Embed Size (px)
Citation preview

Improving Care Transitions and Decreasing Readmissions
through Public and Private Partnerships
11th Annual Small & Rural Hospital Conference November 9, 2011

What is “Transition of Care”
The movement of patients from one health care practitioner or setting to another as the individual’s condition and care needs change
Occurs at multiple levels Within Settings
ICU Ward
Between Settings Hospital Home or Hospital Long Term Care Facility
Across health states Curative care Palliative care/Hospice
(c) Eric A. Coleman, MD, MPH

Ineffective Transitions lead to Poor Outcomes
Wrong treatment Delay in diagnosis Severe adverse events Patient complaints Increased length of stay Increased healthcare costs

Increase in Care Transitions
53% increase in patients discharged from hospital to home health
25% increase in patients discharged from hospital to nursing homes or rehab facilities
50% of older adults discharged from the hospital
to long term care facility experienced 4+ transitions to another institution over 12-months

Understanding Rehospitalizations
Who is at risk of Rehospitalizations? According to IHI…Individuals with:
Chronic Illnesses (heart disease, COPD) Frail Elderly In Nursing Homes or Receiving Home Health End-of-Life Psychiatric Illnesses Substance Abuse Complex Social Challenges (poverty)

20% Medicare Beneficiaries readmitted within 30 Days
33% readmitted within 90 Days
Hospitalizations account for 33% of total Medicare $
Readmissions result in $17.4 Billion annually
76% of Medicare readmissions potentially avoidable
Estimated $12 Billion Preventable Expenditures
Readmissions: By the Numbers

The Challenge
“If re-hospitalizations are frequent, costly, and able to be reduced,
why haven’t they been?”
Hospital-level barriers Community-level barriers
State-level barriers

How does our community navigate this transition?
Nursing Home
Assisted Living
Rehabilitation Continuing Care
Retirement Community
Home
County Council/
Department on Aging
Area Agency
on Aging
Cooperative Extension
Mental Health
Provider
Community Resource Connection
Home Health Care
Senior Center
Adult Day Services
Faith Community
County Social
Services
?

New Models of Care
There are a number of proven & promising models to improve outcomes during transitions:
Common Elements:
Interdisciplinary Communication/Collaboration Transitional Care Staff Patient Activation Enhanced Follow-up (by phone / home visit)

Transitional Care Models Care Transitions Intervention (www.caretransitions.org)
Transitional Care Model (www.transitionalcare.info )
Project RED (www.bu.edu/fammed/projectred)
Project BOOST (www.hospitalmedicine.org/BOOST)
Resources National Transitions of Care Coalition’s Compendium
(www.ntocc.org) “Health Care Leader Action Guide to Reduce Avoidable Readmissions” (www.commonwealthfund.org)

