Embed Size (px)
Citation preview

VSM
PatellofemoralPatellofemoral Dislocation Dislocation and Instabilityand Instability

VSM
Functions of the PatellaFunctions of the Patella
•• Patella functions as the fulcrum of a lever, Patella functions as the fulcrum of a lever, maximizing flexion & extension with a maximizing flexion & extension with a given quadriceps forcegiven quadriceps force
•• Also acts as pulley, changing direction of Also acts as pulley, changing direction of quadriceps forcequadriceps force
•• Effect greatest at 20Effect greatest at 20°° of flexionof flexion•• Absorbs Absorbs patellofemoralpatellofemoral joint reaction joint reaction
forcesforces

VSM
Patella Patella –– anatomical considerationsanatomical considerations
•• Triangular sesamoid boneTriangular sesamoid bone•• Multiple facets, unique to Multiple facets, unique to
each individualeach individual•• Passive and dynamic Passive and dynamic
stabilizing factors stabilizing factors influence position in influence position in femoral femoral sulcussulcus–– VMO is the major dynamic VMO is the major dynamic
stabilizerstabilizer–– Medial Medial patellofemoralpatellofemoral
ligament is major ligament is major ligamentousligamentous stabilizerstabilizer

VSM
Patellofemoral joint reaction forcePatellofemoral joint reaction forceForce through PFJ Force through PFJ Level (Dahl 2006)Level (Dahl 2006)•• WalkingWalking 0.5 x BW0.5 x BW•• Stair climbingStair climbing 33--4 x BW4 x BW•• SquatSquat--120120ºº 77--8 x 8 x
BWBW•• JoggingJogging 7x BW7x BW•• DecelDecel/Jump/Jump 77--8 x 8 x
BWBW
Varying compressive forces helpVarying compressive forces helpmaintain cartilage health (perfusion)maintain cartilage health (perfusion)

VSM
Patellar DislocationPatellar Dislocation
•• Indirect injury more Indirect injury more commoncommon–– Quad contraction combined Quad contraction combined
w/ rotation (Dahl 2006)w/ rotation (Dahl 2006)–– Flexed, Flexed, valgusvalgus kneeknee–– Internally rotated femur on Internally rotated femur on
externally rotated tibiaexternally rotated tibia–– Reduces with knee Reduces with knee
extensionextension
•• Direct blow less commonDirect blow less common

VSM
Lateral Dislocation: HistoryLateral Dislocation: History
•• Patients may believe it to be a medial Patients may believe it to be a medial dislocation because of prominence of dislocation because of prominence of uncovered MFCuncovered MFC
•• Most often associated with soccer, Most often associated with soccer, gymnastic and ice hockey (Dahl 2006)gymnastic and ice hockey (Dahl 2006)

VSM
Direction of DislocationDirection of Dislocation
•• Most commonly lateralMost commonly lateral•• Medial is usually iatrogenic (Medial is usually iatrogenic (overzealous lateral overzealous lateral
release, overrelease, over--medializationmedialization of of tibialtibial tubercletubercle))•• Superior dislocations occur more commonly in Superior dislocations occur more commonly in
the elderly: hyperextension with patella the elderly: hyperextension with patella obstructed by femoral obstructed by femoral osteophyteosteophyte (Dahl 2006)(Dahl 2006)
•• IntraIntra--articulararticular or horizontal dislocations: Rare. or horizontal dislocations: Rare. Quadriceps tendon detaches from patella w/ Quadriceps tendon detaches from patella w/ rotation of patella into rotation of patella into intercondylarintercondylar notchnotch

VSM
RadiographsRadiographs
•• AP, Lateral, Merchant AP, Lateral, Merchant axialaxial–– Gross malalignment or Gross malalignment or
fracturefracture
–– Underestimate Underestimate articular surface articular surface lesionslesions
–– Identify <50% of Identify <50% of osteochondral loose osteochondral loose bodiesbodies
DeLee 2003

