Embed Size (px)
Citation preview
Patient-centered HIT: a pediatric case study
Stephen C. Porter MD, MPH, MSAssistant Professor, Harvard Medical School
Affiliate Faculty, Harvard-MIT Division of Health Sciences and TechnologyFaculty, Division of Emergency Medicine,Children’s Hospital Boston
Email: [email protected]
The challenge
• How can technology empower patients as the drivers of safe and effective care?
• How can patients’ knowledge and expertise be systematically– captured– analyzed– disseminated to all stakeholders in the health
care process?
Rules to bridge the quality chasm
• Care based on continuous relationships
• Customization based on patient needs
• Patient as source of control
• Shared knowledge and free flow of info
• Evidence-based decision-making
• Safety as system priority
• Cooperation among clinicians
The scope of patient report
• Symptoms– Illness specific– Guideline specific
• Current medications
• Previous reactions to medications
• Current disease management practice
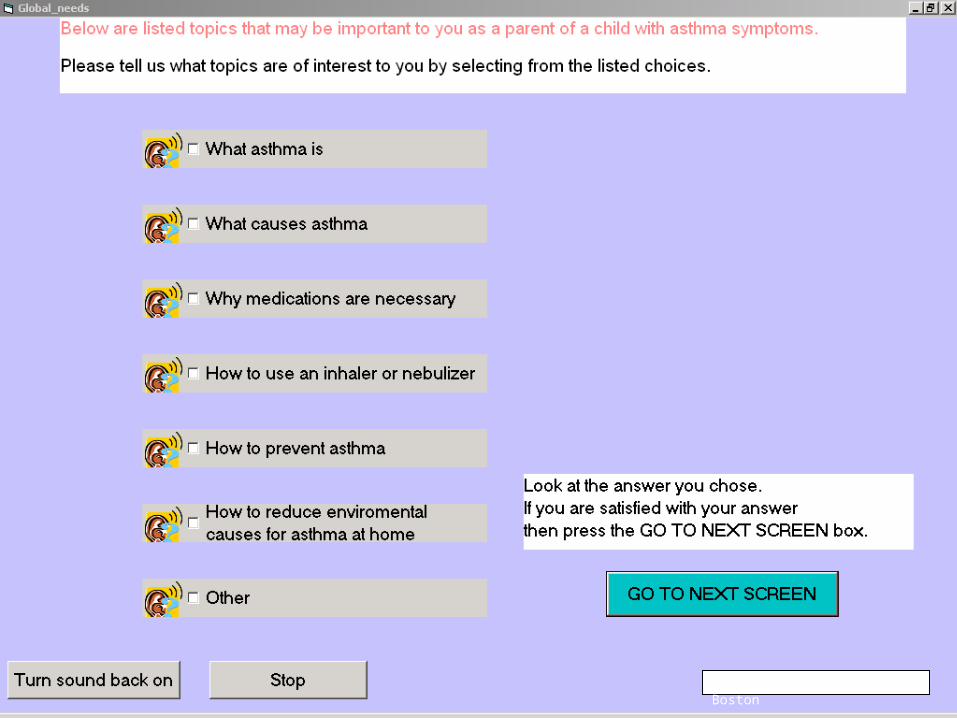
• Unmet needs
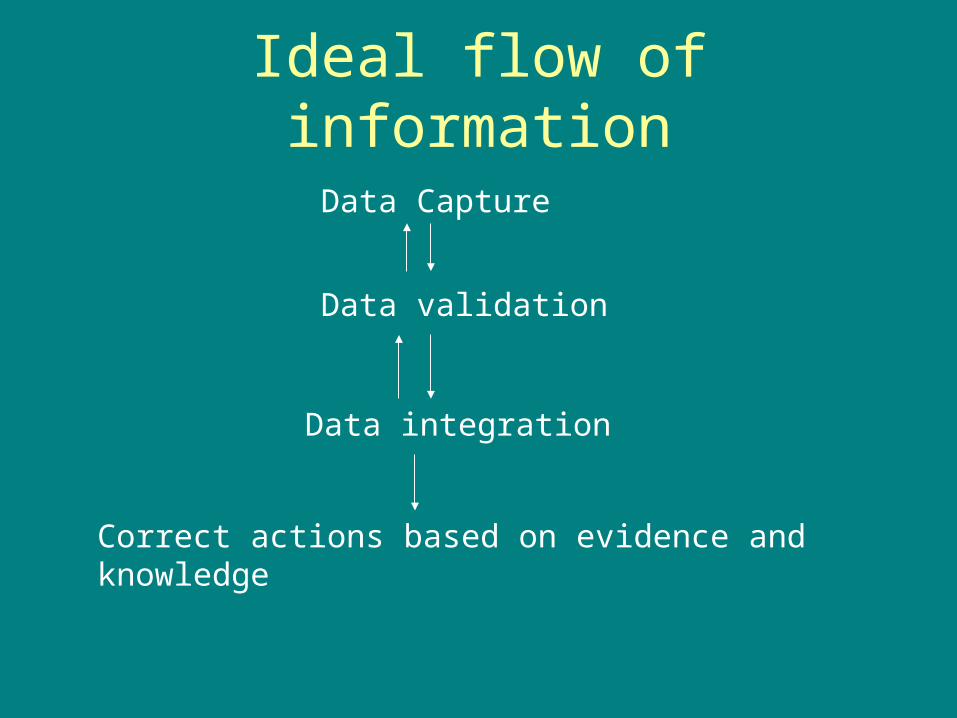
Ideal flow of information
Data Capture
Data validation
Data integration
Correct actions based on evidence and knowledge
Information gaps in emergency medicine
• Critical data points– Medications– Allergies to medications– Immunization history
• Specific disease states– Asthma– Appendicitis
• Specific patient-provider barriers– Language– Literacy
ED Care for Asthma
• ED visit itself a marker of poor control• Significant percentage of patients discharged to
home report persistent morbidity one month later• ED-based barriers to improved care
– Under-recognition of chronic severity– Lack of awareness of patients’ medications– Communication barriers– System constraints– Insufficient discharge planning
Guidelines for Asthma
