Embed Size (px)
Citation preview

_____________
CHAPTER 26 -------~------------
PATHOPHYSIOLOGY OF CLINICAL DISORDERS OF URINE CONCENTRATION AND DILUTION
MANUJ£L MARTINEZ-MALDONADO AND SUSAN OPAVA-STITZER
INTRODUCTION
A
Clinical Diagnosis of Disorders in Concentration and Dilution
DEFECT IN THE ABILITY to concentrate or dilute the urine can be easily rec
ognized by the maximum or minimum urine concentration the patient is able to achieve. Maximum concentrating ability (Umax) is determined by the urine osmolality reached after a fixed period of dehydration and maximal diluting ability (Umin) by the minimum osmolality of the urine after the oral inges tion of a fixed water-load. These indices, however, do not allow an understanding of the pathophysiological alterations leading to the presence of the defect.
Inability to maximally concentrate the urine can be attributed to one or both of two basic tubular defects: first, a failure of maximal free-water generation by the diluting segment in the ascending limb of Henle's loop and second, a failure of the distal tubular epithelium to achieve maximum permeability to water during water deprivation. These changes singly or combined are capable of reducing maximum concentrating ability. The first brings about the reduction in Umax by diminishing the cortico-papillary solute gradient and thus reducing the gradient for freewater reabsorption from collecting duct lumen to interstitium. The second re
duces Umax by preventing osmotic equilibration of collecting duct Huid with the medullary interstitium (1-3).
Inability to produce a maximally dilute urine may likewise be attributed to one or both of two basic tubular defects: first, the failure of maximal free-water generation by the diluting segment, and second, an inappropriately high permeability to water of the distal tubular epithelium during water diuresis. The former, while reducing maximal concentrating ability, also diminishes maximal diluting' ability by resulting in a less than normal dilution of tubular fluid. The second results in the inappropriate reabsorption of water from the collecting duct in response to the interstitial solute gradient generated by solute reabsorption in the ascending limb.
It is readily apparent that a failure of the ascending limb and other diluting segments to generate normal amounts of free water can result, at low tubular flow rates, in a diminution of both maximal concen· trating and maximal diluting ability. Nevertheless, a comparison of Umax and Umin may be utilized to distinguish between a permeability defect and a defect in free-water generation. If both concentrating and diluting ability are reduced, a defect in free-water generation is suggested. Such a defect must involve the active solute reabsorption process in the medullary por
992

993 PathojJh)'siolofo,'Y of Clinical Disorders of Urine
tion of the ascending limb of Henle's loop, since involvement of cortical segments alone would affect only diluting ability. In addition, it could represent a reduction in the relative water impermeabili ty of the ascending limb which is essential for freewater generation. If concentrating ability alone is reduced, a defect in appropriate free-wa ter reabsorption in the collecting duct is suggested. On the other hand, if diluting ability is compromised in the presence' of a normal Umax, either abnormal sodium reabsorption in the cortical diluting segment or inappropriately high H 20 permeability in the collecting duct is indica teel. These two defects can be distinguished from each other by the effect on sodium excretion (Table 26-1) .
nature in the distal convolution or collecting duct would be expected to alter only diluting ability, as illustrated in Table 26-I.
The assessment of maximal concentrating and diluting ability by measurement of the urine osmolality alone may be subject to misinterpretation. Tubular defects other than those already mentioned, or conditions which alter solute delivery to the si tes of free-water generation, can also alter the maximum urine concentration achieved during dehydration or the minimum urine concentration attained during water diuresis. Thus, a more precise index of urine concentration and dilution is needed. Such all index is provided by the measurement of free-water reabsorption
Table 26-1� Clinical Use of Ulilin and Umax for Characterization of Defects in COllcelllration and Dilution�
Umas
1.� Normal 2.� Ascend; I1g lim b defect
in NaCI transport 3.� Cortical diluting ~egment
defect in NaCI transport 4.� Collecting duct defect
in NaCl transport 5.� Loss of ascending limb
impermcability to water 6.� Loss of collecting duct
water permeability in response to ADH
7.� Ehanced collecting Cltlct water permeability (in wa tel' diuresis)
In addition, a comparison of concentrating and diluting ability can yield information on the particular nephron segment in which a defect in free-water generation lies. A defect in free-water generation in the ascending limb of Henle's loop would be expected to alter both concentrating and diluting ability, while a defect of the same
N .j.
N
N
.j.
.j.
N
Ulllin
N
t
t
t
t
N
t
Fmclio?/aZ�
UNaV�
<1% >2%
>2%
<2%
<1%
<1%
<1%
(TOH20) and free-water generation (OH20) over a range of distal solute delivery (Figure 26-1). During measurement of TOH20, circulating levels of antidiuretic hormone must be maximal. To insure this, hypertonic solutions are administered at increasing rates, allowing the calculation of free-water reabsorption from the equation:

994 Pathophysiology of the Kidney
GENERAL FEATURES OF FREE WATER REABSORPTION AND FREE WAfER CLEARANCE
Casm
-V CH20 + eN.
CH20 + CCI
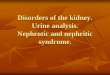
Figure 26-1. Idealized curves for free water reabsorption and free water clearance. In the case of free water clearance, the similarity of the relationship regardless of the delivery form will only be the case eluring hypotonic NaGI infusion.
TCBoO =cosm - V where V = urine n;w in ml/min
UosmV cosm=the osmolar clearance =: -----coc--
PoSill
Uosm =: the urine osmolality Posm = the plasma osmolality.
In this way the capacity to reabsorb free water under conditions of maximal water permeability can be studied at varying rates of solute delivery to the sites of solute reabsorption. A normal relationship between TCH20 and osmolar clearance can thus be established (Figure 26-la) and deviations
from this normal curve can be identified. This method is invaluable for determining defects in concentrating ability in situations where solute delivery to the distal nephron may also be altered. In addition, subtle defects in the concen tra ting mechanism, which may not be readily apparent at the low rates of solute excretion which prevail during the measurement of Umax, may be revealed at higher rates of solute excretion. As will be discussed, however, even this measure of urine concentration fails to distinguish the nature of the defect.
In a similar manner, free-water generation or clearance (CH20) can be expressed as a function of solute delivery to the diluting segmen ts of the nephron. In this case, varying amounts of solute are administered as hypotonic solution in order to suppress endogenous ADH release so that a condition of minimal water permeability of the distal nephron prevails. Freewater clearance is calculated from the eguation, cH20 = V - cosmo The correct index of solute delivery in this circumstance has been hotly debated. It is generally agreed that cosm is not an accurate reflection of distal solute delivery during infusion oE hypotonic solution. More acceptable indices are V, cH20 + eNa, and cH20 + eCl (49). The relative merits of these three are currently under scrutiny. In any case, a normal relationship between cH20 and one of these indices can be established, as shown in Figure 26-2b, and deviations from the normal curve can be identified. A more precise measure of diluting ability is thus obtained, since variations in solute de· livery are accounted for, and defects not apparent at low osmolar clearances may be unmasked. Even this measure of diluting ability, however, fails to characterize the defect, and, as in the case of maximal and minimal urine concentrations, more information can be gleaned from a compari

• Pathophysiology of Clinical Disorders of Urine 995
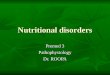
RELATIONSHIP BETWEEN T'H20 AND COSM DURING MANNITOL AND the TCH2 0 curve alone. A greater than HYPERTONIC SALINE DIURESIS
normal water permeability during water A. Mannitol diuresis would allect only the 01-1 20 curve.
In the event that a defect in free-water generation is indicated by an effect on both curves, the defect can be localized in the ascending limb of the loop of Henle. A defect in free-water generation which docs
COSM- not reside in the loop but in the distal convolution would be expected to alter only the cH2 0 curve. As in the case of alteration in Umin alone, this can be distinguished from a higher than normal water permeability during water diuresis by the effect on sodium excretion.
The tubular defects listed in Tables 26COSM I and 26-II, which result in alterations in
Umax, Umin, TCH2 0 and cH20, may ocFigure 26-2. Idealized curves (with approxicur alone or in combination as will be apmate ranges) for free water reabsorption. parent in the following discussion. These may be intrinsic defects or may result from
son of TCH20 and cH20 curves as sum a variety of factors including drug therapy marized in Table 26-II. A defect in free and various types of renal disease. water generation might be expressed in an Even in the absence of the tubular dealteration of both curves, but a less than fects described above, reductions in the maximal water permeability of the collect ability to concentrate or dilute the urine ing duct during antidiuresis would aIlect may occur. Such could be the case if de-
Table 26-II Use of T"H20 and cH20 in the Characterization of Clinical Disorders of
Urine Concentration and Dilu tion
TOH2 O OH2O FENa
1. Normal N N <J% 2. Ascending limb defect ,J. ,J. >2%
in NaCl transport 3. Cortical diluting segment N ,J. >2%
defect in NaCl transport 4. Collecting duct defect N ,J. <2%
in NaC! transport 5. Loss of ascending limb ,J. ,J. <1%
im permeability to water 6. Loss of collecting eluct ,J. N <1%
water permeability in Tesponse to ADI-!
7. Enhanced collecting' cluct N <1% water permeability (in water diuresis)

996
-�Pathophysiology of the Kidney
livery of solute to the distal nephron were decreased or medullary blood 110w significantly increased over normal. The former situation deprives the diluting segments of the substrate for free-water generation and thus reduces the ability to both concentrate and dilute the urine (Umax and Umin). TCHzO ancl cHzO curves, however, would be perfectly normal, since these are obtained over a range of solute deliveries. Increased medullary blood How, on the other hand, will result in washout of the corticomedullary gradien t, thus reducing concentrating ability alone. This defect would influence both Umax and the normal TCHzO curve, I t should be noted here that small decreases in medullary blood flow, which do not limit cellular metabolism, should actually enhance concentrating ability since interstitial osmolality will rise.
PATHOPHYSIOLOGICAL� MECHANISM�
Abnormal NaCl Transport By the Loop of Henle
Despite in vitro evidence indicating that the thin ascending limb of the loop of Henle does not carry out active sodium chloride transport (10-11), these structures when presen t, * particularly in nephrons dipping into the inner medulla, are important [or the excretion of a maximally concentrated urine (14-18). The main function of thin limbs, however, appears to arise from the permeabili ty characteristics o[ their walls to sodium, urea, and wa tel', combinecl with urea trapping in the interstitium of the inner medulla. Urea and
"As shown by the comparative sLUdies of Tisher and his collaborators (12-13), thin loops may be absen t and yet concentrated urine will be excreted. On the other hand, ablation of long' thin loops when present abolishes the elaboration of maximally concentrated urine.
sodium chloride will largely determine the steepness of the corticornedull ary concentration gradient, insuring maximal water abstraction from fluid traversing the collecting duct:. The major determinant of the metlullary accumulation of urea, in addition to adequate dietary protein illtake, appears to be the transfer of energy from the thick ascending limb, to the inner medulla in its process of active sodium chloride transport:. It is clear, therefore, that the "single effect" is responsible not only for a sodium chloride corticomedullary gradient but will also influence the urea gradient (16,18). In situations wherein collecting duct permeabili ty is normal, in the presence or absence of ADH, and medullary blood flow rate is unchanged from the control state, the integrity of the NaCl reabsorptive mechanism in the thick portion of the loop will determine the excretion of a maximally concentrated urine (Umax). Furthermore, during infusion of hypertonic saline, the reabsorption of solute-free water (TOH 20) as solute excretion rises will also depend on the intactness of the NaCl reabsorptive process in the thick limb* (19). Similarly, the capacity to excrete a maximally dilute urine, in the absence of ADH, will be significantly curtailed. IE NaCl reabsorption in the loop were impaired, the presence of both a concentrating and diluting defect would occur iF the thick limb were involved throughout its length or in its outer medullary region. If the involvement were confined to its cortical portion, only dilu ting capacity would be impaired. This is the case because very little free-water reabsorption takes place in the cortex even in the pres
*Often, during hypertonic saline infusion, TOI-IoO will plateau or actually fall as osmolar clearal~ce mounts. This is due to the failure of the large volumes of hypotonic urine which enter the collecting duct to achieve equilibrium with the interstitium (20).

997 Pathophysiology of Clinical DisOl'de1"S of Urine
encc of ADH. The nature of the reabsorptive process
in the thick limb is largely unknown. Although in ,JilTO studies of these structures appear to indicate that chloride is the major actively transported ion species (10, 2] ,22), the cellular and molecular details of this event are obscure at best. It is possible that a Na+-K+-stimulated membrane adenosine triphosphatase (Na+-I<'-ATPase) is involved (23-25), but its relationship to the movement of chloride has not been examined closely and remains to be elucidated.
In the clinical context it is c1ifficuJ t to assess whether pure defects in urine concentration or dilution exist which are clue ta diminution in sodium transport by the thick ascending limb wi thout alterations in collecting duct permeability or intrarenal hemodynamics. Nevertheless, in this part of our discussion we shall focus on disturbances far which there is both clinical and experimental evidence that a transport defect may be involved in its genesis.
Hypercalcemia Inability to concentrate the urine and
to maximally reabsorb solute-free water during hypertonic saline infusion or to maximally generate free water during water diuresis has been observed clinically and experimentally in hypercalcemic subjects (26-29). Experimentally, the defect may be reproduced by the administration of calcium, ergocalciferol, or parathyroid extract (27-29). Clinically, hypercalcemia secondary to hyperparathyroidism, hyperthyroidism, Addison's disease, vitamin D intoxication, sarcoidosis, and milk alkali syndrome has been observed to lead to reduced Umax and abnormal TCH20 and cH20 curves (30).
There is evidence, to be discussed later, that the impaired ability to concentrate or
dilute the urine observed in hypercalcemia may result from alterations in collecting duct permeability to water or changes in renal hemodynamics. EvicJence also exists suggesting that sodium reabsorption per se is impaired. The content of sodium in the medullary interstitium of rats and dogs made hypercalcemic by vi tamin D or calcium loads is markedly diminished (31-33). Although possibly the resul t of climinishetl GFR with reduced sodium delivery to the loop of Henle, the observation that absolute and fractional sodium excretion is greatly increased during brief periods of hypercalcemia suggests a direct inhibitory effect of calcium on the renal tubular epithelium (29). Also, acute hypercalcemia in the dog, in contrast to prolonged hypercalcemia, reduces free-water clearance at any level of distal delivery when compared to normal animals (29). Failure to observe this change ill animals with chronic elevation of serum calcium may be the result of reduction in nephron mass with severe decreases in GFR. Of note is the fact that changes in GFR induced by reduction in aortic blood flow to levels observed in acute hypercalcemia do not lead to reductions in cH20 of the same magnitude, suggesting that the elevated calcium per se may impair sodium reabsorption (29). Studies in the rabbit seem to strengthen the suggestion of a direct effect of hypercalcemia on renal tubular sodium reabsorption. In this species the differences between hypertonic saline and mannitol TCH20 curves are abolished, indicating diminished sodium reabsorption by the loop despite adequate distal delivery (Figure 26-2) (34). Studies in renal and other epithelia have provided some evidence for an inhibitory eHeet of calcium on sodium transport. In frog skin, calcium reduces the permeability of the epithelium to sodium (35) while it does not alter vasopressin-induced sodium trans

