Embed Size (px)
Citation preview
Tragedy to Transformation
Patient and Family Advocacy and
Carolinas HealthCare System HEN
Julia Lanham
Michael Ruhlen
Linking Patient and Family Engagement
(PFE) to Outcomes • Completed Deep Dive with each hospital on PFE criteria
• Evaluated hospitals based on PFE criteria
– Identify PFE “high performers” – 3+ score on PFE criteria
– 7 PFE high performing hospitals; 22 hospitals other cohort
• Reestablished HEN baselines for each measure
– Aggregate of hospitals in each cohort – High performers cohort
and other cohort baselines
• Aggregated HEN performance results for both cohorts
• Evaluated two questions for each measure:
– Which cohort performed at a lower rate?
– Which cohort achieved a greater reduction?
2
2013: Our Pivotal Year for PFE
• Late 2012 – creation of Chief Patient Experience Officer
• Patient and Family Advisory Councils established in
many hospitals
• System Patient Experience Steering Committee - June
2013
• Leadership Development Institute (LDI) for System focus
on patient experience – August 2013
• System agreement to incorporate patient experience
scores as corporate goal in 2014 – August 2013
• HEN PFE rounding pilot launched
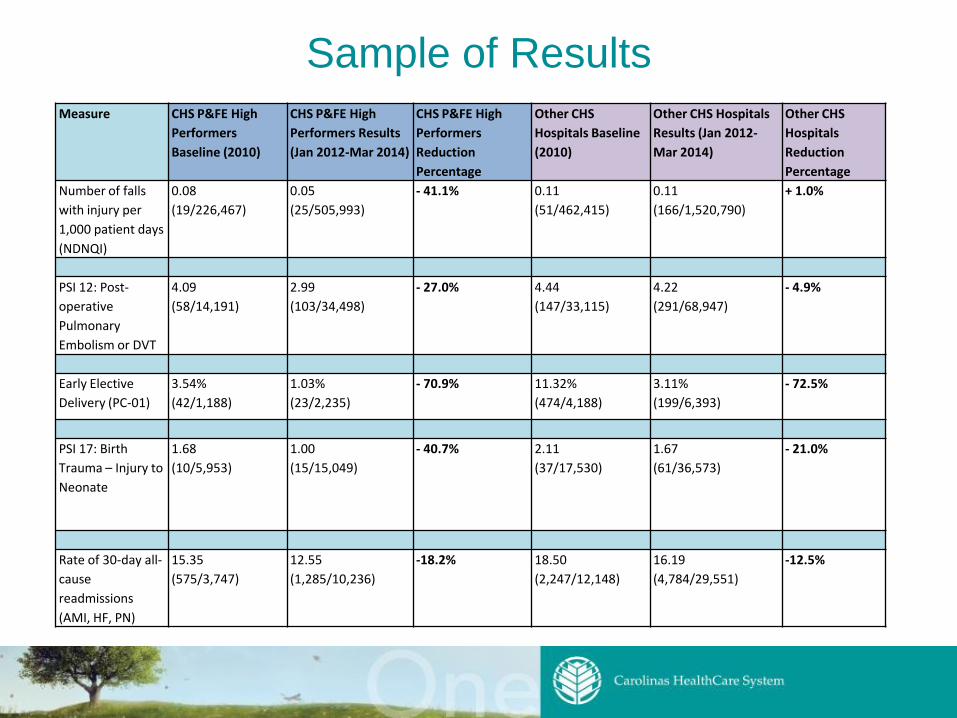
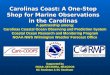
Sample of Results
Measure CHS P&FE High
Performers
Baseline (2010)
CHS P&FE High
Performers Results
(Jan 2012-Mar 2014)
CHS P&FE High
Performers
Reduction
Percentage
Other CHS
Hospitals Baseline
