Embed Size (px)
Citation preview

Clinical Insights: Diuretics and Aldo Blockade versus Potassium and Renal Function
Paul J. Hauptman MD, FHFSA
University of Tennessee Graduate School of Medicine
Knoxville TN

Disclosures
• Data Safety and Monitoring Committee: REDUCE LAP HF Randomized Trial (Corvia Medical); CAPACITY-HF (Ironwood)
• Clinical Events Committees: CardioMEMS Post-Marketing study (St. Jude Medical), ANTHEM HFrEF-2 (LivaNova)
• Speaker’s Bureau: none
• Consultant: Relypsa, Array Biopharma
• Remuneration from Heart Failure Society of America as editor of the Journal of Cardiac Failure

Additional Disclosures
• I am not certain what the title means
• Talks about diuretics tend to be boring
• Aldosterone blockade remains an intriguing topic
• I am glad that we are all here!

A Recent Transformation…


What Other Transformations Might We See?



Given the Title of the Talk….

Objectives
• Review the current status of diuretic therapy and aldosterone blockade in HFrEF and HFpEF
• Recognize limitations of guidelines with respect to MRAs
• Assess potential complications and outstanding clinical questions associated with the use of these agents

Where Do We Start?
• Dyspnea remains the primary symptom that patients report
• Daily weights remain one of the mainstays of outpatient disease management/monitoring

Weight and Dyspnea Correlate
Pang PS et al. Eur Heart J. 2009;30(18):2233-2240.
Dyspnea on a Likert scale and change in wt at day one in the
EVEREST trial

Weight and Dyspnea Correlate…Not?

Lack of Weight Loss in Patients Admitted
for Acute Heart Failure
7% 6%
13%
24%
30%
15%
3% 2%
0
5
10
15
20
25
30
En
rolle
dD
isc
ha
rge
s
(<-20) (-20 to -15) (-15 to -10) (-10 to -5) (-5 to 0) (0 to 5) (5 to 10) (>10)
Change in Weight (lbs)
20%
discharged
without weight
loss or weight
gain

An Interesting Segue Way to Vegetarianism
• From the New Yorker


prescribing diuretics

Loop Diuretics: Not Going Anywhere
• Generally isotonic urine
• Cause neurohormonal upregulation
• Implicated in cardiorenal syndrome
• Can exacerbate hyponatremia if simultaneous free water intake

Ann Intern Med. 1985 Jul;103(1):1-6.Acute vasoconstrictor response to intravenous furosemide in patients with chronic congestive heart failure. Activation of the neurohumoral axis.Francis GS, Siegel RM, Goldsmith SR, Olivari MT, Levine TB, Cohn JN.
The Complexity of Loop Diuretics:An Acute Vasoconstrictor Effect
• Classic Paper • Remarkable findings“Hemodynamic and neurohumoral responses to acute diuretic therapy were measured in 15 patients with severe HF given intravenous furosemide, 1.3 ± 0.6 (SD) mg/kg body weight. --Left ventricular pump function deteriorated by 20 minutes, as indicated by a fall in stroke volume index (27 ± 8 to 24 ± 7 mL/min · m2 body surface area, p < 0.01) and an increase in left ventricular filling pressure (28 ± 7 to 33 ± 9 mm Hg, p < 0.01). --Increases occurred in HR, MAP (90 ± 15 to 96 ± 15 mm Hg, p < 0.01), SVR, PRA, plasma NE level and plasma AVP level. --During the next 3.5 hours the patients had diuresis (2085 ±1035 mL) and the expected fall in filling pressure (28 ± 7 to 22 ± 10 mm Hg, p < 0.01). Neurohumoral indicators also returned toward the control levels.”

