Embed Size (px)
Citation preview

PDF hosted at the Radboud Repository of the Radboud University
Nijmegen
The following full text is a publisher's version.
For additional information about this publication click this link.
http://hdl.handle.net/2066/21358
Please be advised that this information was generated on 2017-12-05 and may be subject to
change.

The Use of Monoclonal Antibody G250 in the Therapyof Renal-Cell Carcinoma
E. Oosterwijk, F.M.J. Debruyne, and J.A, Schalken
S INCE KOHLER AND MILSTEIN described
the technique to isolate monoclonal antibod
ies (MoAbs),1 much effort has been focused to
isolate MoAbs reactive with tumor antigens for
diagnostic and therapeutic applications.2'0 Despite
intense research, the isolation of clinically relevant
MoAbs has been disappointing. Preferably, such
MoAbs are reactive with tumor-specific antigens
(TSA) which should be expressed by all tumor cells
of a certain tumor type. However, unequivocal
evidence for unique TSA in human malignancies is
still lacking. Most human malignancies have weak,
if any, detectable immunogenic properties, indicat-
ing that most human cancers either are nonimmu-
nogenic or mediate strong immunomodulatory ef
fects. Current MoAbs of interest recognize tumor-
associated antigens (TAA) which are either
differentiation antigens (transiently) expressed dur- ing organogenesis, or aberrantly expressed anti
gens, which are (transiently) expressed elsewhere
in nonrelated normal tissue(s).
Administration of MoAbs that react with an
antigen present on many normal tissues may result
in unwanted side effects and diminish the amount
of MoAb delivered to the tumor, influencing the
efficacy of MoAb treatment. Therefore, 1) little
cross-reactivity with nontumorous tissues is prefer
able; 2) the TA A density on the tumor cells should
be high to achieve sufficient accumulation of
MoAb; and 3) all tumor cells must express the
TAA to enable the MoAb to specifically target to
all tumor sites, eg, to accomplish visualization of all
tumor sites or to achieve complete tumor remis
sion. Unfortunately, for the vast majority of TAA
that have been defined by anticarcinoma MoAbs,
these criteria are not met: 1) the TAA is usually
expressed on more than one type of carcinoma; 2)
not all tumors within a given tumor type express
the TAA (intertumor heterogeneity); 3) not all
From the Departm ent of Urology, A cad e m ic Hospital Nijmegen, T/ie Net/ier/ands.
Address reprint requests to E. Oosterwijk, P h D , Urological
Research Laboratory, Department of U ro logy , A cad e m ic Hos])itai Nÿmegen, Geert Grootepicin Zuid. 16, PO B o x 9 10 1 , 6 5 0 0 H ß Nÿmegen, T h e Netherlands.
Copyright © J 995 by W .B . Saunders Company 0 0 9 3 ~ 7 7 5 4 f 9 5 / 2 2 0 l '0 0 0 8 $ 0 5 . 0 0 / 0
cells within a tumor lesion, including métastasés,
express a particular TAA (intratumor heterogene
ity); 4) lesions of one patient express a TAA to a
varying degree; 5) temporal modulation of TAA
may occur; and 6) TAA expressed on most cells of
a particular carcinoma are often expressed on some
normal adult tissues. In general, with higher percent
age of positive tumor cells and tumors expressing
the TAA, cross-reactivity with normal tissues in
creases.
MOABS REACTIVE WITH RENAL-CELLCARCINOMA
A number of MoAbs reactive with cell surface
antigens of renal-cell carcinoma (RCC) have been
identified.7'15 The specificity of the majority of
RCC-related MoAbs has been established using
immunohistochemistry. Less is known about their
targeting abilities and antitumor efficacy. The
MoAbs can be divided into two groups: 1) MoAbs
recognizing differentiation antigens,7'14 and 2)
MoAbs recognizing RCC-TAA aberrantly ex
pressed in RCC, ie, recognizing an RCC-antigen
absent from normal kidney.8'10,14,15 Most MoAbs of
the latter category show very restricted cross
reactivity with normal tissues as judged using
immunohistochemistry. It appears that these MoAbs
identify different RCC-TAA because they display
different cross-reactivity with normal tissues. In
view of their restricted cross-reactivity with normal
tissues in combination with expression of a given
RCC-TAA in most RCC, these MoAbs are prime
candidates for clinical investigations.
One of the MoAbs recognizing an aberrantly
expressed RCC-TAA, MoAb G250, was obtained
after fusion of spleen cells from a mouse immunized
with fresh RCC homogenates.15 This MoAb identi
fies an antigen absent from normal kidney and
other normal tissues examined, with the exception
of gastric mucosal cells and cells of the larger bile
ducts. In the initial study, G250 antigen expression
of 55 RCC was examined: 42 of 47 primary RCC
showed homogeneous G250 antigen expression
(89%), four tumors showed heterogeneous G250antigen expression and only one primary tumor was
completely devoid of G250 antigen expression.
