Embed Size (px)
Citation preview

Integrative Care for Diabetes
Patana Teng-umnuay MD PhD

Why we fail to treat T2DM?
• Poor diet and lack of exercise.
• Refuse to prevent diabetes with metformin.
• Unaware of disease progression and beta cell failure.
• Current blood sugar lowering agents (despite recommended by American Diabetes Association) provide risk of hypoglycemia, beta cell apoptosis, obesity, and hyperlipidemia.
• Unwilling to switch from oral hypoglycemic agent to insulin therapy
• Lack of integrative approach

How to Approach Patents with Diabetes?
• Diabetes is the sign of early aging, so anti-aging
medicine is the key for diabetes prevention and
treatment.
• However, most patients, doctors, health care providers,
and insurance company rely on DRUGS so most of the
useful and integrative care won’t get reimbursement!
• The patients are their best doctors. We can only give
them practical advice.
• Exercise and Diets that fit their life styles are the keys.
• Supplements can do wonders.

A Lot of problems come from drugsHow can you ask patients to refrain from it?
• In my experience, a lot of patients were better when they stopped taking certain drugs!
• However, don’t ask patients to stop their medicine unless you know for sure that it is harmful.
• Lower the dosage with caution (statin, anti-depressants). Use only medicine that you know well.
• Understand side-effects of each medicine. Keep telling yourself that the patients problem may be caused by drugs.
• Use counter actions (advice coenzyme Q10 to patients who receive statin, melatonin and 5HTP against sleeping pills, baking soda against proton pump inhibitors, stanol against lipid lowering agent, fish oil instead of anti-platelets)

Common Medical Side Effects
• Statin – cramps, muscle pain – can be resolved by dosage reduction and high dose coenzyme Q10 (200 mg/day), renal failure, diabetes, dementia, hepatitis.
• Diuretic – hypokalemia, hyponatremia, hyperuricemia, and renal failure – stop or change to spironolactone (K-sparing diuretic)
• Sulfonylurea – renal failure, beta cell apoptosis
• Calcium antagonists can cause edema – reducing the dosage in half usually solves the problem.
• Omeprazole – kidney failure, dementia
• Warfarin – atherosclerosis
• Aspirin – bleeding
• Paracetamol – hepatic failure, renal failure
• Prednisolone – diabetes, weight gain, adrenal fatigue, infection

Integrative treatment for diabetes
• Stop sulfonylurea drugs, control blood sugar with metformin and if necessary insulin.
• Cut down sugar and refined carbohydrate (sugar is toxin)
• Grains over rice
• Mixed vegetables or seeds and nuts with rice and pasta.
• Cut down high-inflammatory food such as soy bean oil, cow’s milk, and overcooked animal fats
• Add simple exercise program in patients lifestyle
• Vitamin D3
• Benfotiamine
• Pyridoxamine
• Lipoic acid
• Since atherosclerosis is common in diabetes integrative approach to prevent atherosclerosis is important.
But… do not over prescribe supplements
• Patients who have chronic diseases have already had a huge
load of medicine and they are sick of their medicine, so they
will not want to hear about taking more supplements.
• Supplements can be expensive, understand how much the
patients can pay or are willing to pay.
• So, you need to cut down their medicine and use vitamins as
a substitute… little by little.
• Don’t try to prescribe over 2-3 new supplements during each
visit.
• Explain to them that vitamins are not drugs and they will help
the patient’s body to adapt and repair themselves.

Exercise• Preventing diabetes, hypertension, osteoarthritis, spondylosis,
cardiovascular disease.
• Good time for cardiovascular exercise is 1-2 hour after big meal (to
get rid of high blood glucose)
• Weight bearing exercise is important. It should be followed by
stretching.
• Need to have some physical stress but not mental stress.
• However, light exercise is better than none.
• Drink mineral water, not reverse osmosis water.
• Adjust exercise program to fit your patients’ medical condition.
Sometimes, you may want to consult physical therapist.
• Find motivation for your patient, not everyone can do the same thing.
Some can swim and some can not. Some can ride a bike and some
can not.

