Embed Size (px)
Citation preview

Patrick C. D'Haese Patrick C. D'Haese
Faculty of Medicine Faculty of Medicine University of Antwerp, BelgiumUniversity of Antwerp, Belgium
Controversies in the hyperphosphataemia treatment. Are there alternatives?
Slide show design: Dirk De Weerdt

Introduction (1)Introduction (1)
• Hyperphosphataemia in end-stage renal disease (ESRD) dialysis patients is an important contributor to morbidity and mortality

1.00
1.25
1.50
1.1–4.5 4.6–5.5 5.6–6.5 6.6–7.8 7.9–16.9Serum phosphorus quintile (mg/dL)
Rel
ativ
e m
orta
lity
risk
1.00 1.001.02
1.18*
1.39†
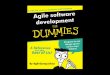
Elevated serum phosphorus increases mortality risk (1)Elevated serum phosphorus increases mortality risk (1)
*P = 0.03; †P < 0.0001 (n = 6407)Note: 1 mmol/L = 3.1 mg/dL
Block GA et al. Am J Kidney Dis 1998;31:607–17.

Elevated serum phosphorus increases mortality risk (2)Elevated serum phosphorus increases mortality risk (2)
Rel
ativ
e ris
k of
CV
dea
th
Serum phosphorus concentration (mmol/L)
0.97 1.03 1.00
1.52* 1.55†
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
1.80
<1.1 1.1–1.3 >1.81.3–1.5 1.5–1.8
Ref
*P < 0.005; †P < 0.0005 (n = 4544)Note: 1 mmol/L = 3.1 mg/dL
• Nowadays up to 70% of end-stage renal failure patients have hyperphosphatemia• Phosphate control has not improved over the last 2 decades

Achieving multiple K/DOQI targetsAchieving multiple K/DOQI targets
0
10
20
30
40
50
60
PTH Ca × PCa P All 4 targets
70
% o
f pat
ient
s ac
hiev
ing
targ
et
27
5144
8
62 n = 3540
Kim J et al. J Am Soc Nephrol 2003;14:269A.
K/DOQI targets

Elevated serum phosphorus increases mortality risk (2)Elevated serum phosphorus increases mortality risk (2)
Rel
ativ
e ris
k of
CV
dea
th
Serum phosphorus concentration (mmol/L)
0.97 1.03 1.00
1.52* 1.55†
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
1.80
<1.1 1.1–1.3 >1.81.3–1.5 1.5–1.8
Ref
*P < 0.005; †P < 0.0005 (n = 4544)Note: 1 mmol/L = 3.1 mg/dL
• Nowadays up to 70% of end-stage renal failure patients have hyperphosphatemia• Phosphate control has not improved over the last 2 decades

Achieving multiple K/DOQI targetsAchieving multiple K/DOQI targets
0
10
20
30
40
50
60
PTH Ca × PCa P All 4 targets
70
% o
f pat
ient
s ac
hiev
ing
targ
et
27
5144
8
62 n = 3540
Kim J et al. J Am Soc Nephrol 2003;14:269A.
K/DOQI targets

Control of serum phosphorus levelsControl of serum phosphorus levels
• Aluminum hydroxide
• Calcium acetate, - carbonate
• Magnesium
• Iron dextran - hydroxide
• Sevelamer HCl
• Organic non-calcium, non-aluminum containing phosphate binder
• Has good safety profile
• Lipid lowering effects
• Benificial in the progression of vascular calcifications
• Phosphate binding potency is limited
• Has been associated with acidosis
• Lanthanum carbonate

Introduction (1)Introduction (1)
• Hyperphosphataemia in end-stage renal disease (ESRD) dialysis patients is an important contributor to morbidity and mortality
• Lanthanum carbonate is a new non-calcium, non-aluminium-based phosphate binder that has been shown to effectively control serum phosphate levels in patients with ESRD

• Potent binding
• Selective= Efficacy
Important characteristics of a new phosphate binder
Lowefficacy
Highpill burden
Poorcompliance
The Vicious Cycle of
Low Efficacy
• Low systemic absorptionLow systemic absorption
• Non-toxic at therapeutic dosesNon-toxic at therapeutic doses
• Non-calciumNon-calcium