998 Pathophysiology of the Kidney
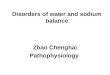
port in toad bladder (36). :rvIicropuncture experiments in the rat have also indicated that acute hypercalcemia or the presence of high calcium in the filtrate is associated with a pronounced reduction in tubular fluid reabsorption, indicating reduced sodium transport (37-39). The interference with transepithelial sodium transport may be the result of a number of cellular changes. Calcium has been shown to reduce Na+-K:-ATPase activity ('10) which, particularly in the ascending limb (25), seems to playa central role in transcellular sodium transport. This would result in cHminished extrusion of sodium entering the cell from luminal !tuid, which would eventually lead to reduced sodium movemen t from lumen to cell interior. On the other hand, calcium may directly inhibit the active transport of chloride at the luminal membrane, thus reducing both Na+ and Cl- reabsorption. The inhibition of NaCI reabsorption may also be the result of uncoupling of medullary mitochondria resulting in reduced high energy phosphate supply to either Na+ or CI- pumps. Lastly, the apical or basal permeabilities to chloride or sodium may be altered resulting in diminished entry of Na+ or diminished exit of Cl'- from the cell. Singly or combined, the above possibilities would result in decreased net NaCI transport (Figure 26-3).
It is of interest that the renal concentrating defect produced by clinical or experimental hypercalcemia may be reversible in periods ranging from hours to days (29,30,41). This finding strongly suggests that the changes observed, as described above, are predominantly functional or biochemical, in contrast to morphological. This is not to say that in chronic forms of hypercalcemia, even as early as twenty-four to forty-eight hours, morphological changes are not important. In fact, observations of
ASCENDING LIMB CELL
LUMEN PERITUBULAR SPACE
No' -+ (I)
--------- - ...
Fig'ure 26-3. Schematic representation of ascending limb (thick portion) cell showing possible changes which may be reduced NaCl reabsorption. (1) Inhibition of Na+K+ATPase; (2) Inhibition of luminal active Cl-pump; (3) Inhibition of metabolism (oxidative phosphorlylation or glycolysis); and (4) Changes in ion permeability of either luminal or periluminal cell membrane.
the cellular alterations, which eventually take place, may provide indirect evidence that calcium concentration is high at the sites of the proposed functional derangements. For example, the concentration oE calcium is normally greater in the medulla than in the cortex, and medullary changes tend to occur earlier and to be more severe in hypercalcemia (30). Focal lesions in the loop of Henle and distal tubules including calcification of cell cytoplasm, basement membrane, and mitochondria have also been observed (42).
Although far from settled, hypercalcemia may affect renal concentrating and diluting ability by reducing net reabsorption of Nael from lumen to interstitium. In the intact kidney the evidence is inconclusive, but information which sheds light on the issue may be forthcoming from the use of isolated perfused tubules.

u
Pathoj)hysiology of Clinical Disorders of Urine 999
Potassium Depletion The mechani~m by which potassium de
pletion leads to a reduced Umax has attracted the interest of a number of investigators, yet it still remains unclear (t1353). A principal problem is that there may be some significant species differences; in many instances, clearance studies have provided different results depending upon the experimental animal. A Umax defect ha~
been described in man (43,4'1). In the dog', demonstration of a defect in the generation of TCH20 or cH20 has been inconsistent (51,52) , while a serious disturbance of both has almost always been uncovered in the hamster, the rat, and the rabbit ('15·'J7,4951). It is apparently clear that in rodents the effect of potassium deficiency on renal function is different from that in carnivores. The role played by reduced filtered load to the diluting site is not clear. Although this may well be the cause of the concentrating defect under some circumstances, most investigators have almost alway~ observed a disorder of TCH20 in potassium deficiency de~pite a normal GFR An exception to this may be found in studies in the dog by Bennett (52). This investigator, however, utilized mannitol infusion~ which, per se, may impose a limit on the generation of TCH20 as a function of Cosmo In fact, all curves depicting this relationship in his study are flat and, therefore, difficul t to in terpre t. Despi te the possibility that part of the defect in urine concentration and dilution observed in hypokalemic animals may be the result of enhanced proximal tubular reabsorption secondary to diminished GFR, it is ob· viously not the entire explanation.
An important aspect of the defect in urine concentration seen in hypokalemia is that sodium content of the renal medulla has been shown to be diminished in some
species such as the rat (45,50). Studies by Eknoyan and his collaborators in this species (50) have demonstrated a defect in loop transport manifested by alterations in both TCH20 and cH 20, which, if present in other species, could explain the reduction in tissue sodium concentration. Hypokalemia is known to lead to disorders of ion transport in other cell systems so that reduced NaCl reabsorption in the distal tubule, if not likely, is entirely possible. Evidence also exists to indicate that hypokalemia leads to reduction in the content of enzymes involved in oxidative phosphorylation in the renal medulla of the rat (54). Therefore, the supply of high energy phosphate compounds for the transport process may be defective in hypokalemia.
An alternative to deficiencies in ion transport or solute delivery as causes of the concen trating or diluting defect is the possibility that the anatomical lesions induced by hypokalemia may result in diminished epithelial permeability to water in the distal parts of the nephron. The resultant in tense vacuolization of the cytoplasm of the collecting duct cells could alter the tubular response to the effect of circulating ADH. Evidence has been advanced from potassium-depleted hamsters that despite gross histological lesions in the collecting ducts, osmotic equilibration is achieved across this structure under circumstances in which a defect in urine concentration is demonstrable (47). It does not appear likely, therefore, that altered permeabili ty of the distal nephron ~econclary to the significant anatomical alterations in hypokalemia is responsible for the Umax defect in the rodent. On the other hand, the possibility persists that in both man and dog the presence of prolonged hypokalemia may result in anatomical or biochemical defects which render the collecting duct

1000 PalhojJhysiolog)I of the Kidney
less responsive or refractory to the circulating effects of ADH. Evidence for this has been advanced by the demonstration that patients wi th potassium deficiency, when administered ADH, excrete less cyclic AMP in the urine than normal subjects or patients wi th other disorders of urine concentration, such as sickle cell disease (55).
One other possible mechanism by which hypokalemia could result in reduced Umax could be related to enhancement oE medullary blood flow. Enhanced medullary blood How, by washing out medullary solute, could explain the findings of a reduced tissue sodium and abnormal Dmax and TOH20, as has been shown when a variety of renal vasodilators are infused directly into the renal artery (56-58). It could also explain why, in some species (dog and man) during water diuresis, a defect in cH20 might not be apparent or why Dmin might be normal, since medullary washout is maximal in water diuresis. 1£ diminished solute content were secondary to increased medullary blood flow, however, it could not explain data on medullary metabolism obtained by Kannegiesser and Lee (59) and those of Weiner et aI. (5'1). The demonstration by V\Teiner that medullary mitochondrial enzymes have diminished specific activities and that sodium-potassium-ATPase is normal in hypokalemia would suggest that both TOH20 and 0H20 may be impaired through interference with transport processes. Yet Kannegiesser and Lee have demonstrated that hypokalemic animals (rabbits) have a defect in oxidative phosphorylation which is only manifest in hyperosmotic environments but not under hypoosmotic or isosmotic conditions, as would be the case during water diuresis. Should renal medullary blood How be increased under basal conditions, thus preventing the formation of a hyperosmotic interstitium, it would
tend to limit the defect in TCH20 rather than enhance it. Further studies in this direction are needed, however, before the cellular events occurring in hypokalemia arc clearly elucidated.
Hypertension An increasing body of evidence points
to the possibility that intrarenal physical forces (so-called Starling forces) play an important part in the regulation of sodium reabsorption (60). Nevertheless, it is apparent that increases in peri tubular hydrostatic pressure may lead to diminished tubular reabsorption of NaCI and water. The experimental work generated by the interest in the role of physical factors in the maintenance of salt and water homeostasis has provided a theoretical explanation Eor the observation that hypertensive man excretes a sodium chloride load faster than his normotensive counterpart (61-6"1). The fact that raising systemic blood pressure by occlusion of the carotid arteries (G5) or by the infusion of a variety of pressor agents could reproduce the situation observed in hypertensive man suggests tha t the elevated blood pressure is responsible for the observed natriuresis (66). Similar results have been obtained in experimental animals, particularly under circums tances where renal vasodilatation precedes the elevation o[ blood pressure (66-69). The relaxation of pre- and postglomerular capillary sphincters permits the more eI-Iective transmission of pressure to the peri tubular capillaries, leading to a greater reduction in net reabsorption of salt and water. Micropuncture and clearance studies suggest that the proximal convoluted tubule is an important site where elevated hydrostatic pressure acts to diminish reabsorption (67-7]). In addition to this, evidence exists indicating inhibition of reabsorption along the distal tubule or loops of Henle

1001 PathojJhysiology of Clinical Disorders of Urine
(72-76). Despite the fact that direct micropuncture data have indicated a diminished fractional proximal tubular rea bsorption in hypertension, many of these studies have failed to provide information as to what happens to absolute reabsorption in this segment. In a recent study, elevation of blood pressure in the rat was accompanied by a rise in peri tubular capillary hydrostatic pressure, hut protein concentration in efferent arteriolar blood rose sufficiently to result in enhanced net peritubular reabsorptive force; yet, natriuresis still resulted (77,78). These findings suggest that, in the absence of prior vasodilatation, the effect of hypertension is beyond the superficial proximal convoluted tubule. On the other hanel, data as to what may be happening in juxtamedullary nephrons is not available. Conceivably, because of the anatomical location of these nephrons, pressure changes may be translated more elIectively and lead to a reduced reabsorptive rate.
Studies in man have demonstrated that the presence of hypertension leads to inability to maximally concentrate the urine. This reduction in Umax is accompanied by diminished TCH20 and cH20 when examined as functions of C'osm and V respectively (79). This combination of findings points to reduced N 'lCI reabsorption by the ascending limb of Henle's loop which Buckalew and his collaborators suggest is the result of transmission of elevated hydrostatic pressure to the peri tubular capillaries of the outer medulla. This attractive hypothesis received some experimental support from the studies of Daugherty and his coworkers (74). As was the case in hypertensive patients, cH20 at any rate of distal delivery was less in dogs made acutely hypertensive by the infusion of angiotensin than in control dogs. It is clear that the reduced NaCI transport in the distal neph
ron, whether in the loop or in more distal diluting sites, is not the result of an Intrinsic abnormality of the transport mechanism but rather an indirect dfect of the elevated blood pressure. As has been described for the proximal tubule, an elevation of peri tubular hydrostatic pressure could reduce net reabsorptive force by increasing back flux of Nael and entry of water into the lumen. The net result will be a greater volume of luminal fluid of higher than normal sodium concentration. Direct evidence for the effect of physical factors on loop reabsorption, however, is lacking, at present.
Diuretics The most commonly utilized diuretics,
such as thiazides and their derivatives including furosemide, affect the active transport of sodium chloride in the distal parts of the mammalian nephron (1,21,22). Such is also the case for ethacrynic aciel (22). The administration of these drugs, therefore, leads to a sharp reduction in the capacity to concentrate and dilute the urine. Because 0 f inability to pump sodi· urn chloride into the interstitium of the renal medulla, fluid emerging into the early portion of the distal convolution is less hypotonic than normal and remains essentially unchanged as it enters the collecting duct. Since the medullary interstitium is less hypertonic than normal and the tubular fluid less hypotonic there is a reduction in the removal of water leading to the formation of urine which, in the hydropenic state, will be less concentrated than normal. During water diuresis the difference in the gradient between lumen and interstitium is narrowed, and the degree of hypotonicity of the final urine will be dependent on the removal of solu te in the ascending limb. Interference with this process will resul t in urine having a higher

1002 Pathoj)hysiology of the Kidney
osmolality than normal. Under some circumstances patients taking diuretics for ill-advised weight-reducing schemes, (unknown to the physician) , may present with polyuria.
The precise mechanisms of action of diuretics are still unknown. It is conceivable, however, that they may affect, directly or indirectly, a sodium-potassium-activated adenosine triphosphatase related to Na' or CI- translocation across the tubular cel1 epithelium (80-84). The relationship of this enzyme to chloride transport remains to be clarified, but, conceivably, the movement of chloride across the cel1, particularly in the ascending limb of Henle's loop where CI- transport appears to be the primary event in NaCI reabsorption, is linked in some fashion to the activity of the enzyme which is known to be present at the basal side of the cell (85). It is of interest that the ascending limbs of Henle's loop contain the highest concentrations of enzyme found in the nephron (25). Diuretics may also interfere wi th energy-producing mechanisms in the tubule, including the production of ATP by mitochondria (86). Irrespective of the effects of diuretics on metabolism it is also known that they may alter the ability to
concen trate or dilu te the urine through reduction in extracellular fluid volume (ECFV). The shrinkage of ECFV, which occurs after prolonged diuretic therapy leads to reductions in renal blood flow and glomerular filtration rate (87). This, in turn, leads to reduced delivery of NaCI to the loop of Henle, reducing concentrating and dilu ting function. Enhanced or avid reabsorption of sodium chloride proximal to the diluting and concentrating sites will also have the same effect (Figure 26-1). Fortunately, recovery of these functions is usually swift after discontinuation of the medication, and in the individual that had
otherwise normal renal function and is hemodynamically stable, the changes are completely reversible. It should be noted that in patients with a prior concentrating defect such as central or nephrogenic diabetes insipidus, diuretic therapy, by a reduction in ECFV, results in the excretion of a concentrated urine by decreasing solute load to the diluting site (88).
Decreased Delivery of Solute to Diluting or Concentrating Sites
As in the case of diuretics, other conditions which reduce delivery of sodium chloride to the distal nephron wil1 limit the amount of substrate arriving at the diluting and concentrating sites (see Figure 26-4). This will lead to a lower than normal Umax in hydropenia and a higher
NoCI ®
@NoCI No cr HIO
H,O
H20 H,O
No CI
®
Figure 26-4. Schematic representation of the nephron. Decreases in G.F.R. (1) and increases in NaCI reabsorption; (2) proximal to diluting segment will result in alterations in urine concentration and dilution by climinishing delivery. Distal tubular reabsorption may be decreased at sites (3), (3'), and (3") and will alter renal dilution. Decreased NaCl reabsorption at (3) will also reduce urine concenlration. ConcentratiOll will also be reduced by changes in the secretion or the response to ADH «4) collecting dUCl).
than normal Umin during water diuresis. Experimental evidence that this may hap