Resistance Training Lowers Risk of
Metabolic SyndromeMayo Clinic Proceedings 2017;92:1214-1222
• Roughly 7400 middle-aged adults underwent detailed physical
exams and provided information on their aerobic and resistance
exercise habits. During a median 4 years' follow-up, 15% of
participants developed metabolic syndrome.
• After adjustment for potential confounders like aerobic exercise
levels, doing any resistance exercise was associated with lower risk
for metabolic syndrome, compared with no resistance training
(hazard ratio, 0.83). People who met guidelines for recommended
amounts of both resistance exercise (≥2 days/wk) and aerobic
exercise (≥500 metabolic equivalent min/wk) had a 25% lower risk
for metabolic syndrome than those who didn't hit the recommended
amounts.

Primary care-led weight management for
remission of type 2 diabetes (DiRECT)Lean MEJ et al. Lancet: Dec 5, 2017.
• Nearly 50 U.K. primary care practices were randomized to deliver
either a weight loss intervention or best-practice care (control) to
300 non-insulin-dependent adults with type 2 diabetes (diagnosed
within past 6 years) and a BMI of 27–45.
• For the intervention, patients discontinued antidiabetic and
antihypertensive drugs and followed a low-calorie formula diet (825–
853 calories daily) for 3 months. This was followed by reintroduction
of food and physical activity strategies for 2–8 weeks, and then
weight loss maintenance.
• At 12 months, 24% of participants in the intervention group lost 15
kg or more; none in the control group did. Diabetes remission was
also higher with the intervention (46% vs. 4%).

Dietary Advice for Diabetes
• Caloric restriction or try intermittent fasting
• Grains over Rice
• Sugar is toxin
• Olive oil or rice bran oil
• Avoid dairy products, non-sweetened milk contains sugar called lactose
• Soil-grown vegetables
• Too much fruit = too much sugar
• Mineral water or alkaline water
• Sugar free soft drink is acidic and not healthy.
Regular Consumption of Sugar-Sweetened Beverages Is Associated with Excess Risk for Type 2 Diabetes
BMJ 2015; 351:h3576
• Researchers performed a systematic review and meta-analysis of
17 multinational cohort studies (>460,000 adults; age range, 19–84).
Median follow-up ranged from 3.4 to 21.1 years. About 28,000 study
patients developed type 2 diabetes.
• Higher consumption of sugar-sweetened beverages was associated
with significantly higher risk for type 2 diabetes: 18% higher risk per
1 serving daily. After adjustment for baseline adiposity, risk was still
13% higher. Consuming artificially sweetened beverages also
was associated with higher risk (25% and 8% higher risk per 1
serving daily, before and after adjusting for adiposity) as was
consuming fruit juices (5% and 7% higher risk per 1 serving
daily, before and after adjustment).

Artificial sweeteners like are not associated with reduced BMI and may even increase it!
CMAJ 2017;189(28).
• Researchers identified 37 studies that looked at the effects of
artificial sweeteners in 400,000 people over age 12.
• In randomized trials with a median 6 months' follow-up, the primary
outcome, BMI, was not associated with intake of artificial
sweeteners.
• Three long-term cohort studies suggested a modest increase in BMI
over time with increased artificial sweetener consumption.
• For secondary outcomes like weight, metabolic syndrome, and type
2 diabetes, the observational studies again found higher risk with
increased intake.
According to a reanalysis of 45-year-old data,swapping out saturated fats with omega-6 fatty acid doesn't seem to improve clinical outcomes and may even be tied to
worse survival among seniors. BMJ 2016;353:i1246
• In the 1968–73 Minnesota Coronary Experiment, a cohort of adults in mental institutions or a nursing home were randomized to one of two diets: one that replaced saturated fats with vegetable oil rich in omega-6 linoleic acid or a control diet high in saturated fat. Researchers have now reanalyzed the data, including unpublished material, of 2400 participants who followed the diets for at least 1 year.
• The intervention group had a greater reduction in serum cholesterol than the control group. However, this didn't translate to a lower mortality rate. Among seniors, mortality risk seemed higher with the intervention diet, but there were not enough data to confirm this finding.
A high-fat Mediterranean diet doesn't lead to weight gain and might help with weight loss
Estruch R et al. Lancet Diabetes and Endocrinology 2016;4:666-676
• Roughly 7500 older men and women in Spain were randomized to follow a high-fat Mediterranean diet supplemented with either nuts or extra-virgin olive oil, or a lower-fat control diet.
• The Mediterranean diets aimed to increase fat intake to more than 40% of daily calories, while the control diet aimed to reduce fat intake to less than 30% of calories.
• During 5 years' follow-up, participants following the olive oil-rich Mediterranean diet lost significantly more weight than the control group (about half a kilogram more).
• In addition, waist circumference was lower with the two Mediterranean diets than with the control diet.

