Embed Size (px)
Citation preview
PATIENT SELECTION PUSHING THE FRONTIERS
OF DAY SURGERY
Dr Theresa Hinde
Anaesthetic ST7
Council Member
British Association of Day Surgery
HOW A DAY SURGERY MINDSET CAN TRANSFORM THE OUTCOMES FOR
BOTH YOUR PATIENTS AND YOUR HOSPITAL
How a your
AIMS
• Is anyone medically inappropriate for day surgery?
• Additional considerations for urgent/emergency surgery
• Different approaches to social factors limiting suitability
• What procedures can we tackle?
BACKGROUND: PATIENT SELECTION
• More complex procedures
• Patients with significant co-morbidities
EMERGENCY AMBULATORY SURGERY
• Demand for emergency surgical activity increasing
• Need more effective ways to
• evaluate and care for patients whilst avoiding
unnecessary admissions
• maximise theatre utilisation
• improve in-patient access for sickest patients
BACKGROUND
• To maximise day surgery possibilities in your organisation are there
• Robust assessment systems?
• Options of
• Advanced surgical techniques?
• Advanced anaesthetic techniques?
• Different ways to care post discharge?
• Ways to rapidly access urgent lists for certain procedures?
ROBUST ASSESSMENT SYSTEMS
• Appropriate staff making decisions regarding suitability
• Experienced nurses using well established protocols
• Experienced clinicians available for advice and support if criteria not clearly met
• Both will help to overcome perceived barriers
• Early stages of new pathways
WHAT ARE WE TRYING TO ESTABLISH
• Are this patient’s risks increased in any way by
treatment on a day stay basis?
• Would management be different if he/she were
admitted as an inpatient?
IF THE ANSWER IS ‘NO’… . .
…..the patient is probably suitable for day surgery
Consider day surgery as default for elective surgery

MEDICAL FACTORS 1980 ’S
Royal College of Surgeons of England:
• 1985 and 1992
Selection Criteria:
• Age limit 65-70 years
• ASA I & II
• BMI<30
• Max 60 minutes operating time
NOUGHTIES
Default to Day Surgery
“Patients should only be excluded from day
surgery after full pre-operative assessment
shows a contraindication”
Day Surgery: Operational guide. DoH, London (2002)
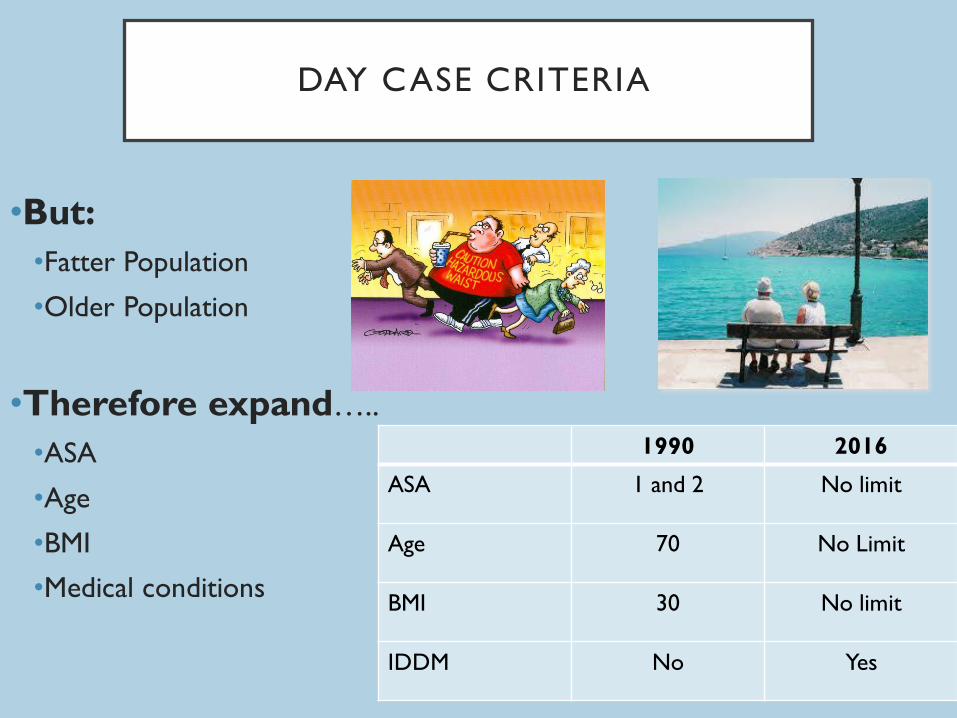
DAY CASE CRITERIA
•But:
•Fatter Population
•Older Population
•Therefore expand…..