(2010)
Other CHS Hospitals
Results (Jan 2012-
Mar 2014)
Other CHS
Hospitals
Reduction
Percentage
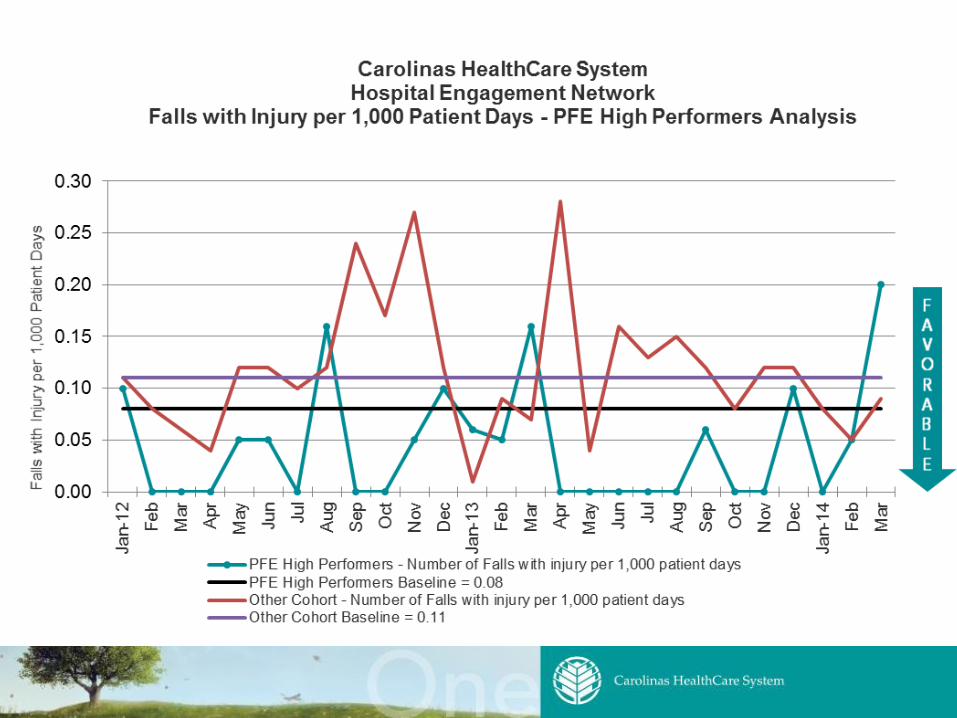
Number of falls
with injury per
1,000 patient days
(NDNQI)
0.08
(19/226,467)
0.05
(25/505,993)
- 41.1% 0.11
(51/462,415)
0.11
(166/1,520,790)
+ 1.0%
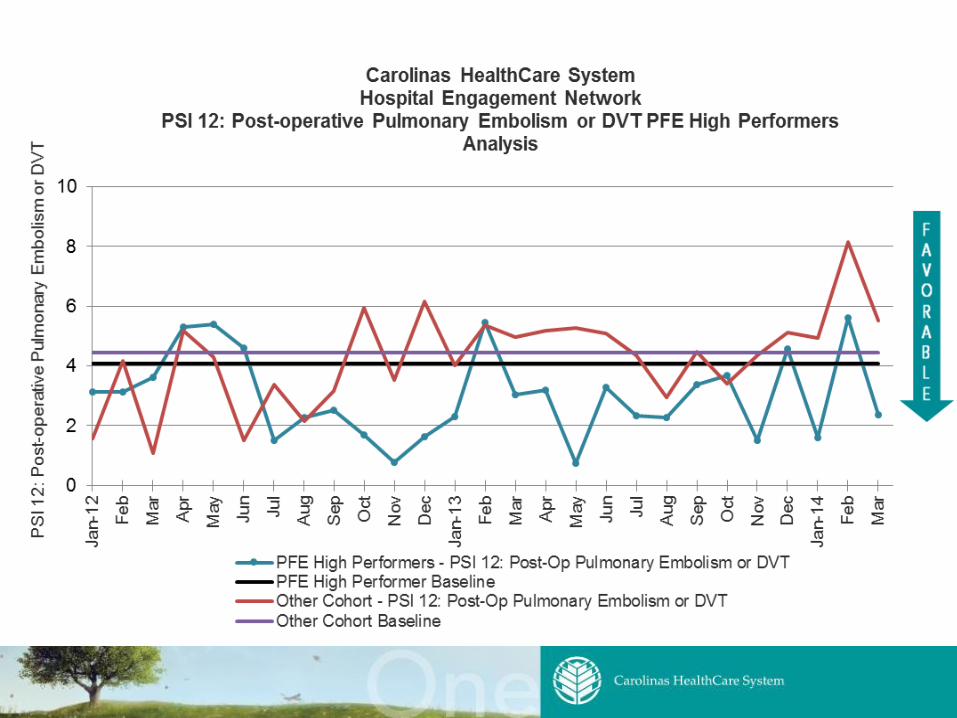
PSI 12: Post-
operative
Pulmonary
Embolism or DVT
4.09
(58/14,191)
2.99
(103/34,498)
- 27.0% 4.44
(147/33,115)
4.22
(291/68,947)
- 4.9%
Early Elective
Delivery (PC-01)
3.54%
(42/1,188)
1.03%
(23/2,235)
- 70.9% 11.32%
(474/4,188)
3.11%
(199/6,393)
- 72.5%
PSI 17: Birth
Trauma – Injury to
Neonate
1.68
(10/5,953)
1.00
(15/15,049)
- 40.7% 2.11
(37/17,530)
1.67
(61/36,573)
- 21.0%
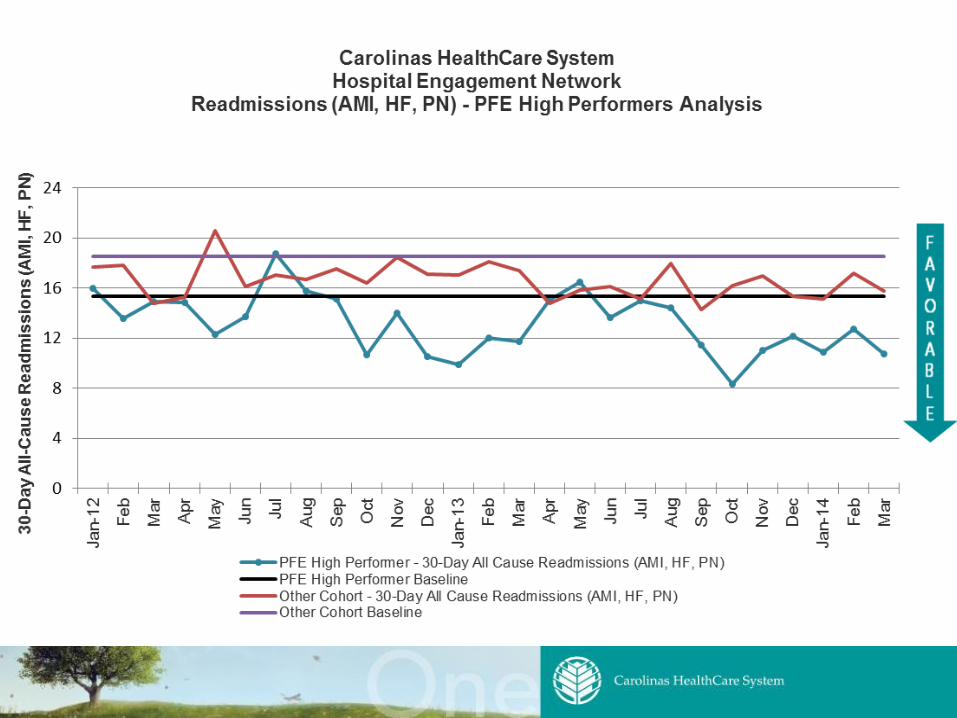
Rate of 30-day all-
cause
readmissions
(AMI, HF, PN)
15.35
(575/3,747)
12.55
(1,285/10,236)
-18.2% 18.50
(2,247/12,148)
16.19
(4,784/29,551)
-12.5%
5
6
7
Tragedy to Transformation
Julia Lanham
Patient and Family Advocate

9
Andrea’s Story (Julia Lanham)
The future is not a result of choices among alternative paths offered
by the present, but a place that is created--created first in the
mind and will, created next in activity. The future is not some place
we are going to, but one we are creating. The paths are not to be
found, but made, and the activity of making them, changes both the
maker and the destination. John Schaar
Tragedy to Transformation
Michael Ruhlen, MD, MHCM, FAAP
Chief Medical Officer