More importantly, of eight métastasés examined,
34 Sem/ntfrs in Oncology, Voi 22, No I (February), 1995: pp 34-41

MoAb G250 IN RENAL CANCER 35
five showed homogeneous G250 expression (62%),
two showed heterogeneous U250 expression and
one metastasis failed to express U250 antigen.b
With an increased number of RCC tested, no
difiere nee with respect to the percentage of RCC
expressing G250 antigen has been observed. In 77
of 95 (81%) primary RCC cases that were investi
gated, more than 50% of tumor cells were scored
positive and in an additional eight patients, primary
tumor cells also stained, albeit with lower fre
quency; ie, approximately 90% of primary RCC
express C250 antigen. For the metastatic lesions,
G250-positive tumor cells were noticed in 18 of 22
tumors (82%) examined, with homogeneous stain
ing in 9 of 17 metastatic RCC examined (53%). in
general, clear cell RCC tend to show homogenous
G250 antigen expression, whereas non-clear cell
RCC show heterogenous G250 expression. In view
of the restricted cross-reactivity with normal tissues
and the homogeneous expression in most RCC
examined, this MoAb seemed useful as a therapeu
tic and/or radiodiagnostic agent,
EXPERIMENTAL DATA
Tumor Studies
The preferential accumulation of MoAb G250 was investigated in a RCC xenograft model.16
BALB/c nu/nu mice were xenogrufted with human
RCC and/or human noivRCC tumors, and in
jected with 12̂ I-labeled MoAb G250 lgGl, F(ab')2
or Fab'. Specific MoAb G250 accumulation was
observed in the RCC tumors for all antibody forms.
G250-negative tumors did not show any MoAb
G250 uptake, nor did the G250-positive tumors
show increased uptake of nonrelevant immuno
globulin. Higher uptake was generally found with
intact G250 than with G250 F(ab')¿ or Fab'
fragments, most probably because of slower blood
clearance, leaving the antibody more time to diffuse
to the tumor cells. The lowest uptake was observed
for Fab' fragments, related to a short biological
half-life and lower avidity. Similar studies were
performed by Chiou et al with MoAb A6H, an
MoAb that reacts with a normal kidney-difierentia-
tion antigen.17 For MoAb G250 as well as MoAb
A6H relatively high tu mor/blood ratios were ob
served compared with other mouse targeting stud
ies. This is possibly related to a general increase in
permeability of the vascular bed in RCC xeno
grafts.18
In addition to these mouse-targeting studies,
supplementary studies were performed with ex vivo
perfused tu mor-bearing human kidneys.19 In this
model system tumor-bearing kidneys are flushed
with preservation fluid immediately after surgery,
whereupon the kidneys can be perfused with the
MoAb of interest. Using this model system, the
tumor targeting ability of 99mTc-labeled MoAb
G250 was investigated. yy,nTc MoAb G250 imaging
of tumor-bearing kidneys resulted in clear images of
RCC, with no MoAb G250 uptake in normal renal
tissue. Despite the low temperature (0 to 4°C to
assure appropriate pressures) and the relatively
short circulation time (16 hours), tumor to kidney
ratios were approximately 8:1.19 The preferential
uptake of MoAb G250 in these ex vivo experi
ments were a clear indication that this MoAb held
promise for clinical use.
MoAb G250 Mediated ThcraljyTumor cells may be lysed by MoAb-directed
effector cells, so-called antibody-dependent cell-
mediated cytotoxicity (ADCC). Several cell types
have been shown to be active in ADCC, including
macrophages, natural killer (NK) cells, killer (K)
cells, and neutrophils. Experimental studies have
highlighted the importance of antibody subclass»20
and mouse MoAbs of the IgG2a subclass have been
shown to have the greatest activity in ADCC
a si'* ; 21.22
The antitumor effect of MoAb 0250 alone and
in combination with biological response modifiers
(BRMs) was tested in a nude mouse model.23
Because the original MoAb G250 clone produced
immunoglobulin of lgGl subclass, a poor mediator
of ADCC, an IgG2a class switch variant of the
original clone was developed. As a consequence,
MoAb G250 specificity, idiotype and avidity were
retained. Mice carrying established subcutaneous
RCC tumors of approximately 50 mm* were treated
with different doses. Administration of 100 pug
MoAb G250 per mouse for 6 weeks with three
weekly injections resulted in a significant (P < .01)
inhibition of mean tumor growth to 50% of control
tumors. Increasing the MoAb G25Ö dose to 500
fJLg/dose, showed an inhibition of mean tumor
growth to 35% of controls (P < .0001 versus
control group). However, this increased tumor
growth inhibition was not statistically different
from the 100-|xg dose schedule. No complete
tumor regression was observed in any of the treated
animals.

36 OOSTERWIJK, DeBRUYNE, AND SCHALKEN
For this RCC xenograft (NU12), the optimal
treatment schedule with biological response modifi
ers had been established in earlier studies.24 BRM
treatment alone resulted in significant tumor growth
inhibition, but complete tumor regression was
never observed, despite the intense treatment sched
ule. We combined the best BRM treatment, rIFNa
plus rTNFa, with MoAb G250 treatment to inves-
tigate whether the efficacy of this combined treat'
ment was superior to either treatment alone. This
combination treatment significantly reduced NU12
tumor growth as compared with MoAb G250 or rIFNa/rTNFa alone (P < .0006 versus MoAb
G250 alone, P < .003 versus rlFNa plus rTNFa).
