Embed Size (px)
Citation preview
35
Bulletin of Prosthetics ResearchBPR 10-34 (Vol . 17 No . 2) Fall 1980Pages 35—45
M . PATR!ohunnUnnAv Ph . D.
ChiefKinesiology Research LaboratoryVeterans Administration Medical
Center, 5000 West National AvenueWood, Wisconsin 53193
Clinical Prof . of Physical TherapyMarquette University
Prof . of AnatomyMedical College of Wisconsin
SUSAN B . SEPIC, B .S.GEnmKx . GARDNER .B.S.LOUISE A . xoOLuNGB0.B.S.
Research Physical TherapistsVeterans Administration Medical
Center, Wood, Wisconsin
aThis investigation was supported in partby U. S. Public Health Service GrantNo . 13854 from the National Institute ofArthritis, Metabolism, and DigestiveDiseases, and bvtheRvhabxitahvnEn-gineering Research and DevelopmentService, Veterans Administration .
~~~~~~ .~~ ~~~~~~~~~~ of Above-Knee
Amputees~~ Patterns
«~~~`~.~0
~~~K~ Constant-Friction,~ . .~~
Knee Components a
ABSTRACT
Quantitative measurements of multiple simultaneous gaitcomponents for both free-speed and fast walking of 10 activeabove-knee amputees with constant-friction knee componentsare presented and compared with standards of normal variabil-ity . In addition, interrelationships between the various gait ab-normalities are identified.
INTRODUCTION
Constant-friction knee components for above-knee amputeeshave been on the market for many years and are still prescribedand worn by many amputees . Several advances in artificialknee components have been made since the development ofthe constant-friction knee, and future designs of artificial limbswill most certainly improve on those available now.
Other investigators have documented selected aspects of thegait of above-knee amputees (1-10) . This paper documents aev-eral previously unreported patterns of motion of the lowerlimbs and the trunk of above-knee amputees using prostheseswith constant-friction knee components . In addition, the paperdescribes relationships between simultaneous displacementpatterns of multiple body segments during walking with thistype of prosthesis.
It is hoped that this information will contribute to a deeperunderstanding of the pathomechanics of amputee locomotion,and will ultimately result in improvements in the design andprescription of artificial limbs and in the rehabilitation processof the amputee.
METHODS
The gait of 10 men with unilateral above-knee amputationswas studied . In all cases the amputation was the result oftrauma . The average age of these men was 41 years (range 33to4Oyeoru) ; the height, 177 cm (range 169 to 187 cm) ; and theweight, 79 kg (range 69 to 85 kg) . Each man had worn a pros-thesis with a constant-friction knee component for several yearsand wore the limb every day . Half of the amputees had suctionsuspension and the other half had pelvic band suspension . Fitand alignment were checked and considered satisfactory . Sixhad a SACH foot, and four had a single-axis ankle and either awooden foot orm wooden foot with compressible heel and toe .
36
MURRAY at al . : GAIT PATTERNS OF AK AMPUTEES
Six had an extension aid on the prosthetic kneeand four did not . The constant-friction device ineach case had been set for free speed, and wasnot altered . None of the amputees had any otherconcomitant disability.
Reflective targets were secured to specific ana-tomic landmarks and to the prosthesis . An inter-rupted-light technique was used to photograph theserial displacements of the targets in the sagittaland transverse planes as the men walked at acomfortable speed (free speed) and at a fast speed(11) . The target images were photographed at arate that varied from 15 to 30 exposures per sec-ond, depending on the walking speed of the sub-ject.
The following measurements were made fromthe photographs : velocity ; stride and step lengths;stride widths ; foot angles ; stance, swing and dou-ble-limb-support durations ; patterns of aagi1tal ro-tation of the shoulder, elbow, hip, knee and ankle;patterns of vertical, lateral and forward motion atthe head and neck ; and patterns of vonLiool dis-placement of the heel and toe . To quantitate irreg-ularity in forward progression, a velocity indexwas calculated : this index was the ratio of the for-ward velocity during prosthetic swing to the for-ward velocity during sound swing . Thus a velocityindex of less than 1 .00 indicated slower forwardmovement during prosthetic than during soundswing.
The measurements of the amputees were com-pared to measurements of normal men (12-14). At-test was used to assess the significance of thedifferences between the measurements oftheam-putees andthe normal men.
Stride dimensions and temporal components
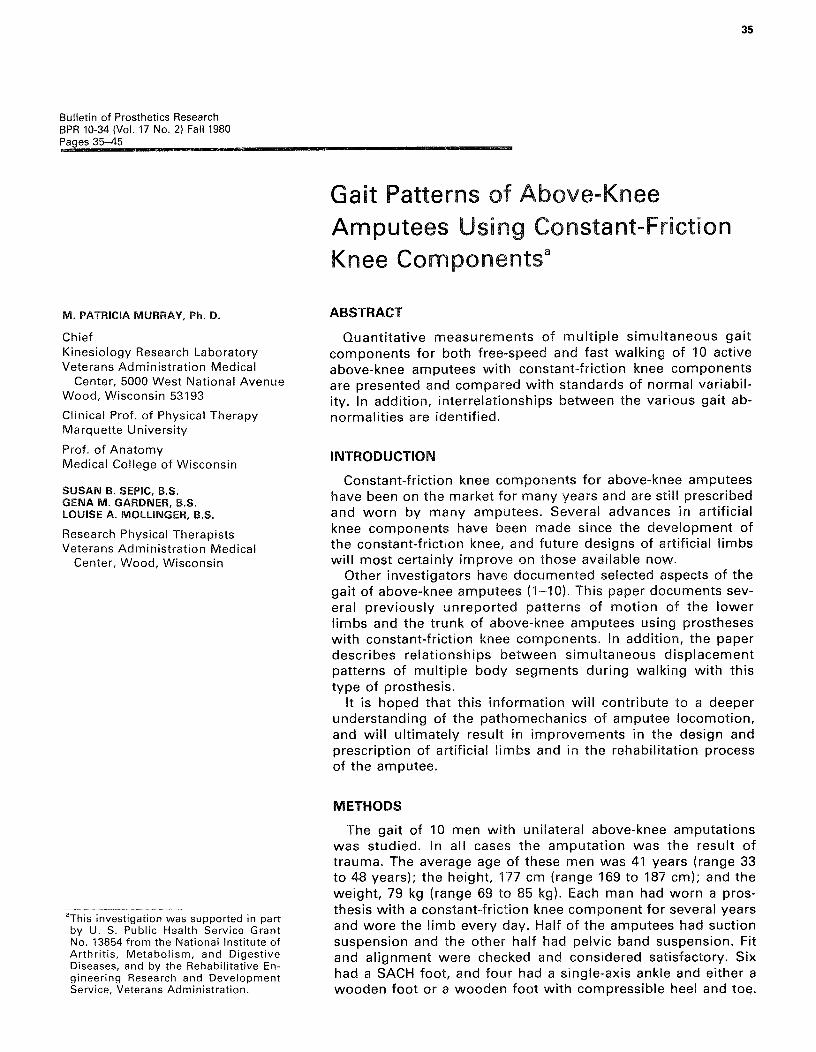
Table I contains the means and standard devia-tions of the measurements of velocity, stride di-mensions, and stance and swing durations for theamputees, and indicates the significance of the dif-ferences between the measurements of the am-putees and the normal men . The mean walkingspeed of the amputees was about two-thirds thatof norrnal men for both free-speed walking andfast walking . The amputees' subnormal velocitywas mainly due to their longer cycle durations(thus slower cadences) although their stride lengthsalso tended to be subnormal . This is illustrated inFigure 1, which shows that the stride lengths ofmost of the individual amputees were within the
TABLE IVelocity, stride dimensions and temporal components
FREE FAST
Walking speed (cm/sec)Amputees 100±16° 140±25°Normal men 151 ±20 218 ±25
Cycle duration (sec)Amputees 1 .38±]1° 1 .18 ± .11°Normal men 1 .0U± .09 .87 ± .06
Cadence (steps/min)Amputees 87 ± 7* 102 ± 9*Normal men 113 ±10 138 ±10
Stride length (cm)Amputees 136 ±15** 184±22fNormal men 150±13 188±18
Step length (cm)
Sound 04±8° 81 ±12**Prosthetic 72 ±8 83 ±11fNormal 78 ±7 93 ± 9
Stride width (cm)Amputees 17.4 ±3.6* 18.3 ±4.3°Normal men 7 .7 ±3.5 9 .1 ±4.1
Foot angles (deg)Sound 10.S±72 10.2 ±5.8tProsthetic 2.3 ± 5 .0 2 .1 ±4.6Normal 8.3±5J 5.3 ±5.5
Stance Phase (sec)Sound .94±J2° .78 ± .09*Prosthetic .80 ± .07° .62 ± .08*Normal .65 ~ .07 49± .05
Swing Phase (sec)Sound .43± .04 .41 .