Lanthanum: the element
• Discovered in 1839 by MosanderDiscovered in 1839 by Mosander
• MW: 139 Da (2 stable isotopes)MW: 139 Da (2 stable isotopes)
• Silvery white, malleable, ductile rare earth element; occurring at Silvery white, malleable, ductile rare earth element; occurring at varying concentrations in terrestrial crust and surface water.varying concentrations in terrestrial crust and surface water.
• Tri-valent cation Tri-valent cation high affinity for phosphate high affinity for phosphate
La3+
CO32-
CO32-
CO32- La3+
PO43-
PO43-
+PO4
3-La3+
PO43-La3+
+
CO32-
CO32-
CO32-
Ks= [La3+][PO43-] = 7.08 x 10-27
= solubility constant

Introduction (2)Introduction (2)
• An extensive development programme has defined specific An extensive development programme has defined specific features of lanthanum carbonate, such as:features of lanthanum carbonate, such as:
• Potency of phosphate bindingPotency of phosphate binding
• Low pill burdenLow pill burden
•High phosphate binding at clinically relevant pH (unlike other High phosphate binding at clinically relevant pH (unlike other agents, effective before phosphate reaches small intestine)agents, effective before phosphate reaches small intestine)
•Reduced requirement for fluid intake with tabletsReduced requirement for fluid intake with tablets
•Independent control of serum phosphate and calcium levelsIndependent control of serum phosphate and calcium levels
•Compatibility with vitamin D supportCompatibility with vitamin D support
• A number of clinical trials have established effective management A number of clinical trials have established effective management of hyperphosphataemia in patients with chronic kidney disease of hyperphosphataemia in patients with chronic kidney disease
(CKD)(CKD)

Introduction (2)Introduction (2)
• An extensive development programme has defined specific An extensive development programme has defined specific features of lanthanum carbonate, such as:features of lanthanum carbonate, such as:
• Potency of phosphate bindingPotency of phosphate binding
Damment SJ & Shen V: Clin Nephrol 63: 127-137, 2005

Introduction (2)Introduction (2)
• An extensive development programme has defined specific An extensive development programme has defined specific features of lanthanum carbonate, such as:features of lanthanum carbonate, such as:
• Potency of phosphate bindingPotency of phosphate binding
• Low pill burdenLow pill burden
•High phosphate binding at clinically relevant pH (unlike other High phosphate binding at clinically relevant pH (unlike other agents, effective before phosphate reaches small intestine)agents, effective before phosphate reaches small intestine)
•Reduced requirement for fluid intake with tabletsReduced requirement for fluid intake with tablets
•Independent control of serum phosphate and calcium levelsIndependent control of serum phosphate and calcium levels
•Compatibility with vitamin D supportCompatibility with vitamin D support
• A number of clinical trials have established effective management A number of clinical trials have established effective management of hyperphosphataemia in patients with chronic kidney disease of hyperphosphataemia in patients with chronic kidney disease
(CKD)(CKD)

In VitroIn Vitro Phosphate- Phosphate-BBinding Profileinding Profile
pH 5pH 5
pH 3pH 3
pH 7pH 7 Ph
osp
ho
rus
Ph
osp
ho
rus
RRem
ove
d (
%)
emo
ved
(%
)
0
20
40
60
80
100
Lanthanumcarbonate
Calciumcarbonate
Calcium acetate Aluminumhydroxide
0
20
40
60
80
100
Lanthanumcarbonate
Calciumcarbonate
Calcium acetate Aluminumhydroxide
0
20
40
60
80
100
Lanthanumcarbonate
Calciumcarbonate
Calcium acetate Aluminumhydroxide
Damment and Webster, Damment and Webster, [Abstract]. J Am Soc Nephrol 2003; 14:204A.[Abstract]. J Am Soc Nephrol 2003; 14:204A.

