Embed Size (px)
DESCRIPTION
Journal Article
Citation preview

Pathogenesis of Osteoarthritis
DAVID S. HOWELL, M.D. Miami, F/oriQa
This article reviews the etiology and pathogenesis of osteoarthritis, particularly one of several current concepts concerning the possi- ble central mechanisms regulating degradation of cartilage. Ac- cording to this theory, degradation involves diffuse or focal expo- sure of the extracellular matrix to active neutral metalloproteinases, which then results In injury as well as initiation of repair processes. Diffuse matrix exposure is probably not a physiologic aberrancy but rather a pathologic result of either physical injury to local chondro- cytes or inflammatory mediators.
Osteoarthritis is a complex response of joint tissues to aging, as well as to genetic and environmental factors, that is characterized by bone remod- eling, overgrowth of bone, and cartilage degradation [l]. This ancient disease accounts for disability beyond that of almost all currently known ailments [2]. According to yearly United States surveysover the last de- cade, osteoarthritis keeps 10 million Americans with related back dis- orders out of work. It also accounts for 90 percent of patients with rheu- matic symptoms over 65 years of age and for six million patients in need of knee or hip replacement. Disappointingly little interest in support for osteoarthritis-related research has evolved, however, despite the preva- lence and morbidity of this condition [2].
The term “idiopathic” (primary) osteoarthritis refers to the common va- riety encountered during aging, which is unrelated to known systemic or local disease, as well as to certain erosive and hereditary clinical subsets. “Secondary” osteoarthritis, although not separable from the idiopathic type on a pathologic basis, refers to the type that is clearly evoked by preceding events, including endocrine, inflammatory, metabolic, develop- mental, or heritable disorders. In addition, repeated microtrauma, mac- rotrauma, or prolonged immobilization of normal joints may predispose joints to secondary osteoarthritis [2].
From the Veterans Administration Medical Center and University of Miami Medical School, Miami, Florida. Requests for reprints should be addressed to Dr. David S. Howell, Department of Medicine (D26), University of Miami School of Medicine, P.O. Box 016960, Miami, Florida 33101.
Although numerous causes for the disorder have been proposed, all theories seem to converge on a final common pathway of cellular and joint tissue responses. Within cartilage, there is fissuring of superficial and, later, deep erosions, which culminates in loss of cartilage and bony eburnation. Concomitantly, marginal bone remodels, bone microfractures occur, subchondral bone thickens, and bone cysts form. Reparative re- sponses include proliferation of chondrocytes with expanded lacunae and the formation of cell clusters 111. . .
Whether the earliest pathologic changes occur in bone or cartilage is controversial [l]. Also unsettled is whether cartilage breakdown is purely a mechanical response of affected ‘tissue [3] or the result of injury of chondrocytes with consequent cell-mediated matrix breakdown. Synovial
24 April 28,1888 The American Journal ol Medicine Volume 80 (suppl 48)

SYMPOSIUM ON DICLOFENAC SODkIM AND INFLAMMATORY DISEASE-HOWELL
inflammation develops sooner or later but is usually sec- ondary to these earlier changes.
This article focuses on some of these events in more detail, with special emphasis on cartilage. Developmental defects of ischemic necrosis of bone, heritable disorders, and other subjects are discussed elsewhere [4].
PATHOGENESIS
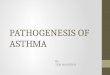
The etiologic factors involved in the pathogenesis of oste- oarthritis are shown in Figure 1. There are currently two major categories of theories regarding etiopathogenesis. The first category (theory A) is composed of those causes that share common abnormalities of weight bearing or load transmission through the joirit, either in terms of dis- tribution of loading forces or intensity of such forces. Biomaterial (rheologic) properties of cgrtilage and joint capsules are assumed to be normal in this first category. The second category (theory B) assumes normal loading forces being transmitted ihrough joint structures but in: eludes factors involving abnormal biomaterial properties of joints [3].