• Establish patient-clinician partnership• Prescribe anti-inflammatory medications to patients
with persistent asthma– inhaled steroids: recommended first line therapy
• Reduce exposures to precipitants of asthma symptoms
• Train all patients to monitor their asthma
Linking parents’ data to guidelines
• A child with persistent asthma who is not on a controller should be prescribed one– Identify persistent asthma symptoms– Identify current medications
• Establish whether a mismatch exists
• A child with asthma exposed to secondary smoke should have that exposure eliminated– Identify exposure to tobacco
• A child on inhaler(s) whose parent reports non-use of a spacer device should receive device/ teaching– Identify whether spacer device is used for sub-set of
patients who report inhaler medications
A Role for a Patient-driven Information Solution
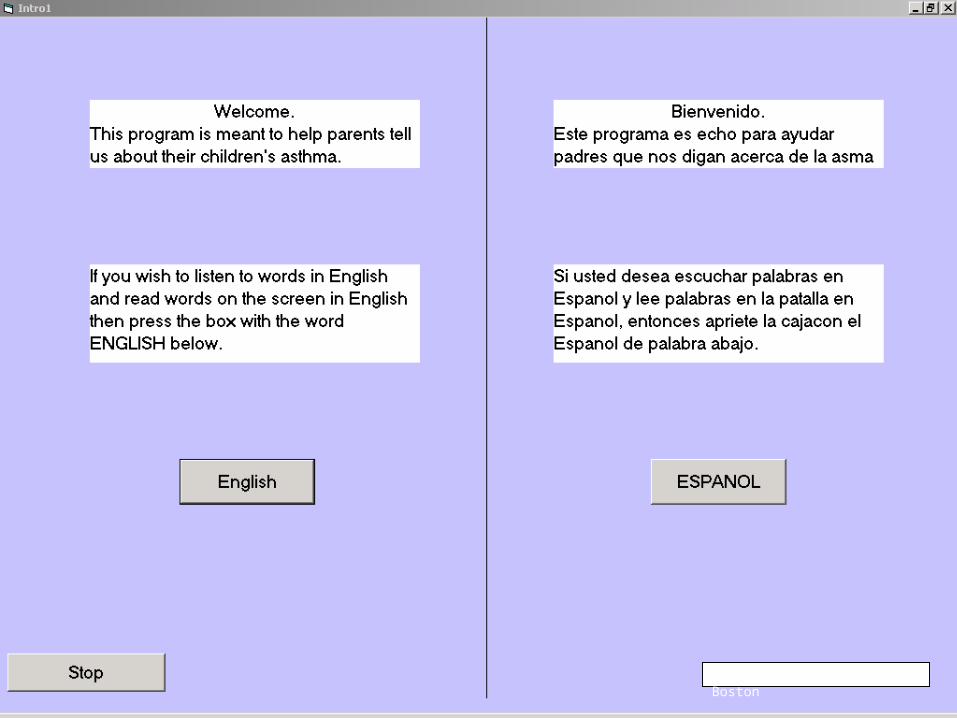