•ASA
•Age
•BMI
•Medical conditions
1990 2016
ASA 1 and 2 No limit
Age 70 No Limit
BMI 30 No limit
IDDM No Yes
‘ASA’ CLASSIFICATION (AMERICAN SOCIETY OF ANAESTHES IOLOGISTS)
• ASA I: Normally healthy
• ASA II: Mild systemic disease
• ASA III: Severe systemic disease
that is not incapacitating
• ASA IV: Incapacitating disease that
is a constant threat to life
• Most stable conditions can
be managed as a day case
• Most patients with unstable
conditions should not be
undergoing elective surgery
• Urgent or emergency
surgery in these patients
may require inpatient stay
ASA III PATIENTS
• ASA III patients form a disparate group
• Studies show ASA III does not predict unplanned admissions
• Ansell and Montgomery (BJA, 2004)
• Case matched study
• Admission rate is low (<3%) ASAIII = 2.9% vs non ASA II =1.9%
• Low incidence of unplanned contact with healthcare services in both
groups
• Low post operative complication rate
ASA III PATIENTS
• Conclusions:
• ASA III need not be an exclusion criterion
• Certain ASA III patients can be safely treated with good
pre operative assessment and preparation
ELDERLY BENEFITS OF DAY SURGERY
• Decreased impact on patient and family
• Usually better managed in their own environment
• Maintains daily routine and autonomy
• Decreases cognitive dysfunction and delirium
• Resumption of ‘active mobility’
PREOPERATIVE ASSESSMENT OF ELDERLY
• Follow standard protocols for evaluation and preparation
• Consider ‘frailty’ scores
• Use of these is increasing
• Social planning: involve
• Family
• Primary care physicians
• Other allied health professionals
ANAESTHETIC AND SURGICAL TECHNIQUES
• Schedule early in day
• Avoid prolonged fasting
• Employ minimally invasive surgical options
• Avoid opiates
• Local anaesthetics as far as possible
• Maintain temperature
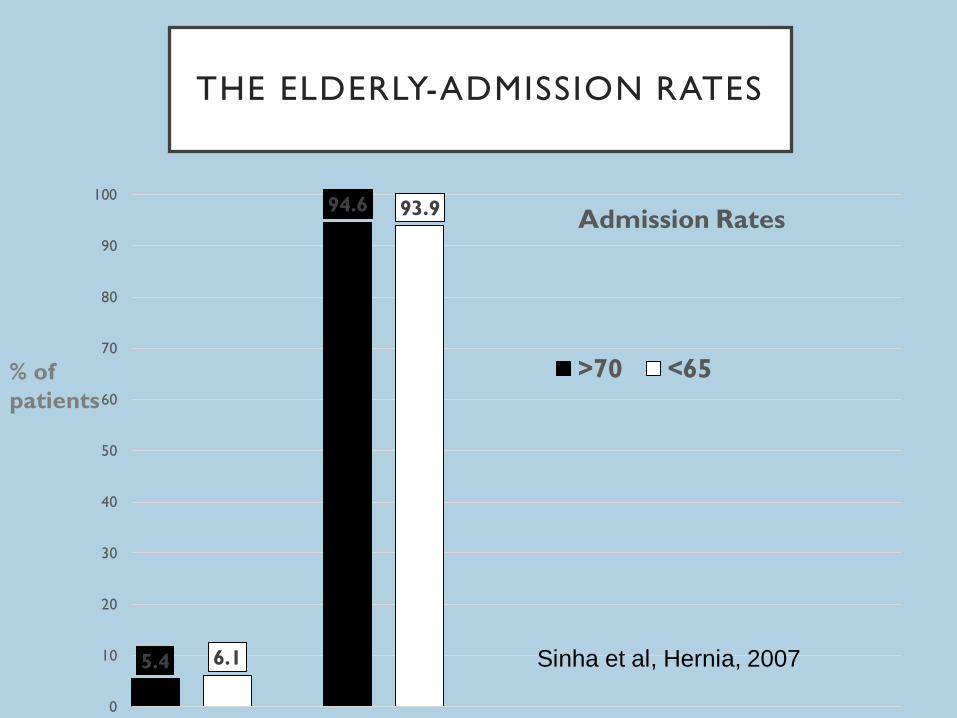
THE ELDERLY-ADMISSION RATES
5.4
94.6
6.1
93.9
0
10
20
30
40
50
60
70
80
90
100
unplanned admission successful discharge
Admission Rates
>70 <65
Sinha et al, Hernia, 2007
% of
patients
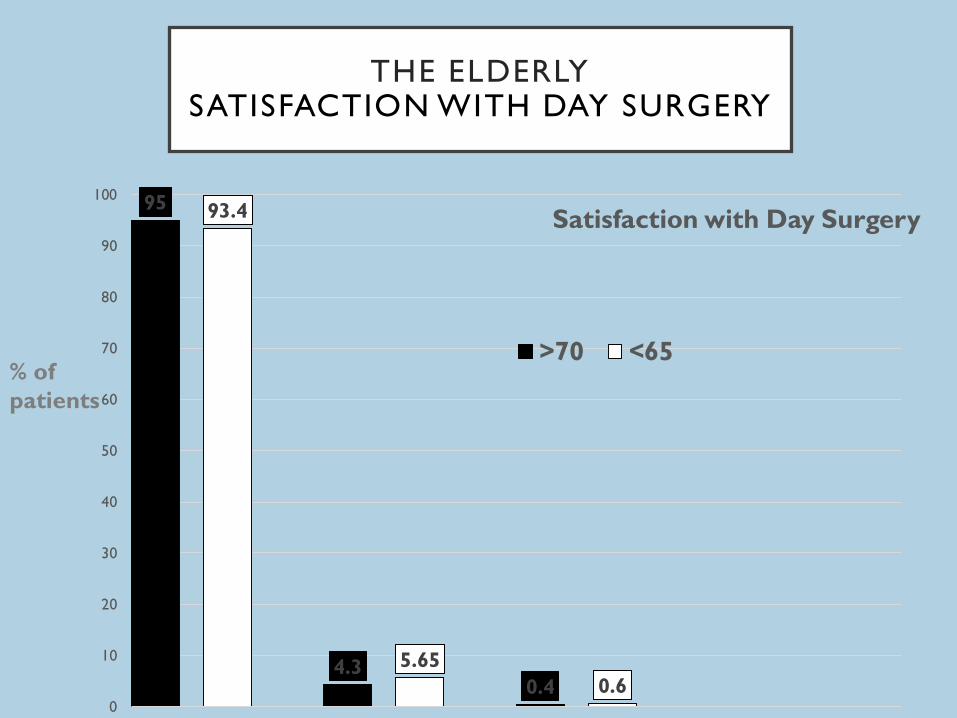
THE ELDERLY SATISFACTION WITH DAY SURGERY
95
4.3 0.4
93.4
5.65
0.6 0
10
20
30
40
50
60
70
80
90
100
Very satisfied Satisfied Not satisfied
Satisfaction with Day Surgery
>70 <65% of
patients
