Upload
vankhanh
View
221
Download
0
Embed Size (px)
Citation preview
Pathogens Penetrating the Central Nervous System: InfectionPathways and the Cellular and Molecular Mechanisms of InvasionSamantha J. Dando,a Alan Mackay-Sim,b Robert Norton,c Bart J. Currie,d James A. St. John,b Jenny A. K. Ekberg,b,e Michael Batzloff,a
Glen C. Ulett,f Ifor R. Beachama
Institute for Glycomics, Griffith University, Gold Coast, Queensland, Australiaa; Eskitis Institute for Drug Discovery, Griffith University, Brisbane, Queensland, Australiab;Townsville Hospital, Townsville, Queensland, Australiac; Menzies School of Health Research and Royal Darwin Hospital, Darwin, Northern Territory, Australiad; School ofBiomedical Sciences, Queensland University of Technology, Brisbane, Queensland, Australiae; School of Medical Science and Griffith Health Institute, Griffith University,Gold Coast, Queensland, Australiaf
SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .692INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .692
Meningitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .692Pneumococcal meningitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .692Meningococcal meningitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .693H. influenzae, L. monocytogenes, and other bacterial causes of meningitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .693
Encephalitis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .693Focal Infections. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .694
BARRIERS OF THE CNS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .694The Blood-Brain Barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .694The Blood-Cerebrospinal Fluid Barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .694Immunosurveillance of the CNS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .695
MICROBIAL ENTRY TO THE CNS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .696In Vivo and In Vitro Models of CNS Invasion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .696
BACTERIAL INVASION THROUGH THE BLOOD-BRAIN AND BLOOD-CEREBROSPINAL FLUID BARRIERS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .697Sites of Entry. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .697Mechanisms of Entry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .697Transcellular Penetration of Brain Microvascular Endothelial Cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .699
E. coli . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .699N. meningitidis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .700S. pneumoniae . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .700Group B streptococcus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .701S. suis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .701L. monocytogenes and B. pseudomallei . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .702M. tuberculosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .703
Paracellular Penetration of Brain Microvascular Endothelial Cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .703E. coli . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .703H. influenzae. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .704N. meningitidis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .704Streptococcus spp. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .704
Trojan Horse Penetration of Brain Microvascular Endothelial Cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .705THE OLFACTORY NERVE AS A PORTAL TO THE BRAIN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .705THE TRIGEMINAL NERVE AS A PORTAL TO THE BRAIN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .707PROTECTING THE CNS FROM MICROBIAL INVASION VIA THE NASAL CAVITY. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .707PATHOGENS THAT ENTER THE BRAIN THROUGH THE NOSE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .708
Bacteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .708S. pneumoniae . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .708N. meningitidis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .709B. pseudomallei . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .709L. monocytogenes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .710
Viruses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .710Protozoa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .712Yeasts and Fungi . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .712
(continued)
Address correspondence to Glen C. Ulett, [email protected], or Ifor R.Beacham, [email protected].
G.C.U. and I.R.B. contributed equally to this work.
Copyright 2014, American Society for Microbiology. All Rights Reserved.
doi:10.1128/CMR.00118-13
October 2014 Volume 27 Number 4 Clinical Microbiology Reviews p. 691726 cmr.asm.org 691
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://dx.doi.org/10.1128/CMR.00118-13http://cmr.asm.orghttp://cmr.asm.org/CONCLUDING REMARKS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .712REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .713AUTHOR BIOS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .725
SUMMARY
The brain is well protected against microbial invasion by cellularbarriers, such as the blood-brain barrier (BBB) and the blood-cerebrospinal fluid barrier (BCSFB). In addition, cells within thecentral nervous system (CNS) are capable of producing an im-mune response against invading pathogens. Nonetheless, a rangeof pathogenic microbes make their way to the CNS, and the re-sulting infections can cause significant morbidity and mortality.Bacteria, amoebae, fungi, and viruses are capable of CNS invasion,with the latter using axonal transport as a common route of infec-tion. In this review, we compare the mechanisms by which bacterialpathogens reach the CNS and infect the brain. In particular, we focuson recent data regarding mechanisms of bacterial translocation fromthe nasal mucosa to the brain, which represents a little explored path-way of bacterial invasion but has been proposed as being particularlyimportant in explaining how infection with Burkholderia pseu-domallei can result in melioidosis encephalomyelitis.
INTRODUCTION
Microbial infection involving the central nervous system(CNS) is an important and relatively common presentation.CNS infections are frequently caused by viruses, such as the en-teroviruses, which cause the majority of cases of aseptic meningitisand meningoencephalitis (13). Other neurotropic viruses, suchas human cytomegalovirus, herpes simplex viruses, varicella-zostervirus, and the emerging viruses West Nile virus, henipaviruses, Japa-nese encephalitis virus, chikungunya virus, Ebola virus, and rabiesvirus, may also cause CNS infections (47). There are many bacterialpathogens that are associated with CNS invasion. Rapid detection ofa bacterial agent in such presentations and the initiation of appropri-ate antibiotic therapy influence morbidity and mortality (810). Theclinical presentations of bacterial CNS infection range from menin-gitis and meningoencephalitis to focal CNS syndromes.
Meningitis
Meningitis, or inflammation of the meninges, is usually acute butcan also be subacute and most frequently presents with headache,fever, and neck stiffness (11). Meningitis can be pyogenic (pusforming), which is associated with common bacterial etiologies(described below), or aseptic, in which pyogenic bacteria are notisolated from the cerebrospinal fluid (CSF) and the causativeagent may be viral or mycobacterial or there is a noninfectiveetiology. Features of CSF which would generally exclude a bacte-rial etiology for meningitis include a protein concentration of600 mg/liter and a white cell count of 90 106/liter (2). Theclassic triad of fever, neck stiffness, and a change in mental state isobserved in 44% of patients with bacterial meningitis (11).
A prospective, laboratory-based surveillance study in 1986 de-fined the epidemiology of bacterial meningitis in a population of34 million in the United States (12). This study reported an aver-age of 6.7 cases of bacterial meningitis per 100,000 populationacross six states and demonstrated that Haemophilus influenzae,Neisseria meningitidis, and Streptococcus pneumoniae caused 77%
of cases, which was consistent with a previous report by the Na-tional Surveillance of Bacterial Meningitis (13). More recently, itwas reported that the incidence of bacterial meningitis in theUnited States declined by 31% during the surveillance period of1998 to 2007, most likely due to the success of vaccine programs(14). S. pneumoniae was the most common cause of bacterialmeningitis (58.0%), followed by Streptococcus agalactiae (group Bstreptococcus) (18.1%), N. meningitidis (13.9%), H. influenzae(6.7%), and Listeria monocytogenes (3.4%). Staphylococcus aureusand Escherichia coli are also important causes of bacterial menin-gitis (15), and Streptococcus suis is emerging as a zoonotic etiologyof meningitis (16); however, it must be noted that meningitis canbe caused by a plethora of different bacteria (17). The most com-mon alternative bacterial cause of meningitis is Mycobacteriumtuberculosis, which is recognized particularly in pediatric popula-tions of the developing world (18, 19). These infections involve aclinical onset that is usually insidious, with hydrocephalus being aprominent feature.
Bacterial meningitis is usually preceded by nasopharyngeal ormiddle ear colonization, followed by (i) microbial invasion of thetissue and intravascular space and (ii) bacteremia. Meningeal in-vasion occurs following penetration of the cellular barriers of theCNS. High-level bacteremia was shown to be necessary for thedevelopment of meningitis in experimental animal models (20,21), which is consistent with clinical observations in humans (2224). Bacteria that commonly cause meningitis express antiphago-cytic capsular polysaccharide, which enables survival/multiplica-tion within the blood. Several species-specific factors thatpromote bacterial survival in blood, resistance to complement,and survival within phagocytes have been identified (2530). Bac-terial meningitis resulting from nonhematogenous spread is lesscommon and is a consequence of infection preexisting in an adja-cent intracranial site. Such infections include mastoiditis, frontalsinusitis, and rupture of an intracerebral abscess into the ventri-cles of the brain and may occur following head trauma or neuro-surgical procedures.
Pneumococcal meningitis. There are no specific distinguishingclinical features of pneumococcal meningitis. While a rash is un-common, it is occasionally seen in splenectomized patients withoverwhelming sepsis. There is a close correlation between bacte-remic and meningitic serotypes of S. pneumoniae, implicating he-matogenous spread as the commonest mode of acquisition (31). S.pneumoniae is the most frequent cause of bacterial meningitis inthe United States and has a case fatality rate of 14.7% (14). Afterthe introduction of the 7-valent pneumococcal conjugate vaccine(which contains serotype antigens 4, 6B, 9V, 14, 18C, 19F, and23F) in the United States, the incidence of pneumococcal menin-gitis declined by 30.1%, from 1.13 cases per 100,000 population in1998 to 1999 to 0.79 cases per 100,000 population in 2004 to 2005(32). In patients of 2 years and 65 years of age, the incidence ofpneumococcal meningitis throughout the surveillance period de-clined by 64.0% and 54.0%, respectively. Across all age groups, thenumber of meningitis cases caused by S. pneumoniae serotypes
Dando et al.
