Embed Size (px)
Citation preview
Authorization Review Process Physician Services
UPDATE
December 2013
1
Introduction to eQHealth
2

• eQHealth is the Agency for Health Care
Administration’s contracted quality
improvement organization (QIO), responsible
for the Comprehensive Medicaid Utilization
Management Program for the state of Florida
• Local office/operations in Tampa Bay area
5802 Benjamin Center Drive, Suite 105
Tampa, FL 33634
Partnership: Agency for Health Care
Administration and eQHealth
3
Scope of Services
5

Service Requirements
6
Recipients must be:
• Enrolled in a Medicaid benefit program that covers
the service requested:
• Fee for service
• MediPass
• Medically Needy
• Dually eligible (Medicare/Medicaid &
Commercial/Medicaid)
• Waiver Recipients
• Eligible at the time services are rendered
Not Subject to Prior Authorization
by eQHealth
7
Recipients who are:
• Members of a Medicaid HMO
• Members of a Medicaid Provider Service
Network (PSN)
• Members of Children’s Medical Services (CMS)
Medicaid reimburses services that do not duplicate
another provider’s service and are medically
necessary for the treatment of a specific documented
medical disorder, disease or impairment.
The fact that a provider has prescribed, recommended, or approved medical or allied care, goods, or services does not, in itself, make such care, goods or services medically necessary or a medical necessity or a covered service.
Medical Necessity
8
Multi-Specialty Services
9
Effective 1/1/14: Authorization of physician services have been expanded to include services currently requiring the Agency to review claim documentation to establish reimbursement or medical necessity.
Examples:
Procedures defined as “unlisted”
On the fee schedule as “by report” (BR)
A full list of the additional codes to be reviewed is included in this presentation.

Authorizations
10
Prior Authorization numbers are valid for 120 days; if
an extension is needed, contact eQHealth Customer
Service.

