Embed Size (px)
Citation preview

Eur J Haernatol 1987:38:426-432
Key words: acquired BM failure - erythroid function - classification
Pathophysiological classification of acquired bone marrow failure based on quantitative assessment of erythroid function
Mario Cazzola, Gaetano Bergamaschi, Helmut A. Huebers & Clement A. Finch
Department of Internal Medicine and Medical Therapy, University of Pavia, Italy, and University of Washington School of Medicine, Hematolgy Research, Seattle, WA, U.S.A.
Bone marrow failure encompasses a broad spectrum of disorders including aplastic, dysmyelopoietic and myelophtisic anemias. In the present study, these anemias were characterized according to the degree of erythroid proliferation and efficiency of erythropoiesis. Total erythropoietic activity was evaluated in 43 patients by measuring the erythron transferrin uptake (ETU). It averaged 20% of basal (range 3-43%) in 13 patients with severe aplastic anemia, 75% of basal (range 60-103%) in 3 patients with extensive bone marrow infiltration by neoplastic cells, 131 % of basal (range 50-217%) in 16 patients with refractory anemia, and 452% of basal (range 63-720) in 11 patients with idiopathic refractory siderobastic anemia. Respective efficiencies of erythropoiesis were 74% in aplastic anemia, 70% with bone marrow infiltration, 46% in refractory anemia, and 14% in sideroblastic anemia. Based on the ETU, patients could be categorized into absolute marrow failure, relative marrow failure, and adequate erythropoietic response to anemia. This simple determination of proliferating activity of the erythroid marrow can provide useful information on the pathophysiology of marrow failure and a basis for the selection of therapeutic approaches.
Accepted for publication December 1, 1986
CLINICAL BEARING These studies indicate the possibility of evaluating the proliferative activity of the erythroid marrow in patients with acquired bone marrow failure by means of a simple ferrokinetic test which can be routinely carried out in a clinical setting. This estimation can provide useful infor- mation on the pathophysiology of marrow failure and a basis for the selection of therapeutic approaches.
Acquired bone marrow failure encompasses a variety of disorders whose common denomina-
tor is reduced delivery of cells to the circulation plus peripheral cytopenia (1). As far as ery- thropoiesis is concerned, such disorders are usu- ally divided into two major categories (2) . When proliferation of red cell precursors is prevented, it is assumed that the abnormalitie(s) reside in the stem cell compartment. When pro- liferation of red cell precursors still occurs but developing red cells are unable to circulate in the blood, there is a maturational disorder

ERYTHROPOIESIS IN BONE MARROW FAILURE 427
referred to as ineffective erythropoiesis. Various names are employed fo r these disorders, aplas- tic anemia fo r the first (3), and such terms as refractory anemia, sideroblastic anemia, pre- leukemia, and more recently myelodysplastic syndromes for the latter (1, 4). T h e present study was undertaken to evaluate the feasibility of classifying such disorders on the basis of proliferation o f the erythroid cells in the mar- row and efficiency of erythropoiesis.
Material and methods Patients Ferrokinetic studies were performed in a total of 43 patients with acquired bone marrow failure. Experi- mental protocols for these studies were approved by the University of Washington Human Subjects Com- mittee and informed consent was obtained from all subjects. The following diagnostic criteria were adopted in the clinical definition of disorders of bone marrow failure:
(a) Severe aplastic anemia (SAA) (13 patients, aged 9-67). Criteria for the diagnosis of severe aplastic ane- mia included a hypocellular bone marrow on bone marrow biopsy (less than 25% cellularity) and two of the following three: reticulocyte index < 1 , gran- ulocytes < 0.5 x 109/liter and platelets < 20 x lo9/ liter (3).
(b) Bone marrow infiltration (BMI) by malignant cells (3 patients, aged 50-67). 2 patients had massive mar- row infiltration by non-Hodgkin lymphoma cells and the 3rd by lung cancer (microcytoma). In all 3 cases, marrow failure was the presenting problem.
(c) Refractory anemia (RA) (16 patients, aged 27-83). Criteria were an idiopathic acquired anemia character- ized by variable cytopenia of circulating cells and mar- row cellularity greater than 25% with less than 10% ring sideroblasts.
(d) Idiopathic refractory sideroblastic anemia (IRSA) (11 patients, aged 46-86). Diagnostic criteria were the same as for the previous category except that these patients had ring sideroblasts in the bone marrow rang- ing from 30 to 90%.
