Embed Size (px)
Citation preview

Patella Fractures & Extensor Mechanism Injuries
Lisa K. Cannada, MDRevised: October 2008; May 2011

Anatomy
• Largest sesamoid bone• Thick articular
cartilage proximally• Articular surface
divided into medial and lateral facets by longitudinal ridge
• Distal pole nonarticular

Anatomy
• Patellar Retinaculum– Longitudinal tendinous
fibers
– Patellofemoral ligaments
• Blood Supply– Primarily derived from
geniculate arteries

Biomechanics
• The patella undergoes approximately 7 cm of translation from full flexion to extension
• Only 13-38% of the patellar surface is in contact with the femur throughout its range of motion

Biomechanics
• The patella increases the moment arm about the knee– Contributes up to 30%
improvement in lever arm
• Patella withstands compressive forces greater than 7X body weight with squatting

Biomechanics
• 2 X Torque:– Extend final 15°
– Than to extend from a fully flexed position to 15 degrees of flexion

Physical Examination
• Pain, swelling, contusions, lacerations and/or abrasions at the site of injury– Can determine timing of operative intervention
• Palpable defect
• Assessment of ability to extend the knee – Cannot perform a straight leg raise with no
extensor lag

Radiographic Evaluation• AP & Lateral
– Note patella height (baja or alta)
– Note fracture pattern• Articular step-off, diastasis
• Marginal impaction
• Special views– Axial or sunrise
• CT Scan- Occult Fractures
- Complex or Marginal Impaction Fractures

Radiographic Evaluation
• Bipartite Patella:• Don’t get fooled!
– Obtain bilateral views
– Often superolateral corner
(Saupe Classification, 1923)
– Accessory ossification center
– Occurs 1-2% of patients

Etiology
• Direct trauma– Direct blow to flexed knee (dashboard)– Increasing cases with penetrating trauma– Comminution & articular marginal impaction
• Indirect trauma– Flexion force directed through the extensor
mechanism against a contracted quadriceps– Simple, transverse fracture

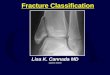
Classification• Allows guidance with
treatment • Types
– Transverse
– Marginal
– Vertical
– Comminuted
– Osteochondral
– Avulsion (not pictured)
Tip: Vertical fractures may not result in disruption of extensor mechanism

OA/OTA Classification

Nonoperative Treatment
• Indicated for minimally or nondisplaced fractures– < 2mm of articular step-off & < 3mm of diastasis with an
intact extensor mechanism (extensor retinaculum)
– If difficulty assessing, consider intra-articular injection of local anesthetic to better assess ability to extend
• Consider for minimally displaced fractures in low demand patients (evaluate comorbidities & function)
• Patients with a extensive medical comorbidities

Nonoperative Treatment
• Long leg cylinder cast for 4-6 weeks– May consider a knee immobilizer or hinged
knee brace for the elderly/low demand
• Immediate weight-bearing as tolerated
• Rehabilitation includes range of motion exercises with gradual quadriceps strengthening
• Protect eccentric contraction 3 months

Operative Treatment• Goals
– Preserve extensor function– Restore articular congruency
• Preoperative Setup– Tourniquet (debatable)
• Prior to inflation, gently flex the knee
• Approach– Longitudinal midline incision
recommended– Transverse approach alternative (dotted
lines) – potentially higher risk wound problems, can limit initiation of ROM
– Consider future surgeries!

