Embed Size (px)
Citation preview

CentralBringing Excellence in Open Access
JSM Bone and Joint Diseases
Cite this article: Zacharia B, Subramanian D (2018) Pathogenesis and Sequels of Septic Arthritis of Hip in Children. JSM Bone and Joint Dis 2(1): 1014.
*Corresponding authorBalaji Zacharia, Additional Professor, Department Of Orthopedics, Government Medical College, Kozhikkode, Kerala, India, PIN-673008; Email:
Submitted: 12 March 2018
Accepted: 05 April 2018
Published: 07 April 2018
Copyright© 2018 Zacharia et al.
OPEN ACCESS
Research Article
Pathogenesis and Sequels of Septic Arthritis of Hip in ChildrenBalaji Zacharia* and Dhiyaneswaran SubramanianDepartment of Orthopedics, Government Medical College, India
Abstract
Septic arthritis of hip joint is a relatively common infection in neonates and infants. The most common organism causing it is gram positive cocci. High index of suspicion is necessary for the diagnosis. Early diagnosis and prompt treatment can prevent long term complications. Our objective is to describe the pathogenesis and sequels of septic arthritis of hip in children of various ages.
INTRODUCTIONSeptic arthritis most commonly affects hip joint. It is more
commonly seen in neonates, infants and young children [1]. The most common route of infection is haematogenous [1-4]. It can also occur as a direct extension of proximal femur osteomyelitis since proximal metaphysis of femur is intra-articular. Exogenous infection can occur via arthrotomy [1]. Most of the infections are caused by staphylococcus aureus, group B streptococcus, haemophilus influenza [1,5-8]. MRSA infection prevalence has increased with the continuously increasing amount of antibiotic resistance which also associated with more complications, longer duration of antibiotics, and increased mortality [9]. Rarely, organisms like pnemococci, gonocococci and Candida albicans also cause septic arthritis [1,6]. Primary focus of infection is the genitourinary tract, gastrointestinal tract, respiratory tract or in the ENT area in most children [1,10,11]. In neonates and young infants umbilical vein catheterisation, femoral venepuncture can be the source of infection [1,9]. Diagnosing septic arthritis in children is not a big deal but sometime may be confusing. The differential diagnosis that should be considered are Aseptic synovitis of the hip, Viral arthritides, Osteomyelitis, Juvenile rheumatoid arthritis, Legg-Calve-Perthes disease, Lyme disease (borreliosis), Slipped capital femoral epiphysis, Reactive arthritis and Sickle cell anemia [12].
PATHOGENESIS The infecting organism produces infection in the synovium.
Bacteria will be deposited in the sub synovial plexus leading to synovial inflammation. Synovial fluid containing large quantities of neutrophils and fibrin fill the joint cavity, which gets distended. If proper treatment is given at this stage or the host defence mechanism is able to contain the infection at this stage, there will not be permanent joint damage. If infection continues mesothelium lining the synovial membrane is destroyed and
replaced by granulation tissue. As a result pannus formation and articular cartilage damage can occur. Subsequently growth plate damage or dislocation of joint, avascular necrosis with bony or fibrous ankylosis can occur [13-16].
The vascular tamponade produced by increased intra-articular pressure is the main cause of avascular necrosis of capital femoral epiphysis. Doud et al. (1993), showed Meta physeal osteomyelitis, producing subperiosteal abscess in the poster superior aspect of the femoral neck, can occlude the retinacular vessels leading to avascular necrosis.
The proteolytic enzymes released during the breakdown of neutrophils can destroy the articular cartilage. It occurs maximally at the points of contact between the opposing areas, especially in hip joints. The glycosaminoglycan breakdown can occur due to collagenase produced from synovial lining cells. The enzyme plasmin is produced by the activation of plasminogen in the blood. Plasminogen activation is by the streptokinase and staphylokinase released by the organism. Plasmin causes break down of protein – chondroitin sulphate complex of the cartilage. Lastly, the release of acid and neutral proteases from chondrocytes, when stimulated by bacterial lipopolysaccharides or by interleukin 1, is another reason for articular cartilage damage. Both avascular necrosis and cartilage destruction can lead to damage to the growth plate [15,16].
