Embed Size (px)
Citation preview

PATIENTS WHO LEAVE THE EMERGENCY
DEPARTMENT WITHOUT BEING SEEN
Authors: Michele Johnson, RN, Stephanie Myers, RN, June Wineholt, RN, CEN,Marc Pollack, MD, PhD, and Amy L. Kusmiesz, MS, York, PA
Introduction: Patients who present to the ED for care andleave without being seen (LWBS) represent a significant problem.The objective of this study was to determine why patients LWBS,how long they perceived waiting versus actual time waited beforeleaving, and factors that might have prevented LWBS.
Methods: We conducted a prospective, scripted phone surveyof all patients who left without being seen over a two-monthperiod in 2006 at an ED with approximately 65,000 yearly visits.Outcome measures were number leaving, ability to obtain careafter leaving, reason for leaving, would they return to this ED,perceived and actual time waited, number with a primaryphysician, and factors associated with leaving.
Results: One-hundred and twenty-seven of 11,147 total patients(1.1%) patients left without being seen. Seventy-two (56.7%)were interviewed within 8 days. Eighty-four and seven-tenthspercent stated they had a primary physician. The mean age was29.9 years, and 44.4% were male. The patient-reported meantime waited before leaving was 73.2 minutes while the actualmean time waited was 70.4 minutes. The reasons for leavingwere the length of wait (76.7%), the problem resolved (12.3%),and for other reasons (11.0%). During the week after leaving theED, 56.3% were able to obtain medical care. Sixty-five percentwould seek future emergency care at this ED, 15.3% would not,
and 19.7% would possibly return. During the wait, patientswanted information, lab tests/X-rays, and analgesics.
Discussion: Most would return for future ED care. Most had aphysician and were able to obtain care elsewhere. ReducedLWBS might be accomplished by triage testing, communicationand attention to pain.
Keywords:Wait time; Emergency department; Medical examination
There are approximately 110 million patient visits toemergency departments in the United States everyyear, and 0.5% to 8% leave without being seen
(LWBS).1 According to a Centers for Disease Controland Prevention report on ED use in the United States in2000, at least 1.8 million patients left emergency depart-ments without being seen, although the exact number isdifficult to determine. A large national study revealed thatthe number of patients who LWBS increased by approxi-mately 67% between 1995 and 2002.2 This phenomenonhas been associated with long wait times, ED and hospitalovercrowding, delay in medical care, and possibly seriousadverse events.3 Evidence suggests that reducing wait timeswill reduce the number of patients who LWBS.4 Prolongedwait time is often the result of excess demand exceeding thecapacity to provide quality services in a patient-acceptabletime frame, and patients leaving without being seen is adirect consequence. Determining the reason for patientsleaving without being seen, subsequent patient outcomes,and preventative measures is important.5,6 It is possiblethat potential ED patients leave before registering in theemergency department or never even enter because of theovercrowded waiting room or parking lot and are unlikelyto be counted in research studies evaluating the problem.
Innovative programs have been instituted to reducethe LWBS population. The University of California–SanDiego emergency department initiated an ED rapid-entryprocess and accelerated-care triage process that resulted in a3.2% reduction in the number of patients who LWBS.7 Ateam triage process of doctor and nurse in a Belfast, UnitedKingdom, emergency department reduced the time tomedical assessment, although the investigators did not spe-cifically measure the LWBS rate.8 Another study in a mili-
Michele Johnson,Member, ENA Chapter 49, is Clinical Nurse, Department ofEmergency Medicine, York Hospital, York, PA.
Stephanie Myers,Member, ENA Chapter 49, is Clinical Nurse, Department ofEmergency Medicine, York Hospital, York, PA.
June Wineholt, Member, ENA Chapter 49, is Clinical Nurse, Assistant NurseManager, Department of Emergency Medicine, York Hospital, York, PA.
Marc Pollack is Research Director, Department of Emergency Medicine, YorkHospital, York, PA.
Amy L. Kusmiesz is Clinical Research Associate, Department of EmergencyMedicine, York Hospital, York, PA.
For correspondence, write: June Wineholt, RN, 1001 S George St, York, PA17405; E-mail: [email protected].
J Emerg Nurs 2009;35:105-8.
Available online 27 August 2008.
0099-1767/$36.00
Copyright © 2009 by the Emergency Nurses Association. Published byElsevier Inc. All rights reserved.
doi: 10.1016/j.jen.2008.05.006
R E S E A R C H
March 2009 35:2 JOURNAL OF EMERGENCY NURSING 105

tary emergency department showed that having a nurse attriage instead of unlicensed assistive personnel reducedwait times and the number of LWBS patients.9 Theseinvestigators speculated that increased training and skillof the nurse allowed more efficient triage.