4 Steps for Hospital Leaders
1. Examine your hospital's current rate of readmissions
2. Assess and prioritize your improvement opportunities
3. Develop an action plan
4. Monitor your hospital’s progress
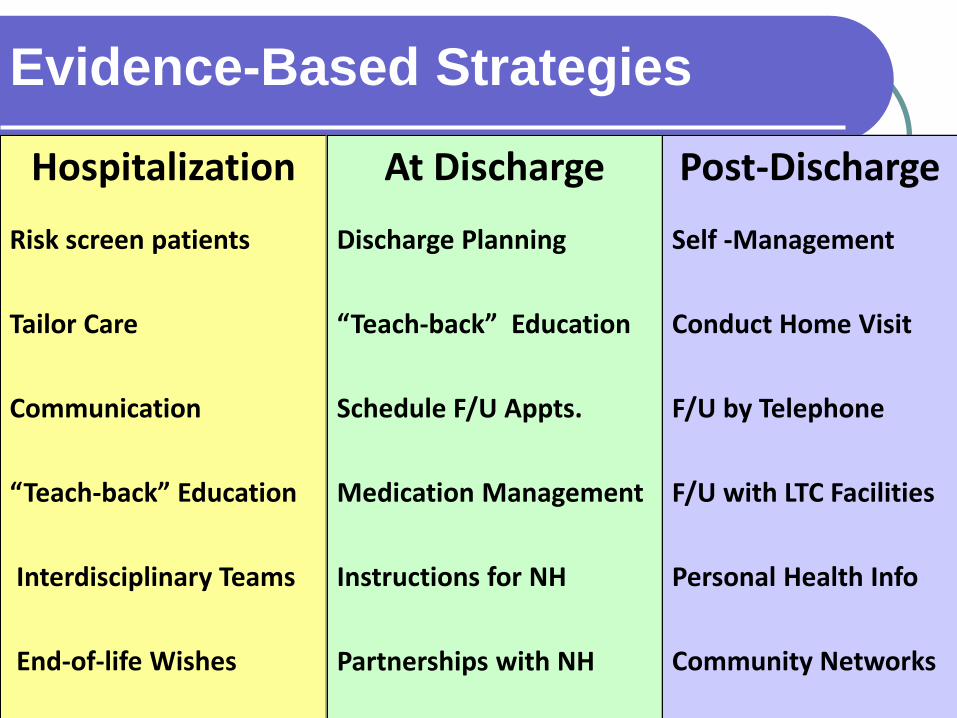
Evidence-Based Strategies Hospitalization
Risk screen patients Tailor Care Communication “Teach-back” Education Interdisciplinary Teams End-of-life Wishes
At Discharge
Discharge Planning
“Teach-back” Education
Schedule F/U Appts.
Medication Management
Instructions for NH
Partnerships with NH
Post-Discharge
Self -Management Conduct Home Visit
F/U by Telephone
F/U with LTC Facilities
Personal Health Info
Community Networks

Aging & Disability Resource Centers: ADRCs The federal ADRC initiative began with 3 core
functions: Awareness, Assistance & Access
The set of expectations has grown over time to include improving care transitions
AoA and CMS are viewing ADRCs as the platform to catalyze broader systems change
Health reform adds new fuel to the fire! $500M - Section 3026: Community-Based Care Transitions Program
ADRCs - Local Core Collaborators Consumers Aging Services Agencies Disability Services Agencies In-Home services Senior Centers Community Agencies Dept. of Social Services Area Agencies on Aging Community Health Centers Hospitals

Anson
Beaufort
Bertie
Brunswick
Carteret
Columbus
Craven
Duplin
Gaston
Gates
Greene
Halifax
Harnett
Hertford
Hoke
Hyde Johnston
Jones
Lee
Lenoir
Lincoln
Martin
Moore
Nash
Northampton
Onslow
Pender
Pitt
Robeson
Sampson
Scot- land
Tyrrell
Union
Wayne
Wilson
Alam
ance
Alleghany Ashe
Caldwell
Caswell
Catawba
Chatham Davidson
Davie
Forsyth Franklin Guilford
Iredell
Person
Randolph
Rockingham Stokes Surry Warren
Watauga Wilkes
Yadkin
Wake
Avery
Cherokee Clay
Graham Henderson
Buncombe McDowell
Macon
Polk
Rutherford Swain
Madison
Mont- gomery
Stanly
Cabarrus
Rowan Burke
Orange
Durham
Bladen
Dare
North Carolina: Community Resource Connections (CRCs)
CRCs in Operation
Program Areas where CRC Development is in process with launches in mid-2012
Programs Areas Launching or Expanding Fall 2011
DHHS Office of Long Term Services & Supports

South Carolina ADRCs

Person-Centered Hospital Discharge Planning Model Enhance the ability of community organizations to
plan for person-centered hospital discharges
Develop models that ensure that individuals have maximum options to return home
Create processes for communities to share tools, resources, outcomes & lessons learned

Lessons Learned
Identify a Change Agent
Bring Stakeholders Together & Make the Case
Encourage Collaboration: Public & Private
Celebrate Early & All Successes
Demonstrate Impact (Now vs. Future)
Choose Intervention – Outcomes – Fit
Capture the Data
Sustainability is Critical!