1003 Pathophysiology of Clinical Disorders of Urine
pen, despite the presence of antidiuretic hormone and of normal response to it of the dis tal nephron, was obtained in the classical experiments of Levinsky, Davidson, and Berliner (89) and Berliner and Davidson (90). These autI-lars clemonstrated that reduction in GFR to around 30 percent or less of normal, during hydropenia, resulted in a dilute urine. During maximal water diuresis, reduction of GFR in one kidney led to the excretion of urine of a higher osmolality (isotonic or slightly hypertonic to plasma) while the contralateral kidney continued to excrete maximally dilute urine. Clinically speaking there are three major situations in which reduced distal delivery may result in abnormal urine dilution and concentration. These are salt-retaining states such as congestive heart failure, cirrhosis of the liver and nephrotic syndrome, hypothyroidism (myxedema), and low salt diet.
Salt-Retaining States Controversy still exists as to the site in
the nephron of increased salt reabsorption in the salt-retaining states. It appears clear that the inability to excrete a maximally concentrated or a maximally dilute urine in these circumstances must be the consequence of some malfunction of the distal nephron. In view of the fact that retention may occur anywhere between the glomerulus and the turn of the loop, these conclitions will be equivalent to having reduced sodium chloride presented to the reabsorptive sites in the ascending limb. Clinical studies have been suggestive of distal sodium retention (91,92). If the increased reabsorption takes place in the ascending limb of Henle's loop, some other important feature of the countercurrent mechanism must be at fault in order to result in decreases in dilution or concentration. Changes in permeability character
is tics of the ascending limb and collccting duct might be involved, yet evidence for these changes is not available. On the other hanel, changes in intrarenal hemodynamics Inight be an important cletenninant of the defect. For example, in all the sodium-retaining states medullary blood flow might be increased so as to continuously maintain reduced solute content of the medulla, resulting in the defect already described. In most of the conditions being examined total renal blood flow is usually reduced, and it is unlikely that there is <l
c1isproportiona te increase in meduHary blood flow. :Moreovcr, any increase in medullary blood flow which did occur would be expected to increase sodium reabsorption. li\Thile this mechanism could explain a defect in Umax it should result in an enhanced diluting ability which is not found in these patients. Another site of enhanced reabsorption might be the distal convolution or the collecting duct, but one would also expect a maximally dilute urine under conditions of enhanced delivery to these sites, wllich is not the case. Attempts to clarify the issue by micropuncture studies in animal models of salt retention states are not at all satisfactory. In the first place, the models lead to hemodynamic alterations not entirely comparable to those in man (93-96). Second, when attempts are made to determine the site of retention by micropuncture only superficial nephron segments may be stuclied, and little or incomplete information regarding the loop of Henle can be obtained. Perfusion of superficial nephron loops will provide some information on the function of structures which, because of their anatomical location, may not contribute significantly to the formation of a maximally dilute urine. On the other hand, clata gathered from the descending or ascending limbs of deeper nephrons at the papilla do

1001 Pathophysiology of the Kidney
not allow precise knowledge of the changes occurring in the filtered fluid prior to the descending limb.
Sodimn Restriction (Low Salt Diet or Acute Salt Depletion)
The consequences of salt restriction on renal function, particularly on the ability to maximally concentrate the urine, is still incompletely understood. One of the results of acute sodium depletion is a limitation of the ability to reabsorb solu te-free water (TCH20). This disturbance is of such extent that it may be noticeable at moderate urine Haws and may even be accompanied by the excretion of hypotonic urine (97). These observations in the clog are in accord with those in man (98). Of interest is that Umax may be altered in a trivial way or not at all. Two major explanations have been advanced to explain these findings: first, a decreased penneability to water in the distal convoluted tubule (97); second, a decreased rate of sodium delivery resulting from a lowered plasma soclium ancl reduced GFR (98). For this last possibility to be strongly considered one would expect to find a diminished solute (sodium, possibly urea) concentration in the medulla. A priori this seems unlikely, in view of the fact that Umax is normal. Conceivably, since Umax represen ts fluid equilibration with papillary tissue interstitium, if the defect is confined to the outer medulla, TCI-I20 might be impaired, but not Umax. To examine this, Khoyi et a1. (99) measured renal tissue solutes in acutely salt depleted and control animals. Four hours after acute salt depletion there was a marked reduction in solute content of outer and inner medulla. On the other hand, at twenty-four and forty-eight hours, inner medullary solute concentration had been restored to normal, while outer medullary solute concentration
remained low. Of particular note was the fact that inner medulla sodium concentration was normal, but urea concentration was almost double that seen during control periods.
These observations in the dog deserve to be corroborated since they imply that in this species, the thin ascending limbs might generate the "single effect" and act as countercurrent multipliers. Alternatively, under some circumstances, such as acute salt depletion, the collecting duct may be capa ble of enhancing its capacity for sodium chloride transport into the medullary interstitium (129,130). The acute salt depletion state could perhaps make the papillary collecting duct more permeable to urea than it normally is, even in the presence of ADH. The issue remains unsettled. As far as we know, studies determining cH20 have not been performed. The explanation as to why the defect would be restricted to the outer medulla is not clear. '!\Te are not aware of data bearing on the possibility that the permeability of the collecting duct is altered.
Hypothyroidism (Myxedema) Deficiency in the secretion of thyroid
hormone usually results in profound alterations in renal function. Decreases in glomerular filtration rate (GFR) , in eJIective renal plasma How, and reduced tubular transport maximum for Diodrast and paraaminohippurate (PAH) have been reported (100,101). A marked impairment in excretion of water loads has been described in myxedematous patients (102-105) and in experimental animals rendered hypothyroid by organ ablation or by antithyroid agents (106-108). Accompanying these findings is a low Umax and, at least in man, abnormal free-water generation and reabsorption (109-110). Clinically, the most important consequence of the alteration in

1005 PathojJhysiology of Clinical Disorders of Urine
renal function is water retention and hyponatremia (105). Several mechanisms have been proposed to explain this defect. Suggestions have included: (a) defective distal sodium reabsorption (106,109), (b) relative deficiency of adrenocortical hormones (104), (c) inappropriate secretion of or increased tubular sensitivity to vasopressin (111-113), and (el) decreased delivery of filtrate to the diluting site (l08).
In man, DiScala and Kinney (109) have demonstrated that both °H20 and TCH20, when examined as a function oE V and Cosm respectively, are abnormal in myxedema. Although at the moment when patients were studied GFR was low, it was clemonstra ted that during therapy, TUH20 remained abnormal at a time when GFR had returned to control values. In fact, the defect in diluting the urine was also retained after CFR had been corrected. In contrast, from studies in the rat, Holmes and DiScala (107) and Michael et al. (114) have concluded that in this species, as in man, the main fault lies in the capacity for distal nephron sodium reabsorption. A striking finding in these studies was the demonstration of a substantial leak of sodium by the kidney. For instance, early during 5% saline infusion, when cosm, cNa, and TCI-I2 0 were comparable in hypothyroicl and control rats, the filtered load of sodium was 31 percent lower in the hypothyroid animals (107). A similar finding was obtained in Michael's experiments. This also seems to be the case in man. Vaamonde and his coworkers (106) have observed that in severely myxedematous patients, there is a prolongation of the time required to reduce Na' excretion by 50 percent (Na tl/2) following a natriuresis, and cumulative Na+ losses are increased when compared to euthyroid patients. In the study of Emmanouel et al. (115), fractional Na clearance was higher
in hypothyroid rats than in controls during administration of massive sodium loads. Nevertheless, in the same experiments, net sodium excretion remained unchanged. Also, both net and fractional sodium excretion were lower in hypothyroid rats during water diuresis experiments in which the amount of sodium infused was smaller. The significance of the finding' of impaired renal sodium handling in either man or rat is not apparent and remains to be clari· fiecI. The relationship between filtered load and distal soclium reabsorption has been Eurther examined by Katz and Lindheimer (lOS). In an ingenious study these investigators demonstrated that in the experimentally-hypothyroid rat, the reduction in N a+·I(+·ATPase activity observed in both cortex and medulla results from the diminished filtered load of N aCI. Thus, the concentrating defect is not the result of the reduced enzyme activity but of the reduced distal delivery of Na+. The findings with Na-·K!-ATPase conform with other findings by Katz and Epstein (1l6), demonstrating that enzyme activity is influenced importantly by the filtered load of NaG!.
Experiments by Reville and Stephan (117,118) have shown that the defect in sodium metabolism is unchanged in the hypothyroid l"at, despite adrenalectomy. Furthermore, addi tion oE mineralocorticoid hormones did not abolish the alterations in sodium excretion, making it unlikely that adrenal conical hormones playa major role in the abnormality of renal function.
More conclusive data from the studies of Emmanouel and his colleagues (115) have eliminated the possibility that inappropriate secretion of, or undUly high sensitivity to, ADH can explain the findings of altered water metabolism in the experimental animal. Studies in the hypothyroid Brattleboro rat, a strain with can

1006 Pathophysiology of the Kidney
genital absence of ADH, have shown that the changes in Umax and in absolute values for cH20 and T G f-I2 0 are identical to those occurring in hypothyroid rats from normal strains. Furthermore, in this species, tissue osmolality and sodium concentration of cortex, medulla, and papilla in rats made hypothyroid is identical to that of control rats. Perhaps of greater significance is the fact that fractional TCH20 curves are identical in hypothyroid and normal rats regardless of the species utilized, indicating that at low rates of urine flow, the llefect is primarily the result of diminished delivery to the diluting site. In addition, during hypotonic (0."15%) saline infusion, absolute sodium delivery to the diluting segment and free-water clearance were markedly lower in hypothyroid rats. Despite this, hypothyroid and control animals had similar fractional distal sodium delivery and fractional free-water clearance, suggesting also that the reduction in absolute freewater formation in hypothyroid rats was due to decreased net distal delivery.
Alterations in Medullary Blood Flow Altered renal blood flow is possibly re
sponsible for the defects in urine concentration seen in sickle cell disease, multiple myeloma, and pyelonephritis.
Sickle Cell Hemoglobinopathies Inability to maximally concentrate the
urine is one of the characteristics of HbS in its homozygous (HbSS) or heterozygous state (HbSA), as well as of HbSC disease. The observation has also. been made that the administration of vasopressin does not raise urine concentration above the mbmaximal levels attained by dehydration (119,120). Although less consistently, similar observations have been made in patients with sickle cell trait (119) and sickle cell disease (120). An early report demonstrated
that the inability to excrete maximally concen trated urine is directly related to the sickling phenomenon, rather than to other inherited or acquired defects (121). It was shown that urine can be concentrated following exchange transfusions of normal blood to young (five years of age or less) sickle cell anemia patients. Also demonstrated in this importan t study was that with time, the defect becomes irreversible, being permanent in the adult suffering from HbSS disease. It is also of importance that there is a significant progressive decrease in renal concentrating ability with age in HbSA subjects (lIS).
A possible mechanism for the development of the defect could be direct or indirect in terference by the sickling process with active NaCI transport in the ascending limb of Henle's loop. Several lines of evidence mitigate against this possibility. Measurements of free water reabsorption (TOH2 0) during mannitol diuresis in HbSS adults and children have been found to be essentially identical to those of normal individuals (122,123). Initially, during manni tol loading, TCH2 0 rises progressively with increasing rates of osmolar clearance (Cosm) until TCI-I20 either levels off in plateau fashion or slowly declines (19). The flat or descending portion of the curve describing the TOH20 to °osm relationship during mannitol diuresis, is the consequence of the l'eduction in tubular fluid sodium chloride COllcell tration caused by the osmotic agent. This imposes a limitation on the transport of NaCI into the medullary interstitium by the ascending limb (19). Therefore, at rates of cosm prior to the plateau, NaCl transport by the ascending limb must be normal in HbSS disease. Because of the possibility that the flattening of the curve imposed by mannitol may obscure a NaCI transport defect in the loop at higher rates of cosm,

1007 Pathoj)hysiology of Clinical Disorders of Urine
Hatch and his collaborators (124) examined the effects of 3% NaCl infusion 011 the TCI-I:!O to Gosm relationship. In this circumstance, TOH:!O rises with increasing cosm without any evidence of a limit being reached, since luminal sodium chloride concentration in the loop does not fall (19). It was found that in HbSS subjects, in contrast to normal individuals, TCH20 reached a maximum at levels of cosm similar to those at which a plateau occurred during mannitol infusion. Although this suggests impairecl sodium reabsorption at high rates of sodium chloride delivery to the loop, free-water clearance (OH20) was found to be normal throughout wide ranges of dis tal delivery, indicated by the rate of urine flow (V). Furthermore, the fractional excretion of sodium during mannitol, saline, or water diuresis or at control rates of solute excretion dill not differ between control and HbSS subjects (124). These results make it unlikely that a gross defect in active sodium chloride transport by the ascending segment of the loop of Henle is the cause of the concentrating disorder.
The combination of a diminished Umax and the impaired TOH20 during hypertonic saline diuresis could be ex})lained on the basis of an abnormal permeability to water in the collecting duct. Deficient secretion of ADH, diminished responsiveness of the collecting duct to ADH, or a primary alteration in the permeability of the distal nephron to water could lead to the findings in sickle cell patients.
Absence or decreased secretion of ADH by sickle cell patients does not seem to be responsible for the concen trating defect. As already noted, transfusion of normal blood into young patients leads to 11m-mal Umax (121,123). Thus, secretion of ADH must be normal at least at an early age. Conceivably, at later stages of the disease, the areas of the hypothalamus which regu
late secretion of the hormone might be so involved by microinfarction, that despite the appropriate stimulus, circulating titers might be suboptimal. This seems unlikely, in view oE the fact that water loading is promptly accompanied by reductions in urine osmolality to levels equal to those seen in normals (120,124,125). Disruption of anatomical pathways sufficient to result in altered honnone secretion would not be expected to be accompanied by maintenance of an intact feedback mechanism. Furthermore, in HbSA subjects, it would be difficult to invoke vascular involvement of the bypothalamic-posterior pituitary axis, in view of the lack of thrombotic episodes in this group (126,127).
On the basis of the experience with young patients, similar arguments may be leveled against the suggestion that the basic defect is one of diminished responsiveness of the collecting duct to ADH. Since the defect becomes progressively worse with increasing age (120,128), an effect on the cellular actions of ADH at the level of the collecting duct may be involved. The nature of this alteration is probably not in the response of the collecting duct to ADH. The urinary excretion of cyclic AMP in sickle cell anemia patients underg'oing water diuresis reaches levels similar to those of normals following the intravenous administration of vasopressin (55). Also, urinary osmolality rises albeit less than in normals (55). This indicates that there is some cellular response to endogenously formed cyclic AMP, the presumed physiological messenger of ADH. In view of the fact that urine is not maximally concentrated, structural defects in some cells may make them refractory to the action of cyclic AMP, thus contributing to the reduced Umax. Nevertheless, this alone cannot entirely explain the defect.
A primary alteration in the permeabil