All patients were studied at clinical onset before any treatment.
Ferrokinetic measurements Details of the measurement of plasma iron turnover have been previously summarized ( 5 ) . In these studies it was stardard practice to inject 59FeS0, (0.2 wg con- taining 2 pCi 59Fe at pH 2) intravenously over a period of 5 min. However, in individuals with transferrin saturation > 70%, radioiron was bound to normal plasma in vitro, and then the tracer saturation was adjusted to that of the patient's own plasma using cold ferrous ammonium sulfate ( 5 ) .
Plasma iron turnover was routinely calculated employing the formula:
PI ( d d 0 PIT (mg/dl whole hlood/day) = X (100 - Hct x 0.9)
TI/Z(min) x 100
Additional calculations, discussed in more detail elsewhere ( 5 , 6 ) , were made to convert the plasma iron turnover to the transferrin-iron complex uptake by the erythron. This involved (i) a correction of the extravascu- lar plasma flux (EVF), (ii) a correction designed to con- vert tissue iron uptake (IU) to tissue transferrin uptake (TU), and (iii) the subtraction of nonerythroid transferrin uptake to leave erythron transferrin uptake (ETU).
EVF (mg/dl whole blood/day) = (100 - Hct x 0.9)
100 = PI (pg/dl) x x 0.0015
IU (mg/dl whole blood/day) = PIT - EVF
TU (+mol/l whole blood/day) = IU (mg/dl whole blood/day) x 10000 200 + 2.2 S
56 200 + 6.4 S
where S is the percent transferrin saturation. The final correction to allow for transferrin-iron
going to nonerythroid receptors was made by subtract- ing the mean normal value of 11 pmol/l whole blood/d (5) from the calculated transferrin uptake:
ETU (pmol/l whole hlood/day) = TU (Fmol/l whole hlood/day) - I1
An estimate of the total efficiency of erythropoiesis was obtained from the patient's ETU and hidher hem- atocrit, each expressed in relation to the normal:
Efficiency of erythropoiesis (fraction of normal) =
normal ETU patient's hematocrit
patient's ETU 45 - "
Plasma iron and transferrin saturation were mea-

428 CAZZOLA ET AL
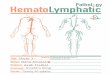
10 I 0.51
0.1 0-0.1 000
S A A BMI R A IRSA
Figure 1. Distribution of ETU values in patients with acquired bone marrow failure. Erythron transferrin uptake is expressed as times the mean normal value of 60 bmol/l whole blood/day, in order to provide a more direct estimate of erythroid hyper- or hypoproliferation. SAA: severe aplastic anemia; BMI: bone marrow infiltration by malignant cells; RA: refractory anemia; IRSA: idiopathic refractory sideroblatic anemia. The shaded area represents the normal range.
sured as described elsewhere (7, 8). Hematocrit was determined by the micromethod. 59Fe activity was determined by gamma counting.
Statistical analysis Statistical analyses were performed using the CLINFO computer system, University of Washington, Seattle, Washington. All results are given as mean * 1 S.D. The significance of the difference between means was tested by the Student’s t test.
Results The overall results are reported in Table 1 and Figure 1 . All patients with severe aplastic anemia had values for ETU below the normal range, from 3 to 43% of basal level. On bone marrow biopsy, 4 of the 13 patients showed islands of intense hemopoiesis (“hot pockets”) within an otherwise empty marrow. 2 of them had the highest values for ETU in this group (23 and 26 ymol/l whole blood/d, respectively), but the remaining 2 showed values overlapping those of subjects without such foci.
The proliferative activity of the erythroid mar- row, as judged by ETU, was in the normal range in the 3 anemic patients with bone marrow infil-
TABLE 1 Hematologic values and ferrokinetic estimates of erythroid function (mean f S.D.)
ETU (bmol/l Efficiency of erythropoiesis
Retics Plasma Transferrin PIT index iron saturation (mg/dl Hct
(070) (070) (wddl) (070) wb/day) wb/day)
Subjects (no.)
