Embed Size (px)
Citation preview

J. clin. Path. (1968), 21, 744-747
Pathology of hereditary nephritisV. V. JOSHI1
From the Department ofPathology, Medical College of Virginia, Richmond, Va, USA
SYNOPSIS This report describes the renal pathology in three siblings with hereditary nephritis.All three cases showed combined features of chronic glomerulonephritis, pyelonephritis, andinterstitial nephritis. Foam cells were seen in only one case. These findings support the contentionof Krickstein, Gloor, and Balogh (1966) that the renal changes in hereditary nephritis are those ofa mixed nephritis.
In the past few years there have been several reportson hereditary nephritis Krickstein et al,1966; Mulrow, Aron, Gathman, Yesner, andLubs, 1963; Perkoff, 1967) and up to 196525 families with the disease were reported (Johnsonand Hagan, 1965). The clinical aspects of the diseasehave been well described (Marin and Tyler, 1961;Mulrow et al, 1963; Perkoff, Stephens, Dolowitz,and Tyler, 1951).
Haematuria, proteinuria, hypertension, andepisodes of urinary tract infection are usualmanifestations of the disease. In the involvedfamilies the male members develop progressiverenal insufficiency and die in uraemia between theages of 20 and 30 in most cases. However, thefemale members of the involved families have muchless severe renal disease and few are thought to dieof it. Extrarenal abnormalities such as nervedeafness, congenital cataract, or congenital strabis-mus may be associated with the disease. Themechanism of inheritance is uncertain. Althoughseveral authors have described the renal pathologyin their reports on hereditary nephritis, there isdisagreement as to the significance of the renalchanges. Krickstein et al (1966) believe that therenal pathology is that of 'mixed nephritis'. Thepurpose of this paper is to describe the renalpathology in three siblings witb hereditarynephritis.
CASE REPORTS
The three patients were siblings, two of them twinbrothers. Necropsies were performed on two of the threepatients. On the third patient a renal biopsy was done.As far as is known other members of the family have not
Received for publication 26 March 1968.'Present address: Cancer Research Laboratory, University ofWestern Ontario, London, Canada.
shown obvious evidence of renal disease. However, theyare spread over two states and it has not been possible toget a detailed family history.
CASE 1 A 30-year-old Negro male (T.B.) was admitted tothe Norfolk General Hospital for the first timetthree-and-a-half weeks before death; with increasing weakness,fatigue, hypertension, and anaemia. He had been treatedfor uraemia (blood urea nitrogen between 150 and 170 mg%O) in other hospitals during the six months before ad-mission with peritoneal dialysis. Physical examinationshowed an obese Negro male who was lethargic but notcomatose. Blood pressurewas 170/115 mm Hg.There wascardiac enlargement with a soft, blowing apical systolicmurmur. Clinically, there was no evidence of nerve deaf-ness. Audiometric studies were not done. Urine analysisshowed 3+ proteinuria, 3 to 5 white blood cells, and afew epithelial cells per high-power field. The specificgravity was 1-015. Blood urea nitrogen was 220 mg %,and creatinine 16 mg %. During his hospital stay, thepatient developed increasing dyspnoea, restlessness,tachycardia, and oliguria. He died after the suddenonset of massive bloody diarrhoea.At necropsy, there was hypertensive cardiomegaly
with left ventricular hypertrophy, fibrinous pericarditis,and uraemic colitis with diffuse mucosal haemorrhage.The renal pathology is described below.
CASE 2 A 24-year-old Negro male (N.B.) was transferredto the Medical College of Virginia Hospitals on 5 June1967 for treatment of chronic renal disease and hyper-tension of about two years' duration. On physicalexamination he was obese and lethargic. There wascardiac enlargement. Blood pressure was 180/116 mmHg. Examination of the ocular fundi revealed smallexudates, several punctate haemorrhages, and probableoptic atrophy. There was no clinical evidence of nervedeafness. Audiometric studies were not done. Urineanalysis showed 1 + proteinuria, 10 white blood cellsand 20 red blood cells per high-power field, and anoccasional granular cast. Blood urea nitrogen was234 mg % and creatinine 27 mg %. The patient died 10days after admission.