A Community-Based Approach
“Communities across the US are
beginning to consider transitions of care as a community–based challenge that requires shared ownership and close collaboration across settings.” (Institute for Healthcare Improvement)

Community Care of North Carolina (CCNC) Transitional Care Highlights
Jennifer Cockerham, RN, BSN, CDE Director of Chronic Care and Quality Improvement [email protected] Communitycarenc.com

North Carolina Medicaid 1,516,803 Medicaid Recipients
Medicaid Managed Care *Community Care of NC (CCNC) 1,127,958 Enrollees 1542 Practices 4500+ Providers *Carolina Access I (CA I = 57,092) Straight Medicaid (331,753)

Community Care Networks
Cherokee
Graham
Swain
Clay Macon
Jackson
Haywood
Madison
Buncombe
Henderson
McDowell
Rutherford
Polk
Burke
Cleveland
Watauga
Caldwell Alexander
Catawba
Lincoln
Gaston
Ashe
Wilkes
Alleghany
Surry
Yadkin
Iredell
Mecklenburg
Union
Stanly Cabarrus
Rowan
Davie
Stokes
Forsyth
Davidson
Anson
Rockingham
Guilford
Randolph
Montgomery
Richmond
Caswell
Chatham
Orange
Person
Lee
Moore
Hoke
Scotland
Robeson
Cumberland
Harnett
Wake
Franklin
Warren
Johnston
Sampson
Bladen
Columbus
Brunswick
Pender
Duplin
Wayne
Wilson
Nash
Halifax
Northhampton
Edgecombe
Pitt
Greene
Lenoir
Jones
Onslow
Craven
Pamlico
Beaufort Hyde
Martin
Bertie
Hertford
Gates
Washington Tyrrell
Dare
Alam
ance
Durham
Granville
Hanover
Chow
an
a r
Legend AccessCare Network Sites Community Care Plan of Eastern Carolina AccessCare Network Counties Community Health Partners Community Care of Western North Carolina Northern Piedmont Community Care Community Care of the Lower Cape Fear Northwest Community Care Carolina Collaborative Community Care Partnership for Health Management Community Care of Wake and Johnston Counties Community Care of the Sandhills Community Care Partners of Greater Mecklenburg Community Care of Southern Piedmont Carolina Community Health Partnership

CCNC Infrastructure
14 Networks - private, non-profit organizations Community-based, physician-led, emphasis on
medical homes Local partners = hospital, health department,
DSS, specialists, etc Partner with the state to better manage Medicaid
population = improve quality and contain cost Enhanced pmpm to Medical Home

FOCUS of CCNC
improved quality, utilization and cost
effectiveness of chronic illness care
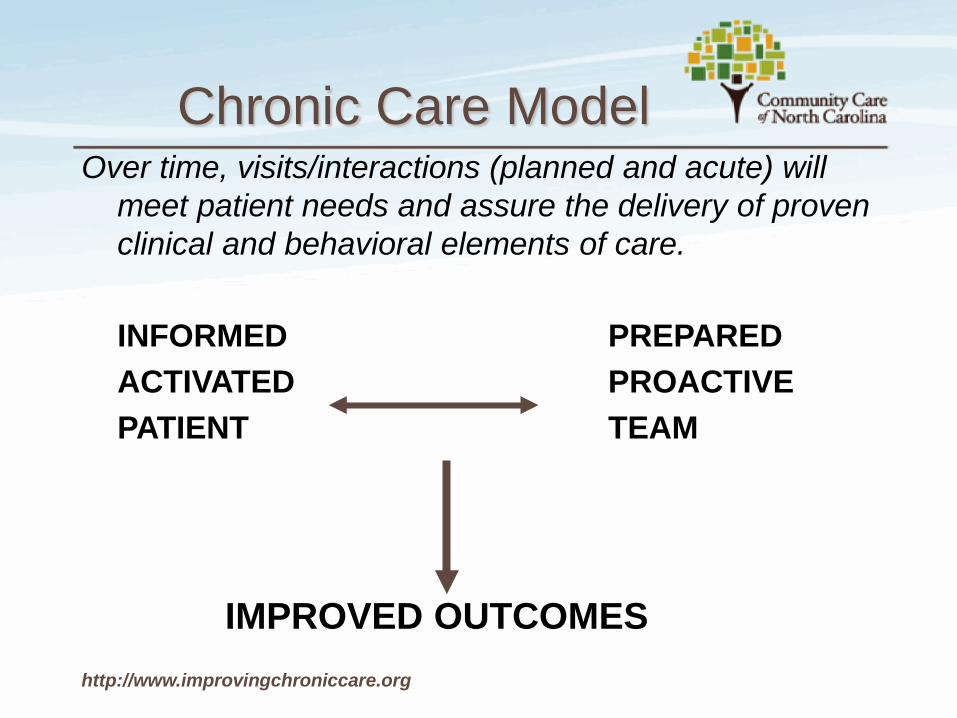
Chronic Care Model Over time, visits/interactions (planned and acute) will
meet patient needs and assure the delivery of proven clinical and behavioral elements of care.
INFORMED PREPARED ACTIVATED PROACTIVE PATIENT TEAM IMPROVED OUTCOMES http://www.improvingchroniccare.org

