Embed Size (px)
Citation preview

Patients With Traumatic Patients With Traumatic InjuriesInjuries
Condell Medical CenterCondell Medical CenterEMS SystemEMS SystemECRN PacketECRN Packet
CE Module II 2008CE Module II 2008
Prepared by: Sharon Hopkins, RN, BSN, EMT-P

Viewing Packets on the Viewing Packets on the WebsiteWebsite• To see the packet in larger print or to review To see the packet in larger print or to review
the packet and you no longer have a paper the packet and you no longer have a paper copy, go to the Condell websitecopy, go to the Condell website
• www.condell.org/emergency/www.condell.org/emergency/• On right side of page choose “ECRN CE”On right side of page choose “ECRN CE”• This will take you immediately to the CE This will take you immediately to the CE
page and then choose your year and module.page and then choose your year and module.• Contact your EMS office for a copy of the Contact your EMS office for a copy of the
quiz.quiz.• You must complete 4 modules per year to You must complete 4 modules per year to
maintain current ECRN licensuremaintain current ECRN licensure

ObjectivesObjectives
• Upon successful completion of this Upon successful completion of this module, the ECRN should be able to:module, the ECRN should be able to:– Identify the differences between a Identify the differences between a
Category I, II and III trauma patientCategory I, II and III trauma patient– State EMS pre-hospital transport State EMS pre-hospital transport
decisions for trauma patients based on decisions for trauma patients based on Region X guidelinesRegion X guidelines
– Understand what the mechanism of Understand what the mechanism of injury is and the information it providesinjury is and the information it provides
– Understand the difference between the Understand the difference between the index of suspicion and the general index of suspicion and the general impressionimpression

Objectives cont’dObjectives cont’d– Describe assessment and field treatment Describe assessment and field treatment
appropriate for the patient with traumatic appropriate for the patient with traumatic insult based on Region X SOP’sinsult based on Region X SOP’s•Burns, tension pneumothorax, sucking chest Burns, tension pneumothorax, sucking chest
wound, flail chest, pericardial tamponade, wound, flail chest, pericardial tamponade, eviscerated organseviscerated organs
– Understand where the landmark for chest Understand where the landmark for chest needle decompressionneedle decompression
– Review trauma scenariosReview trauma scenarios– Successfully calculate the GCS and RTS given Successfully calculate the GCS and RTS given
the patient’s parametersthe patient’s parameters– Identify and appropriately state interventions Identify and appropriately state interventions
for a variety of EKG rhythmsfor a variety of EKG rhythms– Identify ST elevation on a 12 lead EKGIdentify ST elevation on a 12 lead EKG– Successfully complete the quiz with a score of Successfully complete the quiz with a score of
80% or better80% or better

Leading Causes of DeathLeading Causes of Death
• In the age groups from 1 to 44, unintentional In the age groups from 1 to 44, unintentional injury is the leading cause of deathinjury is the leading cause of death
• 45 and over, the leading causes of death are 45 and over, the leading causes of death are diseasedisease– cardiovascular disease and cancerscardiovascular disease and cancers
• These statistics point to a financial burden These statistics point to a financial burden placed on the patient as well as society for placed on the patient as well as society for unintentional injuriesunintentional injuries
• Source: National Vital Statistics System, National Center for Source: National Vital Statistics System, National Center for Health Statistics, CDCHealth Statistics, CDC

Level I Trauma Centers Level I Trauma Centers • Prepared and committed to handle all Prepared and committed to handle all
types of specialty trauma 24/7types of specialty trauma 24/7• Provides leadership and resources to Provides leadership and resources to
other levels of trauma care in the other levels of trauma care in the RegionRegion
• Participates in data collection, research, Participates in data collection, research, continuing education, and public continuing education, and public education programseducation programs
• Level I Region X: Evanston Hospital, St. Level I Region X: Evanston Hospital, St. Francis in EvanstonFrancis in Evanston
• Level I non-Region X: Advocate Level I non-Region X: Advocate Lutheran General, Froedtert (Wisconsin) Lutheran General, Froedtert (Wisconsin)

Level II Trauma CentersLevel II Trauma Centers
• Increased commitment to trauma care Increased commitment to trauma care for the most common trauma for the most common trauma emergencies with surgical capability emergencies with surgical capability available 24/7available 24/7
• Participates in data collection, continuing Participates in data collection, continuing education, and public education education, and public education programsprograms
• Level II in Region X: Condell, Glenbrook, Level II in Region X: Condell, Glenbrook, Highland Park, Lake Forest, Rush North Highland Park, Lake Forest, Rush North Shore, Vista Medical Center East (VMH)Shore, Vista Medical Center East (VMH)

Additional Level II Trauma Additional Level II Trauma Centers - Not Centers - Not Geographically In Region XGeographically In Region X
• Centegra – McHenry, IllinoisCentegra – McHenry, Illinois
• Good Shepherd Hospital (GSH) – Good Shepherd Hospital (GSH) – Barrington, IllinoisBarrington, Illinois
• Northwest Community Hospital Northwest Community Hospital (NWCH) – Arlington Heights(NWCH) – Arlington Heights

Region X SOP -Trauma Region X SOP -Trauma TransportTransport
•Systolic B/P Systolic B/P << 90 on 2 90 on 2 consecutive readings (or peds consecutive readings (or peds << 80) 80)– Transport to the Transport to the highest levelhighest level Trauma CenterTrauma Center within 25 within 25 minutesminutes
– 25 minute clock starts from the 25 minute clock starts from the time of injurytime of injury

Region X SOP Trauma Region X SOP Trauma TransportTransport•Traumatic arrest, isolated burns >20%Traumatic arrest, isolated burns >20%
– Transport to the Transport to the closestclosest Trauma Trauma CenterCenter
•No airway No airway – Transport to the Transport to the closest closest Emergency DepartmentEmergency Department

Hospital on By-passHospital on By-pass
The closest appropriate The closest appropriate hospital must still accept hospital must still accept
any patient in a life-any patient in a life-threatening condition even threatening condition even
if they are on by-passif they are on by-pass

Region X SOP Trauma Region X SOP Trauma TransportTransport•Category ICategory I Trauma Patient Trauma Patient
– Unstable vital signsUnstable vital signs– Based on anatomy of the injuryBased on anatomy of the injury– Transport to the Transport to the highest levelhighest level Trauma CenterTrauma Center within 25 within 25 minutesminutes
– 25 minute clock starts from the 25 minute clock starts from the time of injurytime of injury

Region X SOP Trauma Region X SOP Trauma TransportTransport•Category IICategory II Trauma Patient Trauma Patient
– Based on mechanism of injuryBased on mechanism of injury
•High potential for injury but patient is High potential for injury but patient is stable for nowstable for now
– Based on existence of co-morbid factors Based on existence of co-morbid factors that increase the risk of complications to that increase the risk of complications to recoveryrecovery
– Transport to the Transport to the closestclosest Trauma CenterTrauma Center

Region X SOP Trauma Region X SOP Trauma TransportTransport• Category IIICategory III Trauma Patient Trauma Patient
– All other traumatic injuries and All other traumatic injuries and where routine care is being providedwhere routine care is being provided
– Isolated traumatic injury (generally Isolated traumatic injury (generally GCS >10)GCS >10)•Isolated fracturesIsolated fractures•Minor burnsMinor burns•LacerationsLacerations
– Transport the patient to the Transport the patient to the closestclosest Trauma CenterTrauma Center

Transport DecisionsTransport Decisions
When possible, EMS and When possible, EMS and Medical Control are to Medical Control are to
honor the patient’s honor the patient’s request for hospital request for hospital
destinationdestination