Examples of the first c&gory include remodeling of adult cartilage in bone or developmental defects, such a+ acetabular dysplasias or Legg-Calv&Perthes disease. Late onset of biomechanical abnormalities may be caused by damage to cartilage or subchondral bone from the le- sions of gouty tophi, Paget’s disease, hyperparathyriid cysts, or destructive joint inflammation from rheumatoid arthritis or sepsis. The second category, due to bio- material failure, is exemplified by cartilage in which de- posits of metabolites injure the matrix, as occurs in hemo- chromatosis and ochronosis. As additional causes of biomaterial failure (aging, etc.) become better understood [2], more and-more cases of osteoarthritis are being in- cluded in this second category of etiology.
CARTILAGE PHYSIOLOGY IN DEVELOPMENT OF OSTEOARTHRITIS
Cartilage is both an aneural and avascular tissue in the adult and obtains its nutrition primarily from synovial fluid. The chondrocytes, which occupy about 5 percent of the cartilage volume, are stimulated to sustain norinal repair and turnover of relevant proteins partly by a normal range o! loading forces but also by nutritional factors and hor- mones
Too weak a force or stimulation (as exemplified by pa- tients who are bedridden foi prolonged periods or by joints splinted wifh casts) reduces the synthetic functions of chror@ocytes and promotes dartilage atrophy [2]. Ca@- lage so affected can even break down ‘and ulcerate. In fact, ihroughout life, surface eros’ions are often observed on the tibia1 plateau of the knee or under the round liga- ment of the hip at sites where there is normally little con- tact .during joint motion. Such minor erosions, or “soft- ened:’ areas, are believed to remain in this quiescent state
April 28, 19d
(one or both) 1 l
-A
Cell injuty
Degradatlw responses increased
Inhibitors reduced
Pmwytii enzymes incmawd
Pluteaglycan collagen end other plOt6lflSdestrayed
+ L CAHTILAGE BREAKOCWN 1
Figure 1. Two popular viewpoints of the etiopakhogenesi of osteoarthritis. Theories A and B apply with vatiable over- lap depending on the subset of osfeoarthritis under consid- eration. Reproduced with permission from [2].
without progressing to further damage throughout one’s lifetime [l]. However, when the cartilage becomes loaded from excessive force, it can be damaged further. If, on the other hand, the joint is loaded iri a graded manner over an adequate time period, the cattililge can u&ally be re- stored to normal [2].
Evidence for these concepts evolves from animal re- $earch in which the influence of iminobilization, followed by subsequent exercise, or! cartilage para@ers has beeh evaluated. In addition to the superficial e&ions, deeper lesions may develop at weight-bearing portions of adult articblar cartilage, eithq& de n&o forms or possi- bly as eiensions from non-weight-bearing sites [2]. These deeper erosions can progress tq exposure of ca!ci- fied cartilage and bone, tind depend oh a number of poorly understood local eiinditioning factors. Some re- searchers believe that features cr/tical to deep cartilage erosions are prolonged subchondral bone remodeling and reopening of microscopi$ growth plate sites [1,2].
CARTlLAijE DEGdADATlON AND COLLAgENOLmC ENZYMES
There are a wide variety of causes and multiple condition- ing factors leading to osteoarthritis, all of which are cur- rently under study by a number of investigators. Although bone rem&Ming may be a paramount etiologic factor, cartilage and synovial membrane changes have caughf
The American Journal of &dicl~, Volume 80 (suppl4B) 25

SYMPOSIUM ON DICLOFENAC SODIUM AND INFLAMMATORY DISEASE-HOWELL
(N=14) (N=14)
T (N=2l)
into the media. Potent inhibitors of these enzymes were also demonstrated in culture systems [11,12] and were partially purified from intact tissues [13,14].
(N=13) (N=14)
T T
(NF~)
L ll - Normal A
L , s&c - ?hi n bxier 3 Mild
-- Cartilage Zone Histologh Grade
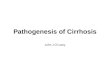
(Mankin Scale) . -_.. - igure 2.
