Embed Size (px)
Citation preview

CIHRT Exhibit P-2625 Page 1
PATHOLOGYOF THE BREAST
SECOND EDITION
Fattaneh A. Tavassoli, 1\10, AFlPChairman
Department of Gynecologic & Breast PathologyArmed Forces Institute of Pathology
Washington, DC
Adjunct Professor or PathologyGeorge Washington University
Washinglon, DC
Consultant in PathologyNational Cancer Institute
Bethesda, Maryland
APPLETON & LANGEStamford, COllnecticul

CIHRT Exhibit P-2625 Page 2
Notice: The author and the pnblisher of this volnme have taken care t·o make certain that thedoses of drugs and schedules of treatment are correct and compal-iblc wil h HIe standardsgenerally accepted at HlC time of publication. evertheless, as new information becomesavailable. changes in treatment and in the use of drugs uecome necessary. The render is advised
to carehlll)' consnlt the instruction and information material inclnded in the package insert of eachdrug or therapeut ic agent before administration. This advice is especially important when nsing,administering, or recommending new or infreqnently nsed drugs. The anthor and publisherdisclnim all responsibility for any liability. loss. injury, or dnmage incurred as a conseqllellce,directly or indirectl)" of the use and application of an)' of the conlents of this volnme.
Copyright © 1999 b)' Appleton & LangeCopyright© J992 b), Appleton & Lange
All rights reserved. This book, or any parts thereof, may not be nsed orreproduced in any mallner without written pernlission. For informal ion,
address Appleton & Lange, Four Stamford Plaza, PO Box 120041,Stamford, Connecticnt 06912-0041.
www.applet·onlange.COlll
99 00 01 02 03 / .10 9 8 7 6 5 4 3 2 1
Prentice Halllnteruational (UK) Limited, l.olldolll'renl'ice Hall of Australia Pty. Limited, S)'dlleyPrentice Hall Canada, Inc., TorolltoPrentice Hall Hispanoamericana, S.A., MexicoPrentice I-Iall of India Private Limited, New DelhiPrentice I-Iall ofJapan, Inc., TokyoSimon & Schuster Asia Pte. Ll.d., SillgaporeEditora Prentice Hall do Brasil Uda., Rio dejalleiroPrentice Hall, Upper Saddle Hiver, Nelli Jersey
Librar)' of Congress Cataloging-ill-Publica! ion Data
Tavassoli, Fattaneh A., 1949-Pathology of the breast / Fatl:aneh A. Tavassoli. - 2nd ed.
p. cm.Includes bibliographical references and index.1SBN 0-8385-770'1-0 (case: aile paper)1. Breast-Cancer-Diagnosis. 2. Breast-Histopathology.
3. Breast-Diseases. I. Tille.IDNLJVJ: 1. Breast Diseases-pathology. 2. Breast-pathology.
3. Breasl" Neoplasms-pathology. WI' 840 T231p 1999JHC280.B8T39 J999616.99'249-dc2 L
DNI.JVJ/DLC1'01' Library of Congress 98-50680
CipISBN 0-8385-7704-0
Acgllisitions Editor: Michael P. MedinaProduction Editor: Sondra GreenfieldDesigner: Janice Barsevich BielawaCover Design: Aimee Nordin
PHINTED IN liaNG KONG

CIHRT Exhibit P-2625 Page 3432 • PATHOLOGY OF Til E BREAST
A B
Figure 9-22. Infilliating lobular carcinoma, alveolar variant. (A & B) Closely packed islands of uniform small cells [11M, (A) x 120; (B) x240)
Axillary Node MetastasesIn Haagensen's series2980f 76 Columbia stage A small-cell carcinomas (comparable to infiltrating lobular carcinoma), the frequency of axillary node metastases was 39.7%, compared wilh30.8% for similar stage carcinomas of all types. Two other studies also found a lower frequency of nodal metastases (32% inboth studies) for lobular carcinoma compared with 37%321 and35%317 for infiltrating ductal carcinoma. Fechner292 has suggested that the variant patterns may be associated with a 10IVerfrequency of axillary node metastases.
Infiltrating lobular carcinoma is notorious for simulatinghistiocytes in metastatic foci andlVhen populating subcapsularand medullary sinuses in axillary lymph nodes.279.30' The sheetlike aggregation of the tUlllor cells and subt"le distortion of thenodal archilecture are helpful in arriving at the accural"e diagnosis. When a distinction is difl1cult, special staining for mucinor imlllunostains for cytokeratin helps resolve the issue; a positive reaction for mucin or cytokeratin establishes the diagnosisof carcinoma. In the eyelids, the histiocytic appearance of themetastatic tumor cells Illay cause misinterpretation of the lesion as a chalazion.301.333
The metastatic pattern of lobular invasive carcinoma differsfrom that of invasive ductal carcinoma with a higher frequencyof skeletal, gaslTointestinal tract, uterine, ovarian, meningeal,genitourinary, skin, diffuse serosal, peritoneal and retroperitoneal metastases observed in lobular carcinomas.281.283.299,317.
324.325 The gastrointestinal, gynecologic, and peritoneal-retroperi-
toneal mel aslases are markedly more prevalent in lobular carcinoma 281 In the central nervous system, melasl'ases from invasivelobular carcinoma form meningeal intillrales, whereas. ductalcarcinomas sholV parenchymal deposits.212.322 Other investigators, however, found an eqlla[ proportion of lobular and ductalcarcinomas among patients lVilh meningeal carcinomalosisfrom breast cancer.212 Metastases 10 the ovary and u ten IS arecommon. In the endometrium, metastases cause bleeding, butbecause of the small cell size and diffuse pal tern of infiltration inthe endometrium, these metastases are easily overlooked. Furthennore, even when the cells are larger wil"h pink cytoplasm,they are often misinterpreted as a decidual reaction to progestins, which many of the patients receive for their irregularbleeding prior to the cllret tage. Bone mnrrolV mel"aslases are particularly common,322 and constil"uted the most common site ofmetastases in DiCostanzo and colleagues' series.286
Hormone Receptors and PloidyAbout 70-92% of lobular carcinomas are EH_positive.s.JlI6.120.317 EH
positivity is observed in the classic form and all other variants,309with the alveolar variant appearing to have a greal"er likelihood ofEH positivity.3()" Progesterone recept.ors are fonnel in 63-67% ofthe tUlllors317.508.511 Carcinoembryonic ant igen (CEA) has beenreported in 33-63% of cases.85.309 Milk-related proleins, SIIch asladalbumin and casein, have been detected in some cases.29 J.327Also, 60% of these tumors sholV a positive reaction (or 5-] 00 protein, underscoring the lack of specificity of5-100 protein.36