Mechanism of InjuryMechanism of Injury
• The process and forces that cause The process and forces that cause traumatrauma
• Mentally recreate the incident from Mentally recreate the incident from the evidence notedthe evidence noted
• Identify strength of forces involvedIdentify strength of forces involved• Identify direction forces came fromIdentify direction forces came from• Identify areas of the patient’s body Identify areas of the patient’s body
most likely affected by the forcesmost likely affected by the forces• Start to identify the mechanism of Start to identify the mechanism of
injury during the scene size-upinjury during the scene size-up

Accepting The Radio ReportAccepting The Radio Report
• Start forming a mental picture as you Start forming a mental picture as you receive reportreceive report
• You are mentally forming an opinion You are mentally forming an opinion based on mechanism of injurybased on mechanism of injury
• You’ll think differently for the patient You’ll think differently for the patient who fell 5 feet versus 30 feetwho fell 5 feet versus 30 feet
• Form a general impression based on Form a general impression based on the paramedic report of mechanism the paramedic report of mechanism of injury with their field assessmentof injury with their field assessment

Injury Patterns – PedestriansInjury Patterns – Pedestrians
• AdultsAdults– Generally turn away & present lateral Generally turn away & present lateral
surfacessurfaces– Anatomically, impact is low on the bodyAnatomically, impact is low on the body– Injuries to tibia, fibula, femur, knee, lateral Injuries to tibia, fibula, femur, knee, lateral
chest, upper extremity, then head & neckchest, upper extremity, then head & neck• PediatricsPediatrics
– Generally turn and face the vehicleGenerally turn and face the vehicle– Injuries anatomically higher on the body Injuries anatomically higher on the body
than adultsthan adults– Injuries to femur, pelvis and then those Injuries to femur, pelvis and then those
sustained when run over or pushed aside sustained when run over or pushed aside by the vehicleby the vehicle

Injury Patterns – Motor Injury Patterns – Motor VehicleVehicle• Rotational (38% of MVC)Rotational (38% of MVC)
– Injuries similar to frontal & lateralInjuries similar to frontal & lateral– Deceleration is usually more gradual & Deceleration is usually more gradual &
injuries less serious although the vehicles injuries less serious although the vehicles look worselook worse
• Frontal (32% of MVC)Frontal (32% of MVC)– Up and over the steering wheel pathwayUp and over the steering wheel pathway
•Femur fracturesFemur fractures•Blunt abdominal injury via compressionBlunt abdominal injury via compression•Lower chest injuries after steering wheel Lower chest injuries after steering wheel
impactimpact•Head & neck injuries with windshield Head & neck injuries with windshield
impactimpact

Injury Patterns – Motor Injury Patterns – Motor VehicleVehicle
– Down and under the dashboard pathwayDown and under the dashboard pathway•Lower leg injuries from sliding under the Lower leg injuries from sliding under the
dashdash•Chest injuries with steering wheel impactChest injuries with steering wheel impact•Collapsed lungs from breath holding at Collapsed lungs from breath holding at
time of impacttime of impact– EjectionEjection
•27% of fatalities 27% of fatalities •2 impacts – with interior vehicle & then 2 impacts – with interior vehicle & then
the objects outside the car (ground, trees, the objects outside the car (ground, trees, fences, etc)fences, etc)

Injury Patterns – Motor Injury Patterns – Motor VehicleVehicle• Lateral impact – T-bone (15% of MVC; 22% Lateral impact – T-bone (15% of MVC; 22%
of all MVC fatalities)of all MVC fatalities)– Much less structural steel for protection between Much less structural steel for protection between
victim and impact site victim and impact site – Vehicle damage may not look severe but internal Vehicle damage may not look severe but internal
injury potential is highinjury potential is high– Upper & lower extremity fractures on impact sideUpper & lower extremity fractures on impact side– Lateral compression with a large amount of Lateral compression with a large amount of
internal injury to chest & abdominal organsinternal injury to chest & abdominal organs– Unrestrained passengers are missiles and add to Unrestrained passengers are missiles and add to
injuries other passengers already sustainedinjuries other passengers already sustained

Injury Patterns – Motor Injury Patterns – Motor VehicleVehicle
• Rear end (9% of MVC)Rear end (9% of MVC)– Head rotates backward and then snaps Head rotates backward and then snaps
forwardforward– Less neck injury if the head rest is properly Less neck injury if the head rest is properly
positionedpositioned
• Rollover (6% of MVC)Rollover (6% of MVC)– Occupant experiences impact every time Occupant experiences impact every time
vehicle impacts a point on the groundvehicle impacts a point on the ground– Vehicle sides and roof provide less crumple Vehicle sides and roof provide less crumple
zones for absorbing impact forceszones for absorbing impact forces– Ejection is common in unrestrained personsEjection is common in unrestrained persons

Index of SuspicionIndex of Suspicion
•Your anticipation of injury to a Your anticipation of injury to a body, region, organ, or structure body, region, organ, or structure based on identification of the based on identification of the mechanism of injurymechanism of injury
•Your index of suspicion is honed Your index of suspicion is honed from experience and time on the from experience and time on the jobjob

General impressionGeneral impression
•Formed from mechanism of Formed from mechanism of injury and index of suspicioninjury and index of suspicion
•Will guide the EMS provider Will guide the EMS provider regarding a direction on how regarding a direction on how to proceed in caring for this to proceed in caring for this patientpatient

Putting It All Together Putting It All Together SampleSampleReport:Report:
•The mechanism of injury is a frontal The mechanism of injury is a frontal MVCMVC
The steering wheel is broken, chest The steering wheel is broken, chest wall is bruised, breath sounds wall is bruised, breath sounds decreaseddecreased on the right on the right
• Your index of suspicion is chest injuryYour index of suspicion is chest injury
• Your general impression is pneumothoraxYour general impression is pneumothorax

Documentation of The Documentation of The Complaint To Include:Complaint To Include:
•O - onsetO - onset
•P – provocation/palliationP – provocation/palliation
•Q - qualityQ - quality
•R - radiationR - radiation
•S – severity (0 – 10)S – severity (0 – 10)
•T – timing – when did it startT – timing – when did it start

DocumentationDocumentation
•Provide answers to:Provide answers to:– Who (the patient you’re caring Who (the patient you’re caring
for)for)– What (happened)What (happened)– When (did it happen)When (did it happen)– Where (which body part)Where (which body part)– How (did it occur)How (did it occur)

EMS Trauma Care – Amputated EMS Trauma Care – Amputated PartsParts• Routine trauma careRoutine trauma care
• To remove gross contamination, gently rinse To remove gross contamination, gently rinse with normal salinewith normal saline– DO NOT use distilled water to irrigate open DO NOT use distilled water to irrigate open
woundswounds– Normal saline is isotonic and less harmful to Normal saline is isotonic and less harmful to
tissuetissue
• Cover stump with damp (normal saline) sterile Cover stump with damp (normal saline) sterile dressing and ace wrapdressing and ace wrap– Ace provides uniform pressure to stumpAce provides uniform pressure to stump
• Cover wounds with sterile dressingCover wounds with sterile dressing

EMS Care of Amputated EMS Care of Amputated PartsParts
•Place part in a plastic zip Place part in a plastic zip lock baglock bag
•Place bag in larger bag or Place bag in larger bag or container over ice and container over ice and waterwater
•Do not ice the part aloneDo not ice the part alone

EMS Pain Management EMS Pain Management Including for Adult BurnsIncluding for Adult Burns
•Morphine for pain controlMorphine for pain control– 2 mg slow IVP over 2 minutes2 mg slow IVP over 2 minutes– May repeat every 2 minutes as May repeat every 2 minutes as
needed to a maximum of 10 mgneeded to a maximum of 10 mg– Watch for respiratory depressionWatch for respiratory depression– Monitor for a drop in blood Monitor for a drop in blood
pressure due to vasodilation pressure due to vasodilation from the medicationfrom the medication