Care Management Support to the Medical Home
Improved Care
Process Improvement
Evidence-Based Guidelines
Provider Impact
Improved Utilization
Outcome Improvement
Education, Referrals, Follow-Up
Patient Impact
Care Manager

Chronic Disease Prevalence of NC’s ABD Medicaid Population
3 or More Major Co-morbidities
43% 3 or More Major Co-morbidities

Major Co-morbid Conditions
Within the 200,000 ABD Medicaid Recipients 45% Hypertension 24% Diabetes 14% Asthma 14% COPD 13% Ischemic Vascular Disease 12% Neurological Disorders 6% Chronic Kidney Disease 3% Heart Failure 41% Mental Health conditions p

$0 $1K $2K $3K $4K $5K $6K $7K $8K $9K $10K $11K $12K $13K $14K $15K $16K $17K $18K $19K $20K
Expected Preventable Inpatient Costs for this CRG
Actual-to-Expected Difference
Treo PPL
All individuals within the same Clinical Risk Group (CRG)

ED and Inpatient Utilization of ABD Population (over 6 month period)
At Least 1 ED Visit At Least 1 Hospitalization
41%17%
t

Susan
10 y.o. with asthma ED visit on the weekend Multiple ED visits over
the last 6 months for asthma
More prednisone fills than pulmicort fills in previous year's drug claims
No Asthma Action Plan

Susan
Informatics Center ED & Hospital Visit Report Patient contact - left message for mom to call PCP
and make an appointment PCP RN notified CM of appt date/time CM conference with MD prior to appt CM met with Susan, parents, and MD MD completed AAP while CM provided asthma
education and resources

TARGET : Tool for Adjusting Risk - A Geriatric Evaluation for Transitions 7 P Risk Scale: 1. 1. Prior Hospitalization 2. 2. Problem Meds (Coumadin, insulin, Digoxin)
3. Punk (depression) 3. 4. Principal diagnosis 4. 5. Polypharmacy 5. 6. Poor health literacy (50% higher risk) 6. 7. Patient support
Project BOOST (Better Outcomes for Older Adults thru Safe Transitions)
www.hospitalmedicine.org/BOOST

Hospital Readmits
17.6 % are readmitted within 30 days of discharge 6% in the first week
50% had not followed up with PCP or
any physician before being readmitted 25-30% occur at a different hospital
Institute for Healthcare Improvement t

Medication Management Issues
o High Risk Meds (Coumadin, insulin, digoxin)
o Polypharmacy o 20% of pts D/C’d from hospital at least 1
medication discrepancy (UCHSC) o 1/3 of meds prescribed at D/C are not
taken (Beers et al) o New meds at D/C not noted in outpt.
record 50% of time