VSM
Associated InjuriesAssociated Injuries
•• OsteochondralOsteochondral and and chondralchondral injuryinjury•• StanitskiStanitski and Paletta: 48 patients with and Paletta: 48 patients with
acute initial patellar dislocation submitted acute initial patellar dislocation submitted to arthroscopy (to arthroscopy (DeLeeDeLee 2003):2003):–– 71% with 71% with articulararticular damagedamage–– 32% seen on 32% seen on preoppreop xx--raysrays–– 29% of 29% of osteochondralosteochondral loose bodies identifiedloose bodies identified

VSM
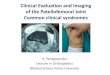
MRI ImagesMRI Images
Sanders et al, AJR 2006
Classic bone bruise pattern: lateral aspect of LFC, posteromedial patella

VSM
MRI of MRI of ChondralChondral DefectDefectSmall arrows: chondraldefect at posterior margin of bone contusion.Large arrow: small osteochondral fragment

VSM
MRI of MRI of OsteochondralOsteochondral Defects of Defects of LFCLFC
•• Sanders et al, Am J Sanders et al, Am J RoentgenologyRoentgenology, 2006. , 2006. •• 476 consecutive knee 476 consecutive knee MRIsMRIs reviewedreviewed•• 25 w/ evidence of prior patellar dislocation25 w/ evidence of prior patellar dislocation•• M:F 9:16, age range 10M:F 9:16, age range 10--31 yrs, mean 17 31 yrs, mean 17
yrs.yrs.

VSM
Results (1)Results (1)
•• 10 patients had 10 patients had osteochondralosteochondral defects of defects of LFC by MRILFC by MRI
•• 8 of the 10 underwent arthroscopy8 of the 10 underwent arthroscopy•• 6 of 8 had 6 of 8 had chondralchondral defects of LFC by defects of LFC by
arthroscopyarthroscopy

VSM
Results (2)Results (2)
•• 40% incidence of 40% incidence of osteochondralosteochondral injury of injury of LFC after patellar dislocation (31% LFC after patellar dislocation (31% reported by Nomura et al)reported by Nomura et al)
•• 12% with injury to lateral 12% with injury to lateral trochleartrochlear groove groove (5% reported by Elias et al)(5% reported by Elias et al)
•• All were fullAll were full--thicknessthickness•• All located at posterior margin of bone All located at posterior margin of bone
bruisebruise

VSM
Epidemiology and Natural History of Epidemiology and Natural History of Acute Patellar Dislocation: Acute Patellar Dislocation: FithianFithian et et al, 2004al, 2004
•• Prospective cohort studyProspective cohort study•• Enrolled pts 1992Enrolled pts 1992--1996 presenting to Orthopedic Knee 1996 presenting to Orthopedic Knee
Injury Clinic w/ Injury Clinic w/ dxdx of acute patellar dislocationof acute patellar dislocation•• 125 first125 first--time time dislocatorsdislocators w/o w/o hxhx of prior instabilityof prior instability•• 64 with prior patellar 64 with prior patellar subluxationsubluxation or dislocationor dislocation•• Initial Initial evaleval: PE with x: PE with x--ray and subset w/ MRI.ray and subset w/ MRI.•• FollowFollow--up 2up 2--5 years later5 years later•• Repeat exam, xRepeat exam, x--ray (and bone scan on random ray (and bone scan on random
subset)subset)

VSM
Epidemiology of Patellar Epidemiology of Patellar Dislocation: ResultsDislocation: Results
•• Highest risk among females 10 to 17 Highest risk among females 10 to 17 y.oy.o..•• Patients presenting with prior Patients presenting with prior hxhx of of
instability more likely to be female (P < instability more likely to be female (P < 0.05) 0.05)
•• Rates of further instability during followRates of further instability during follow--up (2up (2--5 years):5 years):–– 17% of first17% of first--time time dislocatorsdislocators–– 49% of those with prior 49% of those with prior hxhx of dislocationof dislocation–– P < 0.01 P < 0.01