Adult Burns - ElectricalAdult Burns - Electrical
• Immobilize the patientImmobilize the patient– High potential for traumatic injuryHigh potential for traumatic injury
•Muscle spasms during contact Muscle spasms during contact with sourcewith source
•Thrown when power source cutThrown when power source cut– Assess for dysrhythmia – place on Assess for dysrhythmia – place on
cardiac monitorcardiac monitor– Assess distal neurovascular status Assess distal neurovascular status
of affected partof affected part– Cover wounds with dry sterile Cover wounds with dry sterile
dressingsdressings

Adult Burns - InhalationAdult Burns - Inhalation
• High risk for airway compromiseHigh risk for airway compromise• Note presence of wheezing, hoarseness, Note presence of wheezing, hoarseness,
stridor, carbonaceous sputum, singed stridor, carbonaceous sputum, singed nasal hairnasal hair
• High flow oxygen via non-rebreather High flow oxygen via non-rebreather maskmask
• Monitor for need of advanced airway Monitor for need of advanced airway devicedevice– ETT – consider using ETT one size ETT – consider using ETT one size
smaller than normal due to potential smaller than normal due to potential swelling of the airwayswelling of the airway

Adult Burns - ChemicalAdult Burns - Chemical
• HAZ-MAT team may be involved in the fieldHAZ-MAT team may be involved in the field
• If powdered chemical, first brush away If powdered chemical, first brush away excess dry materialexcess dry material
• Clothing removed if possibleClothing removed if possible
• Area flushed with sterile salineArea flushed with sterile saline
• If eye involvement, remove contact lenses If eye involvement, remove contact lenses and flush continuously with sterile salineand flush continuously with sterile saline
• Avoid contamination of noninvolved areasAvoid contamination of noninvolved areas

EMS Care for Adult Burns - EMS Care for Adult Burns - ThermalThermal
• Superficial – 1Superficial – 1stst degree degree– Area cooled with sterile salineArea cooled with sterile saline– <20% BSA involved, apply sterile <20% BSA involved, apply sterile
saline soaked dressings for transportsaline soaked dressings for transport– >20% BSA, apply dry sterile dressing >20% BSA, apply dry sterile dressing
for transportfor transport• Do not overcool major burns or apply Do not overcool major burns or apply
ice directly to burned areasice directly to burned areas

Adult Burns - ThermalAdult Burns - Thermal• Partial or full thickness (2Partial or full thickness (2ndnd or 3 or 3rdrd degree) degree)
– Wear sterile gloves and mask while burn areas Wear sterile gloves and mask while burn areas are exposedare exposedDecreases additional risk of wound contaminationDecreases additional risk of wound contamination
– Cover burn wound with dry sterile dressingsCover burn wound with dry sterile dressingsPreventing air flow over exposed burn areas Preventing air flow over exposed burn areas reduces pain levelsreduces pain levels
– EMS will place a clean sheet over the patientEMS will place a clean sheet over the patient– Protect the patient from hypothermiaProtect the patient from hypothermia

Infant differences: back 13%, each buttocks 2.5%, each entire leg 14%

Case Study #1Case Study #1• Adult patient reached over a charcoal grill Adult patient reached over a charcoal grill
just as the match was thrown onto the just as the match was thrown onto the soaked coalssoaked coals
• Injury is restricted to the right forearmInjury is restricted to the right forearm
• What type of burn is this?What type of burn is this?
• Using the Rule of Nines, what is the TSBA Using the Rule of Nines, what is the TSBA burned?burned?
• What type of care is appropriate?What type of care is appropriate?
• How can the pain be managed?How can the pain be managed?
• What does the documentation look like? What does the documentation look like?

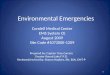
Case Study #1 – Patient with Case Study #1 – Patient with BurnsBurns
Skin is reddened and some blistering is present

Case Study #1 – Category IIICase Study #1 – Category III• Combination of superficial and partial thickness burns Combination of superficial and partial thickness burns
approx 4.5% TSBA (circumferential around forearm)approx 4.5% TSBA (circumferential around forearm)– Evidence of redness with a blistered area although Evidence of redness with a blistered area although
blister is brokenblister is broken• Appropriate care includes cooling burn, applying Appropriate care includes cooling burn, applying
sterile saline soaked dressing (<20% TBSA)sterile saline soaked dressing (<20% TBSA)• Additional helpful careAdditional helpful care
– Elevation of arm, removal of ring before fingers Elevation of arm, removal of ring before fingers swellswell
• For pain controlFor pain control– Morphine 2 mg slow IVP; can repeat 2 mg in 2 Morphine 2 mg slow IVP; can repeat 2 mg in 2
minutes up to 10 mg minutes up to 10 mg

Chest Injuries – Traumatic Chest Injuries – Traumatic Arrest – Category I TraumaArrest – Category I Trauma
• Begin CPRBegin CPR• Transport to closest Trauma CenterTransport to closest Trauma Center
– A hospital on by-pass must take a A hospital on by-pass must take a patient in life threatening condition if patient in life threatening condition if they are the closest appropriate hospitalthey are the closest appropriate hospital
• EMS to perform bilateral chest EMS to perform bilateral chest decompressiondecompression– Use common sense – does the scene Use common sense – does the scene
size –up, evaluation of mechanism of size –up, evaluation of mechanism of injury and general impression indicate a injury and general impression indicate a potential chest wall injury?potential chest wall injury?

Chest Injuries – Tension Chest Injuries – Tension Pneumothorax – Category I Pneumothorax – Category I TraumaTrauma
• History of injury to the chest wallHistory of injury to the chest wall– On rare occasions can be spontaneousOn rare occasions can be spontaneous
• Diminished breath soundsDiminished breath sounds
• Hyperresonance if percussion done Hyperresonance if percussion done
• Severe dyspneaSevere dyspnea
• Hyperinflation of chestHyperinflation of chest
• Jugular vein distentionJugular vein distention
• TachycardiaTachycardia
• HypotensionHypotension


In-field Needle In-field Needle DecompressionDecompression•Landmarks anterior approachLandmarks anterior approach
– 22ndnd intercostal space in the midline intercostal space in the midline of the claviclesof the clavicles
– Place prepared flutter valve needle Place prepared flutter valve needle over the top of the ribover the top of the rib
•Avoids potential injury to vessels Avoids potential injury to vessels and nerves that run along the and nerves that run along the bottom of the ribbottom of the rib

Quick Way to Find 2Quick Way to Find 2ndnd ICS ICS• Feel for the top of the sternumFeel for the top of the sternum
• Roll your finger tip to the anterior surface at Roll your finger tip to the anterior surface at the top of the sternumthe top of the sternum
• Feel the little bump near the top of the Feel the little bump near the top of the sternumsternum– This bump is the Angle of LouisThis bump is the Angle of Louis
• From the Angle of Louis slide your fingers From the Angle of Louis slide your fingers angled slightly downward toward the angled slightly downward toward the affected side following the rib spaceaffected side following the rib space– You are automatically in the 2You are automatically in the 2ndnd ICS ICS
• Identify the midline of the clavicleIdentify the midline of the clavicle– The midline is more lateral than persons realize The midline is more lateral than persons realize
and usually runs in line with the nippleand usually runs in line with the nipple

Alternate Method to Find 2Alternate Method to Find 2ndnd Intercostal Space Intercostal Space • Palpate the clavicle and find the midlinePalpate the clavicle and find the midline
– The midline is farther out (more lateral) from The midline is farther out (more lateral) from the sternum than most persons realizethe sternum than most persons realize
• Move your finger tips under the clavicle Move your finger tips under the clavicle into the 1into the 1stst intercostal space intercostal space– 11stst rib is under the clavicle and is not palpated rib is under the clavicle and is not palpated– Spaces identified for the numbered rib above Spaces identified for the numbered rib above
the spacethe space
• Feel for the firm 2Feel for the firm 2ndnd rib and palpate the rib and palpate the soft space below the ribsoft space below the rib– This is the 2This is the 2ndnd ICS ICS