. . . . . . - Acrivrty ot neutral meraioprorease capable of pro-
teoglycan digestion, measured in samples of osteoarthritic human arficular cartilage obtained at tori/ knee replacement and from the same site in “normal” control subjects. Zone A = center of osteoarthritic erosional tissue; zone B = cartilage at the edge of the erosions; and zone C = cartilage distant from the erosion. Enzyme activities are expressed as percent of endogenous proteoglycan degraded in 42 hours of incubation (+SEM). Reproduced with permission from 081.
The presence of collagenase in cultures of human oste- oarthritic cartilage and the relationship of this enzyme to disease severity was first documented by Ehrlich and as- sociates [15,16]. Later, with techniques devised to handle the very small samples obtained at surgery, Pelletier and co-workers [I 71 investigated cartilage. Extensions of these preliminary studies have focused on proteoglycan- and collagen-degrading enzymes in human and animal model cartilages (17,181. These studies, utilizing direct assays on tissues per se, have confirmed Ehrlich’s origi- nal findings. The data showed a highly significant eleva- tion of both types of enzyme activity present in erosional and marginal tissue of knee cartilage available at surgery at the time of total joint replacement (Figure 2). Moreover, enzyme activity strongly correlated with the histologic grade of disease (severity) as well as the site of collection (Figure 2) [17,18]. Data from studies with the Pond-Nuki dog model of osteoarthritis [19] showed that the level of collagenolytic activity increases within two weeks follow- ing surgical joint destabilization and continues at high lev- els for as long as measurements are made [20].
the attention of many scientists, since these findings may hold greater hope for future therapeutic intervention. Chondrocytic enzymes have received much attention as the most likely principal early mediators of cartilage deg- radation [2,4]. A comprehensive review of this subject can be found in a number of recent publications [l-8].
Suppression of the collagenolytic activity in synovial membranes of the Pond-Nuki dogs by administration of low-dose corticosteroids was much less complete than its suppression in cartilage [21]. Because of this finding, it was suggested that mononuclear cell factor or catabolin factors known to respond to low dosages of steroids in vitro were suppressed, thereby “turning off” the cartilage degradation. Another interesting finding was that in knee articular cartilage of rheumatoid patients who underwent total joint replacement, a high level of proteoglycan- degrading enzyme activity was found Selectively in all samples except in those of patients who had just received low or moderate doses of corticosteroid treatment [22].
In studies by Woessher and associates, neutral metal- loproteases in human cartilage have for the first time beeh partially biochemically characterized, their increased presence in human patellar atticular cartilage has been documented, and the concept that acid proteases cannot act anywhere except at the margins of chondrocytes or within them has been demonstrated [8]. In contrast, the neutral proteases are active at the prevalent pli of the extracellular cartilage matrix and are thus feasible agents for degradation throughout the matrix as observed in humans and animal models [9,10].
Collaborative studies have shown that proteoglycan- degrading enzymes and a probably true collagenase are elaborated in various cell cultures from chondrocyte prep- arations [l 1 ,121. This occurred in such a manner that al- most no enzyme activity remained in association with the cultured cell fraction but almost all enzyme was liberated
Recent studies provide a clear-cut explanation of why proteoglycan degradation products are not found in osteo- arthritic articular cartilage [23,24]. Proteoglycan mono- mers are retained in articular cartilage generally in the form of large aggregates bound to hyaluronic acid. Con- sequently, even slightly degraded proteoglycan mono- mers lacking the capacity to bind to hyaluronic acid may diffuse from cartilage, leaving only the undegraded mole- cules in the tissues per se [24]. More recently, epitopes of proteoglycan have been found in the synovial fluid of pa- tients with arthritis, suggesting that cartilage degradative mechanisms may occur early in the course of disease of some patients [25].
