, 1979.
76. DeLapp, N. W., and Dicckmlln, D. K. I~(l'cct of basic fibroblastgrowth factor (bFOF) and in!!ulin-likc ¡:rowl!1 factor!! tYlle 1(IGF-I) and typc 11 (IGI;,-II) on adult humlln kcratinocyte ¡:rowthand fibroncctin Rccretion. J. [nve..¡t. [Jermatlll. 94: 777,1990.
77. Chamberlain, C. G., McAvoy,.J. W., Ilml Richllrd!!on, N. A. 'l'heell'ccts of insulin IInd bll!!ic fibroblllst I(rowl!, fllculr on libre dif-fercntiation in rnt lens cpithclial cxplllnt!!. Grlllllth FllctlJr..¡ 4:183, 1991.
78. Kranc, J. F., Murphy, D. P., Cartcr, D. M., ami Krucl(er, .J. G.Synergistic cll'ectR of cpidcrmal growth factor (I~GI") and in!!u-lin-like growth factor I/somatomcdin C (IGF-I) on kcratinocyteproliferation muy be rncdiated by IGF-I transmodulation of thcEGF receptor. J. Inucst. Dcrmatol. 96: 419, 1991.