Field Field EquipmentEquipment
• Long needle (preferably 2-3 inch) and large Long needle (preferably 2-3 inch) and large bore needle (preferably 12-14G)bore needle (preferably 12-14G)
• Flutter valve – finger cut from a gloveFlutter valve – finger cut from a glove• Cleanser to prepare skin overlying the siteCleanser to prepare skin overlying the site• Method to secure needle in placeMethod to secure needle in place
– Skin will most likely be diaphoreticSkin will most likely be diaphoretic– Tape may not stickTape may not stick– May need to maintain manual control of needleMay need to maintain manual control of needle

Skin PreparationSkin Preparation
Midline ofclavicle
Angle of Louis
2nd ICS

Inserting the Inserting the NeedleNeedle
• Remove proximal end cap from Remove proximal end cap from needle if presentneedle if present– Will be able to hear trapped air escapingWill be able to hear trapped air escaping
• Needle inserted over top of ribNeedle inserted over top of rib– Once hiss of air heard continue to advance Once hiss of air heard continue to advance
catheter while withdrawing styletcatheter while withdrawing stylet• Stabilize catheter as best as possibleStabilize catheter as best as possible• Patient should symptomatically improvePatient should symptomatically improve
– Do not expect to hear improved breath sounds; Do not expect to hear improved breath sounds; takes time for the lung to reexpandtakes time for the lung to reexpand

Case Study #2Case Study #2
• EMS is called to the scene for a 52 year-old EMS is called to the scene for a 52 year-old male with c/o sudden onset dyspnea with male with c/o sudden onset dyspnea with pain between his shoulder blades while pain between his shoulder blades while watching TV at home. The patient is agitated, watching TV at home. The patient is agitated, short of breath, with increased respiratory short of breath, with increased respiratory rate and SaOrate and SaO22 of 89%. of 89%.
• Further assessment reveals decreased breath Further assessment reveals decreased breath sounds on the right and clear on the leftsounds on the right and clear on the left
• Vital signs: 98/62; HR 118; RR 32 and shallowVital signs: 98/62; HR 118; RR 32 and shallow
• Your impression & intervention plan?Your impression & intervention plan?

Case Study #2Case Study #2• Spontaneous tension pneumothoraxSpontaneous tension pneumothorax
– They don’t all develop from traumaThey don’t all develop from trauma
• Supplemental oxygen support via non-Supplemental oxygen support via non-rebreather, cardiac monitor, preparation rebreather, cardiac monitor, preparation for IVfor IV
BUTBUT
• This patient needs needle decompression This patient needs needle decompression while the above are being preparedwhile the above are being prepared– Patients with a tension pneumothorax can’t Patients with a tension pneumothorax can’t
wait and will deteriorate without needle wait and will deteriorate without needle decompressiondecompression

Sucking Chest Wound – Sucking Chest Wound – Category I TraumaCategory I Trauma• Most common with penetrating woundsMost common with penetrating wounds• Free passage of air between the Free passage of air between the
atmosphere and pleural space if the atmosphere and pleural space if the open wound is at least open wound is at least 22//33
rdrd the size of the size of the diameter of the tracheathe diameter of the trachea– Size of trachea about the size of pt’s 5Size of trachea about the size of pt’s 5thth
fingerfinger
• Air is drawn into the chest cavity, not Air is drawn into the chest cavity, not into the lungsinto the lungs
• Air replaces lung tissueAir replaces lung tissue• Lung collapsesLung collapses

Sucking Chest WoundSucking Chest Wound
• Severe dyspneaSevere dyspnea
• Open chest woundOpen chest wound– Check anterior, posterior, axilla areasCheck anterior, posterior, axilla areas
• Frothy blood at wound openingFrothy blood at wound opening
• Sucking sound as air moves in and Sucking sound as air moves in and outout
• Tachycardia with hypovolemiaTachycardia with hypovolemia

Treatment Sucking Chest Treatment Sucking Chest WoundWound• Immediate treatment is to seal the Immediate treatment is to seal the
openingopening– May start by placing a gloved hand over the May start by placing a gloved hand over the
woundwound– When able, place an occlusive dressing, When able, place an occlusive dressing,
taped on 3 sides, over the woundtaped on 3 sides, over the wound
• Wound now converted to a closed Wound now converted to a closed pneumothoraxpneumothorax
• Monitor for signs of tension Monitor for signs of tension pneumothoraxpneumothorax– May need to lift a corner of the dressing to May need to lift a corner of the dressing to
release trapped air via burping dressingrelease trapped air via burping dressing

Flail Chest – Category I Flail Chest – Category I TraumaTrauma• 3 or more adjacent ribs broken in 2 or 3 or more adjacent ribs broken in 2 or
more placesmore places– Segment becomes free with pardoxical chest Segment becomes free with pardoxical chest
wall motion during respirationswall motion during respirations– Paradoxical movement more evident after the Paradoxical movement more evident after the
muscles splinting the flail segment fatiguemuscles splinting the flail segment fatigue
• Usually takes a tremendous amount of Usually takes a tremendous amount of blunt trauma to cause a flail chestblunt trauma to cause a flail chest
• Associated severe underlying injury (ie: Associated severe underlying injury (ie: pulmonary contusion) will often be presentpulmonary contusion) will often be present
• Respiratory volume reduced and Respiratory volume reduced and respiratory effort increasedrespiratory effort increased

Treatment Flail ChestTreatment Flail Chest• Place patient on the injured side Place patient on the injured side (may not be (may not be
possible to do this in the field based on mechanism of possible to do this in the field based on mechanism of injury)injury)
• High flow oxygen – non-rebreather maskHigh flow oxygen – non-rebreather mask– Monitor for need to assist ventilations via BVM Monitor for need to assist ventilations via BVM
to deliver positive pressure ventilationsto deliver positive pressure ventilations
•Evidence of underlying pulmonary injuryEvidence of underlying pulmonary injury
•Effort and fatigueEffort and fatigue
•Pulse oximetryPulse oximetry
• EKG monitoringEKG monitoring– Tremendous amount of force is delivered to Tremendous amount of force is delivered to
the chest wall and cardiac injury is highly the chest wall and cardiac injury is highly likely as a resultlikely as a result

Pericardial Tamponade – Pericardial Tamponade – Category I TraumaCategory I Trauma
• Blood or other fluid fills the pericardial sac Blood or other fluid fills the pericardial sac restricting cardiac filling & contractilityrestricting cardiac filling & contractility
• Most often related to penetrating traumaMost often related to penetrating trauma
• Venous return to the heart is restrictedVenous return to the heart is restricted
• Decreased cardiac outputDecreased cardiac output
• Pressure on the coronary arteries restricts Pressure on the coronary arteries restricts blood flow to the myocardiumblood flow to the myocardium

Pericardial Tamponade Signs & Pericardial Tamponade Signs & SymptomsSymptoms• Usually history of penetrating traumaUsually history of penetrating trauma• Agitated patientAgitated patient• Diminished strength of pulses (weak and thready) Diminished strength of pulses (weak and thready)
with tachycardiawith tachycardia• Narrowing pulse pressureNarrowing pulse pressure
– Diastolic & systolic numbers moving closer Diastolic & systolic numbers moving closer togethertogether
• Distended neck veins (JVD)Distended neck veins (JVD)• Diaphoretic and paleDiaphoretic and pale• Muffled, distant heart tonesMuffled, distant heart tones• HypotensionHypotension