Because the problems of ED overcrowding and ade-quate staffing are likely to remain a challenge, the objectiveof this study was to determine the demographics of patientswho LWBS, the factors associated with leaving the emer-gency department before being seen by a physician, theability of these patients to subsequently obtain medicalcare, and factors that might have prevented patients fromleaving without being seen by a physician. The researchquestions addressed by this study were as follows: (1)Why do patients leave the emergency department beforebeing evaluated? (2) What are the demographics of patientswho LWBS? (3) Are patients able to obtain medical careafter leaving without being seen? (4) What factors mighthave prevented patients from leaving without being seen?
Methods
STUDY DESIGN
This was a prospective descriptive study of patients wholeft the ED triage/waiting room area before being seen bya physician.
STUDY SETTING AND POPULATION
The study took place in a mid-Atlantic level II traumacenter and community teaching hospital with approxi-mately 65,000 annual patient visits. The staffing in thetriage area during 11 AM to 11 PM, the peak hours forpatient volume, consisted of 1 emergency care technicianat the front desk and 2 registered nurses (RNs) in the triageexamination rooms. After 11 PM, triage staffing consisted of1 RN and 1 emergency care technician. Upon arrival in theED triage area, patients complete an information form withtheir name, chief complaint, contact phone number, andtime of arrival. Patients are subsequently interviewed bythe triage nurse and then wait for an available ED room.Patients were eligible for enrollment in this study if theywere no longer present in the ED waiting area when calledby a triage nurse for placement in an ED treatment room.Patients were enrolled 24 h/d throughout the study period.
The study protocol was approved by the hospital’s in-stitutional review board.
STUDY PROTOCOL
Enrolled patients had an “entered” time and a “left” timeon their patient information forms. The patient marked the“entered” time as per ED procedures, and the triage nurseentered the “left” time on the patient information form.
The “left” time was the time when the triage nurse calledthe patient for placement in a treatment room and he orshe was no longer present in the triage area. Because it wasuncertain when the patient actually left, the “left” time wasthe latest possible time the patient could have left the emer-gency department. A standardized scripted phone survey wasconducted at 4 to 8 days after the ED visit by 1 of 3 trainedresearch RNs. This follow-up time was selected because wewanted to be certain that patients had timely follow-up andwere still able to remember the details of the ED visit.
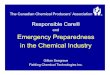
The protocol consisted of a scripted telephone inter-view with the subject. Verbal consent was obtained at thebeginning of the phone call. A maximum of 3 attemptsover a period of 4 to 8 days were made to contact each sub-ject. A standardized form that consisted of 6 questions wasused to conduct the scripted interview (Figure). Additionaldata points collected included maximum time the patientwaited before leaving, age, gender, and chief complaint.All data were deidentified and then entered into a securedspreadsheet for analysis.
DATA ANALYSIS
Mean and percentage were described for age and gender ofpatients treated in the emergency department and thosewho LWBS. Reasons for leaving without being seen weresummarized. A paired-samples t test was performed to de-termine differences in wait times. χ2 Analysis was used todetermine differences in age and gender.
Results
During the study period, 127 patients left without beingseen. In the LWBS patient population, the mean age was27.9 years, and 42.7% were male; in the total ED pop-ulation, the mean age was 41.3 years and 48% were male(P < .001 for age). The LWBS population represented1.1% of our total ED visits (11,147) during the 2-monthstudy period. Of the eligible patients, 72 (56.7%) werecontacted by phone, consented to be interviewed within8 days of their LWBS ED visit, and completed the survey;thus our final sample size was 72. The sample had a meanage of 29.9 years and 44.4% were male—not significantlydifferent from the entire LWBS population. Eighty-fivepercent of the LWBS group stated that they had a primarycare physician. However, only 16.4% saw their primarycare physician within 8 days of leaving the emergencydepartment. After leaving the emergency department,56.3% reported obtaining medical care within the 4- to8-day time period.
Of our sample, 30 patients reported a mean wait timeof 73.2 minutes before leaving compared with the actual
RESEARCH/Johnson et al
106 JOURNAL OF EMERGENCY NURSING 35:2 March 2009

mean wait time of 70.4 minutes (P = .59; t = 0.546).Pediatric patients waited for a mean of 93.1 minutes andadults waited for a mean of 70.4 minutes. Of the patients,32 (43.8%) reported that during their wait, they wouldhave liked information, laboratory tests, radiographs, andanalgesics. Patients stated that having these things mighthave increased the amount of time that they would havebeen willing to wait.