1008 Pathophysiology of the Kidney
ity o[ the distal nephron appears even less plausible in older patients with the sickling phenomenon. Reduced permeability to
water (to account for diminished Umax) would not allow the generation of normal TCH20 during mannitol diuresis nor would TCH20 values reach levels shown to
occur before a defect is demonstrated during 3% saline diuresis. Furthermore, cH20 would be supernormal, since the volume of water which is normally reabsorbed from the collecting duct during water diuresis (1,8,129,130) would be excreted in the urine.
In 1961, Herbin and his collaborators (131) demonstrated that sickling could be induced in vitro by placing erythrocytes of patients with HbS in hyperosmolar solutions. They postulated that entry of cells into the medulla leads to sickling, sludging of cells because of increased viscosity, and diminished medullary and papillary blood flow with disruption of the concentration profile. Perillie and Epstein (132) extended these observations by careful analysis o[ the different factors which may lead to sickling in the renal medulla. It was shown by these investigators that other factors which are usually associated with the production of sickle cells, such as low pH and hypoxia, are superceded by the effect of hyperosmolar salt solutions under all conditions in which this situation was tested. Furthermore, the viscosity of the solution of sickle cell anemia blood and hypertonic sodium chloride was greater than that of thalassemia major or normal blood mixed with hypertonic saline. Of particular importance was the finding that unlike the sickling promoted by low oxygen tension, which takes two to four minutes to become apparent at body temperature, sickling induced by hypertonic solutions occurs and may be reversed practically instantaneously. These investigators there
fore suggested a sequence of alterations produced by the sickling of erythrocytes similar to those postulated by Herbin et '11. (131).
In the model proposed by Herbin et al. (131) and Perillie and Epstein (132), failure to excrete a maximally concentrated urine would be the consequence of interference with active sodium chloride transport in the ascending limb of Henle's loop or alterations in the impermeability to water of this structure. Evidence has already been cited which does not support the notion that active sodium chloride reabsorption in the ascending limb is responsible for the defect in urine concentration. Changes in the impermeability to water of the ascending limb would not be associated with normal TOH~O during mannitol diuresis nor with normal cH~O
during water diuresis. ·Were water reabsorption to follow sodium chloride reabsorption in the loop, the osmolality of interstitial fluid would be reduced, and freewater reabsorption would be severely limited throughout wide ranges of cosmo During water diuresis, water reabsorption in the ascending limb would permit Huid of higher osmolali ty to emerge into the distal convolution and enter the collecting duct. Throughout a wide range of V, urine would be less dilute than normal, and cH20 would be lower than normal. Furthermore, maximal urine diluting ability would be impaired, which is not the case in sickling hemoglobin disease.
The findings of a low Umax amI an abnormal TCH20 at high rates of cosm may be explai ned if the disease has selectively destroyed juxtamedullary nephrons with long thin limbs of Henle which descend into the papilla. In view of the normal capacity to excrete maximally dilute urine, the assumption must be made that long thin loops arc not necessary for

1009 Pathophysiology of Clinical Disorders of Urine
the elaboration of a maximally dilute urine. In order for this to be the case, the major site of active NaGI transport in the ascending limb, if not the only site, has to be the thick portion. Long thin loops dipping into the papilla would only be involved in the concentration of urine at low rates of flow by a mechanism other than active transport. Kokko and Rector (18) have proposed that the permeability characteristics of thin loops with respect to Nael, urea, and water, rather than active sodium transport by these structures, arc what determines urine concentration. In this model, papillary accumulation of urea and active NaCI transport by the thick ascending limb play the central role in urine concentration at low rates of urine flow. Similar proposals have been made by Stephenson (16) and by Stewart and Valtin (17). Elimination of the papilla would remove the major mechanism of urea recirculation, in addition to reducing the length of the collecting duct. This last feature would also explain the finding of an abnormal TOHzO at high rates of flow. The large volumes of hypotonic fluid entering into the shortened collecting duct will have less time to equilibrate with the interstitium as flow rises. Consequently, cosm will rise, but TCHzO will either plateau or fall. The evidence that thin ascending limbs are not essential for the excretion of maximally concentrated urine, and that their function may not involve active NaGl transport, can be naturally found or artificially created. In Macaque (13) and Rhesus (12) monkeys, Tisher and his collaborators have shown that long thin loops are SCal"ce; yet, Umax is normal as is TOHzO at low rates of flow, but at high rates of osmolar clearance, reductions in TCHzO are apparent. By surgical ablation of the papilla in the rat, Lief et al. (14) and MartinezMaldonado et al. (15) have shown that
Umax is reduced, but TCHzO remains normal during solute loading until high levels of °osm are achieved. Furthermore, in this model, as in the case of sickle cell states, °1-120 remains intact throughout a wide range of urine flow (15).
One may visualize that therecluction in blood flow to the papilla, which occurs as a result of increased viscosity induced by sickled erythrocytes, results in a functional papillectomy. This is reversible in the early stages by transfusions, but, as time elapses, irreversible damage takes place and blood exchanges will not correct the defect. On the other hanel, the changes in Umax and TCH20 described above will persist.
Multiple Myeloma Changes in urine concentration and
dilution may take place during the course of multiple myeloma as a consequence of its various complications. Thus, hypercalcemia, pyelonephritis, and renal insufficiency may all be found as causes of Umax defects (41).
Of interest is the possibility that when hyperviscosity secondary to hypergammaglobulinemia is found, it may interfere with the function of the countercunent system. In fact, two subjects with this syndrome in whom Umax was affected have been reported (133). The hyperviscosity syndrome, however, is a life-threatening condition, the treatment of which takes precedence over any desires to solve the mechanism by which the countercurrent system is affected.
Should there be massive plasma cell infil tra tion of the kidney, and were this to predominate in the medulla, a Umax defect might develop. The authors are aware of one patient in which this may have contributed to abnormal renal function (41).
A curious possibility is that amyloid

1010 Pathophysiology of the Kidney
})roduced by the myeloma cells may selectively surround some of the structures within the medulla. This, as in the case reported by Carone and Epstein (13"1), could lead to a syndrome of nephrogenic diabetes insipidus (should it involve the collecting duct) , or a disorder of reduced filteredloacL to the diluting site if the glomeruli are beavily involved.
Pyelonephritis The association between chronic urin
ary tract infection and an impairment in renal concentrating ability is well known. In the past fifteen years it has also been found that normal and pregnant women with acute pyelonephritis or asymptomatic bacteriuria have a defect in urine-concentrating ability (136-138). The reduced Umax, in fact, is probably the earliest evidence of the invasion by bacteria of the renal medulla. Experimentally, a similar functional disorder has been reproduced in rats innoculated intravenously with gram positive cocci or gram negative bacilli (140, )41). The direct relationship between the localization of the bacteria in the genitourinary tract and its functional and therapeutic import may be appreciated from the studies of Ronald et al. (142) and Clark et al. (143). Utilizing selective catheterization of the ureters, these authors determined the precise site of bacteriuria in approximately sixty-six individuals in which this had been a recurrent problem. It was established beyond doubt that renal but not bladder bacteriuria is associated with decreased urinary concentrating ability. Patients in whom bacteriuria had a renal origin presented, in addition to the low Umax, [771 ± 122(SD)mOsmjKg; n:::::38] , a reduced urine urea concentration (Uurea). It has been sugges ted that this reduction in Umax may be the consequence of increased renal blood flow (particularly medullary
blood flow) as a result of the pyrogenic reaction (144). In acute pyelonephritis of animals or man this may well be the case. In fact, Gonick et a1. (145) studied rats with acute pyelonephritis induced by enterococci and found that in the medulla, the concentration of sodium was normal and that of urea markedly reduced. Since the initial event may be a marked increase in renal medullary blood flow, this would lead first to increased U urea, yet, with time, should the hemodynamic alteration persist, Uurea would fall. The pyrogen response need not be systemic but could be localized to the medulla. Evidence for this may be gleaned from patients with unilateral renal bacteriuria where the control kidney continued to excrete urine with an osmolality comparable to normal, while Umax was distinctly lower in the diseased kidney despite comparable GFR in both (1"12,1'13). This finding also rules out the possibility that dietary factors, such as protein or water intake, may determine the presence of the Umax defect. The direct relationship between the abnormal Umax and the bacteriuria is also suggested by the fact that appropriate therapy tends to revert Umax to normal as the bacteria are eradica teel (1'16,147) .
Studies attempting to elucidate the nature of the concentrating defect were performed in patients with acute pyelonephritis by Suki, Axelrad, Eknoyan, and Martinez-Nlalclonado (148). The subjects were, in general, women who presented with fever, flank pain, dysuria and positive urine culture (bacterial counts: 100,000 coloniesjm1 urine). Within twenty-four hours of subsidence of acute symptomatology, a Umax was performed. Despite an average GFR value of 125 mljmin / 1.73 m2 (control 120 mljminj1.73m2) there was a severe limitation in Umax (468 to 850 mOsmjKg as compared to controls of

Pathophysiology of Clinical Disorden of UTine 1011
904 to 1072 mOsm/Kg). TCH20 at any level of cosm was less in patients with acute pyelonephritis than in controls. On the other hand, cH20 versus V was identical in controls and patients. 1n view of the clata on Uurea in humans and experimental animals, these results are best explained by ei ther increased medullary blood flow with urea washout or altered permeability of the collecting duct to urea and water. An alternative is that both these mechanisms may be operative. Clearly, this is related to the bacteria. ·Whether these interfere directly, through the production of toxins or pyrogens, or by disrupting the normal archi tecture of the medulla is, at present, still a matter of conjecture.
Changes in Nephron Membrane Permeability
Figure 26-5 demonstrates the supposed effect of ADH on a renal tubular cell and the presumed physiological consequences that follow. It is now well accepted that cyclic AMP is the physiological messenger of the cellular actions of ADH, and that this nucleotide is responsible for changes in tubular permeability and ion transport
POSSIBLE SITElS) OF ACTION OF SUBSTANCES WHICH MAY LEAD TO NEPHROGENIC OIABETES INSIPIDUS
(SEROSA) BLOOD ;'00''" r@
\ la!".
,,,...,,1 ;:;.' ....
AlP, ~: HtO
~'!
Cyclic AMP J (""'O'AI
UfllHE
~' AMP
Figure 26-5. Schematic representation of a collecting duct all indicating possible sites where drug effects may lead to the generation of nephrogenic diabetes insipidus.
(149). By blocking any of the steps which follow the release oE ADH into the cirClllation, a variety of therapeutic compounds may lead to abnormal urine concentration and/or dilution. The most common clinically utilized agents responsible for functional disorders involving the adenylate cyclasecyclic AMP system include lithium salts, tetracycline, amphotericin-B, and methoxyflurane.
Lithium Therapy Lithium salts, which have their main
clinical usage in the treatment of manicdepressive states, has been observed to lead to polyuria and a defect in urine concentration (150,151). Even when doses are prescribed to maintain serum levels in the range between 0,5 and 1.5 mEg /1, it may lead to the procluction of polyuria and polydipsia. III man it has been shown that the reduced Umax is accompanied by a defect in TCH20 formation, but that the 01-12 ° to V relationship is no different than that of controls (152). Experimental evidence advanced by Martinez-Maldonado and his collaborators (153) and by Forrest et al. (154) has corroborated that this is also the case in rats. It is clear that lithium polyuria cannot be completely abolished by the administration of large doses of vasopressin. In fact, the excretion of urinary cyclic AMP, a measure oE the responsiveness of the distal nephron to ADH, is diminished under basal conditions or in response to exogenous ADH. A finding of great interest is that the change in water excretion in response to cyclic AMP in animals which have been rendered polyuric by the administration of lithium, appears to be somewhat better than those produced by vasopressin (153). This suggests that the defect is in the formation of cyclic AMP or at the site of hormone stimulation oE the adenyl cyclase receptor. On the
I!
I
f_ I

1012 Pathophysiology of the Kidney
other hand, there might also be some defect at a step beyond the forma60n of cyclic Al\J[P since the observation has been made that some doses of cyclic AMP do not revert the Uosm defect to normal (154). Studies in isolated anuran epithelia have been equivocal (155-] 58). In these studies an eHect of Li+ has been proposed before cyclic AMP formation and after this step. As in the case of other drugs leading to nephrogenic diabetes insipidus, the possibility that, in the whole animal, the defect may result from the loss of another ion needs to be considered. The possibility that prolong-ed lithium therapy may lead to potassium depletion with subsequent inability to concentrate the urine has been suggested, but it appears quite clear that this is a specific effect of the lithium ion. Usually, there are no changes in GFR and renal blood How, so that hemodynamic alterations as the cause of the defect seem unlikely.
Tetracycline TheralJy Demethylchlortetracycline (demeclocy
cline) has been reported to produce a syndrome of nephrogenic diabetes insipidus in some patients (159-161). The use of other tetracyclines have been implicated 111
several renal tubular syndromes, and nephrotoxic effects have been observed during utilization of outdated (degraded) tetracyclines (162,163). The renal changes produced by degraded and other tetracyclines simulate the Fanconi Syndrome and involve, in addition to polyuria, hypokalemia and defects in the renal transport of P04 , urate, and glucose. By contrast, the changes produced by demeclocycline appear limited to the distal nephron. "Vilson et aI. (1M) studied three patients receiving demeclocydine and two patients receiving nondegraded tetracycline. In the former, Umax, after sixteen hours of clehy
dration, fell to 48 percent of control, while it only fell by 9 percent in the latter. Similarly, TOH20 was markedly reducecl by the usc of clemeclocycline, while it was not altered in the subjects ingesting tetracycline. Urinary cyclic Arvrp excretion after the administration of vasopressin to patien ts on demecIocycline, was essen tiaIly unchanged, indicating lack of response to the hormone in these patients. Further evidence for a major effect of demeclocycIine in the permeability of the distal tubule to water was advanced by Singer and Rotenberg (165). In eight out of twenty-four patients receiving clemecIocycline for acne, there was a clearly abnormal Umax. Further studies on three patients in whom Umax was below 450 mOsm/Kg revealed grossly abnormal TCH20 to cosm curves in two, while it was borderline in the other. Proof that ascending limb function was normal was provided by the fact that Dmin, °H20 and urine flow rate were equal when control and demeclocyclinetreated subjects with abnormal Umax were compared. In vitro studies by Singer and Rotenberg (165) disclosed that addition of demeclocycline to the serosal side of toad urinary bladders resulted in inhibition of ADH-inducecl and cyclic-AMP-induced water flow. Water How induced by ADH was inhibited more significantly. These findings suggest that demeclocycline probably inhibits both cyclic-AMP production and cyclic-AIVIP action. Of clinical import:ance was that the effect was rapidly reversible after removal of the antibiotic from the serosal bath. Supporting evidence for in terference of demeclocycline with the cellular action of ADH has been accrued by Dousa and '\'\Tilson (166). Renal medullary extracts containing adenylate cyclase, protein kinase, and cyclic AMP phosphodiesterase activity were isolated and exposed to various concentrations of demecIoeycline.

