Embed Size (px)
Citation preview
Patients’ Private Property Guidelines
Patients’ Private Property Guidelines
Table of Contents
1. Policy ......................................................................................................................................................2
2. Purpose ..................................................................................................................................................2
3. Scope of application of PPP Guidelines ...............................................................................................3
4. Legislation/Other Related Policies .......................................................................................................4
5. Glossary of Terms & Definitions ...........................................................................................................5
6. Roles & Responsibilities ........................................................................................................................6
7. Guidelines ..............................................................................................................................................6
7.1 Fundamental Concepts .........................................................................................................6
7.2 Clients with Capacity .............................................................................................................6
7.3 Clients who may lack Full Capacity .......................................................................................7
7.4 HSE’s Responsibility where there are doubts around Client Capacity ...............................7
7.5 Involvement of Key Client Contacts ....................................................................................8
7.6 Appropriate Local Discretion ................................................................................................8
7.7 Clients Funds versus HSE Funds ............................................................................................8
7.8 Assessment of Client’s Capacity ..........................................................................................11
7.9 Application for Circuit Court Direction .............................................................................12
7.10 Third Party Payment of Monies ........................................................................................13
7.11 Fund and Other Property of Deceased Clients ................................................................13
7.12 Availability of information on PPP Activity .....................................................................16
7.13 Complaints & Appeals .......................................................................................................17
7.14 Support for Staff/Interpretation of PPP Guidelines ........................................................18
8. Revison & Audit ..................................................................................................................................18
9. Appendices ..........................................................................................................................................19
Appendix 1 – Procedure for Withdrawal/Payment of monies fromPatients’ Private Property Accounts in Favour of Third Parties .........................................19
Appendix 2 – Form P10 – Withdrawal/Payment from PPP to 3rd Parties ................................................23
Appendix 3 – Form P20 – Re-imbursement of Receipts ........................................................................25
Appendix 4 – FAQ, Frequently Asked Questions ..................................................................................26
Appendix 5 – Probate Forms - Declaration & Deed of Indemnity & Flow Charts ...................................29
Appendix 6 – Flowcharts & Forms .......................................................................................................39
1
Introduction
The Health Service Executive (HSE) operates in excess of15,000 Patients’ Private Property Accounts (PPPA’s) forclients at over 170 locations nationally.
These accounts are generally held on behalf of clients whoare in long term residential care, primarily within thefollowing services:
� Older People� Mental Health� Intellectual Disability� Physical and Sensory Disability� Acute Hospitals (long stay)
The purpose of this document is to set out the procedureto be followed by HSE employees, or agents, in theadministration of clients’ patients’ private property.
The following Guidelines set out the steps that must betaken to ensure that the interests of the client areprotected and gives clear guidance to HSE employees inthe management of clients’ property in the care of theHSE.
This document provides clear guidance on the use of fundsfor the benefit of clients, particularly where a client maynot have full capacity to manage, or to make decisionsaround the best use of their funds.
1.0 Policy 2.0 Purpose
Patients’ Private Property Guidelines
2
Patients’ Private Property Guidelines
3.0 Scope of Application of PPP Guidelines
These Guidelines apply to all staff employed by the HSEwho administer patients’ private property.
These guidelines apply to all patients’ privateproperty held by the HSE under the followingcircumstances:
3.1 Where the HSE directly holds the client’smonies for safekeeping
The relevant sections of the Health (RepaymentScheme) Act 2006 and these Guidelines apply to allpatients’ private property which is held insafekeeping in respect of clients in its care in its ownfacilities or in those of third party providers (typicallyprivate and voluntary nursing homes and similarfacilities).
3.2 Where a third party provider holds the moniesand the contract for care is between HSE andthe provider
The relevant sections of the Health (RepaymentScheme) Act 2006 also apply to monies held forsafekeeping on behalf of clients by the operators ofthird party facilities where the contract in respect ofthe care of the client is between the HSE and theprovider.
This is typically in relation to voluntary residentialservice providers (Section 38 funded locations) and“contract” or “fully subvented beds” in privatenursing homes. For the avoidance of doubt on eachparty’s responsibilities, the detail of sucharrangements should be included in the ServiceLevel Agreement between the HSE and the thirdparty provider.
These Guidelines are adjusted in the manneroutlined when the following third party legalauthority is in place over the financial affairs ofa client:
3.3 Wards of Court/Enduring Power of Attorney/Court Appointed Next Friend
Where a client is a Ward of Court or has in placean Enduring Power of Attorney (EPA) then thepower to make any requests in relation to fundsheld in safekeeping for the client rests with theWards of Court Office or the person who hasregistered and activated the EPA with the HighCourt. A Court Appointed Next Friend may alsohave authorisation over a client’s financial affairs.
In relation to Wards of Court you should seekdirection from the Wards of Court office or fromlocal management. The PPPA Central Unit can alsoadvise on such cases, should management wish torefer specific cases.
In situations where an EPA may be in place it isnecessary to confirm that the EPA has beenactivated and that the registered person has theproper authorisation under the EPA to makerequests over the client’s funds.
Court Appointed Next Friends may also haveauthorisation over a client’s financial affairs. It willbe necessary to confirm the actual authorisation ineach individual case as such appointments arenormally for specific purposes and would notautomatically include control over a client’sfinances.
In all of the above scenarios, local managementshould refer cases to the PPPA Central Unit for anyadvice required.
3

Relevant Legislation, Regulations & Standards
The HSE must ensure that the operation of PPP accountsis in accordance with all legislation and regulations. TheHSE operates PPP accounts under the authorisation of theHealth (Repayment Scheme) Act 2006. Certain legislation,regulations and standards refer to clients at specific typesof Care Centre only, such as Mental Health, Disability orOlder Persons’ services. All relevant staff at such CareCentres should make themselves aware of the content ofthis legislation and standards and the requirements theyplace on the HSE in the management of patients’ privateproperty. The guiding principles and decision-makingprocess over managing client funds outlined in thisdocument are in line with the requirements of relevantlegislation, regulations & standards.
Older Persons Services
The HIQA National Quality Standards for ResidentialCare Settings for Older People in Ireland outlinesstandards specifically on Client Finances in such caresettings. Some other standards within that document alsoimpact on how clients’ private property should bemanaged.
Disability Services
The HIQA National Quality Standards: ResidentialServices for People with Disabilities also outlinesstandards specifically on Client Finances in such caresettings. Some other standards within that document alsoimpact on how clients’ private property should bemanaged.
Mental Health Services
Sections 62 and 63 of the Mental Health Act 2001 defineApproved Centres for the purpose of the Act. A number ofarticles within Statutory Instrument No. 551 of 2006,issued pursuant to Section 66 of the above Act, arerelevant to decisions on the management of client PPPfunds and provide direction on clothing, resident’s personalproperty and possessions, individual care plans and theprovision of information.
HSE National Financial Regulations
The HSE PPP National Financial Regulations should befollowed at all times in managing PPP funds. Greater detailon the accounting and other requirements around themanagement of PPP is provided in the PPP NationalFinancial Regulations.
Future Legislation and Regulations
Any further legislation or regulations relevant to PPP will becirculated to all relevant staff along with a briefing on anyimpact on these Guidelines.
4.0 Legislation/Other Related Policies
Patients’ Private Property Guidelines
4
Patients’ Private Property Guidelines
5.0 Glossary of Terms and Definitions
Definition of Patient’s Private Property
A Patient’s Private Property account is defined in Section 2the Health (Repayment Scheme) Act 2006 as:
“patient’s private property account means so much of themoney and personal property of-
a) a person provided with in-client services referred to inSection 53 of the Health Act 1970 (as amended bysection 4 of the Health (Amendment) Act 2005),
b) a person provided with institutional assistance underSection 54 of the Health Act 1953,
c) a person in residence used wholly or partly as a settingto provide care for persons with physical or mentaldisability, or
d) a person otherwise being cared for by, or on behalf of,the Executive due to a physical or mental disability or ill-health,
that is managed, on behalf of that person, by the Executiveor by another person under an arrangement with theExecutive whether before, on or after the commencementof Section 9.”
The above definition of client’s private property includespersonal effects such as:
� Clothing� Footwear� Jewellery and other small valuable items� Luggage� Personal items of furniture, ornaments etc� Other personal effects
In respect of the above items, with the exception ofJewellery and other small valuable items, the primaryrequirement, as part of the routine care of clients andoperations generally, is for HSE and its staff to seek to limitany loss or damage to clients; personal effects in so far asis practicable.
In respect of Jewellery and other small valuable itemsclients should be advised that such items cannot besafeguarded by HSE unless they are handed in forsafekeeping to the appropriate staff. Proper records of thereceipt of such valuables should be retained and allvaluables should be stored in a secure area. Localprocedures over the receipt and storage of valuablesshould be followed in all cases.
Property may also include monies or documents such aspension books that provide access to monies or facilitatethe future transfer of monies to the HSE to be held in safekeeping for the client.
There is a practical requirement on the HSE and its staffbeing made aware of, or having knowledge of, theexistence of any property in order to implement theseguidelines effectively.
There is however, an onus on the HSE and its staff to makeall reasonable enquiries on admission, and subsequentlyif appropriate, to establish the existence and extent of anyproperty that a client may have brought into the facility.The HSE’s formal position remains that it cannot acceptresponsibility for funds or other property not handed in forsafekeeping to its staff.
5
Each Regional Director of Operations is responsible for theimplementation of these Guidelines within their area ofresponsibility.
Each HSE employee, or agent, who deals with PPP isrequired to make themselves familiar with the content ofthese Guidelines and is responsible for theirimplementation within their area.
The PPP Governance Committee is responsible for theongoing review of these Guidelines.
Fundamental Concepts which inform theseGuidelines
7.1 General
7.1.1 Client funds held in PPPA’s belong to the client andto no other person or body including the HSE. TheHSE has an implied trustee relationship with itsclients in respect only of those clients’ PPP funds.
7.1.2 Any net interest earned on investment of PPP fundsbelongs to the clients and cannot be retained by theHSE. The HSE may however retain a portion ofinterest earned on funds invested by the PPPACentral Unit, Tullamore as provided for in StatutoryInstrument No. 639 of 2007.
7.1.3 The HSE is committed to promoting the continuedindependence of its clients to the greatest extentpracticable, consistent with the provision of safeand appropriate care. In this context clients must beencouraged and supported to make their ownarrangements regarding safekeeping of their funds.However, where necessary and/or requested by oron behalf of the client the HSE offers the PPPservice.
7.1.4 The HSE has a duty to be able to properly recordand account for any movements in the funds heldby it in safekeeping for clients.
7.1.5 This duty is an integral part of the overall care ofour clients.
7.1.6 These guidelines must be read in conjunction withthe HSE National Guidelines on Charges for In-Patient Services and the HSE’s Financial Regulations.
7.2 Clients with capacity
7.2.1 There is a general legal presumption that anindividual has the mental capacity to make theirown decisions.
7.2.2 HSE must assume a person has capacity to makeany given decision unless there is a strong basis tobe concerned that this may not be the case.
7.2.3 HSE must not allow any client’s funds in itssafekeeping to be utilized for any purpose withoutthe clear permission of the client other than wherethe client is unable to give that permission due to alack of capacity – see 7.3 below.
6.0 Roles and Responsibilities 7.0 Guidelines
Patients’ Private Property Guidelines
6
Patients’ Private Property Guidelines
7.2.4 IF THERE IS NO REASON TO DOUBT THECAPACITY OF THE CLIENT THEN THE GOLDENRULE IS TO ASK THE CLIENT AND GET THEIRPERMISSION BEFORE DOING ANYTHING WITHTHEIR FUNDS – The HSE’s only role is to carry outthe reasonable request of the client as effectively aspossible.
7.3 Clients who may lack full capacity/Assessmentof Clients’ Capacity
7.3.1 Wherever these guidelines refer to the HSE or itsstaff making decisions about clients’ funds theimplication is that the client(s) in question do nothave the capacity to do so themselves. This is theonly situation in which the HSE would make suchdecisions.
7.3.2 This complexity cannot be allowed to prevent theHSE from meeting its responsibilities to its clientswhich includes respecting and reinforcing theirpersonal dignity and their freedom to determinematters relevant to them.
7.3.3 The HSE, in keeping with the recommendations ofthe Law Reform Commission, does not wish toadopt the Status based concept of capacitywhereby all clients are classified as either having fullcapacity or not having capacity.
7.3.4 The HSE seeks to use the functional interpretationof capacity to the greatest extent practicable i.e.that capacity is specific to the particular act ordecision at the time it is being made.
7.3.5 Whether a client is deemed to have capacity or not,he or she must be involved in decisions affectingthem, including decisions around their funds, to thegreatest extent practicable and consistent with theiroverall well being.
7.3.6 A full mental capacity assessment (MCA), such asfor the purposes of wardship applications, requiresthe input of one or more medical practitionerspreferably consultant psychiatrists/geriatricians/psycho-geriatricians.
7.3.7 However on a practical level, it is entirelyappropriate that non-medical clinical and other staffcontinue to play a key role in identifying andassessing, on an ongoing basis, any clients whopotentially may lack the mental capacity to makecertain decisions without assistance, or at all. This is
a core part of the existing duties of medical,nursing, therapy and other health service staff andrelates to decisions facing clients regarding anyaspect of their care and well being.
7.3.8 Clients’ funds are by no means the most complexor critical area where HSE staff are called upon touse their professional judgement concerning thecapacity of clients in the interests of protecting theirclients.
7.4 The HSE’s responsibility where there are doubtsaround clients’ capacity
7.4.1 The HSE’s sole duty, concerning the PPP funds ofsuch clients, is to ensure their funds held by the HSEare safeguarded for their direct benefit and theirbenefit alone (see below regarding dependants).
7.4.2 The HSE has no clear legal power to hand over,without their informed consent, the funds of anyclient, to any other person other than where thatclient is a Ward of Court (WOC), or has in place anoperative Enduring Power of Attorney (EPA) or haspassed away.
7.4.3 These guidelines set out the safeguards to beapplied where a doubt exists as to capacity – inpractice these safeguards will protect the client andHSE staff in situations where:
a. A doubt has been raised as to capacity of a clientOR
b. A formal assessment of capacity, by a medicalpractitioner or other qualified professional(s) isawaited OR
c. A formal assessment has already been carriedout and the client is deemed to lack the capacityto make the decision around their fundsthemselves.
7.4.4 It follows that the HSE has no clear legal power tohand over to any person, the funds of a client wholacks the capacity to give permission for thattransfer.
7.4.5 In allowing any utilisation of PPP funds where aclient does not have capacity and therefore cannotgive an informed permission, the HSE must beguided by the overriding requirement that it acts in
7
the clear best interests of the client and the clientalone. In doing so in a transparent manner the HSEis acting within the requirement placed on it bySection 9 of the Health (Repayment Scheme) Act2006.
7.4.6 For the avoidance of any doubt the HSE cannotpermit any “pooling” or “general use” of thefunds of many clients for the general benefitof some clients – each client’s funds can only beused for that specific client’s benefit.
7.5 Involvement of Next of Kin
7.5.1 The HSE will seek to involve next of kin (and otherinterested persons) in as much as is practical andappropriate in the care of clients including thoselacking capacity. Any involvement must be in thebest interest, and for the benefit, of the client andrespect the client’s right to privacy andconfidentiality.