Gottlieb SS et al. Circulation. 2002;105:1348–1353.
Diuretic Therapy Results in a Significant Decline in Glomerular Filtration Rate
Glomerular Filtration Rate (GFR) was estimated using a 7-hour creatinine clearance
-25
-20
-15
-10
-5
0
5
10
15
0 500 1000 1500 2000 2500
Cumulative Urine Output, 0–8 h (mL)
Placebo
80 mg IV Furosemide
GF
R (
% c
han
ge)
N = 16 patients with NYHA III CHF
Mean EF = 28%

Fortunately or Unfortunately, We Have To Mention DOSE
• 2x2 Factorial Design
• High (2.5x home dose, IV) versus Low (home dose, IV) Dose and Bolus versus Intermittent administration

DOSE Study Findings
• Primary endpoint: Patient Global Assessment at 72h:
NS difference
• Primary safety endpoint: Change in serum creatinine at 72h:
Intermittent: +0.05, Continuous: +0.07
Low dose: +0.04, High dose: +0.08
• Death, rehospitalization, ED visit at 60 days
NS difference between the groups

DOSE StudyLow dose (combined continuous and intermittent), n=151
High dose (combined continuous and intermittent), n=157
P-value
Congestion(% free)
11 18 0.09
∆ Weight(lbs)
-6.1 -8.7 0.01
Net Volume
3575 4899 0.001
∆NT-proBNP(pg/ml)
-1194 -1882 0.06
Cr>0.3mg/dl increase
14 23 0.04

Markers of Decongestion: Analysis from DOSE
• % reduction in NT-proBNP was significantly associated with symptom relief (r=0.13, P = 0.04)…. but weight loss or net fluid loss were not
Kociol et al, Circ HF 2013

Markers of Decongestion: Analysis from DOSE
• Favorable changes in each of 3 markers of decongestion were associated with improvement in time to death, re-hospitalization or ED visit at 60 days– Weight per 4 lbs. weight lost: HR 0.91 (95% confidence interval 0.85,
0.97)
– Fluid loss per 1000ml: HR 0.94 (0.90, 0.99)
– NT-proBNP per 10% reduction: HR 0.95 (0.91, 0.99).
– Patients with 2 or 3 markers of decongestion (above the median value for each marker) had improved clinical outcomes versus those with 0 or 1 marker above the median value (39.0% versus 53.8%; P=0.03)
Kociol et al, Circ HF 2013

Kociol et al, Circ HF 2013

How Do We Measure Decongestion?
If We Can’t Define It, We Can’t Measure It
If We Can’t Measure It, We Can’t Assess Diuretic Dosing

How Do We Measure Decongestion?
If We Can’t Define It, We Can’t Measure It If We Can’t Measure It, We Can’t Assess Diuretic Dosing
• Physical Exam and symptoms • CXR• Reduction in BNP or NT-proBNP• Weight loss• Hemoconcentration• Serum Osmolality• Urinary Biomarkers / Lytes• IVC diameter• Intrathoracic Impedence or similar measures• Invasive hemodynamic monitoring

“Cardio-Renal Syndrome”: Simplified
Three contributors
• Loop diuretic leads to neurohormonal upregulation, worsening vasoconstriction, decreased blood flow and renal hypoperfusion
• Low cardiac output (“forward failure”)
• Increased central / renal venous pressure (“backward failure”)
But when is an increase in creatinine a “good thing” and when is it not?
A major clinical challenge during ADHF admissions

Loop Diuretic Resistance: Potential Mechanisms
1. Decreased renal function
2. Reduced and delayed peak concentrations of loop diuretics in the tubular fluid
3. Postdiuretic salt retention with waning of diuretic effect
4. Compensatory hypertrophy of epithelial cells downstream from the thick ascending limb

Loop Diuretic Resistance: Response
1. Diuretic-free time
-Marinate in Milrinone (™ pend) or vasodilator -Consider aquaretic in hyponatremic patients
2. Torsemide over furosemide / bumetanide for right heart failure with ascites
3. Thiazide (zaroxolyn, diuril pre treatment)

Are Loop Diuretics Harmful?
• Beware the study that says yes
– Lack of control for severity of disease (residual confounding)

Key Points about Diuresis
1. Monitor electrolytes
2. Consider use of torsemide if there is significant right sided failure
3. There is no difference between bumetanide and furosemide except potency (not efficacy)
4. In patients with HFrEF: don’t stamp out all peripheral edema. This is especially true in the elderly

Key Points about Diuresis
5. In patients with HFpEF: don’t stamp out all peripheral edema. This is especially true in the elderly.
(a) Preload dependence?
(b) Vigilance in salt restriction is reasonable
6. In patients with restrictive CMP: Ditto!