Codes No Longer Covered
11
Effective 1/1/14
99070 – Supplies and materials (except spectacles), provided by the
physician over and above those usually included with the office visit or
other services rendered.
Q4050 - Cast supplies, for unlisted types and materials of casts
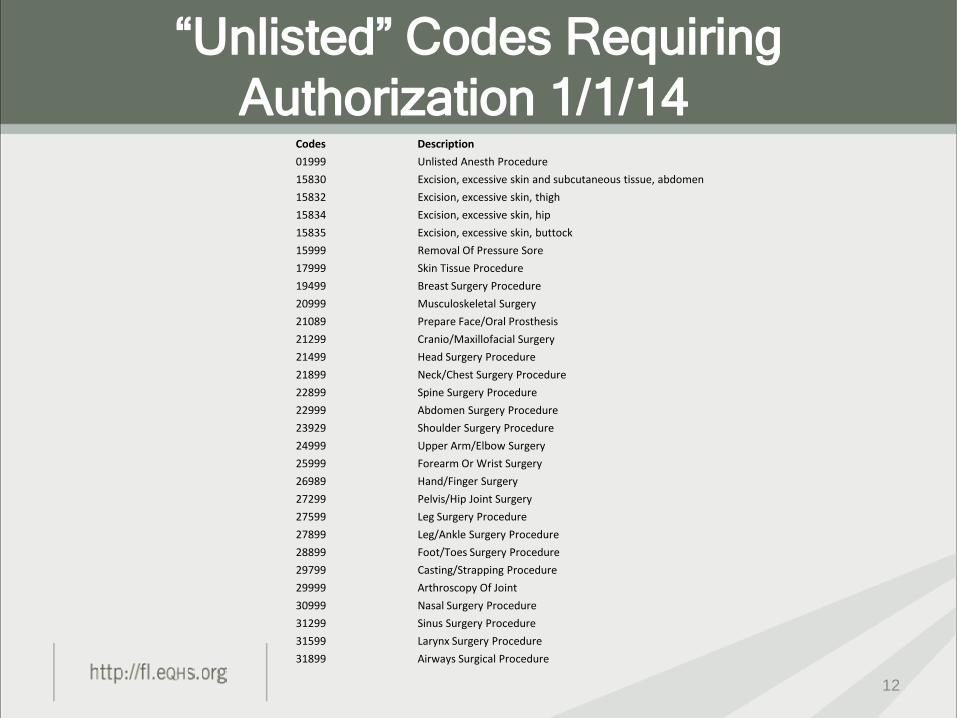
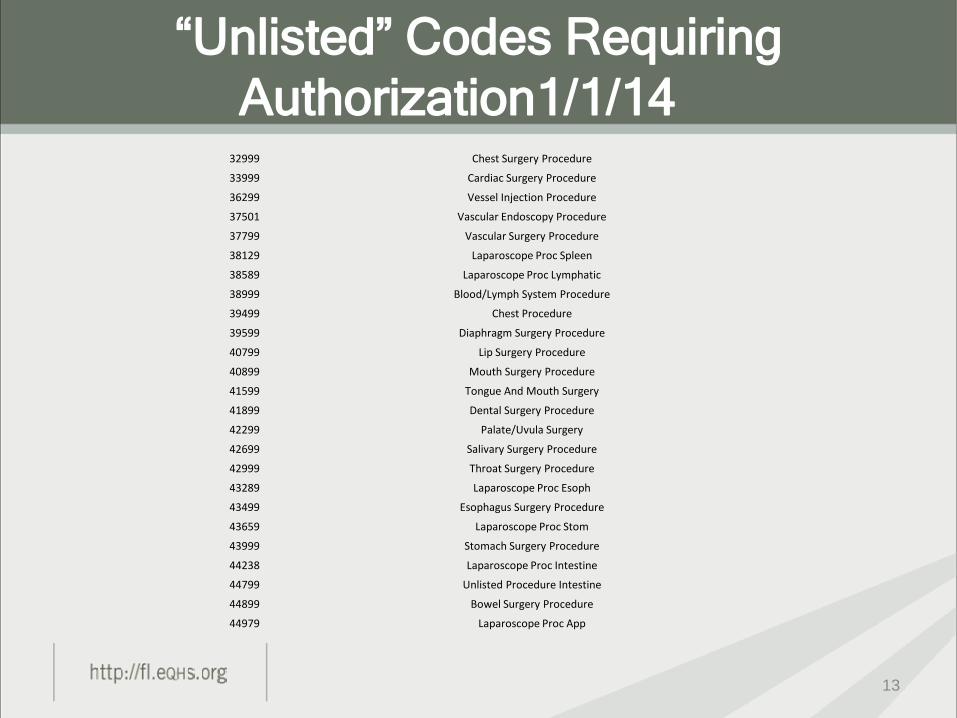
“Unlisted” Codes Requiring
Authorization 1/1/14
12
Codes Description
01999 Unlisted Anesth Procedure
15830 Excision, excessive skin and subcutaneous tissue, abdomen
15832 Excision, excessive skin, thigh
15834 Excision, excessive skin, hip
15835 Excision, excessive skin, buttock
15999 Removal Of Pressure Sore
17999 Skin Tissue Procedure
19499 Breast Surgery Procedure
20999 Musculoskeletal Surgery
21089 Prepare Face/Oral Prosthesis
21299 Cranio/Maxillofacial Surgery
21499 Head Surgery Procedure
21899 Neck/Chest Surgery Procedure
22899 Spine Surgery Procedure
22999 Abdomen Surgery Procedure
23929 Shoulder Surgery Procedure
24999 Upper Arm/Elbow Surgery
25999 Forearm Or Wrist Surgery
26989 Hand/Finger Surgery
27299 Pelvis/Hip Joint Surgery
27599 Leg Surgery Procedure
27899 Leg/Ankle Surgery Procedure
28899 Foot/Toes Surgery Procedure
29799 Casting/Strapping Procedure
29999 Arthroscopy Of Joint
30999 Nasal Surgery Procedure
31299 Sinus Surgery Procedure
31599 Larynx Surgery Procedure
31899 Airways Surgical Procedure
“Unlisted” Codes Requiring
Authorization1/1/14
13
32999 Chest Surgery Procedure
33999 Cardiac Surgery Procedure
36299 Vessel Injection Procedure
37501 Vascular Endoscopy Procedure
37799 Vascular Surgery Procedure
38129 Laparoscope Proc Spleen
38589 Laparoscope Proc Lymphatic
38999 Blood/Lymph System Procedure
39499 Chest Procedure
39599 Diaphragm Surgery Procedure
40799 Lip Surgery Procedure
40899 Mouth Surgery Procedure
41599 Tongue And Mouth Surgery
41899 Dental Surgery Procedure
42299 Palate/Uvula Surgery
42699 Salivary Surgery Procedure
42999 Throat Surgery Procedure
43289 Laparoscope Proc Esoph
43499 Esophagus Surgery Procedure
43659 Laparoscope Proc Stom
43999 Stomach Surgery Procedure
44238 Laparoscope Proc Intestine
44799 Unlisted Procedure Intestine
44899 Bowel Surgery Procedure
44979 Laparoscope Proc App