.O4tProsthetic .58 ± .00° .58± .04°Normal .41 ± .04 .38 ± .03
Double-Limb Support (sec).11 ± .03**1st in cycle .20 ± .06**
2nd in cycle .17± .04°° .10 ± .04tNormal .12 ±- .03 .06 -1- .03
*The amputees were significantly different from normal
limits of nonnol variability, while the individua!values for velocity and cadence tended to be near

37
Bulletin of Prosthetics Research BPR 10-34 (Vol . 17 No . 2) Fall 1980
NORMAL MEAN ± 2 S .D.X INDIVIDUAL A-K AMPUTEES
VEL CITY — cm/sec
200 -
xxxxx xx 0
x
100-x
0-
STRIDE LENGTH - cm
100 -
0-
FAST SPEED
FIGURE 1.The free-speed and fast-walking ve-locities, cadences, and stride lengthsof 10 individual amputees areshown by "x"'s . The vertical barsbisected by a hollow circle repre-sent the mean and 2 standard de-viations above and below the meanfor 30 normal men.
the lower threshold of normal variability . Stridelength (expressed in percent of stature) averaged77 percent for the amputees as compared to 89percent for normal men during free-speed walkingand averaged 93 percent for the amputees as com-pared to 106 percent for normal men during fastwalking.
In contrast to the walking of normal men, whosesuccessive step lengths are remarkably equal inlength, the successive step lengths of the ampu-tees were uneven during free-speed walking, andto a lesser degree during fast walking (Table I) . Atfree speed all of the men—and at fast speed most
of the men—took a longer step when the pros-thetic limb was directed forward.
The stride widths of the amputees were abnor-mally wide. Their foot angles were different fromthose of normal men in that, on an average, theirsound foot was in about eight degrees more out-toeing than the foot on the side of the prosthesis(Table I).
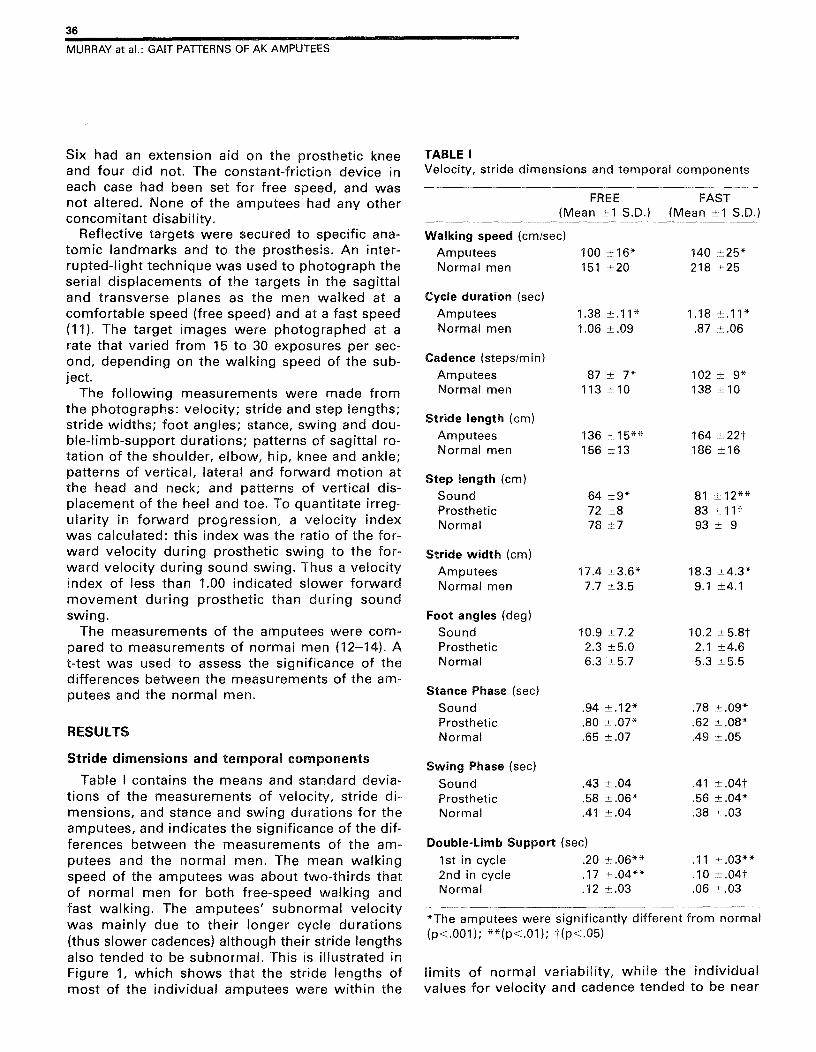
In normal men, the successive stance phases ofthe right and left limbs are approximately equal induration as are the successive swing and double-limb-support phases . In the amputees at bothwalking speeds, the duration of the sound stancephase was longer than the duration of the pros-thetic stance phase, but the duration of the soundswing phase was shorter than the duration of theprosthetic swing phase . The average inequalitiesin successive stance and swing phases, as ex-pressed in percent of the walking-cycle time, aregraphed in Figure 2.