Severe aplastic anemia (13) 22 f 6 0.1 f 0.1 249 f 99 8 6 f 13 0.54 f 0.10 12 f 8 0.73 f 0.15
Bone marrow infiltra- tion by malignant cells (3) 22 f 2 0.3 f 0.2 216 + 80 77 & 31 0.87 f 0.27 45 f 14 0.70 f 0.22
Refractory anemia (16) 26 f 7 0.7 f 0.5 147 f 71 58 f 29 1.00 f 0.26 79 f 30 0.46 f 0.21
Idiopathic refractory sideroblastic anemia (11) 26 f 4 0 . O f 0.4 172 f 55 68 f 19 3.00 f 1.15 271 f 121 0.14 f 0.06
Normal subjects (53) 42 f 4 - 1 112 * 43 35 f 1 1 0.71 + 0.17 60 f 13 - 1
ETU values from patient with severe aplastic anemia were significantly lower than those from normal controls (p < 0.001). Those from patients with bone marrow infiltration and refractory anemia did not differ significantly from the normal ones (p < 0.05). ETU values from patients with idiopathic refractory sideroblastic anemia were significantly greater than those from normal controls (p < 0.001).

ERYTHROPOIESIS IN BONE MARROW FAILURE 429
tration by malignant cells, and ranged from 50 to 217% of basal in the 16 patients with refractory anemia. Within this latter group, there was no difference in the degree of erythroid proliferation between the 6 patients showing an excess of 6-20% blasts in the marrow and the remaining 10 patients whose marrow blasts were below the upper normal limit of 5 % (t = 1.4, p > 0.05).
All but 1 patient with idiopathic refractory sideroblastic anemia had values for ETU above 3 times basal. The only exception was a woman whose conventional hematologic parameters were indistinguishable from those of the remaining subjects in this group. Her erythropoietic activity was only 63% of normal and she had a need for frequent blood transfusions. She later evolved into acute non-lymphocytic leukemia.
The efficiency of erythropoiesis could be cal- culated only in those patients who had not been transfused in the 2 months before the study. As shown in Table 1, it was almost normal in patients with aplastic anemia or bone marrow infiltration, showed more variability in patients with refractory anemia, and was very low in patients with idiopathic refractory sideroblastic anemia. There was an inverse relationship between ETU and efficiency of erythropoiesis (r
When the degree of erythroid proliferation, as measured by ETU, was plotted against the hema- tocrit, it was apparent that there was no relation- ship between these parameters for those patients who had values for ETU below 3 times basal. On the contrary, an inverse relationship (r = -0.66, p < 0.05) was found among patients having an erythroid proliferation above 3 times normal.
= -0.93, p < 0.001).
Discussion Marrow dysfunction may involve stem cells, their regulators or some aspects of precursor prolifera- tion and maturation (2), all of these mechanisms resulting in decreased production of formed ele- ments of peripheral blood. Levels of circulating blood cells, while they may determine symptoms and outcome, do not therefore indicate the pathophysiological nature of marrow dysfunc-
tion or what form of therapy should be under- taken.
A number of methods are available for eval- uating physiological defects of the bone marrow and defining the mechanisms of marrow failure (1, 2). Stem cell quantitation provides a unique opportunity to react individual factors with stem cells and thus for determining the cause of stem cell dysfunction (9). However, in vitro factors influencing results are difficult to standardize, and it is hard to determine what proportion of the total marrow is being analyzed. So far, attempts to correlate inhibition of in vitro colony growth with clinical recovery after immunosup- pressive treatment in aplastic anemia have been disappointing, the best results being not suffi- ciently accurate to warrant a decision for or against immunosuppressive therapy (10). Sim- ilarly, reduced erythroid and myeloid colony growth appear to be an early manifestation of abnormal marrow function in myelodysplastic syndromes and do not allow distinguishing sub- sets of patients with clearly different clinical courses (11, 12).
Morphologic evaluation of the marrow by biopsy and aspirate indicates distribution and density of active marrow. It has been recognized, however, that any spot-sampling of an organ as large as the marrow may be misleading, and that the posterior iliac bone cavity may contain an excessive amount of fat (2, 13). Marrow cel- lularity in normal subjects may range from 20 to 80% (14). Most importantly, a recent study has shown a comparable variability in aplastic ane- mia, marrow cellularity ranging from 2 to 40% in severe aplastic anemia, and from 5 to 75% in moderate aplasia (10). Furthermore, it has proved to be of no use in distinguishing between different myelodysplastic syndromes (15).
One way of characterizing disorders of bone marrow failure is the extent to which prolifera- tion of red cells and other elements is impaired and the extent of maturation abnormalities. From a quantitative standpoint, the most useful approach to erythropoiesis is the use of fer- rokinetic techniques (2). The major objections to their use have been: (a) plasma iron turnover,

430 CAZZOLA ET AL
which represents the most simple ferrokinetics measurement, gives a poor description of the erythroid proliferation in conditions of normal or reduced erythropoietic activity (2, 13); (b) ferrokinetic studies more specifically characteriz- ing erythropoiesis require considerable time and effort and are impractical for general clinical usage (1, 16).