Benefits of the Mediterranean Diet Go Beyond Cardioprotection A randomized clinical trial
JAMA Intern Med 2015 Sep 14
• To examine the effect of the MeD on breast cancer incidence,
researchers in Spain conducted a secondary analysis of a large
randomized trial originally designed to assess cardiovascular effects
of the MeD (supplemented either with extra-virgin olive oil [EVOO] or
nuts) versus a conventional reduced-fat diet in persons at high
cardiovascular risk The trial was stopped after a median of 4.8 years
because of cardiovascular benefit.
• The estimated 5-year incidence of breast cancer was significantly
lower in the MeD-plus-EVOO group than in the control group
(approximately 0.5% vs. 1.3%) — roughly one case fewer per 100
women on the EVOO diet.
Cinnamaldehyde induces fat cell-autonomous
thermogenesis and metabolic reprogrammingMetabolism 2017:77:58-64
• Researchers treated adipocytes from human volunteers with
cinnamaldehyde, an organic compound that gives cinnamon its
flavor.
• The volunteers varied in age, ethnicity, and body-mass index.
• The researchers found that the treated cells showed increased
expression of genes and enzymes that improve lipid metabolism.
Metabolic proteins involved in thermogenesis also increased in
treated cells.

การสวนลางล าไสColon Hydrotherapy
• เปนการลางอจจาระทตกคางในล าไสออก ซงควรท าโดยผเชยวชาญ
• เหมาะในคนทมปญหาทองอด ทองผก ภมแพ และปญหาทางผวพรรณ
• หามท าในคนทเคยผาตดล าไส มแผลททวารหนก หรอมโรคตดเชอในล าไส
• อาจท าใหเกดภาวะเกลอต าในเลอด ซงปองกนไดดวยการทานน าเกลอแร
18

Digestive Enzymes
• ตบออน มหนาทสราง อนสลน และ เอนซยม ยอยอาหาร คนไขทเปนเบาหวาน จงมกจะมปญหาในการยอย
• คนไข รวมทงแพทย ยงเขาใจผดวา ยาขบลม หรอยาลดกรดคอยาชวยยอย แตยาชวยยอยคอ เอนซยม
• เอนซยม ควรบรรจใน แคปซลททนกรด และควรมเอนซยมทยอย ไดทง โปรตน แปง ไขมน น าตาลแลคโตส และ เอนซยมยอยผก ทมนษย ไมม
• Serratiopeptidase มฤทธลดการอกเสบ
• Nattokinase มฤทธกนเลอดแขงตว
เอนซยมชวยยอยอาหารชวยลดสารพษในระบบทางเดนอาหาร และลดการอกเสบ
• Amylase
• Protease
• Lipase
• Cellulase
• Pectinase
• Lactase
• Serratiopeptidase

ประโยชนของเชอโรคในล าไสทมอยตามธรรมชาต หรอ โพรไบโอตคProbiotics
(yogurt, natto, fermented vegetables)
• ชวยสรางวตะมน
• ปองกนการตดเชอโรค
• ชวยก าจดสารพษ
• ปรบสมดลยของภมตานทานในรางกาย
21

• The formation of advanced glycation end products (AGEs) of mainly glucose-protein interactions, which form chemically cross-linked molecules
• Rate of formation of AGEs is proportional to the blood glucose level.
• AGEs have been identified in hemoglobin, b-2 microglobulin, b-amyloid protein, collagen, and lens crystalline.
• Deposition of AGEs results in protein dysfunction and inflammation
Advanced Glycation End Products
AdvancedGlycationEndproducts
Good carbohydrate is GRAINS
Low glycemic index
Reduce sugar absorption
High in vitamin B’s and EHigh in minerals