Displacement patterns of the lower limbs
The mean patterns of hip flexion-extension areshown in Figure 3 . Unlike normal, the pattern ofmotion of the hip on the prosthetic side was char-acterized by immediate and continuous hip exten-sion beginning with the onset of prosthetic stance.In addition, the amputees' hip pattern on the pros-thetic side was abnormal in that there was a sharprather than gradual reversal from extension toflexion midway through the walking cycle, andthis sharp reversal occurred just after sound heel-strike. These two characteristics were observed in8 of the 10 amputees . The average total excursionof hip motion used on the prosthetic side wasslightly less than that used on the sound side, andthe residual hip of the amputees usually did notextend as much as the sound hip . The pattern ofmotion of the sound limb on figure 3 and subse-quent graphs is shifted to the right compared tothe pattern of normal men because the stancephase of the sound limb comprised 66 to 69 per-cent of the cycle duration, depending on walkingspeed, as compared to 57 to 61 percent for normalmen.
The mean patterns of flexion-extension of theknee are shown in Figure 4 . The patterns for theprosthetic knee illustrate two abnormalities char-acteristic of all of the amputees : the absence ofthe yielding knee flexion that normally occurs dur-ing the early stance phase ; and secondly, contin-ued knee extension during the last 5 percent of thecycle, particularly at fast walking, when knee ex-
200 -
100-
0-
160-
80-
0-
200 -
100 -
0-
X X X Xx
X x x x
FREE SPEED
XxXxxXxX xx
160 -
80 - Xx XXXXX xx
x
0-
CADENCE - steps/min
xx XXx
xx
x X x
200 -
xx
x
38
MURRAY at al . : GAIT PATTERNS OF AK AMPUTEES
FREE-SPEED WALKING 30 NORMAL MEN
10 A-K AMPUTEES
NORMAL `EFTRIGHT
PROSTHETIC
SOUND
FAST-SPEED WALKING
NORMAL `EFTRIGHT
STANCE 57%
~'iiliYii`OM .STANCE 57%
PROSTHETICSOUND
I
I
I
'
'
1
10.4
0 .6
0.8
1 .0
1 .2
1 .4
1 .6
SECONDS
I
I0
0.2
FIGURE 2.Average stance and swing dura-tions during free-speed and fastwalking for the sound and pros-thetic limbs of 10 above-knee am-putees with constant-friction kneecomponents (which are adjusted forfree speed) and for the left and rightlimbs of 30 normal men . The num-bers within the timing bars expressthe stance and swing durations inpercent of the walking cycle dura-tions .
NORMAL MEAN ± 2 S .E.-- SOUND LIMB, 10 A-K AMPUTEES PROSTHETIC LIMB
1
I
1
I
I
I
I
180 100
0
20 40 60 80 100
PERCENT OF CYCLE
PERCENT OF CYCLE
2
-H POX FREE SPEED
0
Nww 60
C9w
80 —
2Oz 100 —
wI- t 1 txw 20 40 60
FIGURE 3.Mean patterns of hip flexion-exten-sion for the sound and prostheticlimbs of 10 above-knee amputeeswith constant-friction knee compo-nents, during free-speed and fastwalking . The shaded areas repre-sent 2 standard errors above andbelow the mean for 30 normal men.The ordinate scale values representthe anterior angle between the lat-eral thigh target (from hip center toknee center) and a lateral pelvic tar-get (from anterior superior iliacspine to posterior superior iliacspine).
This and other graphs originate atfoot contact.

39
Buoemn of Prosthetics Research BPR 10-34 (Vol . 17 No . 2) Fall 1980
KNEEq• 80
w
FREE SPEED 80 —
60 -
\\\n
40 ~
\\ 20-
FAST SPEED
/`
40 60 80 100
/
*zu▪ O 0
z
!m
.~--rxuu
0 20 40 60 80 100
0 20
60.~
.
~
~
u* /
«
/w !
0
//mir
4O-
w• !
o
//o ! U //
/
NORMAL MEAN ±z S.E.
–SOUND LIMB, 10 A-K AMPUTEES
PROSTHETIC LIMB
FIGURE 4.Mean free-speed and fast walkingpatterns of knee flexion-extensionfor the sound and prosthetic limbsof ten above-knee amputees withconstant-friction knee components.The shaded areas represent twostandard errors above and belowthe mean for thirty oormal men.Zero degrees represents full kneeextension.
PERCENT OF CYCLE
PERCENT OF CYCLE
tension normally is decelerating preparatory toheel-strike . In addition, the mean pattern of theprosthetic knee shows near-normal flexion duringthe swing phase at free-speed walking—but exces-sive flexion during the swing phase during fastwalking . That excessive knee flexion during swingat fast walking was not characteristic of all of theamputees but instead was related to the relativeamount of friction of the knee component, to thespeed of reversal from hip extension to flexion, orto the adjustment of the extension aid.
Figure 5 shows the mean patterns of the verticaltrajectories of the hael and toe during free-speedand fast walking . During free-speed walking, peakheel rise was similar for the sound and prostheticlimbs. During fast walking, the average patternsshow that prosthetic heel-off occurred earlier thannormal and peak prosthetic houl rise was exces-sive. The toe-floor clearance distance was also ex-cessively high for the prosthetic side during theswing phase, particularly during fast walking . Inaddition, the descent of the toe after heel-strikewas slower than normal for the prosthetic side.
The mean patterns of dorsiflexion and plantarflexion of the sound ankle of the amputees ascompared to those of normal men are shown inFigure 6 . During free-speed walking the amputeesused less than norrnol dorsiflexion during thesound stance phase . During fast walking the meanpattern was different from normal in that therewas an abnormally early reversel into plantar flex-ion during the mid-stance phase. This type ofab-
NORMAL MsAm± oacSOUND LIMB . 10 A-K AMPUTEES
- PROSTHETIC LIMB
VERTICAL DISPLACEMENT OF THE HEEL
FREE SPEED
FAST SPEED40
40-
30-
20-
lo
".o20 m60 810 100
o20 41 0 610 8'0 100PERCENT OF CYCLE
PERCENT OF CYCLE
VERTICAL DISPLACEMENT OF THE TOE40-
FREE SPEED
40-FAST SPEED
30-
20-
p snoswro p cvcLE
PERCENT OF CYCLE
FIGURE 5.Mean vertical pathways of the heel and toe of the prostheticand sound limbs during free-speed and fast walking for tenabove-knee amputees with constant-friction knee components.The shaded areas represent two standard errors above andbelow the mean for the thirty normal men . Zero centimetersrepresents the !evol of the floor .