7.6 Appropriate Local Discretion
7.6.1 It is neither practical nor appropriate for the HSE toseek to be fully prescriptive in setting out guidelinesconcerning the administration of PPP particularly onissues impacted by the lack of capacity of clients.
7.6.2 The HSE supports the principle of its clinical andother staff, who deal directly on an ongoing basiswith clients and their relatives/friends, in makingdetailed decisions about the management of PPP.Local clinical and other staff are best placed toknow what may be both safe and appropriate inrespect of one client and their funds while beingclearly inappropriate in respect of another client.
7.6.3 Any such local discretion must be exercised purelyon the basis of the client’s best interests and theirinterests alone and must be within the parametersset by these guidelines, taking account of therequirements placed on the HSE in operating clientPPP a/c’s by the Health (Repayment Scheme) Act2006, the Mental Health Act 2001, relatedStatutory Instruments and National QualityStandards.
7.7 Clients Funds Versus HSE Funds – who shouldpay for what?
Central to the effective administration of patients’ privateproperty is the need to clearly separate clients’ funds fromHSE funds. This ensures appropriate protection for bothclients and staff.
In order to implement this separation we require clarity asto what clients are expected to fund from their ownresources and what they can reasonably expect the HSE toprovide for as part of its care obligation.
It should be noted that funds raised by the HSE fromcharges correctly levied on clients under relevant legislationare HSE funds and cease to be clients’ funds once collectedby the HSE.
Process for accessing client PPP funds for the benefitof the client
It is not possible to provide a definitive list of items thatmay or may not be purchased from an individual client’sPPP funds. Rather, each client’s ability to derive benefitfrom any item or service that might potentially bepurchased using their PPP funds must be assessed byclinical staff in the context of his/her overall Care Plan. Eachclient must be assessed individually and in line with localpolicy.
In cases where there is an agreed defined decision by theclinical team that a client would benefit from the purchaseof an item or service not deemed to be necessary for theclient’s care, application can be made to use the PPP fundsof that client to purchase same.
To access this funding the following process must befollowed:
1. There must be a documented valid reason for thebenefit of the client to purchase an item or service;
2. The intervention (equipment, service, therapy etc.)must be documented as part of the client’s Care Planand reviewed as per the therapeutic intervention;
3. The request must be put in writing to the Director ofNursing/Unit Manager or their designate and signed offas appropriate by them; and
4. For ongoing services and therapies, an appropriatemonitoring and review date must be agreed notgreater than three months.
Please refer to Appendix 6, which outlines inflowchart format the steps to be taken in arriving ata decision to use client PPP funds to purchase an itemor service.
The following sections provide guidance to staff in makinga decision on the appropriateness of utilising client PPPfunds for the benefit of clients. This should be used as aguide only and does not purport to be a definitive list of
Patients’ Private Property Guidelines
8
Patients’ Private Property Guidelines
items that may or may not be purchased from PPP funds.The overriding factor in all decisions is whether the clientwill benefit from the purchase of an item or service, as pertheir Care Plan.
It is not appropriate to request or utilise clients’ fundsfor the following:
7.7.1 Facilities Upkeep/Refurbishment /Maintenance/Decoration – Such costs are a matter for the HSEto fund.
7.7.2 Ongoing In-patient Charges or Arrears ofCharges – Such charges should not be deductedfrom a client’s PPP a/c without the authorisation ofthe client themselves. All charges should be fundedfrom the client’s ongoing income on which theircharge has been assessed. This is of particularrelevance where the HSE is not the appointed Agentto collect DSFA allowances and a key client contactis paying ongoing In-Patient charges from theclient’s income.
7.7.3 Furniture/Fittings/Equipment - It is the HSE’sresponsibility to fund from its own resources, thecost of necessary furniture, fittings and equipmentwithin wards, residences, day areas etc.
Please refer to situations, below, where it maybe possible to use client PPP funds for theirbenefit in the purchase of certain items.
7.7.4 Medicines – The costs of medicines required byclients are generally covered directly or indirectly (viapublic demand led schemes) by the HSE.
Should any issues arise in this area it is reasonablefor the HSE to only cover the costs of medicineswhich its care professionals are satisfied are bothnecessary and appropriate for the care and wellbeing of the client.
7.7.5 Aids/Appliances – To the extent that the HSE issatisfied that aids/appliances are required for theappropriate care of the client then it is generally amatter for the HSE to fund same, to the extent thatit is in a position to do so within available resources.
Please refer to situations, below, where it maybe possible to use client PPP funds for theirbenefit in the purchase of certain items.
7.7.6 Nutrition Supplements/Food – Generally for theHSE to fund.
The client may augment what HSE provides, fromtheir own funds, additional personal items of food/nutritional supplements that the client desires,which are over and above the norm of what HSEprovides and which are not considered necessaryfor the care of the specific client or clients ingeneral.
7.7.7 Personal Hygiene/Personal Grooming - Thestandard hygiene items such as soap, toothbrush,toothpaste, deodorant, etc., should be provided atHSE expense.The client may augment, from their own funds,these basic products with additional groomingproducts such as make-up, perfumes, aftershave,etc.
In regard to hair dressing this is normallyundertaken at the client’s expense.
However, appropriate local professional discretioninvolving the use of HSE funds must be exercised toensure clients personal grooming, including hair,does not fall below a minimum standard consistentwith their general well being.
7.7.8 GP/Chiropody/Optical/Aural/Immunisation etc -These services, to the extent that HSE is in a positionto provide them within available resources, willnormally be provided either as part of the facilitiesof the unit or may be accessed through theresident’s medical card/GP visit card.
It will be necessary for appropriate local professionaldiscretion, involving use of HSE funds, to beexercised in respect of the small minority of clientswho are both:
a) not eligible for a medical card and
b) in need of additional services beyond thosedirectly provided by the unit they reside in.
It may be appropriate to request or utilise clients’funds for the following:
7.7.9 Trips/Outings/Other Social Activities - A residentshould only be liable for reasonable costs fortrips/outing /other social activities (including partiesetc).
Local discretion must play a significant role inrelation to this area and in considering what isreasonable the following must be taken intoaccount:
9
1. It is not appropriate for any costs relating to HSEstaff attending or facilitating such trips, outingsor social activities to be borne by clients’ funds;
2. Residents should only be asked to contribute tothe costs of trips etc that they will be attendingor are likely to attend;
3. Where a group of clients are taking part in agroup activity,
� Each client must get an equitable benefit of themoney spent from their PPP a/c. PPP funds mayonly be spent for group activities from the PPPfunds of those clients actually participating inthe activity,
� A record of clients’ participation in the activitymust be kept, e.g. in such a scenario, a list ofthose who attended the activity is recorded, sothat the spending of PPP funds can be linked toparticipation in the activity.
Example
A family member has suggested that they wouldaccompany John to Lourdes on a pilgrimage. Staffat the Care Centre are aware that John alwaysliked travelling and are happy that he wouldbenefit from such a trip and is consistent with hisCare Plan. It is appropriate to fund John’sexpenses for this trip from his PPP funds.
In certain circumstances, the necessary andreasonable cost of a third party to accompanyJohn on this trip could also be funded from hisPPP a/c. Great care would need to be exercised inensuring that it was necessary to provide atravelling companion and that the costs werereasonable. Such a payment must be approved bya senior manager, such as a Director of Nursingor a Senior Administrator, prior to travel.
Furniture/Enhanced Aids & Appliances for PersonalUse - A client may augment, from their own funds, thesebasic items with additional items that the client desireswhich are over and above the norm of what HSE providesand which are not considered necessary for the care of thespecific client or clients in general. This might include thepurchase of chairs, items of bedroom furniture orenhanced aids & appliances from which the client wouldbenefit.
Examples
Mary is resident at an Older Person’s Care Centre.She takes great pride in her appearance and usesmake-up daily. It is decided that she would benefitfrom her own dressing table at which she couldsit to apply her make up and store all of herbeauty products. It is appropriate to use theclient’s PPP funds to purchase this dressingtable. The dressing table is the property of theclient and should not be used by others.
A Client at a Care Centre has insufficient storagespace for his clothes. The manager decides toinstall fitted wardrobes in all clients’ rooms. It isnot appropriate to use the client’s PPP fundsto pay for the fitted wardrobes.
Mary is resident at a Long Term Care facility whereshe sits out every day. When living at home sheused a particular armchair which she found to bevery comfortable. Mary is assessed by anOccupational Therapist who decides that theexisting chair provided at her Care Centre meetsher needs. In this case it is appropriate to useher PPP funds to purchase an armchair similarto the one she used at home.
Lily is in the bed adjacent to Mary and also sitsout daily. After assessment by the OccupationalTherapist it is decided that she requires a specialTilt & Space chair. This chair must be purchasedfrom HSE funds only. Lily’s PPP funds cannot beused as the chair is a requirement of her care.
7.7.10 Clothing – The general position is that clothing issomething which clients should provide from theirown funds if for no other reason than the fact thatthis reinforces their personal dignity andindependence. A client’s tastes and needs should beconsidered when deciding on types of clothing tobe purchased and costs incurred should bereasonable.
However, appropriate local professional discretioninvolving use of HSE funds must be exercised toensure clients clothing does not fall below aminimum standard consistent with their generalwell being.
Patients’ Private Property Guidelines
10
Patients’ Private Property Guidelines
7.7.11 Link to Long Stay Charges assessment
There are a number of expenses that are allowablewhen calculating the appropriate Class 1 or Class 2charge, hence the resident should pay for theseexpenses from their own funds.
The “Long Stay Charges – National Guidelines”highlights these as including: -
� Dependant adult/child (maintaining)� Life Assurance� Medical Insurance� Medical Costs (including prescription costs –
relates primarily to dependants)� Rent/Mortgage Allowances� Loans/Repayments� Maintenance Payments� Travel Costs� Other Outgoings
It follows that the above items fall primarily to bedealt with by clients from their own funds.
This highlights the importance of ensuring that theadministration of patient’s private property and theassessment of long stay charges are appropriatelyco-ordinated.
7.7.12 General Saver re Eligibility
Nothing in these regulations is intended toalter the status quo or set a precedent inrelation to clients who may not be eligible forthe Medical Card Scheme, the GP Visit onlyscheme or the other various public schemeswhich medical card eligibility provides primaryaccess to.
This has particular relevance in relation to clients inprivate nursing home care.
7.8 Assessment of Clients’ Capacity
While, in general, society assumes that all adultspossess both testamentary and financial capacity,the HSE has a special duty to protect the financialinterests of those vulnerable adults under its care.
A formal determination of financial capacity shouldbe part of the assessment process for entry to HSE-approved or funded extended care facilities. Thiswill establish a baseline against which futuredeterminations of capacity can be compared.
Assessment of clients’ capacity is a normal part ofthe ongoing duties of HSE staff operating within themany care professions and consideration offinancial capacity should form part of the ongoingmonitoring of the client/client’s health status withinthe care facility.
Assessment of clients’ capacity regarding PPP fundsmay be necessary:
a. where there are doubts about the generalcapacity of a client to manage their funds on aday to day basis,
b. to determine the degree of support withmanaging PPP funds that is required by clientsin this regard, or
c. where doubts exist about the capacity of clientsto give an informed consent to specificwithdrawals or payments from their funds infavour of third parties(spouse/children/relatives/friends).
In the absence of a request for such an assessment,the working presumption is that the client iscapable of managing their finances and should befacilitated to act as they wish even if this appearsinappropriate to an external observer.
Where assessment is considered necessary as aresult of requests to release clients’ funds to thirdparties, it is important to realise that HSE’s concernis for the interests of the client solely.
While the HSE is committed to workingcollaboratively in so far as is practical with relativesand friends it is not feasible or appropriate to seekto have all clients speedily subjected to Full MentalCapacity Assessments (MCA), where the sole driverfor same is the desire for access by a third party tothe funds of the client. An MCA can only be carriedout by a consultant psychiatrist, geriatrician orpsycho-geriatrician.
The need to protect the dignity and well being ofclients, as well as obvious resource constraints,demands that the HSE only carries out assessmentsto the extent necessary and appropriate in theoverall context of the care and well being of theclient.
Where appropriate, the HSE should use generallyaccepted assessment tools available to it (forexample MMSE – Mini Mental State Examination)
11

to determine if there is a need for a full MCA. TheMMSE and other generally accepted clientassessment tools can be carried out by other clinicalstaff provided they have the appropriate trainingand experience. Where practical and available, it ispreferable to involve the full care team in assessingthe client.
It is important to bear in mind that there is nostandard test of capacity, e.g. Mini-Mental StateExamination (MMSE). However, the MMSE is auseful standardized assessment tool available toCare Centre staff. Staff should be aware that ininterpreting the results, a normal test does notexclude impaired financial capacity and conversely,an abnormal result does not always indicate thatthe person lacks capacity. It is appropriate to usethis tool as long as the interpretation is based on ageneral global impression of the client.
If there are any concerns of coercion by a thirdparty or that tests are being requested withoutthe client’s best interest being uppermost, thenthe case should be referred to the HSE’s ElderAbuse Service.
7.9 Application to the Circuit Court for Directionon using Client PPP Funds
Introduction
Section 9 (2) (c) of the Health (Repayment Scheme)Act 2006, below, allows the HSE to seek directionof the Circuit Court as to how it may use any moneyof a PPP account holder in excess of €5,000 for thebenefit of that client.
“The Executive
(c) may, in respect of the patient’s private propertyaccounts of all or some of the account holdersresiding in the same hospital or other institution,make an application, not more than once in eachcalendar year, to a judge of the Circuit Court inwhose circuit the hospital or institution, as the casemay be, is situated, for directions as to how theexecutive may use any money in excess of €5,000or the amount prescribed in regulations madeunder Section 20 (1)(c), whichever is the greater, inany of those accounts for the benefit of the accountholder in whose patient’s private property accountthe excess is lodged.”
HSE Policy
It is HSE policy that the direction of the Circuit Courtbe sought in all cases where the HSE uses in excessof €5,000 (or the amount prescribed in regulationsmade under Section 20 (1) (c)) in client funds forthe benefit of the client in a calendar year, except inexceptional circumstances, and after seniormanagement approval, as outlined below.
Care Centre staff must monitor planned spendingfrom clients’ PPP a/c’s who lack capacity to managetheir own funds to ensure that relevant plannedhigh value purchases are identified in time to allowapplication to the Circuit Court. The initial decisionto spend such funds will have been made afterreview of the client’s Care Plan where it will havebeen decided by a multi-disciplinary team that suchspending will be for the benefit of the client.
Exceptional Circumstances
In exceptional circumstances, Court direction maybe replaced by the authorisation of the relevantRegional Director for Operations, on receipt of arecommendation from the Local Health Managerwithin whose area the relevant client is resident.Any such recommendation must be reviewed by theManager of the PPPA Central Unit before beingforwarded to the Regional Director for Operationsto ensure that all technical issues with such anapplication are in order.
Please note that it is expected that in the vastmajority of cases, the use of client funds in excess of€5,000 will require the direction of the CircuitCourt. Care Centres should contact to PPPA CentralUnit to discuss the detail of individual cases beforecommencing the process of seeking the direction ofthe Circuit Court.