OBESITY
• “most potential complications of obesity are limited to the intra
and immediate post operative environment and so obese
patients can still be managed as a day case”
• The Pathway to Success – Management of the Day Surgical Patient
• BADS Publication 2012
OBESITY
• Even morbidly obese patients can be safely managed in expert hands, with appropriate resources.
• Obese patients benefit from:
• short duration anaesthetic techniques
• early mobilisation
• decreased hospital stay and associated hospital
acquired complications
Day Case and Short Stay Surgery (2)
Association of Anaesthetists of Great Britain and Ireland
British Association of Day Surgery 2011
PREOPERATIVE ASSESSMENT
• Careful assessment mandated
• Medical case note review
• Increased incidence of
• Hypertension
• Ischaemic heart disease
• Diabetes
• Reflux
• Optimise these conditions
• Particular attention when assessing for urgent surgery
• Obesity alone should not preclude day surgery
OBESITY
• Challenges:
• Problems occur early (induction/primary recovery)
• Everything may be more difficult and take longer
• Senior staff required
• Additional kit
• Plan for difficult airway, long instruments, special table etc..
OBESITY-COMPLICATIONS
• Retrospective analysis of DSU patients
• 258 patients with BMI>35
• No statistically significant difference in:
• Unplanned admission rate
• BMI >35=3.0% vs. BMI<35 = 2.7% (p=0.98)
• Post operative complications
• Unplanned usage of community and hospital based services (p=0.59)
• Conclusion:
• No evidence that BMI>35 solely an exclusion criterion for day surgery
Davies, Houghton and Montgomery, Anaesthesia 2001
OBESITY
• May not be appropriate for surgery in an isolated site, but
can still be day cases through main hospital facilities
• Once they are through primary recovery no increased risk
of complications necessitating overnight stay
OSA
• May require CPAP post-op
• Are they more likely to get this at home or in hospital?
• Beware of strong opiates
• Significant OSA in patients undergoing tonsillectomy is a
contraindication to day surgery
IDDM: AAGBI GUIDELINES(2016)
• If HbA1c greater than 69mmol.mol-1 delay elective surgery
until controlled
• Diabetics are usually better at managing their own diabetes
than we are!
