Pathways to Work: Progress in Government initiatives
24
CORPORATE MEDICAL GROUP Website: www.dwp.gov.uk/medical Pathways to Work: Progress in Government initiatives Dr Philip Sawney AOHNP(UK) Symposium 13 May 2004
Pathways to Work: Progress in Government initiatives
Pathways to Work: Progress in Government initiatives. Dr Philip Sawney AOHNP(UK) Symposium 13 May 2004. Department for Work and Pensions. Created 2001 [from former DSS and part DfEE ] Corporate centre and agencies Jobcentre Plus Pensions Service Disability and Carers Service - PowerPoint PPT Presentation
Citation preview
Default slide showCreated 2001 [from former DSS and part DfEE
]
Corporate centre and agencies
120,000 staff
CORPORATE MEDICAL GROUP
10 Public Service Agreement targets
Working with others:
Health Depts [England,Scotland,Wales]
People of working age
Objective: to promote work as the best form of welfare whilst
protecting the position of those in greatest need
Delivery Targets (PSA):
Increase overall employment rate over economic cycle
Increase the employment rate of people with disabilities, taking
account of the economic cycle, and significantly reduce the
difference between their employment rate and the overall
rate.
Work to improve the rights of disabled people and to remove
barriers to their participation in society’
CORPORATE MEDICAL GROUP
Helps employers fill their vacancies
Front office services for others eg DCS
Implements labour market policies
Disability Employment Strategy
Focus on what people can still do - with support to work
Systems support/encourage activity rather than inactivity
Interventions at earlier stage
Agencies working together
Healthcare systems treat work outcomes as a key element of clinical
management
Employer engagement
CORPORATE MEDICAL GROUP
Why do we need this strategy ?
2.7 million people of working age on a state incapacity benefit
[< 1 million unemployed]
1 million report sick each week; 3000 remain off work at 6 months
and 80% of these will not work again in next 5 years
20% of people of working age have a long term disability
50% of the disabled population in the UK are economically inactive
(versus 15% of the non-disabled)
CORPORATE MEDICAL GROUP
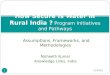
Reasons for this growth are complex:
Economic cycle – one way ratchet detaching people from the labour
market during economic downturn but not able to return when economy
picked up - particuarly so in certain parts of the country
Working age recipients of Invalidity and Incapacity Benefits,
including NI Credits Only, 1979-2001
0
500
1,000
1,500
2,000
2,500
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Year
Thousands
Incapacity Benefit Claims Source: 1% sample of all IB
claimants
62370000
91176000
79670000
115897000
105849000
158412000
131536000
198282000
192752000
225435000
229931000
219863000
235932000
198191000
]]]]]]]]]Sheet1
thousands
Notes: Figures have been rounded to the nearest thousand
]]]]]]]]]Sheet1
0
0
0
0
0
0
0
0
0
0
0
0
0
0
CORPORATE MEDICAL GROUP
CORPORATE MEDICAL GROUP
Health
Social
Economic
There is a three-fold rationale for government action to increase
employment of disabled people.
economic : disabled people make up a significant proportion of the
working age population, and a failure to deploy this resource
effectively will impact on economic growth
social rationale: that disabled people have a right to participate
as fully as possible in society, which includes participation in
the world of work - there is abundant evidence that this does not,
and will not happen without government intervention.
health outcomes: in general people in work have better health
experiences and outcomes than those not in work; work can be seen
as a key route to reducing health inequalities
CORPORATE MEDICAL GROUP
Return to work should be a positive & realistic option
Satisfying Personal Capability Assessment (PCA) does not
necessarily mean “incapable of any sort of work”
Almost everyone moving onto Incapacity Benefit says they want to
work again
Most have more manageable conditions where outlook should be
positive
For most people return to full activity (incl. work) will improve
health and well-being
People on IB have aspiration and potential
870,000 recipients tell us they want to work
160,000 recipients already move into work each year
Barriers to work faced by this group combine health and non-health
factors - over 40% do not mention health as a barrier. For masny
others health need not be a fundamental barrier; for others till it
is about a conombination of factors including - barriers such as
job availability, confidence and skills, financial considerations,
discrimination
despite positive outlook of more than 90% of those flowing onto IB
over 40% will still be on benefit at 12 months and most of these
will be on for much longer
Even after only 6 months on benefit there is a 50% chance that they
will still be there at 5 years – after a year on benefit there is
more chance of the person dying or retiring than of leaving IB for
a job.