692 cmr.asm.org Clinical Microbiology Reviews
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://cmr.asm.orghttp://cmr.asm.org/covered by the 7-valent vaccine dropped by 73.3% (32). Similarreductions in invasive pneumococcal disease caused by 7-valentserotypes have also been reported in Australia, England, andWales (3335); however, this has led to a replacement phenome-non, in which the rates of disease caused by non-7-valent S. pneu-moniae serotypes have significantly increased (32, 34, 35).
Meningococcal meningitis. N. meningitidis is most likely tocause meningitis in children and adolescents and has a mortalityrate of 10.1% in the United States (14). The serotypes most com-monly implicated are A, B, C, W135, and Y (14, 3638), and men-ingitis without shock is the most common presentation (38). Thepredominant clinical feature, which can distinguish N. meningiti-dis from other causes of bacterial meningitis, is the presence of apetechial rash. It can rapidly become purpuric, which in the pres-ence of meningitis or sepsis strongly implicates N. meningitidis asthe etiologic agent. These lesions are a consequence of meningo-cocci adhering to the endothelial cells of the capillaries and smallveins in the skin, thereby altering the antithrombotic surface of theendothelium. This results in the formation of clots and the ex-travasion of erythrocytes, which appear as skin hemorrhages. Le-sions of 1.0 cm usually occur in patients developing shock, withhigh levels of circulating endotoxin (38).
Immunization against N. meningitidis serotypes A and C hasresulted in a significant decrease in meningococcal disease. TheUnited Kingdom was the first country to introduce routine im-munization with a monovalent serotype C conjugate vaccine, in1999. During the first follow-up surveillance period (2000 to2001), the incidence of serotype C meningococcal disease fell by80% in target age groups (39). Meningococcal serotype C vacci-nation programs in Australia have also led to a marked decrease indisease due to N. meningitidis serotype C. Of the 90% of menin-gococcal cases in Australia in 2010 that had serotype data avail-able, N. meningitidis serotype B caused 84.0% of cases (40). In2013, a recombinant meningococcus serotype B vaccine (Bexsero)was added to the Australian Register of Therapeutic Goods for usein individuals of 2 months of age and was also approved for usein Europe. In New Zealand, the introduction of an outer mem-brane vesicle vaccine against an epidemic N. meningitidis serotypeB clone in New Zealand was reported to be 80.0% effective in fullyimmunized children aged 6 months to 5 years (41).
H. influenzae, L. monocytogenes, and other bacterial causes ofmeningitis. H. influenzae as a cause of meningitis is now uncom-mon in most Western countries due to widespread immunizationagainst H. influenzae capsular type B, which was previously re-sponsible for the majority of cases of H. influenzae meningitis. Asa cause of meningitis, H. influenzae has fallen from 45.0% in 1986(12) to 6.7% in 2003 to 2007 (14). L. monocytogenes is also aninfrequent cause of meningitis; however, it is associated with highmortality rates (17.0% to 28.0%) (14, 42, 43). L. monocytogenesmeningitis occurs primarily in children of 2 months of age andin immunocompromised and elderly individuals (14, 42, 43). Thesigns and symptoms of L. monocytogenes meningitis are not dif-ferent from those associated with other causes of community-acquired meningitis, but CSF findings may be atypical (43, 44).Listeriosis is associated with the consumption of contaminatedfood, implicating the gastrointestinal tract as the portal of entry tothe bloodstream.
Group B streptococcus and E. coli are common causes of men-ingitis in neonates (45, 46), with group B streptococcus account-ing for 86.1% of bacterial meningitis cases in patients of 2
months of age (14). Gram-negative aerobic bacteria, such as Kleb-siella pneumoniae, Serratia marcescens, Salmonella spp., and Pseu-domonas aeruginosa, can occasionally be responsible for meningi-tis in certain patient groups, including infants and patients withhead injuries or those undergoing postneurosurgical proceduresor immunosuppression (31, 47, 48). M. tuberculosis is a commoncause of chronic or subacute meningitis (49) and is associated withnonspecific symptoms and an absence of neck stiffness duringearly disease (50). Tuberculosis meningitis occurs following he-matogenous spread of bacilli from the lungs and the establishmentof a caseating Rich focus (tuberculous granuloma) in the braincortex, meninges, or choroid plexus. Bacteria are subsequentlyreleased from the foci and enter the subarachnoid space (51).
Encephalitis
In certain circumstances, acute meningitis can be clinically indis-tinguishable from acute encephalitis, which refers to inflamma-tion of the brain parenchyma in association with neurologic dys-function (52). Encephalitis is typically characterized by headachewith an acute confusional state, with or without seizures. TheCalifornia Encephalitis Program identified the clinical profilesand etiologies of encephalitis in a large cohort of immunocompe-tent patients from 1998 to 2005 (7). A confirmed or probableetiology was identified in only 15.8% of cases; among these, vi-ruses were the causative agent in 68.5% of cases. Herpes simplexvirus is the most common cause of encephalitis in Western coun-tries (6, 53, 54). Enteroviruses, varicella-zoster virus, Epstein-Barrvirus, measles virus, and arboviruses, such as Japanese encephali-tis virus, West Nile virus, and Murray Valley encephalitis virus,have also been implicated as causes of encephalitis (6, 7, 54, 55).Beckham and Tyler provided a comprehensive list of other impor-tant and emerging viral causes of encephalitis (52). L. monocyto-genes may cause meningoencephalitis, a syndrome where featuresof both meningitis and encephalitis are present.
Burkholderia pseudomallei, the causal agent of melioidosis, has arelatively uncommon association with CNS involvement, ac-counting for around 4% of cases in northern Australia (56, 57),with distinctive clinical features being brain stem encephalitis, of-ten with cranial nerve palsies, together with peripheral motorweakness, or occasionally just flaccid paraparesis alone (myelitis),and presenting with urinary retention (5658). Fevers are usuallya prominent feature, and headaches are common, but neckstiffness is usually mild or absent. The computed tomography(CT) scan is often normal, but dramatic changes are seen onmagnetic resonance imaging, most notably a diffusely increasedT2-weighted signal in the midbrain, brain stem, and spinal cord,with variable symmetry and enhancement with gadolinium. CSFshows high protein, normal or slightly decreased glucose, and,most notably, a pleocytosis with lymphocytes usually predomi-nant. Bulbar palsy and decreased respiratory drive often necessi-tate ventilation, which may be required for many weeks (56, 5962). In northern Australia, patients infected with the flavivirusMurray Valley encephalitis virus can present with clinical featuresindistinguishable from those seen with melioidosis encephalomy-elitis.
Neurologic melioidosis is occasionally seen outside Australia,although it appears to be less common in melioidosis patients inSoutheast Asia than in Australia. Rather than the distinctive brainstem encephalitis and/or myelitis seen in Australia, patients withneurological melioidosis in Southeast Asia usually present with
Bacterial Mechanisms of Brain Invasion
October 2014 Volume 27 Number 4 cmr.asm.org 693
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://cmr.asm.orghttp://cmr.asm.org/macroscopic cortical brain abscesses (63), suggesting that in thesecases there has been bacteremic spread to the brain. Frank men-ingitis is rarely seen in melioidosis. A recent report described thefirst case of neurological melioidosis in the United States, in a58-year-old male who presented with low-grade fever, nausea,vomiting, headaches, diplopia, left-sided ptosis, and transient ep-isodes of marked somnolence, after recent travel to Cambodia(64). CSF demonstrated increased levels of glucose, protein, andlymphocytes; however, microbiological investigation consistentlyshowed no organisms by Gram stain and failed to detect any or-ganisms on culture medium. B. pseudomallei was diagnosed onlyfollowing the culture of biopsy material collected during a suboc-cipital craniectomy. The mortality of neurological melioidosis isup to 30%, with ongoing residual neurological deficits in up to50% of patients overall (5658).