In the majority of mice tumors stabilized, and in
several mice complete tumor regression was ob-
served. No effects were observed when mice were
treated with irrelevant IgG or with MoAb G250
F (ab') 2 fragments, indicating that the effect was
MoAb G250 specific and Fc-dependent. The Fc-
dependency also indicated that ADCC was prob'
ably playing a role in the destruction of tumor cells.
Histochemical examination revealed that MoAb
G250- or rlFNa/rTNFa-treated tumors were infil
trated by very few macrophages, if any, similar to
control tumors in which macrophage infiltrates
were absent. In contrast, massive macrophage tu
mor infiltration was observed in MoAb G250/
rIFNa/rTNFa-treated tumors. These infiltrates
seemed to be infiltrating viable tumor nests and
surrounded large necrotic areas. Most likely, BRM
treatment leads to activation of mouse NIK cells
and macrophages, both mediators of ADCC, result
ing in effective macrophage-mediated ADCC.23
Although these results are encouraging! it re
mains to be investigated whether unmodified MoAb
G250 IgG2a will be useful therapeutically. We have
performed in vitro ADCC experiments using fresh
isolated human monocytes as effector cells, and
have not observed any tumor cell lysis. Different
RCC cell lines were used to circumvent problems
that may occur because of the use of a lysis -
resistent cell line, and to assure that antigen densi ty
(which has been shown to be important in active
ADCC,25) did not play a role. MoAb G250 IgG2a
may not be effectively recognized by these human
effector cells or, alternatively, these effector cells
may have to be activated to mediate ADCC or
G250-antigen density is too low. The latter possibil
ity seems unlikely in view of the high number of
antibody binding sites on these RCC cell lines.9
Enhancement of the ADCC capability of MoAb
G250 can probably be achieved by chimerization of
the antibody (chimeric MoAbs consist of mouse Ig
variable regions grafted onto human Ig constant
regions). However, preliminary ADCC experi
ments with chimeric G250 lgGl and purified
human monocytes as effector cells have been
unsuccessful. Combining activated human lympho
cytes with chimeric MoAb G250 may facilitate
ADCC.
CLINICAL EXPERIENCE
Significant clinical experience with radiolabeled
murine MoAbs that detect TAA has been acquired
in the last decade.2'6 Radioimmunoscintigraphy
studies of RCC with MoAbs have been limited,
generally restricted to animal models.16,17,26'29 Ves-
sella et al performed an imaging/radiotherapy trial
in RCC patients with MoAb A6H, an MoAb that
recognizes a kidney differentiation antigen.30,31 Posi
tive images were obtained in 5 of 15 patients
examined. The low number of positive images was
attributed to the presence of circulating antigen,
and the formation of antigen-antibody complexes.
The number of positive images increased with an
altered dosing schedule, but the number of imaged
lesions remained unsatisfactory.
Based on our targeting studies in RCC-bearing
mice and in ex vivo perfused tumor-bearing kid
neys, a phase I study with 13iI-labeled MoAb G250
was performed.32 In this protein dose escalation
study, the primary study objectives were evaluation
of the toxicity, pharmacokinetics, and localization
capabilities of 1311 MoAb G250. More than 90% of
primary and metastatic disease as demonstrated by
magnetic resonance imaging (MRI) and computed
tomography (CT) scans was imaged by ml MoAb
G250. Metastatic lesions in lymph nodes, bone, and
lung were visualized. Furthermore, additional meta
static disease documented at surgery but not de
tected by MRI and CT scans was visualized. For example, radioimmunoscintigraphy with l3lI MoAb
G250 showed a small hot spot in the liver of one of
the patients which was not visualized by other
means. Nine months later, the patient showed
recurrence of RCC in that precise location. 1311i
MoAb G250 scanning also revealed diffuse meta
static RCC not recognizable by MRI or CT in a
polycystic kidney of another patient.
From the ability of MoAb G250 to yield sharp
images and visualize small tumor lesions it was

MoAb G250 IN RENAL CANCER 37
concluded that MoAb G250 has considerable poten-
tial as an imaging agent. However, not all primary
or metastatic RCC lesions express G250 antigen,
and some express it only in a minority of cells. This
emphasizes the need for additional RCC-specific
MoAbs because problems of antigen heterogeneity
have to be overcome for therapeutic efficacy.