Preventing AGE with Special B’s
• Benfotiamine (active B1)
– Thiamine derivative with better bioavailability. Blocks three
major pathways of hyperglycemic damage (hexosamine,
advanced glycation end product, and diacylglycerol-protein
kinase pathway) and prevents experimental diabetic
complications.
• Pyridoxamine (active B6)
– Natural intermediate of vitamin B6 metabolism. Reduce AGE
accumulation in association with Improvemnets in renal and
vascular funtion in experimental diabetes. (Kidney Int
2002;61:939-50)
• Cancer chemopreventive activities.
(Science 1997;275:218)
• Increased lifespan in yeast, worms, and flies.
• Enhanced mitochondria activities.
• Increased aerobic capacity in mice.
(Nature 2004;430:686)
• Protected mice against diet-induced obesity and insulin resistance.
(Cell 2006;127:1109)
• Prevent the development of fatty liver in high-fat-diet mice.
(Nature 2006;444:337)
Resveratrol: Caloric restriction mimeticPolyphonolic compound found in red wine, grapes, blueburries, peanuts
Phytoestrogenic and antioxidant properties

Vitamin D Actions
• Source of vitamin D are from sunlight, food, and supplements.
• Vitamin D2 (plant) is 30% effective compared to vitamin D3 (skin).
• Metabolized in the liver to 25-OH vitamin D and in the kidneys to active form, 1,25-dihydroxy vitamin D.
• Normal vitamin D level: 30-50 ng/ml.
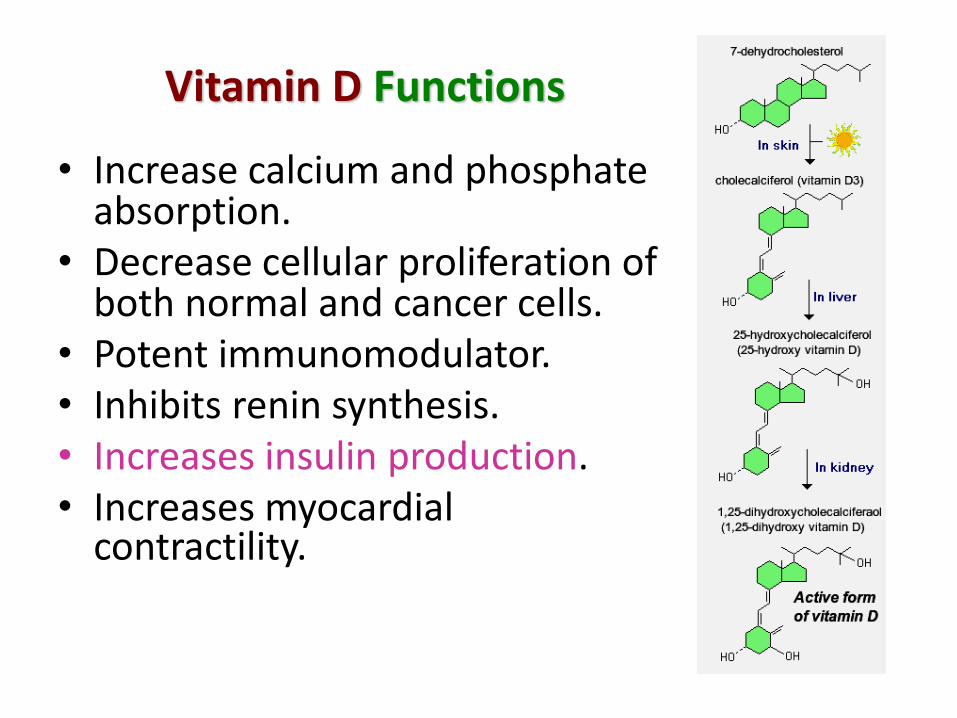
Vitamin D Functions
• Increase calcium and phosphate absorption.
• Decrease cellular proliferation of both normal and cancer cells.
• Potent immunomodulator.• Inhibits renin synthesis.• Increases insulin production.• Increases myocardial
contractility.