744
on March 3, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.21.6.744 on 1 Novem
ber 1968. Dow
nloaded from

Pathology ofhereditary nephritis
At necropsy there was hypertensive cardiomegaly withleft ventricular hypertrophy and dilatation, andpulmonary oedema. The renal changes are describedbelow.
CASE 3 A 24-year-old Negro male (K.B.), twin brotherof the patient above (case 2), was admitted to the MedicalCollege of Virginia Hospitals for evaluation of his renaland cardiovascular status in view of the family history ofhereditary nephritis. On physical examination he wasobese, with a blood pressure of 180/120 mm Hg and agrade III hypertensive retinopathy. There was no clinicalevidence of nerve deafness. Audiometric studies were notdone. Urine analysis revealed proteinuria of 1 to 2+ anda few white blood cells per high-power field. The bloodurea nitrogen ranged from 14 to 26 mg % and creatininewas 1-9 mg %. A pyelogram showed bilateral delay inexcretion. A kidney biopsy was done.
PATHOLOGY OF THE KIDNEYS
Gross examination of the kidneys from the twonecropsied patients showed that they were reducedin size, the combined weight being 190 g in the first
case and 230 g in the second case. The corticalsurfaces were uniformly coarsely granular with afew capsular adhesions. The cortical thicknessesaveraged 4mm with blurring of the cortico-medullaryjunctions. The calyces and pelves of all four kidneyswere normal. Fatty streaks or yellow colorationdue to fat were not present. The histological pictureof the kidneys in all three cases was fundamentallythe same with a few individual variations as describedbelow.
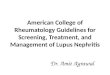
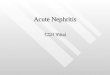
GLOMERULI The glomeruli in all cases showed severechanges. These were involved by a process whichranged from basement membrane thickening in afew to severe fibrosis and hyalinization involvingmost glomeruli (Fig. 1). Some showed epithelialcrescents (Fig. 2). Periglomerular fibrosis was presentaround a few glomeruli (Fig. 3.) Foam cells wereseen in a few glomeruli from case 1 (Fig. 4) but werenot present in the glomeruli or in the interstitialtissues in the other cases. Some glomeruli werenormal.
V -FIG. 1 FIG. 2FIG. 1 . Hyalinization of glomerulus. Interstitial inflammatory infiltrate and tubular atrophy are also seen.Haematoxylin and eosin x 245.FIG. 2. Glomerulus showing epithelial crescent. Haematoxylin and eosin x 245.
745
on March 3, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.21.6.744 on 1 Novem
ber 1968. Dow
nloaded from

V. V. Joshi
FIG. 3. Periglomerular fibrosis. There is also interstitial FIG. 4. Glomeruli showing foam cells. Atrophic tubulesinflammatory infiltrate. Haematoxylin and eosin x 245. are also seen. Haematoxylin andeosin x 245.
.0
.0
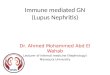
e. FIG. 5. Interstitial fibrosis andtubular atrophy. A few dilated
vf tubules are also seen. Haematoxylinandeosin x4-245.
746
on March 3, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.21.6.744 on 1 Novem
ber 1968. Dow
nloaded from

Pathology ofhereditary nephritis
TUBULES The predominant change in the tubuleswas atrophy and collapse (Figs. 1 and 4), but therewere a few areas of tubular dilatation in the super-ficial portions of the cortex. Tubular epithelium didnot appear foamy in any of the cases.
INTERSTITIAL TISSUES There were varying degreesof interstitial fibrosis (Fig. 5) with chronic inflam-matory infiltrate (Figs. 1 and 3). The interstitialfibrosis was more prominent than the inflammatoryinfiltrate.