SEQUELS OF SEPTIC ARTHRITIS OF HIPThere are many sequels to the septic arthritis in childhood.
The sequels developed depend on the age of occurrence and the delay in getting treatment [17]. In neonates and up to six months of age, the proximal femoral epiphysis may not develop and an untreated septic arthritis at this age can lead to complete destruction of proximal femoral epiphysis leading to unstable hip [18-21]. After the development of capital femoral epiphysis the sequels can be a completely normal hip if diagnosed early and

CentralBringing Excellence in Open Access
Zacharia et al. (2018)Email:
JSM Bone and Joint Dis 2(1): 1014 (2018) 2/3
treated properly [22,23]. Sometimes, due to increased vascularity there can be coxamagna [24]. Infection can lead to physeal growth arrest which can lead to shortening of femoral neck coxabreva, shortening of the femur there by limb length discrepancy and/ or abnormal shape of the proximal femur resulting in breaking of the femoral neck. Various deformities like coxa vara, coxa valga can develop as sequels [25,26]. Pseudarthrosis of the neck of femur can occur associated with coxa vara [23]. In older children, the main sequel is pathological dislocation. The head in a dislocated hip can be either normal or avascular. Rarely, there can be dislocation of a sequestrated femoral head. In older children untreated septic arthritis of hip can lead to stiff hip due to bony ankyloses [20,27,28].
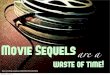
The treatment of the sequelae of septic arthritis of hip needs to be delayed. There is high chance for remodelling, due to growth of some of the minor deformities getting corrected by remodelling. The shape and vascularity of femoral head and neck are better known after remodelling. There is chance of reactivation of infection if interventions are done early. Besides, the strength and quality of bone may improve over time [26]. Choi et al., described a classification for the sequels of septic arthritis in neonate hip joint following evaluation of 34 children who had septic arthritis before the age of one [28] (Figure 1).
Type I: This group consisted of those patients with a normal radiographic appearance (Ia), and those with evidence of avascular necrosis.
1a-Normal radiograph
1b-Avascular necrosis
Type II: Involvement of the epiphysis, physis, and metaphysis: This type results from avascular necrosis, with or without significant damage to the capital femoral physis.
2a-Coxabrevia
2b-Coxa vara/Coxavalga
Type III: Damage to the femoral neck.
3a-coxa vara, coxa valga, with or without excessive femoral ante version or retroversion
3b-pseudarthrosis of the femoral neck
Type IV: Loss of the femoral head/neck
4a- segment of the femoral neck is preserved,
4b-no femoral neck remnant
TREATMENT PRINCIPLESTreatment of septic arthritis ranges from a intravenous
antibiotics, simple joint aspiration under ultrasound guidance, formal arthrotomy and arthroscopic lavage based on patients general condition and surgeons preference. But once acute condition is not managed properly, it will leads to sequlae which are having poor outcome even at best hands [29].
A moderate degree of coxa magna, coxa vara of less than 10 degrees and valgum of 15 degree can be left alone. Coxa magna with uncoverage of femoral head needs to be contained. Deformities can be treated either by open or closed wedge
osteotomy. Coxabreva can be managed by trochanteric epiphyseodesis. Pseudarthrosis may require bone grafting with or without osteotomy [26,27,30-32].
Pathological dislocation can be reduced. Sometimes femoral varus rotational osteotomy or salter or chairi osteotomy is helpful in reducing the pathological dislocation. Rarely, stabilisation procedures like Schanz pelvic support osteotomy, is done. Colonna greater trochanteric arthroplasty by placing the trochanteric apophysis into the acetabulum and distal transfer of abductors into the shaft for improving the abductor muscle function. This osteotomy is followed by a varus osteotomy at the subtrochanteric region later [33,34]. A sound bony ankylosis in functional position can be accepted, where as a sound ankylosis in non functional position requires a femoral osteotomy to make it in to a functional position [31,32]. Limb length discrepency can be treated by epiphyseodesis of the opposite limb or lengthening of ipsilateral limb at appropriate age.