Treatment Pericardial Treatment Pericardial TamponadeTamponade
• Treatment in the field is limited to Treatment in the field is limited to being supportivebeing supportive
• Patient requires high index of Patient requires high index of suspicion and/or rapid identification suspicion and/or rapid identification with rapid transportwith rapid transport– In ED will perform needle thoracentesis In ED will perform needle thoracentesis
and then transfer the patient to the OR and then transfer the patient to the OR for open heart surgeryfor open heart surgery

General Assessment PearlsGeneral Assessment Pearls
• Restlessness and agitationRestlessness and agitation– You must consider You must consider hypoxia, hypoxia, shock, shock,
influence of alcohol and/or drugsinfluence of alcohol and/or drugs– This is one time you need to assess This is one time you need to assess
for all reasons of restlessness and for all reasons of restlessness and not just stop when you discovered not just stop when you discovered one cause – there may be more than one cause – there may be more than one pathology going on at a timeone pathology going on at a time

Evaluation Pearls – Low Evaluation Pearls – Low SaOSaO22• SaOSaO22 reading may be inaccurate in the presence reading may be inaccurate in the presence
of:of:– Hemorrhagic shock with delayed capillary refill Hemorrhagic shock with delayed capillary refill – HypothermiaHypothermia– Lung damageLung damage
• Evaluate all parameters together to get the best Evaluate all parameters together to get the best overall picture in ventilated patientoverall picture in ventilated patient– What does the ETCOWhat does the ETCO22 indicate? indicate?– Are you able to ventilate the patient?Are you able to ventilate the patient?– Are there extenuating circumstances where Are there extenuating circumstances where
the circulation is affected and would affect the the circulation is affected and would affect the pulse ox reading like those listed above?pulse ox reading like those listed above?

More More Case Case StudiesStudies

Case Study #3Case Study #3• Your 34 year-old Your 34 year-old
patient received a patient received a GSW to the right GSW to the right upper abdomen.upper abdomen.
• They are conscious They are conscious and alert; B/P 90/62; and alert; B/P 90/62; HR 120; RR 28; HR 120; RR 28; bleeding is minimalbleeding is minimal
• Category trauma?Category trauma?
• What interventions What interventions are appropriate in are appropriate in field?field?

Case Study #3 – Category I Case Study #3 – Category I TraumaTrauma• Consider need for spinal immobilizationConsider need for spinal immobilization
• During assessment of wound, consider During assessment of wound, consider thoracic injury in addition to abdominal thoracic injury in addition to abdominal injury depending on the angle of the GSW.injury depending on the angle of the GSW.
• Examine for an exit wound Examine for an exit wound – Check the back and the axillaCheck the back and the axilla
• Prepare for the worst – assume the patient Prepare for the worst – assume the patient will deteriorate before ED arrivalwill deteriorate before ED arrival
• Repeat VS: B/P 80/; HR 140; RR 32, Repeat VS: B/P 80/; HR 140; RR 32, remains conscious and in painremains conscious and in pain
• Category I is transported to the highest Category I is transported to the highest level Trauma Center within 25 minuteslevel Trauma Center within 25 minutes

Case Study #3 - TreatmentCase Study #3 - Treatment
• Routine trauma careRoutine trauma care
• Question – is this an isolated abdominal Question – is this an isolated abdominal wound or is it a combination abdominal/ wound or is it a combination abdominal/ chest wound?chest wound?– Need to treat patient for potential injuries Need to treat patient for potential injuries
of both body cavitiesof both body cavities– EMS cannot determine in the field the EMS cannot determine in the field the
angle of the trajectory angle of the trajectory
• Cover the wound and watch for eviscerationCover the wound and watch for evisceration
• Fluid resuscitation – keep B/P at low levels; Fluid resuscitation – keep B/P at low levels; the higher the B/P the faster the patient the higher the B/P the faster the patient bleeds outbleeds out

Case Study #4Case Study #4• A 10 year-old patient A 10 year-old patient
has a penetrating has a penetrating injury to the right leg injury to the right leg near the knee while near the knee while playing in his backyardplaying in his backyard
• Initial VS: B/P 90/70; Initial VS: B/P 90/70; HR; 130; RR 32; no HR; 130; RR 32; no active bleedingactive bleeding
• Category trauma? Field Category trauma? Field interventions?interventions?

Case Study #4 – Category IIICase Study #4 – Category III
• Next VS: B/P 92/64; HR 110; RR 20.Next VS: B/P 92/64; HR 110; RR 20.
• Stabilize foreign body in place (gauze, Stabilize foreign body in place (gauze, trauma dressing)trauma dressing)
• Obtain distal neurovascular statusObtain distal neurovascular status– Distal pulsesDistal pulses– Movement – “can you wiggle your toes?”Movement – “can you wiggle your toes?”– Sensation – “close your eyes and tell me which Sensation – “close your eyes and tell me which
toe I am touching”toe I am touching”
• Document distal neurovascular status and Document distal neurovascular status and describe how the foreign object is describe how the foreign object is stabilized in placestabilized in place

Case Study #5Case Study #5• Your 62 year-old patient had abdominal Your 62 year-old patient had abdominal
surgery 1 week ago. Today at home he surgery 1 week ago. Today at home he sneezed hard and felt a tearing sneezed hard and felt a tearing sensation in his sensation in his abdomen and abdomen and called EMS. called EMS.
• VS: B/P 100/60; VS: B/P 100/60; HR 110; RR 24HR 110; RR 24
• No active No active bleedingbleeding
• What What interventionsinterventions are appropriate are appropriate in the field? in the field?

Case Study #5 - Case Study #5 - InterventionsInterventions
• Immediately cover the woundImmediately cover the wound– Need to minimize contaminationNeed to minimize contamination– Need to prevent more organs from protrudingNeed to prevent more organs from protruding– Need to prevent loss of fluidsNeed to prevent loss of fluids
• Place a saline moistened dressing over the Place a saline moistened dressing over the exposed tissueexposed tissue
• Place dry gauze over the saline dressingsPlace dry gauze over the saline dressings
• Can place light manual control over the Can place light manual control over the organs to prevent further evisceration organs to prevent further evisceration especially during movement, coughing, especially during movement, coughing, sneezing, deep breathssneezing, deep breaths

Case Study #6Case Study #6• Your 45 year-old patient is a Your 45 year-old patient is a
construction worker who was construction worker who was accidentally shot in the head with a accidentally shot in the head with a nail gunnail gun
• Upon EMS arrival, the patient is Upon EMS arrival, the patient is awake, alert, talking (GCS 15)awake, alert, talking (GCS 15)
• VS: B/P 132/78; HR 96; RR 20; VS: B/P 132/78; HR 96; RR 20; complains of a minor headache; complains of a minor headache; minimal bleeding at a few puncture minimal bleeding at a few puncture wounds noted on the occipital area of wounds noted on the occipital area of the scalp (patient has thick hair).the scalp (patient has thick hair).

X-ray X-ray from from EDED
No No deficitdeficitssnotednoted

Case Study #6 - TreatmentCase Study #6 - Treatment• Consider any injury above the level of the Consider any injury above the level of the
clavicles to include a c-spine injury until clavicles to include a c-spine injury until proven otherwise and immobilize the patientproven otherwise and immobilize the patient
• Control bleedingControl bleeding– The face and scalp have such a rich blood supply The face and scalp have such a rich blood supply
small wounds tend to bleed heavilysmall wounds tend to bleed heavily
• Protect from further contaminationProtect from further contamination– The open wound may be in direct contact with the The open wound may be in direct contact with the
brainbrain
• Document neurological evaluation to establish Document neurological evaluation to establish baseline for comparison (AVPU, GCS, baseline for comparison (AVPU, GCS, movement)movement)

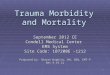
Case Study #7Case Study #7• EMS was called to the scene for a 10 year-EMS was called to the scene for a 10 year-
old female who has been run over by a old female who has been run over by a busbus
• As patient exited bus, she bent down to tie As patient exited bus, she bent down to tie her shoe and was caught under the wheels her shoe and was caught under the wheels of the busof the bus
• EMS noted a large amount of avulsed EMS noted a large amount of avulsed tissue with bleeding from the left hip, left tissue with bleeding from the left hip, left buttock, and left upper thigh areabuttock, and left upper thigh area
• The patient is screaming in painThe patient is screaming in pain• VS: B/P 110/70; HR 110; RR 26 GCS 15VS: B/P 110/70; HR 110; RR 26 GCS 15• What is your impression?What is your impression?• What is your treatment plan? What is your treatment plan?