1013 Pathophysiology of Clinical Disorders of Urine
Basal and Huoride and ADH-stimulated adenylate cyclase activity were inhibited. Similar doses of the antibiotic also produced inhibition of the cyclic AMP- depenclen t cytosol protein kinase. These findings indicate that clemeclocycline has the potential to inhibit cyclic AMP formation and its accumulation in the renal medulla in response to AD H. It also has the potential to inhibit the cyclic AMP-dependent phosphorylation of proteins in the renal medulla. An important observation in these studies was that tetracycline and chlortetracycline can produce in vitro in similar concentrations, the same effect as demeclocycline, yet in vivo they do not produce nephrogenic diabetes insipidus. Although not clear, it is likely that the penetration of these other tetracyclines into distal renal tubular cells may well be poor or of lesser degree than in the case of clemeclocyeline.
Anesthesia (Fluoride Toxicity) Patients who have received methoxy
flurane (Penthrane@) anesthesia, with the usual anesthetic adjuvants, have developed dose-related abnormalities in renal function (167). Exposure to minimum alveolar concentration of the anesthetic for 2.5 to 3 Ius, i.e. 2.5 to 3 MAC/hr (serum inorganic fluoride above 50 fLmol I I) has resulted in subclinical toxicity. By contrast, all patients in whom doses greater than 5 MACI hr (serum inorganic fiuoride above 90 jLmol/l) have been utilized, have developed clinical toxicity (167,168). The major manifestation of this clinical toxicity appears to be the development of a polyuric syndrome which is resistan t to the effect of vasopressin (169). Most likely associated with the presence of the fluoride ion, it is conceivable that this is a result of inabili ty to reabsorb sodium in the ascending limb of the loop of Henle since fluoride, a
well-known inhibitor of anaerobic metabolism, might interfere with sodium reabsorption at this site (170). On the other hanel, inhibitors of anaerobic metabolism may also result in inabili ty of the papillary collecting duct to respond to vasopressin (171). Studies utilizing inhibitors of anaerobic metabolism in the toad bladder and frog skin have shown that both the hydroosmotic eiTect and the stimulation of sodium transport induced by ADH afe blocked (172) .
AmphQtericin-B Therapy The antifungal agent amphotericin-B
has also been demonstrated to induce a defect in maximal urine concentration (173). Polyuria and nocturia occur frequently, and there is resistance to the effect of exogenous vasopressin (174). It should be clear, however, that the Umax defect is associated with marked impairment in GFR (173). The fall in filtration rate often represents as much as 50 percent of normal which, by reducing distal delivery, could curtail the development of a hypertonic medullary interstitium and result in a reduced Umax. Furthermore, potassium depletion is a frequent companion of amphotericin nephrotoxicity and could be the sole or compounding factor in the development of the urine-concentrating defect (175-177). Another contributing factor may be an actual reduction in the number of functioning nephrons, particularly juxtamedullary, as a result of structural defects produced by the drug (173, 17'1). Lastly, amphotericin-B may directly interfere with the permeability or solute selectivity of the distal nephron membranes. Furthermore, the effect of antidiuretic hormone on the collecting duct may be altered. Studies in isolated membranes such as toad bladder, have demonstrated that amphotericin-B increases the

101 <1: Pathophysiology of the Kidney
permeability of the plasma membranes to urea, thiourea, potassium, and chloride (178). Other membranes are also known to be affected. In erythrocytes, amphoteri cin-B increases the permeability to potassium, sodium, and chloride and to hydrophilic nonelectrolytes smaller than sucrose (179). It is possible, therefore, that an enhancement of the permeability of the nephron cell membranes to these ions, together with conformational changes which prevent normal water movement across the cells of medullary structures, may result in an inability to concentrate the urine. Also, it is entirely conceivable that the same effects noticed in the collecting duct may take place in the ascending limb of Henle's loop, making this structure less impermeable to water. This would result in diminished genera tion of free water and reduced interstitial solute concentration. Tvlore precise knowledge of the mechanism of amphotericin-B-induced nephrotoxicity is clearly needed.
Defects Resulting from Alterations in Medullary Architecture
Cystic Disease of the Kidneys A number of inherited and acquired
diseases may result in alterations of the anatomical interrelationships between the loop of Henle collecting-duct system and the medullary vasculature, leading to defects in urine concentration and dilution. Classical examples of congenital anomalies which are accompanied by defects in Umax are polycystic kidneys, medullary cystic disease, and medullary sponge kidney. Some acquired disorders, in particular obstructive uropathy, may well represent situations in which architectural derangements in the medulla are the major reason for changes in concentration and dilution. Clinically, all these patients may have polyuria and hyposthenuria, even in the absence of
severe renal failure. Inability to maximally concentrate the
urine is probably the earliest functional disturbance in patients with polycystic kidneys and medullary cystic disease (180,181). Hyposthenuria in these states may be uncovered in the absence of renal insufficiency (180,182). In view of the low Umax, despite normal GFR, one of the possible mechanisms leading to the defect is abnormal sodium chlorille transport in the distal nephron. In the case of polycystic kidney disease this does not appear to be the case since patients, throughout a wide range of renal function, possesses the abili ty to dilute the urine maximally, and they exhibit normal free-water clearances (I 80). The authors are not aware of detailed studies bearing on this point in patients with medullary cystic disease. Nevertheless, in one case of sponge kidneys, both Umin and free-water clearance were perfectly normal in the presence of a low Umax. A priori, it is conceivable that urinary diluting ability and capacity in medullary cystic disease are abnormal. This disorder is accompanied by salt-losing nephritis, suggesting a defect in the handling of NaCl in the distal nephron. Utilizing a similar reasoning, one might infer that TOH20 as a function of °osm is also impaired. Despite this speculative argument, one cannot discard the fact that a significant anatomical derangement exists which may compound the functional disorder.
Obstructive Nephropathy Obstruction of the urinary tract results
in impaired ability to excrete a maximally concentrated urine (183). This abnormality depends on the duration and completeness of the obstruction (184-189) ancl of the presence or absence of infection (190,191). Acute complete obstruction is accompanied by loss of the ability to maximally concen

1015 Pathophysiology of Clinical Disorders of Urine
trate the urine, so that Umax on the affected side is considerably lower than in the contralateral kidney (186,187). In this case the associated finding that tissue concentration of solute is sharply reduced has led to the suggestion that medullary blood How is increased and thus leach to washout of solute (192). This conclusion, however, was based on the demonstration that the renal extraction of PAH from renal arterial blood was decreased. This inference is at best tenuous, since incomplete extraction does not necessarily represent perfusion of tissue (medulla) incapable of secreting PAR (193). Studies employing 851(1' washout (191,195) and indocyanine green mean transit time (196) have not corroborated that medullary blood flow is increased. The origin of the low Umax is most likely the result of two other factors: first, a sharp reduction in GFR, leading to reduced NaCI delivery to the diluting site which, in turn, would explain the reduced medullary tissue solute concentration if the analysis were made without the reestablishment of urine flow; second, should urine flow be reestablished, and then analysis of Umax and tissue solute concentration done, the time to replenish medullary solute and raise Umax might be insufficient. "When obstruction has been present for twelve to twenty-four hours, changes in collecting duct function may already be present. At this time, studies in the rat (197) and the rabbit (198) have demonstrated dilation of the collecting duct at the inner stripe of the outer zone. In addition, engorgement and dilation of the radicals of the renal veins and numerous small hemorrhages can be seen. These alterations may result in failure of these structures to respond to ADH in a normal way and lead, even after replenishment of medullary solute concentration, to low Umax.
In contrast to complete acute obstruc
tion, partial acute obstruction is not associated with a reduced Umax (188). This appears to be the case in the hydropenic an tidiuretic animal, as well as during enhanced distal delivery through the infusion of hypertonic saline. Since, in these two models, medullary blood flow increases [as measured by fiber-optics (196)], it is clear that it is most unlikely that this hemodynamic change can explain the fll1dings in complete obstruction. The maintenance of Umax during acute incomplete obstruction suggests, in fact, enhanced NaCl reabsorption in the ascending limb (188,199).
The duration of urinary tract obstruction in man is difficult to ascertain so that, by necessity, most of the aforementioned studies have been in the experimental animal. Nevertheless, it is dear that according to the alterations in I'enal function, one may clinically categorize obstruction into acute and chronic. Clinically, the latter may be characterized by polyuria with inability to concentrate the urine and mimicking nephrogenic diabetes insipidus (200203) , while the former will be accompanied by reduced urine flow, and diminished freewater excretion with a higher Uosm (188). The differences between acute and chronic obsti'uction have been best characterized by the classical studies of Suki, Eknoyan, Rector, and Seldin (204). Studies in dogs revealed that acute unilateral ureteral elevation led to reduced urinary sodium concentration, sodium excretion, and cH20/100 ml GFR, a pattern similar to that of renal arterial constriction and thus suggesting diminished delivery of NaCI to the ascending limb. On the other hand, unilateral chronic hydronephrosis resulted in an increase in urinary solute com:entra· tion and urinary sodium excretion, Absolute 0HzO was decreased but °HzOjlOO ml GFR was actually increased, indicating increased solute delivery to the diluting

1016 Pathophysiology of the Kidney
site. The possibility that back-diffusion of free water in the collecting duct may have played a role was also considered. Further evidence that loop function is intact was obtained by Eknoyan, Suki, MartinezMaldonado, and Anhalt (205). In dogs with unilateral chronic obstruction it was demonstrated that free-water reabsorption is normal, as was the renal tissue content of Na. In fact, despite marked reduction of GFR and RPF, the corticopapillary gradient for sodium during hypertonic saline diuresis was essentially the same in the hydronephrotic and control kidneys. This finding ellectively eliminates reduced GFR as a factor in this case. Other factors, therefore, must be responsible for the low Umax. It is possible that, as has been mel1lioned, cellular atrophy secondary to the increased intraluminal pressure renders the collecting duct hypo- or unresponsive to ADH. This seems unlikely, in view of the normal TDH~O during hypertonic saline diuresis. The nephron hyperperfusian state (increased GFR per nephron), on the other hand, may be responsible. Because of the increased distal delivery, large volumes of hypotonic fluid will el1ler the distal tubule following the removal of solute in the ascemling limb. The fluid will en tel' the collecting duct and be excreted without attaining equilibrium with the interstitium. Alternatively, the most attractive possibility is that the normal equilibration of fluid between collecting duct and interstitium is not attained, because the normal architecture of the medulla and the physiological charatceristics of its structures have been disrupted. Perhaps the solute transported into the medulla is, in a sense, "compartmentalized", because the distances from its site or: accumulation to the collecting duct do not permi t an effective osmotic pressure to be exerted under these circumstances. This
will lead to polyuria, which is unresponsive to ADH administration.
Analgesic Nephropathy Disrup tion of medullary architecture is
also responsible for the abnormality of urine concentration seen in analgesic nephropathy. In most cases, the defect in urineconcentrating ability seen in these patients is the result of reductions in glomerular filtration rate (206). Nevertheless, in some patients, the magnitude of the reduction in urine concentnuion is greater than can be accounted for by diminished GFR (207). It is in these patients that the functional defect may result from anatomical changes in the area of the medulla. It is also clear that papillary necrosis, which is a common consequence of analgesic abuse, amply explains the abnormality in urine concentration in some cases. In fact, marked medullary interstitial sclerosis and loss of tubules, as well as tubular basement membrane sclerosis, are frequently observed even in patients whose creatinine clearance is as high as 90 ml/min or more. Histological changes may lead to the observed defect without the need to invoke a direct toxic effect of the analgesic on inherent functional parameters 0 f the cell. N evertheless, Bluemlc and Goldberg (208) have advanced evidence suggesting that accumulation of metabolites of phenacetin may have toxic effects on the cells of the medulla. Since a defect in urine acidification is frequently seen under these conditions, structural or functional damage to the collecting duct may well be of importance in the concentrating defect (209).
Miscellaneous Another condition in which medullary
interstitial swelling and edema may interfere with normal concentration, by increasing pressure in the area, is lympho

1017 Pathophysiology of Clinical Disorders of Urine
matous infiltration of the kidney. A case representing this phenomenon has been observed by one of the authors (210), and a similar case has been recently reported by Steele and his associates (211). In the latter case, X-ray therapy of the involved kidney reduced cellular infiltration by the tumor and reverted the Umax toward normal, demonstrating the direct relationship between edema of the medullary area and the abnormality in urinary concentration.
Acquired Chronic Renal Disease The ability to concentrate the urine is
impaired in chronic renal disease. In contrast to the case in chronic obstruction, this aberration rarely takes the form of nephrogenic diabetes insipidus but rather urine, most likely reduced in volume, has an osmolality which approaches and becomes isotonic to plasma. On some occasions urine may become hypotonic to plasma and will remain so despite the administration of vasopressin. This syndrome of vasopressin-resistant hyposthenuria had been described rarely in patients with chronic pyelonephritis (212,213) and in children with chronic renal disease (214). More recently, Tannen and his collaborators (215) have demonstrated that this disorder is not as rare as previously thought. Vasopressin-resistant hyposthenuria was present in eleven of thirteen patients with chronic renal disease of various etiologies studied by this group. The mechanisms by which these changes in urine concentration arise are not perfectly clear. Of interest is that urine dilution remains intact even after Far-advanced renal failure is present (21'1-216), suggesting that function of the loop of Henle is intact. The experimental studies of Bricker et al. (217) have provided strong evidence for the in tegrity of function of the ascending limb. In dogs
with three varieties of unilateral experimental renal disease, the values for TCH20 and cH20, when expressed as a fraction of the GFR, were within normal limits. In fact, cH20, whether fractional or absolute, tended to be higher in the diseased kidney than in the control. By contrast, in subjects with GFR's ranging from "1 to 127 mIl min, the administration of hypotonic mannitol under conditions of maximal hydration resulted in an increased fractional sodium excretion in those with a low GFR. Because fractional distal sodium reabsorption (or-I20 /GFR) appeared lower in subjects with low GFR than in those with normal GFR, it was concluded that an alteration in distal sodium reabsorption was present in chronic renal disease (216). This conclusion seems unwarranted, since it only demonstrates that flooding of the distal nephron by fluid contalning a nonreabsorbable solu te will limi t cH2 0 generation more in subjects with low GFR than in normals. This may well be compounded by the increased delivery of proximal tubular Iiuid, which may be normally present in patients with chronic renal insufficiency (218). The importance of solute load per nephron on distal sodium reabsorption in chronic renal disease has been demonstra teel by Coleman and his collaborators (219). These authors were able to reduce the excretion of sodium by reducing filtered load in subjects with chronic renal disease. On the other hand, as in the studies of Kahn et al. (216), infusion of mannitol led again to a fixed amount of sodium loss in the urine.
In addition to solute load per nephron, it is possible that uremic toxins render ineffective the action of ADH. This possibility has not been thoroughly explored, although circumstantial evidence suggests that, if present, the toxin is not llialyzable (215) .