Intravenous Fluid during ADHF Admissions
• PREMIER data, n=131,430, IVF in 1st 2 days (13,806, 11%), 80% NS for a median of 1L (must have received at least 500cc).
IVF + IVF - Risk-Adjustedhospitalization outcomes (HR)
Critical care admit 5.7 3.8 1.57
Intubation 1.4 1.0 1.46
Dialysis 0.6 0.3 2.04
In-hospital death 3.3 1.8 2.02
Bikdeli et al JACC HF2015:3:127-33

Ultrafiltration: Another Way to Remove FluidThe UNLOAD Trial

Costanzo, M. R. et al. J Am Coll Cardiol 2007;49:675-683
Primary Efficacy and Safety End Points
Not a treatment for hyponatremia

Timing of UF
• Prefer to reserve for patients with anasarca for whom volume removal is not successful with loop diuretic ± low dose inodilator
• It’s invasive and associated with a risk of infection / vascular complications

Fluid and Salt Removal can be Low Cost and Fun

JCF 2018;24:204

JCF 2018;24:205

A Good Bowl of Soup….Can “Beat” a Loop Diuretic and Sauna Every Time!

ACEi/ARB, ARNI, MRA from 50,000 Feet
NYHA Class Pivotal studies Guidelines
ACEi/ARB I,II,III, IV CONSENSUS CHARMSOLVD (2) Val-HeFTSAVE HEALLHOPEEUROPAPEACE
ACC/AHA 2013ACC/AHA/HFSA 2017
ARNI II, III PARADIGM ACC/AHA/HFSA 2017
MRA II, III, IV RALESEPHESUSEMPHASIS
ACC/AHA 2013

Effect of MRAs in Patients with HFrEF

ACCF/AHA Guidelines for MRAs
• Class I HFrEF indications:
EF ≤0.40 Post MI with HF or DM
EF ≤0.35, NYHA 2-4 with cr ≤ 2.5 (M), ≤2.0 (F), cr cl >30, K< 5.0• NYHA 2 if prior CV hospitalization and/or
elevated BNP

ACCF/AHA Guidelines

MRA Dose Adjustment Recommendations in the Guidelines
• Dosing based on eGFR and serum potassium
• Efficacy of lower doses not tested in clinical trials

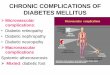
Rates of Hyperkalemia Are Higher inPatients on MRA in Clinical Practice
1. Pitt B, et al. N Engl J Med. 1999;341(10):709-717.2. Zannad F, et al. N Engl J Med. 2011;364(1):11-21.3. Shah KB, et al. J Am Coll Cardiol. 2005;46(5):845-849.4. Bozkurt B, et al. J Am Coll Cardiol. 2003;41(2):211-214.
2 2.5
6
12
0
2
4
6
8
10
12
14
RALES EMPHASIS Shah 2005 Bozkurt 20031
Clinical Trials Clinical Practice
n=822 n=1364 n=840 n=104 2 3 4
Pat
ien
ts (
%) K+ ≥ 6.0

MRAs and HFpEF
TOPCAT
ALDO HF

Entry Criteria and Outcomes in TOPCAT
• “Heart Failure” and EF ≥45%
• Either HF hospitalization in the prior 12 months; or BNP ≥100pg/ml or NT-proBNP ≥360 pg/ml within 60 days. Exclude: cr ≥2.5mg/dl or estimated GFR<30ml/min per 1.73m2 BSA
• Primary outcome: composite of CV death, aborted cardiac arrest, HFH