Of the patients in this study, 78% (n = 56) reported thatthey left because the wait time was too long; 12% (n = 9) leftbecause the original reason for the ED visit resolved duringtheir wait; and the remaining 9.7% (n = 7) gave other reasonsfor leaving such as having had something important to do,perceived triage inequity, and rude ED staff.
Of the LWBS patients, 65% (n = 47) stated during thephone interview that despite the outcome of the visit, theywould return to this emergency department for futureemergency needs. Only 15.3% (n = 11) would not return,and 19.7% (n = 14) would possibly return for future emer-gency care.
Discussion
ED crowding is defined, in part, as waiting more than1 hour to see a physician.10 Our study has shown that this
is the point in time when a patient may LWBS. The pediat-ric patients in this study waited approximately 23 minuteslonger than adults before leaving without being seen. Alarge number of our patients (84.7%) had a primary phy-sician, and over half of the patients were able to obtainmedical care within 8 days of leaving the emergency depart-ment. The reasons for not initially seeing their primaryphysician are uncertain. One can speculate that they wereunable to obtain a timely appointment or were unable toobtain an appointment because of an outstanding bill.
The majority (76.7%) of patients left because of thelong wait. Almost half (43.8%) of our patients stated thatthey might have waited longer if provided with some “com-fort measures,” such as analgesics, information, or initiationof diagnostic testing. These measures can be incorporatedinto the triage process and possibly reduce the LWBS num-ber. Diagnostic testing in triage is becoming more com-mon, using chief complaint–driven protocols.
A significant number of patients (12.5%) left becausethe original problem resolved while waiting to be seen. Wemight speculate that these were self-limited and benignillnesses. Future studies should evaluate this subgroup ofpatients. Eleven percent left for other reasons that includedhaving had something important to do, perceived inequityin triage, and rude ED staff. These problems are potentiallycorrectable with staff training, explanation of the triagesystem, and discussing with patients the approximate waittimes.11 Our LWBS patients might have waited longer iftriage testing was performed, including radiography orlaboratory tests, and attention given to pain managementwith ice or analgesics. Since the completion of this study,we have developed protocols for initiation of diagnostictesting in triage.
Our LWBS patients were significantly younger thanour general ED population and more likely to be pediatricpatients. Other studies have shown that the LWBS popula-tion is younger, nonwhite, and uninsured.2 It is uncertainwhy these patients are more likely to LWBS. However, thetriage nurse should direct attention to these populationsduring periods of long waits. This might include commu-nication regarding the triage process and comfort measures.
Compared with national data, our LWBS number issmall. However, it is still important to decrease or eliminatepatients who LWBS. This group has a significant financialimpact on the health care system12 and might suffer ad-verse health consequences. By use of the methodology ofFalvo et al,12 net revenues lost from LWBS patients peryear can be calculated for our emergency department (aver-age gross charge [$858] multiplied by average collectionrate [0.64], multiplied by number of LWBS patients peryear [n = 715] = $392,621). If 1% to 2% of ED patients
Study Number _________
Hello, I am (nurse name) calling from the XXXX Hospital Emergency Department. Howare you feeling today? We are conducting a research project. Are you willing to answer afew questions regarding your recent visit to the Emergency Department? The information collected will be completely confidential and not shared with any other health care department or provider.
Age____ Sex____ Race______
1. Why did you come to the Emergency Department?
2. Why did you leave?
3. How long did you wait before leaving?
4. What services could we have provided while you waited?
5. If the above services were provided, how much longer would you have waited?
6. Did you seek care for this illness after leaving? YES NO
a. When______________
b. Where_____________
7. Do you have a family doctor? YES NO
8. Would you seek care at the XXX XXXX Emergency Department in the future?
YES NO
Thank you for your time and participation. Any additional comments?
F I G U R E
Telephone survey.
RESEARCH/Johnson et al
March 2009 35:2 JOURNAL OF EMERGENCY NURSING 107

leave the emergency department (an optimistic scenario),this represents 1.1 to 2.2 million patients who leave emer-gency departments per year nationwide. Using the formulaof Falvo et al would yield a staggering $1.2 billion of lostrevenue to health care providers because of LWBS patients.The true number might be larger than this figure if we wereto use actual LWBS data.