The limits of ferrokinetic measurements were mainly due to the difficulties in distinguishing between the iron taken up by the erythron and that going to extravascular circulation or non- erythroid tissues (2) . In addition, the amount of iron taken up by the erythron is affected by the plasma iron and transferrin saturation, this effect being due to the greater iron delivery from diferric as compared to monoferric transferrin ( 5 ) . To overcome these limits, we have developed a modification of the standard measurement of plasma iron turnover in which erythron transfer- rin uptake rather than iron uptake is calculated ( 5 , 6). In a study of 80 patients with various erythroid disorders, it has been shown that the measurement of ETU provides a more direct ferrokinetic evaluation of erythroid activity in anemic states (6). This determination of pro- liferating activity of the erythroid marrow can be performed in a few hours and does not require access to computer facilities.
In this work we have examined the value of ETU in the study of bone marrow failure. Prop- er interpretation of results requires definition of normal behavior of the erythron under basal conditions and the increased erythropoietic re- sponse expected with anemia (2). In the basal state, when oxygen supply is adequate, red cell production is effective and red cell survival is normal, erythron transferrin uptake averages 60 pmol/l whole blood/d (6). Under the stimulus of anemia, the marrow is able to increase its level of production several-fold. There is the time lag of several days before the full proliferative response of the marrow is observed, and the magnitude of the response is directly related to the severity of anemia and the level of iron supply (2). If the iron supply to the erythron is adequate and the erythron retains its normal proliferative capacity,
the erythroid activity is expected to be at least 3 times basal at hemoglobin levels below 10 to 11 g/dl, or hematocrit values below 30% (6). Mar- row production will increase still further with decreasing hemoglobin values, with some vari- ability due to the type and duration of anemia, the adequacy of iron supply, and the physiologi- cal variations of marrow proliferation at dif- ferent ages (17). When all these considerations are taken into account, we can reasonably assume that an erythropoietic activity equal to or greater than 3 times normal in the presence of long-lasting anemia indicates an adequate mar- row response or proliferative capacity. When the erythropoietic activity is lower in the presence of long-lasting anemia and the iron supply is ade- quate, a proliferative impairment can be as- sumed.
On the basis of the present results, the clinical classification of acquired marrow failure into two main categories, aplastic anemia and ineffec- tive erythropoiesis, appears to be an over- simplification. We found a large spectrum of erythroid proliferation, with many patients showing combined mechanisms in the production of their anemia.
Patients with severe aplastic anemia had values for erythroid activity under the lower normal limit. This can be defined as absolute marrow failure (2). Despite the low levels of proliferative activity, some variability was found with 6 out of 13 patients having values between 20 and 45 % of normal (Figure l), with 3 of these latter subjects showing persistent foci of intense hemopoietic activity, so-called “hot pockets” (18). It remains to be established whether the persistence of some residual erythroid proliferation can have prog- nostic implications. Torok-Storb et a1 (10) have recently found that there is a close association between clinical recovery of aplastic anemia after immunosuppressive therapy and the presence in the peripheral blood of a population of small cells that are phenotypically associated with the erythroid lineage. They studied ferrokinetics in only 4 subjects and apparently the patients with the lower plasma iron turnovers had the highest scores for circulating erythroid cells. This could

ERYTHROPOIESIS IN BONE MARROW FAILURE 431
indicate that immunological mechanisms are responsible for the nearly complete suppression of erythroipoiesis and the release in circulation of abnormal erythroid cells.
Massive bone marrow infiltration by neoplas- tic cells in the 3 patients we studied did not suppress erythroid proliferation at degree com- parable to those observed in aplastic anemia. In patients with refractory anemia, values for erythropoietic activity ranging from normal to about 2 times normal were also found. There- fore, the erythroid marrow of most of these subjects had a greater proliferative activity when compared to that of patients with aplastic anemia. Nevertheless, the erythropoietic effort was less than 3 times normal in the presence of anemia, i.e. inadequate for the degree of ery- thropoietin stimulation. This can be defined as relative marrow failure and implies that the stem cell compartment is compromised but retains some proliferative capacity. However, inadequate erythroid proliferation, not ineffec- tive erythropoiesis, was the major mechanism of anemia in these subjects. Erythroid prolifera- tion appeared to be adequate for the degree of anemia in all but 1 patient with idiopathic refractory sideroblastic anemia, and ineffective erythropoiesis was responsible for anemia in these patients. The only exception was a patient who later developed acute non-lymphocytic leu- kemia and who could not be distinguished from the other cases by means of conventional clini- cal data. This confirms previous observations that low erythroid proliferation is a poor prog- nostic sign (19).