Procedure
Longitudinal Incision
Clean Fracture Site
Torn Retinaculum
Longitudinal Incision
Clean Fracture Site
Torn Retinaculum

ProcedureReduce & Compress Fracture

Operative Techniques
• K-wires w/ tension band wiring (TBW)
• Lag-screw fixation
• Cannulated lag-screw with TBW (tension band screw – TBS)
• Partial patellectomy
• Total Patellectomy

Tension Band Wiring• Transverse, non-comminuted
fractures
• Reduce and clamp, then place two parallel 1.6mm K- wires placed perpendicular to the fracture
• 18 gauge wire passed behind proximally and distally
• Double Figure-8 wire for equal compression

Tension Band Wiring
• Wire converts anterior distractive forces to compressive forces at the articular surface
• Two twists are placed on opposite sides of the wire– Tighten simultaneously to achieve
symmetric tension
• Retinacular Injury– Keep open until the end
– Window to assess articular reduction
– Repair the retinacular injury last

Lag-Screw Fixation
• Indicated for stabilization of comminuted fragments in conjunction w/ cerclage wires if necessary
• May also be used as an alternative/adjunct to TBW for transverse or vertical fractures

Example

Example

Lag-Screw Fixation
• Contraindicated for extensive comminution and osteopenic bone
• Small secondary fractures may be stabilized with 2.0mm, 2.7mm or 3.5mm cortical screws
• Reduce out of plane fragments to main fragments superiorly and inferiorly
• Transverse or vertical fractures require 3.5mm, 4.0mm, or 4.5mm cortical screws– Retrograde insertion of screws may be technically
easier

Cannulated Lag-Screw With Tension Band (TBS)
• Partially threaded cannulated screws (4.0mm)
• Wire through screws and across anterior patella in figure of eight tension band
• Make sure tip of screw remains buried in bone so it will not compromise wire

Cannulated Lag-Screw With Tension Band
• More stable construct – Screws and tension band wire combination
eliminates both possible separation seen at the fracture site with K wire/TBW and screw failure due to excessive three point bending

Suture vs. Wire Tension Band
Gosal et al Injury 2001• Wire v. #5 Ethibond• 37 patients• Reoperation 38% wire
group vs. 6%• Infection 3 pts wire
group vs. 0
Patel et al, Injury 2000McGreal et al, J Med
Eng Tech, 1999• Cadaveric models• Quality and stability
of fixation comparable to wire
• Conclude suture an acceptable alternative

Partial Patellectomy
• Indicated for fractures involving extensive comminution not amenable to fixation
• Larger fragments repaired with screws to preserve maximum cartilage
• Smaller fragments excised– Usually involving the distal pole

Partial Patellectomy
• Tendon is attached to fragment with nonabsorbable suture passed through drill holes in the fragment– Drill holes should be near the articular surface
to prevent tilting of the patella
• Load sharing wire passed through drill holes in the tibial tubercle and patella may be used to protect the repair and facilitate early range of motion

Total Patellectomy
• Indicated for displaced, comminuted fractures not amenable to reconstruction
• Bone fragments sharply dissected
• Defect may be repaired through a variety of techniques
• Usually results in extensor lag (30°) and loss of strength (30%) – H Kaufer, JBJS

Postoperative Management
• Immobilization with knee brace, WBAT in extension• Early range of motion
– Based on intraoperative assessment of repair & bone quality– Active flexion with passive extension
• Quadriceps strengthening– Begin when there is radiographic evidence of healing,
usually around 6 weeks• Modify depending upon fracture, osteoporosis,
comorbidities, tenuous fixation and/or wounds at risk

Complications
• Knee Stiffness– Most common
complication
• Infection– Rare, depends on soft
tissue compromise
• Loss of Fixation– Hardware failure in up
to 20% of cases
• Osteoarthritis– May result from
articular damage or incongruity
• Nonunion < 1% with surgical repair
• Painful hardware– Removal required in
approximately 15%

Nonunion

Loss of Fixation

Malunion

Extensor Tendon Ruptures
• Patients are typically males in their 30’s or 40’s– Patellar < 40 yo
– Quadriceps > 40 yo
• Mechanism– Fall
– Sports “The weekend warrior”
– MVA
– Tendonopathies, Steroids, Renal Dialysis