Structural studies of proteoglycans in osteoarthritic car- tilage indicate, as previously mentioned, that residual pro- teoglycan monomers are usually intact or only slightly degraded and that the other factors required for aggregat- ing proteoglycans-hyaluronic acid or glycoproteins from
26 April 28, 1986 The American Journal of Medicine Volume 80 (suppl 4B)

SYMPOSIUM ON DICLOFENAC SODIUM AND INFLAMMATORY DISEASE-HOWELL
r--l Multiple Etiologies
+ Elaboration of I I
Figure 3. Left, schema for mechanisms of protease regu ion I Icogenous or pnmarrly enuogenous) as stucl,ecf In cam/age cultures and sypovial fibroblast cultures [l-4,36,37]. Right, the current hypothesis is based on the belief that the balance of net activated neutral metalloproteases versus specific tissue inhibitors is disturbed in osteoarthritis. The selective suppression of this disturbance might be associated with improved tissue repair.
Current Hypothesis
I Synovial and Cartilage Mediators I
Cartilage Proteases
I Exogenous* Proteases
I
+ Exogenous to cartilage
“Therapeutic” Protease Inhibitors
a) acid pH adjacent to cell processes
b) neutral or slightly acid pH distant from cells
osteoarthritic cartilage so far sampled-fail in comparison to normal controls to reconstitute a normal profile of prote- oglycan aggregates [26]. The findings are consistent with those of previous studies with osteoarthritic cartilage in which low concentrations of hyaluronic acid [27] and rapid turnover of hyaluronic acid were shown [26,29]. These findings could be interpreted as indicating either degrada- tion of these factors or errors in repair synthesis.
The importance of inflammatory monokine and lympho- kine regulation of chondrocyte behavior in regard to ana- bolic and catabolic functions, inhibition of matrix synthe- sis, and acceleration of degradation is reviewed else- where [30-321. Further research is needed to disclose which nonsteroidal, steroidal [32], or other agents might turn off the “catabolin” [6] or anti-anabolic monokine without interfering with matrix synthesis.
This latter problem of suppressed matrix synthesis in osteoarthritic cartilage by nonsteroidal anti-inflammatory agents was first identified by Palmoski and Brandt [33]. It exists not only for corticosteroids but also for many non- steroidal anti-inflammatory drugs, both in vivo and in vitro.
In black mice of the C57 strain in whom spontaneous os- teoarthrosis develops, there is histologic evidence of long- term improvement of affected joint tis$ues following treat- ment with diclofenac sodium [34]. The favorable results observed with diclofenac were unique and in sharp con- trast to the deleterious effects reported with other nonste- roidal anti-inflammatory drugs.
Studies on growth factors methodologically tested in well-defined cell culture systems provide hope that pep- tide mediators of a catabolin nature can be overcome by assistance from stimulated growth factors of a physiologic nature [2]. Possibly, synthetic inhibitors of cartilage prote- ases could yield, under properly constructed conditions of delivery, an environment favorable for promoting healing tissue responses in early lesions of osteoarthritis (Fig ure 3) [35]. Chances for success in this objective are con- stantly improving as we gain a clearer understanding of the regulatory mechanisms for the synthesis, secretion, activation, and inhibition of a classically important neutral metalloprotease-collagenase [36,37]-which is now being studied successfully in synovial cell cultures.
April 26, 1666 The American Journal of Medicine Volume 80 (suppl 4B) 27

syMPo.sluM 0N OICL~FENAC SODIUM AND ~NFUM~~AT~RY DISEASE-HOWELL
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
Sokolofl L: Aging and degenerative diseases affecting cartilage. Ini Hall B, ed. Cartilage. Vol. Ill. New York: Academic Press, 1983; 109-141.
Moskowitz RW, Howell DS, Goldberg VM, Mankin HJ Jr, eds: Osteoarthritis: diagnosis and management. Philadelphia: WB Saunders, 1984; l-585.
Maroudas A, Holborow EJ, eds: Studies in joint disease. Vols. 1 and 2. London: Pitman Medical, 1981.