The absorbed dose to the tumor delivered by the
best MoAb/radionuclide combination studies thus
far has been calculated at 2,000 to 3,000 cGy, while
maintaining less than grade IV toxic effects.27
Vaughan et al calculated the minimal requirement
for effective therapy with 13lI and 90Y-labeled
MoAbs injected intravenously assuming an avarage
accumulation of 0.005% of the administered dose/g
of tumor and a maximum reasonable whole body
dose of 2 Gy.33,34 These investigators concluded
that the tumor uptake should be increased by a
factor 10 for effective therapy, Calculation of the
maximal fraction of the injected dose 1311 MoAb
G250 recovered in tumor sites showed that this was
generally 10 to 100 times greater than previously
reported accumulation of radiolabeled MoAb in
solid tumors. The mean accumulation of the admin
istered dose was also approximately tenfold higher
than previously reported, fulfilling die require
ments of Vaughan et al.33,34
Based on these findings, a phase I/II trial with
escalating doses of 131I labeled to 10 mg of MoAb
G250 was undertaken in groups of three patients
with inoperable metastatic RCC.35 Thus far, 21
patients have been treated. The maximum adminis
tered dose has been 90 mCi/m2. Targeting of
radioactivity to all known sites of disease was seen
in all G250-antigen positive patients (19 of 21).
Elevation of hepatic enzymes was observed in 18
patients, starting approximately 10 days after treat
ment and returning to baseline by 3 weeks. This
elevation is probably due to MoAb G250 accumula
tion in the liver. G250 antigen is expressed in the
larger bile ducts, and examination of liver biopsy
specimens in the phase I protein dose escalation
trial revealed MoAb G250 accumulation in bile
duct epithelium. However, the amount of MoAb
G250 necessary to saturate the hepatic compart
ment was minimal, and estimated in the range of
200 ]xg. Nevertheless, this amount seems to be
sufficient to induce mild liver toxicity. At the
75-mCi/m2 dose level, one of six patients had
reversible grade IV thrombocytopenia, with a nadir
at 4 weeks. No other major toxicity has been
observed. There have been no major responses, but
it is encouraging that stable disease was noted in 11
patients up to 9 months postradioimmunotherapy,
as these patients with disseminated inoperable
RCC tend to do very poorly.
CHIMERIZED MoAb G250
Generally, administration of murine MoAbs to
patients elicits a human antimouse antibody
(HAMA) response. This HAMA response is often
directed against the Fc part of the immunoglobulin
and independent of the amount of MoAb, or
administration route. In all sera obtained from
MoAb G250-injected RCC patients, HAMA of
the IgM and IgG subclasses were detected.32 For
repeated administration, eg, multiple radioimmuno
therapy or multiple treatment with naked antibody
to induce ADCC, HAMA responses need to be
minimized because circulation HAMA reduces the
tumor uptake of MoAb at subsequent administra
tion because of MoAb-HAMA cross-linking. With
recombinant technology, mouse MoAb variable regions can be grafted onto human Ig constant
regions, and these constructs can be subsequently
transfected into mammalian cells, which now pro
duce chimeric immunoglobulin.36'38 Substitution of
the mouse Fc part by human Fc has the additional
advantage that all Fc-related effector functions are
now matching the human effector cells. Principally,
the use of chimeric IgG should augment ADCC
mediated tumor cell lysis, and unmodified chimeric
MoAb might be suitable to destroy (minimal)
residual disease. Chimerized antibodies are ex
pected to be less immunogenic in man. We have
produced chimeric MoAb G250 (lgGl subclass)
and are currently testing their efficacy in ADCC
and will start a phase I protein dose escalation trial
to investigate the pharmacokinetics and targeting
ability of chimerized MoAb G250.
G250-RELATED ANTI-IDIOTYPE ANTIBODIES
In the preceding sections, the use of MoAb G250
as a passive immunotherapeutic agent was dis
cussed. Another strategy is to use MoAbs to induce
active immunization. In 1974̂ Jerne proposed that
the immune system is at a steady state by an
equilibrium of lymphocytic clones bearing comple
mentary receptors.39 This equilibrium can be dis
turbed either by a foreign or self-antigen, resulting
in a response which aims at the restoration of the
balance. In this response, anti-antibodies (Ab2)

38 OOSTERWIJK, DeBRUYNE, AND SCHALKEN
play a major role. This hypothesis has become
known as the network theory and has been substan
tiated by many investigators. The critical feature of
this theory is that the binding pocket of the
antibody that determines its specificity elicits anti-
antibodies. Several so-called idiotypic determinants
can be present on one immunoglobulin molecule.
In some cases anti-idiotypic antibodies will mimic
the original antigen. These so-called internal image
Ab2 offer promise as “vaccines” to various infec
tious agents, and they might be used to induce
immune responses to tumor antigens.40'46 One of the advantages of this appealing approach is the
long-lasting protection that vaccination with TAA- mimicking MoAbs might achieve. Principally, the
requirements of these internal image MoAbs are
the same as those for MoAbs recognizing TAA that
might be useful for passive immunotherapy. Cross
reactivity with normal tissues should be minimal, to
minimize undesired side effects related to organ
toxicity elicited by vaccination with internal image
MoAbs resembling normal differentiation antigens.