1018 Pathophysiology of the Kidney
More important may be alterations in the normal relationship between tubules and their vascular supply. The marked distortion of anatomical relationships in the diseased kidney is well known, and the likelihood that water movement is markedly altered could well explain some of the findings. This would be particularly the case if nephrons with long loops of Henle were involved out of proportion to short loop nephrons.
SUMMARY STATEMENT
In the preceding discussion we have attempted to characterize the pathophysiology of disorders of urine concentration and dilution. Clearly, there are areas in which our knowledge of the mechanisms involved are incomplete and in which further clarification is needed. Some subjects we have purposely dissected in more detail than others. Concerning sickle cell hemoglobinopathies, we feel that these clinical entities provide a model to which the latest theoretical analyses of the countercurrent system may be applied. Other clinical entities, such as drug-induced nephrogenic diabetes insipidus, may not continue to be observed clinically, through avoidance of their lise. Their use in experimental models, however, may provide further insight into the molecular mechanisms involved in one of the kidney's most important functions.
REFERENCES
1.� Seldin, D.W. Eknoyan, G., Suki, W.N., and Rector, F.C., Jr.: Localization of diuretic aCLion from the pattern of water and electrolyte excretion. Ann NY Acad Sci, 139:328, 1966,
2.� Berliner, R.vV. and Bennett, C.M.: Concentration of urine in the mammalian kidney. Am J iVIed, 42:777, 1967.
3. Wirz, H. and Dirix, R.: Urinary concen
tration and dilution. In Orloff, J. and Berliner, R.W. (Eels,): Section 8, Renal Physiology. Washington, American Physiological Society, 1973.
4.� Eknoyan, G" Suki, W.N., Rector, F.C., Jr., and Seldin, D.W.: Functional char· acteristics of the diluting segment of the dog nephron anel the effect of extracellular volume expansion on its reabsorptive capacity. J C lin Invest, 46:1178, 1967.
5.� Stein, R.M., Abramson, R.G., Kahn, T., and Levitt, M.F,: Effects of hypotonic saline loading in hydrated dog: Evidence for a saline-induced limit on distal tubular sodium transport. J Clin Invest, 46:1205, 1967.
6.� Rosin, J.M., Katz, M.A., Rector, F,e., Jr., and Seldin, D.W.: Acetazolamide in studying sodium reabsorption in diluting segment. Am J Physiol, 219:1731, 1970.
7.� ·Wallin, J.D., Barratt, L.J., Rector, F,C., Jr., and Seldin, D.W.: The influence of flow rate and chloride delivery on TOH20 formation in tile rat. Kidney Int, 3:282, 1973.
8.� l\'!artinez-Maldonaclo, M., Eknoyan, G., and Suki, W.N.: Influence of volume expansion on renal diluting capacity in the rat. Clin Sci l'dol 1\![ed, 46:331, 197<1.
9.� Danovitch, G.lVI., Schmidt, R. Wm., and Bricker, N.S.: On tile apparent inhibition of NaCI reabsorption in the diluting segments of the nepllron by ECF volume expansion. Clin Res, 22:522a, 1974.
10.� Rocha, AS. and Kokko, J.P.: Sodium chloride and water transport in the medullary thick ascending limb of Henle: Evidence for aCLive chloride transport. ] CUn Invest, 52:612, 1973.
11.� Imai, M. and Kokko, J.P.: Sodium chloride, urea, and water transport in the thin ascending limb of Henle. J Clin Invest, 53:393, 1974.
12. Tisher,� C.C.: Relationship between rena] sLmcture and concentrating ability in the Rhesus monkey. Am ] Physiol,

1019 Pathophysiology of Clinical Disorders of Urine
220:1100,1971.
13.� Tisher, C.C., Schrier, R.W., and McNeil, J.S.: Nature of urine-concentrating mechanism in the Macaque monkey. Am J Physiol, 223:1128, 1972.
14. Lief, P.D., Sullivan,� A., and Goldberg, M.: Physiological contributions of thin and thick loops of Henle to the renal concentrating mechanism, (abstr.). J Glin Invest, 48:52a, 1969.
15. Martinez·Maldonado,� M., Eknoyan, G., and Suki, W.N.: Functional importance of thin limbs of Henle's loop in urine concentration and dilution. In Book of Abstracts, Mexico City, Vth International Congress of Nephrology, Oct. 8-13, 1972, p. 80.
16. Stephenson, J.L.:� Concentration of urine in a central core model of the renal counterflow system. Kidney Inl, 2:85, 1972
17.� Stewart, J. and Valtin, H.: Computer simulation of osmotic gradient without active transport in renal inner medulla. Kidney Int, 2:264, 1972.
18.� Kokko, J.P. and Rector, F.e., Jr.: Countercurrent mUltiplication system without active transport in inner medulla. Kidney Int, 2:214, 1972.
19.� Goldberg, M., McCurdy, D.K., and Ramirez, M.A.: Differences between saline and mannitol diuresis in hydropenic man. J Glin Invest, 44:182, 1965.
20. Jamison, R.L., Buel'kert,� ]., and Lacy, F.: A micropuncture study of collecting tubule function in rats with hereditary diabetes insipidus. J Glin Invest, 50: 2444, 1971.
21. Burg, M.B.� and Green, N.: Function of the thick ascending limb of Henle's loop. Am] Physiol, 224:659, 1973.
22.� Burg, M.B, and Green, N,: Effect of diuretics on the thick ascending limb of Henle's loop (abstr). J Glin Invest, 52: 15a, 1973.
23.� Martinez-Maldonado, M., Allen, J., Eknoyan, G., Suki, VV., and Schwartz, A.: Renal concentrating mechanism: Possible role for sodium-potassium activated adenosine triphosphatase, Science,
165 :807, 1969. 24, Hendler, E.D" Torretti, J, and Epstein,
F.R.: The distribution of sodium-potassium-activated adenosine triphosphatase in medulla and cortex of the kidney. J Clin Invest, 50:1329, 1971.
25, Schmidt, U, and Duback, U.C.: Activity of (Na+K+)- stimulated adenosintriphosphatase in the rat nephron. Pfluegers Al'eh, 306:219, 1969.
26.� Cohen, S.L, Fitzgerald, M.G., Fourman, P., Griffiths, W.J., and De Wardener, H,E.: Polyuria in hyperparathyroidism. Q J Med, 26:'123, 1957.
27. Epstein,� F.R., Beck, D., Carone, F.A., Levitin, H., and :Manitius, A.: CLlanges in renal-concen trating ability procluced by parathyroid extract. J Clin Invest, 38:1214, 1959.
28.� Gill, J.R., Jr. and Bartter, F.C.: On the impaimlent of renal,concentrating ability in prolonged hypercalcaemia and hypercalciuria in man. J Glin Invest, 40:716, 1961.
29. Suki,� W.N., Eknoyan, G., Rector, F.e., Jr., and Seldin, D.W.: The renal diluting and concentrating mechanism in hypercalcemia. Nephl'on, 6:50, 1969.
30. Epstein,� F.R.: Calcium and the kidney. Am J iHed, 45:700, 1968.
31.� j\'[anitius, A, Levitin, H., Beck, D., and Epstein, F.H,: On the mechanism of impairment of renal-concentrating ability in hypercalcaemia. I Clin Invest, 39: 693, 1960.
32. Eigler,� ].O.e., Salassa, R.M., Balm, R.C., and Owen, C.A., Jr.: Renal distribution of sodium in potassium-depleted and vitamin D-intoxicated rats, Am J Physiol, 202:1 I 15, 1962.
33.� Porter, R.\i\T. and Wells, C.H.: Urinaryconcentrating ability changes and associated renal tissue sodium concentra· tion changes induced by calcium excess. Tex Rep Bioi Meel, 22:165,1964.
34.� Guignard, J-P., Jones, N.F., and Barra. clough, IVLA.: Effect of brief h ypercalcaemia on free-water reabsorption during solute diuresis: Evidence for im· pairment of sodium transport in I-len

1020 Pathophysiology of the Kidney
Ie's loop. Clin Sci, 39:337, 1970. 35.� Curran, P.F., Herrera, F.C., and Flanigan,
W.J.: The effect of Ca and antidiuretic hormone on Na transport across frog skin. II. Sites and mechanisms of action. I Gen Physiol, 46:1011, 1963.
36.� Peterson, M.J. and Edelman, 1.S.: Calcium inhibition of the action of vasopressin on the urinary bladder of the toad. I Clin limest, 43:583, 1964.
37.� Guttman, Y. and Gottschalk, C.W.: Microinjection study of the effect of calcium on sodium transport in the rat kidney. 1srJ ivIed Sci, 2:2'13,1966.
38.� Fulgratf, G. and Heidenreich, 0.: Mikropunktionsuntersuchungen uber die Wirking von Calciumionen auf die Resorptionskapazitat und auf die prozentuale resorption im proxima]en Konvulut von Ratten, Arch Phar Exp Pat/wi, 258: '140,1967.
39.� Di Bona, G.: EFfect of hypercalcemia on renal tubular sodium handling in the rat. Am] Physiol, 220:49, 1971.
40.� Epstein, F.B. and Whittam, R.: The mode of action of inhibition by calcium of cell-membrane adenosine-triphosphatase activity. Biochem I, 99:232, 1966.
41.� Martinez-Maldonado, M., Yium, J.J., Suki, W.N., and Eknoyan, G.: Renal complications in multiple myeloma: Pathophysiology and some aspects of clinical management. ] Chron Dis, 24:221, 1971.
42.� Heptinstall, R.H.: Pathology of the kidney. London, Churchill, 1966.
43.� ReIman, AS. and Schwartz, W.B.: The nephropathy of potassium depletion. A clinical and pathological entity. N Engl I Med, 225:195,1956.
44.� ReIman, AS. and Schwartz, W.B.: The kidney in potassium depletion. Am I iVIed, 24:76'l, 1958.
45.� Manitius, A., Levitin, H., Beck, D. and Epstein, F.H.: On the mechanism of impairment of renal-concentrating ability in potassium deficiency. I Clin Invest, 39:684, 1960.
46. Holliday,� M.A. and Egan, T.J.: Changes in GFR and CH20 before and after
repair of K deficiency in rats. Am I Physiol, 202:773, 1962.
47.� Gottschalk, C.W., Mylle, lVr., Jones, N.F., Winters, R.W., and Welt, G.G.: Osmolality of renal tubular fluids in potassium-depleted rodents. Clin Sci, 29:249, 1965.
48.� Jones, N.F., ]\{ylle, M., and Gottschalk, C.VV.: Renal tubular microinjection studies in normal and potassium-depleted rats. Clin Sci, 29:261, 1965.
49.� Brunner, F.P., Rector, F.C., and Seldin, D.V\'.: The mechanism of the urinaryconcentrating defect in potassium-deficient rats. Pfluegers Arch, 290:202, 1966.
50.� Eknoyan, G., Martinez-Maldonado, M., Suki, W.N., and Richie, Y.: Renal diluting capacity in the hypokalaemic rat. A m I Physiol, 219 :933, 1970.
51.� Kunau, R.T.: Function of ascending loop of Henle in the potassium-deficient dog. Am ] Physiol, 219:1071, 1970.
52.� Bennett, C.M.: Urine concentration and dilution in hypokalemic and hypercalcemic dogs. I Clin Invest, 49:1447, 1970.
53.� Barraclough, M.A, Guignard, j-P., and Jones, N.F.: Urine concentration during solute diuresis in potassium-depleted rabbits. Evidence for a defect in tubular sodium transport. I Physiol, 212:763, 1971.
54.� 'Weiner, NUN., Sauer, L.A, Tonetti, J., and Epstein, F.H.: Renal mitochondrial enzymes in potassium depletion. Am I Physiol, 221:613, 1971.
55.� Pawlson, L.G., Taylor. A., Mintz, D.H., Field, lB., and Davis, B.B.: Effect of vasopressin on renal cyclic AMP generation in potassium deficiency and patients with sickle hemoglobin. Metabolism, 19:694, 1970.
56.� Earley, L.E. and Freidler, R.i\'L: Studies on the mechanism of natriuresis accompanying increased renal blood flow and its role in the renal response to extracellular volume expansion. J Clin Invest, 44:1857, 1965.
57.� Davis, B.B., Walter, lVL]., and Murdaugh, H.V.: The mechanism of the increase

1021 Pathophysiology of Clinical Disorders of Urine
in sodium excretion following dopamine infusion. Proc Soc Ext) Bioi .Mal, 129:210, 1968.
58.� Martinez-Maldonado, M., Tsaparas, N., Eknoyan, G., and Suki, W.N.: Renal actions of prostag"1andin.,: Comparison with acetylcholine and volume expansion. Am J Physiol, 222:1l47, 1972.
59.� Kannegiesser, H. and Lee, J.B.: Role of outer renal medullary metabolism in the concentrating defect of K depletion. Am J Physiol, 220:1701, 1971.
60.� Brenner, n.M. (Cllairman): Renal handling of sodium. Symposium. American Physiological Society. Feel Pl'OC, 33 :13, 197'1.
61.� Papper, S., Belsky, rL., and Bliefer, K.: The response to the administration of an isotonic sodium chloride-lactate solution in patients with essential hypertension. J Clin Invest, 39 :876, 1960.
62.� Birchall, R., Tuthill, S.W., Jacobs, 'N.S., Trautman, W.]., Jr., and Finley, T.: Renal excretion of water, sodium and chloride. Comparison of the response of hypertensive patients with those of normal subjects, patients with specific adrenal or pituitary defects, and a normal subject primed with various hormones. Circulation, 7:258, 1953.
63.� Hollander, W. and Judson, W.E.: Electrolyte and water excretion in arterial hypertension. 1. Studies in nonmedicallytreated subjects with essential hypertension. ] Clin Invest, 36:1460, 1957.
64.� Hollander, W. and Judson, 'V.E.: Electrolyte and water excretion in arterial hypertension. II. Studies in subjects with essential hypertension after antihypertensive drug treatment. Circulation, 17: 575, 1958.
65.� Raeder, M., Omvic, P., Jr., and Kiil, F.: Effect of acute hypertension on the natriuretic response to saline loading. Am ] Physiol, 226:989, 1974.
66. Vaamonde,� C.A., Sporn, N., Lancestremere, R.G., Belsky, ].L., and Papper, S.: Augmented natriuretic response to acute sodium infusion after blood pressure elevation with metaraminol in
normotensive suhjects. ] Clin Invest, 43: 496,196'1.
67. Earley,� L.Eo and Friedler, R.M.: The ef· fects of combined renal vasodilatation and pressor agents on renal hemody. namics and the tubular reabsorption of sodium. J Clin Invest, 45:5'12, 1966.
68. Earley, L.E.,� Martino, rA., and Friedler, R.J\!!.: Factors affecting sodium reabsorption by the proximal tubule as determined during blockade o[ distal so(Hum reabsorption. ] Clin Invest, 45: 1668,1966.
69.� Hebert, C.S., Martinez-Maldonado, r.iI., Eknoyan, G., and Suki, W.N.: The relation of bicarbonate to sodium reabsorption in dog kidney. Am ] Physiol, 222:1014, 1972 .
70.� Koch, K.M., Aynedjian, H.S., and Bank, N.: Effect of acute hypertension on sodium reabsorption by the proximal tubule. ] Clin Invest, 47:1696, 1968.
71. Dresser, T.P.,� Lynch, R.E.. Schneider, E. G., and Knox, F.G.: Effect of increases in blood pressure on pressure and reabsorption in the proximal tubule. Am ] Physiol, 220:444, 1971.
72. Stumpe, K.O., Lowitz, H·D., and Ochwadt, B.: Function of juxtamedullary neph· rons in normotensive and chronically hypel·tensive rats. Pfluegers Arch, 313: 13, 1969.
73. Stumpe, lCO., Lowitz, H-D., and Ochwaldt, B.: Fluid reabsorption in Henle's loop and urinary excretion of sodium and water in normal rats and rats with chronic hypertension. ] Clin Invest, 49: 1200, 1970.
74.� Daugharty, T.M., Belleau, L.J., Martino, J.A., and Earley, L.E.: Interrelationship of physical factors af-fecting sodium reabsorption in the dog. Am ] Physiol, 214:1442,1968.
75. Navar, L.G.: Distal� nephron diluting seg· men t responses to altered arterial pressure and solute loading. Am ] Physiol, 222 :945, 1972.
76. Bank, N., Aynecljian, H.S., Bansal, V.K., and Goldman, D.M.: Effect of acute hypertension on sodium transport by