Transitional Care
“ A set of actions designed to ensure the coordination and continuity of health care as patients transfer between different locations or different levels of care within the same location”
Source: Position Statement from the American Geriatrics Society, 2003
CCNC Transitional Care 02/2011
I

Charlie 62 y.o. with developmental
disability and multiple chronic conditions
Very little family support Dependent on CAP-DA and
other in-home services prior to admit
2 month hospital stay wound care and unstable conditions
Multiple team meetings during inpatient stay to coordinate discharge plans
Linked to multiple services - CAP-DA, Home Health, Palliative Care, DME, Specialists

Charlie
Discharged home on Labor Day Home Visit by CCNC Care Manager Home Health for B.I.D. dressing changes had not
yet begun No dressing change supplies Pain regimen had been denied by Medicaid had
not been communicated, resulting in 3 days without pain med
CAP-DA was unable to resume services until 3 days after discharge, resulting in no assistance with personal care

CCNC Transitional Care Process
1)Notification/identification of hospitalized patients 2)Screening & Assessment Process 3)Hospital Visit 4)Facilitate Optimal Hospital Stay and Discharge
Plan 5)Home Visit with Medication Reconciliation/med
management 6)Medical Home Linkage 7)Disease Management, Red Flags, Community
Linkages, improved self-management

FACE -TO-FACE INTERACTIONS
Hospital Home Medical Home
The Primary Role of the CCNC CM in the Transitional Care process is to:
facilitate interdisciplinary collaboration across transitions
encourage the patient and caregiver to play a central and active role in the formation and execution of the plan of care
promote self-management skills and direct communication between the patient/caregiver, primary care provider, and other service providers
achieve medication reconciliation through consultation with network pharmacist, the hospital, the PCP, the Specialists, and the patient

Self-management Tasks of Chronic Care Patients
Medical management of condition (MEDICAL) Creating and maintaining new
meaningful life roles (SOCIAL) Coping with anger, fear, frustration of
having chronic condition (EMOTIONAL)
Based on work by Clark, Corbin, Strauss and Glaser

Highlights of our Progress
Real-Time data, Hospital & ED reports in IC, ADT CM embedded in hospitals CM & Pharmacists teams Process for Face-to-Face encounters with patient Support to Medical Home/PCP follow-up appointments Work with hospitals to obtain more complete D/C Instructions Strong linkages with Mental Health Providers Provider Portal & Care Alerts Addition of Psychiatrists & Behavioral Health Pharmacist Palliative Care Physician Champions Value of Home Visits Enhanced features in CMIS to track and evaluate Transitional Care The value of Community Partnerships

Embedded Staff
Care Managers 118 practices 48 hospitals Pharmacists 14 practices 18 hospitals

What we are learning…
Complexity of the population – medically & socially Majority have either a dominant or moderate chronic
condition, a malignancy, or a catastrophic health condition
Motivational Interviewing techniques are key for positive patient engagement
Population management appears to be having a positive impact on access to care, ED, and inpatient utilization
2011 cumulative Medicaid costs for enrolled ABD population (dual and non-dual combined) were $196 lower per member per month for the fiscal year as compared to fiscal year 2008.

Challenges…
Defining the “impactable” patient & interventions
Incorporating palliative care, mental health & other new info without creating more silos
Challenges obtaining Real-Time Hospital Data
Unable to locate the patient
Narrow time frame for the most beneficial intervention
Promoting effective self-management
Growing population and level of complexity
Building capacity in the Medical Homes
Competing agendas

Susan
“It was a positive experience. Mom said the ED told her to call and schedule a follow-up visit, but she had forgot until she received my voice message. The family is looking forward to Susan being in better control of her asthma than she has been.”
- CCNC Care Manager

THANK YOU

U N
C H E A L T H C A R E S Y S T E M
U N
C H E A L T H C A R E S Y S T E M
Care Transitions and
Readmissions at Chatham Hospital
Small and Rural Hospital Conference November 9, 2011