CONCLUSION Acute septic arthritis of hip is a relatively common osteo-
Figure 1 Diagrammatic representation of Choi et al., classification of hip septic arthritis sequlae Type I: 1A-Normal radiograph; 1B-Avascular necrosisType II: Involvement of the epiphysis, physis, and metaphysic: 2A-Coxabrevia; 2B-Coxa vara/CoxavalgaType III: Damage to the femoral neck: 3A-coxa vara, coxa valga, with or without excessive femoral anteversion or retroverion; 3B-pseudarthrosis of the femoral neckType IV: Loss of the femoral head/neck: 4A- segment of the femoral neck is preserved;4B-no femoral neck remnant.

CentralBringing Excellence in Open Access
Zacharia et al. (2018)Email:
JSM Bone and Joint Dis 2(1): 1014 (2018) 3/3
Zacharia B, Subramanian D (2018) Pathogenesis and Sequels of Septic Arthritis of Hip in Children. JSM Bone and Joint Dis 2(1): 1014.
Cite this article
articular problem in neonates and infants. It can produce many sequels. The prevention of such complications is better than its treatment. Early diagnosis and prompt treatment is the way to prevent it.
CONFLICT OF INTERESTWe have no conflict of interest for this manuscript and we
have not accepted any financial assistance from within or outside of our institution for collecting data, writing manuscript and for its publications
REFERENCES1. Erich Rutz, Muriel Spoer. Septic arthritis of the paediatric hip – A
review of current diagnostic approaches and therapeutic concepts. Acta Orthop Belg. 2013; 79: 123-134.
2. Klein R S. Joint infection, with consideration of underlying disease and sources of bacteremia in hematogenous infection. Clin Geriatr Med. 1988; 4: 375-394.
3. Al Saadi MM, Al Zamil FA, Bokhary NA. Acute septic arthritis in children. Pediatr Int 2009; 51: 377-380.
4. Rutz E, Brunner R. Septic arthritis of the hip – current concepts. Hip Int. 2009; 19: 9-12.
5. Yamagishi Y, Togawa M, Shiomi M. Septic arthritis and acute hematogenous osteomyelitis in childhood at a tertiary hospital in Japan. Pediatr Int. 2009; 51: 371-376.
6. Young T P, Maas L, Thorp AW, Brown L. Etiology of septic arthritis in children: an update for the new millennium. Am J Emerg Med. 2011; 29: 899-902.
7. Naithani R, Rai S, Choudhry VP. Septic arthritis of hip in a neutropenic child caused by Salmonella typhi. J Pediatr Hematol Oncol. 2008; 30: 182-184.
8. Peltola H, Pääkkönen M, Kallio P, Kallio MJ, Group O-SAO-SS. Prospective, randomized trial of 10 days versus 30 days of antimicrobial treatment, including a short-term course of parenteral therapy, for childhood septic arthritis. Clin Infect Dis. 2009; 48: 1201-1210.
9. Kristen Combs, Kyle Cox. Clinical outcomes involving patients that develop septic arthritis with methicillin sensitive staphylococcus aureus versus methicillin resistant staphylococcus aureus. J Orthop. 2018; 15: 9-12.
10. Kang SN, Sanghera T, Mangwani J, Paterson JM, Ramachandran M. The management of septic arthritis in children: systematic review of the English language literature. J Bone Joint Surg. 2009; 91-B: 1127-1133.
11. Shah SS. Abnormal gait in a child with fever: diagnosing septic arthritis of the hip. Pediatr Emerg Care. 2005; 21: 336-341.