VSM
Other FindingsOther Findings
•• No significant arthritis in either group on No significant arthritis in either group on repeat evaluation (by Xrepeat evaluation (by X--ray)ray)
•• Small but significant difference in Q angle Small but significant difference in Q angle and footand foot--thigh angle between females of thigh angle between females of the 2 groupsthe 2 groups

VSM
PatellofemoralPatellofemoral: Instability: Instability
•• Maenpaa AJSM Maenpaa AJSM ’’97 Nonoperative 97 Nonoperative treatment of initial patella dislocationtreatment of initial patella dislocation–– 100 pts, 13 yr f/u100 pts, 13 yr f/u–– 44% 44% redislocatedredislocated–– 19% stable but dissatisfied19% stable but dissatisfied

VSM
PatellofemoralPatellofemoral InstabilityInstability
•• NonNon--operative treatmentoperative treatment–– Straight leg raise to Straight leg raise to evaleval extensor mechanism extensor mechanism
integrityintegrity–– XX--rays after reduction to look for intrarays after reduction to look for intra--articulararticular
fragmentsfragments–– Short term immobilization (<3 days) Short term immobilization (<3 days) –– Early quad activation, pain and swelling control Early quad activation, pain and swelling control
(aspiration as needed)(aspiration as needed)–– Resume full weight bearing ASAPResume full weight bearing ASAP–– Orthotic support, closed chain exercisesOrthotic support, closed chain exercises

VSM
Indications for Operative Indications for Operative ManagementManagement
•• IntraIntra--articulararticular fragments (fragments (DathDath 2006)2006)•• Suspected large Suspected large osteochrondralosteochrondral fracturefracture•• Asymmetric, Asymmetric, subluxedsubluxed or tilted patellaor tilted patella

VSM
Early Operative ManagementEarly Operative Management
•• Repair of medial ligamentsRepair of medial ligaments•• Lateral releaseLateral release•• Excision or internal fixation of Excision or internal fixation of
osteochondralosteochondral fragmentfragment
•• From From DathDath 20062006

VSM
Evidence Based MedicineEvidence Based Medicine
•• Recent literature search for best operative Recent literature search for best operative technique to treat patellar instabilitytechnique to treat patellar instability
•• Most studies examine outcomes for a particular Most studies examine outcomes for a particular technique (any one or combination techniques). technique (any one or combination techniques).
•• Few articles compare 2 or more techniquesFew articles compare 2 or more techniques•• Much of the literature on this topic is older, and Much of the literature on this topic is older, and
many are case series with small patient many are case series with small patient populationspopulations
•• There is a mix of retrospective and prospective There is a mix of retrospective and prospective reports, but there is very little use of controls or reports, but there is very little use of controls or randomization. randomization.

VSM
Surgical Options for InstabilitySurgical Options for Instability
•• Lateral retinacular releaseLateral retinacular release
•• Proximal realignmentProximal realignment
•• Distal realignmentDistal realignment–– Soft tissueSoft tissue–– Tibial tubercle transferTibial tubercle transfer

VSM
Skeletal MaturitySkeletal Maturity1.1. DonDon’’t t ASSUMEASSUME, especially , especially
malesmales2.2. Most common injuries:Most common injuries:
•• Salter Salter fxfx distal femur distal femur vsvs MCLMCL•• Bony avulsion ACLBony avulsion ACL•• TibialTibial tubercle avulsiontubercle avulsion•• Immature Immature tibialtibial tubercle ACL tubercle ACL
teartear

VSM
HEMARTHROSIS:HEMARTHROSIS:Differential Diagnosis (Differential Diagnosis (DdxDdx))
1.1. Timing rapid effusionTiming rapid effusion2.2. AspirationAspiration3.3. Fat/fluid MRIFat/fluid MRI
1.1. ACL TearACL Tear2.2. Patellar dislocationPatellar dislocation3.3. PhysealPhyseal (GF) (GF) fxfx4.4. Occult Occult fxfx MRIMRI5.5. PCL tearPCL tear6.6. Peripheral meniscus tearPeripheral meniscus tear
DiagnosisDiagnosis DdxDdx

