Embed Size (px)
Citation preview

Patient Outcomes After Severe Lower
Extremity Injuries: Limb Salvage vs. Amputation
Lisa Reider, PhD

THE MAJOR EXTREMITY TRAUMA & REHABILITION CONSORTIUM
improving care through collaborative research The goal of METRC is to produce the evidence needed to establish treatment guidelines for the optimal care of the wounded warrior and ultimately improve the clinical, functional and quality of life outcomes of both service members and civilians who sustain major orthopaedic trauma.
WWW.METRC.ORG

METRC Established in 2009 with funding
from the DoD to support a network of 20+ U.S trauma centers, 4 Military Treatment Facilities and one data coordinating center (at Hopkins) to conduct large, multi-center studies addressing treatment and recovery challenges in patients with lower extremity trauma.
Secured over $100 million in funding from the DoD, PCORI & NIH to expand the clinical network and scope of research

Government Steering Committee
Data Standards &Adjudication
Publications
Data Coordinating
Center
Consortium Committee
Consortium Director and Executive Committee
Data Safety Monitoring
Board
Anchor Clinical Sites
(Military & Civilian)
Other Clinical Sites
(Military & Civilian)
Mentoring & Emerging
Investigator
Implementation & Quality
Science

METRC MCC ORGANIZATIONDirector (MacKenzie)
Deputy Director (Castillo)Principal Biostatistician
(Scharfstein)
Associate Director(Frey)
Associate Director (Reider)
COREProtocol Development & Implementation
COREMonitoring, Training & Quality Improvement
COREData Management& Analysis
CORECRF Development & Maintenance
COREInformatics
Chief Operating
Officer(Allen)

METRC ResearchFocus Areas Studies
Early Acute Management PACSPrevention & Treatment of Infection FIXT, BIOBUDEN,
POvIV, OXY, VANCO
Surgical Management to Improve Fracture Healing pTOG, NERVE, OUTLET
Prediction/Prevention of Secondary Conditions METALS II, Long term effects, PRECISE, EMS-BIND, Prevent CLOT
Management of Pain & Psychosocial Factors TCCS, PAINRehabilitation Interventions REPAIR, AlterG,
CBPT
Optimization of Prosthetic & Orthotic Function PRIORITI-MTF,ProFit, TAOS

Research along the care continuum
Cross Cutting Areas: Economic Impact & Cost of Care Measuring Outcomes with PROMIS
Pre hospital management
Acute Care
Rehabilitation
Secondary Outcomes

OUTLET Study
Prospective multi-center observational study comparing 18-month outcomes of patients treated with limb salvage versus early amputation (within 6 weeks of injury) following severe foot & ankle injuries.
We hypothesized that there would be a subgroup of salvage patients who would have had better outcomes had they undergone early amputation

Background
The decision to salvage or amputate severe ankle and foot injuries is still under debate Limb salvage often requires multiple surgeries
to manage soft tissue damage & other injury complications
Significant pain, problems with walking, return to usual activities and in some cases, permanent disability.
No guidelines to inform treatment decisions and it’s unclear who benefits most from an early amputation.

Background
Lower Extremity Assessment Project (LEAP) showed no difference in 2 year outcomes among patients with a bad leg injury treated with limb salvage versus amputation (n=569).
A subset of these patients with open foot and ankle injuries (n=183) that also had significant soft tissue damage reported worse outcomes: Worse self reported function (Sickness Impact
Profile- SIP) More hospital readmissions for complications Longer time to return to full weight bearing
Purpose of the OUTLET Study
Build upon the LEAP sub-study and compare 18 month outcomes of patients undergoing limb salvage versus amputation for treatment of severe foot and ankle injuries.
Identify the injury and patient characteristics that help define the subgroup of patients that would have done better under amputation.
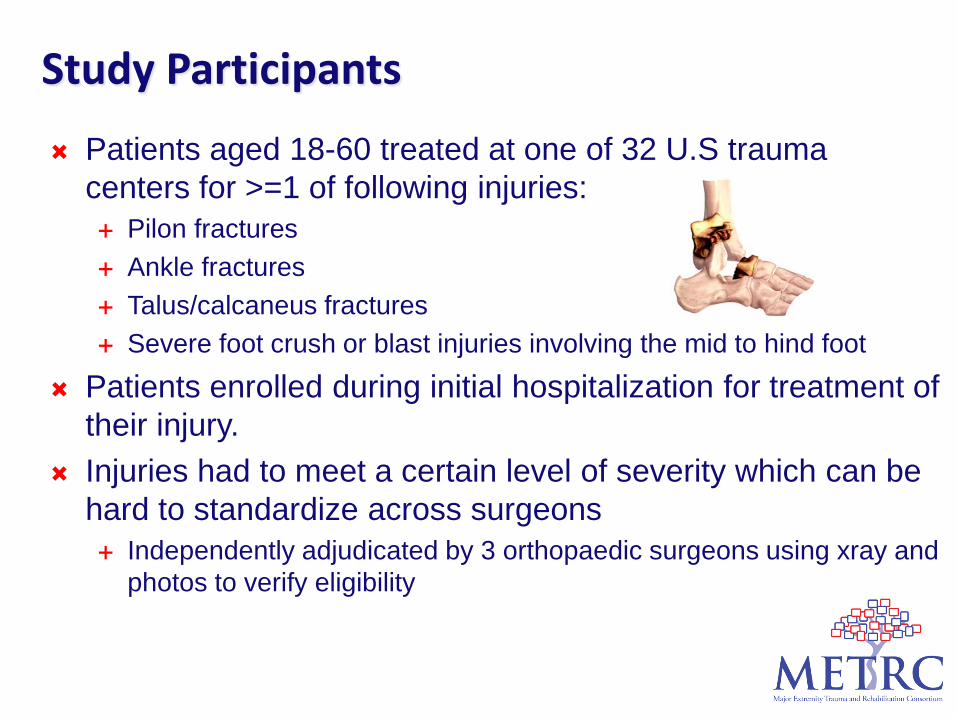
Study Participants
Patients aged 18-60 treated at one of 32 U.S trauma centers for >=1 of following injuries: Pilon fractures Ankle fractures Talus/calcaneus fractures Severe foot crush or blast injuries involving the mid to hind foot
Patients enrolled during initial hospitalization for treatment of their injury.
Injuries had to meet a certain level of severity which can be hard to standardize across surgeons Independently adjudicated by 3 orthopaedic surgeons using xray and
photos to verify eligibility