Faecal excretion
p.o.p.o.
lanthanum
lanthanum
carbonate
carbonate
ESRD in dialysis
marginal lanthanum intake through
breathing and food
Faecal excretion
NORMAL RF exp.
p.o.p.o.
lanthanum
lanthanum
carbonate
carbonatemarginal lanthanum
intake through breathing and food
Kidneys not involved in excretion (<2% of injected dose)
Gastro-int. abs.
<0.002%Biliary elimination
Metabolism of Lanthanum in Humans
Kidneys not involved in excretionno increased risk for deposition in ESRD
Gastro-int. abs.
<0.002%Biliary elimination
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Day 1 Day 2 Day 3 Day 4 Day 5 Day 6(no dose)
Day 7
24h
Uri
ne
La
Exc
reti
on
(µ
g) Healthy volunteers, multiple La doses
Dose = 1 g lanthanum t.i.d.
Urinary excretion: 0.6-1.0 µg/day
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Day 1 Day 2 Day 3 Day 4 Day 5 Day 6(no dose)
Day 7
24h
Uri
ne
La
Exc
reti
on
(µ
g) Healthy volunteers, multiple La doses
Dose = 1 g lanthanum t.i.d.
Urinary excretion: 0.6-1.0 µg/day
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50
Time after dosing (days)
Cu
mu
lati
ve
% d
ose
Faeces Bile Gut transfer Urine
Faeces
Bile
Gut transfer
Urine
La excretion in rats after i.v. LaCl3 (0.3 mg/kg/day)
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50
Time after dosing (days)
Cu
mu
lati
ve
% d
ose
Faeces Bile Gut transfer Urine
Faeces
Bile
Gut transfer
Urine
La excretion in rats after i.v. LaCl3 (0.3 mg/kg/day)La excretion after single iv LaCl3 (0.3 mg/kg/day)
rats
Behets GJ et al: Curr Opin Nephrol Hypertens 13, 403-409, 2004

Plasma Plasma llanthanum anthanum cconcentrations oncentrations in din dialysis ialysis ppatients atients LLanthanum anthanum ccarbonatearbonate treatment treatment up to 3000 mg/dayup to 3000 mg/dayUSA USA pphase 2 and 3 hase 2 and 3 cclinical linical ttrialsrialsMean+SDMean+SD
3369
Lanthanum carbonateLanthanum carbonateas a phosphate binderas a phosphate binder

Introduction (2)Introduction (2)
• An extensive development programme has defined specific An extensive development programme has defined specific features of lanthanum carbonate, such as:features of lanthanum carbonate, such as:
• Potency of phosphate bindingPotency of phosphate binding
• Low pill burdenLow pill burden
•High phosphate binding at clinically relevant pH (unlike other High phosphate binding at clinically relevant pH (unlike other agents, effective before phosphate reaches small intestine)agents, effective before phosphate reaches small intestine)
•Reduced requirement for fluid intake with tabletsReduced requirement for fluid intake with tablets
•Independent control of serum phosphate and calcium levelsIndependent control of serum phosphate and calcium levels
•Compatibility with vitamin D supportCompatibility with vitamin D support
• A number of clinical trials have established effective management A number of clinical trials have established effective management of hyperphosphataemia in patients with chronic kidney disease of hyperphosphataemia in patients with chronic kidney disease
(CKD)(CKD)

Clinical programme: CompletedClinical programme: Completed
Completed Phase II/III studies Completed Phase II/III studies • 202 UK202 UK
• 204 USA204 USA
• 205 USA 205 USA 1-yr safety extension 1-yr safety extension
• 301 Parts I301 Parts I–IV–IV EU EU
• 301 Part V301 Part V–VI–VI EU 2.5-yr safety extension EU 2.5-yr safety extension
• 302 USA302 USA
• 303 EU + SA bone biopsies303 EU + SA bone biopsies
• 307 USA, SA, Poland307 USA, SA, Poland
• 308 USA 308 USA 1-yr safety extension 1-yr safety extension
• 309 USA, EU 309 USA, EU 2-yr safety extension 2-yr safety extension
• 315 Taiwan315 Taiwan
PK/PD, pharmacokinetics/pharmacodynamics;EU, Europe; SA, South Africa
Completed Phase I studiesCompleted Phase I studies• 101 UK101 UK
• 104 UK104 UK
• 105 UK105 UK
• 108 Japan108 Japan
• 109 Japan109 Japan
• 110 UK110 UK
• 111 USA 111 USA PK/PD dialysis patients PK/PD dialysis patients
• 112 UK 112 UK citrate citrate
• 113 UK 113 UK warfarin warfarin
• 114 UK 114 UK digoxin digoxin
• 115 UK 115 UK metoprolol metoprolol
• 116 UK 116 UK bioequivalence bioequivalence
• 117 UK – excretion, i.v.117 UK – excretion, i.v.
• 121 UK121 UK
3000 patients have been enrolled to date (1996–2005); 1700 have contributed to filed studies
Efficacy, safety, tolerability, pharmacokineticsComparison with placebo, calcium-based agents and other commercillay available phosphate binders