• Preoperative optimisation from specialist diabetic nursing
teams is invaluable for patients with poor control
• Urgent surgery may require pragmatic approach
HYPERTENSION: AAGBI GUIDANCE (2015)
• BP >180/110:
• Refer to GP for assessment
• Aim to control to <160/100
• BP >140/90 but less than 180/110:
• Refer to GP but no reason to postpone surgery
• Urgent surgery may require pragmatic approach
CARDIAC RISK
• The likelihood of perioperative cardiac complications
cannot be entirely predicted.
• There are major, intermediate and minor predictors for
peri-operative cardiac complications.
• Refer those with major risk factors for further management
• Assessment of exercise tolerance is fundamental.
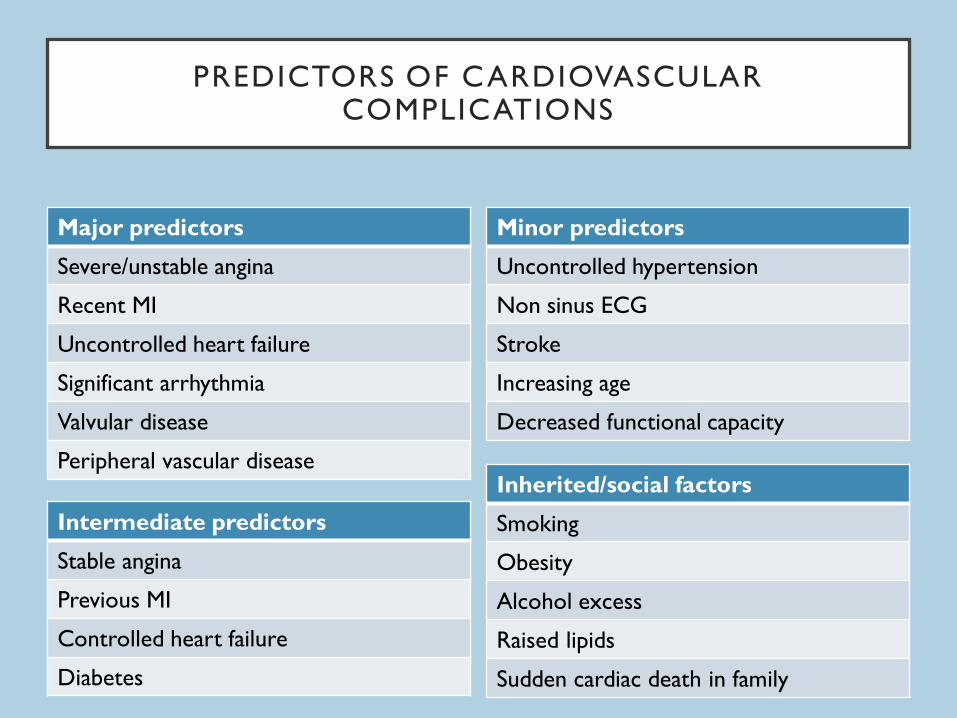
PREDICTORS OF CARDIOVASCULAR COMPLICATIONS
Minor predictors
Uncontrolled hypertension
Non sinus ECG
Stroke
Increasing age
Decreased functional capacity
Intermediate predictors
Stable angina
Previous MI
Controlled heart failure
Diabetes
Inherited/social factors
Smoking
Obesity
Alcohol excess
Raised lipids
Sudden cardiac death in family
Major predictors
Severe/unstable angina
Recent MI
Uncontrolled heart failure
Significant arrhythmia
Valvular disease
Peripheral vascular disease
MEDICAL EXCLUSIONS
• unstable ASA III, ASA IV/V
• any poorly controlled abnormality
• neonates
• ex-prem infants < 60 wks post conceptual age
• young sibling of SIDS child
• Specific to Emergency Surgery pathways:
• Sepsis or haemodynamic instability
CRITERIA IN 2017
• Abandon universal selection criteria