10 y/o run over by bus10 y/o run over by bus

Case Study #7 – Category I or Case Study #7 – Category I or II?II?• General impressionGeneral impression
– Category II minimally – pedestrian run-over Category II minimally – pedestrian run-over – Category I trauma – if unstable pelvis or 2 or Category I trauma – if unstable pelvis or 2 or
more long bones (proximal bones) fractured more long bones (proximal bones) fractured or unstable vital signsor unstable vital signs
• Potential problems to consider & addressPotential problems to consider & address– Massive hemorrhage & control of Massive hemorrhage & control of
hemorrhagehemorrhage– Spinal injurySpinal injury– Additional injuriesAdditional injuries– Airway control Airway control – Equipment to fit a 10 year-oldEquipment to fit a 10 year-old– Further wound contaminationFurther wound contamination

1 year F/U with skin grafts1 year F/U with skin grafts

Glasgow Coma Scale – GSCGlasgow Coma Scale – GSCReview and PracticeReview and Practice• Tool used to evaluate and monitor a Tool used to evaluate and monitor a
patient’s conditionpatient’s condition
• EvaluatesEvaluatesBest eye openingBest eye openingBest verbal responseBest verbal responseBest motor responseBest motor response
• Serves as an indicator/predictor of Serves as an indicator/predictor of survivalsurvival
• To be obtained on all EMS patientsTo be obtained on all EMS patients

GCSGCS•Possible total score 3 (lowest) – 15 (highest)Possible total score 3 (lowest) – 15 (highest)
•Minor head injury – patient scores 13 – Minor head injury – patient scores 13 – 1515
•Moderate head injury – patient scores 9 – Moderate head injury – patient scores 9 – 1212
•Severe head injury – patient scores Severe head injury – patient scores <<88– Significant mortality riskSignificant mortality risk

GCS PearlsGCS Pearls• The change in the GCS is more important The change in the GCS is more important
than the absolute scorethan the absolute score
• Check for associated injuries Check for associated injuries – Manage a head injury as a multiple injured Manage a head injury as a multiple injured
patient until other injuries ruled outpatient until other injuries ruled out
• Stabilize the neck for any head injuryStabilize the neck for any head injury
• Don’t assume the level of consciousness is Don’t assume the level of consciousness is altered just because of ETOH and/or drugsaltered just because of ETOH and/or drugs– Is there an occult (hidden) injury present?Is there an occult (hidden) injury present?
• Provide accurate, clear, detailed Provide accurate, clear, detailed documentationdocumentation

GCS – Eye Opening 1-4 GCS – Eye Opening 1-4 PointsPoints
• Spontaneous (4) – eyes open; may or may not focus Spontaneous (4) – eyes open; may or may not focus • To voice (3) – prior to touching the patient, eyes will open To voice (3) – prior to touching the patient, eyes will open
to sounds around them calling/yelling to them to open eyesto sounds around them calling/yelling to them to open eyes– Often difficult to accurately assess due to EMS gaining Often difficult to accurately assess due to EMS gaining
immediate c-spine control so difficult at times to immediate c-spine control so difficult at times to determine if patient responded to voice or touch (pain). determine if patient responded to voice or touch (pain). Eyelid flutter to voice is 3 pointsEyelid flutter to voice is 3 points
• To pain (2) – doesn’t necessarily imply you must apply To pain (2) – doesn’t necessarily imply you must apply painful stimulus, could be just to touchpainful stimulus, could be just to touch– Flutter of eyelids when touched is scored as 2Flutter of eyelids when touched is scored as 2
• None (1) – eyes remain closed with no eyelid flutter or None (1) – eyes remain closed with no eyelid flutter or other eye movement; eyes do not openother eye movement; eyes do not open

What’s the Eye Opening What’s the Eye Opening Score?Score?• When the patient is asked to open their When the patient is asked to open their
eyes, they refuse and actually close them eyes, they refuse and actually close them tightertighter
• What is their eye opening?What is their eye opening?– The score is 3 (don’t open their eyes but there is The score is 3 (don’t open their eyes but there is
eyelid movement to voice command)eyelid movement to voice command)– Later, if the patient is more cooperative and Later, if the patient is more cooperative and
then open their eyes, their GCS will improvethen open their eyes, their GCS will improve
MAKE SENSE?MAKE SENSE?

GCS – Verbal Response 1-5 GCS – Verbal Response 1-5 PointsPoints• Oriented (5)Oriented (5)• Confused (4)Confused (4)
– Words may be appropriate to situation but pt does Words may be appropriate to situation but pt does not respond to questionsnot respond to questions
• Inappropriate words (3)Inappropriate words (3)– Words are spoken and understood but nonsensical Words are spoken and understood but nonsensical
to the situation (“over there”)to the situation (“over there”)• Incomprehensible words (2)Incomprehensible words (2)
– Includes mumbling, unintelligible speech, moaning, Includes mumbling, unintelligible speech, moaning, groaninggroaning
• None (1) None (1)

What’s the Verbal Response What’s the Verbal Response Score?Score?• You have touched the patient’s injured You have touched the patient’s injured
arm and the patient yells “stop, ow, don’t arm and the patient yells “stop, ow, don’t you’re hurting me”you’re hurting me”
• The patient does not carry on any other The patient does not carry on any other conversation with youconversation with you
• The comments were appropriate for the The comments were appropriate for the situation but the patient is not oriented situation but the patient is not oriented nor are the words inappropriate. nor are the words inappropriate.
So by default this patient is scored So by default this patient is scored a 4 for confuseda 4 for confused

GCS – Motor Response 1-6 GCS – Motor Response 1-6 PointsPoints• Obeys command (6)Obeys command (6)• Localizes pain (5)Localizes pain (5)
– Patient who pulls equipment off; Patient who pulls equipment off; pushes your pushes your hands away; purposeful movementhands away; purposeful movement
– This patient knows where the obnoxious stimuli This patient knows where the obnoxious stimuli is contacting his bodyis contacting his body
• Withdraws to pain (4)Withdraws to pain (4)– Pt cannot isolate where they feel the noxious Pt cannot isolate where they feel the noxious
stimuli so just stimuli so just pulls back/withdrawspulls back/withdraws• Flexion (3) – arms bent towards midline Flexion (3) – arms bent towards midline
when stimulated (decorticate)when stimulated (decorticate)• Extension (2) – arms extended when Extension (2) – arms extended when
stimulated (decerebrate)stimulated (decerebrate)• None (1) – remains flaccidNone (1) – remains flaccid

What’s the Motor Response What’s the Motor Response Score?Score?
• This patient is constantly trying to pull off This patient is constantly trying to pull off the cervical collar, take off the B/P cuff, and the cervical collar, take off the B/P cuff, and pull out the IV (you call this uncooperative)pull out the IV (you call this uncooperative)
• This patient is aware of what part of the This patient is aware of what part of the body is feeling some noxious stimuli so body is feeling some noxious stimuli so they are trying to get rid of it/escape from itthey are trying to get rid of it/escape from it
This is purposeful movement (the This is purposeful movement (the patient localizes the annoyance) patient localizes the annoyance)
and is scored 5and is scored 5