/»
°
O .-Tr
0-0 20 40 60 80 100 0 20 40 60 80 100
lo
o
30-
20-
30-
20-

40
MURRAY at al . : GAIT PATTERNS OF AK AMPUTEES
NORMAL MEAN It 2 S .E.--- SOUND LIMB, 10 A-K AMPUTEES
FREE SPEED
FAST SPEED
0 20 40 60 80 100
0 20 40 60 80 100
PERCENT OF CYCLE
PERCENT OF CYCLE
FIGURE 6.Mean pattern of dorsiflexion andplantar flexion of the sound anklefor ten above-knee amputees dur-ing free-speed and fast walking . Theshaded area represents two stund'p,d errors above and below themean for thirty no,mal men . Theordinate scale values represent theanterior angle between targets onthe lateral leg and heel of the shoe.
_
120
ANKLE
80--
100 v
80 —
oo-
b
normality was observed in seven of the amputeesduring fast walking and in two during free-speedwalking . Excessive plantar flexion at the end of thestance phase was observed at both walking speeds,and was typical of the sound ankle of all of theamputees.
The arm swing patterns of the amputees variedconsiderably from one subject to another . In gen-eral, the arm swing of the amputees was abnormalin that there was usually less shoulder and elbowmotion on the prosthetic than on the sound side.There were seldom step-related reversals of thedirection of motion at the elbow . The diminishedexcursions of arm swing by the amputees weremainly due to subnormal flexion at the shoulderand subnormal extension at the elbow for mostamputees.
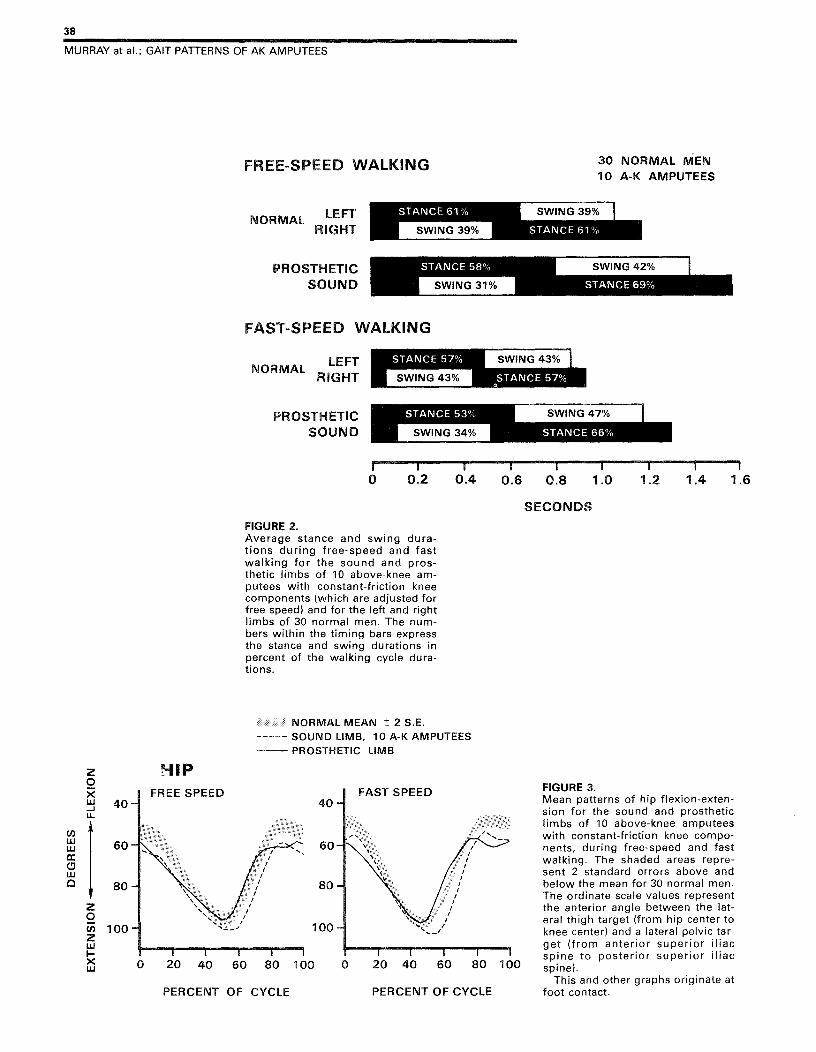
The patterns of vertical, !oteral and forward mo-tion at the head are illustrated in Figure 7 . The pat-terns of vertical displacement for the amputeesshow asymmetrical peaks rather than the twosymmetrical peaks typical of normal walking . Thepeak during prosthetic stance was subnormal atboth walking speeds, and the peak during soundstance (prosthetic swing) was in excess of normalduring fast walking . The amputees had excessive!ateral deviation of the head and trunk toward theprosthetic side during prosthetic stance, and this!atenal deviation was more pronounced during free-speed than fast walking . For free-speed walkingthe mean !oterol excursion measured at the headwas 11 .6 ±1 .0 b cm for the amputees as comparedto a mean value of 5 .9 ±0.3 cm for normal men of
One standard error of the mean .
comparable ages . For fast walking, the mean ex-cursion of !ateral motion measured at the headwas 10.2 ±0 .7 cm for the amputees as comparedto 5 .0 ±0.4 cm for normal men. For normal men,the forward displacement pattern indicates thatforward motion as measured at the head and neckis remarkably uniform . In contrast the amputeesmoved forward more rapidly during the prostheticsingle-limb-support phase than during the prum-thetioovving phase .'
In Table 2, nurnerionl data are given for themeasured gait factors which relate to smoothnessand symmetry in walking . All of the measure-ments of the amputees were significantly differentfrom normal . Increases in speed from free-speedto fast walking were accompanied by improve-ment in the ratio of successive step lengths but bygreater inequality in successive vertical excursionsof the head . Both the swing ratios and the irregu-lar forward motion of the head (velocity index)were similar for both free-speed and fast walking.
DISCUSSION
Study of the data presented suggests that thegait abnormalities of the amputees are ones whichensure safety and compensate for the problemsinherent in walking with an artificial limb . Al-though these compensatory maneuvers seem toserve an important function, the maneuvers per semust increase the nnechanicol energy cost of walk-ing for the amputee. While the exact relationshipbetween nnoohaniool and metabolic energy ex-
cForward displacement in Figure 7 represents variation aboutthe average forward velocity .