Cooke TD, Dwosh I, Cossairl J: Clinical pathological osteoarthri- tis workshop. J Rheumatol 1983; 20 (suppl 9): l-l 18.
Peyron JG, ed: Osteoarthritis. Current clinical and fundamental problems. Paris: Ciba-Geigy, 1985; 13-320..
Howell DS, Talbott JH, eds: Osteoarthritis symposium. Semin Arthritis Rheum 1981; 11 (suppl 1): 1-149.
Armstrong CC, Mow VC: Biomechanics of normal and os- teoarthrotic cartilage. In: Wilson PD Jr, Straub LR, eds. Clini- cal trends in orthopaedics. New York: Thieme-Stratton, 1982; 189-197.
Barrett AJ, Saklatva J: Proteinases in joint disease. In: Kelley WN, Harris ED Jr, Ruddy S, Sledge CB, eds. Textbook of rheumatology. 2nd ed. Philadelphia: WB Saunders, 1985; 182-198.
Sapolsky Al, Keiser HD, Woessner JF Jr, Howell DS: Metal- loproteases of human articular cartilage that digest cartilage proteoglycan at neutral and acid pH. J Clin Invest 1976; 58: 1030-1041.
Sapolsky Al, Howell DS: Further characterization of a neutral metalloprotease isolated from human articular cartilage. Ar- thritis Rheum 1982; 25: 981-988.
Malemud CJ, Norby DP, Sapolsky Al, Matsuta K, Howell DS, Moskowitz RW: Neutral proteinases from articular chondro- cytes in culture. 1. A latent collagenase that degrades human cartilage type II collagen. Biochim Biophys Acta 1981; 657: 517-529.
Sapolsky Al, Malemud CJ, Norby DP, Moskowitz RW, Matsuta K, Howell DS: Neutral proteinases from articular chondro- cytes in culture. 2. Metal-dependent latent neutral proteoglycanase and inhibitory activity. Biochim Biophys Acta 1981; 658: 138-147.
Morales Tl, Kuettner KE, Howell DS, Woessner JF Jr: Charac- terization of the metalloproteinase inhibitor produced by bo- vine articular chondrocytes in culture. Biochim Biophys Acta 1983; 760: 221-229.
Killackey JJ, Roughley PJ, Mart JS: Proteinase inhibitors of human articular cartilage. Coll Relat Res 1983; 3: 419-430.
Ehrlich MG, Houle PA, Vigliani G, Mankin HJ: Correlation be- tween articular cartilage collagenase activity and osteoarthri- tis. Arthritis Rheum 1978; 21: 781-788.
Ehrlich MG. Mankin HJ. Jones H. Wright R. Crisoen C. Vialiani G: Collagenase and ‘collagen&e Ghibitors in ostebarthritic and normal human cartilage. J Clin Invest 1977; 59: 226-233.
Pelletier JP, Martel-Pelletier J, Howell DS, Ghandur-Mnaymneh L, Enis JE, Woessner JF Jr: Collagenase and collagenolytic activity in human osteoarthritic cartilage. Arthritis Rheum 1983; 26: 63-68.
Martel-Pelletier J, Pelletier JP, Cloutier JM, Howell DS, Ghandur-Mnaymneh L, Woessner JF Jr: Neutral proteases capable of proteoglycan digesting activity in osteoarthritic and normal human articutar cartilage. Arthritis Rheum 1984; 27: 305-312.
Pond MJ, Nuki G: Experimentally induced osteoarthritis in the dog. Ann Rheum Dis 1973; 32: 387-388.
Pelletier JP, Martel-Pelletier J, Altman RD, Ghandur-Mnaymneh L, Howell DS, Woessner JF Jr: Collagenolytic activity and col- lagen matrix breakdown of the articular cartilage in the Pond-
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
Nuki dog model of osteoarthritis. Arthritis Rheum 1983; 28: 866-874.