Focal Infections
The range of focal CNS infections includes brain abscesses, sub-dural empyema, and epidural abscesses. Brain abscess refers to anintracerebral infection that usually begins as localized cerebritis,which develops into a collection of pus that is surrounded by awell-vascularized capsule (65). The clinical presentations of brainabscesses are variable and depend on the anatomical area of thebrain that is compressed or affected. Brain abscesses commonlyoriginate from a contiguous focus of infection, such as the middleear, mastoid cells, or paranasal sinuses. Brain abscesses may alsooccur following (i) hematogenous spread of bacteria from a dis-tant focus of infection or (ii) brain trauma or neurosurgery (66). Arecent systematic review and meta-analysis of 123 brain abscessstudies reported between 1935 and 2012 demonstrated that Strep-tococcus and Staphylococcus spp. were the most frequently isolatedmicroorganisms, causing 34.9% and 18.9% of infections, respec-tively (67). Gram-negative enteric bacteria were responsible for15.0% of cases of brain abscess and were frequently associatedwith polymicrobial infections. Other, less common causativeagents include anaerobic bacteria (Bacteroides spp., Peptostrepto-coccus spp., and Fusobacterium spp.), Actinomycetales, Haemophi-lus spp., and Pseudomonas spp. (6668).
Subdural empyema refers to a collection of pus in the subduralspace, which is located between the dura mater and arachnoidmater layers of the meninges (see Barriers of the CNS, below). Incontrast, epidural abscesses are defined as a collection of pus be-tween the dura mater and the skull or vertebral column (69). Theetiologies of subdural empyema and epidural abscesses are similarto those of brain abscesses; however, due to the anatomical loca-tion of these infections, bacteria do not need to penetrate theblood-brain barrier (BBB) to establish disease.
BARRIERS OF THE CNS
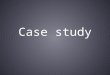
The CNS is physically protected from injury by bony structures,such as the vertebrae and the cranium, and is also enveloped by themeninges and surrounded by CSF. The meninges comprise threelayers: the dura mater, arachnoid mater, and pia mater. The arach-noid mater and pia mater are separated by the subarachnoidspace, which is filled with CSF that is produced by the choroidplexus in the ventricles of the brain (Fig. 1) (70). The CSF providesmechanical support, regulates ion composition, and maintainschemical stability. Once it has circulated through the ventricles ofthe brain, the CSF enters the subarachnoid space and drains intothe blood through arachnoid villi and granulations. CSF also
drains through the cribriform plate into the lymphatics within thenasal mucosa (7173).
The complex functions of the brain are dependent on homeo-static mechanisms that regulate the ionic composition of the in-terstitial fluid that surrounds neurons in the parenchyma (74).This homeostasis is maintained by two cellular barriers which sep-arate the CNS from the systemic circulation: the BBB and thebrain-CSF barrier (BCSFB) (Fig. 1). These barriers protectthe brain from abrupt changes in blood biochemistry while at thesame time allowing delivery of nutrients and removal of metabo-lites. Importantly, these barriers also protect the CNS from inva-sion by microbes that may be present within the blood.
The Blood-Brain Barrier
The BBB (Fig. 1) exists at the level of cerebral microvessels andrepresents the largest interface for blood-brain exchange (75). TheBBB is composed of endothelial cells that line cerebral microves-sels in association with pericytes, astrocytes, and the basementmembrane (collectively referred to as a neurovascular unit, in as-sociation with neurons, microglia, and peripheral immune cells).Pericytes are attached to the abluminal surface of the endotheliumand, together with the astrocytic end feet, form a contiguousmembrane barrier. A physical barrier is formed at the interendo-thelial cleft by complex junctions that regulate the flux of ions,polar molecules, and macromolecules from the systemic circula-tion (74, 75).
At the interendothelial cleft, two types of junctions comprisethe BBB: adherens junctions and tight junctions. These junctionsblock the transport of a wide range of molecules, restricting para-cellular permeability across the BBB (75). In addition, endothelialcells forming the BBB lack fenestrations in their plasma mem-branes and have a reduced number of pinocytotic vesicles com-pared to endothelial cells in other tissues, which restricts transcel-lular flux (76). Despite this, certain solutes and macromoleculesmay be transported across the BBB via specific and nonspecificmechanisms, such as passive diffusion and receptor and/or ad-sorption-mediated transcytosis, or via ATP-binding cassettetransporters and solute carrier transporters, which are expressedon cerebral microvessels (75, 7779). The transcellular and para-cellular routes of entry to the CNS are highly relevant for micro-bial pathogens.
The Blood-Cerebrospinal Fluid Barrier
The BCSFB (Fig. 1) is formed by tight junctions between (i) epi-thelial cells located at the choroid plexus, in the lateral, third, andfourth ventricles of the brain; and (ii) endothelial cells of the veinsand venules within the subarachnoid space. Tight junctions be-tween the epithelial cells of the arachnoid mater also contribute tothe BCSFB by forming a barrier between the subarachnoid spaceand the leaky fenestrated blood vessels of the dura mater. Of theseBCSFB locations, the choroid plexus has a large vascular surfacearea and represents the major interface between fenestrated bloodvessels and CSF. Similar to the BBB, the BCSFB functions to pro-tect the CNS and helps to maintain homeostasis; however, thechoroidal epithelial cells of the BCSFB also secrete CSF from thechoroid plexus into the brain ventricular system, and the tightjunctions between the epithelial cells have a lower electrical resis-tance than that of BBB endothelial cells (80). Thus, the choroidplexus BCSFB may be more vulnerable to microbial penetrationvia paracellular mechanisms. The BCSFB at the arachnoid mater
Dando et al.
694 cmr.asm.org Clinical Microbiology Reviews
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://cmr.asm.orghttp://cmr.asm.org/has a smaller total surface area than those of other barriers of theCNS and is not thought to be an important route for the entry ofsolutes into the brain (74). However, the arachnoid BCSFB mayrepresent an important site of microbial entry.
Immunosurveillance of the CNS
The brain parenchyma and spinal cord are populated throughoutby resident immune cells, the microglia, which are highly special-ized tissue macrophages that are maintained through in situ self-renewal without reconstitution from the bone marrow (8183).
Microglia continuously survey the brain parenchyma by samplingtheir microenvironment with highly motile processes and protru-sions (84). Recent data have also revealed that cells expressingCD11c are localized within the juxtavascular parenchyma of thehealthy mouse brain and extend processes to the glia limitans(astrocytic foot processes at the parenchymal basement mem-brane, surrounding the brain under the pia mater) (85). In agree-ment with a previous study (86), this raises the possibility thatdendritic cells, which are characterized by high-level CD11c ex-pression, may reside within the brain parenchyma. However, a
FIG 1 Anatomical locations and organizations of the blood-brain and blood-cerebrospinal fluid barriers and the olfactory portal. The skull and the meninges,which consist of the dura mater, arachnoid mater, and pia mater, protect the brain. The arachnoid mater and pia mater are connected by strands of connectivetissue called arachnoid trabeculae, which course through the CSF-containing subarachnoid space. At the cellular level, the BBB and BCSFB maintain homeostasisof the brain. The BBB is formed by tight junctions between endothelial cells lining cerebral microvessels, in addition to pericytes and astrocytes. The BCSFB isformed by tight junctions between (i) epithelial cells at the choroid plexus, (ii) endothelial cells of the veins and venules within the subarachnoid space, and (iii)the epithelial cells of the arachnoid mater. The olfactory system bypasses the cellular barriers of the CNS and provides a direct portal from the nasal cavity to theolfactory bulb within the brain.
Bacterial Mechanisms of Brain Invasion
October 2014 Volume 27 Number 4 cmr.asm.org 695
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://cmr.asm.orghttp://cmr.asm.org/range of cells of the myeloid lineage (including activated micro-glia) also express CD11c, albeit at lower levels. Thus, the CD11c-expressing cells described within the brain parenchyma may alsorepresent a subpopulation of microglia (85).
Other resident immune cells of the CNS include perivascularmacrophages in addition to small populations of blood-deriveddendritic cells and macrophages within the choroid plexus andmeninges. Dendritic cells constitute approximately 1% of im-mune cells within the choroid plexus and meninges (87, 88), butunlike the putative dendritic cells of the brain parenchyma, cho-roid plexus and meningeal dendritic cells are distinct from micro-glia and closely resemble classical dendritic cells that require FMS-like receptor tyrosine kinase 3 ligand for development (88). TheCSF also contains a trafficking population of mononuclear cells,comprising T cells (90%), B cells (5%), monocytes (5%), and den-dritic cells (1%) (89).
Normal CNS immune surveillance occurs when centralmemory T cells migrate from the blood across the choroidplexus epithelium, enter the CSF, and scan the subarachnoidspace. In the absence of recognizing ligands presented by localantigen-presenting cells, T cells exit the subarachnoid spaceand drain to the secondary lymphoid organs via the nasal mu-cosa (90, 91). In contrast, recognition of presented antigensresults in the formation of immunological synapses and is ac-companied by cellular signaling that results in the recruitmentof peripheral inflammatory cells to the CNS via paracellular ortranscellular diapedesis (92).