“Unlisted” Codes Requiring
Authorization1/1/14
14
45499 Laparoscope Proc Rectum
45999 Rectum Surgery Procedure
46999 Anus Surgery Procedure
47379 Laparoscope Procedure Liver
47399 Liver Surgery Procedure
47579 Laparoscope Proc Biliary
47999 Bile Tract Surgery Procedure
48999 Pancreas Surgery Procedure
49329 Laparo Proc Abdm/Per/Oment
49659 Laparo Proc Hernia Repair
49999 Abdomen Surgery Procedure
50549 Laparoscope Proc Renal
50949 Laparoscope Proc Ureter
51999 Laparoscope Proc Bla
53899 Urology Surgery Procedure
54699 Laparoscope Proc Testis
55559 Laparo Proc Spermatic Cord
55899 Genital Surgery Procedure
58578 Laparo Proc Uterus
58579 Hysteroscope Procedure
58679 Laparo Proc Oviduct-Ovary
58999 Genital Surgery Procedure
59897 Fetal Invas Px W/Us
59898 Laparo Proc Ob Care/Deliver
59899 Maternity Care Procedure
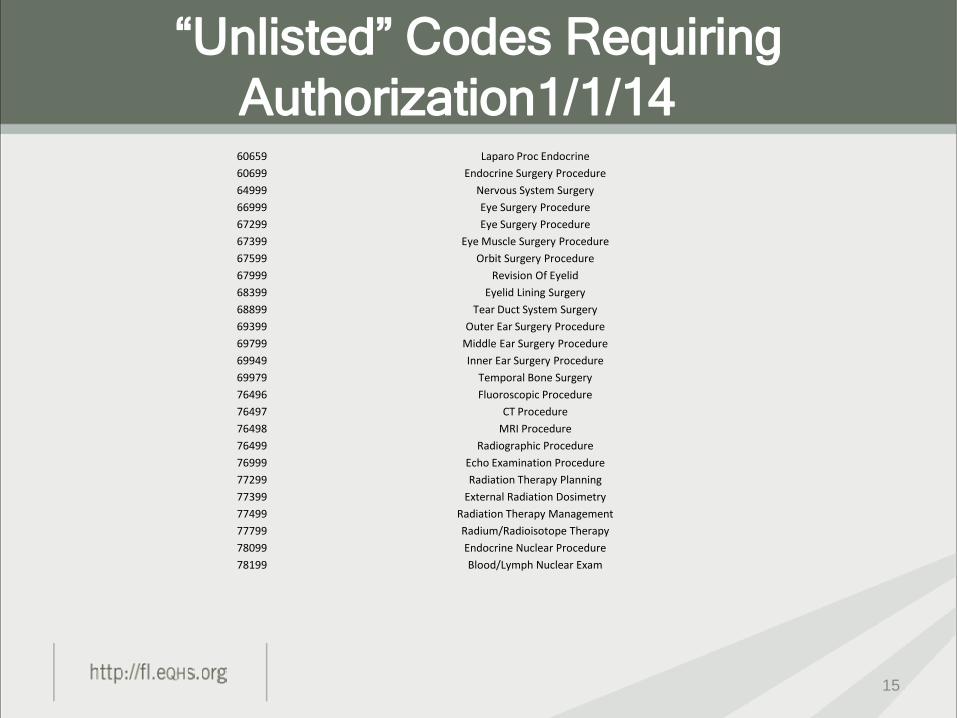
“Unlisted” Codes Requiring
Authorization1/1/14
15
60659 Laparo Proc Endocrine
60699 Endocrine Surgery Procedure
64999 Nervous System Surgery
66999 Eye Surgery Procedure
67299 Eye Surgery Procedure
67399 Eye Muscle Surgery Procedure
67599 Orbit Surgery Procedure
67999 Revision Of Eyelid
68399 Eyelid Lining Surgery
68899 Tear Duct System Surgery
69399 Outer Ear Surgery Procedure
69799 Middle Ear Surgery Procedure
69949 Inner Ear Surgery Procedure
69979 Temporal Bone Surgery
76496 Fluoroscopic Procedure
76497 CT Procedure
76498 MRI Procedure
76499 Radiographic Procedure
76999 Echo Examination Procedure
77299 Radiation Therapy Planning
77399 External Radiation Dosimetry
77499 Radiation Therapy Management
77799 Radium/Radioisotope Therapy
78099 Endocrine Nuclear Procedure
78199 Blood/Lymph Nuclear Exam