Quadriceps Tendon Rupture
• Typically occurs in patients > 40 years old
• Usually 0-2 cm above the superior pole
• Level often associated with age– Rupture occurs at the bone-tendon junction in
majority of patients > 40 years old– Rupture occurs at midsubstance in majority of
patients < 40 years old

Quadriceps Tendon Ruptures
• Risk Factors– Chronic tendonitis
– Anabolic steroid use
– Local steroid injection
– Inflammatory arthropathy
– Chronic renal failure
– Systemic disease

History
• Sensation of a sudden pop while stressing the extensor mechanism (eccentric load)
• Pain at the site of injury
• Inability to extend the knee
• Difficulty weight-bearing

Physical Exam
• Effusion • Tenderness at the
upper pole• Palpable defect above
superior pole• Loss of extension• With partial tears,
extension will be intact

Quadriceps Tendon Rupture
Radiographic Evaluation• X-ray- AP, Lateral, and
Tangential (Sunrise, Merchant)– Distal displacement of
the patella (patella baja)
• MRI– Useful when diagnosis
is unclear
Treatment• Nonoperative
– Partial tears and strains
• Operative– For complete ruptures

Operative Treatment
• Reapproximation of tendon to bone using nonabsorbable sutures with tears at the muscle-tendon junction– Locking stitch (Bunnel, Krakow) with No. 5
ethibond passed through vertical bone tunnels– Repair tendon close to articular surface to avoid
abnormal patellar tilting

Operative Treatment
• Midsubstance tears may undergo end-to-end repair after edges are freshened and slightly overlapped– May benefit from
reinforcement from distally based partial thickness quadriceps tendon turned down across the repair site (Scuderi Technique)

Treatment
• Chronic tears may require a V-Y advancement of a retracted quadriceps tendon (Codivilla V-Y-plasty Technique)

Postoperative Management
• Knee immobilizer, Hinged Knee Brace, or cylinder cast for 5-6 weeks
• Immediate weight-bearing as tolerated
• At 2-3 weeks, hinged knee brace starting with 45 degrees active range of motion with 10-15 degrees of progression each week

Complications
• Rerupture• Persistent quadriceps
atrophy/weakness• Loss of motion• Infection

Patellar Tendon Rupture
• Less common than quadriceps tendon rupture
• Associated with degenerative changes of the tendon
• Rupture often occurs at inferior pole insertion site

Patellar Tendon Rupture
• Risk Factors– Rheumatoid arthritis– Systemic Lupus
Erythematosus– Diabetes– Chronic Renal Failure– Systemic
Corticosteroid Therapy– Local Steroid Injection – Chronic tendonitis

Anatomy
• Patellar tendon– Averages 4 mm thick but widens to 5-6 mm at
the tibial tubercle insertion– Merges with the medial and lateral retinaculum– 90% type I collagen

Blood Supply
• Fat pad vessels supply posterior aspect of tendon via inferior medial and lateral geniculate arteries
• Retinacular vessels supply anterior portion of tendon via the inferior medial geniculate and recurrent tibial arteries
• Proximal and distal insertion areas are relatively avascular and subsequently are a common site of rupture

Biomechanics
• Greatest forces are at 60 degrees of flexion
• 3-4 times greater strain are at the insertions compared to the midsubstance prior to failure
• Forces through the patellar tendon are 3.2 times body weight while climbing stairs

History
• Often a report of forceful quadriceps contraction against a flexed knee
• May experience and audible “pop”
• Inability to weightbear or extend the knee

Physical Examination
• Palpable defect• Hemarthrosis • Painful passive knee
flexion• Partial or complete
loss of active extension
• High riding patella on radiographs (patella alta)

Radiographic Evaluation
• AP and Lateral X-ray– Patella alta seen on lateral view
• Patella superior to Blumensaat’s line
• Ultrasonagraphy– Effective means to confirm diagnosis by determining
continuity of tendon– Operator and reader dependant
• MRI– Effective means to assess patellar tendon, especially if
other intraarticular or soft tissue injuries are suspected– Relatively high cost