Key Features
The prescribed €5,000 threshold:
� Only applies where the HSE is using its powersunder the 2006 Act to use a client’s funds fortheir benefit where the client does not have thecapacity to make that decision themselves, andfunds in excess of €5,000 will be used for theclient’s benefit in that calendar year;
Patients’ Private Property Guidelines
12
Patients’ Private Property Guidelines
� Does not apply where the client has thecapacity to manage their own funds, in whichcase the HSE will not be making such decisions.In such cases, the client must approve allspending from his/her PPP account before theHSE will provide funds from that client’s PPP a/c;
� Does not apply to small value spending byclients who have capacity to make decisionsaround such spending but may not havecapacity to decide on larger value purchases. Insuch cases, only the larger value purchasesshould be included in the calculation of the€5,000 limit;
� Does not apply to committees of a Ward ofCourt, Court Appointed Next Friends orAttorneys acting under an activated EnduringPower of Attorney, providing they are actingwithin the terms of their appointments (must beconfirmed in individual cases);
� Excludes Long Stay charges deducted on theclient’s behalf by the HSE;
� Is in respect of a calendar year; and
� Must not in any way be seen as a ceiling thatinfluences decisions over the use of client fundsfor their benefit. Any concerns about thepractical issues associated with making CircuitCourt applications must be treated as a matterentirely separate to determining the extent towhich relevant clients would benefit from theHSE arranging for their PPP funds to be utilised.
Circuit Court Application Process
The preparation of applications to the Circuit Courtis dictated by the Circuit Court Rules outlined inStatutory Instrument No. 446 of 2007. A FlowChart attached in Appendix 6:
� Outlines the key stages in preparing such anapplication,
� Identifies who should undertake each stage, and
� Provides a list of documents required.
This application process is a legal requirement, asper the Statutory Instrument, and must be fulfilledbefore an application can be submitted to theCircuit Court. A detailed explanation of the Circuit
Court Rules is available within the separate CircuitCourt Rules Procedure document, available fromthe PPPA Central Unit, Tullamore. The handling ofsubmissions to the Circuit Court will be managedat Regional level.
7.10 Withdrawal/Payment of monies from Patients’Private Property Accounts in favour of 3rdParties
For the purposes of these guidelines third partypayments relate to requests to pay over clients’funds to someone other than the client.
It is under this heading that requests for access toclients’ funds by spouses/children/dependants/relatives/friends etc are dealt with.
A procedure for such payments is set out atAppendix 1 which covers:
a. Payments to third parties and
b. Reimbursement to third parties on production ofreceipts for items purchased for the directbenefit of the client.
Templates for each of the above are attached atAppendix 2 and Appendix 3.
Where there is no doubt about the capacity of theclient to make the necessary decision then thirdparty payments present little difficulty for HSE andits staff. All such requests must be requested andapproved by the client.
Where a client is a Ward of Court, has in place anEnduring Power of Attorney (EPA) or is a CourtAppointed Next Friend, then the power to approveany requests in relation to funds held in safekeepingfor the client rests with the Wards of Court Office/Committee of the Ward or may rest with theperson who has registered and activated the EPAwith the High Court or a Court Appointed NextFriend.
7.11 Funds and other Property of Deceased Clients
7.11.1 Funds of a deceased client should be passed to theclient’s Legal Personal Representative for themto administer the estate of the deceased faithfullyaccording to law.
13
Legal Personal Representatives may be:
a. Executorsappointed within a will – they becomeresponsible for the client’s assets immediatelyupon death – their function is to obtain a “grantof probate to the estate (all savings andproperty)”, from the Probate Office in Dublin ora District Probate Registry outside Dublin, and toadminister the estate.
b. Administratorsmay be appointed by the Probate Office inDublin or a District Probate Registry (outsideDublin) where no will has been made by thedeceased i.e. the person has died “intestate”– do not become responsible until appointed bymeans of a “grant of representation” – theirfunction is to obtain “a grant ofadministration/letters of administrationintestate” and to administer the estate.
For the purposes of these Guidelines, the term“Legal Personal Representative” (LPR) embodiesboth executors and administrators as well as thosewho are entitled to apply for a grant ofadministration.
In the ideal situation all clients would have made awill and the HSE would be made aware of same andof details of the Executor(s) and Solicitors acting forsame.
In so far as is appropriate and feasible in the contextof ensuring the overall care and well being of theclient, the HSE should seek to establish whetherclients have made a will and who the Executor(s)and solicitor for same is.
If this information is not available to the HSE at thetime of death then all reasonable enquiries torelatives, friends and others, as appropriate, to theextent that they can be established by the HSE,should be made.
7.11.2 Release of PPP Funds to the Legal PersonalRepresentative
In deciding who is entitled to act as the LegalPersonal Representative, staff should refer to theDeceased Clients Procedure Flow Chart, whichwill provide guidance and key information on howto manage each individual case.
Staff should trace the flow chart from the ‘StartHere’ box and follow the relevant directional arrowsbetween the decision boxes, depending on theparticular circumstances. In difficult cases where theflow chart does not provide the necessary direction,staff should firstly raise the issue with localmanagement, who may decide to refer the case tothe PPPA Central Unit for advice.
The key issue for staff to consider is that the HSE isseeking to establish who is best entitled to act asLPR, rather than who is entitled to inherit the funds.
7.11.3 Release of Funds where no Executors orAdministrators are appointed
Where, having made all reasonable enquires1, HSEis advised that there is no will and no intention toseek the formal appointment of an administrator,the HSE may pay out client funds in certaincircumstances where the balance held is no morethan €20,000 provided:
� The requirements of the Deceased ClientsFlow Chart (Appendix 6) are followed;
� The HSE has no valid reason to believe that theperson wishing to act as LPR is not entitled todo so and that we are not aware of any disputeor potential dispute over the inheritance or aperson’s right to act as LPR.
� Written confirmation of their right to act as LPRand of their intention to distribute the assets asper law is provided by the Legal PersonalRepresentative by fully completing the HSEDeclaration and Deed of Indemnity form.(Appendix 6).
In cases where the above requirements are not met,staff should refer such cases to local management,who may forward same to the PPPA Central Unit tomanage on their behalf.
Standard letters to accompany the DeceasedClients Flow Chart are provided for staff to assistthem in corresponding with family and LPRs duringthis process.
1 All reasonable enquiries includes written communication with anyindividuals known by the HSE who may have information as to the existenceof next of kin including any persons mentioned in the client’s files, otherregular visitors of the client, CWO services where appropriate.
Patients’ Private Property Guidelines
14
Patients’ Private Property Guidelines
7.11.4 Funeral Expenses
It is important that each unit/residential locationtake as proactive an approach as possible,consistent with the overall care and wellbeing of theclient, in assisting clients/their families to preparefuneral arrangements in advance so that thenecessary arrangements can be made when thetime comes and any distress for relatives and friendsassociated with same can be minimised.
Each unit/residential location should ensure that:
� It takes the necessary steps to update its clientfiles so that details of next of kin are readily tohand;
� If necessary, each location should review theextent and quality of next of kin informationavailable to it on client files and take whateversteps are practical to address any possible gapsin same;
� On admission or as soon as practical thereafterfull particulars of all next of kin should beobtained;
� Where appropriate, client’s wishes aroundarrangements for their funerals should beestablished; and
� Clients with appropriate capacity who have notmade a will to date should be encouraged to doso. This is, of course, a decision entirely for theclient themselves and some clients may decidenot to do so.
A - Managing claims for funeral expenses
When deciding how to manage claims for thepayment of funeral expenses, HSE staff should referto the Funeral Expenses Flow Chart (Appendix 5)for advice on the procedure to follow.
Again, Staff should trace the flow chart from the‘Start Here’ box and follow the relevant directionalarrows between the decision boxes, depending onthe particular circumstances. In difficult cases,where the flow chart does not provide thenecessary direction, staff should firstly raise theissue with local management, who may decide torefer the case to the PPPA Central Unit for advice.
B – Where funeral arrangements are dealt withby relatives/friends
The HSE preference is, for all clients who die whilein care, to have their funeral arrangements carriedout in accordance with their own wishes and for thenecessary arrangements to be handled by relatives/friends as dictated by the client.
Clients’ funds can be released to the LPR to enablethem, amongst other things, to retrospectively meetallowable funeral expenses.
Once funds have been released to the LPR it is thena matter for them to make any decisions asappropriate around usage of those funds includingto discharge any funeral expenses.
It is also acceptable for HSE to pay the bill(s)associated with the funeral arrangements (from thedeceased’s PPPA) provided they are reasonable andthat the relevant manager is satisfied that the costshave been appropriately incurred and there aresufficient funds in the clients account to coversame. In such circumstances you should refer to thedefinition of Allowable Funeral Expenses includedon the Funeral Expenses Flow Chart.
In cases where relatives incur extra costs associatedwith a funeral, they should be advised that theyshould seek to recoup same subsequently from theLPR. The main purpose of this provision is to protectthe HSE from instances where potentialbeneficiaries to a deceased persons estate may,subsequent to the funeral, take issue with theextent of the client’s funds that have been used upin paying for same.
C – Where, in exceptional cases, HSE makes thenecessary funeral arrangements
Where clients have not or are unable to make theirwishes known and/or there are no available legalpersonal representatives/relatives/friends to makethe necessary arrangements, then in exceptionalcases HSE may have to make the necessary funeralarrangements.
Where HSE makes the funeral arrangements thenthe cost of same is to be charged on the client’sfunds held in their patient’s private propertyaccount. Again, the Funeral Expenses Flow Chartshould be followed to provide guidance to staff inmanaging such cases.
15
If there are insufficient funds in the specific client’saccount, then any balance of cost must be chargedagainst the funds of the HSE itself – there can beno charging against “general clients’ funds” –options to recoup any balance of cost cansubsequently be followed up i.e. in terms of grantsfrom Department of Social Welfare and/orrecoupment from any balance of the client’s estatewhich may be held outside of the patient’s privateproperty account.
7.11.5 Monies Outstanding to HSE
It is not appropriate for HSE to unilaterally deductmonies owed to it from client’s funds following thedeath of the client.
Any such monies fall to be dealt with by agreementwith the Executors or Administrators where sameare appointed or by consultation with appropriateLegal Personal Representative prior to any decisionto make payments in the absence of legallyappointed executor(s) or administrators(s).
Agreement should be reached regardingoutstanding monies due to HSE before any balanceheld on client’s funds is paid over.
7.11.6 Property other than monies
Legal Personal Representatives are the appropriatepersons to make decisions around the personaleffects including clothing, jewellery and other itemsthat are the property of deceased clients. Items offurniture or equipment etc. purchased from clients’PPP funds should also be advised to the LPR so thatthey can decide on their disposal.
A receipt must always be obtained from the LPR toprovide evidence for the HSE that the personalitems were handed over to the correct person.
Bank/Credit Union/Post Office books should also beforwarded to the LPR after the return of acompleted Declaration & Deed of Indemnity Form.A record of the balances noted in such booksshould be retained and a receipt must also beretained, outlining the number of books, theFinancial Institution and the balance amount noted.(It must be remembered that the actual balancemight be different from that noted in such books.)It will then be a matter for the LPR to establishhis/her entitlement to receive any funds held by theFinancial Institution with that Institution directly.
7.12 Availability of Information on PPP Activity
Introduction
Care Centre staff receive ongoing requests forinformation on individual client PPP a/c balancesand transactions from clients themselves and alsofrom third parties, including spouses, children,parents, siblings and more distant relatives.
Clients Capable of Managing their ownFinancial Affairs
In cases where a client is capable of managing theirown financial affairs, information on any aspect oftheir PPP a/c will only be provided to the clientthemselves or to a person nominated in writing bythe client to receive such information. Clientsshould be provided with ongoing information ontheir PPP balances and transactions.
Any third parties requesting information on clientPPP a/c activity in such cases should be advised thatthis information is private and confidential to theclient and that the HSE cannot release same tothem without the express permission of the client.
Clients not Capable of Managing their ownFinancial Affairs
In general, all client financial information is privateand confidential to the client themselves,irrespective of whether the client is cognitivelyimpaired or not. Third parties, even when closerelatives, do not have a general right to accessinformation on client’ PPP activity or balances, evenwhen a client is cognitively impaired.
There are, however, a number of circumstanceswhere a third party will have a legal authority overthe financial affairs of the client and may be entitledto information.
There are also a number of limited circumstanceswhere the HSE may provide some financialinformation to a third-party, when provided for thebenefit, and in the best interest, of the client. Insuch circumstances the HSE must be in a positionto demonstrate that the release of this limitedinformation in such circumstances is justifiable, validand in the legitimate interest of the relevant client.
Patients’ Private Property Guidelines
16
Patients’ Private Property Guidelines
Legal Authority
In cases where a client has an Enduring Power ofAttorney in place which may grant the appointedAttorney access to the client’s financial information.A certified copy of the EPA should be sought andthe extent of the authority should then beestablished before any client information isprovided.
A Court Appointed Next Friend may also have aright to access information on a client’s PPPaccount. Again the exact nature of the authoritygranted to the next friend must be established ineach individual case before information is provided.
Information on the balance in a client’s PPP a/c canalso be provided to a person for the purpose ofthem making a Wardship application to theOffice of the Wards of Court. The release ofinformation in such cases should only occur on footof a formal request from the Solicitor acting on theinstructions of the proposed Committee.
Other Limited Circumstances
There are a number of limited circumstanceswhere the HSE may issue PPP a/c information tothird parties. Any decision to release information inthese limited circumstances must always be for thebenefit of the client and in their best interest:
� To the person(s) acting as Key Client Contact,and nominated as such by the client onadmission, who was at that time not cognitivelyimpaired. All clients being admitted should beasked to provide this information, if they sowish, on the attached Key Client ContactNomination Form (Appendix 7). You will notethat there is no requirement on clients tonominate such a person;
� To the partner, parent, child or other familymember of the client when that person is actingas the Key Client Contact where the client wascognitively impaired on admission. Suchinformation should be released only to allow theKey Client Contact assist the HSE to managethe PPP funds of the client in the best interest ofthe client, as provided for in the Health(Repayment Scheme) Act 2006.
In the latter situation, above, the decision to providelimited information to the Key Client Contactshould be made by the Director of Nursing or CareCentre Manager at the relevant Care Centre andshould be recorded on the client’s file.
Note
Key Client Contact is the person who is recordedas such on the client’s file and/or who normallyliaises with HSE staff on the care of the client. It ispossible that there may be more than one KeyClient Contact.
Deceased Clients
The PPP a/c balance of a deceased client may bereleased to the Legal Personal Representative, orsolicitor acting on behalf of such a person, to allowthem deal with the proper distribution of the assetsof the deceased client. Any queries from otherpersons on PPP balances or activity in the account ofa deceased client should be referred to the LPR forthem to deal with.
Requests for Information under FOI & DataProtection Legislation
Nothing in this document alters existingarrangements and procedures in place to deal withrequests for information under the Freedom ofInformation Act or the Data Protection Act. Anyqueries under FOI or the Data Protection Act shouldcontinue to be dealt with in the normal manner,following existing HSE procedures.
Please Note
If there are any concerns of coercion by a thirdparty or that information is being requestedwithout the client’s best interest beinguppermost, then the case should be referred tothe HSE’s Elder Abuse Service.
7.13 Complaints and Appeals
Complaints about any aspect of the serviceprovided by HSE staff as part of the administrationof Patients' Private Property are subject to the HSEYour Service Your Say Comments, Complimentsand Complaints process.