“Unlisted” Codes Requiring
Authorization1/1/14
16
78299 GI Nuclear Procedure
78399 Musculoskeletal Nuclear Exam
78499 Cardiovascular Nuclear Exam
78599 Respiratory Nuclear Exam
78699 Nervous System Nuclear Exam
78799 Genitourinary Nuclear Exam
78999 Nuclear Diagnostic Exam
79999 Nuclear Medicine Therapy
87999 Microbiology Procedure
90399 Immune Globulin
90749 Vaccine Toxoid
90899 Psychiatric Service/Therapy
90999 Dialysis Procedure
91299 Gastroenterology Procedure
92499 Eye Service Or Procedure
92700 ENT Procedure/Service
93799 Cardiovascular Procedure
93998 Noninvas Vasc Dx Study Proc
94799 Pulmonary Service/Procedure
95199 Allergy Immunology Services
95999 Neurological Procedure
96379 Ther/Prop/Diag Inj/Inf Proc
96549 Chemotherapy Unspecified
96999 Dermatological Procedure
97039 Physical Therapy Treatment
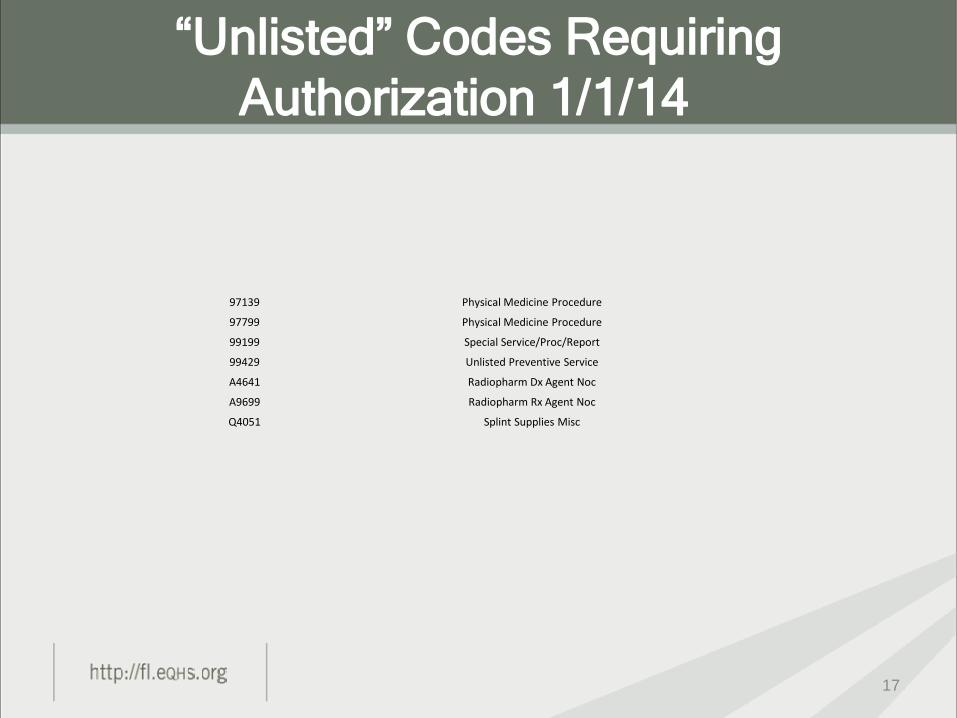
“Unlisted” Codes Requiring
Authorization 1/1/14
17
97139 Physical Medicine Procedure
97799 Physical Medicine Procedure
99199 Special Service/Proc/Report
99429 Unlisted Preventive Service
A4641 Radiopharm Dx Agent Noc
A9699 Radiopharm Rx Agent Noc
Q4051 Splint Supplies Misc