SPD405-204: Dose-ranging placebo-controlled trialSPD405-204: Dose-ranging placebo-controlled trial
Intention-to-treat (ITT; n = 144): 112 lanthanum carbonate, 32 placebo;91 patients completed double-blind phase;La = lanthanum carbonate
2-week placeborun-out
Screening
1–3-week placeborun-in
Randomization6-week double-blinded treatment
Placebo, n = 29
La 225 mg/day, n = 29
La 675 mg/day, n = 30
La 1350 mg/day, n = 26
La 2250 mg/day, n = 32

SPD405-204 (USA)SPD405-204 (USA): Evolution of serum phosphate: Evolution of serum phosphate
Difference in serum phosphate between week-in-treatment and end-of-washout (EOW) for all patients randomised
(Mean ± SD)
La 0 mg La 225 mg
La 675 mg
La 1350 mg La 2250 mg
Ch
ang
es
in s
eru
m P
(m
g/d
L)
fro
m E
OW
2
1
0
–1
–2
–3Treatment groups
Week 1Week 2Week 3Week 4Week 5
Week 6

SPD405-204: SummarySPD405-204: Summary
Results for the ITT population (Results for the ITT population (nn = 144) showed that: = 144) showed that:
• Change from baseline analysis identifies > 675 mg as Change from baseline analysis identifies > 675 mg as minimal effective doseminimal effective dose
• Serum phosphate levels are likely to be significantly Serum phosphate levels are likely to be significantly reduced within 2 weeks in patients receiving daily doses reduced within 2 weeks in patients receiving daily doses between 1350 and 2250 mgbetween 1350 and 2250 mg
• Patient compliance was good; overall mean compliance Patient compliance was good; overall mean compliance during the treatment period was 91%during the treatment period was 91%

European (202), USA (302) and Taiwan (315) clinical trials: Study designEuropean (202), USA (302) and Taiwan (315) clinical trials: Study designPlacebo-controlled, double-blind, randomized trials
• Similar inclusion/exclusion criteria
• Starting dose 375 mg/day (Europe) or 750 mg/day USA
• Maximal dose: 3000 mg/day (USA, Taiwan) or 2250 mg/day (Europe)
1–3-weekwashout
4- or 6-week dose titration
Lanthanum carbonate (4 weeks)
Placebo (4 weeks)
Doses of lanthanum carbonate incrementally increased to achieve target serum phosphate levels
Double-blind, parallel-group phase

European study (202)European study (202)
P < 0.0001
Time (weeks)
Titration period (all patients)
Placebo
Lanthanumcarbonate
Hutchison AJ et al. Nephrol Dial Transplant 2004;19:1902–6
–1 0 1 2 3 4 5 6 7 8
8
7
6
5
4
Ser
um
ph
osp
hat
e (m
g/d
L)
Pre-dosing Randomized treatment
Titration phase

Control of serum phosphateControl of serum phosphate European (202), USA (302) and Taiwan (315) clinical trialsEuropean (202), USA (302) and Taiwan (315) clinical trials
• Results demonstrate similar efficacy in different Results demonstrate similar efficacy in different populationspopulations
• Doses of lanthanum translate to low pill burden Doses of lanthanum translate to low pill burden
• New formulations of 750 and 1000 mgNew formulations of 750 and 1000 mg
• 3 pills per day, 1 pill per meal3 pills per day, 1 pill per meal
• Patient compliance was good in all three studiesPatient compliance was good in all three studies
• Mean compliance over double-blind period: Mean compliance over double-blind period:
• 87% (USA)87% (USA)
• 91% (Europe)91% (Europe)
• 95% (Taiwan)95% (Taiwan)

Part 66
months
European study (301): DesignEuropean study (301): DesignProspective, randomized, multicentre, open-label, comparative trial
Weeks of treatment
–3 –1 0 5 25 48 178
Enrollment
Washout
La treatment group (n = 510)
Titration phase
Maintenance phase
Open-label extension
Optional extension phase
Ca treatment group (n = 257)
Part 13
weeks
Part 25
weeks
Part 36
months
Part 46
months
Part 52
years
154

European study (301): European study (301): Serum phosphate levelsSerum phosphate levels
Ser
um
ph
osp
hat
e (m
mo
l/L)
Comparator-controlled trial
1.5
1.0
0.5
0.00
Weeks on treatment
La
Ca
Hutchison AJ. Nephron Clin Pract 2005;100:c8–19; Hutchison et al. Poster presented at the 40th ERA–EDTA World Congress of Nephrology, Berlin, Germany, 2003
2.5
3.0
2.0
3.5
1 2 3 4 5 9 13 17 21 25 29 41 45 4933 37
Modal dose of lanthanum carbonate: 1500 mg/day
Modal dose of calcium carbonate: 3000 mg/day
Switched to La