• Adopt an inclusion rather than an exclusion
philosophy
• Apply limitations to the procedure rather than the
patient
EMERGENCY AMBULATORY SURGERY
• Novel approaches:
• University Hospital Bath
• Emergency ambulatory surgery clinic
• Careful and timely case and patient selection may allow
urgent/emergency day case surgery
• Preoperative assessment may therefore be required for
• acutely unwell patients
• to be operated on the same or next day
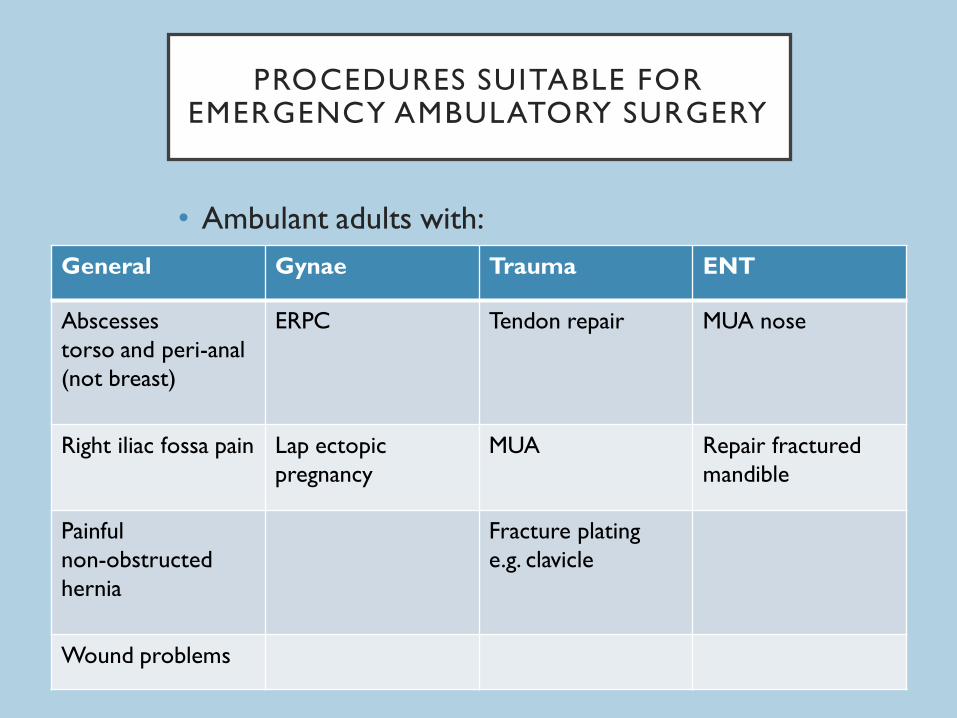
PROCEDURES SUITABLE FOR EMERGENCY AMBULATORY SURGERY
• Ambulant adults with:
General Gynae Trauma ENT
Abscesses
torso and peri-anal
(not breast)
ERPC Tendon repair MUA nose
Right iliac fossa pain
Lap ectopic
pregnancy
MUA Repair fractured
mandible
Painful
non-obstructed
hernia
Fracture plating
e.g. clavicle
Wound problems
PATIENTS NOT SUITABLE FOR EMERGENCY AMBULATORY SURGERY
• Children
• Evidence of sepsis or haemodynamic instability
• Significant concurrent illness
• Condition that cannot safely be left or too painful to
manage at home
• Reduced mobility/no home input/lives alone or some
distance away
• Cognitive or communication difficulties
BENEFITS OF EMERGENCY AMBULATORY SURGERY
• Avoids unnecessary admission and associated in-patient
waits
• Saves bed days
• Freeing up capacity for emergencies
SOCIAL FACTORS
• Responsible adult
• Maximum 1 hours drive
• Adequate facilities
• inside toilet
• telephone access
• heating
• stairs
RESPONSIBLE ADULT
• How long is 24 hours?
• Who can provide this care?
• Are all anaesthetics equal?