Outcomes Patients followed at 3, 6, 12 & 18 months post-injury Main study outcomes assessed at 18 months:
Self-reported function using the Short Musculoskeletal Function Assessment (SMFA)
Objective measures of physical performance Secondary Outcomes:
Participation in sports and leisure activities (Paffenbarger Activity Scale)
Return to usual major activities & work productivity

SMFA Validated 46 item questionnaire measuring function in 4
domains (dysfunction index) and the impact of functional deficits (bother index)
Dysfunction index (34 items) Daily activities Arm and hand function Mobility Emotional status
Each domain scored on a scale of 0-100; higher scores= worse function.
No validated MCID; 9 points is considered to be a significant difference.

Physical Performance Agility
Four square step Illinois agility test
Strength Sit to stand Stair ascent
Speed Self selected walk Shuttle run

Physical Performance Tests were selected by an expert panel of PTs
and orthopaedic trauma surgeons Selection criteria:
Easy to conduct in clinic by a trained Coordinator Measures performance at different levels of difficulty
All tests are timed in seconds; faster the time indicates better performance.
Patients who were unable to perform a test due to impairment were included in the analysis as having the worst performance for that given test.

Screened1400
Limb Salvage510
Amputation86
SMFA:67 (78%)
Performance: 58 (67%)
Eligible779
Consented610
Enrolled596 (77%)
Ineligible621
Refused116
Admin withdraw
14
Consent not administered
53
SMFA: 410 (81%)
Performance: 357 (71%)
TAOS Amputation
41
SMFA:20
Performance: 19
SMFA: 87PA: 77

Baseline DemographicsAmputation
(n=112) Salvage(n=510)
Mean Age 40.0 37.7% Male 80% 64%% Non-Hispanic White 71% 68%% Some college 42% 49%% Working Pre-Injury 83% 77%% in Excellent/Very Good Health 71% 62%Mean BMI 29.4 30.1% Current Tobacco User 47% 38%% Non-Extremity ISS > 17 6% 11%

Analysis
Since we can’t randomize patients to limb salvage or amputation, we use a counterfactual approach.
Outcomes observed for salvage patients were compared to the outcomes they would have had, if they had undergone amputation
The analysis uses patient characteristics (i.e. age, co-morbidities, pre-injury function, education) and other injury characteristics (contralateral injuries or injures to other body systems) to impute the outcome of the salvage patients if they had been treated by amputation
Calculate the difference between observed and predicted outcomes

Observed Outcomes: SMFA Scores
Mean SMFA ScoresSMFA Domain
Pop Norm
Salvage Amputation
Dysfunction 12.5 28.9 23.7Mobility 13.6 38.5 29.8Daily Activities
11.8 33.9 28.3
Emotional 20.5 37.4 30.5Hand/Arm 6.0 4.1 4.7
Higher Scores=Worse Function
9 SMFA Points is consider to be a significant difference

Difference in SMFA Score for Patients Treated with Limb Salvage HAD THEY Been Amputated
Observed SMFA score (Under Salvage) –Predicted SMFA score (Under Amputation)
All Patients Pilon/Ankle
Open Mid/Hindfoot
Other Severe Foot
Dysfunction 4.89** 6.11** 4.55** 3.65
Daily activities 5.40 7.00** 4.63 3.96
Mobility 7.97 ** 9.17** 7.71** 6.71**
Emotional status
6.51** 7.04** 6.10** 5.9**