Chattopadhyay et al have demonstrated that vacci
nation with Ab2 resembling a melanoma-associ
ated TAA that is expressed on a restricted number
of normal tissues can induce TAA-specific re
sponses, indicating that TAA expression on a
restricted number of tissues does not hamper the
successful implementation of Ab2 vaccination.47
Considering the restricted expression of G250,
vaccination with internal image Ab2 resembling
this RCC-T A A might represent a new therapy for
RCC patients. Therefore, we have started to isolate
Ab2 bearing the internal image of MoAb G250. Six
MoAbs were isolated after fusion of spleen cells
from mice immunized with MoAb G250 which
showed a dose-dependent inhibition of binding of
i25I-MoAb G250 to antigen. Because Abl-Ab2
interactions in close vicinity of Ab 1-antigen inter
actions will interfere with Ab 1-antigen binding,
competition for antigen binding was insufficient
evidence to conclude that true internal image Ab2
were isolated. To investigate whether these Ab2
could substitute for the initial G250 antigen, mice
and rabbits were immunized with the Ab2 to
monitor for the occurrence of Ab3 resembling
MoAb G250 (so-called Abl'). Indeed, for all six
Ab2 Abl' antibodies were detected, showing the
functional identity of the six MoAbs and G250
antigen.48
Initially, these six MoAbs were divided into two
immunologically distinct groups, recognizing two
partly overlapping epitopes.48 However, additional
fine specificity studies have shown that the six
internal-image MoAbs can be divided into four
mutually exclusive groups, evidence that the six
Ab2s recognize four slightly different idiotopes in
the Abl binding pocket.49 Because they seem to
recognize unique epitopes in the MoAb G250
binding pocket, it implies that not all six internal
image MoAbs are true representations of G250
antigen. Consequently, one of the MoAbs may
show superior antitumor characteristics.
To investigate the antitumor efficacy of immuni
zation with Ab2, serum of Ab2-immunized mice
was transferred to nu/nu BALB/c mice challenged
with human RCC cells. In this Winn-type assay,
transfer of any Ab3-serum resulted in significant
tumor growth inhibition (4 weeks; P < .05 versus
all control groups, 8 weeks; P < .01 versus all
control groups) and lower tumor take as compared
with control groups (Table 1). Four weeks after
tumor challenge, no significant difference between
Ab3 treatment groups was seen. Small tumors were
detectable in all Ab3-treated animals. However, 8
weeks after tumor challenge (3 weeks after cessa
tion of therapy), remarkable differences between
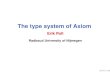
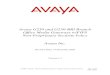
the different treatment groups were observed (Fig
1). All mice treated with Ab3-91 showed complete
tumor regression. Macroscopically as well as micro
scopically no tumor remnants could be detected.
Ab3-31 treatment resulted in tumor regression in
the majority of animals and tumor stabilization of
the remaining tumors. Similarly, Ab3-82 treatment
effected tumor regression in the majority of ani
mals, with extremely slow growing tumors in the
remaining animals. After Ab3-71 treatment, slow
growing tumors were measurable in all animals.
The doubling time of tumors remaining after Ab3
treatment was significantly lengthened. Four weeks
after cessation of therapy the tumors started to
grow with doubling times comparable to control
tumors. It is likely that 4 weeks after discontinua
tion of therapy the circulating levels of Abl'
antibody and serum factors were depleted and too
low for continuation of tumor control. Likewise,
the early growth of the tumors treated with Ab3-91
can be explained by a dose effect. Because the Abl '
titers were moderate, several treatments may be
necessary to achieve sufficient high levels of Abl'
for tumor control and regression. Based on these
results we conclude that NUH-91 immunization

MoAb G250 IN RENAL CANCER 39
Table 1. Summary of Representative Protection Experiment With Ab3 Sera•
TreatmentNo. of Mice
Tumor Take (% ) 4 w 8 w
Tumor Volume (mm3 ± SE) 4 w 8 w
Ab3-31 5 100 80 9.8 ± 2.5* 11.8 ±5.6+Ab3-71 5 100 100 10 ± 2.2* 26.7 ± 5.2+Ab3-82 6 100 66.7 8.1 ± 2.7* 17.9 i 8.7+Ab3-91 6 100 0 7.7 ± 2.2* 0+Nontreatment 6 100 100 23.5 ± 4.4 126 ± 16.6Ab3-MOPC 5 100 100 29 ± 7.5 98.9 ± 12.3NMS* 5 100 100 31.8 ± 14.4 114 ± 21.0
*P < .05.tP < .01 compared with last three cases in this list. ^Abbreviation: NMS, treated with normai mouse serum.
elicits the most powerful antitumor effects, and
that this Ab2 might be the best candidate for
clinical trials.
Because the animals were treated with whole
serum, the antitumor effects can also be explained
by circulating serum factors, eg, T cell factors and
cytokines. We and others have shown that combi
nation therapy with BRMs, which are serum circu
lating factors, can result in significant tumor growth inhibition. Treatment of established RCC xeno
grafts with interferon-alfa, tumor necrosis factor
and MoAb G250 resulted in tumor growth inhibi
tion and tumor regression.23 However, preliminary
experiments have shown that Ab3 treatment is
superior to BRM/MoAbG250 treatment. It is there
fore likely that at least part of the antitumor effects
are Abl' related. We are currently investigating
the therapeutic efficacy of Ab3 serum in mice with
established RCC xenografts.