BR Codes Requiring Authorization
1/1/14
18
By Report Codes Description
15876 Suction Assisted Lipectomy
19316 Suspension Of Breast
19328 Removal Of Breast Implant
19330 Removal Of Implant Material
19340 Immediate Breast Prosthesis
19357 Breast Reconstruction
19370 Surgery Of Breast Capsule
19371 Removal Of Breast Capsule
19380 Revise Breast Reconstruction
20962 Other Bone Graft Microvasc
21084 Prepare Face/Oral Prosthesis
21088 Prepare Face/Oral Prosthesis
21121 Reconstruction Of Chin
22818 Kyphectomy 1-2 Segments
22819 Kyphectomy 3 Or More
25246 Injection For Wrist X-Ray
31620 Endobronchial US Add-On
33935 Transplantation Heart/Lung
37182 Insert Hepatic Shunt (Tips)
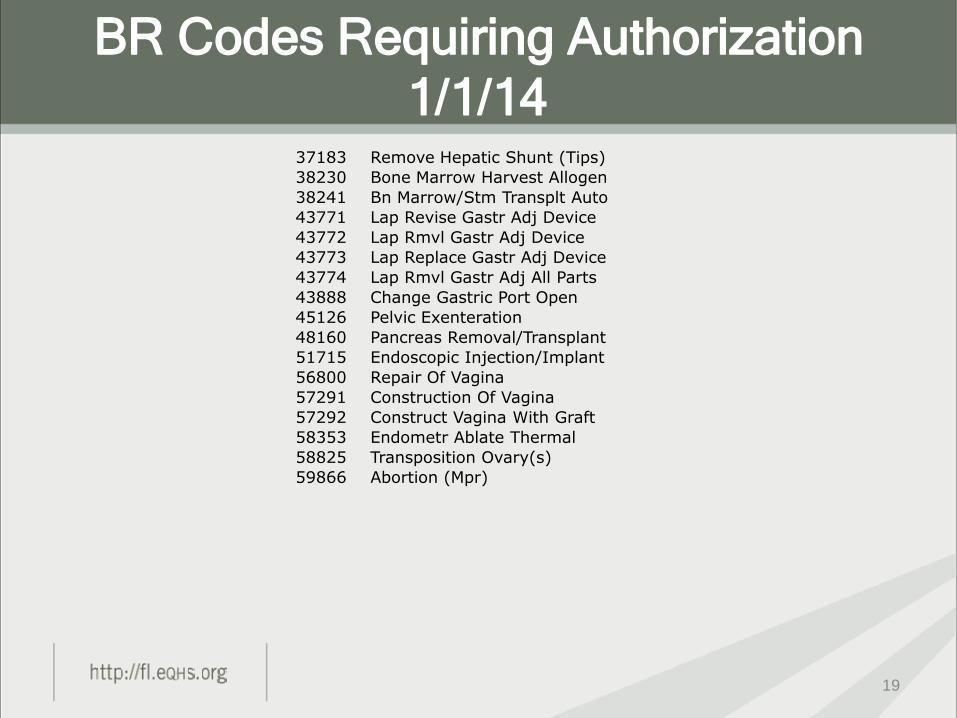
BR Codes Requiring Authorization
1/1/14
19
37183 Remove Hepatic Shunt (Tips)
38230 Bone Marrow Harvest Allogen
38241 Bn Marrow/Stm Transplt Auto
43771 Lap Revise Gastr Adj Device
43772 Lap Rmvl Gastr Adj Device
43773 Lap Replace Gastr Adj Device
43774 Lap Rmvl Gastr Adj All Parts
43888 Change Gastric Port Open
45126 Pelvic Exenteration
48160 Pancreas Removal/Transplant
51715 Endoscopic Injection/Implant
56800 Repair Of Vagina
57291 Construction Of Vagina
57292 Construct Vagina With Graft
58353 Endometr Ablate Thermal
58825 Transposition Ovary(s)
59866 Abortion (Mpr)
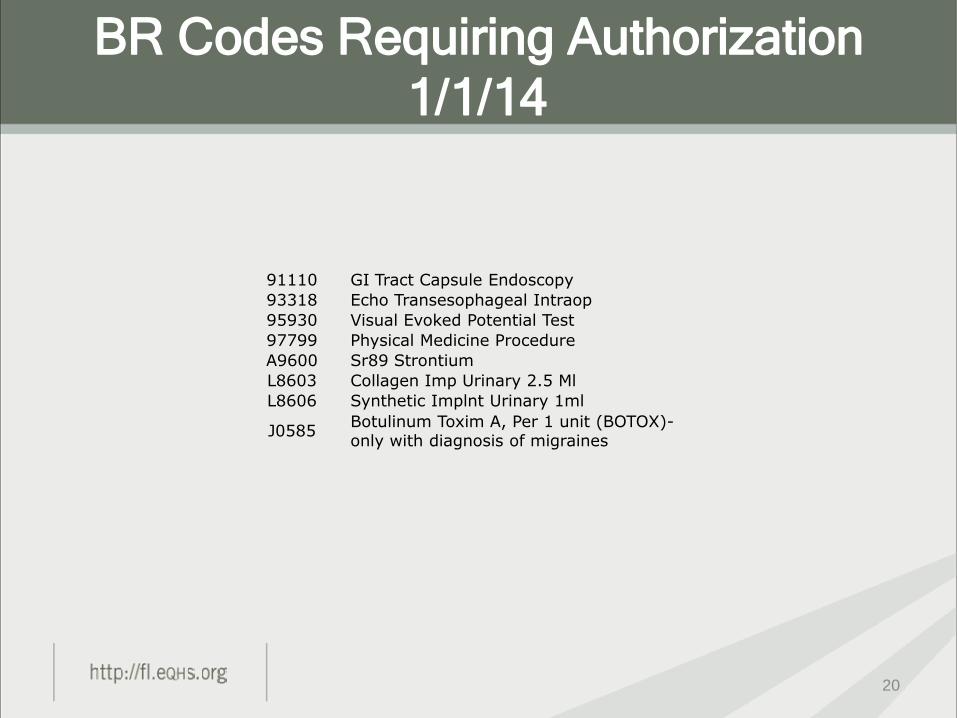
BR Codes Requiring Authorization
1/1/14
20
91110 GI Tract Capsule Endoscopy
93318 Echo Transesophageal Intraop
95930 Visual Evoked Potential Test
97799 Physical Medicine Procedure
A9600 Sr89 Strontium
L8603 Collagen Imp Urinary 2.5 Ml
L8606 Synthetic Implnt Urinary 1ml
J0585 Botulinum Toxim A, Per 1 unit (BOTOX)- only with diagnosis of migraines
Review Requests
21

