Embed Size (px)
Citation preview

The Patient Pathway & Administration The Patient Pathway & Administration of CReSTof CReSTof CReSTof CReST
Laura MagillLaura MagillLaura MagillLaura MagillCReST Trial CoordinatorCReST Trial Coordinator
CReST is funded by CRUK and was developed by the NCRI Colorectal Cancer CSGCancer CSG

Participating CentresParticipating Centres
71 confirmed or interested CReST centres –
37 Northern centres

Eli ibilit C it iEligibility Criteria
Inclusion criteria:Radiologically proven colonic obstruction of left colon/upper rectum
presumed secondary to a carcinomapresumed secondary to a carcinomaFit for surgery
Exclusion Criteria:Signs of peritonitis and/or perforation Right iliac fossa tenderness & features of incipient caecal perforationObstruction in the rectum, that may require neoadjuvant therapy (i.e. tumours
in the mid or lower rectum)Unfit for surgical treatments or refuse surgical treatment.

Patient Pathway in CReSTPatient Pathway in CReST

Id tif i Eli ibl P ti tIdentifying Eligible Patients
Patients admitted acutely
Patient has FBC, U&E estimation and liver function tests
Patient has CT scan or contrast enema to confirm obstruction
Patient consent is obtained either from the e co se s ob ed e e o epatient or an appropriate consultee
Patient is randomised & put forward for relief of obstructionwithin 24 hours of admission

i CPatient Consent Process
Fully informed consent always sought, but not always possible in CReST
E t d l M t l H lth A t d EU Di tiEmergency consent procedures apply – Mental Health Act and EU Directive guidelines
Cascade system in place for patients unable to consent for themselves:Cascade system in place for patients unable to consent for themselves:- Informed assent from next of kin or equivalent- Doctor not connected with CReST
Each centre to identify doctor(s) for out-of-hours consent
If i f ti t th t bl t th t t ti l ti t ldIf no information to the contrary, reasonable to assume that a potential patient would wish to enter the trial.

Patient Consent & Randomisation
Randomisation by
i) Telephone 0800 953 0274i) Telephone – 0800 953 0274
ii) https://www.trials.bham.ac.uk/CReST
Once patient randomised BCTU send reminder e mail to either:reminder e-mail to either:
- CReST radiologist to request Colorectal Stent insertion Form
- CReST surgeon to request Colorectal Intraoperative Form
Sample GP letter –sent out after randomisation

Patient pathway after p yrandomisation
RObstructing Colorectal cancer
Emergency surgery
Insertion of endoluminal stent
Failed stenting
Palliative
Inclusion criteria e.g. diagnosis by CT scan or contrast enema
Successfuldecompression
Elective surgery
Palliative care
surgery
All patients relieved of obstruction within 24 hours of admissionAll patients relieved of obstruction within 24 hours of admission