17
A complaint can be made using any of thefollowing media:
� Talk to any member of HSE staff, servicemanager or Complaint Officers;
� Fill in the 'Your Service Your Say, Informationon how to make Comments, Complimentsand Complaints' leaflet and place it in thefeedback boxes provided;
� E-mail [email protected] with your feedback;
� Send a letter or fax to any HSE location;
� Ring us: 1890 73 73 43 where your call will beanswered by a staff member from consumeraffairs; or
� Contact an advocacy service.
7.14 Support for Staff in making decisions indifficult cases/ Interpretation of PPP Guidelines
Staff should consult with Line Managers in the firstinstance. Where Service Managers/Administratorshave difficulty in deciding or clarifying a matter, theycan escalate it to the designated PPP Liaison Personfor their LHO Area/Hospitals Group for advice, whoin turn can refer issues to the PPPA Central Unit,Tullamore.
All requests for external legal advice should bechannelled through the PPPA Central Unit, who willarrange same for Care Centres.
Staff can also access information on PPP on thePPPA Central Unit HE Intranet site:
http://hsenet.hse.ie/HSE_Central/Integrated_Services/PCCC/Patient_Private_Property_Central_Unit/
Information on PPP for clients and their families isalso available on the PPP pages of the HSE Website:
http://www.hse.ie
These Guidelines will be reviewed in May 2012 by the PPPNational Governance Committee. Any changes deemednecessary at that time will be recommended to the HSESenior Management Team for approval.
Any changes or updated required in the interim will also berecommended by the PPP Governance Committee to theHSE Senior Management Team for approval. Ongoingaudit and review of these Guidelines will be undertakenby the PPP Governance Committee and the PPPA CentralUnit, Tullamore.
8.0 Revision and Audit
Patients’ Private Property Guidelines
18
Patients’ Private Property Guidelines
9.0 Appendices
Appendix 1 – Third Party WithdrawalsProcedure for Withdrawal/Payment of monies from Patients Private PropertyAccounts in favour of Third Parties
Introduction
This procedure sets out the controls necessary to protectthe monies of clients held in safekeeping, andadministered on the client’s behalf, by the Health ServiceExecutive (HSE).
It deals with the receipt and approval of requests forwithdrawals/payments from clients’ private property infavour of third parties where the client has sufficientmental capacity to make the decision around their fundsheld in safekeeping by HSE.
The withdrawals/payments referred to are where the HSEis being asked to pay over monies to a third party includingto a client’s spouse/child/dependant/relative/friend or otherperson.
It also deals with the reimbursement of receipts furnishedby third parties of clients with diminished capacity inrespect of personal effects provided directly for the benefitof clients.
Other than the reimbursement of receipts, it does notpermit the withdrawal and payment to third parties offunds from the accounts of clients who lack the capacityto give informed consent to such withdrawal.
The only exception is where there is an EnduringPower of Attorney in operation or the client is aWard of Court.
The purpose of this financial procedure is to enable theHSE and its staff and agents to demonstrate that we havecomplied in an appropriate way with our obligations inrespect of clients’ monies and to provide a degree ofassurance in this regard to:
� Clients
� Client’s family, next of kin and other concernedparties
� The HSE
� HSE Staff and agents
� Any other relevant parties
Existing Controls/Policies & Standard Movements ofClients Funds
This procedure does not apply to ordinarymovements on patients’ private property accountsfor the direct use of client’s funds by the client orwith assistance of HSE staff.
The controls set out in this document should beapplied in addition to existing controls which dealwith the receipt and security of client’s privateproperty from admission onwards.
Such existing controls/policies already deal with the normalday to day movements in client’s funds including in respectof the provision of client’s comforts, shop money, client’spetty cash etc.
They also already deal with issues around safekeeping ofnon money items.
Responsibilities
It is a matter for the relevant managers includingconsultants and other clinical managers to ensure that theyare aware of and comply with their responsibilities underthis procedure.
It is a matter for each relevant staff member to complywith this regulation as directed by their manager.
Withdrawal/Payment in Favour of Third Party
Process Steps:
Step 1: Complete Patient Private Property AccountWithdrawal Form (Attached as Appendix 3)
Upon receipt of a request from a client, or on their behalf,for a payment to be made to a third party, by HSE out offunds held in safekeeping, the initial requirement is toensure a Client Private Property Account Withdrawal Formis completed.
This form should be filled in by or on behalf of the client.
If necessary, HSE staff can assist in completing the form.
19
Where a member of HSE staff assists in filling in the formwith the client, at least one other HSE staff member mustbe present.
The form must not be signed by the client until a HSEstaff member is present and witnesses the signing of theform by the client.
Staff members signing as witnesses are solely confirmingthat the client signed the form in their presence and did sowithout any apparent undue influence.
Staff members signing as witnesses are not in any wayconfirming anything in their professional capacity orotherwise as regards the clients understanding of the formor their mental capacity around same.
Step 2: The Patient Private Property AccountWithdrawal Form must be approved
The Patient Private Property Account Withdrawal Formmust be approved by two HSE senior staff members whomay or may not include the same staff member(s) whohas witnessed the signing of the form by the client.
The relevant LHO Manager, upon notification to therelevant Assistant National Director of Finance cannominate additional grades of staff for the purpose ofapproving the withdrawal form however staff at or abovethe following grades are authorised to approve theseforms:
� Clinical Nurse Manager
� Public Health Nurse
� Senior House Officer
� Senior Social Worker
� Senior Therapy Grade
� Grade 5 Clerical/Administrative
Before approving the withdrawal form the twosenior staff members must:
a. Have checked or be familiar with the clients recentmedical history and records and
b. Be familiar with the client’s care or have consultedrelevant clinical staff who are familiar with theclient’s care and
c. Read the request form back to the client and seekhis/her confirmation that he/she understands thewithdrawal form and that the details are correct.
In approving the withdrawal form the two senior HSE staffare recording the following, bearing in mind the need tocomply with a) to c) above:
1. Whether to the best of their knowledge the client isthe subject of an operative Enduring Power ofAttorney or is a Ward of Court? – the withdrawal/payment should only be approved if theanswer to this is NO
2. Whether, based on their professional relationshipwith the client, they have any reason to doubt theclient’s capacity to give informed consent to thethird party withdrawal/payment.– the withdrawal/payment should only be approved if theanswer to this is NO
The two staff approving the withdrawal form mustdo so at the same time.
Step 3 [A] – Processing of Withdrawal Form ifapproved
Once the withdrawal form is approved by both senior staffthe following distribution should take place:
1. Original to be forwarded to clients accounts officeor equivalent for processing
2. First copy to be retained on file at ward.3. Second copy to client.
It should be noted that once the withdrawal form isapproved the primary objective is to carry out the wishesof the client in an efficient manner while complying withbest practice financial controls.
Step 3 [B] – Necessary actions if request not approved
In effect what follows is an iterative process with HSEseeking to deal sensitively with the wishes of clients andtheir relatives/friends. HSE must do this while complyingwith our obligation to protect the funds of clients who lackcapacity to give informed consent to the withdrawalrequest, for the benefit of the client and the client alone.
If either of the two senior staff feel it is not appropriate toapprove the request because of their concerns over theclient’s capacity then it is not possible to process awithdrawal. Discussion with the clients/theirrelatives/friends at that stage may lead to the matter beingresolved by means of the “Reimbursement of Receipts”process
Appendix 1 – Third Party Withdrawals
Patients’ Private Property Guidelines
20
Patients’ Private Property Guidelines
Appendix 1 – Third Party Withdrawals
Note
Further assessment of the client is required if there isa desire to continue with the withdrawal process.
Where practical, non-medical clinical staff withappropriate training and experience may be in aposition to carry out an assessment using one of thevarious client assessment tools in general use such asthe MMSE (Mini Mental State Examination).
Such an assessment, while not a formal MentalCapacity Assessment, may be sufficient to confirm agenuine doubt as to the clients capacity to giveinformed consent or may remove that doubt in themind of the senior staff being requested to approvethe withdrawal.
Where such non-medical assessment confirms thatthere is good reason to doubt the clients capacity togive informed consent to the withdrawal then it is notpossible to process the withdrawal.
Further discussion with the client/their relatives/friendsat that stage may lead to the matter being resolved bymeans of the “Reimbursement of Receipts” process.
A full Mental Capacity Assessment (MCA) of the clientis required if there is a desire to continue with thewithdrawal process.
A MCA can only be carried out by a:
� Consultant Psychiatrist
� Consultant Geriatrician
� Consultant Psycho-Geriatrician
In the event that the MCA confirms that the client hasthe capacity to give consent to the withdrawal thenthe withdrawal can be approved and processed inaccordance with Step 3 A above.
If the MCA determines that the client cannot giveconsent to the withdrawal then HSE cannot processsame and that is the end of the process from HSEperspective.
At this stage the “Reimbursement of Receipts” processshould again be discussed with the client and theirrelatives/friends.
It is a matter for client’s relatives or friends to pursuewhatever course of action they deem appropriatethemselves at this stage.
HSE does not have a legal power to act to pay over aclient’s funds where it has been determined that theclient lacks the capacity to give informed consent tosame.
This applies to any persons including a spouse orchildren whether dependents or not.
If there are any other reasons for not approving therequest, other than a concern over capacity, then the twosenior staff should seek the direction of the Director ofNursing / Medical Director / Manager / Administrator asappropriate.
The client and his next of kin should be appropriatelyinformed at all stages of this process.
Private Nursing Homes
The above requirements are amended as follows whereclients are not being cared for in HSE facilities i.e. are inprivate nursing homes or other externally providedfacilities:
1. The nursing home must arrange for a members ofits staff to witness the signing of the withdrawalform by the client
2. The nursing home must arrange for its senior nurseand its manager to approve the withdrawal form.
Where the nursing home staff approving thewithdrawal forms have reason for concern as to thecapacity of the client to make the request theyshould contact HSE with a view to arranging forassessment of the client.
3. Re-imbursement of Receipts Process
This is a practical alternative to processing lump sumpayments from a client’s funds to a third party.
It is considered appropriate for HSE to ensure clientscan benefit from their funds to the greatest extentpractical and consistent with their care and generalwell being.
Where there is a doubt around a client’s capacity tomanage their own funds it is recommended that
21
relatives/friends who wish to purchase items for thebenefit of clients do so following discussion withrelevant HSE nursing or other staff involved in themanagement of the care of the client.
Where items of genuine benefit to clients arepurchased in good faith by their relatives/friendsthen on completion and approval of the relevantform (attached at Appendix 4) the costs of samecan be reimbursed to the relatives/friends.
Appropriate local professional discretion must beexercised in deciding what can be considered to befor the benefit of clients and to avoid anyinappropriate reimbursements.
Receipts must be provided and must be reviewedand attached to reimbursement request forms.
Reimbursement forms can be approved by any oneof the senior staff listed at Step 2 above and againfurther staff can be authorised to approvereimbursements as indicated therein.
4. Wards of Court/Enduring Power of Attorney (EPA)
Withdrawals or Reimbursements must be approvedin advance by the Wards of Court Office/Committeeof the Ward or by the Attorney appointed by an EPAonce it has been formally registered and isoperative.
Appendix 1 – Third Party Withdrawals
Patients’ Private Property Guidelines
22
Patients’ Private Property Guidelines
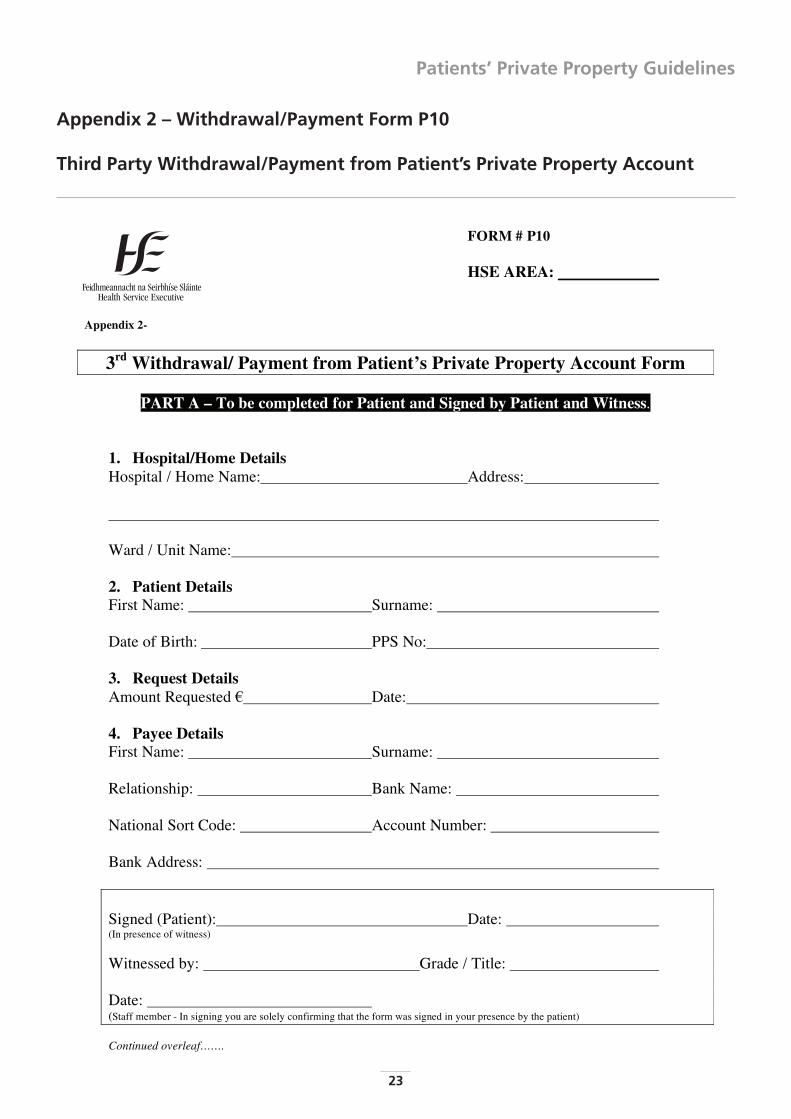
Appendix 2 – Withdrawal/Payment Form P10
Third Party Withdrawal/Payment from Patient’s Private Property Account
23
FORM # P10
HSE AREA:
Appendix 2-
3rd Withdrawal/ Payment from Patient’s Private Property Account Form
PART A – To be completed for Patient and Signed by Patient and Witness.
1. Hospital/Home DetailsHospital / Home Name: Address:
Ward / Unit Name:
2. Patient DetailsFirst Name: Surname:
Date of Birth: PPS No:
3. Request DetailsAmount Requested Date:
4. Payee DetailsFirst Name: Surname:
Relationship: Bank Name:
National Sort Code: Account Number:
Bank Address:
Signed (Patient): Date: (In presence of witness)
Witnessed by: Grade / Title:
Date: (Staff member - In signing you are solely confirming that the form was signed in your presence by the patient)
Continued overleaf…….