Carolinas HealthCare System Pineville
Carolinas Medical Center - Pineville
12
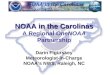
Carolinas Medical Center - Pineville
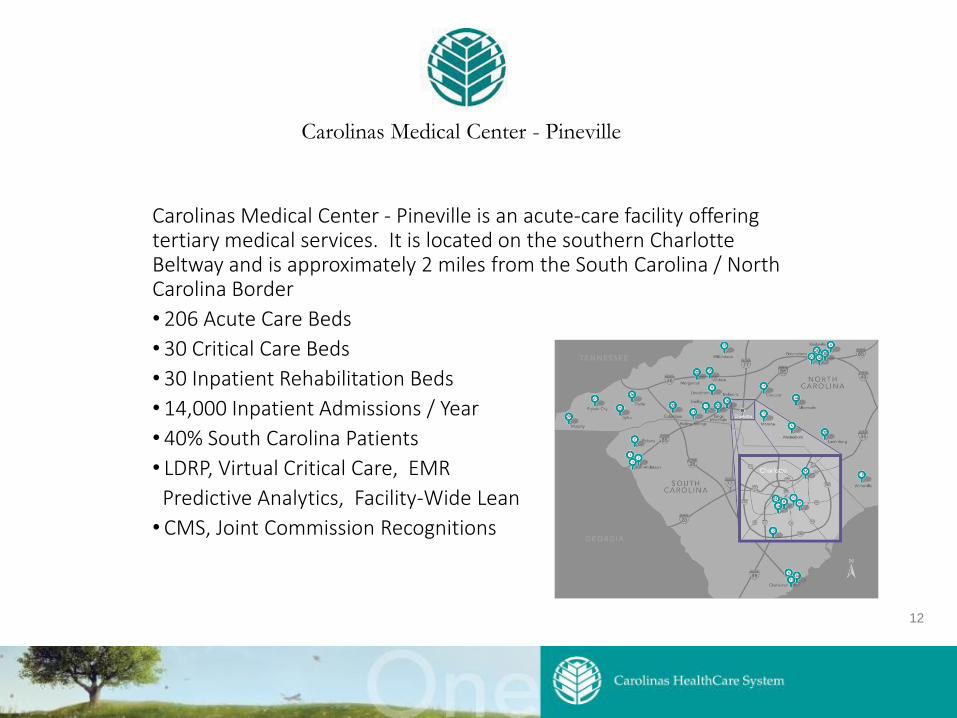
Carolinas Medical Center - Pineville is an acute-care facility offering tertiary medical services. It is located on the southern Charlotte Beltway and is approximately 2 miles from the South Carolina / North Carolina Border
• 206 Acute Care Beds
• 30 Critical Care Beds
• 30 Inpatient Rehabilitation Beds
• 14,000 Inpatient Admissions / Year
• 40% South Carolina Patients
• LDRP, Virtual Critical Care, EMR
Predictive Analytics, Facility-Wide Lean
• CMS, Joint Commission Recognitions
13
Carolinas Medical Center - Pineville
• Commitment to own and understand Andrea’s loss and to change in response
• Meetings with family • Initiated medical staff peer review process and PDSA teams • Reviewed pain management practices facility-wide including
Press-Ganey survey pain results • Identified gaps in medication dosing practices • Initiated pain management steering committee and through this
mechanism, have impacted both inpatient and ED pain care • Implemented a –hospital-wide pain team • Identified care team gaps in knowledge of Sickle Cell Disease and
management
14
Carolinas Medical Center - Pineville
• Commitment to learn • Created and deployed a series of educational interventions on
sickle-cell management including mandatory sessions for physicians