The tumor regression induced by Ab3 serum
transfer could also be explained by the presence of
T cell factors such as specific macrophage arming
factor (SMAF) and mast cell T-Cell factor (MTCF).
These factors can, among others, provide antigen-
specificity to nonspecific cells.50'52 Immunization of
immune competent mice with any of the six Ab2
investigated results in profound transferable anti
gen-specific cell-mediated immunity, with concomi
tant serum transferable early delayed-type hyper
sensitivity responses, attributable toT cell factors.53
Because these factors persist approximately 2 to 16
days after immunization,50 and animals were treated
with immune serum harvested 7 days after immuni
zation, part of the antitumor effects may have been
C Aba -31
Fig I. Individual tumor growth curves of RCC challenged mice treated with Ab3 sera. BALB/c nu/nu mice received s.c. injections of 10s SK-RC-52 cells (G250-posi- tive human RCC cell line) in the right flank, and treatment was started. Four groups of mice were treated with i.p. injections of NUH» Ab3 sera, and three groups served as controls: no treatment was given (None), mice were treated with serum from MOPC21-KLH immunized mice, or mice received normal mouse serum (not shown). Tumor volumes are expressed as mean ± SE. Figure is representative for several independently performed experiments.
200-aaaaa|
150-cm m
3 100 -
050-
< 0 ■?0 3
c3 200-
0150-
m m
3“ 5
100-
50-
n J
D Aba -71200 -
150-
100 -
E Aba -82200 -
150-
100 -
50-
F Ab3-91
3 4 5 6 7 8
week

40 OOSTERWIJK, DeBRUYNE, AND SCHALKEN
elicited by T cell factors. It is likely that similar
factors, with similar anti tumor efficacy will be
induced by Ab2 immunization of RCC patients.
FUTURE PROSPECTS
Our future efforts will be directed at investigat
ing the targeting ability of chimerized MoAb G250.
We anticipate that chimerization of murine MoAb
G250 will allow multiple treatments, because hu-
man antimouse responses are reduced. If that is
true, multiple treatments with, eg, high-dose l31I-
labeled chimeric MoAb G250 would become fea-
sible. Once the targeting ability and pharmacokinet
ics of chimeric MoAb G250 are known, we intend
to investigate the radioimmunotherapeutic poten
tial of high-dose 131I-labeled chimeric MoAb G250.
In addition, chimerization may provide the anti
body with appropriate effector functions. This will
enable engagement of human effector cells with
chimeric MoAb-G250 coated tumor cells, effectuât-
ing tumor cell lysis.
We will also pursue the possibilities of anti
idiotype therapy. Much needs to be resolved with
respect to the identification of the mechanism
behind the observed antitumor efficacy. Currently
we are in the process of identifying which effector
cells are involved in tumor cell elimination, and are investigating which factors are of prime importance
for tumor regression. Regardless of the effector
mechanism, our observation that Ab2 vaccination
results in tumor regression is of clinical relevance
because it seems to indicate that tumor immunity
can be acquired. Patients at risk for tumor recur
rence, eg, patients with T3NoMo disease, may
benefit from adjuvant treatment by Ab2 vaccination.
REFERENCES1 . Köhler G, Milstein C: Continuous cultures of fused cells
secreting antibody of predefined specificity. Nature (London)
256:495-497, 1975
2. Larson SM: Lymphoma, melanoma, colon cancer: Diagno
sis and treatment with radiolabeled monoclonal antibodies. The
1986 Eugene P Pendergrass New Horizons Lecture. Radiology
165:297-304, 1987
3. Larson SM: Clinical radioimmunodetection, 1978-1988:
Overview and suggestions for standardization of clinical trials.