VSM
DIAGNOSIS: PE DIAGNOSIS: PE vsvs MRIMRI1.1. Principle:Principle: Technology (MRI) is NOT Technology (MRI) is NOT
substitute for physical examination substitute for physical examination (PE) skills(PE) skills
2.2. PE Majority:PE Majority: ACL, PCL, pat ACL, PCL, pat dislocdisloc3.3. MRI Majority:MRI Majority: OCD, occult OCD, occult fxfx, meniscus , meniscus tears*tears*
* If joint line pain, * If joint line pain, nlnl XR, effusion, mechanical symptoms, MRI XR, effusion, mechanical symptoms, MRI optionaloptional

VSM
High School Knee Injury High School Knee Injury Algorithm: Algorithm: HISTORY and PEHISTORY and PEACUTEACUTE PHYSICALPHYSICALINJURYINJURY →→ HISTORYHISTORY →→ EXAMEXAM →→SportSport Traumatic?Traumatic? Gait Gait MVAMVA Contact?Contact? EffusionEffusion
Pop?Pop? Point tenderPoint tenderSwelling/timing? MeniscusSwelling/timing? MeniscusWalk?Walk? AP stabilityAP stabilityGiving wayGiving way Varus/valgusVarus/valgus
PFPFNVNV
II
MM
AA
GG
II
NN
GG

VSM
HS Knee Injury Algorithm:HS Knee Injury Algorithm:IMAGINGIMAGING
•• Standing AP, lat, PFStanding AP, lat, PF•• Skeletal maturity?Skeletal maturity?•• R/O FractureR/O Fracture
–– GP GP vsvs apophysisapophysis–– CruciateCruciate avulsionavulsion–– PatellaPatella–– SegondSegond
•• OCDOCD
•• MRIMRI–– GP GP FxFx–– ACLACL–– MeniscusMeniscus–– OCDOCD–– Occult Occult FxFx
•• Stress Stress XRXR’’ss–– ? Role? Role
•• Diagnostic scopeDiagnostic scope–– Very limitedVery limited
Routine XR’sAdvancedImaging
PRIMARY
DIAGNOSIS
or
Ddx

VSM
HS Knee Injury Algorithm:HS Knee Injury Algorithm:TREATMENT OPTIONSTREATMENT OPTIONS
Distal femoral Distal femoral physisphysis (GP) (GP) fxfx Salter ISalter I Salter II, III, IVSalter II, III, IVCruciateCruciate ligament tearsligament tears PCLPCL ACLACLCollateral ligament tear (isolated)Collateral ligament tear (isolated) MCL, LCL GI/IIMCL, LCL GI/II LCL GIII ?LCL GIII ?Meniscus tearMeniscus tear Small tear in season?Small tear in season? MajorityMajorityOCDOCD StableStable UnstableUnstablePatellofemoralPatellofemoral PainPain Instability Instability
recurrentrecurrentApophysisApophysis Inflammation/painInflammation/pain AvulsionAvulsionOccult Occult fxfx MRIMRI MajorityMajority
Primary Diagnosis(es): Nonoperative Surgery

VSM
CASE 1:CASE 1:Patellar Instability EpisodePatellar Instability Episode
•• Adolescent soccer player Adolescent soccer player injures knee during game injures knee during game and doesnand doesn’’t finish. Initial t finish. Initial treatment RICE. Athlete treatment RICE. Athlete limps into your office a few limps into your office a few days later.days later.

VSM
EvaluationEvaluation
•• HxHx:: Initial Initial vsvs recurrent, timing of seasonrecurrent, timing of season•• Mechanism:Mechanism: Traumatic?Traumatic?•• PE keys:PE keys: Patellar tracking 0Patellar tracking 0--9090°° AROM, Q AROM, Q
angle, effusion, point tenderangle, effusion, point tender•• XR:XR: OsteochondralOsteochondral loose bodies, skeletal loose bodies, skeletal
maturitymaturity•• MRI?MRI? If diagnosis in doubt, define If diagnosis in doubt, define pathopatho--
anatomy of injury if relevantanatomy of injury if relevant