• Care team meetings with Studer Coach • Pain team educational sessions on Complementary and
Alternative medicine techniques
15
Carolinas Medical Center - Pineville
• Commitment to engage • Opportunity to meet with CHS Patient Experience leaders • Presentation at System-Wide Leadership Development Institute • Presentations at system and national HEN meetings
16
Carolinas Medical Center - Pineville
• Commitment to sustain and to spread • System-wide Sickle-Cell Awareness activities • Recruitment of nationally-prominent expert in Sickle-Cell Disease
and her entire clinical team • Training of all metro hospitalist teams so that each will be able to
offer state of the art Sickle-Cell management services in collaboration with the Sickle-Cell Center
• Sickle-Cell Collaborative established • System-wide Sickle Cell Steering Committee • Foundation Fund created to receive contributions • First-time disclosures of such nature outside the system
17
Carolinas HealthCare System
Sickle-Cell Program

18
Vision: The Sickle Cell Program at Carolinas HealthCare System & Levine Cancer Institute (CHS/LCI-Sickle Cell Program) provides consultative specialty comprehensive care to adults with sickle cell disease in a patient-centered and culturally sensitive approach to improve the life of those living with sickle cell disease. We strive to be nationally recognized as a leader in the transformation of healthcare delivery for individuals with SCD and to be chosen for the quality and value of services we provide.