The production of cytokines, free radicals (such as reactive ox-ygen species), and matrix metalloproteinases by inflammatorycells within the CSF spaces can subsequently result in degradationof the glia limitans, BBB/BCSFB dysfunction, and cellular death(9395). In bacterial meningitis, neuronal injury also occurs dueto the direct effects of bacterial toxins and virulence factors (9698). A recent study of human bacterial meningitis cases demon-strated that the profile of pro- and anti-inflammatory cytokinesand matrix metalloproteinases within the CSF is dependent uponthe causative pathogen (99). The sequelae of bacterial meningitisand the associated neuroinflammation include vasculitis and ce-rebral venous thrombosis, which can lead to cerebral ischemia. Anincrease in CSF outflow resistance in combination with interstitialedema results in raised intracranial pressure, which causes hy-poxic brain damage and may lead to death (100).
MICROBIAL ENTRY TO THE CNS
Microbial pathogens may access the CNS (i) by penetrating theBBB or the BCSFB or (ii) via the olfactory and/or trigeminalnerves (101). Peripheral nerves other than the olfactory and tri-geminal cranial nerves have also been implicated as routes of entryfor some viruses, but these are not reviewed here. Penetrations ofthe BBB and BCSFB represent common routes of CNS invasion,resulting in encephalitis or brain abscesses and in meningitis, re-spectively. In contrast to a diverse group of neurotropic viruses forwhich mechanisms are described for invasion of the brain via theolfactory sensory nerves, bacterial infection via the olfactory epi-thelium and the olfactory nerve bundles has been described infre-quently. Even less well understood is the fact that, in addition tothe olfactory nerve, the trigeminal nerve may also present a poten-tial pathway to the brain.
In Vivo and In Vitro Models of CNS Invasion
Much of our understanding of the mechanisms of microbial CNSinvasion has been obtained from in vivo and in vitro studies. Miceand rats are the most common animals used to model CNS infec-tions. These animal models have been used to investigate the sitesof microbial entry (20, 102106) and the roles of virulence deter-minants in CNS invasion and pathogenesis (107111). Despiteclear differences in the size and complexity of mouse and humanbrains, comparative transcriptomic studies between mice and hu-mans have demonstrated that gene expression profiles of thehealthy brain and choroid epithelium are highly conserved be-tween the species (112114).
There are, however, several important differences between themouse and human CNS that are relevant to microbial invasionstudies. In mice, the leptomeninges (comprising the arachnoidmater and pia mater) are significantly thinner and less vascularthan the case in humans (115). Additionally, the human choroidplexus epithelium has more abundant fibrovascular stroma alongthe vascular channels and a relatively larger surface area than thoseof the mouse choroid epithelium. Mice also possess very largeolfactory bulbs compared to humans (115), which may result in ahigher incidence of CNS invasion via the olfactory route than thecase in humans. Furthermore, mice lack several anatomically de-fined subclasses of astrocytes that are present in humans (116).These combined anatomical differences may influence the initialsite of microbial attachment and subsequent CNS invasion.
In vitro cell culture systems have been used to model the BBBand to elucidate the cellular and molecular mechanisms of micro-bial CNS invasion. Primary human, rodent, and bovine brain mi-crovascular endothelial cells have been used in some studies (97,117119); however, the isolation of these cells is technically demand-ing, and in vitro culture dramatically alters the transcriptome, leadingto downregulation of genes involved in BBB function (120, 121).Human umbilical vein endothelial cells (HUVECs) (122124),Caco-2 cells, and Madin-Darby canine kidney cells (125) have beenused as surrogate models of the BBB, although the noncerebral originof these cells may limit their relevance. The availability of immortal-ized brain endothelial cell lines (for example, human brain microvas-cular endothelial cells [HBMECs], hCMEC/D3, TY10, and BB19) hasenabled the human BBB to be studied. When grown on Transwellmembranes, HBMECs (i) form tight junctions, as measured by tran-sendothelial electrical resistance; (ii) express the adherens junctionand tight junction proteins zonula occludens-1, junctional adhesionmolecule A, claudin-5, occludin, and vascular endothelial cadherin;and (iii) demonstrate negligible paracellular permeability (126129).
It must be noted that brain microvascular endothelial cellsgrown in static monocultures represent a surrogate model for thehuman BBB, as they lack other components of the neurovascularunit that are required for the development of true BBB properties.Studies using pericyte-deficient mice have shown that pericytes(Fig. 1) are required for BBB integrity. Compared to wild-typemice, pericyte-deficient mice demonstrated an accumulation ofwater and tracer dyes within the brain, structural abnormalities incerebral endothelial tight junctions, and increased expression ofgenes known to increase vascular permeability, endothelial vesicletrafficking, and immune cell recruitment (130132). Astrocytesalso play a key role in regulating the BBB (133136), and as such,a range of coculture systems have been developed to more closelymodel the BBB properties of the neurovascular unit (137139).
Dando et al.
696 cmr.asm.org Clinical Microbiology Reviews
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://cmr.asm.orghttp://cmr.asm.org/Choroid plexus epithelial cell lines that display the characteristicproperties of the BCSFB have been described (140, 141); however,the majority of in vitro microbial invasion studies have been per-formed using monocultures of brain microvascular endothelialcells.
BACTERIAL INVASION THROUGH THE BLOOD-BRAIN ANDBLOOD-CEREBROSPINAL FLUID BARRIERS
Sites of Entry
Classical bacterial meningeal pathogens may potentially enter theCSF by penetrating the BBB of cerebral microvessels and enteringthe extracellular fluid of the brain, which is continuous with theCSF. However, a more likely route involves direct entry to the CSFvia penetration of the BCSFB at either the arachnoid or the cho-roid plexus (142). The highly vascularized choroid plexus has beenfavored as a major site of bacterial entry to the CSF due to lowerelectrical resistances between choroid epithelial cells. Autopsies ofneonates who died from bacterial meningitis demonstrated thatmeningitis was frequently (84.0%) associated with an accumula-tion of a purulent exudate within the ventricles (ventriculitis) andthe choroid plexus (plexitis) (143). Ventriculitis preceding men-ingitis would support the role of the choroid plexus as the initialsite of bacterial invasion; however, ventriculitis frequently occursas a complication of meningitis, and the site of bacterial CNSinvasion remains incompletely understood.
In experimentally infected rhesus macaques, the choroid plexuswas the site where the earliest histopathologic lesions were ob-served in H. influenzae meningitis (144). Following intranasal in-oculation, H. influenzae was isolated from the CSF within the lat-eral cerebral ventricle, and this was associated with intravascularinflammatory infiltration and mild choroid plexitis (145). In 5- to7-week-old pigs, S. suis was localized within the choroid plexusand caused disruption of the brush border of the choroid epithe-lium and loss of the apical cytoplasm (146). Interestingly, autopsyof a 2-month-old infant who died of fulminant meningococcemiaprior to the onset of meningitis revealed adherent bacteria withinthe capillaries of the choroid plexus and, to a much lesser extent,the capillaries within the meninges (147). This would appear tosupport the choroid plexus as the preferential site of N. meningi-tidis entry to the CSF; however, no bacteria were found within orbetween choroid epithelial cells. In contrast, a study of autopsymaterial from symptomatic patients with meningococcal diseaserevealed the presence of N. meningitidis within the choroid plexusepithelium, interstitium, and blood vessels (148).
Neonatal rat models of E. coli meningitis have been used toidentify the potential site of entry to the CSF. Parkkinen et al.demonstrated that E. coli binds to the luminal surfaces of choroidepithelial cells, vascular endothelial cells, and ependymal cells lin-ing the brain ventricles (102). Similar findings were reported byZelmer et al., who suggested that E. coli K1 enters the CSF via thechoroid plexus, circulates to the subarachnoid space, and thenadheres to the meninges (103). In contrast, Kim et al. reported thatin the brains of 5-day-old rats, E. coli was localized within theperivascular areas of the subarachnoid space, not within the cho-roid plexus (20). Recently, the spatiotemporal events of CNS in-vasion were investigated in a BALB/c mouse model of pneumo-coccal meningitis (104). S. pneumoniae preferentially adhered tovessels within the subarachnoid space at 1 h postinfection andformed clusters around the endothelium at this location at later
time points. Remarkably, pneumococci could be detected in thechoroid plexus only at 8 h postinfection, suggesting that this is notthe site of initial entry to the CSF.
Mechanisms of Entry
Bacteria may cross the BBB and BCSFB to access the CNS bytranscellular penetration or paracellular entry or via infected leu-kocytes from the peripheral circulation (the Trojan horse mech-anism) (Fig. 2). Transcellular penetration occurs following bacte-rial adhesion to endothelial or epithelial cells. Bacteria aresubsequently translocated across these barriers by pinocytosis orreceptor-mediated mechanisms. Alternatively, bacteria may in-vade the CNS paracellularly following disruption of the tight junc-tions between cells forming the BBB and/or BCSFB, resulting inincreased permeability. Microorganisms may exploit more thanone of these mechanisms to access the CNS.