BLOOD VESSELS The blood vessels showed markedfibrous intimal thickening of both small-sizedarteries and arterioles in all three cases.
CALYCES AND PELVES The calyces and pelves werenormal histologically.
DISCUSSION
Previous reports of hereditary nephritis haveclassified the renal lesions as chronic glomerulo-nephritis (Dubach, Minder, and Antener, 1966;Whalen, Huang, Peschel, and McIntosh, 1961),chronic pyelonephritis (Goldbloom, Fraser, Waugh,Aronvitch, and Wiglesworth, 1957; Perkoff et al,1951; Whalen et al, 1961) or as interstitial nephritis.Krickstein et al (1966) in their report state that therenal changes of hereditary nephritis consist ofcombined features of chronic glomerulonephritis,pyelonephritis, and interstitial nephritis but lacksome characteristics of each, so they called it a'mixed' type of nephritis. Further, they showed thatfoam cells are frequently present (in 11 of their18 cases) in the tubules, interstitial tissues, andglomeruli. They believe that this combination of'mixed' nephritis with the foam cells is the character-istic lesion of hereditary nephritis.
In our cases, also, the renal changes combine thefeatures of chronic glomerulonephritis (severe hya-linization of many glomeruli, crescent formation),chronic pyelonephritis, and interstitial nephritis(periglomerular fibrosis, chronic interstitial inflam-matory infiltrate, and fibrosis). Yet some character-
istics of each were lacking. For example, in chronicpyelonephritis inflammatory changes in the calycesand pelves are commonly seen, but in our cases theywere absent. Unlike classical chronic glomerulo-nephritis, some glomeruli in our cases werecompletely normal. Interstitial fibrosis and chronicinflammation were not as severe as usually seen inchronic interstitial nephritis.
In one of the three cases reported here, foam cellswere present in the glomeruli. Though otherauthors (Krickstein et al, 1966) have shown thatfoam cells are often present in hereditary nephritis,it appears that their importance has been over-emphasized. Foam cells are certainly not specificfor hereditary nephritis since they are seen in otherconditions such as nephrosis and chronic glomerulo-nephritis (Whalen et al, 1961). Also in the seriesreported by Krickstein et al (1966) foam cells werepresent in only three of the seven young patients inwhom renal biopsies were done. Though abnormal-ities of lipid metabolism based on the presence offoam cells have been suggested as playing a role inthe pathogenesis of hereditary nephritis, it appearsmore likely that the foam cells are a secondarydevelopment in the later stages of hereditarynephritis. The prominent vascular changes in thethree cases reported here are probably secondary tohypertension.
I am indebted to Dr Fairfield Goodale for his advice andcriticism in preparation of the manuscript. Thanks arealso due to Dr Saul Kay and Dr R. R. Stephens formaking material available.
REFERENCES
Dubach, U. C., Minder, F. C., and Antener, I. (1966). Helv. med.Acta, 33, 36.
Goldbloom, R. B., Fraser, F. C., Waugh, D., Aronvitch, M., andWiglesworth, F. W. (1957). Pediatrics, 20, 241.
Johnson, W. J., and Hagan, P. J. (1965). Arch. Otolaryng., 82,166.Krickstein, H. I., Gloor, F. J., and Balogh, K., Jr (1966). Arch. Path.,
82, 506.Marin, 0. S. M., and Tyler, H. R. (1961). Neurology (Minneap.), 11,
999.Mulrow, P. J., Aron, A. M., Gathman, G. E., Yesner, R., and Lubs,
H. A. (1963). Amer. J. Med., 35, 737.Perkoff, G. T., Stephens, F. E., Dolowitz, D. A., and Tyler, F. H.
(1951). Arch. intern. Med., 88, 191.(1967). New Engl. J. Med., 277, 79 and 129.
Whalen R. E., Huang, S., Peschel, E., and McIntosh, H. D. (1961).Amer. J. Med., 31, 171.
747
on March 3, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.21.6.744 on 1 Novem
ber 1968. Dow
nloaded from