GCS PearlsGCS Pearls
• Give the patient the best score Give the patient the best score possiblepossible– If the patient moves the right side of If the patient moves the right side of
their body but no movement on their their body but no movement on their left, score them for the movement they left, score them for the movement they currently exhibit on the rightcurrently exhibit on the right
– If patient deteriorates, easier to see the If patient deteriorates, easier to see the drop or change in the GCS scoredrop or change in the GCS score
• When testing for responses, watch When testing for responses, watch even for minimal activity like eyelid even for minimal activity like eyelid flutter or a grimaceflutter or a grimace

GCS PearlsGCS Pearls
• Acceptable noxious stimuliAcceptable noxious stimuli– Armpit pinch or nailbed pressureArmpit pinch or nailbed pressure– Sternal rub, pinching web space Sternal rub, pinching web space
between fingers, pinching shoulder between fingers, pinching shoulder muscle (trapezius)muscle (trapezius)
– Earlobe pinch is out of favorEarlobe pinch is out of favor
•Can cause movement of head & Can cause movement of head & neck in response to the painneck in response to the pain

GCS and RTS ToolsGCS and RTS Tools
• See end of document for full size See end of document for full size print of the GCS and RTS formsprint of the GCS and RTS forms
• This information is also on the radio This information is also on the radio run reportrun report– The ECRN is to fill out a GCS score on The ECRN is to fill out a GCS score on
every EMS callevery EMS call– The ECRN calculates the RTS on every The ECRN calculates the RTS on every
trauma patienttrauma patient


RTS – Scoring 0 – 12 pointsRTS – Scoring 0 – 12 points

Practice GCS and RTSPractice GCS and RTS
• Calculate the scores for the next 6 Calculate the scores for the next 6 casescases
• Assign GCS (3 – 15 points)Assign GCS (3 – 15 points)• RTSRTS
Convert the raw GCS number to its Convert the raw GCS number to its respective score 0 – 4respective score 0 – 4
Add the converted GCS number to Add the converted GCS number to the points (0 – 4) for the respiratory the points (0 – 4) for the respiratory rate and systolic B/Prate and systolic B/P
Determine the RTS (0 – 12 points)Determine the RTS (0 – 12 points)

GCS & RTS Practice #1GCS & RTS Practice #1
• Patient eyes are open and they watch you Patient eyes are open and they watch you during the examinationduring the examination
• The patient is confused; they don’t The patient is confused; they don’t remember how they got hurt and can’t remember how they got hurt and can’t remember the day of the weekremember the day of the week
• When you ask the patient to “show me 2 When you ask the patient to “show me 2 fingers”, they respond but are slow to do sofingers”, they respond but are slow to do so
• VS: B/P 120/70; HR 88; RR 18 VS: B/P 120/70; HR 88; RR 18
• Total GCS?Total GCS?
• Total RTS?Total RTS?

Practice #1Practice #1• Total GCS – 14Total GCS – 14
Eye opening 4 (spontaneous)Eye opening 4 (spontaneous)Verbal response 4 (confused)Verbal response 4 (confused)Motor response 6 (follows commands)Motor response 6 (follows commands)
• Converted GCS 4Converted GCS 4
• Respiratory rate 4Respiratory rate 4
• Systolic B/P 4Systolic B/P 4
• Total RTS - 12Total RTS - 12

GCS & RTS Practice #2GCS & RTS Practice #2
• The patient does not open their eyesThe patient does not open their eyes• The patient groans when pinched or The patient groans when pinched or
an injured body part is touchedan injured body part is touched• The patient does not follow The patient does not follow
commands and will commands and will pushpush your hands your hands away when you touch themaway when you touch them
• VS: B/P 96/68; HR 102; RR 22VS: B/P 96/68; HR 102; RR 22• Total GCS?Total GCS?• Total RTS?Total RTS?

Practice #2Practice #2
• Total GCS - 8Total GCS - 8 Eye opening – 1 (none)Eye opening – 1 (none)Verbal response - 2 (groans)Verbal response - 2 (groans)Motor response – 5 (pushes you Motor response – 5 (pushes you
away)away)
• Converted GCS - 2Converted GCS - 2• Respiratory rate - 4Respiratory rate - 4• Systolic B/P - 4Systolic B/P - 4• Total RTS - 10Total RTS - 10

GCS & RTS Practice #3GCS & RTS Practice #3
• The patient’s eyes are openThe patient’s eyes are open• When asked “what month is this?”, When asked “what month is this?”,
the patient responds, “he, umm, he…the patient responds, “he, umm, he…my jacket. I don’t ..”my jacket. I don’t ..”
• If touched or pinched, the patient If touched or pinched, the patient pulls awaypulls away from the contact from the contact
• VS: B/P 132/72; HR 96; RR 16VS: B/P 132/72; HR 96; RR 16• Total GCS?Total GCS?• Total RTS?Total RTS?

Practice #3Practice #3• Total GCS – 11Total GCS – 11
Eye opening – 4 (spontaneous) Eye opening – 4 (spontaneous) Verbal response – 3 (inappropriate words)Verbal response – 3 (inappropriate words)Motor response – 4 (pulls away/withdraws)Motor response – 4 (pulls away/withdraws)
• Converted GCS -3Converted GCS -3• Respiratory rate - 4Respiratory rate - 4• Systolic B/P - 4Systolic B/P - 4• Total RTS - 11Total RTS - 11

GCS & RTS Practice #4GCS & RTS Practice #4
• Your patient’s eyes are closed but they Your patient’s eyes are closed but they open wide if the patient’s injury is open wide if the patient’s injury is touchedtouched
• The patient yells “don’t” or “stop” when The patient yells “don’t” or “stop” when there are pinched but does not answer there are pinched but does not answer questions or speak in sentencesquestions or speak in sentences
• The patient will push your hands away The patient will push your hands away when you touch them or try to put on when you touch them or try to put on equipmentequipment
• VS: B/P 108/64; HR 102; RR 18VS: B/P 108/64; HR 102; RR 18• Total GCS?Total GCS?• Total RTS?Total RTS?

Practice #4Practice #4• Total GCS - 11Total GCS - 11
– Eye opening – 2 (opens when touched “pain”)Eye opening – 2 (opens when touched “pain”)– Verbal response – 4 (appropriate to being Verbal response – 4 (appropriate to being
touched but doesn’t carry on a conversation – touched but doesn’t carry on a conversation – marked confusion)marked confusion)
– Motor response – 5 (pushes you away)Motor response – 5 (pushes you away)
• Converted GCS -3Converted GCS -3• Respiratory rate - 4Respiratory rate - 4• Systolic B/P - 4Systolic B/P - 4• Total RTS - 11Total RTS - 11

GCS & RTS Practice #5GCS & RTS Practice #5
• The patient’s eyes are closed but the The patient’s eyes are closed but the eyelids flutter when you loudly call out eyelids flutter when you loudly call out their nametheir name
• The patient does not answer questions The patient does not answer questions but will groan when touched but not say but will groan when touched but not say recognizable wordsrecognizable words
• The patient does not follow commands The patient does not follow commands but will but will push awaypush away your hands when your hands when touchedtouched
• VS: B/P 80/52; HR 112; RR 12VS: B/P 80/52; HR 112; RR 12• Total GCS?Total GCS?• Total RTS?Total RTS?