Pelletier JP, Martel-Pelletier J, Ghandur-Mnaymneh L, Howell DS, Woessner JF Jr: Role of synovial membrane inflamma- tion in cartilage matrix breakdown in the Pond-Nuki dog model of osteoarthritis. Arthritis Rheum 1985; 28: 554-561.
Martel-Pelletier J, Cloutier JM, Howell DS, Pelletier JP: Human rheumatoid arthritic cartilage and its neutral proteoglycan degrading proteases. The effect of anti-rheumatic drugs. Ar- thritis Rheum 1985; 28: 405-412.
Sandy JD, Brown L, Lowther DA: Degradation proteoglycan in articular cartilage. Biochim Biophys Acta 1978; 543: 538- 544.
Carney SL, Sandy JD, Billingham MEJ, Muir H: In vitro turnover of proteoglycans and proteins in normal and degenerating ar- titular cartilage (abstr). In: Chester MA, Heinegard D, Lundblad A, Svenson S, eds. Proceedings of the 7th Interna- tional Symposium on Glycoconjugates. Lund: Rahms Pub- lisher, 1983; 798.
Witter JP, Roughley PJ, Caterson B, Poole AR: The isolation and characterization of proteoglycan fragments derived from articular cartilage in human arthritic synovial fluid (abstr). Transactions of the 30th Annual Meeting. Orthoped Res Sot 1984; 9: 313.
Manicourt D, Howell DS, Moskowitz RW, Goldberg V, Malemud C, Pita JC: Studies of cartilage proteoglycan in an osteoar- thritic rabbit model. In: Peyron JG, ed. Osteoarthritis. Current clinical and fundamental problems. Paris: Ciba-Geigy, 1985; 192-202.
Sweet MBE, Thonar E-J, lmmelman AR, Solomon L: Biochemi- cal changes in progressive osteoarthrosis. Ann Rheum Dis 1977; 38: 387-398.
lnerot S, Heinegard D, Andell L, Olsson SE: Articular proteogly- cans in aging and osteoarthritis. Biochem J 1978; 169: 143- 156.
Ryu J, Treadwell BV, Mankin MJ: Biochemical and metabolic abnormalities in normal and osteoarthritic human articular cartilage. Arthritis Rheum 1984; 27: 49-57.
Dayer JM, Russell RG, Krane SM: Collagenase production by rheumatoid synovial cells: stimulation by a human lymphocyte factor. Science 1977; 195: 181-183.
Jasin HE, Dingle JT: Human mononuclear cell factors mediate cartilage matrix degradation through chondrocyte activation. J Clin Invest 1981; 68: 571-581.
Herman JH, Appel AM, Hess EV: Piroxicam can modulate syn- thesis and activity of anabolic regulatory cytokines produced by osteoarthritic (OA) and rheumatoid (RA) synovium (abstr). Arthritis Rheum 1984; 27(S): 81.
Palmoski MJ, Brandt KD: Aspirin aggravates the degeneration of canine joint cartilage caused by immobilization. Arthritis Rheum 1982; 25: 1333-l 342.
Maier R, Wilhelmi G: Special pharmacological findings with di- clofenac sodium. In: Kass E, ed. Voltaren-new findings. Berne: Hans Huber, 1982; 11-18.
Howell DS, Muniz OE, Carreno MR: Effect of glycosaminogly- can polysulfate ester on proteoglycan-degrading enzyme ac- tivity in an animal model of osteoarthritis. In: Ctterness I, ed. Advances in inflammation research. New York: Raven Press, 1985; 197-208.
Harris ED Jr, Welgus HG, Krane SM: Regulation of the mamma- lian collagenases. Coll Relat Res 1984; 4: 493-512.
Brinckerhoff CE, Benoit MC, Culp WJ: Autoregulation of colla- genase production by a protein synthesized by synovial fibro- blasts: cellular mechanism for control of collagen degrada- tion. Proc Natl Acad Sci USA 1985; 82: 1916-1920.
28 April 28, 1986 The American Journal of Medicine Volume 80 (suppl 48)