Bacterial attachment to HBMECs is a prerequisite for transcel-lular and paracellular penetration. There has been significant re-search into the host-pathogen interactions that occur prior to bac-terial invasion of brain microvascular endothelial cells (Table 1),including the identification of host receptors that mediate theseinteractions. E. coli, H. influenzae, N. meningitidis, and S. pneu-moniae bind to HBMECs via the 37/67-kDa laminin receptor(149152). The 37-kDa laminin receptor is a precursor for themature, 67-kDa laminin receptor, which binds laminin-1 withinthe basement membrane on the abluminal surface of eukaryoticcells (153). Kim et al. (150) demonstrated that the 67-kDa lamininreceptor is expressed on the basolateral side of HBMECs (i.e., theabluminal surface); however, cytoxic necrotizing factor 1 (CNF-1)of E. coli triggered clustering of the 67-kDa laminin receptor on
FIG 2 Mechanisms of blood-cerebrospinal fluid penetration by bacterialpathogens. Bacteria (purple) may invade the CNS via the BCSFB by transcel-lular penetration involving either pinocytosis or receptor-mediated mecha-nisms (A); by paracellular entry following the disruption of junctions (com-prising tight junctions and adherens junctions) between choroidal epithelialcells, endothelial cells of veins/venules within the subarachnoid space, or thecells of the arachnoid membrane (B); and by the Trojan horse mechanism,where microbes may transmigrate with infected leukocytes (such as macro-phages, as shown) (C).
Bacterial Mechanisms of Brain Invasion
October 2014 Volume 27 Number 4 cmr.asm.org 697
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://cmr.asm.orghttp://cmr.asm.org/TA
BLE
1K
now
nba
cter
iall
igan
dsan
dth
eir
hos
tre
cept
ors
for
adh
esio
nto
and
inva
sion
ofth
ebl
ood-
brai
nba
rrie
ra
Bac
teri
alpa
thog
enL
igan
dH
BM
EC
rece
ptor
Fun
ctio
nR
efer
ence
(s)
Esc
heri
chia
coli
(an
dot
her
Gra
m-
neg
ativ
een
teri
cs)
Fim
HC
D48
Adh
esio
nto
HB
ME
Cs;
Fim
Hal
sopr
omot
esin
vasi
onby
acti
vati
onof
Rh
oA,w
hic
hin
duce
sh
ost
cyto
skel
etal
rear
ran
gem
ents
154,
410
Nlp
1U
nkn
own
Adh
esio
nto
and
inva
sion
ofH
BM
EC
s;N
lp1
acti
vate
sh
ost
cyto
solic
phos
phol
ipas
eA
2
174
Om
pAgp
96h
omol
ogu
eLo
ops
1,2,
and
3of
Om
pAfu
nct
ion
inad
hes
ion
toan
din
vasi
onof
HB
ME
Cs;
Om
pA-m
edia
ted
inva
sion
isdu
eto
Rac
1ac
tiva
tion
and
acti
vati
onof
hos
tcy
toso
licph
osph
olip
ase
A2
161,
162,
173,
178
CN
F-1
37/6
7-kD
ala
min
inre
cept
orIn
vasi
onof
HB
ME
Cs;
CN
F-1
acti
vate
sR
hoA
and
recr
uit
sfo
cala
dhes
ion
kin
ase
toth
esi
teof
bact
eria
len
try
149,
150,
171,
172
IbeA
Vim
enti
n,P
SFIn
vasi
onof
HB
ME
Cs;
acti
vate
sR
ac1
178,
411
413
Ibe1
045
-kD
aIb
e10
rece
ptor
Inva
sion
ofH
BM
EC
s41
4,41
5A
slA
Un
know
nIn
vasi
onof
HB
ME
Cs
416
Tra
JU
nkn
own
Inva
sion
ofH
BM
EC
s41
7Y
ijPU
nkn
own
Inva
sion
ofH
BM
EC
s41
8Fl
agel
laU
nkn
own
Adh
esio
nto
and
inva
sion
ofH
BM
EC
s41
9
Hae
mop
hilu
sin
fluen
zae
Ph
osph
oryl
chol
ine
PA
Fre
cept
orP
oten
tial
lyin
volv
edin
inva
sion
ofH
BM
EC
s42
0O
mpP
237
/67-
kDa
lam
inin
rece
ptor
Adh
esio
nto
HB
ME
Cs
151,
152
List
eria
mon
ocyt
ogen
esIn
lAE
-cad
her
inIn
vasi
onof
pola
rize
dh
um
anch
oroi
dpl
exu
sep
ith
elia
lcel
ls23
2In
lBgC
1q-R
,met
rece
ptor
tyro
sin
eki
nas
eIn
vasi
onof
HB
ME
Cs
and
pola
rize
dh
um
anch
oroi
dpl
exu
sep
ith
elia
lcel
ls21
3,23
2,42
1,42
2V
ipgp
96In
vasi
onof
the
brai
nin
vivo
160
IspC
Un
know
nA
dhes
ion
toan
din
vasi
onof
shee
pch
oroi
dpl
exu
sep
ith
elia
lcel
lsbu
tn
otH
BM
EC
s23
3
Myc
obac
teri
umtu
berc
ulos
isR
v098
0c,R
v098
7,R
v098
9c,
Rv1
801
Un
know
nIn
vasi
onof
HB
ME
Cs
118
HB
HA
Hep
aran
sulf
ate
glyc
osam
inog
lyca
ns
Adh
esio
nto
and
inva
sion
ofB
BM
EC
s23
4R
v031
1,R
v080
5,R
v093
1c,
Rv0
986,
MT
3280
Un
know
nIn
vasi
onof
HB
ME
Cs
235
Pkn
DLa
min
inA
ttac
hm
ent
to,i
nva
sion
of,a
nd
surv
ival
wit
hin
HB
ME
Cs
158
Nei
sser
iam
enin
giti
dis
Typ
eIV
pili
Un
know
nA
dhes
ion
toH
BM
EC
s;ty
peIV
pilu
s-m
edia
ted
adh
esio
nle
ads
toth
efo
rmat
ion
ofco
rtic
alpl
aqu
esan
dh
ost
mem
bran
epr
otru
sion
s12
2,12
4
PilQ
and
Por
A37
/67-
kDa
lam
inin
rece
ptor
Adh
esio
nto
HB
ME
Cs
151,
152
Opc
5
1in
tegr
in(m
edia
ted
bybi
ndi
ng
toth
ebr
idgi
ng
mol
ecu
les
vitr
onec
tin
and
fibr
onec
tin
)
Adh
esio
nto
and
inva
sion
ofH
BM
EC
s;ac
tiva
tes
JNK
1,JN
K2,
p38,
and
prot
ein
tyro
sin
eki
nas
esi
gnal
ing
155,
191,
192
Stap
hylo
cocc
usau
reus
Ypf
Pan
dL
TA
Un
know
nIn
vasi
onof
HB
ME
Cs
423
Stre
ptoc
occu
sag
alac
tiae
Lmb
Lam
inin
Inva
sion
ofH
BM
EC
s15
9Ia
gAan
dL
TA
Un
know
nIn
vasi
onof
HB
ME
Cs;
IagA
anch
ors
LTA
toth
est
rept
ococ
calc
ellw
alla
nd
isre
quir
edfo
rin
vasi
on42
4
FbsA
Fibr
inog
enA
dhes
ion
toH
BM
EC
s15
6Sf
bAIn
tegr
ins
(via
S.ag
alac
tiae
bin
din
gto
imm
obili
zed
fibr
onec
tin
)In
vasi
onof
HB
ME
Cs
199
Dando et al.
698 cmr.asm.org Clinical Microbiology Reviews
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://cmr.asm.orghttp://cmr.asm.org/the apical side (i.e., the luminal surface), where it could potentiallyinteract with bacteria within the cerebral microvasculature. In anin vivo model, Orihuela et al. reported that fluorescent micro-spheres coated with laminin receptor-binding adhesins (such ascholine-binding protein A [CbpA] of S. pneumoniae) adhered tothe cerebral endothelium of mice via the 37/67-kDa laminin re-ceptor following intravascular injection, as demonstrated by cra-nial window imaging (151). Several bacterial meningeal patho-gens have been shown to bind host glycoproteins, such asfibrinogen, vitronectin, fibronectin, laminin, and collagen, whichmay act as bridging molecules between the bacterium andHBMECs (109, 154159). In addition, the heat shock proteingp96 and a gp96 homologue act as receptors for the surface-ex-pressed virulence protein (Vip) of L. monocytogenes (160) andouter membrane protein A (OmpA) of E. coli (161, 162), respec-tively.