41
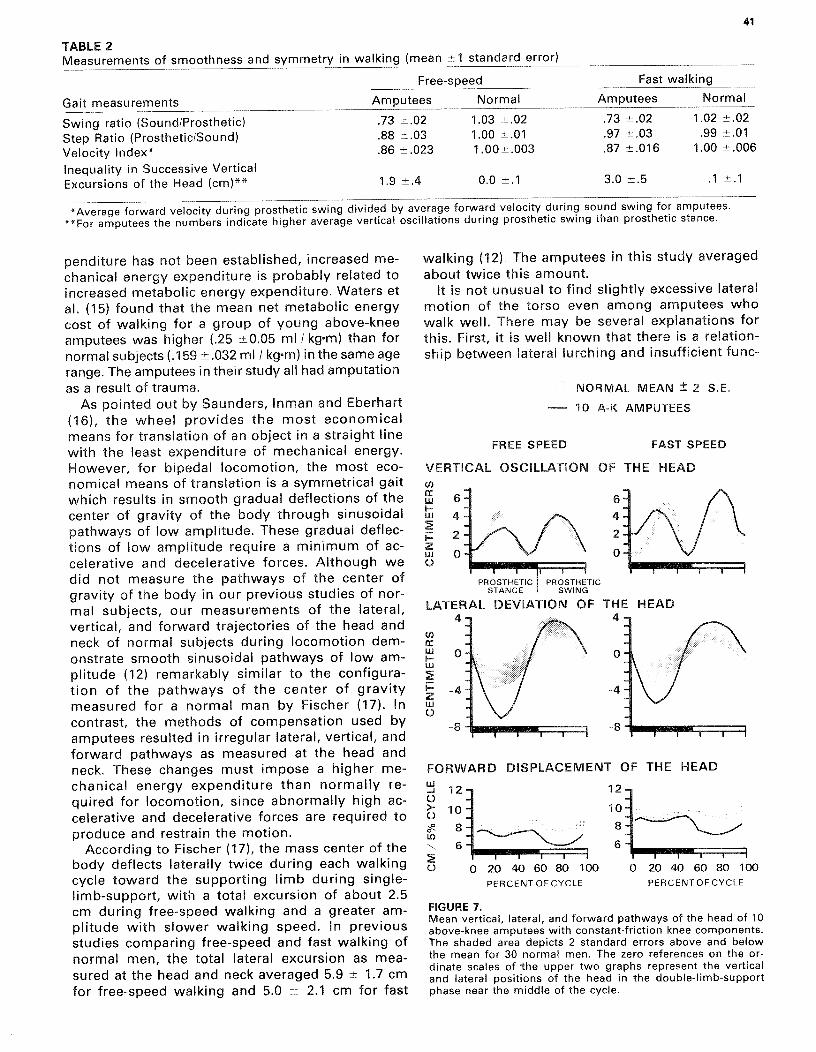
TABLE 2Measurements of smoothness and symmetry in walking (mean ±1 standard error)
Free-speed
Fast walking
Gait measurements
Amputees
Normal
Amputees
Normal
Swing ratio (Sound/Prosthetic)
.73 ±- .02~U2
1 .03 ~ .02
.73 ± .02
1 .02 ±- .02~U~
Step Ratio (Prosthetic/Sound)
.88 ± .03
1 .00 -11- .01
.97 ± .03
.99± .01
Vo!ouhy!nd*x°
.86± .023
1 .00± .003
.87 ± .016
1 .00 ± .006
Inequality in Successive VerticalExcursions of the Head (cm)**
1 .9 ± .4
0 .0 ±1
3 .0 :L- .5
] ~1
*Average forward velocity during prosthetic swing divided by average forward velocity during sound swing for amputees.**For amputees the numbers indicate higher average vertical oscillations during prosthetic swing than prosthetic stance.
penditure has not been established, increased me-chanical energy expenditure is probably related toincreased metabolic energy expenditure . Waters etal . (15) found that the mean net metabolic energycost of walking for a group of young above-kneeamputees was higher ( .25 1E0 .05 rn\/kg~nn) than fornormal subjects ( .159 ± .032 mlml! kgm) in the same agerange. The amputees in their study all had amputationas a result of trauma.
As pointed out by Saunders, Inman and Eberhart(16), the wheel provides the most economicalmeans for translation of an object in a straight linewith the least expenditure of mechanical energy.However, for bipedal locomotion, the most eoo-nornioal means of translation is a symmetrical gaitwhich results in smooth gradual deflections of thecenter of gravity of the body through sinusoidalpathways of low amplitude . These gradual deflec-tions of low amplitude require a minimum of ac-celerative and decelerative forces . Although wedid not measure the pathways of the center ofgravity of the body in our previous studies of nor-mal subjects, our measurements of the lateral,vertical, and forward trajectories of the head andneck of no/rnal subjects during locomotion dem-onstrate smooth ainuuoidml pathways of low am-plitude (12) remarkably similar to the configura-tion of the pathways of the center of gravitymeasured for a norrnal man by Fischer (17) . Incontrast, the methods of compensation used byamputees resulted in irregular lateral, vertical, andforward pathways as measured at the head andneck. These changes must impose a higher rne-chanioal energy expenditure than normally re-quired for locomotion, since abnormally high ac-celerative and decelerative forces are required toproduce and restrain the motion.
According to Fischer (17), the mass center of thebody deflects laterally twice during each walkingcycle toward the supporting limb during single-limb-support, with a total excursion of about 2 .5cm during free-speed walking and a greater am-plitude with slower walking speed . In previousstudies comparing free-speed and fast walking ofnorrnal men, the total !etorel excursion as mea-sured at the head and neck averaged 5 .9 ± 1 .7 cmfor free-speed walking and 5 .0 ± 2 .1 cm for fast
walking (12) . The amputees in this study averagedabout twice this amount.
It is not unueuol to find slightly excessive lateralmotion of the torso even among amputees whowalk well . There may be several explanations forthis. First, it is well known that there is a relation-ship between lateral lurching and insufficient func-
NORMAL MEAN ± 2 S .E.
— 10 A-K AMPUTEES
FREE SPEED
FAST SPEED
VERTICAL
cc
-uj6 -I-
-Lu 4+
-2
z
-Lup
PROSTHETIC PROSTHETICSTANCE
SWING
LATERAL DEVIATION OF THE HEAD
FIGURE 7.Mean vertical, lateral, and forward pathways of the head of 10above-knee amputees with constant-friction knee components.The shaded area depicts 2 standard errors above and belowthe mean for 30 no,m p l men. The zero references ontheor-dinate scales of the upper two graphs represent the verticaland !um,ol positions of the head in the double-limb-supportphase near the middle of the cycle.
0 20 40 60 80 100
0 20 40 60 80 100
PERCENT OF CYCLE
PERCENT OF CYCLE
-
DISPLACEMENT OF THE HEAD
12-
10- -8-
_
e
FORWARD
2

42
MURRAY at al . : GAIT PATTERNS OF AK AMPUTEES
tion of the hip abductor muscles (18) . For the am-putees, even with concentration of weightbearingon the medial aspect of the posterior brim of thesocket, and with a properly-sloped lateral wall ofthe p,ontheoio, the hip abductor muscles of the re-sidual limb are at a mechanical disadvantage ascompared to the hip abductor muscles of a normallimb. In normal men this abductor muscle force isapplied with the foot firmly fixed to the floor byfriction, but when the amputees contract their ab-ductor muscles during prosthetic single-limb sup-port, the femur does not provide a fixed lever armsince it must first compress the soft tissues of the!eteral thigh before purchase is obtained againstthe !eteral wall . Secondly, the hip abductor mus-cles normally undergo a lengthening contractionduring single-limb-support to control the descentof the pelvis on the opposite side where the limbis in the swing phase (19) . If the amputees allowednornnal descent of the pelvis on the sound sideduring the prosthetic single-limb-support phase,they would experience discomfort from compres-sion of the soft tissue below the conjoint ramus ofthe pubis and ischium.
