Embed Size (px)
Citation preview

Lee Ann Norman MSIIIPathology Specialty Clerkship
5 November 2014

Case Report Patient: 23 year-old Caucasian femalePast medical history:
ESRD secondary to Familial Juvenile Nephronophthisis Glaucoma Bell’s Palsy GI bleed s/p renal transplant (age 8) s/p remote atrial septal defect repair (age 3) Peritoneal dialysis Currently undergoing Valdec desensitization for second renal
transplant after first renal transplant failed 3 yrs prior Hemodialysis x 2 wks prior to presentation (including morning of
presentation)Presented to UC ED in cardiac arrest
Suspected cause was hyperkalemia causing dysarrythmia

Nephronophthisis Cystic diseases of Renal Medulla
Medullary Sponge Kidney Nephronophthisis Adult-Onset Medullary Cystic Disease
Nephronophthisis 3 variants:
Sporadic/nonfamilial Familial juvenile nephronophthisis = most common (AR) Renal-retinal dysplasia
Group of progressive renal disorders Variable number of cysts in the medulla, specifically
the cortico-medullary junction Initial injury: distal tubules
Tubular BM disruption chronic and progressive tubular atrophy (medulla and cortex) w/ intersitial fibrosis
The cortical tubulointersitial damage = cause of eventual ESRD

Familial Juvenile Nephronophthisis Autosomal recessive: 7 genes (NPH1, NPH2, NPH3)
NPH1/NPH3 = nephrocystins (primary cilia proteins—fxn unknown) NPH2 = inversin (left-right patterning in embryogenesis)
Manifests in childhood/adolescence The most common genetic cause of ESRD in children and
young adults First manifestations:
Polyuria and polydipsia Due to marked defect in concentrating ability of renal tubules
Sodium wasting Tubular acidosis Extra-renal associations
Ocular motor abnormalities Liver fibrosis Retinal dystrophy Cerebellar abnormalities
Progression to ESRD in 5-10 years

Autopsy Findings 1. Pulmonary edema w/ pleural effusion2. Atrophic bilateral native kidneys 3. Markedly hyperplastic parathyroids (2) associated w/
generalized metastatic calcification involving:1. Media of small arteries (heart, lungs, kidneys, muscle,
pancreas)2. Alveolar septae and terminal bronchiolar walls3. Endocardial foci: leaflets of mitral valve with myxoid
degeneration 4. Centrilobular congestion of liver5. Peritoneal fluid (900 mL) likely ascites6. Multinodular colloid goiter7. S/P remote closure of ASD8. Vitreous fluid potassium: 8.8 mmol/L

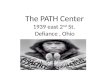
Gross Images

B/L small atrophic 12 gm each


0.2 cm in greatest dimension; c-m junction

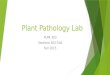
Micro Images

Micro Images




Calcium Homeostasis: A Brief Overview

The Kidney’s Role In Vitamin D Production

Normal Parathyroid Glands
Hyperplastic glands due to CRF w/ Impaired Phosphate Excretion

Etiology Overproduction of PTH secondary to a
chronic abnormal stimulus for its production CHRONIC RENAL FAILURE Vitamin D deficiency also
Develops early in CKD before dialysis is required
Overproduction of PTH in response to hyperphosphatemia, hypocalcemia, and impaired 1,25-dihydroxyvitamin D production by diseased kidneys.
Pathophysiology Hyperphosphatemia
Directly stimulates PTH synthesis and parathyroid hyperplasia
Indirectly promotes secondary hyperparathyroidism by decreasing free calcium
Spectrum of bone disease observed in patients on dialysis: osteitis fibrosa cystica and mixed uremic osteodystrophy
Dialysis patients may have discrete, punched-out bone lesions with minimal resorption or osteoblast activity
Other manifestations: CV calcification, soft tissue calcification, endocrine disturbances, compromised immune system, neurobehavioral changes, altered erythropoiesis

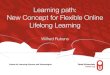
Calciphylaxis
Histology showing ischemic skin changes with ulceration, inflammation, scarring (right) and calcification in the medium-sized arteries in the subcutaneous fat (left), typical of calciphylaxis (H & E, ×200).

Subcutaneous tissue with calcification
Gangrenous lesion
Calcified subcutaneous arterioles

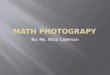
Osteoclastic Bone Resorption

Discussion
ESRD leading to…
Secondary hyperparathyroidism leading to…
Hypercalcemia leading to…
Metastatic calcification of the media of penetrating muscular arteries of the heart, conduction system, and elastic lamina of larger coronary arteries
Arrythmia/dysarrythmia leading to…
ANDMyxoid degeneration and calcification of the mitral valve leading to…
Cardiac failure, cardiogenic pulmonary edema, and death

Systemic metastatic calcification is a common complication of chronic renal failure. Disease of the CV system accounts for around 50% of deaths in patients with ESRD. Metastatic myocardial calcifications from secondary hyperparathyroidism are commonly (59%) discovered at the autopsy in those patients with ESRD undergoing maintenance dialysis. Complications arising from cardiac calcification include complex atrial and ventricular arrythmias, coronary events and sudden cardiac death, with arrhythmia being the most common cause.
The immediate mechanism of death was cardiogenic pulmonary edema secondary to a fatal arrhythmia/heart failure. The underlying cause of death is ESRD (familial juvenile nephronophthisis) leading to secondary hyperparathyroidism and widespread generalized metastatic calcification.

“Patients with chronic renal failure (CRF) are at increased risk for pathological calcifications because of increased serum calcium-phosphorus products. A minority, including those undergoing dialysis, develop a syndrome of deep skin ulcerations in association with calcification of subcutaneous arterioles. The body distribution of the skin lesions may be proximal (central), distal (peripheral), or both. Since 1968, this syndrome has been called ‘calciphylaxis’ in the belief that it is the human analogue of Selye's experimental models of tissue calcification. Our review emphasizes that this syndrome comprises two separate processes not found in calciphylaxis: calcification of subcutaneous arterioles and infarctions of subcutaneous adipose tissue (panniculus adiposus) and skin. The infarctions are acute and clinically dramatic, whereas the calcific arteriolopathy is preexistent, having developed slowly, sometimes over years, and silently. Separating these two processes facilitates analyses of pathogenetic factors, such as those that target subcutaneous arterioles for calcification and those that interfere with blood flow through the calcified arterioles, sufficient in some patients to cause the infarctions, and of why obesity in CRF is a syndrome risk factor. This approach further helps to provide a much needed standardized definition of the syndrome, thereby facilitating comparisons of the results of such treatments as parathyroidectomy, anticoagulants, and phosphate binders. Finally, the separation shows why the application of such terms as calciphylaxis and calcifying panniculitis to this syndrome is inappropiate.”
American Journal of Kidney Disease 1999

Key Lab Values