European study (301): Ca European study (301): Ca P P
Hutchison AJ. Nephron Clin Pract 2005: 100:c8–19
P = 0.961
P = 0.009
P = 0.061
1.0
1.2
1.4
1.6
1.8
2.0
End of titration (Week 5)
Mid-maintenance (Week 17)
End of maintenance (Week 25)
Mea
n C
a x
P r
educ
tion
(mm
ol2 /
L2 )
Study phase
La
Ca

Reduction in incidence of hypercalcaemiaReduction in incidence of hypercalcaemia
• Hypercalcemic episodes (>ULN)
• 6% of lanthanum carbonate-treated patients
• 38% of calcium carbonate-treated patients (P <0.001)
• Hypercalcemia reported as an adverse advent
• 0.4% of lanthanum carbonate-treated patients
• 20.2% of calcium carbonate-treated patients
Hutchison AJ et al. Nephron Clin Pract 2005;100:8–19

US study (307):US study (307):Open-label trial, randomized, parallel group active comparator trial USA, Porto Rico & South-Africa
Screening, then 1–3-week
washout
1–3 weeks 6 weeks 2 years
Standard therapy
Lanthanum carbonate
RandomizationEnd of titration
Finn WF et al. Presented at the 37th Annual Meeting of the ASN, St Louis, MO, USA, 2004
N= 677
N= 682

US study (307):US study (307): Serum phosphate levels Serum phosphate levels (mean ± 95% CI)(mean ± 95% CI)
Finn WF et al. Presented at the 37th Annual Meeting of the ASN, St Louis, MO, USA, 2004
La
Std
Ser
um p
hosp
hate
(m
g/m
L)
Study week Study month
5
6
7
8
1 7 14 26 52 14 18 20 22 240
9

US study (307):US study (307): Median serum PTH levels during the study Median serum PTH levels during the studyS
erum
PT
H (
pg/m
L)
Study week Study month
3 7 26 43 52 14 16 18 20 22 2414
Std
La
Shaded area represents K/DOQI recommended range (150–300 pg/mL);Finn WF et al. Presented at the 37th Annual Meeting of the ASN, St Louis, MO, USA, 2004
100
200
250
0
150
50
300
1

SPD405-309: Long-term control of phosphate levels during lanthanum carbonate SPD405-309: Long-term control of phosphate levels during lanthanum carbonate treatmenttreatment
Ser
um p
hosp
horu
s (m
g/dL
)
0 6 12 18 24 30 36 42 48 54
2
0
4
6
8
Note: 1 mg/dl = 0.32 mmol/LWoods et al. Poster presented at the National Kidney Foundation Clinical Meeting, Washington DC, USA, 2005;
mean (± SD) serum phosphorus levels
Month
10

Lanthanum carbonate: EfficacyLanthanum carbonate: Efficacy
• 1500–3000 mg of lanthanum carbonate reduces serum phosphate levels in the majority of patients
• Treatment has been shown to control serum phosphate levels for up to 5 years
• Similar efficacy in different populations
• Rapidly lowers serum phosphate, without raising serum calcium, offering improved mineral management of ESRD
• Reduced incidence of hypercalcaemia permits optimal use of vitamin D
• Majority of trials to date have used 250- and 500-mg tablets. Use of 750- and 1000-mg tablets will further reduce the pill burden

Most common GI effects in comparative studiesMost common GI effects in comparative studies
0
5
10
15
20
25
30
35
40
Vomitin
gNau
se
a Diarrh
oea
Consti
patio
n
Per
cent
age
of p
atie
nts
A 6-month study(SPD405-301)
A 1-year study(SPD405-303)
A 2-year study(SPD405-307)
La
Ca
Hutchison AJ et al. Nephron Clin Pract 2005;100:8–19; Torres A et al. Poster presented at the 36th Annual Meeting of the ASN, San Diego, CA, 2003; Data on file
Vomitin
gNau
se
a Diarrh
oea
Consti
patio
n
Vomitin
gNau
se
a Diarrh
oea
Consti
patio
n

