Embed Size (px)
Citation preview

Pathology of the Adnexa
Dr. Soekimin, SpPA ; dr. Jessy Chrestella, SpPADept. Patologi Anatomi Fakultas Kedokteran Universitas Sumatera UtaraMedan 2010

PATHOLOGY OF FALLOPIAN TUBES
Congenital Anomalies Parametritis/Salphingitis Ectopic pregnancy Hydrosalpinx Endometriosis Para ovarian cyst Carcinoma




6
Ectopic Pregnancy:
Tubal – common. implantation allows
early placental development, secretion of hCG, and maintainance of the corpus luteum.
Clinically features of a normal pregnancy and the embryo may also complete the early embryonic stages of development.

Pathology of Ovary
Inflam/Infections - rare Ovarian cysts - common.
Non-Neoplastic▪ Follicular, epithelial, Luteal, etc.▪ Polycystic ovary syndrome▪ Ovarian Hyperstimulation synd.▪ Stromal Hyperplasia*▪ Endometriosis
Neoplasms▪ Benign (Cysts)▪ Malignant (Solid)
7

OV. NEOPLASMA Serous cystadenoma Cystoma Papillary cystadenoma serosum Surface papilloma Serous adenofibroma Serous cystadenofibroma Pseudomucinous cystadenoma Teratoma
- dermoid cyst- Solid teratoma.

OV. NEOPLASMA Granulosa cell tumor Theca cell tumor Arrhenoblastoma Adrenal rest tumor Dysgerminoma Brenner tumor Fibroma Meigs syndrome Sarcoma Carcinoma (ad.Carcinoma) Metastase carcinoma.

10
Ovary:
Cysts – Common – benign very large. Solid – rare – malignant – high mortality. 5th common cause of female cancer. But carcinomas of the ovaries account for
more deaths than do cancers of all other female malignancies together. (US stat).
Nulliparity & family history (BRCA) - Risk factor.

Polycystic Ovary Synd Amenorrhoea, hyperoestrogenism
and multiple follicular cysts. Stromal hyperplasia &
anovovulation Important cause of infertility, Endometrial
hyperplasia/Carcinoma. Clinical features:
Acne, alopecia, hirsutism, Hypertension, Insulin resistance, Type 2 DM. Obesity – Syndrome X.
11

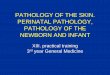
PCOS- Low power view
12
Note: capsule thickening, cystic follicles without ova, thecal hyperplasia.

Endometriosis: chocolate cysts Metastases of hyperplastic
endometrium into ovary. Retrograde
menstruation /Metaplasia. Estrogen related. Pouch of Douglas, the
pelvic peritoneum and the ovary - 'chocolate cysts'.
Periodic Pain, pelvic inflammation, infertility.
13

14
Endometriosis:Chocolate Cysts

Endometriosis:
15
Chocolate Cysts

Neoplasms of Ovary
Common, produce estrogen. 80% are benign, cystic, young (20-45) 20% are Malignant, solid - older (>40) 6% of all cancers in women. 50% deaths due to late detection. The rule:
Cystic tumors are commonly benign
Solid tumors are commonly malignant.16

Risk Factors
Less clear than other Null parity Gonadal Dysgenesis Family History Ovarian cancer genes
BRCA1 (17q12) & BRCA2(13q12)
17

18
Classification of Ovarian Tumours

Epithelial tumors Coelomic mesothelium
Serous (tubal) Mucinous (Cx) Endometrioid (End) Transitional (UT)
90% of malignant tumors of ovary Morphologically
Cystic – Cystadenomas - Benign Solid/cystic – Cystadenoma - Borderline. Solid –Cystadenocarcinoma – Malignant.
19

Serous Tumors
Frequently bilateral (30-66%). 75% benign/bord., 25% malignant. One or few cysts, papillary/solid. Tall columnar ciliated epithelium. Papillary, solid, hemorrhage, necrosis or
adhesions – malignancy. Extension to peritoneum – bad prog.
20

Mucinous Tumors
Less common 25%, very large. Rarely malignant - 15%. Multiloculated, many small cysts. Rarely bilateral – 5-20%. Tall columnar, apical mucin. Pseudomyxoma peritonei.
21

22
Serous Cystadenoma

23
Serous Cystadenoma

24
Serous Cystadenoma
Borderline / Intermediate grade: note larger papillary growth.

25
Serous Cystadenoma
multiloculated, 24cm cystic ovary with attached fallopian tube and uterus. – benign serous cystadenoma.

26
Mucinous Cystadenoma
Note: papillary growths on inner surface

27
Mucinous Cystadenoma
Note: Multi-loculated cystic tumor with some cysts showing hemorrhage.

28
Serous - Cystadenoma - Mucinous
Cuboidal simple – Columnar Mucous

29
Serous Cystadeno-carcinoma
High grade: note large papillary growth extending and covering the cyst.

30
Serous Cystadenoma Borderline
High grade: note large papillary growth extending and covering the cyst.

31
Papillary cystadenoma (bor)

32
Papillary serous cystadenoma (solid/cystic)

33
Serous Cystadeno-carcinoma
High grade: note large papillary growth extending and covering the cyst.

34
Papillary cystadenoma (bor)
Infiltration
Papillary projections

35
Serous cystadeno Ca – bilateral

36
Serous cystadeno Ca.
Solid tumor with atypical cells forming sheets and gland like structures without stroma. (back to back arrangement of
glands)

Germ cell Tumors:
Teratoma – Benign cystic (dermoid cyst) Solid immature Monodermal – struma ovarii, carcinoid
DysgerminomaYolksac tumorMixed germ cell tumor
37

38
Dermoid Cyst:

40
Cystic Teratoma

41
Dermoid Cyst:
Granulation
tissue lin
ing
Skin lin
ing

42
Dermoid Cyst:
Cartilage
Resp. Epith
Sweat Gl.

43
Dermoid Cyst:
Sebaceous Gl.Thyroid
MucosaSq. Epithel
M.A.L.T.Cyst Lumen

44
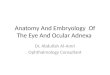
Dermoid Cyst:
Black arrow: Stratified squamous Keratinizing epithelium. Blue arrow: Abundant sebaceous glands.

45
Immature/Malignant teratoma:

46
Immature/Malignant teratoma:
Any type of carcinoma, sarcoma or germ cell malignancy.

47
Staging of Ovarian Ca:

Complications of Dermoid cyst Torsion - infarction, perforation,
hemoperitoneum, and autoamputation
Bacterial infection of the cyst Perforation - sudden acute
abdomen, Slow granulomatous peritonitis
Hemolytic anemia – clears after removal.
<5% malignancy – Sq. carcinoma. 48

Other Tumors of Ovary:
49

50
Endometrioid Ca:

51
Granulosa Cell Tumor:

52
Ovary: Dysgerminoma

53
Ovary: Dysgerminoma
• Teenage / young, 2% of ovarian neoplasms.• 1/2 of malignant germ cell neoplasms• Gonadal dysgenesis – risk factor.

54
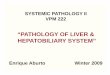
Ovary: Dysgerminoma
Note the pale brown appearance of the parenchyma, along with some central collagenous scar. The gross and microscopic appearance of an ovarian dysgerminoma is essentially same as a seminoma of the testis in a male.

55
Granulosa Cell Tumor:

56
Granulosa Cell Tumor:
Steroid cell tumour of the ovary. A well-circumscribed benign ovarian stromal tumour that caused virilisation in the patient

57
Krukenberg Tumor
Metastases of adenocarcinoma to ovary.

Summary

Thank you