specifically mention proportions of IB caseload who are not better
off in work
CORPORATE MEDICAL GROUP
worklessness as a major risk to health
For the majority being away from work has a significant adverse
effect on health through:
isolation, social exclusion and stigma
changing health related behaviour
disruption to future career
CORPORATE MEDICAL GROUP
Skills and qualifications
……steps to activation are undermined
Activation (Intervention and support) : the vast majority of
out-of-work people with a medical condition or disability are
economically inactive, and by definition need to become
economically active as a precursor to entering work. A crucial
problem is the widespread assumption that disability equals
unemployability and that receipt of IB means that the person is
either unable, or not allowed to work.Support for return to work:
once activated, many clients need ongoing support, including advice
on/ access to available services. They need the support system to
be easy to understand, with a spectrum of help options related to
their needs.Rights and responsibilities: there is genuine concern
about the extent to which disabled people should be expected to
seek work or participate in work-related activities and issues
around the extent to which government and society should be
expected to support them.Skills and qualifications: lower average
levels of qualifications of disabled people are undoubtedly a
factor in their lower employment rates, but we need to beware of
over-simplification because there are a number of factors
underlying this.Medical: academic opinion is strongly in favour of
work as a positive benefit to health in the majority of cases. This
opinion does not yet appear to be shared by many front-line health
professionals (or at least is not reflected in their behaviour);
Jobcentre Plus advisers are not currently equipped to challenge
clients’ views that work would be bad for their health, nor are
most employers likely to challenge such advice.Financial
incentives: for too many people the potential financial gain of
returning to work is small, and in some cases negative. There is a
need to ensure that as many as possible stand to gain from a return
to work; and that the gain is sufficient to motivate them.Support
in work: Many clients will need ongoing support to enable them to
remain in work; this is not simply a retention issue, as the
assurance of the availability of such support will be for many a
necessary precursor to active job search.Employers: attitudes of
employers to the recruitment and retention of disabled people are
clearly crucial; as too is their awareness of legal requirements
and support such as Access to Work.Uncertainty: individuals have
understandable fears about their ability to cope with the demands
of work, their treatment by employers and fellow employees, the
financial implications of a transition to work or of a subsequent
return to benefits; the continuity of support they were receiving
previously. Reducing these perceived risks and uncertainties will
encourage risk-averse individuals to seek a return to work
CORPORATE MEDICAL GROUP
Vocational Rehabilitation: The Way Forward - BSRM, 2nd Ed Dec
2003;
Second UK Bodily Injury Awards Study - Oct 2000
CBI report ‘Business and healthcare for 21st century - Dec
2001
ABI/TUC paper ‘Getting back to work’ June 2002
Employment Opportunities and Psychiatric Disability – RCPsych
2003
CORPORATE MEDICAL GROUP
Key principles:
Better specialist support, esp. health-work aspects
Making sure work clearly pays
Better support for people on JSA with health problems
Jobcentre Plus working in partnership- NHS and employers also
key
Spending Review 2002 - got nearly £100m to pilot the proposals.
Looking to pilot in 7 areas (50-60,000) new claimants a year. 3
pilot areas from around October 2003, 4 from April 2004
Opening up the employment services side of Jobcentre plus to wider
group than the ‘unemployed’ / JSA claimants
Make those services an integral part of claiming a state incapacity
benefit - once claim established clients will discuss their work
goals and return to work plans.
Services delivered by a team of specialist personal advisers
Initial WFI at 8 weeks
Speeding up PCA process (identify exemptions early and make PCA
decision by wk 12)
Capability report - residual capabilities and possible work
adjustments
Repeat WFIs and Work Action Plan
Access to choices package:
Adviser discretionary fund
CORPORATE MEDICAL GROUP
Limitations of traditional health care
Models of disability
Addressing the real obstacles
Developing the evidence base
Traditional health care - symptomatic relief /sufficient recovery
to allow a return to work - increasing evidence base to support
such health-focused interventions.
modern concepts of vocational rehabilitation recognise that there
may be additional obstacles to recovery that are simply not
addressed by medical treatment
Addressing these obstacles is likely to require innovative and
multi-dimensional interventions aimed at restoring function and
self esteem.
There is considerable evidence to justify pursuing this approach to
rehabilitation there is much less evidence about the precise
details of effective interventions.
Studies to date have not produced statistically robust or
generalisable evaluation results.
CORPORATE MEDICAL GROUP
AXIS
ELEMENT
Psycho-
Social
Employer strategy Return to work credit Involving other
stakeholders
CORPORATE MEDICAL GROUP
DWP/Jobcentre Plus cannot provide the whole solution
Other stakeholders to focus on agenda that encourages those with
health problems/disabilities to remain in, or return to, work
CORPORATE MEDICAL GROUP
working with key stakeholders especially NHS (Condition Management
Programmes)
7 pilot areas:
April 04 -Somerset; Essex; E.Lancs; Gateshead
Full evaluation 2003 - 2006
Outcomes:
Help more IB clients back to work as quickly as possible (avoid
drift onto long term IB)
Contribute to reducing child poverty and social exclusion
Find out what works in helping people with an illness or disability
get back to work
CORPORATE MEDICAL GROUP
Job Retention and Rehabilitation Pilots (RCT)
Health Inequalities / Social Exclusion Unit
Securing Health Together
CORPORATE MEDICAL GROUP
Disability and work a mainstream issue
Dynamic nature of conditions
Recognise influence of psychological and social factors
CORPORATE MEDICAL GROUP
including NI Credits Only, 1979-2001
0
500
1,000
1,500
2,000
2,500
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Year
Thousands
Diseases of the
-