Transcellular Penetration of Brain MicrovascularEndothelial Cells
Transcellular penetration of brain microvascular endothelial cells,mainly via receptor-mediated mechanisms (Fig. 2), has been dem-onstrated for several bacteria, including E. coli, N. meningitidis, S.pneumoniae, group B streptococcus, S. suis, L. monocytogenes, andM. tuberculosis.
E. coli. E. coli translocates from the upper compartment to thelower compartment in an HBMEC Transwell model without increas-ing cellular permeability, thus supporting a transcellular mechanismof penetration (163). Electron microscopy studies have demon-strated that E. coli invades HBMECs through a zipper-like, recep-tor-mediated endocytosis mechanism (164). Intracellular E. coliE44 bacteria were observed in membrane-bound vesicles withinHBMECs at 30 min postinfection; by 45 min, the bacteria hadtranslocated to the basolateral side (164). Both early (early endo-some antigen 1 and transferrin receptor) and late (Ras-relatedprotein 7 and lysosome-associated membrane protein 1) endo-somal markers were recruited to vacuoles containing E. coli K1.However, the lysosomal hydrolytic enzyme cathespin D did notaccumulate within the vacuoles, demonstrating that lysosomal fu-sion was prevented. This was found to occur in a capsule-depen-dent manner (165).
Several E. coli proteins contribute to the adhesion to and inva-sion of HBMECs (Table 1). Attachment of E. coli to HBMECsinduces host cytoskeletal rearrangements and actin condensationbelow adherent bacteria (164). This is associated with a CNF-1-mediated recruitment of focal adhesion kinase and the cytoskel-etal protein paxillin to the 67-kDa laminin receptor, which formsclusters that colocalize with adherent E. coli (150). Interactionsbetween E. coli and HBMECs result in tyrosine phosphorylation offocal adhesion kinase and paxillin. The activity of focal adhesionkinase and its autophosphorylation site, tyrosine 397, were shownto be essential for E. coli invasion of HBMECs (166). Furthermore,the Src kinase-dependent activation of phosphatidylinositol 3-ki-nase and its interaction with focal adhesion kinase were requiredfor E. coli K1 invasion and host cytoskeletal rearrangement (167,168). Sukumaran and Prasadarao demonstrated that the associa-tion of phosphatidylinositol 3-kinase with focal adhesion kinaseresulted in the downstream activation of protein kinase C(PKC) in an Omp-A-dependent manner (169). Activated pro-tein kinase C was recruited to the E. coli entry site, where itinteracted with its substrate (myristoylated alanine-rich C kinase
PilA
2
1in
tegr
in(m
edia
ted
byS.
agal
acti
aebi
ndi
ng
toim
mob
ilize
dco
llage
n)
Adh
esio
nto
and
inva
sion
ofH
BM
EC
s;P
ilAbi
ndi
ng
stim
ula
tes
foca
ladh
esio
nki
nas
eph
osph
oryl
atio
nan
ddo
wn
stre
amph
osph
atid
ylin
osit
ol3-
kin
ase
acti
vati
on
109,
425
PilB
Un
know
nIn
vasi
onof
HM
BE
Cs
425
Srr-
1Fi
brin
ogen
(Srr
-1bi
nds
amin
oac
ids
283
to41
0of
the
fibr
inog
en
chai
nvi
aa
dock
,loc
k,an
dla
tch
mec
han
ism
)
Adh
esio
nto
and
inva
sion
ofH
BM
EC
s20
0,20
1,42
6
Hvg
AU
nkn
own
Adh
esio
nto
HB
ME
Cs
198
AC
PG
lyco
sam
inog
lyca
ns
Adh
esio
nto
and
inva
sion
ofH
BM
EC
s;in
vasi
onpo
ten
tial
lyoc
curs
follo
win
gR
ho
GT
Pas
e-de
pen
den
tac
tin
rear
ran
gem
ents
157,
427
Stre
ptoc
occu
spn
eum
onia
eC
bpA
37/6
7-kD
ala
min
inre
cept
orA
dhes
ion
toH
BM
EC
s15
1P
hos
phor
ylch
olin
eP
AF
rece
ptor
Inva
sion
ofH
BM
EC
s;bi
ndi
ng
topl
atel
etac
tiva
tin
gfa
ctor
rece
ptor
indu
ces
colo
caliz
atio
nof
-a
rres
tin
193,
197
Nan
AU
nkn
own
Adh
esio
nto
and
inva
sion
ofH
BM
EC
s19
4,19
5a
AC
P,a
lph
aC
prot
ein
;Asl
A,a
ryl-
sulf
ates
ulf
ohyd
rola
se;B
BM
EC
,bov
ine
brai
nm
icro
vasc
ula
ren
doth
elia
lcel
ls;C
bpA
,ch
olin
ebi
ndi
ng
prot
ein
A;C
NF-
1,cy
toto
xic
nec
roti
zin
gfa
ctor
1;Fb
sA,fi
brin
ogen
-bin
din
gpr
otei
n;F
imH
,typ
e1
fim
bria
ladh
esin
;HB
HA
,hep
arin
-bin
din
gh
emag
glu
tin
inad
hes
in;H
BM
EC
s,h
um
anbr
ain
mic
rova
scu
lar
endo
thel
ialc
ells
;Hvg
A,h
yper
viru
len
tgr
oup
Bst
rept
ococ
cus
adh
esio
n;I
beA
,in
vasi
onof
brai
nen
doth
elia
lcel
lpro
tein
A;I
agA
,in
vasi
on-a
ssoc
iate
dge
ne
A;I
nlA
,in
tern
alin
A;I
nlB
,in
tern
alin
B;L
TA
,lip
otei
choi
cac
id;L
mb,
lam
inin
-bin
din
gpr
otei
n;N
anA
,neu
ram
inid
ase
A;N
lp1,
new
lipop
rote
in1;
Om
pP2,
oute
rm
embr
ane
prot
ein
P2;
Opc
,ou
ter
mem
bran
epr
otei
nC
;PA
F,pl
atel
etac
tiva
tin
gfa
ctor
;PilQ
,pilu
sse
cret
inpr
otei
n;P
orA
,maj
orou
ter
mem
bran
epr
otei
n;P
SF,p
olyp
yrim
idin
e-tr
act-
bin
din
gpr
otei
n(P
TB
)-as
soci
ated
splic
ing
fact
or;S
fbA
,str
epto
cocc
alfi
brin
ogen
bin
din
gpr
otei
nA
;Srr
-1,s
erin
e-ri
chre
peat
1;V
ip,v
iru
len
cepr
otei
n.
Bacterial Mechanisms of Brain Invasion
October 2014 Volume 27 Number 4 cmr.asm.org 699
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://cmr.asm.orghttp://cmr.asm.org/substrate), leading to an accumulation of actin (169). The activatedprotein kinase C also interacted with caveolin-1 colocalized withcondensed actin underneath the bacterial entry site to form caveolae,which are plasma membrane invaginations that are involved in en-docytosis and signal transduction (170). CNF-1 (via the 37/67-kDalaminin receptor) and type 1 fimbrial adhesin (FimH; via CD48) havealso been shown to induce cytoskeletal rearrangements through acti-vation of the GTPase RhoA (149, 171, 172).
In an independent mechanism, E. coli OmpA and new lipopro-tein 1 (Nlp1) promote the activation of host cytosolic phospho-lipase A2 (173, 174). The activation of cytosolic phospholipase A2generated arachidonic acid metabolites, induced host actin cyto-skeletal rearrangements, and was essential for E. coli K1 invasionof HBMECs (173, 175177). OmpA and invasion of brain endo-thelial cell protein A (IbeA) also trigger the phosphorylation ofSTAT3, which results in the activation of Rac1, a Rho familyGTPase that regulates host cytoskeletal rearrangements (178).Notably, OmpA is highly conserved between Gram-negative bac-teria and may play a role in CNS invasion by those whose mecha-nisms of entry are unknown. Similarly, a B. pseudomallei toxin,Burkholderia lethal factor 1 (BLF-1), is structurally similar to E.coli CNF-1 and possesses a number of conserved residues that, inCNF-1, promote deamidation of glutamine and result in the acti-vation of RhoA and subsequent host cytoskeletal rearrangements(179). Thus, OmpA and BLF-1 may be attractive targets for futurestudies of the mechanisms of B. pseudomallei CNS invasion.