1022 Pathophysiology of the Kidney
the distal nephron. Am I Physiol, 219: 275,1970.
77.� Falchuk, K.H. and Berliner, R.vV.: Hydrostatic pressures in peri tubular capillaries and tubules in the rat kidney. Am I Physiol, 220:1422, 1971.
78.� Falchuck, K.H., Brenner, B,M" Tadokoro, M., and Berliner, R.W.: Oncotic and hydrostatic pressures in peri tubular capillaries and fIuid reabsorption by proximal tubules. Am .T Physiol, 220: 1427, 1971.
79.� Buckalew, V.M., Jr., Puschett, j.B., Kintzel, lE., and Goldberg, M.: Mechanism of exaggerated natriuresis in hypertensive man: Impaired sodium transport in the loop of Henle. .J Clin Invest, 48:1007, 1969.
80.� Duggan, D.E. and Noll, R.M.: Effects of ethacrynic acid and cardiac glycosides upon a membrane adenosinetriphosphatase of renal cortex. Arch Biochem Biophys, 109:388, 1965.
81.� Schmidt, U. and Dubach, V.C.: The behavior of Na+-I<!- activated adenosine triphospllatase in various structures of the rat nephron after furosemide application. Nephmn, 7:417, 1970.
82.� Landon, E.]. and Forte, L.R.: Cellular mechanisms in renal pharmacology. Ann Rev Pharmacol, 11:171, 1971.
83. l'vlartinez-rvralcJonado,� ]\if., Allen, lC., Inagaki, G, Tsaparas, N., and Schwartz, A.: Renal sodium-potassium-activated adenosine tripllOsphatase and sodium reabsorption. J Clin Invest, 51 :2544" 1972.
8'1.� Torretli, j., Hendler, E., Weinstein, E., Longnecker, R.E., and Epstein, F.H.: Functional significance of Na+-K'-ATPase in the kidney. Effects of ouabain inhibition. Am J l'hysiol, 222 :1398, 1972.
85. Schmidt,� U. and Dubach, D.C.: Na+-K+· stimulated adenosine-triphosphatase: intracellular localization within the proximal tubule of the rat nephron. Pfluege1'S ATCh, 330:265, 1971.
86.� Suki, W.N., Eknoyan, G., and MartinezMaldonado, M.: Tubular sites and mechanisms of diuretic action. Ann
Rev Phal'macol, 13:91, 1973. 87.� rvrartinez-Maldonado, r"I.: Electrolyte dis
turbances resulting from diuretic therapy. Tex Med, 69:83, 1973.
88.� :Martinez-Maldonado, M., Eknoyan, G., and Suki, vV.N.: Diuretics in nonedematous states: Physiological basis for the clinical use. Arch Intern iVIed, 131: 797, 1973.
89. Levinsky, N.G., Davidson, D.G.,� and Berliner, R.W.: Effects of reduced glomerular filtration on urine concentration in the presence of an tidiuretic hormone. J Clin Invest, 38:730, 1959.
90.� Berliner, R.W. and Davidson, D.G.: Production of hypertonic urine in the absence of pituitary antidiuretic hormone. J Clin Invest, 36:1'116, 1957.
91. Grausz,� R., Lieberman, R., and Earley, L.E.: Effect of plasma albumin on sodium reabsorption in patients with nephrotic syndrome. Kidney lnt, 1 :47, 1972.
92.� Chaimovitz, C., Szylman, P., Alroy, G., and Better, 0.5.: Mechanism of increased renal tubular sodium reabsorption in cinhosis. Am ] Aied, 52:198, 1972.
93.� Levinsky, N.G.: Nonalclosterone influences on renal sodium transport. Ann NY Acad Sci, 139:295, 1966.
94. Cirksena,� W.J, Dirks, ].R., and Berliner, R.W.: Effect of thoracic cava obstruction on response of proximal tubule sodium reabsorption to saline infusion. ] Clin Invest, 45:179, 1966.
95. Kaloyanides,� G.]., Cacciaguida, R.]., Pablo, N.C., and Porush, ].G.: Increased sodium reabsorption in the proximal and distal tubule of caval dogs. J Clin Invest, 48:1543, 1969.
96.� Auld, R.B., Alexander, E.A., and Levinsky, N .G.: Proximal tubular function in clogs with thoracic caval constriction. J Clin Invest, 50:2150, 1971.
97.� Goldsmith, C., Beasley, H.K., Whalley, P.]., Rector, F.C., Jr., and Seldin, D.W.: The effect of salt deprivation on the urinary-concentrating mechanism in the dog. J Glin Invest, 40:2043, 1961.
98. Stein, R.M., Levitt, B., Goldstein, "M.H.,

Pathophysiology of Clinical Disonlen of Urine� 1023
Porush, IG., Eisner, C.M., and Levitt, lVI.F.: The effect of salt restriction on the renal-concentrating operation in normal, hyclropenic man. ] Clin Invest, 41 :2101, 1962.
99. Khoyi,� M.A., Djahanguiri, B., and Babaknia, A.: Electrolyte, water and urea content of dog kidney in acute salt depletion. Isr J Med Sci, 6:351, 1970.
100.� Corcoran, A.C. and Page, LH.: Specific renal functions in hypothyroidism and myxedema; effects of treatment. J Clin En docTino I, 7:801, 1947.
101. Yount,� E. and Little, IN.: Renal clearance in patients with myxedema. J Clin Endacrinal, 15:343, 1955.
102. Crispell,� K.R., Parson, W., and Sprinkle, P.: A cortisone-resistant abnormality in the diuretic response to injected water in primary myxedema. J Clin Endacrinol, 14:640, 1954.
103.� BIeHer, K.H., Belsky, JL., Saxon, L., and Papper, S.: The diuretic response to administered water in patients witll primary myxedema. J CUn Endocrinol, 20:409, 1960.
104·. Vogt, ].H.: Impaired water excretion capacity in primary myxedema improved by corticosteroids, corticotrophin, and thyroid substitution. Acta Endocrinol (Kbh), 35:277, 1960.
105. Goldberg,� M. and Rcivich, M.: Studies on the mechanism of hyponatremia and impaired water excretion in myxedema. Ann Intern Med, 56:120, 1962.
106. Vaamonde,� G.A., Oster, J.R., Lohavichan, C., Carroll, ICE., Jr., Sebastianelli, iVL J., and Papper, S.: Renal response to
sodium restriction in myxedema. PTOC
Soc Exp Bioi i\1ed, 146:936, 1974. 107.� Holmes, E.W., Jr. and DiSca1a, V.A.:
Studies on the exaggerated natriuretic response to a saline infusion in the hypothyroid rat. J Clin Invest, 49:1224, 1970.
108. Katz, A.I.� and Lindheimer, M.D.: Renal sodium- and potassium-activated adenosine triphosphatase and sodium reabsorption in the hypothyroid rat. J Clin Invest, 52:796, 1973.
L09. DiSca1a, V.A. and Kinney, M.J.: Effects of myxedema on the renal diluting and cOIlcentrating mechanism. Am J lded, 50:325, 1971.
llO. De Rubertis, F.R., Jr., :rvIichelis, i'vLF., Bloom, M.E., j\'fintz, D.H., Field, J.B., and Davis, B.B.: Impaired water excretion in myxedema. Ann J Med, 51 :4:1, 1971.
11 I. Chinitz, A. and Turner, l".L.: The association of primary hypothyroidism and inappropriate secretion of the antidiuretic hormone. Arch Intern AJerl, 116: 871, 1965.
112.� Pettinger, "'l.A., Talner, L., and Ferris, T.F.: Inappropriate secretion of antidiuretic hormone due to myxedema. N Engl .T kled, 272:362, 1965.
113. Wesson,� L.G., Jr.: Hormonal inflUEnCES on renal function. Ann Rev iVied, 12: 77, 1961.
114. l\'1ichael,� U.F., Barenberg, R.L., Chavez, R., Vaamonde, GA., ancI Papper, S.: Renal handling of sodium and water in the hypothyroid rat. J Clin Invest, 51 :1405, 1972.
115.� Emmanouel, D.S., Lindheimer, M.D., and Katz, A.I.: Mechanism of impaired water excretion in the hypothyroid rat. J CUn Invest, 54:926, 1974.
116. Katz, A.I.� and Epstein, F.H.: The role of sodium-potassium-activated adenosine triphosphatase in the reabsorption of sodium by the kidney. J Clin Invest, 46:1999, 1967.
117.� Reville, P. and Stephan, F.: Determination du gradient intrarenta1 de concentration de l'uree et du sodium chel des rats hypothyroidicns ct des rats surrenalectomises. CR S()r: Biol (Paris), 161:17"1, 1967.
118. Reville,� P. and Stephan, Y.: Etude comparative de 1a composition cLu plasma de rats hypothyroidiens et de rats surrenalectomises. CR Soc Bioi (Paris), 162:754,1968.
119. Schlitt,� L. and Keitel, H.G.: Pathogenesis of hyposthenuria in persons with sickle cell anemia or the sickle cell trait. Pediatrics, 26:249, 1960.
,I�

Pathophysiology of the Kidney
120. Statius Van Eps, L.W., Schouten, H., Tel' Arch, 306:103, 1969. Haar Romeny-,Vachter, C.c., and La Portc-Wijsman, L.W.: The relation between age and renal concentrating capacity in sickle cell disease and hemoglobin C disease. Clin Chim Aela, 27: 501, 1970.
121. Keitel,� H.G., Thompson, D., and llano, H.A.: Hyposthenuria in sickle cell anemia; a reversible renal defect. I Clin Invesl, 35 :998, 1956.
122.� "Vhitten, C.F. and Younes, AA.: A comparative study of renal-concentrating ability in chilclren with sickle cell anemia and in normal children. I Lab Clin Mecl, 55:400, ]960.
J23. Statius Van Eps, L.W., Schouten, H., La Porte-Wijsman, L.W., and Struyker Houdier, A.M.: The influence of red blood cell transfusions on the hyposthenuria and renal hemodynamics of sickle cell anemia. Clin Chim Acla, 17: 4'19, 1967.
J24.� Hatch, F.E., Culbertson, ].VV., and Diggs, L.VV.: Nature of the renal-concentrating defect in sickle cell disease. I CUn Invest, 46:336, J967.
125.� Levitt, IvLF., Hauser, A. D., Levy, flT.S., and Polimeros, D.: The renal-concentrating defect in sickle cell disease. Am I Med, 29:611, 1960.
126. Lindsay,� J., Jr., Meshel, ].C., and Patterson, R.H.: The cardiovascular manifestations of sickle cell disease. Arch Intern J1iIed, 133:6'13, 1974.
J27. KJug,� 1'_1'., Lessin, L.S., and Radice, P.: Rheological aspects of sickle cell disease. Arch Intern ivIed, 133:577, 197'1.
128. Statius� Van Eps, L.'V., Pinedo-Veels, C., De Vries, G.H., and De Koning, J.: Nature of concentrating defect in sickle cell nephropathy. Lancet, 1:450, 1970.
129.� Sclmermann, j., Valtin, H., Thurau, K., Nagel, W., Horster, lvI., Fischbach, H., Wahl, M., and Liebau, G.: Micropuncture studies on the influence of antidiuretic hormone on tubular fluid reabsorption in rats with hereditary hypothalamic diabetes insipidus. Pfiuegen
130. Jamison, R.L., Buerkert,� ]., and Lacy, F.: .A micropuncture study or collecting tubule function in rats with hereditary diabetes insipidus. I CUn Invest, 50: 2tJ44, 1971.
131.� Herbin, L.F., Ceriani, R., and Gotta, H.: Sickelemia: Estudio sobre la function renal y eritrocinesis. PTensa iVIed ATg, 48:1526,1961.
132. Perillie,� P.E. and Epstein. F.H.: Sickling phenomenon produced by hypertonic solutions; A possible explanation for the hyposthenuria of sicklemia. I Clin Invest, 42:570, 1963.
133. Parrish,� AE., Watt, M.F., Bowman, W.K., and Kramer, N.C.: The effect of increased plasma viscosity on renal function. Clin Res, 12:71, 1964.
134. Carone, F.A.� and Epstein, F.B.: Nephrogenic diabetes insipidus caused by amyloid disease. Am .r iVIed, 29:539, 1960.
135. Kailz,� A.L.: Urinary-concentrating ability in pregnant women willi asymptomatic bacteriuria. I Clin Invest, 40:1331, 1961.
136.� Norden, C.W. and Tuttle, E.P.: Impairment of urinary-concentrating ability in pregnant women with asymptomatic bacteriuria. In Kass. E.H. (Eel.): PTOgress In PyelonetJhrilis. Philadelphia, Davis, 1965, p. 73.
137. Kaitz,� .A.L. and London, A.1Vr.: Osmolar urinary-concentrating ability and pyelonephritis in hospitalized patients. Am .T Med Sci, 248:7, 19M.
138. Williams,� G.L., Campbell, H., and Davies, K.J.: Urinary-concentrating ability in women with asymptomatic bacteriuria in pregnancy. Br Med I, 3:212, 1969.
139. Elder,� H.A. and Rass, E.H.: Renal function in bacteriuria of pregnancy: its relationship to prematurity, acute pyelonephritis and excessive weight gain. Br iVIed I, 3:81, 1969.
1'10.� Beck, D., Freedman, L.R., Levitin, H., Ferris, T.F., and Epstein, F.H.: Effect of experimental pyelonephritis on the renal-concentrating ability of the rat.