Please submit all review requests to:
eQHealth Solutions
Attn: Multi-Specialty Department
5802 Benjamin Center Drive, Suite 105
Tampa, FL 33634
Submission of Review Requests
22
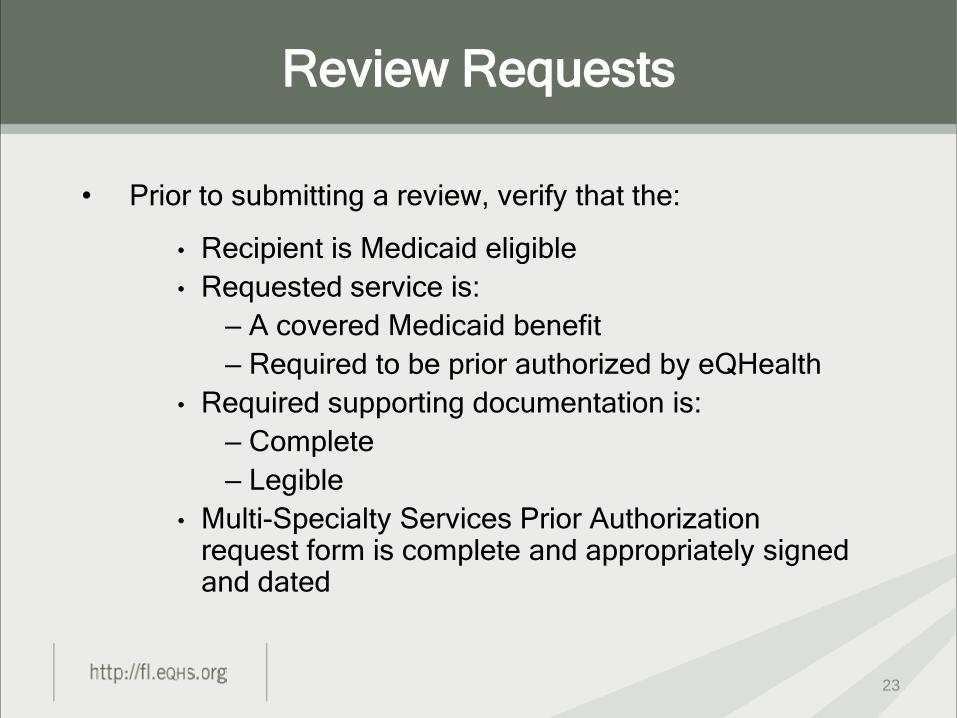
• Prior to submitting a review, verify that the:
• Recipient is Medicaid eligible
• Requested service is:
– A covered Medicaid benefit
– Required to be prior authorized by eQHealth
• Required supporting documentation is:
– Complete
– Legible
• Multi-Specialty Services Prior Authorization request form is complete and appropriately signed and dated
Review Requests
23