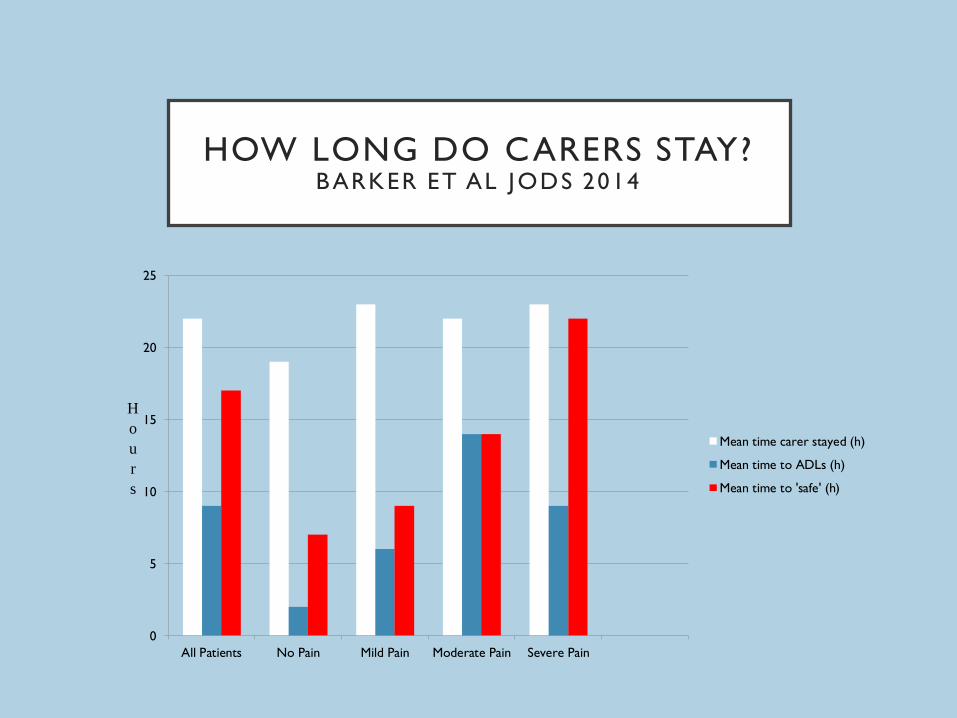
HOW LONG DO CARERS STAY? BARKER ET AL JODS 2014
0
5
10
15
20
25
All Patients No Pain Mild Pain Moderate Pain Severe Pain
H
o
u
r
s
Mean time carer stayed (h)
Mean time to ADLs (h)
Mean time to 'safe' (h)
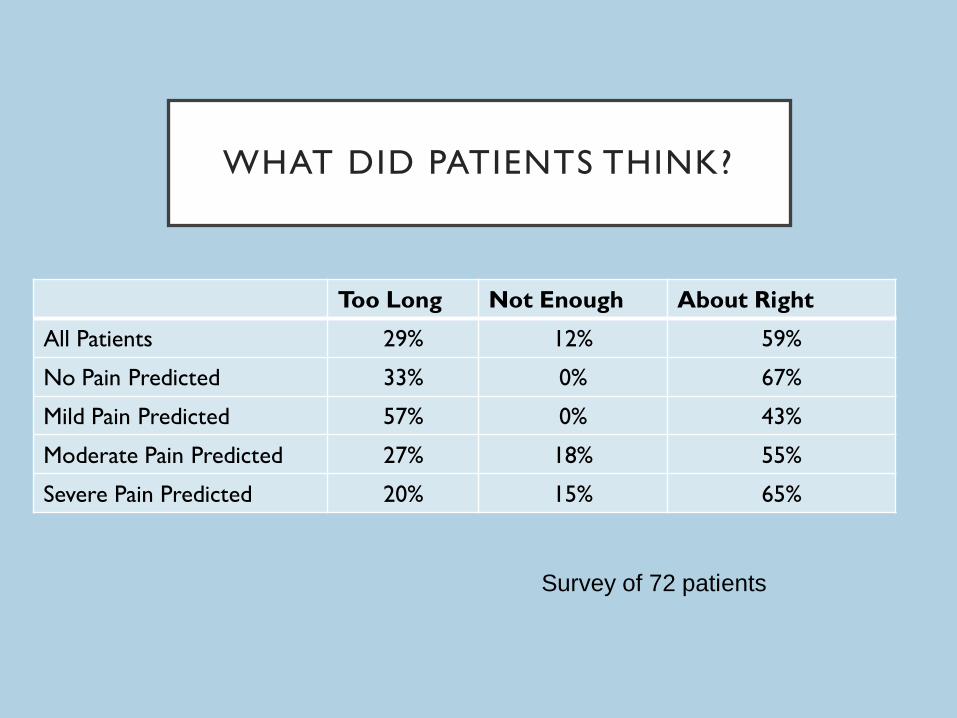
WHAT DID PATIENTS THINK?
Too Long Not Enough About Right
All Patients 29% 12% 59%
No Pain Predicted 33% 0% 67%
Mild Pain Predicted 57% 0% 43%
Moderate Pain Predicted 27% 18% 55%
Severe Pain Predicted 20% 15% 65%
Survey of 72 patients
POSSIBLE SOLUTIONS
• Torbay Model: provide carers into patients homes
• Kings Lynn Model: virtual ward
• Norwich Model: allow some patients home without
carers after certain procedures
• Escort vs 24 hour Care
DISTANCE FROM HOSPITAL
• Rarely a problem (even in mid Wales/rural Devon)
• 1 hour from a hospital that can treat the condition not
necessarily the operating hospital
• Procedure specific

SOCIAL FACTORS
• The vast majority of patients are socially appropriate
for day surgery or can be enabled to be so with
proactive management
SURGICAL CRITERIA
•Which Procedures?