Patient pathway after randomisation
Form completed either immediately for patients allocated emergency surgeryg y g y
Or, form completed at surgery ideally 1 -4 weeks after
d i i f i drandomisation for patients stented
Records surgical complications
Reminder e-mail to surgeon if form not received by BCTU within 30 days of surgery
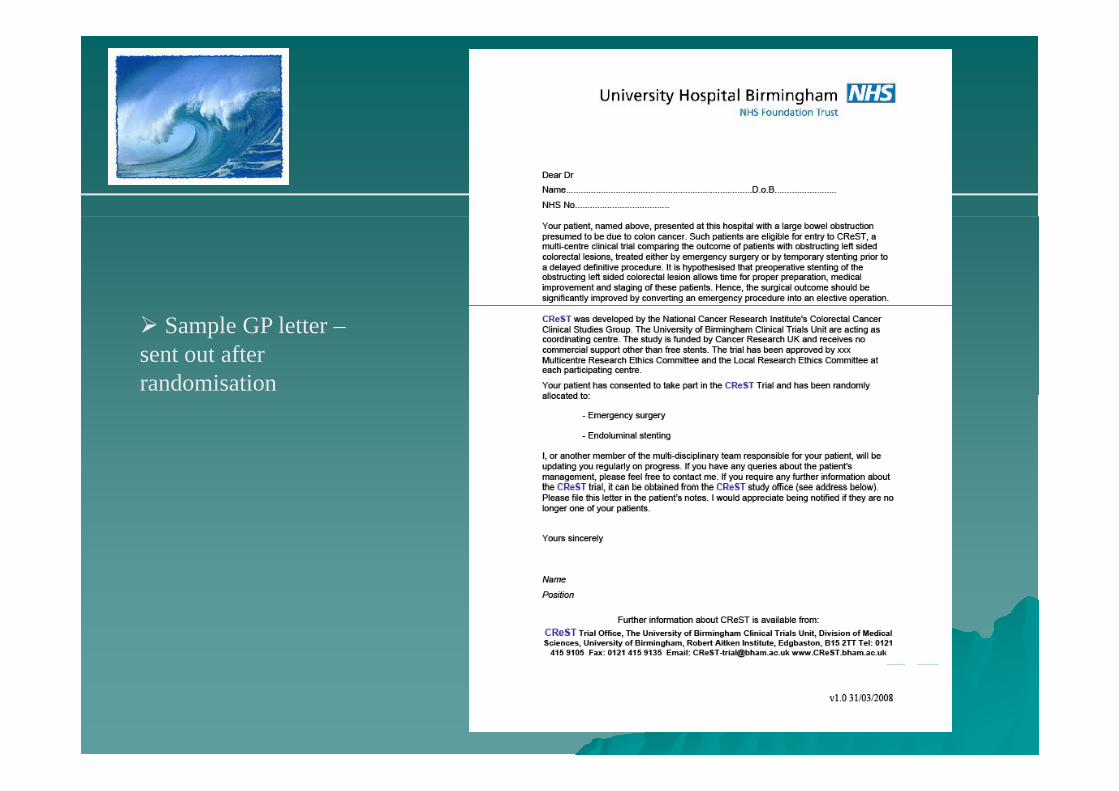
Stent Insertion Form
Collects details of stent procedure
Captures any complications either during or immediately after the stenting procedure

Stent follow-Up form
Records early and lateRecords early and late complications
Stent failure is defined as failure to relieve obstruction within 48 hours
Karnofsky and WHO collected 48 hours post-stent and immediately prior to surgery

C P thCommon Pathway –Hospital Discharge Form
Post-operative complications recorded for all patients at 30-days post surgerydays post surgery
Form completed by research nurse at site
Research nurse sent reminder via e-mail that form due for completion

Common Pathway –F ll UFollow-Up
Follow-up at 6 months
Then annual FU for 3 years
If patient has had surgery? WasIf patient has had surgery? Was surgery curative?
FU form requests recurrence & death info, protocol deviations, events requiring hospitalisation
QoL assessed using EQ 5DQoL assessed using EQ 5D, EORTC QLQ-C29 and C30.

Serious Adverse EventsSerious Adverse Events
SAEs – fatal, life-threatening, require or prolong hospitalisation or are significantly or permanently disabling
For purposes of trial, adverse events include, but aren’t limited to:
- Failure to deploy the stent
- Bowel perforation
- Stent displacement
All SAEs reported to BCTU within 1 week

Serious Adverse Event Reporting
MUST be reported to BCTU within 1 week
Addn info may be requested from siteAdd info may be requested from site
Local PI to assign causality SAE before reporting
F h AE tFor each AE report:- full details with diagnosis, if possible- start and end dates, times
action taken- action taken- outcome- causality
BCTU to report SAEs to DMEC every 3 months, annual safety reports to MREC & TSCMREC & TSC

How to get involved
Complete the PAF
Send to BCTU at [email protected] or post
BCTU apply for LREC & R&D on behalf of site
Once approved – site file sent out, CRFs provided
BCTU will organise supply of stents to each siteBCTU will organise supply of stents to each site
All info on : www.bham.ac.uk/CReST

Contact detailsContact details
Laura MagillCReST Trial CoordinatorBirmingham Clinical Trials UnitDivision of Medical SciencesUniversity of BirminghamRobert Aitken InstituteEd b t
Tel: 0121 415 9105EdgbastonBirminghamB15 2TT
E-mail:[email protected]
bh k/CR STB15 2TT www.bham.ac.uk/CReST