N. meningitidis. The attachment of N. meningitidis toHBMECs is mediated by type IV pili. This initial attachment isinhibited by high cerebral microcirculation shear stress levels;however, once attached, N. meningitidis proliferates and is able toresist high blood velocities by forming microcolonies with strongbacterium-bacterium interactions (124) and bacterium-host interac-tions (122). CD46 was previously identified as the receptor for type IVpili (180); however, this was not corroborated by additional studies,and it is likely that the type IV pilus attaches to host cells indepen-dently of CD46 (181). The type IV pilus protein PilQ, in addition tothe outer membrane porin PorA, was demonstrated more recently tobind to the 37/67-kDa laminin receptor on HBMECs (151). Further-more, studies with human bronchial epithelial cells show that themeningococcal type IV pilus binds to the platelet activating factor(PAF) receptor and that synergy between a pilin-linked glycan andphosphorylcholine decorating moieties is required for pili to effi-ciently engage the receptor (182).
N. meningitidis is thought to invade HBMECs primarily byparacellular mechanisms (see below); however, in vitro studieshave demonstrated that small numbers of both encapsulated andnonencapsulated meningococci are internalized by HUVECs andHBMECs (183185). Following initial bacterial attachment, themeningococcal minor pilin protein, PilV, triggers a cellular re-sponse in which endothelial cells form protrusions around N.meningitidis (122). These cellular projections further protect thebacterial microcolony from the mechanical stresses associatedwith high-velocity blood flow (122) and also lead to the engulf-ment and internalization of N. meningitidis (186). The host sig-naling events that contribute to these interactions have beenelucidated. Following type IV pilus-mediated attachment, N.meningitidis activates the host cell 2-adrenoceptor, leading to thetranslocation of -arrestin to the site of bacterial attachment at theplasma membrane (187). Several host proteins, including ezrinand moesin, which regulate the cortical cytoskeleton through F-
actin-binding sites, are then recruited to the site of bacterial at-tachment and accumulate in honeycombed molecular complexes,referred to as cortical plaques, underneath the meningococcal mi-crocolonies (186, 188, 189). The translocation of -arrestin alsoresults in the docking and activation of the protein tyrosine kinaseSrc, which phosphorylates cortactin (187, 188). Cortical actin isthen polymerized in a Rho GTPase- and Cdc42-dependent man-ner, which leads to the formation of cell membrane protrusions(186). In human bone marrow endothelial cells, the recruitmentof cortactin and formation of membrane protrusions were alsoshown to be dependent on the activation of a phosphoinositide-3-kinase/Rac1 signaling pathway by lipooligosaccharide (190).
Once internalized, the membrane-bound vesicles containingmeningococci associate with transferrin receptor and lysosome-associated membrane protein 1 endosomal markers (185). It islikely that lysosomal fusion is subverted, as live meningococcihave been shown to translocate from the basolateral side to theapical side in a Transwell BCSFB invasion model (140). In vitrostudies have demonstrated that capsular polysaccharide inhibitsthe invasion of N. meningitidis into HBMECs (191) and humanchoroid plexus epithelial cells (140) but is essential for survivaland replication within the intracellular niche (185).
For nonencapsulated meningococcal strains, the invasion ofHBMECs is dependent upon outer membrane protein C (Opc).Opc binds to the human serum factor fibronectin, which acts as abridging molecule and anchors the bacterium to the 51 integrinreceptor of HBMECs (191). This interaction results in the activa-tion of mitogen-activated protein kinase (c-Jun N-terminal kinase1 [JNK1], JNK2, and p38) and protein tyrosine kinase signal trans-duction pathways (192). Pretreatment of cells with specific JNK1,JNK2, and protein tyrosine kinase inhibitors significantly reducedthe internalization of N. meningitidis by HBMECs, without affect-ing bacterial adherence. Blocking of the 51 integrin receptor ofHBMECs also decreased JNK activation in the presence of N. men-ingitidis. Furthermore, the use of Opc-deficient mutant strainsdemonstrated that JNK signaling, but not p38 signaling, was me-diated by Opc expression (192). A more recent study identifiedthat Opc preferentially binds to activated vitronectin within hu-man serum and that this interaction promotes N. meningitidisinvasion of HBMECs (155). In vitro, the enhanced invasion ofnonencapsulated N. meningitidis strains is thought to be due to theunmasking of Opc; however, the role of Opc in vivo has yet to bedetermined.
S. pneumoniae. S. pneumoniae is internalized by human and ratbrain microvascular endothelial cells via receptor-mediated endo-cytosis. This uptake does not involve the formation of cellularmembrane protrusions as discussed for N. meningitidis (193). Theadhesion of pneumococci to HBMECs is mediated by interactionsbetween CbpA and the 37/67-kDa laminin receptor (151) andbetween neuraminidase A (NanA) and an unknown cellular re-ceptor(s) (194). Uchiyama et al. demonstrated that NanA, a sur-face-anchored sialidase, was necessary and sufficient to promotepneumococcal adhesion to and invasion of HBMECs (195). Fol-lowing initial attachment, the laminin G-like domain of NanAinitiates chemokine signaling and inflammatory activation of en-dothelial cells (194). The activation of endothelial cells results inthe increased expression of PAF receptorthe receptor for pneu-mococcal phosphorylcholine, which is a component of the cellwall and acts as a molecular mimic of the chemokine PAF (196).
In HBMECs, S. pneumoniae within vacuoles may (i) transit
Dando et al.
700 cmr.asm.org Clinical Microbiology Reviews
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://cmr.asm.orghttp://cmr.asm.org/through the cell to the basolateral surface, (ii) recycle back to theapical surface, or (iii) be killed within the vacuole (193). Opaque S.pneumoniae variants, which express more capsular polysaccharideand less phosphorylcholine than transparent variants, were effi-ciently killed, suggesting that vacuoles containing these strainswere targeted for lysosomal fusion. In contrast, transparent pneu-mococci may undergo some recycling back to the apical surface;however, by 5 h postinfection in a Transwell system, the majorityof bacteria had translocated to the basolateral chamber (193). Theinvasion of HBMECs by transparent S. pneumoniae depends onphosphorylcholine, the PAF receptor, and -arrestin, which tar-gets G-protein-coupled receptors (such as PAF receptor) to clath-rin-coated vesicles (193, 197). S. pneumoniae induces the translo-cation of -arrestin from the cytosol to the plasma membrane,where it colocalizes with the PAF receptor. This interaction alsostimulates mitogen-activated protein kinase signaling, which isrequired for pneumococcal uptake (197). Vacuoles containing S.pneumoniae colocalized with early and late endosomal markers;however, increased expression of -arrestin subverted these vac-uoles from lysosomal trafficking and promoted the transcytosis ofviable bacteria. The small number of pneumococcus-containingvacuoles that underwent recycling to the apical surface demon-strated colocalization with Ras-related protein 11, which regulatesendosome recycling. These findings suggest that the pneumococ-cus-induced interactions between PAF receptor and -arrestincontribute to the transcellular penetration of HBMECs by S. pneu-moniae (197).
Group B streptococcus. Several group B streptococcal proteinspromote adhesion to and invasion of HBMECs (Table 1). The hyper-virulent group B streptococcus adhesin (HvgA) was identified as asequence type 17 (ST-17)-specific virulence factor which is anchoredto the group B streptococcal cell wall by sortase A (198). ST-17 is aclonal complex belonging to the group B streptococcus capsular se-rotype III and is responsible for 80% of neonatal meningitis cases.Therefore, it was proposed that HvgA expression may contribute tothe hypervirulence of ST-17. In vitro studies using an isogenic hvgAmutant demonstrated that HvgA was required for efficient group Bstreptococcal adhesion to HUVECs, primary rodent choroid plexusepithelial and brain microvascular endothelial cells, and immortal-ized HBMECs. Furthermore, in a murine model of hematogenousmeningitis, HvgA was required for CNS invasion, although it had noeffect on the levels of bacteremia (198).
A common characteristic of several other group B streptococ-cal adhesins/invasins is the ability to bind components of theHBMEC extracellular matrix, such as laminin, collagen, and fi-bronectin (109, 157, 159, 199). The group B streptococcal pilus tipadhesin (PilA) and the recently identified streptococcal fibronec-tin-binding protein A (SfbA) bind immobilized collagen and fi-bronectin, respectively. The collagen and fibronectin then associ-ate with HBMECs via integrins, and these interactions facilitatethe entry of group B streptococcus (109, 199). Similarly, the groupB streptococcal serine-rich repeat 1 (Srr-1) glycoprotein binds thefibrinogen A chain within human blood through a dock, lock,and latch mechanism (200, 201). During this interaction, fi-bronectin docks between two IgG-like folds (N2 and N3 domains)of the binding region of the adhesin, which initiates a conforma-tional change whereby a flexible region of the N3 domain latchesto form a -strand and completes a -sheet within the N2 domain,effectively locking the ligand in place (200). Seo et al. demon-strated that deletion of the latch-like domain of the C-terminal
end of the Srr-1 fibrinogen-binding region significantly reducedgroup B streptococcal adhesion to HBMECs (201). The fibrino-gen-binding protein (FbsA) also mediates group B streptococcaladherence to HBMECs, by binding immobilized fibrinogen (156),although it is unknown if this interaction also occurs via a dock,latch, and lock mechanism.