Open-label multicentre Open-label multicentre randomized prospective randomized prospective controlled studycontrolled studyin dialysis patientsin dialysis patients
A total of 98 patients (age 55A total of 98 patients (age 55 ± ±14.314.3 y; y; 59 males)59 males) recruited from various recruited from various dialysis centresdialysis centres in 12 countries. in 12 countries.
In 63 of them a histomorphometric In 63 of them a histomorphometric analysis of baseline analysis of baseline andand follow-up follow-up bone biopsies was performed.bone biopsies was performed.
Patients discontinued: Patients discontinued: Transplantation (n=10)Transplantation (n=10)Death (n=11)Death (n=11)
C. SWAENEPOEL
A. TORRES
A. FERREIRA
A. HUTCHISON
M. DE BROE
M. LAVILLE
H-H. NEUMAYER W. SULOWICZ
S. SULKOVA
A. BALDUCCIG. COEN
L. DJUKANOVICM. POPOVIC
S. PEJANOVIC
A. SIKOLEG. SPASOVSKI
D'Haese PC et al: Kidney Int 63 (S85): 73-78, 2003
Lanthanum carbonateas a phosphate binderLanthanum carbonateas a phosphate binderEffects on bone ?Effects on bone ?

Open-label multicentre randomized prospective controlled Open-label multicentre randomized prospective controlled study in dialysis patients: study in dialysis patients: Study DesignStudy Design
Maximal dose: Lanthanum Carbonate: 3750 mg/dayCalcium Carbonate: 9000 mg/day
D'Haese PC et al: Kidney Int 63 (S85): 73-78, 2003
3025
Lanthanum carbonateLanthanum carbonateas a phosphate binderas a phosphate binder

Lanthanum
n=33
Norm al
Adynam icbone
M ixed
Hyperpara-thyroidism
Baseline
Osteo-m alacia
Norm al
Adynam icbone
Hyperpara-thyroidism
One year
M ixed
Osteo-m alacia
Calcium
n=30
Norm al
Adynam icbone
M ixed
Hyperpara-thyroidism
Baseline
Osteo-m alacia
Norm al
Adynam icbone
Hyperpara-thyroidism
One year
M ixed
Osteo-m alacia
Open-label multicentre randomized prospective controlled study in Open-label multicentre randomized prospective controlled study in dialysis patients:dialysis patients: Results: Categorisation of bone diseaseResults: Categorisation of bone disease
2994D'Haese PC et al: Kidney Int 63 (S85): 73-78, 2003

Long-term lanthanum carbonate treatment does not adversely Long-term lanthanum carbonate treatment does not adversely affect boneaffect bone
• Data have been confirmed in a more recent study showing that compared with calcium carbonate, treatment with lanthanum carbonate for 2 years in patients with ESRD had no adverse effect on bone-cell function and activity
• Higher levels of PTH, osteocalcin and bone-specific alkaline phosphatase in the lanthanum carbonate group suggest an improved bone turnover
• No evidence of aluminum-like effects on bone could be demonstrated in neither study
Behets GJ et al. Kidney Int 67:1830–1836; D'Haese PC, et al. Kidney Int Suppl 2003;85:s73–8;
Malluche et al. Poster presented at the NKF Clinical Meeting, Washington, DC, USA, 2005; Freemont AJ, Denton J. Poster presented at the 41st Congress of the ERA-EDTA, Lisbon, Portugal, May 2004

Lanthanum bone Lanthanum bone concentration after arrest of concentration after arrest of drugdrug1 year treatment1 year treatment,, 22 years follow up years follow up
Spasovski GB et al, submitted 2005
3431
Lanthanum carbonateLanthanum carbonateas a phosphate binderas a phosphate binder

Long-term lanthanum carbonate treatment does not adversely Long-term lanthanum carbonate treatment does not adversely affect boneaffect bone
• Data have been confirmed in a more recent study showing that compared with calcium carbonate, treatment with lanthanum carbonate for 2 years in patients with ESRD had no adverse effect on bone-cell function and activity
• Higher levels of PTH, osteocalcin and bone-specific alkaline phosphatase in the lanthanum carbonate group suggest an improved bone turnover
• No evidence of aluminum-like effects on bone could be demonstrated in neither study
Behets GJ et al. Kidney Int 67:1830–1836; D'Haese PC, et al. Kidney Int Suppl 2003;85:s73–8;
Malluche et al. Poster presented at the NKF Clinical Meeting, Washington, DC, USA, 2005; Freemont AJ, Denton J. Poster presented at the 41st Congress of the ERA-EDTA, Lisbon, Portugal, May 2004