Vitamin D deficiency is associated with
• Osteomalacia, osteoporosis
• Diabetes (both type 1 and 2) (Diabetes Care 2006;29:650)
• High blood pressure (Hypertension 1997;30:150)
• Congestive heart failure (Am J Coll Cardiol 2003;41:105)
• High blood levels of inflammatory cytokines (Prog Biophys Molbiol 2006;92:39)
• Multiple sclerosis (JAMMA 2006;296:2832)
• Schizophrenia and depression (Schizophr Res 2002;54:199)
• Colon, breast, and prostate cancers (Am J Public health 2006;96:252)
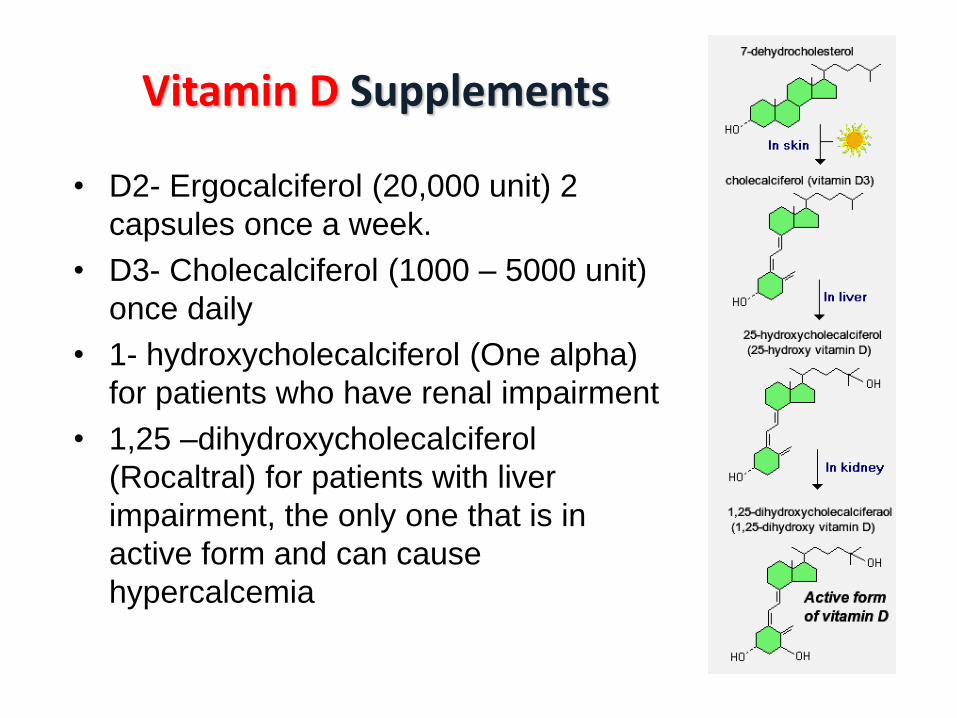
Vitamin D Supplements
• D2- Ergocalciferol (20,000 unit) 2
capsules once a week.
• D3- Cholecalciferol (1000 – 5000 unit)
once daily
• 1- hydroxycholecalciferol (One alpha)
for patients who have renal impairment
• 1,25 –dihydroxycholecalciferol
(Rocaltral) for patients with liver
impairment, the only one that is in
active form and can cause
hypercalcemia
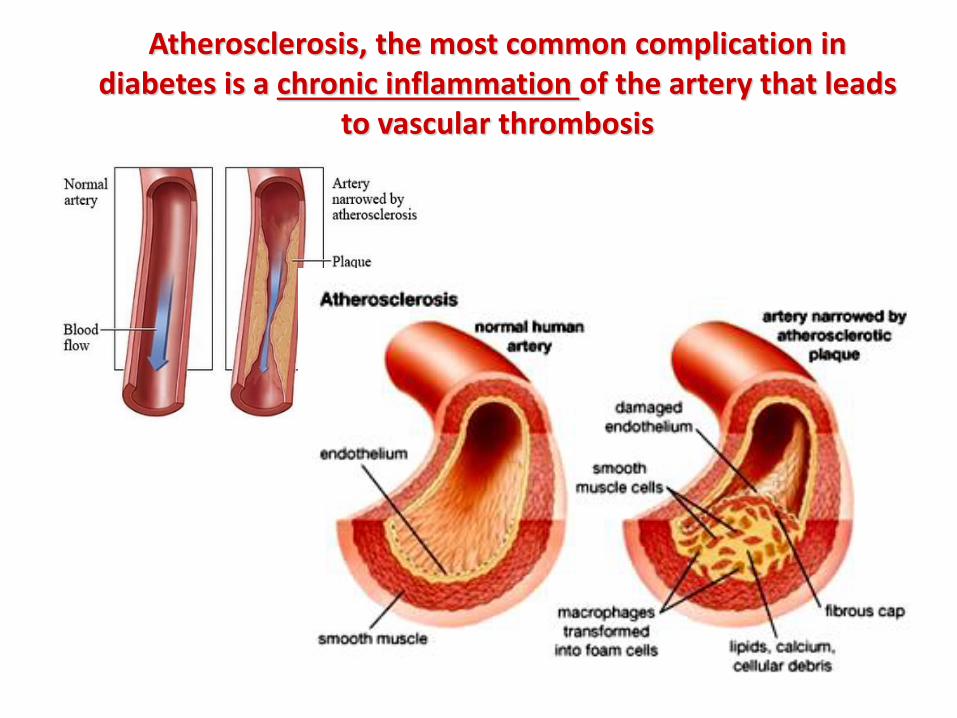
Atherosclerosis, the most common complication in diabetes is a chronic inflammation of the artery that leads
to vascular thrombosis