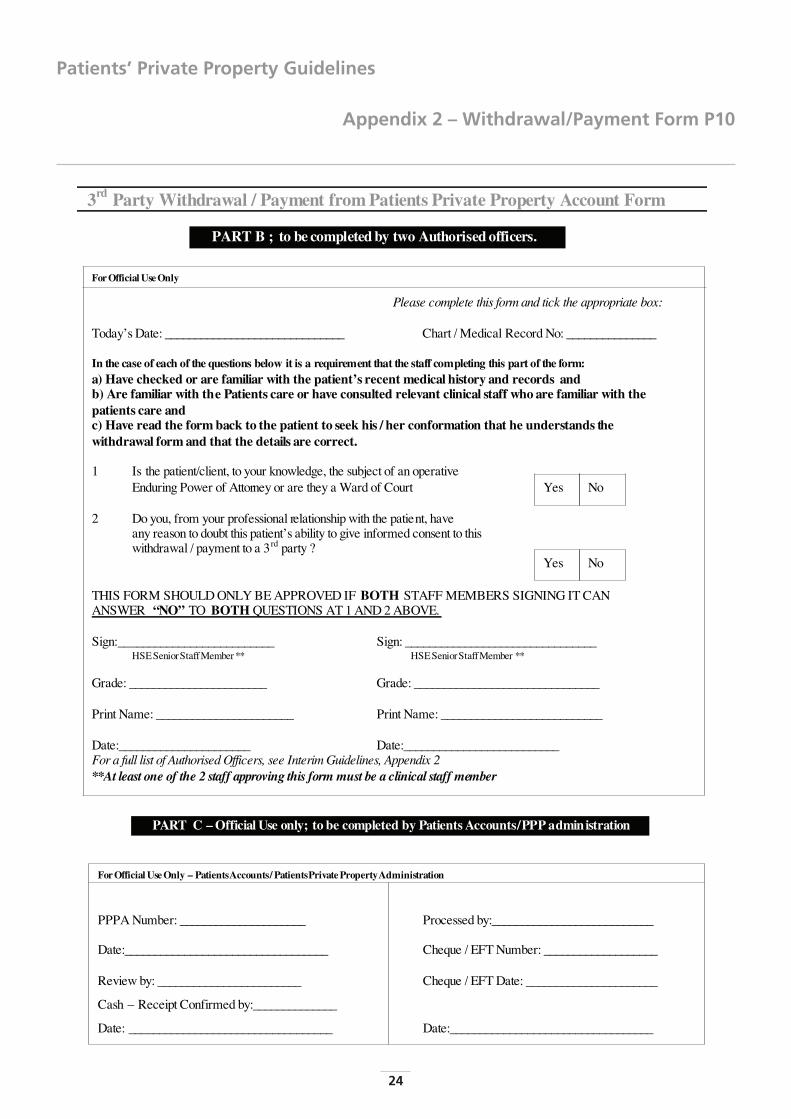
Appendix 2 – Withdrawal/Payment Form P10
Patients’ Private Property Guidelines
24
Patients’ Private Property Guidelines
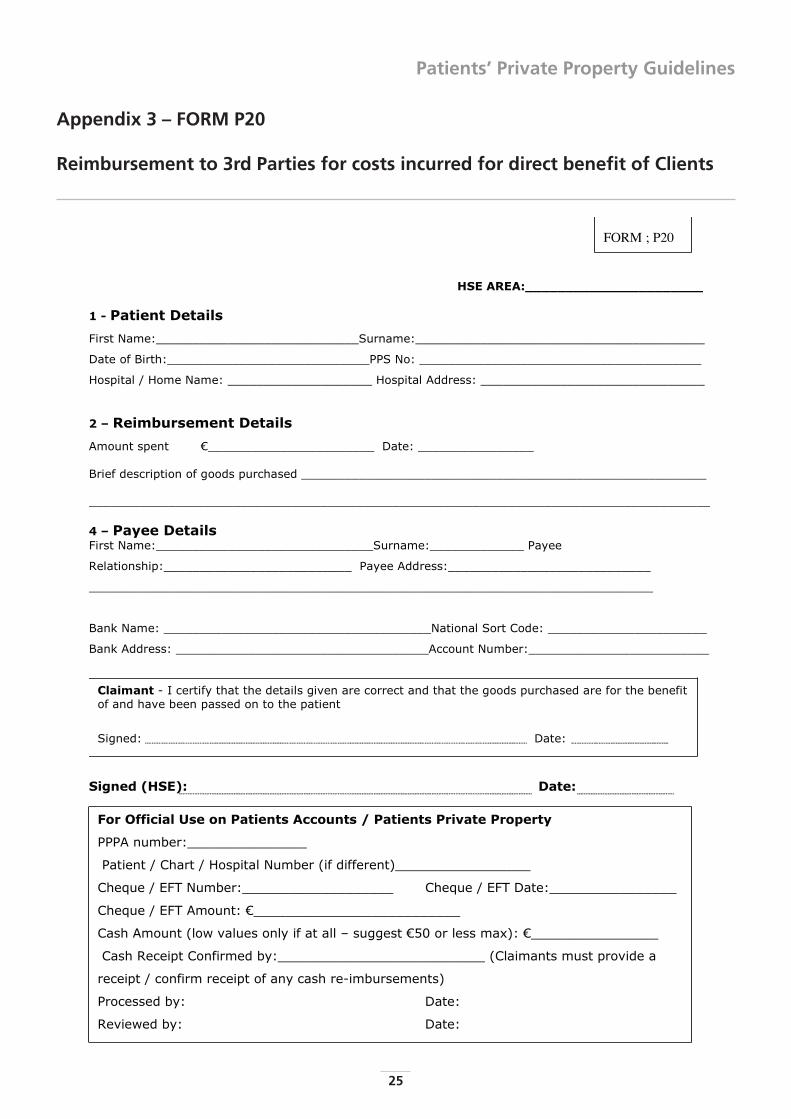
Appendix 3 – FORM P20
Reimbursement to 3rd Parties for costs incurred for direct benefit of Clients
25
HSE AREA:______________________
1 - Patient Details
First Name:____________________________Surname:________________________________________
Date of Birth:____________________________PPS No: _______________________________________
Hospital / Home Name: ____________________ Hospital Address: _______________________________
2 – Reimbursement Details
Amount spent _______________________ Date: ________________
Brief description of goods purchased ________________________________________________________
______________________________________________________________________________________
4 – Payee DetailsFirst Name:______________________________Surname:_____________ Payee
Relationship:__________________________ Payee Address:____________________________
______________________________________________________________________________
Bank Name: _____________________________________National Sort Code: ______________________
Bank Address: ___________________________________Account Number:_________________________
Signed (HSE): Date:
Claimant - I certify that the details given are correct and that the goods purchased are for the benefit of and have been passed on to the patient
Signed: Date:
For Official Use on Patients Accounts / Patients Private Property
PPPA number:_______________
Patient / Chart / Hospital Number (if different)_________________
Cheque / EFT Number:___________________ Cheque / EFT Date:________________
Cheque / EFT Amount: __________________________
Cash Amount (low values only if at all – suggest 50 or less max): ________________
Cash Receipt Confirmed by:__________________________ (Claimants must provide a
receipt / confirm receipt of any cash re-imbursements)
Processed by: Date:
Reviewed by: Date:
FORM ; P20
1) Why can't I withdraw money from my lovedone's PPA? Other families can do it.
A. We have concerns about your loved one'scapacity to consent to this.
B. We provide for all basic needs.
C. Additional items you may feel would bebeneficial to your loved one can be purchasedby you and repaid to you from your loved onesPPA.
D. Purchases should be discussed in advance with amember of the team and you should providereceipts.
E. We can arrange for a team member to discussour assessment of your loved ones capacity Ifyou wish.
2) My relative can sign her name perfectly well onthe withdrawal form. Why aren't you givingme the money.
A. We are concerned that even though yourrelative can sign her name, she may not have thecapacity to understand the financial implicationsof her request.
B. We can arrange for a team member to discussour assessment of your loved ones capacity Ifyou wish.
3) What will happen to the PPA when my relativedies?
A. The account will be closed and the fundshanded over to the legal personal representativeentitled to administer the estate on productionof probate of the will or letters ofadministration.
B. You should contact the probate office or asolicitor for further advice in relation to this.
4) My brother (for example) is written down asthe Next of Kin (N.O.K.) but I should be theN.O.K. because I'm the eldest/am closer to mymother etc
A. Next of kin is a legal term applying to all of yourmother’s blood relatives and we are happy to listyou as next of kin as well in that context.
B. The next of kin/key contact(s) for the purpose of
general matters around your mother’s care is aslightly different matter and is nominated by theclient.
C. If the client has not got full capacity, the next ofkin/ key contact(s) should be agreed by theimmediate family.
D. If your mother has not got full capacity thenmonies in her PPP account will only be paid outon production of receipts for items purchasedfor her direct benefit following discussion inadvance with a member of her care team.
E. Where a client has passed away – see 3 above.
5) Do we have to assess everyone with a PPPAccount if they want to withdraw money?
A. No, only those where we have a doubt abouttheir capacity to consent.
6) What if a client doesn't have a N.O.K.?
A. See 4 above re N.O.K.
B. If the client has capacity, the client can accesstheir account as they wish.
C. A regular visitor/friend etc may, having consultedwith the team in advance, purchase additionalitems for the direct benefit of the client and berepaid for same on production of receipts.
D. If the client has no NOK or visitors a member ofthe team may assess what additionalitems/treats etc over and above what HSE fundsthat the client may benefit from.
E. The team member will arrange purchase andthis can be deducted from the PPPA account.
7) Who should pay for equipment e.g. specialbed, special chair, which might berecommended to improve the comfort andquality of life of a client by, for example, anOccupational Therapist? This equipment maynot be medically necessary. This equipmentmay also be manufactured to individual clients’requirements.
A .If it is medically necessary, it should be providedby the HSE/Service Provider subject to theirrequirement to operate with the limit of theresources available to them.
Appendix 4 – FAQ; “Frequently Asked Questions”
Patients’ Private Property Guidelines
26
Patients’ Private Property Guidelines
Appendix 4 – FAQ
B. Anything that is properly paid for out of thefunds in a PPPA belongs to the specific clientwhose PPPA funded it.
C. Such items must be fully respected as thepersonal property of that client and not in anyway treated by HSE as “generally available” forthe use of clients generally.
8) If a Solicitor states that he is acting for theestate of a deceased client, is it in order toforward a cheque to the Solicitor in the nameof the legal personal reps, where the amount isless than 20,000?
A. The less than 20,000 limit applies in caseswhere it may be possible to pay over monies inthe absence of grant of probate/letters ofadministration.
B. The HSE may consider making such a payment,once we are satisfied that it is a straightforwardcase, as outlined in the Probate Flowchart.
C. In relation to complex cases, the solicitor willneed to produce the written grant of probate orletters of administration before any payment willbe made to him.
D. You should refer all difficult cases to the PPPACentral Unit, Tullamore for further advice.
9) What if a further next of kin presents after HSEhas paid out using the process for accountswith less than 20,000 involving an affidavitand indemnity. Is (a) the indemnity form legallybinding and (b) who pays further next of kin?Is it the first next of kin or is it the H.S.E. whothen recovers from the first next of kin?
A. If such a case arises, contact the PPPA CentralUnit, Tullamore.
B. The “less than €20,000 process” is anaccommodation offered by the HSE – HSE is fullyentitled to insist on grant of probate/letters ofadministration in each and every case andshould always do so where any doubt exists asto potential further next of kin with a betterclaim than those making the request.
C. The affidavit and indemnity will be legallybinding provided it was properly executed whichrequires that the person(s) signing it was fullyand independently informed as to its contentsand the meaning of them.
10) Is it in order to pay funeral bills from the PPPAaccount before issuing the balance to next ofkin?
A. The general principle is that the clients’ legalpersonal representatives/next of kin shouldmake and pay for funeral arrangements.
B. When PPA funds are paid over to the legalpersonal representatives they can deal withwhoever paid for the funeral and repay them asappropriate
C. HSE can pay bills for funeral expenses arrangedby legal personal representatives/next of kin andcharge them against the persons PPPA providedthere is sufficient funds in the PPPA account
D. C. above is limited to the reasonable direct costsof a relatively standard funeral and excludescater/reception costs etc.
E. Only in exceptional circumstances should HSEmake funeral arrangements and the costs ofsame can be charged to the specific clients PPPA– if there are insufficient funds then the balancemust be charged against HSE own funds.
11) What happens my pension when the HSEcashes it each week?
Where appropriate, a maintenance charge isdeducted and the balance is placed in the PPPAaccount or given directly to the client at wardlevel.
12) How do I know the HSE isn't using my moneyfor its own purposes?
A The PPPA accounts are operated in accordancewith legislation and the guidelines issued andare independently audited annually by externalauditors & the C&AG.
B. These guidelines are available on request andspecifically deal with the fact that clients fundsare to be used for the benefit of the client andthe client alone.
C. These guidelines also deal with and separatewhat HSE funds must pay for and what clientsfunds must pay for.
27
13) Does the HSE give me interest on my money?
Interest is credited weekly to all PPP funds heldby the PPPA Central Unit, Tullamore. Local fundsretained to allow for day to day spending do notattract interest.
14) If there is not sufficient funds in the account topay the full funeral bill should it be part paidfrom here and relative informed?
A. The relative should be informed that there is abereavement grant available from theDepartment of Social Protection.
B. In addition the relative could apply to thecommunity welfare service for furtherassistance.
C. See also 10 above.
15) Should next of kin submit a written agreementto allow them purchase items out of the PPPAaccount for the client.
A Prior approval to purchase should be agreedwith the team and receipts must be provided –see also above.
16) Should administration staff look forIdentification from relative when withdrawingmoney.
A The team should use discretion – if the next ofkin is unknown to them, they may ask foridentification where there is a need to do so.
B. HSE preference is to provide withdrawals bycheque to the client who can pass to therelative/other third party or to send by post tothe address listed by the client when theycompleted the withdrawal form.
C. Where the client lacks capacity the only“withdrawal” will be where someone is beingre-imbursed for items purchased for the directbenefit of the client
– the key issue in such cases is did the client getthe item and has a valid receipt been produced
– the I.D. of the person seeking re-imbursementis of secondary importance.
17) When a resident dies, can we give solicitors acopy of the undertaker's bill?
A Yes, provided they are the legal personalrepresentative or acting for them or can showother good cause as to why HSE should do so. .
18) Should we cash the cheques we give to clientsout of the PPP account?
A The handling of cash places an administrative,control and security risk on our already busystaff.