The excessive !otarul trunk motion of the am-putees may also relate to their abnormally widestrides, which may be caused by the presence ofthe medial wall of the socket . Regardless of thecause, these increased stride widths no doubt in-crease !atarol stability . Evidently the gain in sta-bility and comfort is worth the increased energyexpenditure associated with the excessive lateralmotion of the trunk during prosthetic single-limbsupport.
Fischer described the vertical pathways of thecenter of gravity as undulating through two peaksand two valleys of similar amplitude during eachwalking cycle, and the total excursion ranged from3 .4 to 4.4 cm, depending on speed . The valleysoccur during double-limb support and the peaksoccur during single-limb support . The configura-tion of the vertical pathways of normal men asmeasured at the head are identical to those cal-culated by Fischer, but the totel excursions aver-age 5.1 ± 1 .0 cm for free-speed walking and 6 .5± 1 .5 cm for fast walking, and the successive ver-dool excursions within each walking cycle are ofremarkably similar amplitude (12).
The amputees differed from normal in that theydid not have equal successive peaks or equal suc-cessive valleys in their vertical excursions . Thevalley, during double-limb support when the pros-thetic limb was forward, tended to be higher than
FAST WALKING
NORMAL msAm± 2 S .D.— AMPUTEE
VAULT
QUASI-VAULTSOUND ANKLE
AMPUTEE PI
AMPUTEE #6
AMPUTEE Pl
AMPUTEE #6
30-
20 -
m+
20
40
60
80
100PERCENT OF CYCLE
FIGURE 8.Patterns of ankle motion and of thevertical pathway of the heel of thesound limb for above-knee ampu-tees #1 and #6 (solid lines) and themean pathways ±2 standard devia-tions for 30 normal men (shadedarea) during fast walking . The pat-terns of amputee #1 (on the left)show marked premature plantarflexion and heel rise (arrows) whichwould be easily recognized asvaulting by a trained observerwatching for abnonnal vouioal os-cillation of the body and prematureheel rise. The premature plantarflexion and heel rise of #6 was mildand could be called quasi-vaulting.
the valley when the sound limb was forward—par-ticularly during fast walking . This may have re-lated to the fact that the prosthetic knee must befully extended at heel-strike, while normal kneesduring fast walking are flexed at heel-strike . Therelatively lower peak during prosthetic single-limbsupport may relate to the fact that the amputeestended to incline their trunks laterally and forwardat that time, or to the fact that the prosthetic limbwas often slightly shorter than the sound limb.The relatively higher peak during the sound stancephase (prosthetic swing phase), particularly for
-di 2ix X0 1210 u.
0
xm
20
40
6'0
80
100 0
20
6'0
8'0
SOUND HEEL40
20
410
6'0
40PERCENT OF CYCLE
o 00
43
Bulletin of Prosthetics Research BPR 10-34 (Vol . 17 No . 2) Fall 1980
PROSTHETIC
SOUND
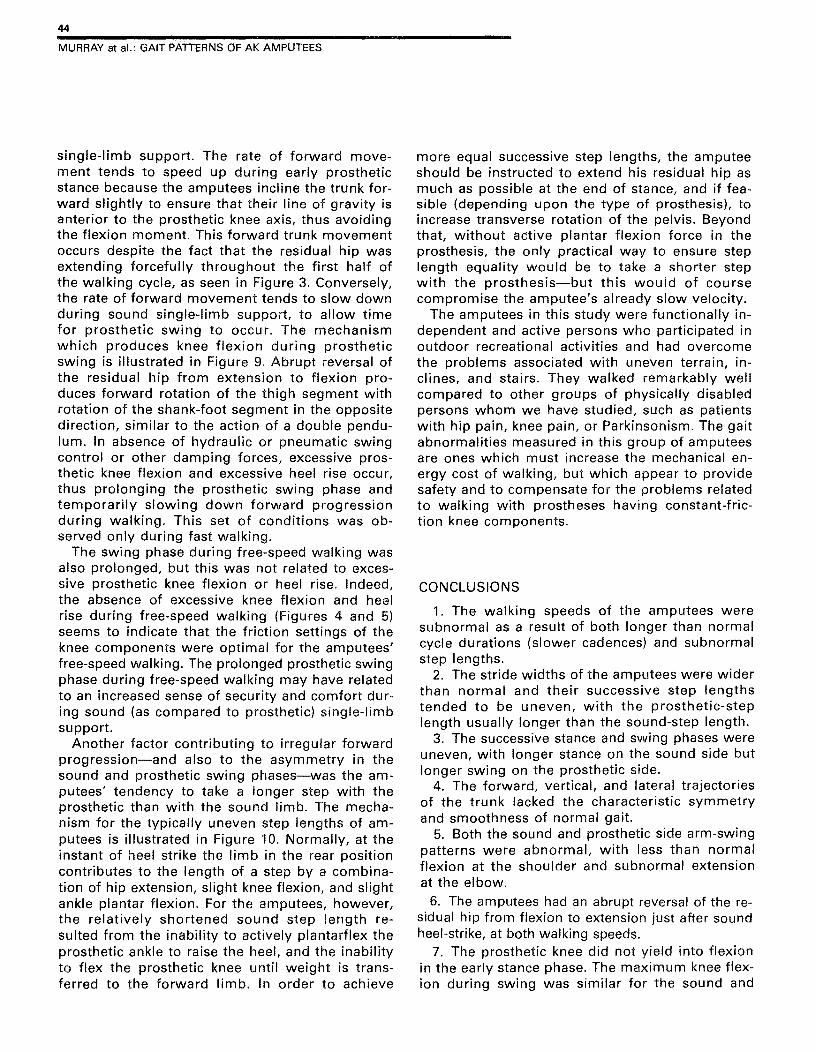
FIGURE 10.Diagrams of an amputee at sound andprosthetic heel strike illustrating that therelatively longer step is taken when theprosthetic limb is forward . The length ofthe step taken by the sound limb (leftdiagram) is limited by the inability ofthe amputee to actively plantar flex theprosthetic ankle and safely flex theprosthetic knee.