Limitations
One limitation of this study is our small sample size. Inaddition, we were unable to contact by telephone 43.3%of the patients who left without being seen during ourstudy period despite 3 attempts to do so. However, thesepatients had similar age and gender distributions whencompared with the final sample. Of the 55 patients whowe were unable to contact, age and gender data were avail-able on 41 patients. Their mean age was 24.5 years and41.5% were male (compared with 29.9 years and 44.4%male in the study group). Though not statistically different,this study was not sufficiently powered to detect differ-ences. Our results are not generalizable to other emergencydepartments with different demographics or staffing.
Implications for Emergency Nurses
The emergency nurse at triage should be aware that in ourstudy, the mean wait time for patients who left withoutbeing seen was 70.4 minutes. Although the national waittime is slightly shorter, at 56 minutes, the triage nurseshould pay careful attention to waiting patients as theirwait reaches the 1-hour point. In addition, ED waitingroom patients should be kept informed, offered comfortmeasures such analgesics, ice packs for painful injuries,and so on, and possibly diagnostic testing, as these mea-sures might increase the time a patient is willing to waitbefore leaving without being seen. The triage nurse caneducate patients about the triage process and potentiallyreduce the number of patient who LWBS. Of course,adequate staffing of the triage area to perform these addi-tional tasks is essential.
Conclusions
Patients leaving the emergency department without fullevaluation are a significant problem in US emergency de-partments from both a health care and financial perspec-tive. The triage nurse can potentially reduce this numberthrough improved patient communication, attention to
patient discomfort, and initiation of diagnostic testing.Younger patients are more likely to leave and do so justbeyond the first hour of waiting.
Acknowledgment
The authors gratefully acknowledge Kristin Thomas, MA, Senior
Research Specialist, Emig Research Center, York Hospital, Pa., for her
participation in this project (statistical analysis).
REFERENCES1. Baker DW, Stevens CD, Brook RH. Patients who leave a public
hospital emergency department without being seen by a physi-cian. JAMA 1991;266:1085-90.
2. Sun BC, Binstadt ES, Pelletier A, Camargo CA. Characteristicsand temporal trends of “left before being seen” visits in US emer-gency departments, 1995-2002. J Emerg Med 2007;32:211-5.
3. Bindman AB, Gumbach K, Keane D, Rauch L, Luce JM. Con-sequences of queuing for care at a public hospital emergencydepartment. JAMA 1991;266:1091-6.
4. Fernandes CMB, Price A, Christenson JM. Does reduced lengthof stay decrease the number of emergency department pa-tients who leave without seeing a physician? J Emerg Med1997;15:397-9.
5. Arendt KW, Sadosty AT, Weaver AL, Brent CR, Boie ET. Theleft-without-being-seen patients: what would keep them fromleaving? Ann Emerg Med 2003;42:317-23.
6. Polevoi SK, Quinn JV, Kramer NR. Factors associated withpatients who leave without being seen. Acad Emerg Med2005;12:232-6.
7. Chan TC, Killeen JP, Kelly D, Guss DA. Impact of rapid entryand accelerated care at triage on reducing emergency depart-ment patient wait times, lengths of stay, and rate of left withoutbeing seen. Ann Emerg Med 2005;46:491-7.
8. Subash F, Dunn F, McNicholl B, Marlow J. Team triageimproves emergency department efficiency. Emerg Med J2004;21:542-4.
9. Paulson DL. A comparison of wait times and patients leavingwithout being seen when licensed nurses versus unlicensed assis-tive personnel perform triage. J Emerg Nurs 2004;30:307-11.
10. Lambe S, Washington DL, Fink A, Laouri M, Liu H, ScuraFosse J, et al. Waiting times in California’s emergency depart-ments. Ann Emerg Med 2003;41:35-44.
11. Lee G, Endacott R, Flett K, Bushnell R. Characteristicsof patients who did not wait for treatment in the emergencydepartment: a follow up survey. Accid Emerg Nurs 2006;14:56-62.
12. Falvo T, Grove L, Stachura R, Zirkin W. The financial impactof ambulance diversions and patient elopements. Acad EmergMed 2007;14:58-62.
RESEARCH/Johnson et al
108 JOURNAL OF EMERGENCY NURSING 35:2 March 2009

![American Journal of Emergency Medicine · Trivial b50 mL Seen only in systole Posterior atrioventricular groove; may be physiologic [8] Small 50–100 mL b10 mm Seen throughout cardiac](https://img.pdfslide.us/doc/110x75/601cab8c3248445e557ee717/american-journal-of-emergency-medicine-trivial-b50-ml-seen-only-in-systole-posterior.jpg)