B. Cash payments should be discouraged wherepossible.
Appendix 4 – FAQ
Patients’ Private Property Guidelines
28
Patients’ Private Property Guidelines
Appendix 5 – Probate Forms & DocumentsDeclaration & Deed of Indemnity
29
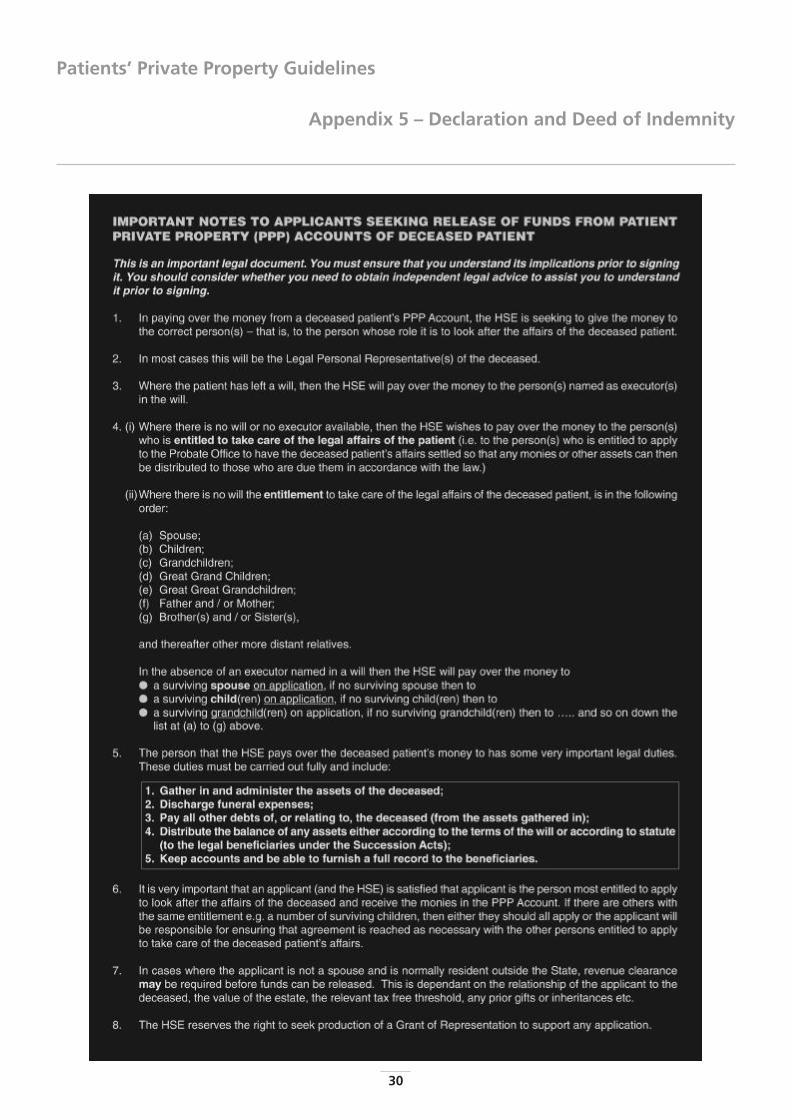
Appendix 5 – Declaration and Deed of Indemnity
Patients’ Private Property Guidelines
30
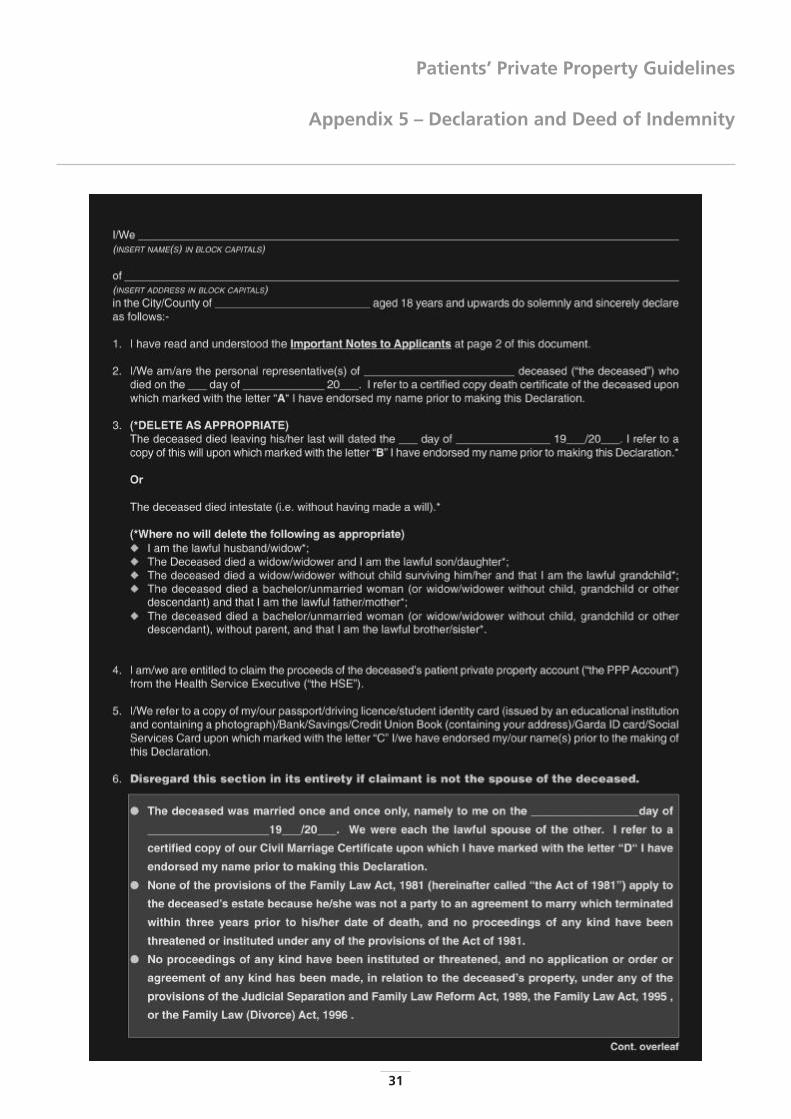
Patients’ Private Property Guidelines
Appendix 5 – Declaration and Deed of Indemnity
31
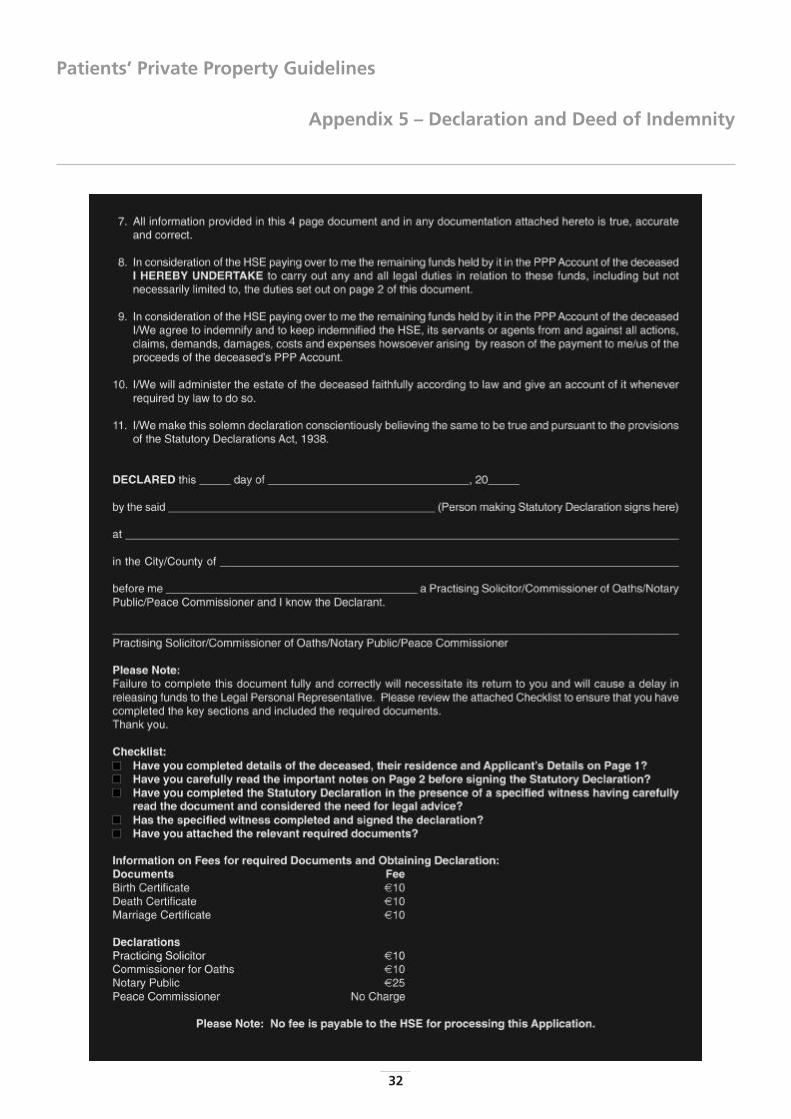
Appendix 5 – Declaration and Deed of Indemnity
Patients’ Private Property Guidelines
32
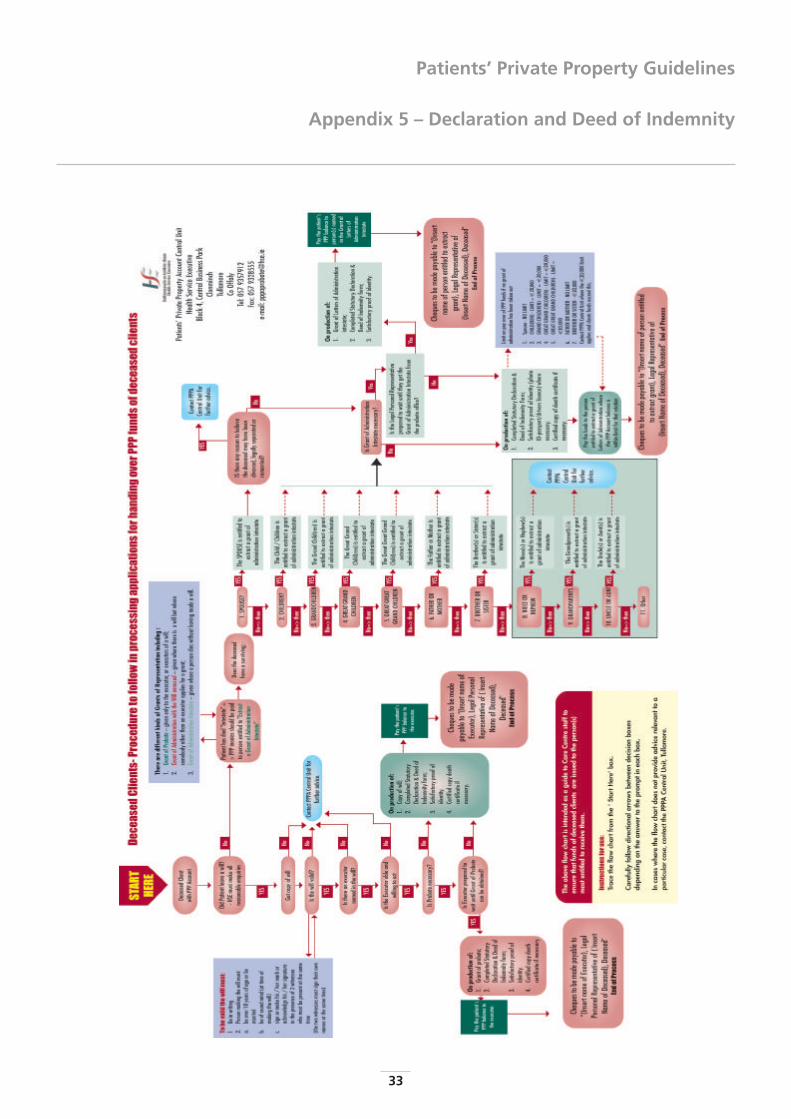
Patients’ Private Property Guidelines
Appendix 5 – Declaration and Deed of Indemnity
33
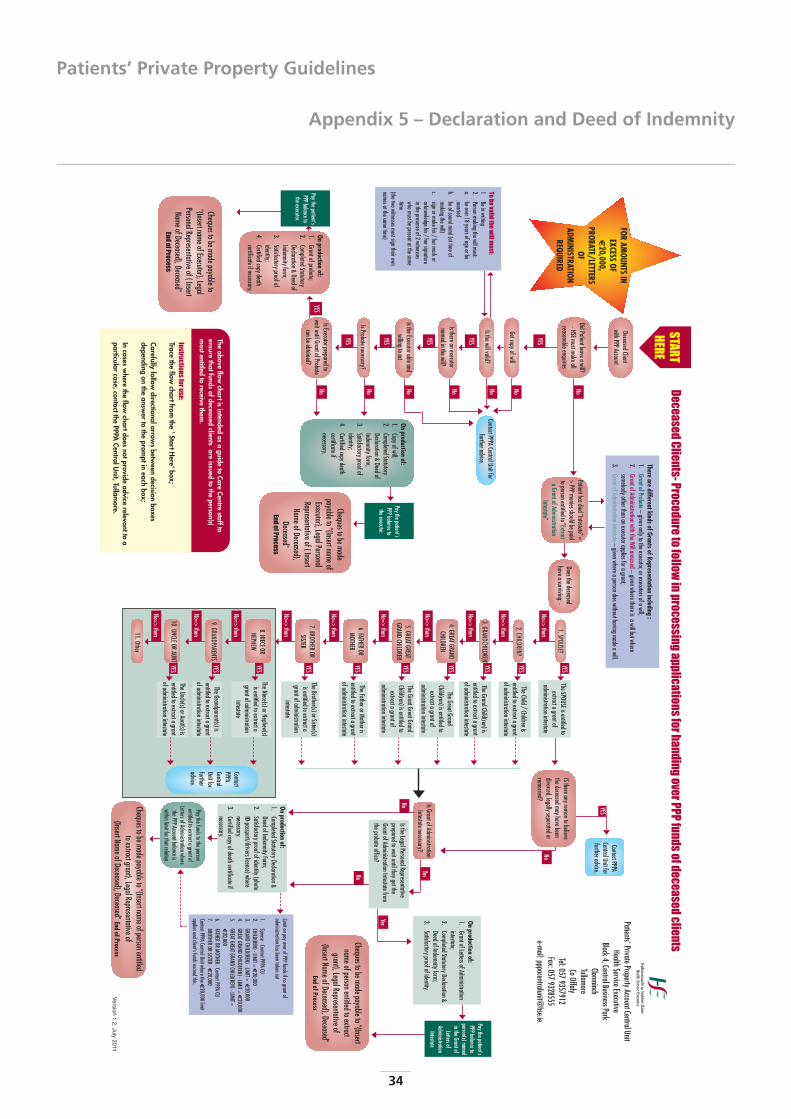
Appendix 5 – Declaration and Deed of Indemnity
Patients’ Private Property Guidelines
34
Yes
No
YES
YES
YES
YES
YES
YES
YES
YES
YES
No=>then
No=>then
No
No
No=>then
No=>then
No=>then
No=>then
No=>then
No=>then
No=>then
NoNoNo
YES
YES
YES
Isthereanexecutornamedinthewill?
YES
Tobevalidthewillmust:
1Beinwriting
2.Personmakingthewillmust:
a.beover18
yearsofageorbemarried
b.beofsoundmind(attimeofmakingthewill)
c.signormakehis/
hermarkoracknowledgehis/
hersignatureinthepresenceof2
witnesseswhomustbepresentatthesametime
(thetwowitnessesmustsigntheirownnamesatthesametime)
DeceasedClientwithPPPAccount
DidPatientleaveawill?-HSEmustmakeallreasonableenquiries
YES
Getcopyofwill
Isthewillvalid?
IstheExecutorableandwillingtoact
IsProbatenecessary?
IsExecutorpreparedtowaituntilGrantofProbate
canbeobtained?
Onproduction
of:1.
Grantofprobate;2.
CompletedStatutoryDeclaration&
DeedofIndemnityform;
3.Satisfactoryproofofidentity;
4.Certifiedcopydeathcertificateifnecessary.
Paythepatient'sPPPbalancetotheexecutor.
Chequestobemadepayableto"{InsertnameofExecutor},LegalPersonalRepresentativeof{InsertNameofDeceased},Deceased"
EndofProcess
Chequestobemadepayableto"{InsertnameofExecutor},LegalPersonalRepresentativeof{InsertNameofDeceased},
Deceased"EndofProcess
No
No=>then
ContactPPPACentralUnitfor
furtheradvice.