VSM
Evidence Based Literature Review Evidence Based Literature Review (EBM)(EBM)
1.1. Single RCT Operative Single RCT Operative vsvs NonoperativeNonoperative Initial DislocationInitial DislocationNikkuNikku R. R. ActaActa OrthopOrthop Scand 68:419, 1997Scand 68:419, 1997
Findings: Compared Findings: Compared multiplemultiple techniques techniques vsvs nonopnonop carecare
2.2. Operative Controversy Repair Technique:Operative Controversy Repair Technique: Not EBM!Not EBM! Distal based Distal based (Fulkerson, Modified E(Fulkerson, Modified E--T) T) vsvs medial medial retinaculumretinaculum repairrepair
Davis & Davis & FithianFithian. CORR, p 38, 2002. CORR, p 38, 2002

VSM
TREATMENT SPECTRUM!TREATMENT SPECTRUM!
1.1.Osteochondral loose Osteochondral loose bodiesbodies
2.2. Recurrent and Recurrent and crepituscrepitus3.3. Initial, Initial, atraumaticatraumatic, , abnlabnl
tracking & increased Q tracking & increased Q angleangle
4.4. Recurrent instabilityRecurrent instability
1.1. Initial, traumatic, Initial, traumatic, nlnltracking & Q angletracking & Q angle
2.2. Skeletally immatureSkeletally immature3.3. Discontinue sportsDiscontinue sports
Operative(Indicated)
Nonoperative(Recommended)Relative

VSM
References (1)References (1)
•• Arendt EA, Arendt EA, FithianFithian DC, Cohen E. Current concepts of DC, Cohen E. Current concepts of lateral patella dislocation. lateral patella dislocation. ClinClin Sports Med. 2002 Jul; Sports Med. 2002 Jul; 21(3): 49921(3): 499--519519
•• BrosseauBrosseau L, L, CasimiroCasimiro L, Robinson V, Milne S, Shea B, L, Robinson V, Milne S, Shea B, Judd M, Wells G, Judd M, Wells G, TugwellTugwell P. Therapeutic ultrasound for P. Therapeutic ultrasound for treating treating patellofemoralpatellofemoral pain syndrome (Review) The pain syndrome (Review) The Cochrane Collaboration 2006.Cochrane Collaboration 2006.
•• Clark DI, Downing N, Mitchell J, Clark DI, Downing N, Mitchell J, CoulsonCoulson L, L, SyzprytSyzpryt EP, EP, Doherty M. Physiotherapy for anterior knee pain: a Doherty M. Physiotherapy for anterior knee pain: a randomisedrandomised controlled trial. Annals of the Rheumatic controlled trial. Annals of the Rheumatic Diseases 2000; 59 (9): 700Diseases 2000; 59 (9): 700--4. 4.
•• DathDath Dr, Chakravarthy J, Porter KM. Patella dislocations. Dr, Chakravarthy J, Porter KM. Patella dislocations. Trauma 2006; 8: 5Trauma 2006; 8: 5--11.11.

VSM
References (2) References (2)
•• Davidson K. Davidson K. PatellofemoralPatellofemoral pain syndrome. American pain syndrome. American Family Physician. 1993.Family Physician. 1993.
•• D'hondtD'hondt NE, NE, StruijsStruijs PAA, PAA, KerkhoffsKerkhoffs GMMJ, GMMJ, VerheulVerheul C, C, LysensLysens R, R, AufdemkampeAufdemkampe G, Van G, Van DijkDijk CN. CN. OrthoticOrthoticdevices for treating devices for treating patellofemoralpatellofemoral pain syndrome. pain syndrome. Cochrane Database of Systematic ReviewsCochrane Database of Systematic Reviews 2002, Issue 2002, Issue 2. Art. No.: CD002267. DOI: 2. Art. No.: CD002267. DOI: 10.1002/14651858.CD002267.10.1002/14651858.CD002267.
•• FithianFithian DC, Paxton EW, Stone ML, Silva P, Davis DK, DC, Paxton EW, Stone ML, Silva P, Davis DK, Elias DA, White LM. Epidemiology and Natural History of Elias DA, White LM. Epidemiology and Natural History of Acute Patellar Dislocation. The American Acute Patellar Dislocation. The American JounralJounral of of Sports Medicine. 32: 1114Sports Medicine. 32: 1114--1121 (2004).1121 (2004).
•• Gaffney K, Gaffney K, FrickerFricker P, Dwyer T, Barrett E, P, Dwyer T, Barrett E, SkibinskiSkibinski K, K, Coutts R. Coutts R. PatellofemoralPatellofemoral joint pain: a comparison of joint pain: a comparison of two treatment two treatment programmesprogrammes. . ExcelExcel 1992; 8: 1791992; 8: 179--189.189.