1025 PalhojJhysiolagy of Clinical Disorders of Urine
Yale J Biol ivIed, 34:52, 1961. HI. Kaye, D. and Rocha, H.: Urinary-concen
trating ability in early experimental pyelonephritis. ] Clin ImJest, 49:JI127, 1970.
1'12. Ronald, A.R., Culler, R.E., and Turck, :M.: Effect of bacteriuria on renal-concentrating mechanisms. Ann Intern Med, iO:723, 1969.
JL13. Clark, R., Ronald, A.R., Cutler, R.E., and Turck, M.: The correlation between site of infection and maximal concentrating ability in bacteriuria. J Infect Dis, 120:47, 1969.
J'H. Lathem, W.: The urinary excretion of sodium and potassium during the pyrogenic reaction in man. ] Clin Invest, 35:947,1956.
145.� Gonick, H.C., Goldberg, G., Rubini, 1\1LE., and Guze, L.B.: Functional abnormalities in experimental pyelonephritis. 1. Studies of concentrating ability. Nephron, 2:193, 1965.
146. Zinner,� S.H. and Rass, E.H.: Long-term (10 to 14 years) follow-up of bacteriuria of pregnancy. N Engl J Med, 285:820, 1971.
1'17.� Pathak, U.N., Tang, K., Williams, L.L., and Stuart, K.L.: Bacteriuria of pregnancy: Results of treatment. J Infect Dis, 120:91, 1969.
148. Suki,� \iV.N., Axelrad, S., Eknoyall, G., and and Martinez-Maldonado, M.: On the impaired urine concentration in patients with acute pyelonephritis. Clin Res, 18:94,1970.
149. Sutherland,� E.W., Robison, G.A., and Butcher, R.W.: Some aspects of the biological role of adenosine !I',5'-monophosphate (cyclic AMP). Circulation, 37:270,1968.
ISO. ;\Iartinez-Maldonado, M. and Terrell, J.: Lithium-induced nephrogenic diabetes insipidus and glucose intolerance. Arch Intern iVIed, 132:881, 1973.
] 51. AngTist,� n.M., Gershon, S., Levitan, S.]., and Blumberg, A.G.: Lithium-induced diabetes insipidus-like syndrome. C01111J1'
PSJ'chiatry, 11 :1'11, 1970. 152. Ramsey, T.A., Mendels, J., Stokes, j.W.,
and Fitzgerald, R.C.: Lithium carbonate and kidney function. A failure in renal-concentrating ability. JAlIUI, 219;1446, 1972.
] 53. Martinez-1VIaldonado, M., Stavrolllaki-Tsapara, A., Tsaparas, N., Suki, W.N. and Eknoyan, G.: Renal effects of lithium administration in rats: 1. Alterations in water and electrolyte metabolism and the response to vasopressin and cyclic adenosine monophosphate during prolonged administration. ] Lab Glin iVIed. 86:445, 1975.
154.� Forrest, IN., Jr., Cohen, A.D., Torretti, J., Himmelhoch, J.M., and Epstein, F.R.: On the mechanism oE lithiuminduced diabetes inspidius in man and the rat. J Clin Invest, 53:1115,1974.
155.� Singer, 1., Rotenberg, D., and Puschett, lB.: Lithium-induced nephrogenic diabetes insipidus: in vivo and in vi/TO studies. J Clin Invest, 51 :1081, 1972.
156. Harris,� C.A. and Jenner, F.A.: Some aspects of the inhibition of the action of an tidiuretic hormone by lithium ions in the rat kidney and bladder of the toad BuLa marinus. Br J Pharmacal, 44:223, 1972.
157. Bentley,� P.]. and 'Wasserman, A.: The effect of lithium on the permeability of an epithelial membrane, the toad urinaTY bladder. Biochim Bioj)hys Acllt, 266:285, 1972.
158.� Singer, 1. and Franko, E.A.: Lithium-induced ADH resistance in toad urinary bladder. Kidney Int, }:151, 1973.
159. Castell,� D.O. and Sparks, H.A.: Nephrogenic diabetes insipidus due to demethy1chlortetracycline hydrochloriele. lAMA, 193:237, 1965.
160. Lazar,� P., Kerman, L., and Kanter, A.: Demethylchlortetracycline hydrochloride and nephrogenic diabetes insipidus. Cut. is, 6:881, 1970.
161.� Roth, H., Becker, K.L., Shalhoub, R.J., and Katz, S.: Nephrotoxicity of elemethylchlonetracydil1e hydrochloride. A prospective study. Arch Intern Med, .120:433,1967.
162. Tandhanancl, S., Vichayanrat, A., Nilwa

1026 Pathophysiology of the Kidney
rangkur, S., and Inthuprapa, M.: Polyuria and hypokalemia secondary to nephropathy caused by degraded tetracycline. J iVied Assoc Thai, 55: 179, 1972.
163.� }'rimpter, G.\V., TimpaneJIi, AE., Eisenmenger, J., Stein, H.S., and Ehrlich, L.I.: Reversible "l'anconi syndrome" caused by degraded tetracycline. JAi\fA, 184:111, 1963.
164.� Wilson, D.NI., Perry, H.O., Sams, W.M., and Dousa, T.P.: Selective inhibition of human distal tubular function by Demeclocycline. Curr The?' Res, J5: 73<1, 1973.
165. Simler,� r., and Rotenberg, D.: Demec1ocydine-induced diabetes insipidus: In vivo and in vitro studies. Ann Intern iVIed, 79:679, 1973.
166. Dousa,� T.P. and 'Wilson, D.M.: Tetracyclines: Interference with ADH-responsive cyclic AMP system III human renal medulla (abstr.) Clin Res, 21:75, 1973.
167. Cousins,� 1V1.J. and Mazze, R.I.: Methoxyflurane nephrotoxicity. A study of dose response in man. .TANIA, 25:16)), 1973.
168. Churcllill,� D., Knaack, J., Chirito, E., Barre, P., Cole, C., Muehrcke, R., and Gault, lVI.H.: Persisting renal insufficiency after methoxyflurane anesthesia. Report of two cases and review of literature. Am] iVIed, 56:575, 1974.
169. Barr,� G.A., Cousins, M..J., Mazze, R. 1., Hitt, B.A., and Kosek, J.C.: A comparison of the renal effects and metabolism of enflurane and methoxyflurane in Fischer 34'1 rats. .T Fhar Ext) The?', 188:257, 1974.
170.� Frascino, J.A.: Effects of inorganic fluoride on the renal concentrating mechanism possible nephrotoxicity in man. .T Lab Clin IvIed, 79:192,1972.
171.� Martinez-Maldonado, IV1., Eknoyan, G., and Suki, \N.N.: Importance of aerobic and anaerobic metabolism in renal concentration and dilution. Am J Physiol, 218:1076, 1970.
172.� Handler, .1., Petersen, M., and Orloff, J.: Effect of metabolic inhibitors on the
response of the toad bladder to vasopressin. Am J Ph)'siol, 211 :1175, 1966.
173.� Douglas, .J.B. and Healy, J,K.: Nephrotoxic effects of amphotericin B, including renal tubular acidosis. Am J il'led, 46:154,1969.
17'1.� McCurdy, D.K., Frederic, M., and Elkinton, .J.R.: Renal tubular acidosis due to amphotericin B. N Engl J M.ed, 278: 124, 1968.
175.� McChesney, J.A. and Marquardt, J.F.: Hypokalemic paralysis induced by amphotericin B. JAlvIA, 189:1029, 1964.
176.� Eknoyan, G. and Roberts, A.D.: Nephrotoxicity of amphotericin B: observations on the mechanism of hypokalemia. In Proceedings of the Second lnten'cience Conference on Antimicrobial Agents and Chemothera!)y. Chicago, 1962, p. 497.
177.� Butler, W.T., Bennett, J.E., Alling, D.W., Wert1ake, PT., Utz, J.p., and Hill, G.J.: Nephrotoxicity of amphotericin B: early and late effects in eighty-one patients. Ann Intern M.ed, 61:175,1964.
178.� Andreoli, T. E.: On the anatomy of amphotericin B-cholestero1 pores in lipid bilayer membranes. Kidney Int, 4:337, ]973.
179.� Butler, \V.T. and Cot1ove, E' Increased permeability of human erythrocytes induced by amphotericin B. J Infect Dis, 123:341,1971.
180.� IVlartinez-Maldonado, M., Yium, J.J., Eknoyan, G., and Suki, W.N.: Adult polycystic kidney disease: Studies of the defect in urine concentration. Kidney Int, 2:107,1972.
18!.� Gardner, lCD., J1'.: Evolution of clinical signs in adult-onset cystic disease of the renal medulla. Ann Intern Mecl, 74:47,197!.
182. Kliger,� A.S. and Scheer, R.L.: The early detection of cystic disease of the renal medulla. Am Soc Neph (abstr.): 60, 1972.
183.� Bricker, N.S.: Obstructive nephropathy. In Black, D.A.K. (Ed.): Renal Disease, 2nd eel. Philadelphia, Davis, 1967, p. 404.
184. Earley, L.E.: Extreme polyuria in obstruc

1027 Pathophysiology of Clinical Disorders of Urine
tive uropathy. Report of a case of water-losing nephritis in an infant, with a discussion of pOlyuria. N Engl J j1{erl, 255 :600, ] 956.
185. Bricker, N.S.,� Shwayri, E.L., Rearden, J. B., Kellogg, D., Merrill, J.P., and Holmes, J.H.: An abnormality in renal function resulting from urinary tract obstruction. A In J Med, 23 :554·, J957.
186.� Jaenike, ] .R. and Bray, G.A.: Effects of acute transitory urinary obstruction in the clog. Am ] Physiol, 199:1219, 1960.
187. Kessler,� R.H.: Acute effects of brief ureteral stasis on urinary ancI renal papillary chloride concentration. Am J Physiol, 19.9:12]5, 1960.
188.� Suki, W.N., Guthrie, A.G., I\Iartinez-Ma1. donaclo, M., and Eknoyan, G,: Effects of ureteral pressure elevation on renal hemodynamics and urine concentration. Am .l Physiol, 220:38, 1971.
189. Kiil,� F. and Auk1and, 1<..: Renal concen tration mechanism ancI hemodynamics at increased ureteral pressure during os· motic and saline diuresis. Scand J Clin Lab Invest, 13 :276, 1961.
190. Vaughan,� E.n., .Tr., Sorenson, E.J., and Gillenwater, J.y,: The renal hemodynamic response to chronic unilateral complete ureteral occlusion. Invest· Urol, 8:78, 1970,
191. Shimamura,� T.: Effects of ureteral obstruction on the structure and function of the renal medulla, Invest Uml) 9:48'1, 1972,
192. Selkurt,� E.E.: Effect of ureteral blockade on renal blood How and urinary-concentrating ability. Am J Ph'ysiol, 205: 286, 1963.
193. Scherrnann,� .T. and Thurau, K.: IVlikropunktionsversuche zum Verhalten del' PAH-l{onzentration im Vasa recta-Blut del' Golhamsterniere. Arch Ges Physiol, 283:171,1965.
194. Carlson, E.L.� and Sparks, H.V.: Intrarenal distribu tion of blood flow during elevation of ureteral pressure in dogs. Circulation Res) 26:601, 1970.
195, Finkle, A.L., Karg, S.J.,� and Smith, D.R.: Parameters of renal functional capacity
in reversible hydroureteronephrosis in dogs. III. Effects of one hour of uni· lateral ureteral occlusion upon UV, cOsm, TOH20, 0Na, 0PAB, FF, and RBFK1• of intact kidneys. Invest Uml, 7:215, 1969.
196. Suki,� vV,N" l'olanyi, M,L., Ostrowski, D"
'l'V"alker, F.E., Martinez-IVlalclonac!o, M" and Eknoyan, G,: Measurement of intrarenal transit time and hemoglobin saturation using .fiberoptics. ] APi;l Physiol) 29:123, 1970.
197. Shimamura,� T., Kissane, J.M., and Gyorkey, F.: Experimental hydronephrosis. Nephron dissection and electron microscopy of the kidney following obstruc· tion of the ureter and in recovery from obstruction. Lab Invest) 15:629, ] 966.
198. Rao, N,R.� and Heptinstall, R.H.: Experimental hydronephrosis. A microangiographic study. Invest Urol, 6:183, 1968.
199. Fulop,� ]VL and Brazeau, P.: Increased ureteral back-pressure enhances renal tubular sodium reabsorption. .l CUn Invest, 49:2315, 1970,
200. Roussak,� N.]. and Oleesky, S.: iA,Tater-Iosiug nephritis: a syndrome simulating diabetes insipidus. Q J Nfed, 23:147, 1954.
201. i,Vinberg,� ].: Renal function in water-losing syndrome clue to lower urinary tract obstruction before and after treatment. Acta Paediatl' (Uppsala), '18: 149, 1959.
202.� Dorhout Mees, E.].: Reversible water-losing state, caused by incomplete ureteric obstruction. Acta 11,11ed Scand, J 68:193, 1960.
203. Berlyne,� G.M.: Distal tubular function in chronic hydronephrosis. Q J iVIed, 30: 339, 1961.
204. Suki,� W., Eknoyan, G., Rector, F.C., Jr" and Seldin, D,"V.: Patterns of nephron perfusion in acute and chronic hydronephrosis. J Glin Invest, 45:122, 1966.
205. Eknoyan,� G., Suki, W.N., 1'dartinez-Ma1· donado, M., and Anhalt, :M.: Chronic hydronephrosis: Observations on the mechanism of the defect in urine concentration. Proc Soc Ext; Biol lHed)

1028 Pathophysiology of the Kidney
173:634, 1970. 206.� Steele, T.W., Gyory, A.Z., and Edwards,
K.D.G.: Renal function in analgesic nephropathy. Br Mecl ], 2:213, 1969.
207.� Gault, M.H., Rudwal, T.G" Engles, W,D., and Dossetor, lB.: Syndrome associated with the abuse of analgesics, A review. Ann Intern Med, 68:906, 1968.
208.� Bluemle, LW., Jr. and Goldberg, "M,: Renal accumulation of salicylate and phenacetin: possible mechanisms in the nephropathy of analgesic abuse. ] Clin invest, 47:2507, 1968.
209.� Gault, M.H., Blennerhassett, J, and Muehrcke, R.C,: Analgesic nephropathy. A clinicopathologic study using electron micros'copy. Am ] iVIed, 51 :740, 1971.
210.� j\fartinez-Maldonado, M. and Ramirez de Arellano, G.A: Reqal involvement in malignant lymphomas: A survey of 49 cases. ] Ural, 95:485, 1966.
211.� Steele, T.H., Presant, C'A' and Serpick, AA.: A reversible concentrating defect in predominantly unilateral renal Hodgkin's disease. Am ] iVIed, 48:375, 1970.
212,� Kleeman, C.R., Hewitt, W.L., and Guze, L.B.: Pyelonephritis. Medicine, 39:3, 1960.
213.� Kleeman, C,R. and Epstein, F.H.: An illustrative case oE chronic pyelonephritis
with persistently hypotonic urine. Am ] ivIed, 23:488, 1957.
21'1. Holliday, M.A., Egan, TJ., Morris, C.R., Jarral1, AS., and Han-ah, JL.: Pitressin-resistant hyposthenuria in chronic renal disease. Am] iVIed, 42:378, 1967.
215.� Tannen, R.L., Regal, E.M., Dunn, M.J., and Schrier, R.vV.: Vasopressin-resistant hyposthenuria in advanced chronic renal disease. N Engl ] iVIed, 280:1135, 1969.
216.� Kahn, T., Mohammad, G., and Stein, R. M.: Alterations in renal tubular sodium and water reabsorption in chronic renal disease in man. Kidney Inl, 2:164, 1972.
217.� Bricker, N.S., Dewey, R.R., Lubowitz, H., Stokes, J., and Kirkensgaard, T.: Observations on the concen trating and diluting mechanisms of the diseased kidney. ] Clin invest, 38:516, 1959.
218.� Scbrier, R.W. and Regal, E.lVL: Influence of aldosterone on sodium, water and potassium metabolism in chronic renal disease. Kidney Int, 1 :156, 1972.
2]9.� Coleman, A.J., Arias, M., Carter, N.W., Rector, F.C., Jr., and Seldin, D.W.: The mechanism oE salt wastage in chronic renal disease. J Clin Invest, <{ 5: 1166, ] 966.