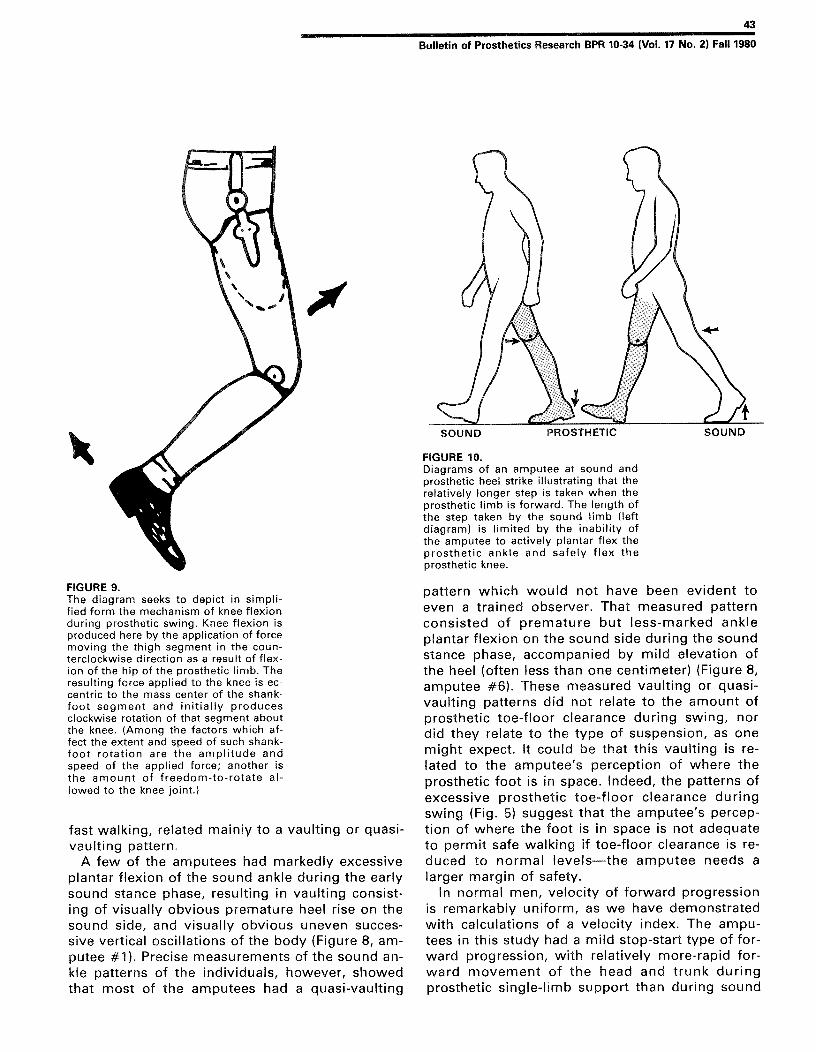
FIGURE 9.The diagram seeks to depict in simpli-fied form the mechanism of knee flexionduring prosthetic swing . Knee flexion isproduced here by the application of forcemoving the thigh segment in the coun-terclockwise direction as a result of flex-ion of the hip of the prosthetic limb . Theresulting force applied to the knee is ec-centric to the mass center of the shank-foot segment and initially producesclockwise rotation of that segment aboutthe knee. (Among the factors which of-fnmtxo extent and speed of such shank-foot rotation are the amplitude andspeed of the applied force ; another isthe amount of freedom-to-rotate al-lowed
fast walking, related mainly to a vaulting or quasi-vaulting pattern.
A few of the amputees had markedly excessiveplantar flexion of the sound ankle during the earlysound stance phase, resulting in vaulting consist-ing of visually obvious premature heel rise on thesound side, and visually obvious uneven succes-sive vertioal oscillations of the body (Figure 8, unn-puiee#1) . Precise measurements of the sound an-kle patterns of the individuals, however, showedthat most of the amputees had a quasi-vaulting
pattern which would not have been evident toeven a trained observer . That measured patternconsisted of premature but less-marked ankleplantar flexion on the sound side during the soundstance phase, accompanied by mild elevation ofthe heel (often less than one centimeter) (Figure 8,amputee #6) . These measured vaulting or quasivau!ting patterns did not relate to the amount ofprosthetic toe-floor clearance during swing, nordid they relate to the type of suspension, as onemight expect . It could be that this vaulting is re-lated to the amputee's perception of where theprosthetic foot is in space . Indeed, the patterns ofexcessive prosthetic toe-floor clearance duringswing (Fig . 5) suggest that the amputee's percep-tion of where the foot is in space is not adequateto permit safe walking if toe-floor clearance is re-duced to normal levels—the amputee needs alarger margin of safety.
In normal men, velocity of forward progressionis remarkably uniform, as we have demonstratedwith calculations of a velocity index . The ampu-tees in this study had a mild stop-start type offor-ward progression, with relatively more-rapid for-ward movement of the head and trunk duringprosthetic single-limb support than during sound
44
MURRAY at al . : GAIT PATTERNS OF AK AMPUTEES
single-limb support . The rate of forward move-ment tends to speed up during early prostheticstance because the amputees incline the trunk for-ward slightly to ensure that their line of gravity isanterior to the prosthetic knee axis, thus avoidingthe flexion moment . This forward trunk movementoccurs despite the fact that the residual hip wasextending forcefully throughout the first half ofthe walking cycle, as seen in Figure 3 . Conversely,the rate of forward movement tends to slow downduring sound single-limb support, to allow timefor prosthetic swing to occur . The mechanismwhich produces knee flexion during prostheticswing is illustrated in Figure 9 . Abrupt reversal ofthe roaiduel hip from extension to flexion pro-duces forward rotation of the thigh segment withrotation of the shank-foot segment in the oppositedirection, similar to the action of a double pendu-lum . In absence of hydraulic or pneumatic swingountrol or other damping forces, excessive pros-thetic knee flexion and excessive heel rise occur,thus prolonging the prosthetic swing phase andtemporarily slowing down forward progressionduring walking . This set of conditions was ob-served only during fast walking.
The swing phase during free-speed walking wasalso prolonged, but this was not related to exces-sive prosthetic knee flexion or heel rise . Indeed,the absence of excessive knee flexion and henlrise during free-speed walking (Figures 4 and 5)seems to indicate that the friction settings of theknee components were optimal for the amputees'free-speed walking . The prolonged prosthetic swingphase during free-speed walking may have relatedto an increased sense of security and comfort dur-ing sound (as compared to prosthetic) single-limbsupport.
Another factor contributing to irregular forwardprogression—and also to the asymmetry in thesound and prosthetic swing phases—was the am-putees' tendency to take a longer step with theprosthetic than with the sound limb . The mecha-nism for the typically uneven step lengths ofarn-puteoa is illustrated in Figure 10 . Normally, at theinstant of hnel strike the limb in the rear positioncontributes to the length of a step by a combina-tion of hip extension, slight knee flexion, and slightankle plantar flexion . For the amputees, however,the relatively shortened sound step length re-sulted from the inability to actively plantarflex theprosthetic ankle to raise the heel, and the inabilityto flex the prosthetic knee undl weight is trans-ferred to the forward limb . In order to achieve
more equal successive step lengths, the amputeeshould be instructed to extend his residual hip asmuch as possible at the end of stance, and iffao-nib!o (depending upon the type of prosthesis), toincrease transverse rotation of the pelvis . Beyondthat, without active plantar flexion force in theprosthesis, the only practical way to ensure steplength equality would be to take a shorter stepwith the prosthesis—but this would of coursecompromise the amputee's already slow velocity.