12. Pääkkönen M. Septic arthritis in children: diagnosis and treatment. Pediatric Health Med Ther. 2017; 8: 65-68.
13. Ferguson A B. Jr: Osteomyelitis in children. Clin Orth. 1973; 96: 51-56.
14. Kemp HBS, Lloyd-Roberts GC. Avascular necrosis of the capital epiphysis following osteomyelitis of the proximal femoral metaphysis. J Bone Joint Surg. 1974; 56-B: 688-697.
15. John A. Ogden. Pediatric Osteomyelitis and Septic Arthritis: The Pathology of Neonatal Disease. Yale J Biol Med.1979; 52: 423-448.
16. Curtiss P H. The pathophysiology of joint infections. Clin Ortho. 1973; 96: 129-135.
17. Forlin E, Milani C. Sequelae of septic arthritis of the hip in children: a new classification and a review of 41 hips. J Pediatr Orthop. 2008; 28: 524-528.
18. Dobbs MB, Sheridan JJ, Gordon JE, Corley CL, Szymanski DA, Schoenecker PL. Septic arthritis of the hip in infancy: long-term follow-up. J Pediatr Orthop. 2003; 23: 162-168.
19. Kaplan SL. Challenges in the evaluation and management of bone and joint infections and the role of new antibiotics for gram positive infections. Adv Exp Med Biol. 2009; 634: 111-120.
20. Baghdadi T, Saberi S, Sobhani Eraghi A, Arabzadeh A, Mardookhpour S. Late Sequelae of Hip Septic Arthritis in Children. Acta Med Iran. 2012; 50: 463-467.
21. Peters W, Irving J, Letts M. Long-term affects of neonatal bone and joint infection on adjacent growth plates. J Pediatr Orthop. 1992; 12: 806-810.
22. Lunseth PA, Heiple KG. Prognosis in septic arthritis of the hip in children. Clin Orthop. 1979; 139: 81-85.
23. Li Y, Zhou Q, Liu Y, Chen W, Li J, Yuan Z, et al. Delayed treatment of septic arthritis in the neonate: A review of 52 cases. Esposito. Medicine. 2016; 95: 5682.
24. El-Tayeby HM. Osteochondroplasty of the femoral head in hip reconstruction for type II late sequelae of septic arthritis: a preliminary report. J Child Orthop. 2008; 2: 431-441.
25. Weissman SL. Transplantation of the trochanteric epiphysis into the acetabulum after septic arthritis of the hip. Report of a case. J Bone Joint Surg Am. 1967; 49: 1647-1651.
26. Choi IH, Shin YW, Chung CY, Cho TJ, Yoo WJ, Lee DY. Surgical treatment of the severe sequelae of infantile septic arthritis of the hip. Clin Orthop Rel Res. 2005; 434: 102-109.
27. Choi IH, Yoo WJ, Cho TJ, Chung CY. Operative reconstruction for septic arthritis of the hip. Orthop Clin North Am. 2006; 37: 173-183.
28. Spiegel DA, Penny J N, Banskota A K, Shrestha O P. Sequelae of Septic Arthritis of the Hip. A Global HELP Public. 2007.
29. Thompson RM, Gourineni P. Arthroscopic Treatment of Septic Arthritis in Very Young Children. J Pediatr Orthop. 2017; 37: 53-57.
30. B. Ilharreborde. Sequelae of paediatrics costeoarticular infection. OrthopTraumatol Surg Res. 2015; 101: 29-37.
31. Rozbruch SR, Paley D, Bhave A, Herzenberg JE. Ilizarov Hip reconstruction for late sequelae of infantile hip. J Bone Joint Surg Am. 2005; 1007-1018.
32. Cen Bytyçi, Hasime Qorraj and Dafina Bytyqi. Treatment of neonatal septic arthritis sequelae of hip: a case report. Cases J. 2009; 2: 6332.
33. Colonna PC. A new type of reconstruction operation for old ununited fracture of the neck of the femur. J Bone Joint Surg. 1935; 17: 110-122.
34. L’Episcopo JB. Stabilization of pathological dislocation of the hip in children. J Orthop Surg Res. 1936; 18: 737-742.