Carolinas HealthCare System
Sickle-Cell Program
YTD SCD Program • Started Clinic 4/24/14
– Total Enrolled in SCD Program 189 YTD
• Staff: Program Manager 1.0; RN 1.0; CSW 1.0; Intern 1.0 (pending hire ACP 1.0; RN 1.0, Psychologist 1.0)
• SCD Clinic: 2 full days /week (case management appts prn daily)
• Instituted ED Care Plans (individualized ED and Inpt Pain management plan) for pts seen in program
• Developing Cerner “SCD VOC Power Plan” or order set for ED for those without an individualized plan
• Nursing Supportive Care Guidelines/Protocol in development for SCD Inpatient
– Working on details with nursing, dedicated SNL for CHG approved
• Inpatient support for CHG/Staff Med (work in progress)
• Established General idea of Tier based system for SCD consults (1-3)
– Fleshing out the details with NMH/CHG and Staff Med
19
Patient
Name 1st clinic date
Avg ED visits
pre clinic/mo.
Avg ED visits
post clinic/mo.
% Change
in ED
visits
Total clinic
visits
Avg clinic
visits/mo.
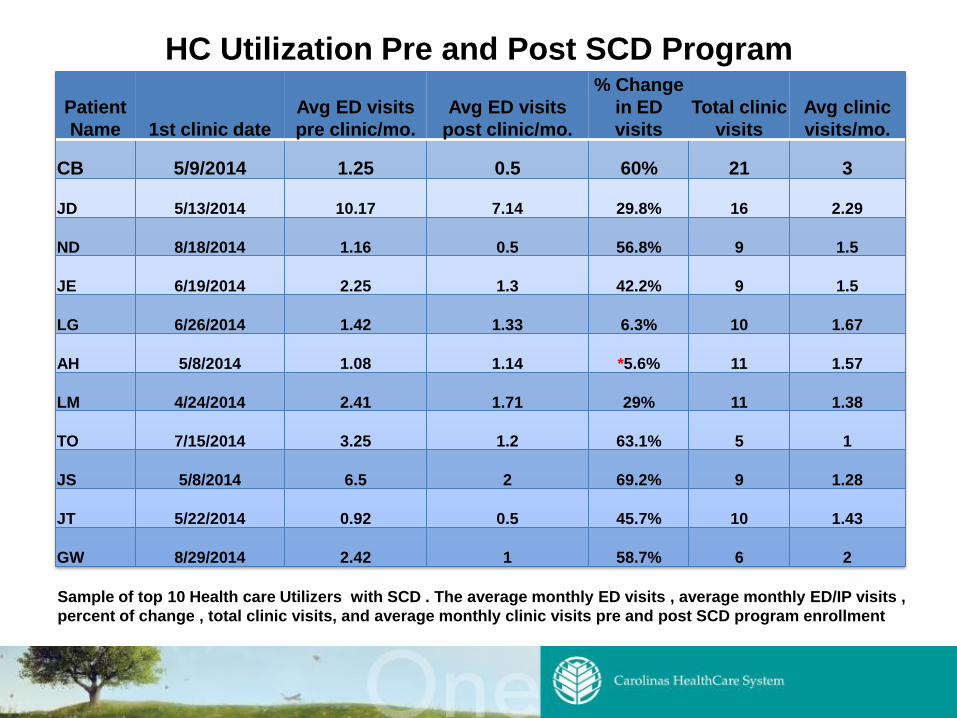
CB 5/9/2014 1.25 0.5 60% 21 3
JD 5/13/2014 10.17 7.14 29.8% 16 2.29
ND 8/18/2014 1.16 0.5 56.8% 9 1.5
JE 6/19/2014 2.25 1.3 42.2% 9 1.5
LG 6/26/2014 1.42 1.33 6.3% 10 1.67
AH 5/8/2014 1.08 1.14 *5.6% 11 1.57
LM 4/24/2014 2.41 1.71 29% 11 1.38
TO 7/15/2014 3.25 1.2 63.1% 5 1
JS 5/8/2014 6.5 2 69.2% 9 1.28
JT 5/22/2014 0.92 0.5 45.7% 10 1.43
GW 8/29/2014 2.42 1 58.7% 6 2
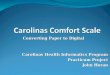
HC Utilization Pre and Post SCD Program
Sample of top 10 Health care Utilizers with SCD . The average monthly ED visits , average monthly ED/IP visits ,
percent of change , total clinic visits, and average monthly clinic visits pre and post SCD program enrollment