SURGICAL CRITERIA
• Can the patient be expected to manage oral nutrition post-
operatively?
• Can the pain be managed by simple oral analgesia
supplemented by regional anaesthetic techniques?
• Is there a low risk of significant immediate post operative
complications (e.g. catastrophic bleeding)?
• Is the patient expected to mobilise with aids post-operatively?
LONG OPERATING TIMES
‘
Millers Anaesthesia 2010: The duration of surgery in the
ambulatory setting was originally limited to procedures lasting
less than 90 minutes...However, surgical procedures lasting 3 to
4 hours are now routinely performed on an ambulatory basis.’
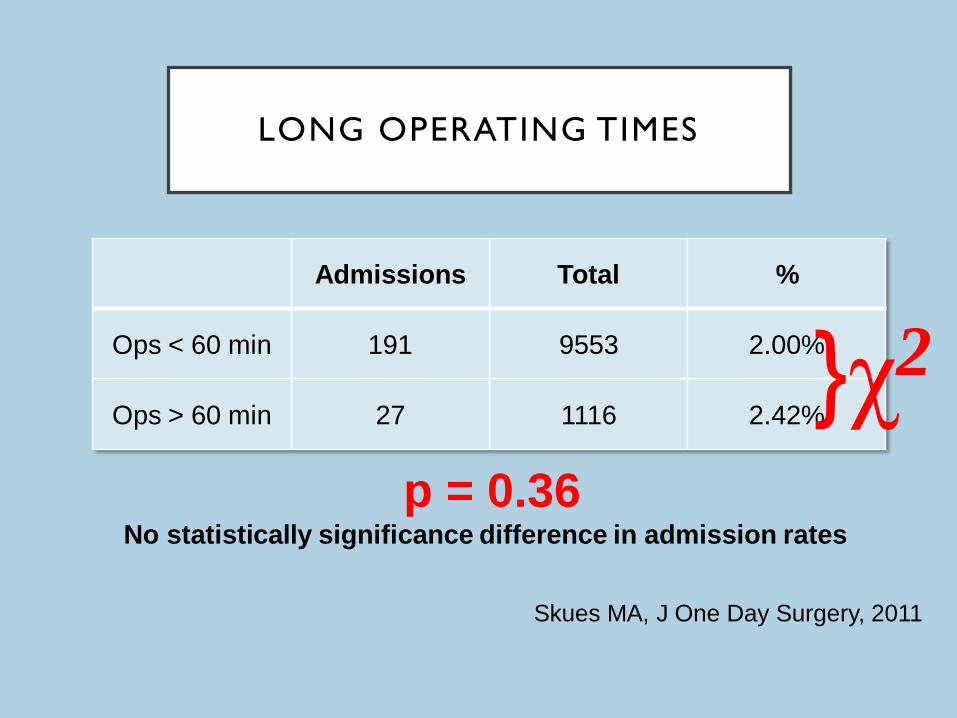
LONG OPERATING TIMES
Admissions Total %
Ops < 60 min 191 9553 2.00%
Ops > 60 min 27 1116 2.42%
p = 0.36 No statistically significance difference in admission rates
}χ2
Skues MA, J One Day Surgery, 2011
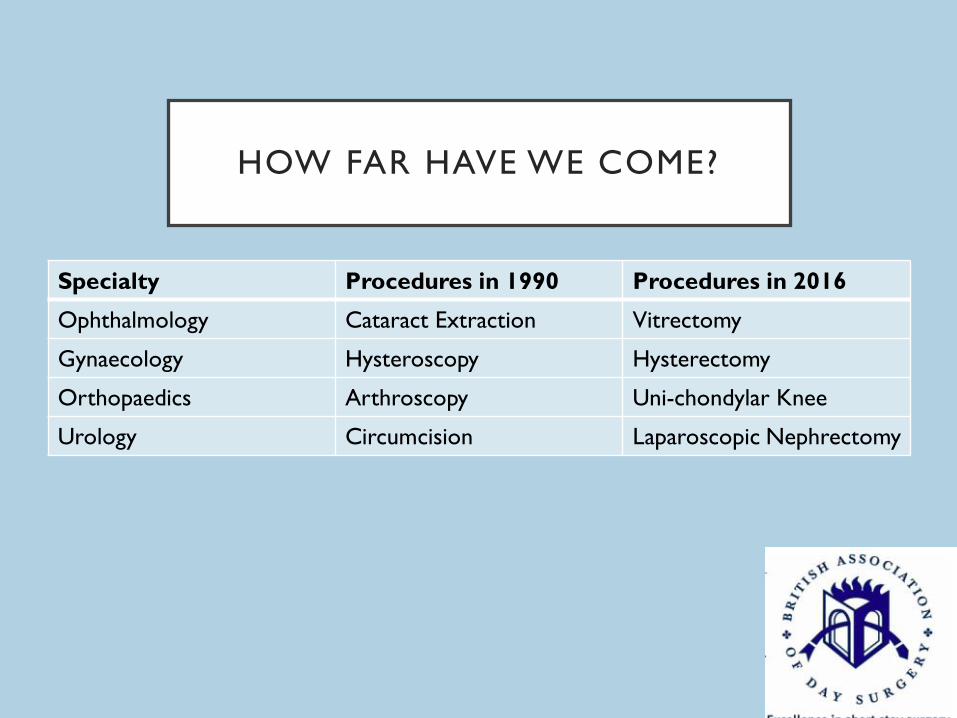
HOW FAR HAVE WE COME?