Electron microscopy studies have demonstrated that in vitro,group B streptococcus associates closely with the cell membraneof HBMECs and is enveloped by microvillous structures (202).Group B streptococci are internalized within membrane-boundvesicles and translocate from the apical side to the basolateral sideof HBMECs without a marked change in transendothelial electri-cal resistance. Serotype III group B streptococci were shown toinvade HBMECs more efficiently than representative strains ofserotypes Ia, Ib, II, and V; however, the serotype III capsule itselfdid not facilitate group B streptococcal invasion (202). Internal-ized group B streptococci did not undergo significant replicationand survived within HBMECs for up to 20 h (202). Intracellularsurvival of group B streptococcus may be promoted by the CiaR-CiaH two-component regulatory system, which regulates severalgenes associated with stress tolerance and the subversion of hostdefenses (203). A serotype III strain that was deficient in the CiaRresponse regulator demonstrated adhesion and invasion levelssimilar to those of the wild-type group B streptococcus inHBMECs but was associated with a significant decrease in intra-cellular survival. Broth inhibition assays demonstrated that CiaRconferred resistance to antimicrobial peptides, lysozyme, and re-active oxygen species (203).
The host signal transduction pathways that are involved in theuptake of group B streptococcus by HBMECs are similar to thosediscussed for E. coli. In vitro, the trimolecular interactions betweenPilA, collagen, and 21 integrins on HBMECs stimulate the phos-phorylation of focal adhesion kinase at tyrosine 397, which then in-duces host cytoskeletal rearrangements and the uptake of group Bstreptococci via the recruitment and activation of phosphatidylinosi-tol 3-kinase and paxillin (109, 204). It has also been demonstratedthat group B streptococcus invasion occurs via cytoskeletal rear-rangements that are induced following the activation of RhoA andRac1 (205). Furthermore, group B streptococcus induces serine 505phosphorylation of host cytosolic phospholipase A2, which leads tothe release of arachidonic acid metabolites, including cysteinyl leuko-trienes (206). In vitro pharmacological inhibition studies demon-strated that the activation of cytosolic phospholipase A2 was requiredfor efficient group B streptococcal invasion of HBMECs. In addition,brain colonization by group B streptococcus was significantly re-duced in mice deficient in cytosolic phospholipase A2 compared towild-type animals in a model of hematogenous meningitis. Followingcytosolic phospholipase A2 activation and the release of cysteinyl leu-kotrienes, downstream signaling activates protein kinase C, which isinvolved in the regulation of actin cytoskeletal rearrangements (206).
S. suis. The zoonotic pathogen S. suis adheres to but does notinvade HBMECs in vitro (207). In contrast, invasion of porcinebrain microvascular endothelial cells has been observed for thisswine pathogen. Inhibition studies demonstrated that S. suis inva-sion of porcine brain microvascular endothelial cells required ac-tin filaments but not microtubular cytoskeletal elements or activebacterial RNA or protein synthesis (208). Electron microscopy stud-ies showed that S. suis adhered to porcine brain microvascular en-dothelial cells at 5 min postinfection, and at 2 h postinfection, thestreptococci were in close contact with the cells, within invagi-
Bacterial Mechanisms of Brain Invasion
October 2014 Volume 27 Number 4 cmr.asm.org 701
on June 30, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
http://cmr.asm.orghttp://cmr.asm.org/nated cell membrane structures and underneath the cell surface,behind the cell membrane. Unlike the case of group B strepto-cocci, following internalization within membrane-bound vacu-oles, the number of viable intracellular S. suis organisms steadilydecreased over time, and viable cocci were not detected after 7 h(208). However, similar to the case with S. pneumoniae and groupB streptococcus, the capsular polysaccharide of S. suis partiallyinhibited interactions with brain microvascular endothelial cells(208).
The S. suis proteins and virulence factors that mediate invasionof porcine brain microvascular endothelial cells remain largelyunknown. Pretreatment of porcine brain microvascular endothe-lial cells with S. suis lipoteichoic acid reduced but did not abolishthe adhesion and invasion of S. suis, in a dose-dependent manner,suggesting that lipoteichoic acid may play a role in S. suis interac-tions with porcine brain microvascular endothelial cells (209).Vanier et al. screened a transposon mutagenesis library of S. suisand identified several genes that may contribute to the invasion ofporcine brain microvascular endothelial cells (210). These geneswere characterized as encoding proteins belonging to the follow-ing groups: surface proteins, transport/binding proteins, regula-tory functions, metabolism, amino acid synthesis, protein synthe-sis, and hypothetical proteins. However, the roles of these genes inS. suis invasion of porcine brain microvascular endothelial cellshave not been confirmed using isogenic mutants.
As discussed above, the choroid plexus may be the site of entryto the CNS for S. suis. In order to study the interactions between S.suis and choroid plexus epithelial cells, Tenenbaum et al. devel-oped an inverted Transwell model in which the translocation of S.suis from the basolateral, blood side to the apical, CSF sidecould be investigated (211). Following S. suis infection of the ba-solateral side, the transepithelial electrical resistance and paracel-lular permeability remained constant for up to 4 h. S. suis invadedporcine choroid plexus epithelial cells from the basolateral side inthe inverted Transwell system; however, invasion was rare when S.suis was inoculated into the apical chamber in the standard Transwellmodel. These findings were also replicated in a human choroid plexusepithelial cell inverted Transwell model (140). This suggested that S.suis may interact with components of the extracellular matrix thatare accessible on the basolateral side. The translocation of S. suisthrough porcine brain microvascular endothelial cells was inhib-ited when cells were treated with a phosphatidylinositol 3-kinaseinhibitor, demonstrating that phosphatidylinositol 3-kinase maybe involved in the uptake of S. suis (211).
L. monocytogenes and B. pseudomallei. L. monocytogenes canenter the CNS by the Trojan horse mechanism (see below) or bytranscellular penetration of HBMECs. Using HUVECs andHBMECs, it was demonstrated that L. monocytogenes can invadeendothelial cells directly or via cell-to-cell spread from adherent,infected mononuclear phagocytes (212, 213). In HUVECs, L.monocytogenes attaches to the cellular surface and induces mem-brane ruffling, which leads to internalization (214). In HBMECs,L. monocytogenes invasion is preceded by intimate interactionsbetween the bacterium and microvilli on the cell surface (215).The invasion of L. monocytogenes into HBMECs requires actinmicrofilaments (213), but unlike the case for other meningealpathogens, it does not involve the activation of phosphatidylino-sitol 3-kinase (213) or cytosolic phospholipase A2 (175).
Once internalized, L. monocytogenes degrades the phagosomevia the activity of a pore-forming toxin (listeriolysin) and two
phospholipases (PlcA and PlcB), and it escapes into the cytoplasmby using actin-based motility, which is driven by the actin assem-bly-inducing protein, ActA. Following escape into the cytoplasm,L. monocytogenes can replicate within HUVECs and HBMECs anduse actin-based motility to spread to adjacent cells (212, 213), thusavoiding an extracellular lifestyle. However, L. monocytogenes canbe isolated from the CSF (216), suggesting that translocationthrough the cellular barriers of the CNS also occurs.
B. pseudomallei has an intracellular lifestyle similar to that of L.monocytogenes: the type III secretion system of B. pseudomallei(particularly the BopE and BopA effector proteins and the Bsatranslocation apparatus) is required for escape from the vacuoleand the subversion of autophagy (217222). In an epithelial cellline or a murine macrophage-like cell line, cell-to-cell spread thenoccurs by cell fusion, with the formation of multinucleated giantcells, in a type VI secretion-dependent process. BimA, which isnecessary for actin-mediated motility, and Fla2, which is thoughtto mediate intracellular motility, are also required and are consid-ered to mediate cell-to-cell contact prior to cell fusion (223227).To our knowledge, the ability of B. pseudomallei to directly invadeHBMECs has not been investigated, but it would be reasonable tohypothesize that the intracellular lifestyle of B. pseudomallei maycontribute to the pathogenesis of CNS invasion. Interestingly, arecent study investigated the variable virulence factors of B. pseu-domallei associated with melioidosis in Australia and reportedthat B. pseudomallei strains harboring a bimA allele that shares95% homology with B. mallei bimA (bimABm) (228) were signifi-cantly associated with neurological melioidosis (229). Patientsthat were infected with B. pseudomallei harboring the bimABmallele were found to be 14 times more likely to present with neu-rological involvement than patients infected with strains harbor-ing the B. pseudomallei bimA variant (bimABp) (229), indicating arole for actin-mediated motility in