50
U N
C H E A L T H C A R E S Y S T E M
Chatham Hospital Facts
• Critical Access Hospital • Owned by the UNC Health Care System • Located in Siler City, NC • Contract with UNC Health Care System for Emergency
Room and Hospitalist physician coverage

51
U N
C H E A L T H C A R E S Y S T E M
Caswell Person Granville
Vance Warren
Franklin
Northampton Halifax
Durham
Wake Chatham
Nash Edgecombe
Wilson
Johnston
Wayne Lee
Moore Harnett
Sampson
Duplin
Pender
Brunswick
Columbus
Bladen Robeson
Cumberland Hoke
Scotland
Guilford
Randolph
Montgomery
Richmond
Stokes
Forsyth
Davidson
Rowan
Stanly
Anson Union
Mecklenburg
Cabarrus
Iredell Davie
Yadkin
Surry
Alleghany Ashe
Wilkes
Alexander
Catawba
Lincoln
Gaston Cleveland
Burke
Caldwell
Watauga
Avery
McDowell
Rutherford
Polk
Mitchell
Yancey
Buncombe
Henderson
Transylvania
Haywood
Madison
Swain
Jackson
Macon
Graham
Clay Cherokee
Onslow
Jones
Lenoir
Greene
Pitt
Martin
Bertie
Hertford
Gates Camden
Pasquotank
Dare Tyrrell
Washington
Beaufort Hyde
Craven
Pamlico
Rockingham Currituck
Perquimans Chowan
Carteret
Orange
New Hanover Chatham Hospital
Chatham County

52
U N
C H E A L T H C A R E S Y S T E M
Why is this a priority?
Partnership for Patients • Keep patients from getting injured or sicker • Help patients heal without complication
We need to fix things in our hospital that are not working Payors are paying more attention and are incentivizing We are all in this together because we share patients It is the right thing to do
53
U N
C H E A L T H C A R E S Y S T E M
There are many causes of readmissions
• Exacerbations of conditions
• Complications of care
• Medication issues
• Missed (or missing) follow-up appointments
• Confusion regards discharge instructions
• Patient non-compliance
54
U N
C H E A L T H C A R E S Y S T E M
Small Hospital Challenges
Small patient volumes Hospital has limited resources Generally less advantaged patients
• Lower income • Less education
Fewer community options

55
U N
C H E A L T H C A R E S Y S T E M
What is Chatham Hospital’s 30-day readmission rate?
Patients Too few to analyze 68 100 Readmits 15 18

56
U N
C H E A L T H C A R E S Y S T E M
Chatham Hospital Status Focus on appropriate transition placement and prevention of
unnecessary readmissions
Majority of patients are elderly
Frequent ED visits from nursing home and assisted living residents
Hospitalists rotate from UNC Hospitals • Accustomed to pressure to discharge quickly • Chatham Hospital length of stay dropping • Readmissions are increasing ??
Many inpatients discharged to local nursing homes or assisted living facilities
Implementing CPOE with new discharge instruction software

57
U N
C H E A L T H C A R E S Y S T E M
Efforts to Reduce Readmissions and ED Returns
Determine baseline readmission and ED returns
Obtain buy-in from local nursing homes and assisted living facilities
Evaluate “Hand Off’ between Chatham Hospital staff and Nursing/Assisted Living staff
• Evaluate nursing home/assisted living documentation provided to hospital
• Interview nursing home/assisted living staff
Develop an educational program based on evaluation findings

58
U N
C H E A L T H C A R E S Y S T E M
UNC Hospitals Partnership
Pilot study with Vendor for patient-centered hospital to home program
• Discharge care plan aligned with hospital medical record
• Personalized transition liaison services
• Medication management and guidance
• Compliance monitoring
• 24-hour nurse assist line

59
U N
C H E A L T H C A R E S Y S T E M
Questions or Comments? What is happening at your facility?
Heather Altman
Carol Woods Retirement Community [email protected] / 919-918-2609
Jennifer Cockerham
Community Care of North Carolina [email protected] / 919-696-8880
Carol Straight
Chatham Hospital [email protected] / 919-799-4001
THANK YOU!





