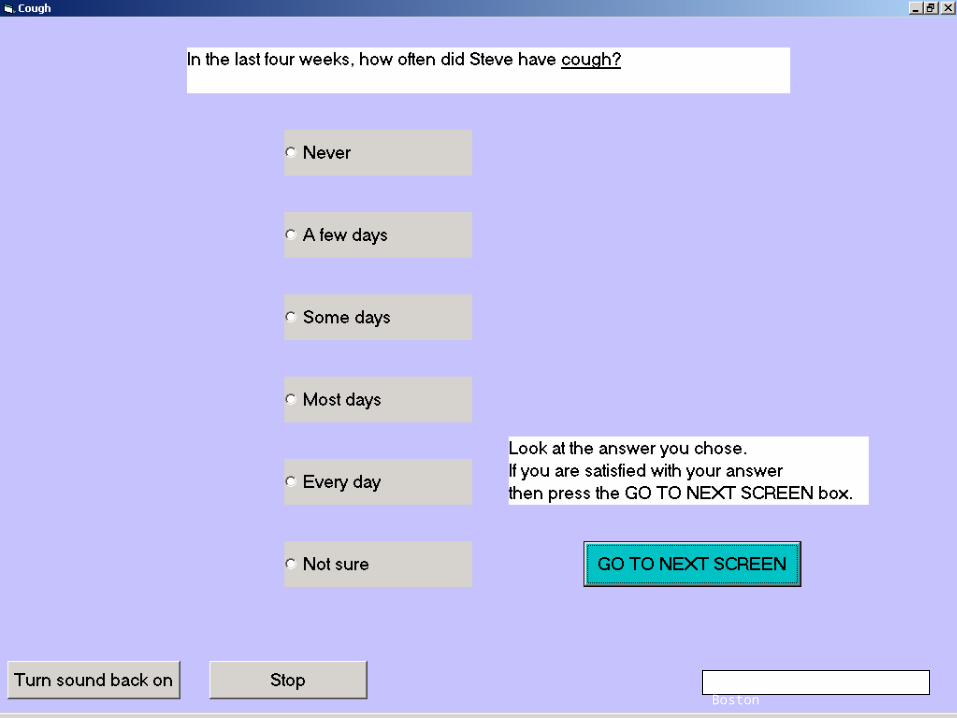
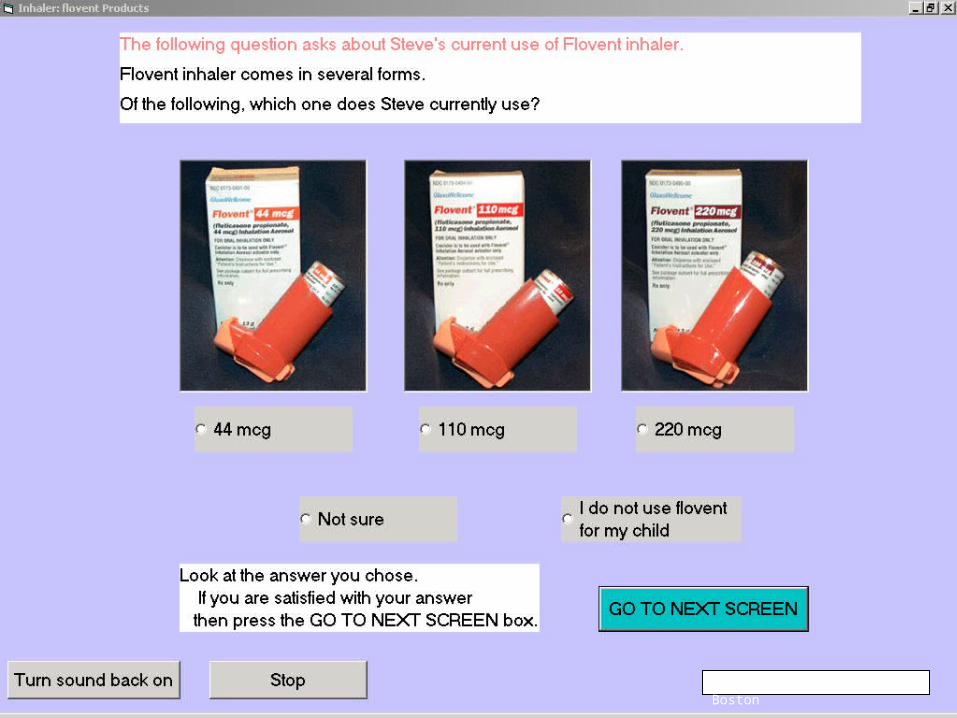
• Parents can independently enter data using a multi-media interface to populate a knowledge engine and drive guideline-endorsed care– Porter et al JAMIA 2004;11:458-467
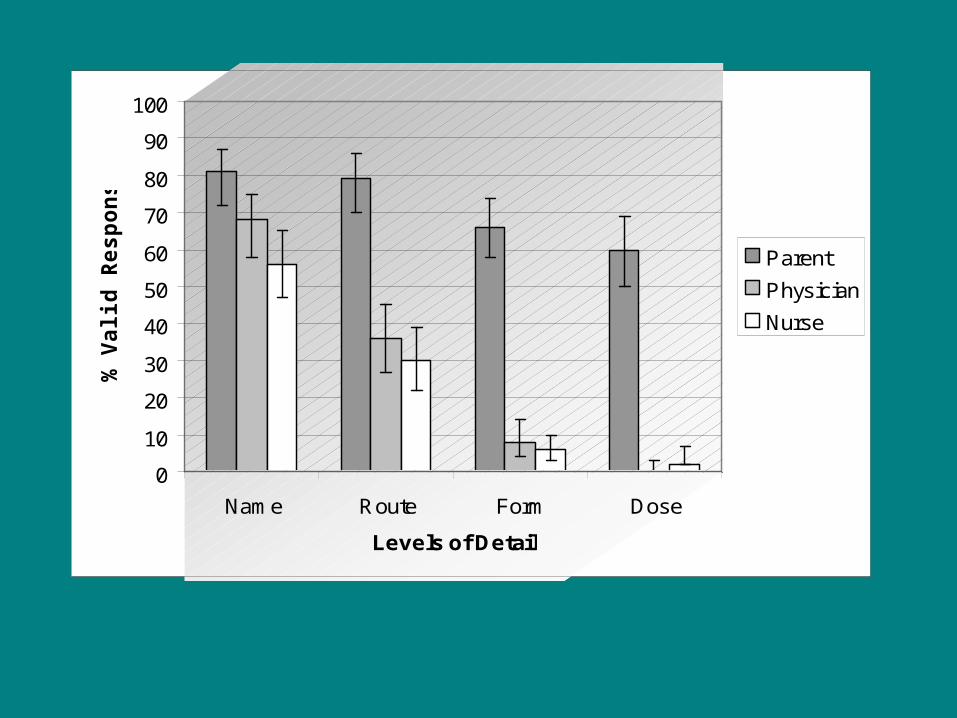
• Parents’ documentation of asthma-specific medication data superior to documentation of ED physicians and nurses– Porter et al JAMIA 2005; 12: 299-305
0
10
20
30
40
50
60
70
80
90
100
Name Route Form Dose
Levels of Detail
% V
alid
Resp
on
ses
Parent
Physician
Nurse

© 2003 Children’s Hospital Boston
© 2003 Children’s Hospital Boston

© 2003 Children’s Hospital Boston
© 2003 Children’s Hospital Boston
© 2003 Children’s Hospital Boston
© 2003 Children’s Hospital Boston
© 2003 Children’s Hospital Boston
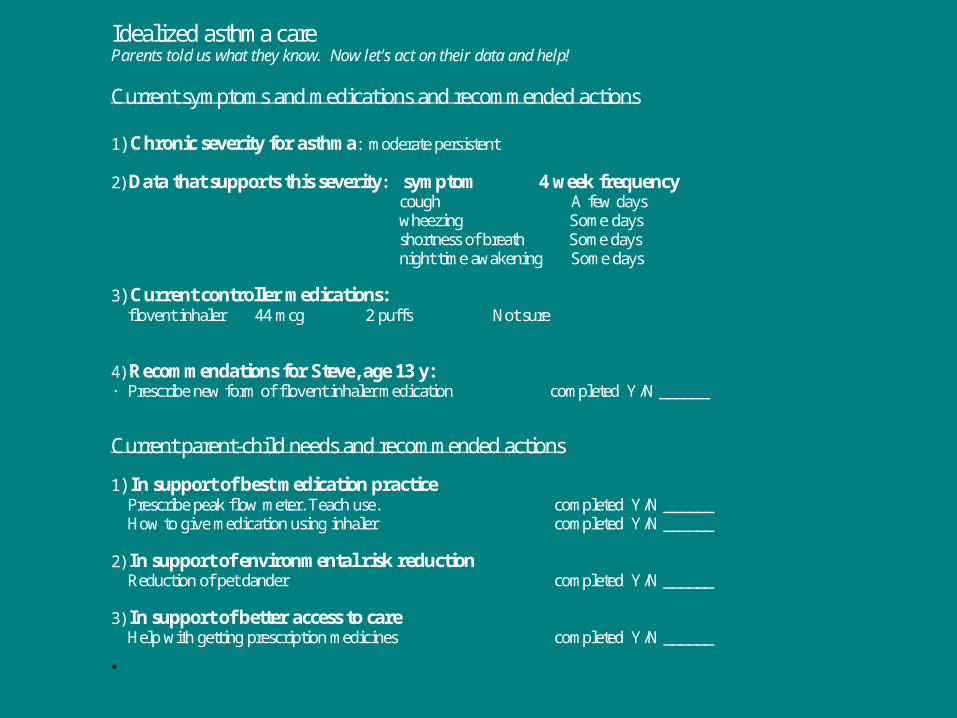
Idealized asthma care Parents told us what they know. Now let's act on their data and help!