Types of Review Requests:
• Initial Authorization
• Retrospective
• Reconsideration review
– response to an adverse determination
Review Requests
24
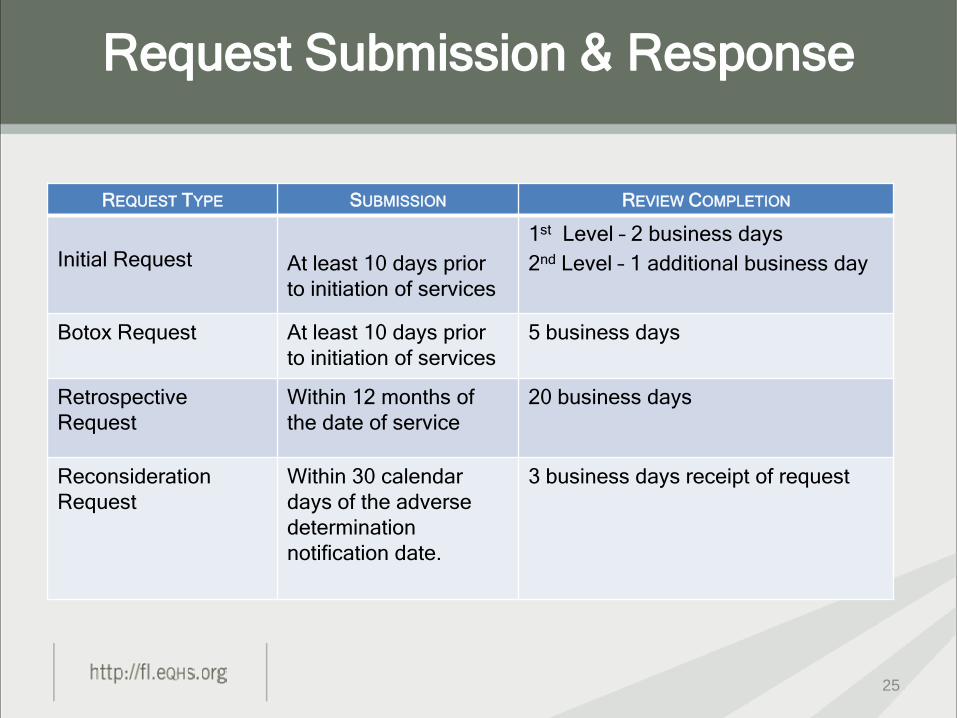
REQUEST TYPE SUBMISSION REVIEW COMPLETION
Initial Request
At least 10 days prior
to initiation of services
1st Level – 2 business days
2nd Level – 1 additional business day
Botox Request At least 10 days prior
to initiation of services
5 business days
Retrospective
Request
Within 12 months of
the date of service
20 business days
Reconsideration
Request
Within 30 calendar
days of the adverse
determination
notification date.
3 business days receipt of request
Request Submission & Response
25