Specialty Procedures in 1990 Procedures in 2016
Ophthalmology Cataract Extraction Vitrectomy
Gynaecology Hysteroscopy Hysterectomy
Orthopaedics Arthroscopy Uni-chondylar Knee
Urology Circumcision Laparoscopic Nephrectomy
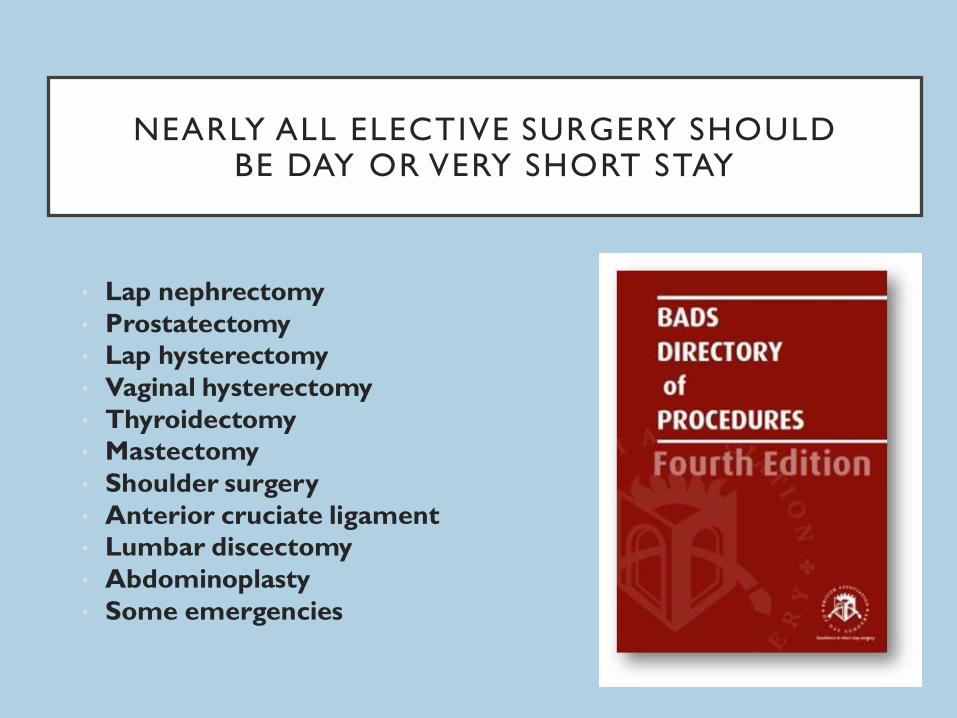
NEARLY ALL ELECTIVE SURGERY SHOULD
BE DAY OR VERY SHORT STAY
• Lap nephrectomy
• Prostatectomy
• Lap hysterectomy
• Vaginal hysterectomy
• Thyroidectomy
• Mastectomy
• Shoulder surgery
• Anterior cruciate ligament
• Lumbar discectomy
• Abdominoplasty
• Some emergencies
SURGICAL CRITERIA
• Pushing the frontiers in your own institution:
• Elective
• Evaluate existing inpatient procedures with short(ish)
LOS
• What would you need to change to enable them to be
day surgery?
IN SUMMARY: PATIENT SELECTION
• Is the patient suitable for day surgery?
• Medical conditions-pushing the boundaries (safely)
• Social circumstances-alternatives
• Surgical considerations-advanced techniques
• Can the patient or procedure be made suitable?
• Special considerations for emergency patients
• Procedure
• Preoperative issues:
• Pain
• Sepsis
• Haemodynamic stability
• Can they safely wait?





