Cancer Res 50:892s-898s, 1990 (suppl)
4> Mach JP, Pelegrirv A, Buchegger F: Imaging and therapy
with monoclonal antibodies in non-hematopoietic tumors. Curr
Opin Immunol 3:685-693, 1991
5. Goldenberg DM: Current status of cancer imaging with
radiolabeled antibodies. Antibody, Immunoconjugates Radio-
pharm 4:517-524, 1991
6 . Goldenberg DM: Targeting of cancer with radiolabeled
antibodies: Prospects for imaging and therapy. Arch Pathol Lab
Med 112:580-586, 1988
7. Oosterwijk E, Ruiter DJ, Wakka JC, et al: Inununohisto-
chemical analysis of monoclonal antibodies to renal antigens:
Application in the diagnosis of renal cell carcinoma. Am J
Pathol 123:301-309, 1986
8. Luner SJ, Ghose T, Chatterjee S, et al; Monoclonal
antibodies to kidney and tumor-associated surface antigens of
human renal cell carcinoma. Cancer Res 46:5816-5820, 1986
9. Vessella RL, Moon TD, Chiou R-K, et al: Monoclonal
antibodies to human renal cell carcinoma: Recognition of shared
and restricted tissue antigens. Cancer Res 45:6131-6139, 1985
10. Finstad CL, Cordon-Cardo C, Bander NH, et al: Specific
ity analysis of mouse monoclonal antibodies defining cell surface
antigens of human renal cancer. Proc Natl Acad Sci USA
82:2955-2959, 1985
11. Bander NH, Finstad CL, Cordon-Cardo C, et al: Analysis
of a mouse monoclonal antibody that reacts with a specific
region of the human proximal tubule and subsets renal cell
carcinomas. Cancer Res 49:6774-6780, 1989
12. Tagliabile E, Canevari S, Menard S, et al: Human renal
antigen defined by a murine monoclonal antibody. J Natl Cancer
Inst 73:363-369, 1984
13. Yoshida SO, Imam A: Monoclonal antibody to a proxi
mal nephrogenic renal antigen: lmmunohistochemical analysis
of formalin-fixed, paraffin-embedded human renal cell carcino
mas. Cancer Res 49:1802-1809, 1989
14. Kochevar ]: A renal cell carcinoma neoplastic antigen
detectable by immunohistochemistry is defined by a murine
monoclonal antibody. Cancer 60:2031-2036, 1987
15. Oosterwijk E, Ruiter DJ, Hoedemaeker Ph], et al: Mono
clonal antibody G250 recognizes a determinant present in
renal-cell carcinoma and absent from normal kidney. Int J
Cancer 38:489-494, 1986
16. Van Dijk J, Zegveld STh, Fleuren GJ, et al: Localization
of monoclonal antibody G250 and bispecific monoclonal anti
body CD3/G250 in renal-cell carcinoma xenografts: Relative
effects of size and affinity. IntJ Cancer 48:738-743, 1991
17. Chiou R-K, Vessella RL, Elson MK, et al: Localization of
human renal cell carcinoma xenografts with a tumor-preferen-
tinl monoclonal antibody. Cancer Res 45:6140-6146, 1985
18. Sands H, Jones PL, Shah SA, et al: Correlation of
vascular permeability and blood flow with monoclonal antibody
uptake by human clouser and renal cell xenografts. Cancer Res
48:188-193,1988
19. Van Dijk J» Oosterwijk E, Van Kroonenhurgh MJPG, et
al: Perfusion of tumor-bearing kidneys as a model for scinti
graphic screening of monoclonal antibodies. J Nucl Med 29:1078-
1082, 1988
20. Herlyn D, Koprowski H: IgG2a monoclonal antibodies
inhibit human tumor growth through interaction with effector
cells. Proc Natl Acad Sci USA 79:4761-4766, 1982
21. Johnson WJ, Steplewski Z, Matthews J, et al: Cytolytic
interactions between murine macrophages, tumor cells, and
monoclonal antibodies. Characterization of lytic conditions and
requirements for effector activation. J Immunol 136:4704-4713,
198622. Kripps TJ, Parham P, Pumt J, et al: Importance of
immunoglobulin isotype in human antibody-dependent, cell-

MoAb G250 IN RENAL CANCER 41
mediated cytotoxicity directed by mouse monoclonal antibodies.
J Exp Med 161:1-17, 1985
23. Van Dijk J, Uemura H, Beniers AJMC, et al: Therapeutic
effects of monoclonal antibody G250, interferons, and tumor
necrosis factor in mice with renal cell carcinoma xenografts. Int
J Cancer 56:262-268, 1994
24. Beniers AJMC, Van Moorselaar RJA, Peelen WP, et al:
Differential sensitivity of three human renal tumor xenografts
towards therapy with interferon-alpha, interpheron-gamma,
tumor necrosis factor and their combinations. Urol Res 19:91-
98,1991
25. Herlyn D, Powe J, Ross A, et al: Inhibition of human
tumor growth by IgG2a monoclonal antibodies correlates with
antibody density of tumor cells. J Immunol 134:1300-1304, 1985
26. Palme DF, Berkopec JM, Elson MK, et al: Dosimetry and
immunotherapy using monoclonal antibody (MoAb) A6H 131-
iodine conjugates: Radiobiological consequences and effect of
escalating dosages. Proc Am Assoc Cancer Res 29:428, 1988
(abstr 1706)
27. Wessels BW, Vessella RL, Palme DF, et al: Radiobiologi
cal comparison of external beam radiation and radioimmuno-
therapy in renal cell carcinoma xenografts, Int J Radiat Oncol
Biol Phys 17:1257-1263, 1989
28. Vessella RL, Palme DF, Berkopec JM, et al: Radiotherapy
of a human renal cell carcinoma (RCC) xenograft: Comparison