Current symptoms and medications and recommended actions 1) Chronic severity for asthma: moderate persistent
2) Data that supports this severity: symptom 4 week frequency cough A few days wheezing Some days shortness of breath Some days night time awakening Some days
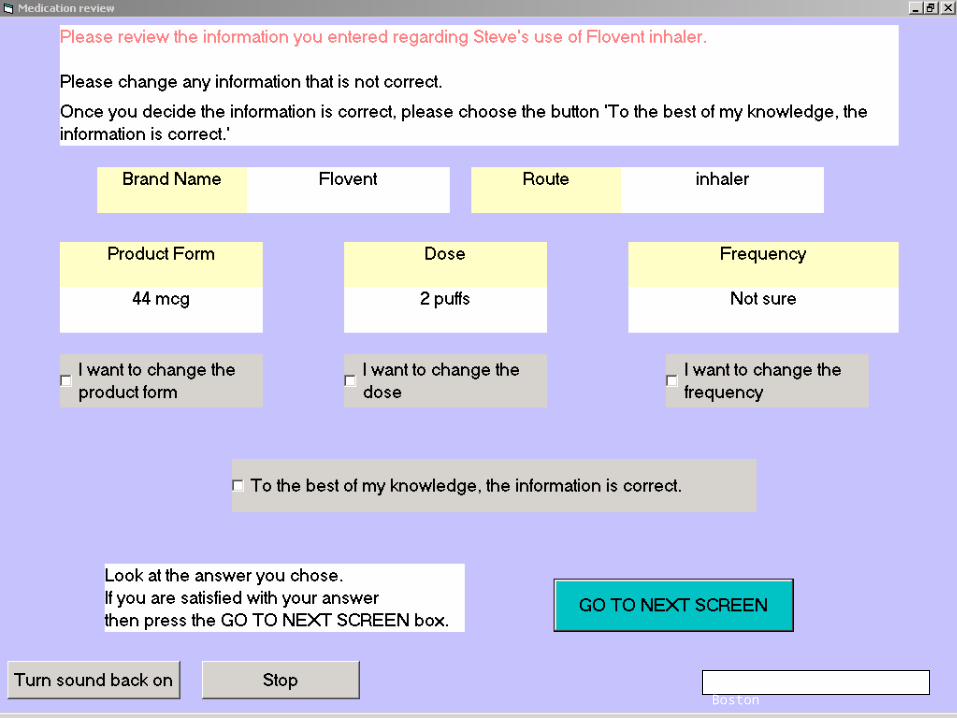
3) Current controller medications: flovent inhaler 44 mcg 2 puffs Not sure 4) Recommendations for Steve, age 13 y: · Prescribe new form of flovent inhaler medication completed Y/N ______
Current parent-child needs and recommended actions
1) In support of best medication practice Prescribe peak flow meter. Teach use. completed Y/N ______ How to give medication using inhaler completed Y/N ______
2) In support of environmental risk reduction Reduction of pet dander completed Y/N ______
3) In support of better access to care Help with getting prescription medicines completed Y/N ______ *