In conclusion, the simple approach to deter- mination of proliferating activity of the erythroid marrow employed in this study can provide use- ful information on the pathophysiology of mar- row failure and a basis for the selection of therapeutic approaches.
Acknowledgments This work was supported by the CNR Special Project Oncology, contract no. 85.02084.44, and AIRC (Asso-
ciazione Italiana per la Ricerca sul Cancro (to MC) and National Institute of Health Grant No. HL 06242 (to CAF).
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12
13
14
15
Wintrobe MM, Lee GR, Boggs DR, et al. Clinical Hema- tology. 8th ed. Philadelphia: Lea & Febiger, 1981:698. Hillman RS, Finch CA. Red Cell Manual, edn 5. Phila- delphia: F. A. Davis Company, 198556. Camitta BM, Storb R, Thomas SD. Aplastic anemia. Pathogenesis, diagnosis, treatment and prognosis. N Engl J Med 1982;306:645-52. Bennett JM, Catovsky D, Daniel MT, et a1 (French-Amer- ican-British Cooperative Group). Proposals for the classi- fication of the myelodysplastic syndromes. Br J Haematol 1982;s 1 : 189-99. Cazzola M, Huebers HA, Sayers MH, MacPhail AP, Eng M, Finch CA. Transferrin saturation, plasma iron turn- over, and transferrin uptake in normal humans. Blood 1985;66:935-9. Cazzola M, Pootrakul P, Huebers HA, Eng M, Eschbach J , Finch CA. Erythroid marrow function in anemic man. Blood 1987;69:296-301. ICSH Expert Panel on Iron. Recommended methods for measurements of serum iron in human blood. Br J Haematol 1978;38:291-4. ICSH Expert Panel on Iron. The measurement of total and unsaturated iron binding capacity in serum. Br J Haematol 1978;38:281-90. Kagan WA, Ascensao JL, Fialk MA, Coleman M, Valera EB, Good RA. Studies on the pathogenesis of aplastic anemia. Am J Med 1979;66:444-9. Torok-Storb B, Doney K, Sale G, Thomas D, Storh R. Subsets of patients with aplastic anemia identified by flow microfluorimetry. N Engl J Med 1985;312:1015-22. May SJ, Smith SA, Jacobs A, Williams A, Bailey-Wood R. The myelodysplastic syndrome: analysis of laboratory characteristics in relation to FAB classification. Br J Haematol 1985;59:311-9. Dessypris EN, Krantz SB. Primary refractory anemia: clinical and laboratory study of erythropoiesis in 16 patients. Am J Med Sci 1985;289:229-35. Erslev AJ. Erythrokinetics. In: Williams WJ, Beutler E, Erslev AJ, Rundles RW, eds. Hematology. New York: McGraw-Hill, 1972; 1386-92. Ho-Yen DO. Assessing bone marrow cellularity. J Clin Pathol 1983;36:835-6. Tricot G, De Wolf-Peters C, Hendrickx B, Verlwilghe RL. Bone marrow histology in myelodysplastic syndromes. I . Histological finding in myelodysplastic syndromes and comparison with bone marrow smears. Br J Haematol 1984;57:423-30.
16. Lintula R. Ferrokinetic abnormalities and red cell life span in myelodysplastic syndromes: A review. Scand J Hae- matol 1986;36(suppl 45):48-52.
Eur J Haematol 1987;38 28

432 CAZZOLA ET AL
17. Lipschitz DA, Udupa HB, Milton KY, Thompson CO. Correspondence to: Effect of age on hematopoiesis in man. Blood 1984; Dr. Mario Cazzola 63: 502-9. Clinica Medica I1
Scand J Haernatol 1976;17:326-34.
evaluation of erythropoietic activity in dysmyelopoiestic syndromes. Br J Haematol 1982;50:55-62.
18. Kansu E, Erslev AJ. Aplastic anemia with “hot pockets”.
19. Cazzola M, Barosi G, Berzuini C, et al. Quantitative Italy
Policlinico S. Matteo 27100 Pavia