between single fraction monoclonal antibody (MoAb) A6H
131-iodine conjugates and single fraction x-ray external beam
irradiation. Proc Am Assoc Cancer Res 29:429, 1988 (abstr
1707)
29. Chiou R-K, Woodson M: Monoclonal antibody-targe ted
radiotherapy (MRT) for renal cell carcinoma: Evaluations of its
potentials and limitations, Proc Am Assoc Cancer Res 29:438,
1988 (abstr 1743)
30. Vessella RL, Chiou RK, Grund FM, et al: Renal cell
carcinoma (RCC) phase I-II trials with 131-1 labeled mono
clonal antibody A6H: Imaging and pharmacokinetic studies,
Proc Am Assoc Cancer Res 28:480, 1987 (abstr 1525)
31. Vessella RL: Radioimmunoconjugates in renal cell carci
noma, in Dehruyne FMJ, Bukowski RM, Pontes JE, et al (eds):
Immunotherapy of renal cell carcinoma. Heidelberg, Germany,
Springer Verlag, 1991, pp 38-46
32. Oosterwijk E, Bander NH, Divgi CR, et al: Antibody
localization in human renal cell carcinoma: A phase I study (if
monoclonal antibody G250. J Clin Oncol 11:738-750, 1993
33. Vaughan ATM, Anderson P, Dykes PW, et al: Limita
tions to the killing of tumours using radiolabelled antibodies. Br
J Radiol 60:567-578, 1986
34. Vaughan ATM, Brad well AR, Dykes PW, et al: Illusions
of tumour killing using radiolabelled antibodies. Lancet 1:1492-
1493, 1986
35. Divgi CR, Bander NH, Scott AM , et al: Phase I
radioimmunotherapy trial of 1-131 labeled monoclonal antibody
G250 in metastatic renal cancer. Proc Am Assoc Cancer Res
35:503, 1994 (abstr 2999)
36. Morrison SL, Johnson MJ, Herzenberger LA, et al:
Chimeric human antibody molecules: Mouse antigen-binding
domains with human constant regions domains. Proc Natl Acad
Sci USA 81:6851-6855, 1984
37. Morrison SL: Transfectomas provide novel chimeric
antibodies. Science 229:1202-1207, 1985
38. Winter G, Milstein C: Man-made antibodies. Nature
(London) 349:293-299, 1991
39. Jerne NK: Towards a network theory of the immune
system. Ann Immunol 125:373-389, 1974
40. Sikorska HM: Therapeutic applications of anti-idiotypic
antibodies. J Biol Response Mod 7:327-358, 1988
41. Ferrane S: Monoclonal antibodies and tumor vaccines.
Curr Opinion Oncol 2:1146-1151, 1990
42. Gaida F-J, Fenger U, Wagener C, et al: A monoclonal
anti-idiotypic antibody bearing the internal image of an epitope
specific to the human carcinoembryonic antigen. Int J Cancer
51:459-465, 1992
43. Kusama M, Kageshita T, Chen JJ, et al: Characterization
of syngeneic antiidiotypic monoclonal antibodies to murine
anti-human high-molecular-weight melanoma-associated anti
gen monoclonal antibodies. J Immunol 143:3844-3852, 1989
44. Lehmann H-P, Zwicky C, Waibcl R, et al: Tumor-antigeti-
specific humoral immune response of animals to anti-idiotypic
antibodies and comparative serological analysis of patients with
small-cell lung carcinoma, Int J Cancer 50:86-92, 1992
45. Mittelman A, Chen ZJt Kageshita T, et al: Active specific
immunotherapy in patients with melanoma: A clinical trial with
mouse antiidiotypic monoclonal antibodies elicited with synge
neic anti-high-molecular-weight-melanoma-associated antigen
monoclonal antibodies. J Clin Invest 86:2136-2144, 1990
46. Robins RA , Denton GW L, Hardcastle JD, et al: Anti-
tumor response and interleukin 2 production induced in colorec
tal cancer patients by immunization of human monoclonal
anti-idiotypic antibody. Cancer Res 51:5425-5429, 1991
47. Chattopadhyay P, Kaveri SV, Byars N, et al: Human high
molecular weight-melanoma associated antigen mimicry by an
anti-idiotypic antibody: Characterization of the immunogenicity
and the immune response to the mouse monoclonal antibody
IMel-1. Cancer Res 51:6045-6051, 1991
48. Uemura H, Okajima E, Dehruyne FMJ, et al: Internal
image anti-idiotype antibodies related to rena I-cel I carcinoma-
associated antigen G250. Int J Cancer 56:609-614, 1994
49. Uemura H, Beniers AJM C, Okajima E, et al: Vaccination
with anti-idiotype antibodies mimicking a renal cell carcinoma-
associated antigen induces tumor immunity. Int J Cancer
56:555-561, 1994
50. Van de Briol RJ, De Weger RA, Van Lovcren G LH, et al:
Two specific T cell factors that initiate immune responses
against muri ne tumor allografts. A comparison of biologic
functions. J Immunol 143:66-73. 1989
51. Van Loveren GLH, Den Otter W, Maede R, et al: A role
for mast cells and the vasoactive amine serotonin in T-cell
dependent immunity to tumors. J Immunol 134:1294-1299,
1985
52. Parmentier HK, Van de Briel RJ, Garssen J, et al:
Antigen-specific T-cell factors, in Roit IM, Delves PJ (eds):
Encyclopedia of Immunology. London, England, Saunders, pp
125-127, 1991
53. Uemura H, Okajima E, Dehruyne FMJ, et al: Immuniza
tion with anti-idiotype monoclonal antibodies bearing the
internal image of the renal cell carcinoma-associated antigen
G25Û induces specific cellular immune responses. Int J Cancer«
(in press)