Were patients randomized to spironolactone taking it? Data from
the TOPCAT Biorepository substudy (206 from US/Canada and 160 from Russia)
Pfeffer et al NEJM 2017

Edelmann et al. JAMA 2013;309:781-791
• N=422 with EF ≥50, HF symptoms, ≥ stage I DD or AF, peak VO2≤25
• Spironolactone 25mg v placebo for 12 weeks
• Endpoints: • ∆E/e’: minor difference
• Peak VO2: no difference
• MWHFQ: no difference
• ∆LVMi: reached statistical difference
• ∆NT-pro BNP: reached statistical difference

Edelmann et al. JAMA 2013;309:781-791
E/e’ Peak VO2

Edelmann et al. JAMA 2013;309:781-791
LVMi NT-proBNP

Wojciech et al. JACC 2016;68:1824-1834
• N=150, EF>50%, exertional E/e’>13 (if E/e’ betw 8-15: other echo parameters or elevated NT-proBNP.
• Spironolactone 25mg vs. placebo
• Endpoint: 2.9 ml/kg/min vs. 0.3 ml/kg/min increase in peak VO2
• Endpoint: Reduction in exercise-induced increase in E/e’
“Spironolactone may be appropriate for patients with elevated LV filling pressure induced by exercise…”

Berbenetz and Mrkobrada BMC 2016;16:246 1-10
Multiple Meta-analyses
• Different number of included studies
• Different inclusion criteria between studies
• Different definitions of HFpEF

Meta Analysis-1
• 14 randomized controlled clinical trials, which included 6,428 patients with HFpEF or myocardial infarction with preserved ejection fraction, MRA therapy (Chen et al 2015)• reduced the number of hospitalizations for HF by 17%
• improved diastolic function
• induced a reversal of cardiac remodeling
• no decrease in all-cause mortality

Meta Analysis-2
• 16,321 patients from 15 randomized controlled trials (Berbenetz2016)
• MRA therapy led to a decreased risk of cardiovascular death, all-cause mortality, and cardiac hospitalizations in subjects with HFrEF but these benefits were not demonstrated in patients with HFpEF.

Chen et al. BMC 2015;13:10 1-12

Chen et al. BMC 2015;13:10 1-12

Chen et al. BMC 2015;13:10 1-12

Proposal
• Use of aldosterone antagonists may be appropriate for carefully selected patients with HFpEF who have clinical heart failure, increased BNP, evidence for elevated left atrial pressures, and lower risk for renal dysfunction or hyperkalemia.
• More study is needed!

High Dose MRA during ADHF Admission:ATHENA
• Acute effect of high dose spironolactone (100mg) v placebo or 25mg on NT-proBNP daily for 96h in patients admitted for ADHF
• No significant difference in the log NT-proBNP reduction between the two groups.
• Similar changes in GFR and potassium

Serum Potassium: Laboratory Monitoring During Initiation of MRAs in Patients with HF
• Evaluation of 10,443 Medicare Beneficiaries with HF and incident MRA therapy
• 91.6% of patients had a serum 1st measured in the 120 days prior to MRA initiation
• However only 13.3% had guideline suggested appropriate measurement of [K+] in the early (1-10 days) follow up period; 29.9% in the 11-90 days after MRA initiation
• Overall, 55% of patients did not receive any monitoring of [K+] in the early post initiation period and 22.3% did not receive any monitoring of [K+] during the extended follow-up period
Cooper L.B et alJAMA 2015;314:1973-5

Key Points about MRAs
• Spironolactone or eplerenone clearly play a role in symptomatic HFrEF and in patients early post MI with HF or diabetes
• Role in HFpEF is still debated but it is not unreasonable to consider spironolactone. This recommendation will likely change depending on the outcome of PARAGON and EMPEROR-Preserved (and similar SGLT-2 inhibitor studies).

In Summary…
• Talks about diuretics and mineralocorticoid receptor antagonists are like the ocean on Amelia Island: always changing but always the same!
• Have fun at this meeting…it’s mandatory!

Thank You

END OF TALK