Practice #5Practice #5
• Total GCS - 10Total GCS - 10Eye opening – 3 (eyelids flutter to voice)Eye opening – 3 (eyelids flutter to voice)Verbal response – 2 (groans)Verbal response – 2 (groans)Motor response – 5 (pushes you away; Motor response – 5 (pushes you away;
purposeful movement)purposeful movement)
• Converted GCS - 3Converted GCS - 3• Respiratory rate - 4Respiratory rate - 4• Systolic B/P - 3Systolic B/P - 3• Total RTS - 10Total RTS - 10

GSC & RTS Practice #6GSC & RTS Practice #6
• The patient’s eyes are closed but will open The patient’s eyes are closed but will open when the patient is touchedwhen the patient is touched
• The patient says “leave me alone” and The patient says “leave me alone” and “what are you doing?” and goes back to “what are you doing?” and goes back to sleep. When eyes are open they respond “I sleep. When eyes are open they respond “I don’t know” to questionsdon’t know” to questions
• They do not follow command and will They do not follow command and will pushpush your hands away when touchedyour hands away when touched
• VS: B/P 110/68; HR 88; RR 20VS: B/P 110/68; HR 88; RR 20• Total GCS?Total GCS?• Total RTS?Total RTS?

Practice #6Practice #6• Total GCS - 11Total GCS - 11
Eye opening – 2 (opens to touch “pain”)Eye opening – 2 (opens to touch “pain”)Verbal response – 4 (appropriate to the Verbal response – 4 (appropriate to the
situation but not oriented – marked confusion)situation but not oriented – marked confusion)Motor response – 5 (pushes you away)Motor response – 5 (pushes you away)
• Converted GCS - 3Converted GCS - 3• Respiratory rate - 4Respiratory rate - 4• Systolic B/P - 4Systolic B/P - 4• Total RTS - 11Total RTS - 11

Practice Rhythm Strip Practice Rhythm Strip Identification and ID of ST Identification and ID of ST elevation on 12 Leadelevation on 12 Lead• Identify the lead II strip and think Identify the lead II strip and think
over the SOP treatment appropriate over the SOP treatment appropriate if the patient is symptomaticif the patient is symptomatic
• Identify the leads/location of the ST Identify the leads/location of the ST elevationelevation– At CMC check the bulletin board At CMC check the bulletin board
outside the EMS office for Cardiac outside the EMS office for Cardiac Alert write-ups and more examples Alert write-ups and more examples of ST elevation of ST elevation

Identify Rhythm Strip #1Identify Rhythm Strip #1

Strip #1Strip #1• Second degree Type I – WenckebachSecond degree Type I – Wenckebach
– PR interval gets longer, longer, longer and then PR interval gets longer, longer, longer and then there is a dropped QRSthere is a dropped QRS
– The PR interval resets and the cycle starts againThe PR interval resets and the cycle starts again– Type I “drops one”Type I “drops one”– Wenckebach “winks” at youWenckebach “winks” at you– Notice grouped beating (group and a space, Notice grouped beating (group and a space,
group and a space)group and a space)– Patient usually not symptomaticPatient usually not symptomatic

Treatment IF Treatment IF SymptomaticSymptomatic BradycardiaBradycardia
• Bradycardia or Type I WenckebachBradycardia or Type I Wenckebach– Atropine 0.5 mg rapid IVP (“when they’re alive give Atropine 0.5 mg rapid IVP (“when they’re alive give
0.5”)0.5”)– May repeat every 3-5 minutes to total of 3mgMay repeat every 3-5 minutes to total of 3mg– If ineffective, begin pacingIf ineffective, begin pacing
• Type II or 3Type II or 3rdrd degree heart block degree heart block– Begin TCPBegin TCP– Valium 2 mg slow IVP for discomfortValium 2 mg slow IVP for discomfort– May repeat 2 mg IVP every 2 minutes to max 10 mgMay repeat 2 mg IVP every 2 minutes to max 10 mg– TCP set at rate 80/minute and start at lowest mATCP set at rate 80/minute and start at lowest mA– Watch for captureWatch for capture– If TCP not effective, give Atropine 0.5 mg rapid IVPIf TCP not effective, give Atropine 0.5 mg rapid IVP– May repeat Atropine 0.5 mg every 3-5 minutes; max May repeat Atropine 0.5 mg every 3-5 minutes; max
3mg3mg

Identify Rhythm Strip #2 – Identify Rhythm Strip #2 – 6 second strip 6 second strip

Strip #2 - Sinus RhythmStrip #2 - Sinus Rhythm
• No treatment necessary for this rhythmNo treatment necessary for this rhythm• Treat the patient’s complaintTreat the patient’s complaint• IF ACS complaint, then ACS SOPIF ACS complaint, then ACS SOP
– Aspirin 324 mg chewed (faster absorption)Aspirin 324 mg chewed (faster absorption)– Nitroglycerin 0.4 mg slNitroglycerin 0.4 mg sl
•May repeat in 5 minutes; watch B/PMay repeat in 5 minutes; watch B/P•Screen for recent Viagra type drug usageScreen for recent Viagra type drug usage
– Morphine if 2Morphine if 2ndnd NTG dose not effective NTG dose not effective•2 mg slow IVP2 mg slow IVP•May repeat every 2 minutes to max 10 May repeat every 2 minutes to max 10
mgmg

Identify Rhythm Strip #3 – Identify Rhythm Strip #3 – 6 second strip 6 second strip

Strip #3 – Atrial fibrillationStrip #3 – Atrial fibrillation
• A risk associated with atrial fibrillation A risk associated with atrial fibrillation is strokeis stroke– Clots form and are stagnant in the atriaClots form and are stagnant in the atria– Clots can break off and migrate into the Clots can break off and migrate into the
circulationcirculation
• Important with new onset atrial Important with new onset atrial fibrillation to determine how long they fibrillation to determine how long they have been in it to guide therapieshave been in it to guide therapies– >48 hours higher risk of throwing a clot if >48 hours higher risk of throwing a clot if
rhythm converted to sinus rhythmrhythm converted to sinus rhythm

EMS Treatment EMS Treatment RapidRapid Atrial Atrial FibrillationFibrillation
• Symptoms most likely dependent on the Symptoms most likely dependent on the heart rateheart rate– The faster the heart rate, the less tolerable The faster the heart rate, the less tolerable
the rhythm is especially for elderly patientsthe rhythm is especially for elderly patients
• Stable patient with B/P Stable patient with B/P >>100 mmHg100 mmHg– Verapamil 5mg SLOW IVP over 2+ minutesVerapamil 5mg SLOW IVP over 2+ minutes– If no response in 15 minutes & B/P stable, If no response in 15 minutes & B/P stable,
repeat 5mg SLOW IVP over 2+ minutesrepeat 5mg SLOW IVP over 2+ minutes
• Unstable patient with B/P <100 mmHgUnstable patient with B/P <100 mmHg– Contact Medical Control for directionContact Medical Control for direction

#1 – Identify ST Elevation

#2 – Identify ST elevation

#3 – Identify ST Elevation

ST Elevation Answer Key – ST Elevation Answer Key – Evaluate the 3 12 Lead EKG Evaluate the 3 12 Lead EKG Examples at the end of the Examples at the end of the packetpacket
• EKG #1 – Leads V 1 - 4EKG #1 – Leads V 1 - 4
• EKG #2 – Leads V 2 - 5EKG #2 – Leads V 2 - 5
• EKG #3 – Leads II, III, aVFEKG #3 – Leads II, III, aVF

BibliographyBibliography
• Bledsoe, B., Porter, R., Cherry, R. ParamedicBledsoe, B., Porter, R., Cherry, R. Paramedic Care Principles & Practices 2Care Principles & Practices 2ndnd Edition Edition
Brady.Brady. 2006.2006.• ITLS Bulletin. Case Study: ITLS Patient ETCOITLS Bulletin. Case Study: ITLS Patient ETCO22.. June 2008.June 2008.• Region X SOP’s Eff date March 1, 2007; Region X SOP’s Eff date March 1, 2007;
Revised JanuaryRevised January 2008.2008.• www.chems.alaska.gov/ems/document/GCSwww.chems.alaska.gov/ems/document/GCS• www.merck.comwww.merck.com• www.swsahs.nsw.gov.au/www.swsahs.nsw.gov.au/