Onproduction
of:1.
Copyofwill;2.
CompletedStatutoryDeclaration&
DeedofIndemnityform;
3.Satisfactoryproofofidentity;
4.Certifiedcopydeathcertificateifnecessary.
Thereare
differentkindsofGrantsofRepresentationincluding
:1.
GrantofProbate–givenonlytotheexecutor,orexecutorsofawill;
2.GrantofAdministrationwiththeWillannexed–
givenwherethereisawillbutwhere
somebodyotherthananexecutorappliesforagrant;3.
GrantofAdministrationIntestate–givenwhereapersondieswithouthavingmadeawill.
Patienthasdied"Intestate"=>PPPmoniesshouldbepaid
topersonentitledto"ExtractaGrantofAdministration
Intestate"
Doesthedeceasedhaveasurviving:-
1.SPOUSE?
2.CHILDREN?
3.GRANDCHILDREN
4.GREATGRANDCHILDREN
5.GREATGREATGRAND
CHILDREN
7.BROTHEROR
SISTER
6.FATHEROR
MOTHER
8.NIECEORNEPHEW
9.GRANDPARENTS
10.UNCLEORAUNT
11.Other
TheSPOUSEisentitledtoextractagrantof
administrationintestate
TheChild/Childrenis
entitledtoextractagrantofadministrationintestate
TheGrandChild(ren)isentitledtoextractagrantofadministrationintestate
TheGreatGrandChild(ren)isentitledtoextractagrantof
administrationintestate
TheGreatGreatGrandChild(ren)isentitledtoextractagrantof
administrationintestate
TheFatherorMotherisentitledtoextractagrantofadministrationintestate
TheBrother(s)orSister(s)isentitledtoextractagrantofadministration
intestate
TheNiece(s)orNephew(s)isentitledtoextractagrantofadministration
intestate
TheGrandparent(s)isentitledtoextractagrantofadministrationintestate
TheUncle(s)orAunt(s)isentitledtoextractagrantofadministrationintestate
ISthereanyreasontobelievethedeceasedmayhavebeendivorced,legallyseparatedorremarried?
ContactPPPACentralUnitforfurtheradvice.
IsGrantofAdministrationIntestatenecessary?
IstheLegalPersonalRepresentativepreparedtowaituntiltheygettheGrantofAdministrationIntestatefromtheprobateoffice?
Onproduction
of:1.
GrantofLettersofAdministrationintestate;
2.CompletedStatutoryDeclaration&DeedofIndemnityform;
3.Satisfactoryproofofidentity.
Onproduction
of:1.
CompletedStatutoryDeclaration&DeedofIndemnityForm;
2.Satisfactoryproofofidentity(photoID-passport/driverslicence)wherenecessary.
3.Certifiedcopyofdeathcertificateifnecessary.
LimitonpayoverofPPPfundsifnograntofadministrationhasbeentakenout
1.Spouse-ContactPPPA
CU2.
CHILD(REN)-LIMIT=€20,000
3.GRAND
CHILD(REN)-LIMIT=€20,000
4.GREATGRAND
CHILD(REN)-LIMIT=€20,000
5.GREATGREATGRAND
CHILD(REN)-LIMIT=€20,000
6.FATHER
ORMOTHER
-ContactPPPACU
7.BROTHER
ORSISTER
-€20,000
ContactPPPACentralUnitwherethe
€20,000
limitappliesandclient’sfundsexceedthis.
Patients'PrivatePropertyAccountCentralUnitHealthServiceExecutive
Block4,CentralBusinessParkClonminchTullamoreCoOffaly
Tel:0579357912
Fax:0579328555
e-mail:[email protected]
STARTHERE
NoNoNo
YES
Instructionsforuse:Trace
theflow
chartfromthe
'StartHere'box;
Carefullyfollow
directionalarrows
between
decisionboxes
dependingon
theansw
erto
theprom
ptineach
box;
Incases
where
theflow
chartdoesnotprovide
advicerelevantto
aparticular
case,contactthePPPA
CentralUnit,Tullam
ore.
Theabove
flowchartis
intendedas
aguide
toCare
Centrestaffto
ensurethatfunds
ofdeceasedclients
areissued
tothe
person(s)m
ostentitledto
receivethem
.
DeceasedClients-ProceduretofollowinprocessingapplicationsforhandingoverPPPfundsofdeceasedclients
Paythepatient'sPPPbalancetotheexecutor.
YES
YES
ContactPPPACentralUnitforfurtheradvice.
Yes
Chequestobemadepayableto"{Insertnameofpersonentitledtoextractgrant},LegalRepresentativeof
{InsertNameofDeceased},Deceased"End
ofProcess
Paythefundstothepersonentitledtoextractagrantof
LettersofAdministrationwherethePPPAccountbalanceiswithinlimitforthatrelation
Paythepatient'sPPPbalancetoperson(s)namedintheGrantofLettersof
AdministrationIntestate
Chequestobemadepayableto"{Insertnameofpersonentitledtoextractgrant},LegalRepresentativeof
{InsertNameofDeceased},Deceased"End
ofProcess
FORAM
OUNTSIN
EXCESSOF
€20,000,
PROBATE/LETTERSOF
ADMINISTRATION
REQUIRED
Version
1.2,July2011
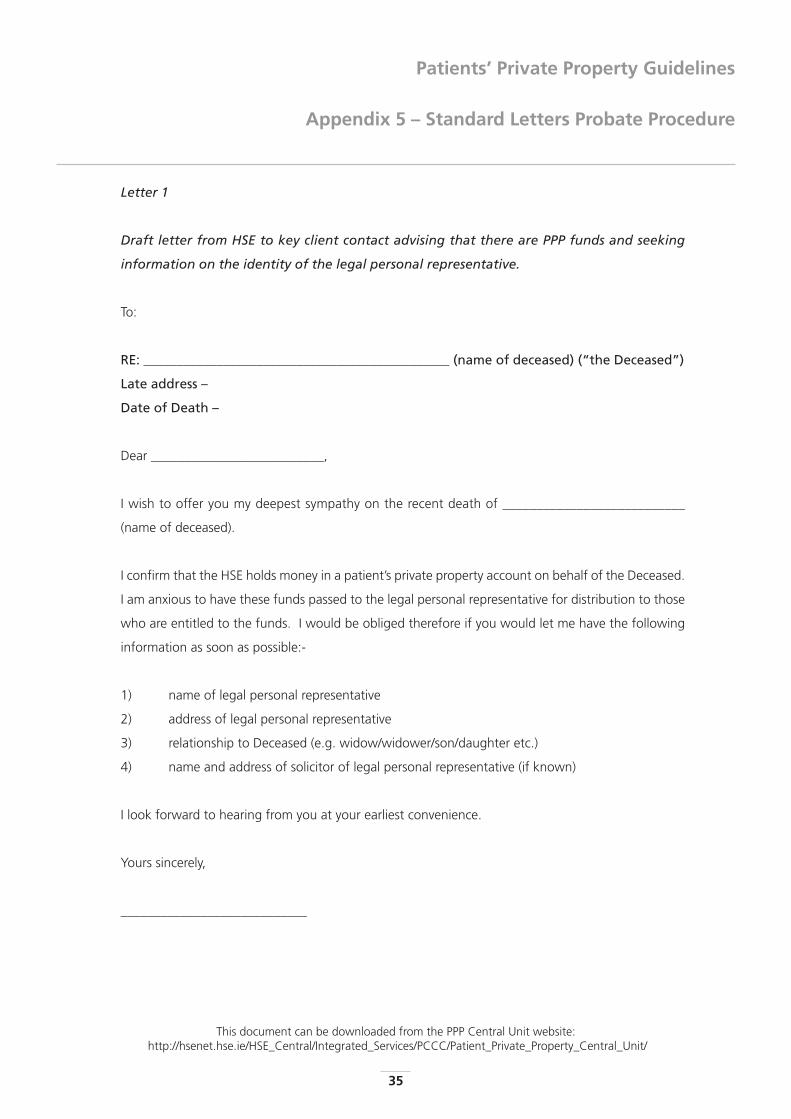
Patients’ Private Property Guidelines
Appendix 5 – Standard Letters Probate Procedure
35
This document can be downloaded from the PPP Central Unit website:http://hsenet.hse.ie/HSE_Central/Integrated_Services/PCCC/Patient_Private_Property_Central_Unit/
Letter 1
Draft letter from HSE to key client contact advising that there are PPP funds and seeking
information on the identity of the legal personal representative.
To:
RE: ______________________________________________ (name of deceased) (“the Deceased”)
Late address –
Date of Death –
Dear __________________________,
I wish to offer you my deepest sympathy on the recent death of ___________________________
(name of deceased).
I confirm that the HSE holds money in a patient’s private property account on behalf of the Deceased.
I am anxious to have these funds passed to the legal personal representative for distribution to those
who are entitled to the funds. I would be obliged therefore if you would let me have the following
information as soon as possible:-
1) name of legal personal representative
2) address of legal personal representative
3) relationship to Deceased (e.g. widow/widower/son/daughter etc.)
4) name and address of solicitor of legal personal representative (if known)
I look forward to hearing from you at your earliest convenience.
Yours sincerely,
____________________________
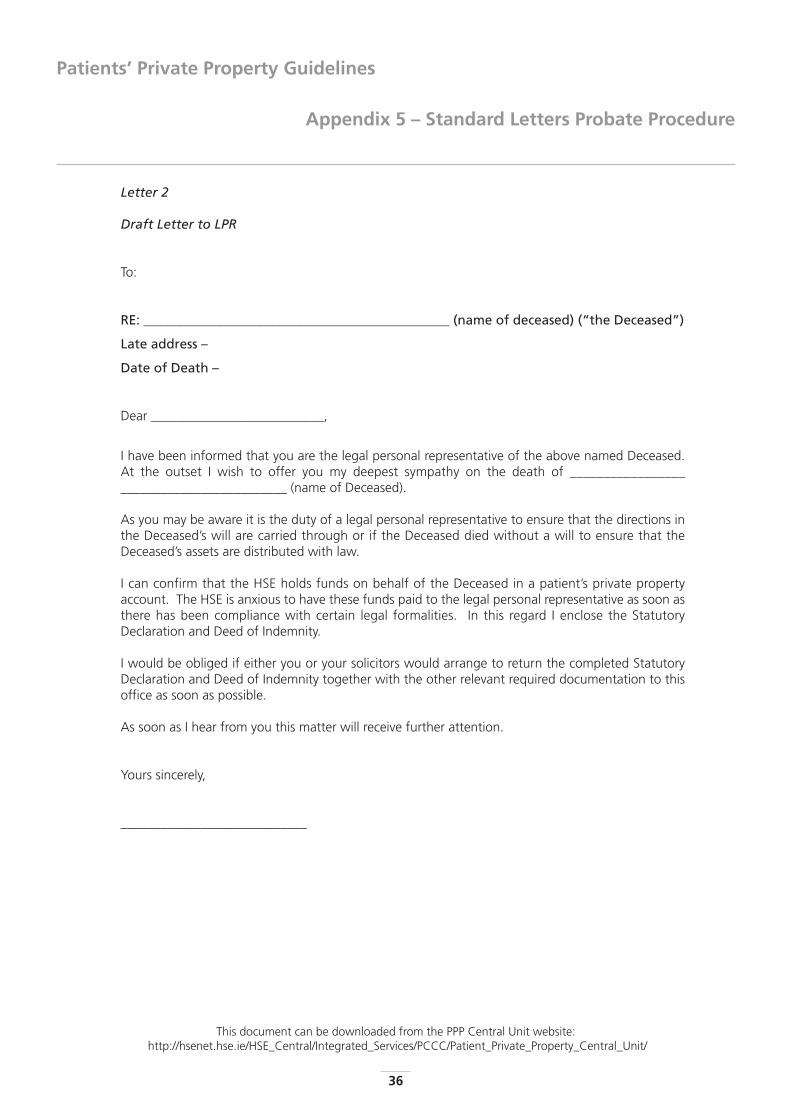
Appendix 5 – Standard Letters Probate Procedure
Patients’ Private Property Guidelines
36
This document can be downloaded from the PPP Central Unit website:http://hsenet.hse.ie/HSE_Central/Integrated_Services/PCCC/Patient_Private_Property_Central_Unit/
Letter 2
Draft Letter to LPR
To:
RE: ______________________________________________ (name of deceased) (“the Deceased”)
Late address –
Date of Death –
Dear __________________________,
I have been informed that you are the legal personal representative of the above named Deceased.At the outset I wish to offer you my deepest sympathy on the death of __________________________________________ (name of Deceased).
As you may be aware it is the duty of a legal personal representative to ensure that the directions inthe Deceased’s will are carried through or if the Deceased died without a will to ensure that theDeceased’s assets are distributed with law.
I can confirm that the HSE holds funds on behalf of the Deceased in a patient’s private propertyaccount. The HSE is anxious to have these funds paid to the legal personal representative as soon asthere has been compliance with certain legal formalities. In this regard I enclose the StatutoryDeclaration and Deed of Indemnity.
I would be obliged if either you or your solicitors would arrange to return the completed StatutoryDeclaration and Deed of Indemnity together with the other relevant required documentation to thisoffice as soon as possible.
As soon as I hear from you this matter will receive further attention.
Yours sincerely,
____________________________
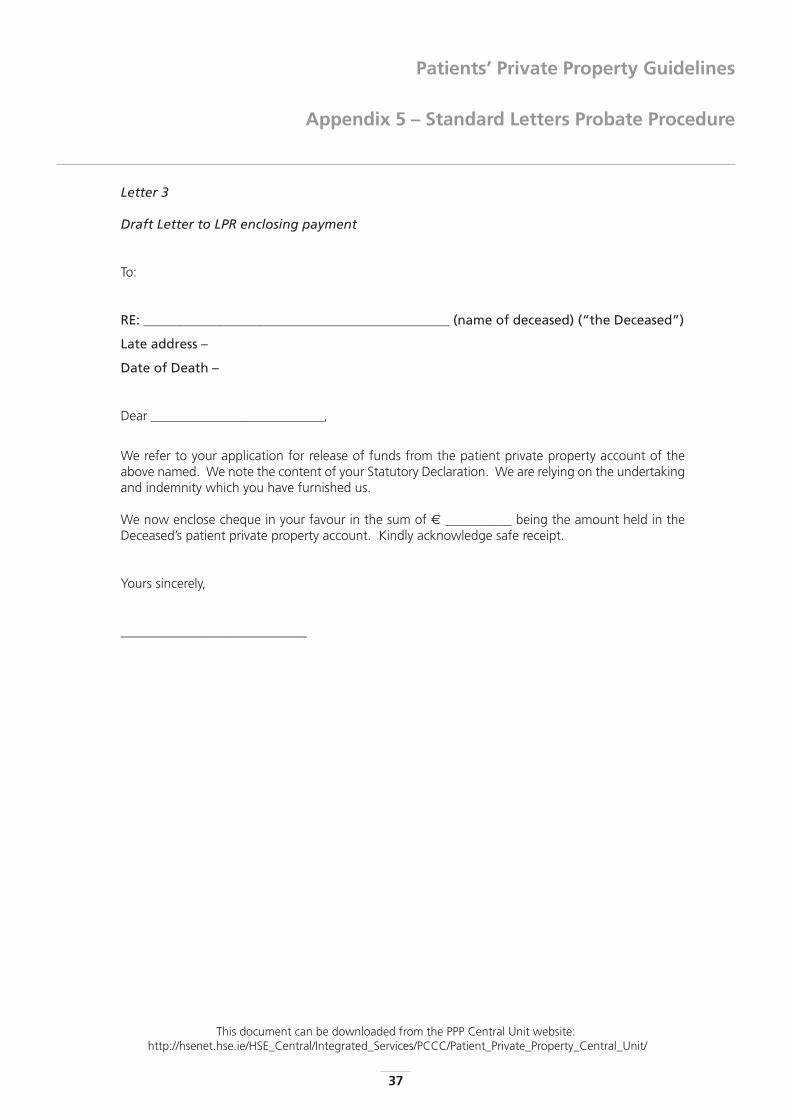
Patients’ Private Property Guidelines
Appendix 5 – Standard Letters Probate Procedure
37
This document can be downloaded from the PPP Central Unit website:http://hsenet.hse.ie/HSE_Central/Integrated_Services/PCCC/Patient_Private_Property_Central_Unit/
Letter 3
Draft Letter to LPR enclosing payment
To:
RE: ______________________________________________ (name of deceased) (“the Deceased”)
Late address –
Date of Death –
Dear __________________________,
We refer to your application for release of funds from the patient private property account of theabove named. We note the content of your Statutory Declaration. We are relying on the undertakingand indemnity which you have furnished us.