VSM
References (3)References (3)
•• GrelsamerGrelsamer RP, Klein JR. The Biomechanics of the RP, Klein JR. The Biomechanics of the PatellofemoralPatellofemoral Joint. Journal of Orthopedic & Sports Joint. Journal of Orthopedic & Sports Physical Therapy. 1998; 28(5): 286Physical Therapy. 1998; 28(5): 286--298.298.
•• HeintjesHeintjes E, Berger MY, E, Berger MY, BiermaBierma--ZeinstraZeinstra SMA, SMA, BernsenBernsenRMD, RMD, VerhaarVerhaar JAN, JAN, KoesKoes BW. Pharmacotherapy for BW. Pharmacotherapy for patellofemoralpatellofemoral pain syndrome (Review). The Cochrane pain syndrome (Review). The Cochrane Collaboration. 2004. Collaboration. 2004.
•• HeintjesHeintjes E, Berger MY, E, Berger MY, BiermaBierma--ZeinstraZeinstra SMA, SMA, BernsenBernsenRMD, RMD, VerhaarVerhaar JAN, JAN, KoesKoes BW. Exercise therapy for BW. Exercise therapy for patellofemoralpatellofemoral pain syndrome (Review). The Cochrane pain syndrome (Review). The Cochrane Collaboration. 2006.Collaboration. 2006.
•• Holmes SW, Holmes SW, GlancyGlancy WG. Clinical classification of WG. Clinical classification of patellofemoralpatellofemoral pain and pain and dysfunctinodysfunctino. Journal of . Journal of Orthopaedic and Sports Physical Therapy 1998; 28(5): Orthopaedic and Sports Physical Therapy 1998; 28(5): 299299--306.306.

VSM
References (4)References (4)
•• KannusKannus P, P, NatriNatri A, A, PaakkalaPaakkala T, Jarvinen M. An outcome T, Jarvinen M. An outcome study of chronic study of chronic patellofemoralpatellofemoral pain pain syndnromesyndnrome. Seven. Seven--year followyear follow--up of patients in a randomized, controlled up of patients in a randomized, controlled trial. Journal of Bone and Joint Surgery. American trial. Journal of Bone and Joint Surgery. American Volume 1999; 81(3): 355Volume 1999; 81(3): 355--63. 63.
•• NatriNatri A, A, KannusKannus P, P, JarvineneJarvinene M. Which factors predict M. Which factors predict the longthe long--term outcome in chronic term outcome in chronic patellofemoralpatellofemoral pain pain syndrome? A 7syndrome? A 7--yr prospective followyr prospective follow--up study. up study. Medicine & Science in Sports & Exercise 1998; 30(11): Medicine & Science in Sports & Exercise 1998; 30(11): 15721572--77.77.
•• Sanders TG, Sanders TG, ParuchuriParuchuri NB, NB, ZlatkinZlatkin MB. MRI of MB. MRI of osteochondralosteochondral defects of the lateral femoral defects of the lateral femoral condylecondyle: : incidence and pattern of injury after transient lateral incidence and pattern of injury after transient lateral dislocation of the patella. American Journal of dislocation of the patella. American Journal of RoentgenologyRoentgenology 2006; 187: 13322006; 187: 1332--1337. 1337.