CIHRT Exhibit P-2625 Page 4
Figure 9-23. Infiltrating lobular carcinoma, pleomorphic varian!. (A) At low magnification the lesion resembles typical infiltrating lobular carcinomawith isolated cells sometimes arranged in cords. (B) The nuclei display significant pleomorphism, and more variation is generally evident in cell size. [H&E,(A) x240; (B) x480j
_.
. ~""-'''p.lI.r......'.
r'
\
•
..)
...,
W~-41.
c...··ti
,.
A
I ..
6,

CIHRT Exhibit P-2625 Page 5434 • PATHOLOGY OF Til E BREAST
~ ~-'- -'.:'.~,,- _:,-f-- -- -..-.:.~- -
C
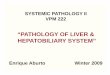
Figure 9-23. (C) Pleomorphic lobular neoplasia (LN3) shows some highly atypical nuclei; curiously, this tumor was ER positive even in the highly atypical cells. (H&E, x300j
Approximately 22% of infiltrating lobular carcinomas areaneuploid. Among ER-positive tumors, ploidy does not appearto influence the likelihood of PR positivityS08
Treatment and Prognosis
Treatment of infiltrating lobular carcinoma should parallel thatof infiltrating mammary carcinomas in general and depends onthe stage of the lesion. Conservative treatment of invasive lobular carcinoma has been sholVn to be an appropriate alternativein selected cases302,312 The results of limited excision and radiotherapy for "19 lobular carcinomas were compared with those of561 cases of inf1ltrating duct carcinoma. The 5-year actuarialrisk of local recurrence was similar for patients with infiltratinglobular or ductal carcinoma: 12% versus 11%. \J\lhen the groupwith infiltrating duct carcinoma was di\rided into those with anextensive DClS component and those without such a component, the 5-year actuarial survival of 12% for lobular carcinomafell between the 5% rate for infiltrating duct carcinomas withextensive DClS component and the 23% for those infiltratingduct carcinomas without extensive DClS. 117
Another study comparing clinicopathologic features of infiltrating lobular carcinoma (726 cases), mixed inl1ltrat-ing lobular/invasive ductal carcinoma (249 cases), and nonlobular infiltrating carcinomas (10,061 cases) also evaluated response of thethree groups to conservative therapy.317 Conservative treatmentwas used in 480 cases (66%) of pure lobular carcinoma, 6797cases (68%) of nonJobular infiltrating carcinomas, and 43 casesof mixed infiltrating lobular/invasive ductal carcinoma. 'vVith amedian follow-up of 82 months, the overall survival rate, locore-
gional control, disease-free interval, and metastaLic spread ratewere not different among the three groups by eiLher univariateor mult-ivariaLe analysis; the investigaLors concluded t.hat conservative therapy may be appropriate treatment for infiltratinglobular carcinoma.317
The 5- and 10-year survival rate for node-negative women,is 86% and 74%, respectively.280 Following radical mastectomy,approximat ely 5.4% of the women develop local recurrenceswithin ]0 years.298 About 50% of patients with positive nodeseventually die from the disease compared with 14% of the nodenegative women.310
Although some studies have suggested a worse prognosisfor infiltrating lobular carcinoma than for ductal cancer,306 several studies have found no significant. difference in survival,280.285.317.323 or even a more favorable outcome for infiltratinglobular carcinoma.321 ,326 In some studies, the observed differences are not substant-ial; about 6% of women with 1'1 OMO infiltrating lobular carcinomas treated by mastectomy died of thedisease within 10 years, compared with 14% of those with infiltrating ductal carcinoma. 133 In Haagensen's experience298 andfollowing radical mastectomy, wOlllenwith Columbia stage A inl1Itrating small-cell carcinomas had a 75% probability ofl O-yearsurvival, compared with 72% for patient·s ""ilh all other types ofbreast carcinoma. In a comparison of sUI-vival between 217women with invasive lobular carcinoma and 1121 women withinfiltrating duct carcinoma, Toikkanen and coworkers326 found5- and 3D-year corrected sUlvival rates of 78% and 50% respectively, among women with lobular carcinoma, compared with63% and 37% survival rates. respectively, for those with infiltrating ductal carcinoma.326 Women with small pTINOIVIO infiltrat-