Verification that there are no review exclusions:
• Recipient is not eligible for the service
• Duplication of service
• Requested service is not covered by Medicaid
First Level Review
Screening
26

Review Determination Process
• 1st Level Clinician Review:
– Administrative Screening
– Clinical Screening
• 2nd Level Peer Review
27

Review Determination Process
First Level Clinical Reviewers may:
• Approve the request
• Issue a technical denial of the request, if
appropriate, for example
– Duplicative service
– Noncompliant with Medicaid policy
• Pend the request back to the provider for:
– Additional or clarifying information
– Supporting documentation
• Refer the request to a second level Peer Reviewer
28
Review Determination Process
Pended Requests (Administrative/Clinical)
• An advisory letter is mailed to the requesting
provider.
• The information should be submitted within five
(5) business days of the request.
29
• Peer Reviewers base their determination on generally accepted professional standards of care, their clinical experience and judgment, Medicaid’s medical necessity criteria, and peer-to-peer consultation with the requesting provider when necessary.
• Peer Reviewers may render an approval or an adverse determination.
• An adverse determination may be a full denial of the requested services or a partial denial of the requested services.
Second Level Review
30
Determination notifications are issued to providers, and
recipients within one (1) business day of the determination.
• The requesting provider will receive a written notification of
the determination via mail.
• The recipient, or legal guardian, also receives written,
mailed notification of the determination via mail.
Review Determination Notification
31
Notifications include:
• Services approved or denied
• Reason for an adverse determination
• Rights to a reconsideration and how to
request one
• Recipient’s right to a fair hearing and how
the recipient may request one
Review Determination Notification
32

A peer reviewer, not involved in the original adverse determination, will:
• Uphold the original adverse determination; • Modify the original determination, approving a
portion of the services requested; or • Reverse the original determination, approving all
the services requested.
Reconsideration reviews are completed within three (3) business days of receipt of a complete and valid request.
Please Note: When requesting a reconsideration, new and/or additional clinical information must be submitted.
Reconsiderations

Any party involved in the case may request a
reconsideration of an adverse determination:
• Requesting Provider
• Recipient or Legal Guardian
Methods to request a reconsideration:
• Phone
• Fax
Reconsiderations
34
Recipients or their legal representatives may appeal
an adverse determination by requesting a fair hearing.
The request must be submitted within 90 days from
the date of the adverse notification letter by calling or
writing:
• The local Medicaid area office; or
• Department of Children Families Office of Appeals
and Hearings
Fair Hearings
35

Supporting documentation is determined by AHCA
policy and is required to substantiate the necessity of
items or services.
All supporting documentation must be submitted with
the request for authorization.
ALL authorizations must be requested using the Multi-
Specialty Services Prior Authorization Request Form.
Required Supporting Documentation
36
.
Supporting Documentation Requirements
37
SERVICE TYPE DOCUMENTATION
Physician Services •Current medical records (within the past 6
months)
•Treating physician referral to specialty
provider
•Radiographs, MRI, laboratory results,
•Photographs
•Diagnostic studies
•Medical clearance letter
eQHealth’s peer reviewers reserve the right to
request additional information or clarifying
information to substantiate the medical necessity
of the service(s) requested.
Supporting Documentation
Additional Information
38
• Submit all supporting documentation along
with the Multi-Specialty Services Prior
Authorization Request form via mail for the
initial request.
• Additional supporting information requested
after the initial request may be submitted via
mail or by fax to 855-677-3747.
Submitting Supporting
Documentation
39
12/31/13: Last date to submit claims with these
procedures to AHCA
1/1/14: First date to submit authorization requests to
eQHealth
1/1/14: eQHealth begins reviewing authorization requests
Transition Timeline
40

– Customer Service: 855-444-3747
Monday-Friday, 8 a.m.–5 p.m. Eastern
Time
– Dedicated Florida Provider Website
http://fl.eqhs.org
– Blast emails
Nancy Calvert, Provider Education and
Outreach Manager [email protected]
Provider Communications
and Resources
41

Questions and Answers
Thank-you for attending.
Your opinion is important to us.
Please complete the survey which will appear on your computer when
the webinar ends.
42