We now enclose cheque in your favour in the sum of € __________ being the amount held in theDeceased’s patient private property account. Kindly acknowledge safe receipt.
Yours sincerely,
____________________________
Appendix 5 – Standard Letters Probate Procedure
Patients’ Private Property Guidelines
38
This document can be downloaded from the PPP Central Unit website:http://hsenet.hse.ie/HSE_Central/Integrated_Services/PCCC/Patient_Private_Property_Central_Unit/
Letter 3
Draft Letter to Solicitor for LPR sending cheque
To:
RE: ______________________________________________ (name of deceased) (“the Deceased”)
Late address –
Date of Death –
Dear __________________________,
We refer to your client’s application for release of funds from the patient private property account ofthe above named deceased. We are relying on the Statutory Declaration furnished and in particularthe undertaking and indemnity contained therein.
We now enclose cheque for € __________ in favour of the legal personal representative. We wouldbe obliged if you would kindly acknowledge safe receipt.
Yours sincerely,
____________________________
Patients’ Private Property Guidelines
Appendix 6 – Flowcharts & FormsKey Client Contact Nomination Form
39
This document can be downloaded from the PPP Central Unit website:http://hsenet.hse.ie/HSE_Central/Integrated_Services/PCCC/Patient_Private_Property_Central_Unit/
Insert Care Centre
Name and Address here
To Whom It May Concern:
I, ___________________________________________________ (Client name), hereby appoint
1 Name ______________________________________________________________________________________
Address _____________________________________________________________________________________
2 Name ______________________________________________________________________________________
Address _____________________________________________________________________________________
3 Name ______________________________________________________________________________________
Address _____________________________________________________________________________________
as my Key Client Contact(s) in respect of the administration of my Patient’s Private Property Account, held by the HSE.
I understand that the Key Client Contact(s) named above is/are the person(s) who normally liaise(s) with HSE staff
on my care and I authorise the HSE to share relevant information with him/her/them to allow my Patient’s Private
Property Account be best used for my benefit. All decisions in respect of my PPP account will be made by me.
The Key Client Contact(s) will not have the authority to instruct the HSE to transfer funds from my PPP account or
to instruct that items or services be purchased.
Signed: __________________________________________________
Date: __________________________________________________
Witnessed by: __________________________________________________ (HSE Staff member)
Date: __________________________________________________

Appendix 6 – Process for deciding on use of client PPP Funds - Flowchart
Patients’ Private Property Guidelines
40
PPPW
orkingGroup
No
te:
Thisflowchartm
ustonlybeused
inconjunction
withthe
HSEPPP
guidelines.
SpendingofclientPPP
fundsinexcessof€5,000
peryearbytheHSE
requiresthepriordirection
oftheCircuitCourt.
TheHSE
makesa
decisionto
spendclientfunds
on
lywhen
aclientisunable
tom
anagetheirown
financialaffairs.
Approvaltouse
clientPPPfundsfortheirbenefit
IsResidentcompetentto
spendown
money?
Whatisthe
decisionregarding
competency?
(SeeSection
7PPP
Guidelines)
Whatis/are
thereason(s)
forspendingclients
money?
SeeSection
7ofPPP
Guidelines.
NotCompetent
NotSureSee
Section7
ofPPPGuidelines
Yes,com
petent
Residentableto
accesstheirown
PPPfunds.
EndofProcess
YesCom
p etent
NotCom
petent
HSEFunded
PatientCareItem
ClientFundedPatientCom
fortItem
Resident'sownm
oneyisaccessed
subjecttocourt
approval,ifrequired,anddocum
ented.End
ofProcessf
HSEpaysforitem
(s)/service
(locallyfunded).End
ofProcess InformKey
ClientContact
StartHere
Isspendingconsistent
withCare
Plan?
YesNo
ShouldCare
Planbe
reviewedto
accomm
odatesuggestions?
ClientPPPfundscannotbe
spentinthiscase.
EndofProcess
NoYes
PPPACentralUnit,Tullam
ore
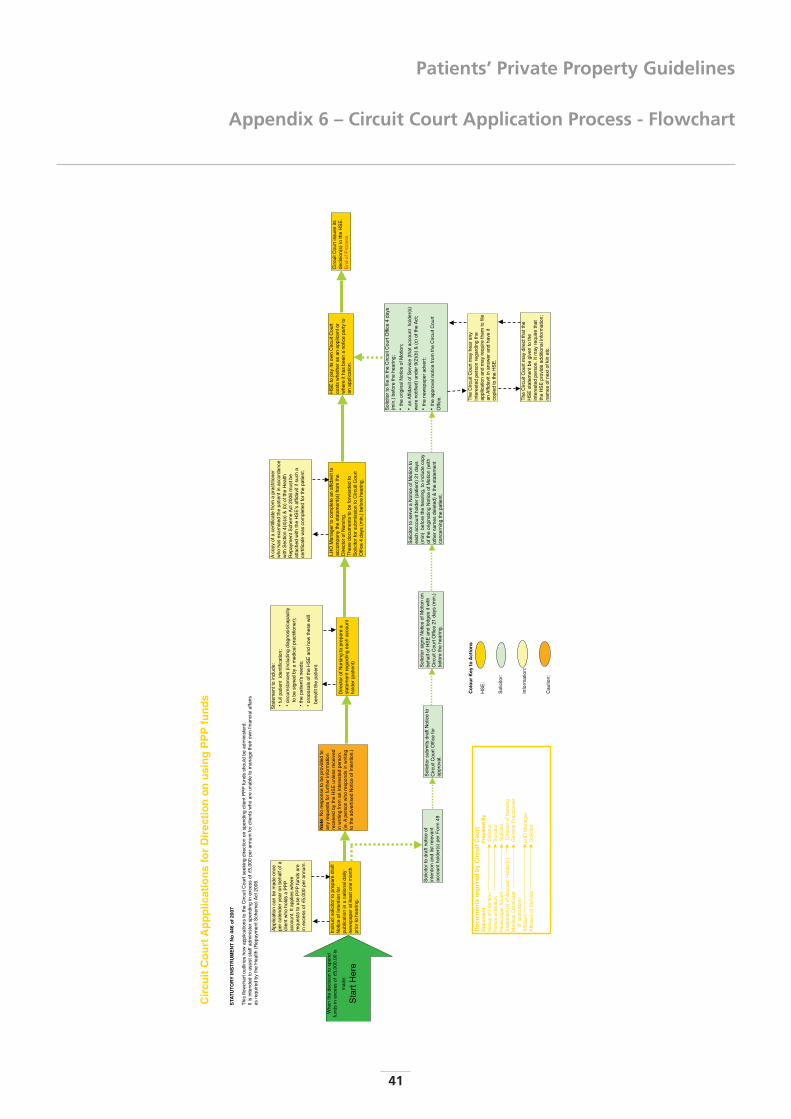
Patients’ Private Property Guidelines
Appendix 6 – Circuit Court Application Process - Flowchart
41
Cir
cuit
Co
urt
Ap
pp
licat
ion
sfo
rD
irec
tio
no
nu
sin
gP
PP
fun
ds
STA
TU
TOR
YIN
ST
RU
ME
NT
No
446
of
2007
This
flowc
hart
outlin
esho
wap
plica
tions
toth
eCi
rcuit
Cour
tsee
king
direc
tion
onsp
endin
gcli
entP
PPfu
ndss
hould
bead
mini
sterd
.It
isint
ende
dto
assis
tsta
ffadm
iniste
rspe
nding
inex
cess
of€5
,000
pera
nnum
forc
lient
swho
are
unab
leto
man
age
their
own
finan
ciala
ffairs
asre
quire
dby
the
Healt
h(R
epay
men
tSch
eme)
Act2
006.
Co
lou
rK
eyto
Act
ion
s
HSE:
Solic
itor:
Info
rmat
ion:
Caut
ion:
Instr
ucts
olicit
orto
prep
are
draf
tNo
tice
ofIn
tent
ionfo
rpu
blica
tion
ina
natio
nald
aily
news
pape
ratle
asto
nem
onth
prior
tohe
aring
.
Solic
itors
ubm
itsdr
aftN
otice
toCi
rcuit
Cour
tOffic
efo
rap
prov
al.
Appli
catio
nca
nbe
mad
eon
cepe
rcale
nder
year
onbe
halfo
facli
entw
hoho
ldsa
PPP
acco
unt.
Itap
plies
wher
ere
ques
tsto
use
PPP
fund
sare
inex
cess
of€5
,000
pera
nnum
.
No
te:N
ore
spon
seto
bepr
ovide
dto
anyr
eque
stsfo
rfur
ther
infor
mat
ionre
ceive
dby
the
HSE
unles
srec
eived
inwr
iting
from
anint
eres
ted
pers
on.
(ie.A
pers
onwh
ore
spon
dsin
writin
gto
the
adve
rtise
dNo
tice
ofIn
tent
ion.)
Solic
itors
ignsN
otice
ofM
otion
onbe
halfo
fHSE
and
lodge
sitw
ithCi
rcuit
Cour
tOffic
e21
days
(min.
)be
fore
the
hear
ing.
Stat
emen
tto
includ
e:•fu
llpat
ient
ident
ificat
ion;
• circ
umsta
nces
(inclu
ding
diagn
osis/
capa
city
tobe
signe
dby
am
edica
lpra
ctitio
ner);
•the
patie
nt's
need
s;•p
ropo
sals
ofth
eHS
Ean
dho
wth
ese
will
Dire
ctoro
fNur
sing
topr
epar
ea
state
men
treg
ardin
gea
chac
coun
tho
lder(
patie
nt)
LHO
Man
ager
toco
mple
tean
affida
vitto
acco
mpa
nyth
esta
tem
ent(s
)fro
mth
eDi
recto
rofN
ursin
g.Th
ese
docu
men
tsto
befo
rwar
ded
toSo
licito
rfor
subm
ission
toCi
rcuit
Cour
tOf
fice
4da
ys(m
in.)b
efor
ehe
aring
.
Solic
itort
ose
rve
aNo
tice
ofM
otion
toea
chac
coun
thold
er(p
atien
t)21
days
(min)
befo
reth
ehe
aring
,to
includ
eco
pyof
the
origi
natin
gNo
tice
ofM
otion
(with
othe
rnam
esde
leted
)&th
esta
tem
ent
conc
ernin
gth
epa
tient
.
Solic
itort
ofile
inth
eCi
rcuit
Cour
tOffic
e4
days
(min.
)bef
ore
the
hear
ing;
•the
origi
nalN
otice
ofM
otion
;•a
nAffid
avito
fSer
vice
(that
acco
unt
holde
r(s)
were
notifi
ed)u
nder
9(2)
(b)&
(c)o
fthe
Act;
•the
news
pape
radv
ert;
• the
appr
oval
notic
efro
mth
eCi
rcuit
Cour
tOf
fice.
Aco
pyof
ace
rtific
ate
from
apr
actiti
oner
who
hase
xam
ined
the
patie
ntin
acco
rdan
cewi
thSe
ction
4(4)
(a)&
(b)o
fthe
Healt
hRe
paym
entS
chem
eAct
2006
mus
tbe
atta
ched
with
the
HSE'
saffid
aviti
fsuc
ha
certi
ficat
ewa
scom
plete
dfo
rthe
patie
nt.
HSE
topa
yits
own
Circ
uitCo
urt
costs
whet
hera
san
appli
cant
orwh
ere
ithas
been
ano
tice
party
toan
appli
catio
n.
The
Circ
uitCo
urtm
ayhe
aran
yint
eres
ted
pers
onre
gard
ingth
eap
plica
tion
and
may
requ
ireth
emto
filean
Affid
aviti
nan
swer
and
have
itco
pied
toth
eHS
E.
The
Circ
uitCo
urtm
aydir
ectt
hatt
heHS
Esta
tem
entb
egiv
ento
the
inter
este
dpe
rson
.Itm
ayre
quire
that
the
HSE
prov
idead
dition
alinf
orm
ation
;na
mes
ofne
xtof
kinet
c.
Solic
itort
odr
aftn
otice
ofint
entio
nan
dlis
trele
vant
acco
unth
older
(s)p
erFo
rm49
Whe
nth
ede
cision
tosp
end
fund
sin
exce
ssof€5
,000
.00
ism
ade:
Star
tHer
e
Do
cum
ents
req
uir
edb
yC
ircu
itC
ou
rtD
ocu
men
tP
rep
ared
By
Notic
eof
Inte
ntion
Solic
itor
Notic
eof
Mot
ionSo
licito
rNe
wspa
perA
dver
tSo
licito
rSt
atem
ent(s
)ofA
ccou
ntHo
lder(s
)Di
recto
rofN
ursin
gM
edica
lCer
tifica
teGe
nera
lPra
ctitio
ner
(Ifap
plica
ble)
Affid
avit
LHO
Man
ager
Affid
avito
fSer
vice
Solic
itor
Circ
uitCo
urtis
sues
itsde
cision
(s)t
oth
eHS
E.En
dof
Proc
ess
bene
fitth
epa
tient
.
Notes
Patients’ Private Property Guidelines
42
Patients’ Private Property Guidelines
Notes
43
Notes
Patients’ Private Property Guidelines
44

Printed by HSE Print & Design Tel: (01) 626 3447 Fax: (01) 626 3159 E-mail: [email protected]













![Welcome [unisonfgpartners.com.au]unisonfgpartners.com.au/pdf/FINDEX-FMGMT.pdf4.0 1.0 1.0 1.0 1.0 1.0 1.0 50.0 43.5 34.5 25.5 12.5 5.5 9.0 9.0 8.0 7.0 5.0 2.0 5.0 5.0 5.0 5.0 5.0 14.0](https://img.pdfslide.us/doc/110x75/5f9881d4934d305cce543099/welcome-40-10-10-10-10-10-10-500-435-345-255-125-55-90-90-80.jpg)