Classification
• No widely accepted means of classification
• Can be categorized by:– Location of tear
• Proximal insertion most common
– Timing between injury and surgery• Most important factor for prognosis
• Acute: < 2 weeks
• Chronic: > 2 weeks

Treatment
• Surgical treatment is required for restoration of the extensor mechanism
• Repairs categorized as early or delayed

Early Repair
• Better overall outcome• Primary repair of the tendon• Surgical approach is through a midline incision
– Incise just lateral to tibial tubercle as skin thicker with better blood supply to decrease wound complications
• Patellar tendon rupture & retinacular tears are exposed• Frayed edges and hematoma are debrided

Early Repair
• With a Bunnell or Krakow stitch, two ethibond sutures or their equivalent are used to repair the tendon to the patella
• Drill holes in patella in mid-sagittal plane to prevent cut out of suture
• Sutures passed through three parallel, longitudinal bone tunnels and tied proximally

Early Repair
• Repair retinacular tears• May reinforce with wire,
cable or umbilical tape• Assess repair
intraoperatively with knee flexion

Postoperative Management
• Maintain hinged knee brace which is gradually increased as motion increases (tailor to the patient)
• Immediate vs. delayed (3 weeks) weightbearing as tolerated
• At 2-3 weeks, hinged knee brace starting with 45 degrees active range of motion with 10-15 degrees of progression each week
• Immediate isometric quadriceps exercises• All restrictions are lifted after full range of motion and
90% of the contralateral quadriceps strength are obtained; usually at 4-6 months

Delayed Repair
• > 6 weeks from initial injury• Often results in poorer outcome• Quadriceps contraction and patellar migration are
encountered• Adhesions between the patella and femur may be
present • Options include hamstring and fascia lata
autograft augmentation of primary repair or Achilles tendon allograft

Postoperative Management
• More conservative when compared to early repair
• Bivalved cylinder cast for 6 weeks; may start passive range of motion
• Active range of motion is started at 6 weeks

Complications
• Knee stiffness
• Persistent extensor weakness
• Rerupture
• Infection
• Patella baja (Insall-Salvati ratio of < 0.8)

References Patella Fractures: New
• Hughes SC, Stott PM, Hearnden AJ, Ripley LG: A new and effective tension band braided polyester suture technique for transverse patellar fracture fixation. Injury 2007:38:212-222.
• Luna-Pizarro D, Amato D, Arellano F, Hernandez A, Lopez-Rojas P: Comparison of a technique using a new percutaneous osteosynthesis device with conventional open surgery for displaced patella fractures in a randomized controlled trial. J Orthop Trauma 2006; 20:529-535.

References Patella Fractures: Classic
• Carpenter JE, Kasman R. Matthews LS: Fractures of the patella. Instr Course Lect 1994: 43:97-108.
• Burvant JG, Thomas KA, Alexander R, Harris MB. Evaluation of methods of internal fixation of transverse patella fractures: A biomechanical study. J Orthop Trauma 1994;8:147-153.
• Einola S, Aho AJ, Kallio P. Patellectomy after fracture: long term follow-up results with special reference to functional disability. Acta Orthop Scand 1976:47:441-447.

References:Extensor Mechanism Injuries
• Siwek CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am 1981; 63:932-937.
• Bhargava SP, Hynes MC, Dowell JK. Traumatic patella tendon rupture: early mobilization following surgical repair. Injury 2004;35:76-79.
• Konrath GA, Chen D, Lock T et al. Outcomes following repair of quadriceps tendon ruptures. J Orthop Trauma 1998;12:273-279.

Thank You!Thank You!
Return to Lower Extremity
Index
E-mail OTA about
Questions/Comments
If you would like to volunteer as an author for the Resident Slide Project or recommend updates to any of the following slides, please send an e-mail to [email protected]