Observed Outcomes: Performance Tests
Median Times (s)Salvage
Time (% impaired)Amputation
Time (% impaired)Four Square Step Test (s) 12.5 (16%) 12.5 (14%
Illinois Agility Test (s) 56.2 (25%) 50.0 (20%)
Sit to Stand Test (s) 14.0 (15%) 12.8 (18%)
Timed Stair Ascent Test (s) 8.5 (20%) 8.0 (15%)
SS Walking Speed (s) 4.5 (11%) 4.0 (10%)
Shuttle Run (s) 35.5 (20%) 32.5 (20%)

All Patients Pilon/Ankle
Mid/Hindfoot
Other Severe foot
Four Square Step Test (s) -1.5 -1.5 -1.5 -1.5
Illinois Agility Test (s) 7.3** 12.0** 9.5** 5.0**
Sit to Stand (s) 1.5 2.3 1.3 1.0 Timed Stair Ascent (s) -1.5 -2.0 -1.0 -1.0
SS Walkingspeed (s) -3.5 -1.0 -1.0 -1.0
Shuttle Run(s) 6.0 ** 12.9** 4.5** 3.3**
Observed Median Time (Under Salvage) –Predicted Time (Under Amputation)

Using regression techniques, we estimated the expected improvement under amputation for salvage patients with these additional characteristics
The following injury characteristics were hypothesized to further impact outcomes: Gustilo type – IIIA,B,C Additional ipsilateral injuries Heel pad degloving Severity of contamination
Impact of Regional Injury Burden

Expected Improvement in SMFA Mobility Open Type III Pilon and IIIB Ankle Fxs if Amputated
Additional Ipsilateral
Ortho Injury
Heel-Pad Degloving
Contamination Expected Improvement Under Amputation
(95% CI)
Yes Yes Yes 13.3 (7.5, 18.5)Yes Yes No 13.5 (7.3, 18.9)Yes No Yes 11.9 (6.8, 17.1)Yes No No 12.1 (6.4, 17.4)
No Yes Yes 10.3 (5, 15.4)No Yes No 10.5 (5, 15.7)No No Yes 8.9 (4.2, 13.8)No No No 9.2 (4.2, 14.3)

Expected Improvement in SMFA Mobility Talus/Calcaneus Fxs if Amputated
Additional Ipsilateral
Ortho Injury
Heel-Pad Degloving
Contamination Expected Improvement Under Amputation
(95% CI)
Yes Yes Yes 10.8 (5.7, 15.8)Yes Yes No 11.1 (5.6, 16.3)Yes No Yes 9.5 (4.6, 14.7)Yes No No 9.7 (4.6, 14.9)
No Yes Yes 7.9 (2.7, 13)No Yes No 8.1 (3, 13.3)No No Yes 6.5 (1.7, 11.7)No No No 6.7 (2, 11.8)

SUMMARY Results suggests that limb salvage patients
with a severe ankle or calcaneus fractures would have had better outcomes had they been amputated Differences are largest among severe pilon/ankle
injuries especially when other ipsilateral injuries and/or heel pad degloving is present
CLINICAL IMPLICATIONS Limb Salvage (even if feasible) might not be the
best option for every patient While these data are not sufficient to generate
patient specific treatment algorithms, they provide a platform for discussions between surgeons and patients related to treatment and expectations for recovery.
Moving in the direction of personalized care.

CLINICAL IMPLICATIONS
These patients (limb salvage and amputees) are still doing poorly 18 months after treatment.
How can we improve outcomes overall? Advances in orthotics (i.e the IDEO brace) Advances in limb prosthetics (ProFit study)

NEXT STEPS
Evaluate secondary outcomes:Return to work/active duty and work
productivity Daily activity using the StepWatchTM activity
monitor

PARTICIPATING CENTERS
Barnes Jewish Hospital, Washington University St. Luke’s Hospital
Carolinas Medical Center St. Vincent's Hospital
Denver Health & Hospital Authority University of Alabama at Birmingham
Duke University Medical Center University of California, San Francisco
Eskenazi Health University of Iowa
Florida Orthopaedic Institute University of Maryland, Shock Trauma Center
Hennepin County Medical Center University of Miami, Ryder Trauma Center
Methodist Hospital University of Mississippi Medical Center
MetroHealth Medical Center University of Oklahoma Medical Center
Naval Medical Center San Diego University of Pennsylvania
New York University, Jamaica Queens University of Pittsburgh
Orlando Regional Medical Center University of Texas Health Science Center, Houston
Orthopaedic Associates of Michigan University of Virginia
Penn State Milton S. Hershey Medical Center University of Washington, Harborview Medical Center
Rhode Island Hospital, Brown University Vanderbilt University
San Antonio Military Medical Center Wake Forest Baptist University Medical Center
St. Louis University Walter Reed National Military Medical Center