Lanthanum bone Lanthanum bone concentration after arrest of concentration after arrest of drugdrug1 year treatment1 year treatment,, 22 years follow up years follow up
Spasovski GB et al, submitted 2005
3431
Lanthanum carbonateLanthanum carbonateas a phosphate binderas a phosphate binder

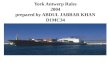
No evidence of toxicityNo evidence of toxicity
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6
Years on Treatment
Bo
ne
La
nth
an
um
(u
g/g
) w
et
wt.
Highest concentrationtested in animals (90ug/g)
No Toxicity
15 year projectionAll absorbed drug into bone
No clearance (46ug/g)
Damment et al, 2004. JASN, 15, 271A (Abstract F-P0948). Studies LAM-IV-301, LAM-IV-303 and LAM-IV-307
Bone lanthanum levels in treated ESRD patients
Lanthanum carbonateLanthanum carbonateas a phosphate binderas a phosphate binder

Localization of Aluminum in Osteomalacic BoneLocalization of Aluminum in Osteomalacic Bone
AluminonAluminon®® Staining Staining

Principle of X-ray fluorescence
ESRF - The European Synchrotron Radiation Facility, Grenoble
Typical X-ray fluorescence spectrum of bone sample
Behets GJ et al: Kidney Int 67: 1830-1836, 2005
Extremely low La levels require sensitive detection methods Extremely low La levels require sensitive detection methods
Deposition of lanthanum Deposition of lanthanum in bonein bone

Normal boneNormal bone
Lanthanum is located on the outer edge of calcified boneLanthanum is located on the outer edge of calcified bone
Deposition of lanthanum Deposition of lanthanum in bonein bone
Behets GJ et al: Kidney Int 67: 1830-1836, 20053275
Rats loaded with 2000 mg/kg/day lanthanum carbonate for 12 weeksRats loaded with 2000 mg/kg/day lanthanum carbonate for 12 weeks

Lanthanum localization is independent of the presence or Lanthanum localization is independent of the presence or amount of osteoid, in animals with a mineralization defectamount of osteoid, in animals with a mineralization defect
3275Behets GJ et al: Kidney Int 67: 1830-1836, 2005
Rats loaded with 2000 mg/kg/day lanthanum carbonate for 12 weeksRats loaded with 2000 mg/kg/day lanthanum carbonate for 12 weeks
Deposition of lanthanum Deposition of lanthanum in bonein bone

LaLa
LaLa
LaLa
LaLa
LaLa
LaLa
LaLa
LaLa
LaLaLaLa
LaLa
LaLa
LaLa
LaLa
LaLa
Possible mechanisms of lanthanumPossible mechanisms of lanthanum deposition in bone deposition in bone
3212
Deposition of lanthanum Deposition of lanthanum in bonein bone
Lanthanum deposition in bone couldnot be associated with a specific ultrastructural localization nor could it be associated with a particular bone lesion

Conclusions (1)Conclusions (1)
• Extensive pre-clinical and clinical trial programme
• Data from over 3000 patients treated with lanthanum carbonate
• Lanthanum carbonate has been shown to be a potent phosphate binder
• Effectively reduced serum phosphate levels in patients with ESRD
• Selective phosphate binder
• Greater phosphate-binding affinity compared to calcium and sevelamer
• Effective at clinically relevant pH range
• Lanthanum carbonate has a simple dosage regimen
• Wide range of tablet sizes available(250, 500, 750 and 1.000 mg)
• Low pill burden, as little as one tablet with each meal(3.000 mg/day or 2.250 mg/day)

Conclusions (2)Conclusions (2)
• Low systemic absorption
• Not renally excreted
• No effect of ESRD on plasma lanthanum exposure
• Deposition in bone and liver is limited. No clearcut evidence for toxic effects established so far
• Excellent non-clinical and clinical safety profiles
• Lanthanum treatment significantly reduced incidence ofhypercalcemia AEs

21/04/23
Aluminum and Lanthanum in the human bodyAluminum and Lanthanum in the human body
Aluminum Lanthanum
Phosphate binding +++ +++
Gastrointestinal absorption ++ +
Renal elimination +++ ±
Biliary elimination + +++
Interference hematopoiesis ++ –
Bone toxicity ++ –
Hypoparathyroidism + –
Encephalopathy +–