The amputees in this study were functionally in-dependent and active persons who participated inoutdoor recreational activities and had overcomethe problems associated with uneven terrain, in-clines, and stairs. They walked remarkably wellcompared to other groups of physically disabledpersons whom we have studied, such as patientswith hip pain, knee pain, or Parkinsonism. The gaitabnormalities measured in this group of amputeesare ones which must increase the rnoohanioal en-ergy cost of walking, but which appear to providesafety and to compensate for the problems relatedto walking with prostheses having constant-fric-tion knee components.
CONCLUSIONS
1. The walking speeds of the amputees weresubnormal as a result of both longer than normalcycle durations (slower cadences) and subnormalstep lengths.
2. The stride widths of the amputees were widerthan normal and their successive step lengthstended to be uneven, with the prosthetic-steplength usually longer than the sound-step length.
3. The successive stance and swing phases wereuneven, with longer stance on the sound side butlonger swing on the prosthetic side.
4. The forward, vertical, and lateral trajectoriesof the trunk lacked the characteristic symmetryand smoothness of normal gait.
5. Both the sound and prosthetic side arm-swingpatterns were abnormal, with less than norrnelflexion at the shoulder and eubnnrrnal extensionat the elbow.
6. The amputees had an abrupt reversal of the re-sidual hip from flexion to extension just after soundheel-strike, at both walking speeds.
7. The prosthetic knee did not yield into flexionin the early stance phase . The maximum knee flex-ion during swing was similar for the sound and
45
Bulletin of Prosthetics Research ~R 10-34 (Vol. 17 No . 2) Fall 1980
prosthetic limbs during free-speed walking, butthe prosthetic knee had excessive flexion duringthe swing phase for fast walking.
8. The prosthetic heel rise was excessive whenprosthetic knee flexion was excessive.
9. The toe-floor clearance distance of the pros-thetic foot was in excess of normal, particularlyduring fast walking.
10. During fast walking, the sound ankle of mostamputees had a premature revoraol into plantarflexion during mid-stance.
References
1. Bresler, Boris, Charles W . Radcliffe,and F .R . Berry : Energy and Power inthe Legs of Above-knee AmputeesDuring Normal Level Walking . SeriesII, Issue 31, Lower-Extremity AmputeeResearch Project, University of Cali-fornia, Berkeley, 1957.
2. Cappozzo, A ., F. Figura, T . Leo, andM . Marchetti : Biomechanical Evalua-tion of Above-knee Prostheses . In oio-moohaniusY .A. P . V . Komi (ed .), Bal-timore, University Park Press, 366-372,1976.
3. Eberhart, Howard o, Herbert Elft-man, and Verne T . Inman : The Locommor Mechanism of the Amputee . In:Human Limbs and Their Substitutes,P . E . Klopsteg and P . D . Wilson (eds .),New York, McGraw-Hill, 472-480, 1954.
4. Fishman, Sydney, Edward Peizer,Hector W. Kay, L . Aldubi, and D.Wright : Metabolic Measures in theEvaluation of Prosthetic and OrthoticDevices : A Progess Report . No . 115 .28,Adult Prosthetic Studies Research Di-vision, College of Engineering, NewYork University, New York, 1962.
5. Godfrey, C . M ., A . T . Jousse, R . Brett,and J . F . Butler : A Comparison ofSome Gait Characteristics With SixKnee Joints . Orthotics and Prosthet-ics, 29(3) : 33-38, 1e75 .
.6. James, Urban and Kurt Oberg : Pros-
thetic Gait Pattern in Unilateral Above-Knee Amputees . Scand . J . Rehab.Med., 5o5-50' 1973.
7. Murphy, Eugene F. : The Swing Phaseof Walking with Above-Knee Pros-theses . Bull . Prosth . Res ., 10-1, Spring1964, 5-39.
8. Peizer, Edward, Henry F . Gardner, and4nmonvStanm : Selection and Appli-cation of Knee Mechanisms. Bull.Prosth . Res ., 10-18, Fall 1972, 90-158.
9. Radcliffe, Charles W . : InformationUnof ! in the Design of Damping Mech-anisms for Artificial Knee Joints . Series3, Issue 13, Prosthetic Devices ResearchProject, University of California, Berke-ley, 1950.
10. Zuniga, Efrain N ., Lewis A . Leavitt,Jon C. Calvert, Joseph Canzoneri, and
Charles R . Peterson : Gait Patterns inAbove-Knee Amputees . Arch . Phys.Med. Rehab ., 53 :373-382, 1e72.
11. Murray, M . Patricia, A. BenjaminDrought, and Ross C . Kory : WalkingPatterns of Normal Men . J . Bone &Joint Surg ., 46-A(2) :335-360, 1964.
12. Murray, M. Patricia, Ross C . Kory,Bertha H . Clarkson, and Susan B . Sepic:Comparison of Free and Fast SpeedWalking Patterns of Normal Men . Am.J . Phys . Med ., 45(1) :8-24, 1966.
13. Murray, M . Patricia, Susan B . Septic,and Elliott J . Barnard : Patterns o/swe
ina! Rotation of the Upper Limbs inWalking . Phys . Ther. ' 47(4) :272-284,1967.
14. Murray, M . Patricia and Bertha H.Clarkson : The Vertical Pathways of theFoot During Level Walking . 1xm . Phys.Thor . Assoc ., 46(6) :585-599, 1966.
15. Waters, Robert L .Helen Hislop, Jac-quelin Perry, dDaniel Antonelli : En-ergetics:Management of Locomotor Disabili-ties . Orth . Clinics of N . Amer .,8(2) :351-377 ' 1978.
16. Saunders, J . B . DeC. M., Verne T.Inman, and Howard D . Eberhart : TheMajor Determinants in Normal andPathological Gait . J . Bone Joint Surg .,35-A13> :543-558 ' 1953.
17. Fischer, Otto : Der Gang desMenschen, II Tex . DieG*xammmchwmnpunmouunu moxus-se,nKmfto .Abxvndid . Math .-Phys . CI.Sachs . Gesellsch . vwssenvux,un :l-l63,1899.
18. Steindler, Arthur : Kinesiology of theHuman Body . Springfield, III . CharlesC Thomas, 1955.
19. Eberhart, Howard D ., Verne T . Inman,J . B . DeC . M. Saunders, A . S . Levens,Boris8n,o!or, and T . D . McCowan : Fun-damental Studies of Human Locomo-tion and Other Information Relating tothe Design of Artificial Limbs . A reportto the National Research Council, Com-mitte on Artificial Limbs, Berkeley,University of California, 1947 .





