Integrative Treatment for Atherosclerosis
• Quit smoking
• Keep reminding your patients that sugar is TOXIN
• Cut down high-inflammatory food such as soy bean oil, cow’s
milk, and overcooked animal fats
• Eating food with high omega 9 such as olive oil, rice bran oil,
almond oil, and nuts
• Fish oil
• Vitamin K2
• Magnesium
• Vitamin C
• Coenzyme Q10 if they need statin
• Stop unnecessary calcium supplements
• Chelation
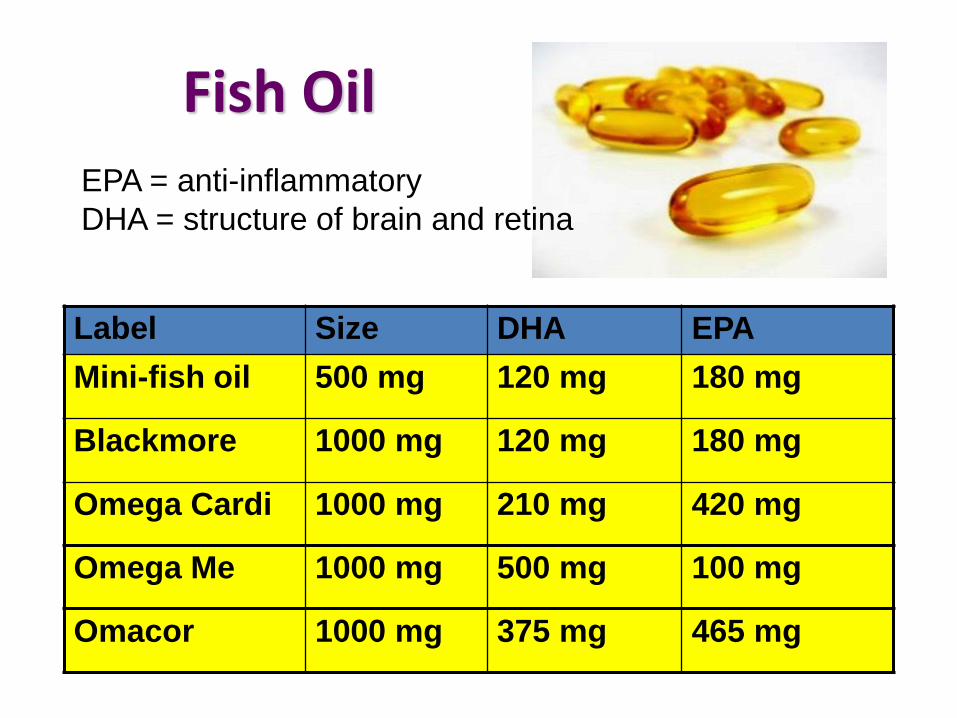
Fish Oil
Label Size DHA EPA
Mini-fish oil 500 mg 120 mg 180 mg
Blackmore 1000 mg 120 mg 180 mg
Omega Cardi 1000 mg 210 mg 420 mg
Omega Me 1000 mg 500 mg 100 mg
Omacor 1000 mg 375 mg 465 mg
EPA = anti-inflammatory
DHA = structure of brain and retina
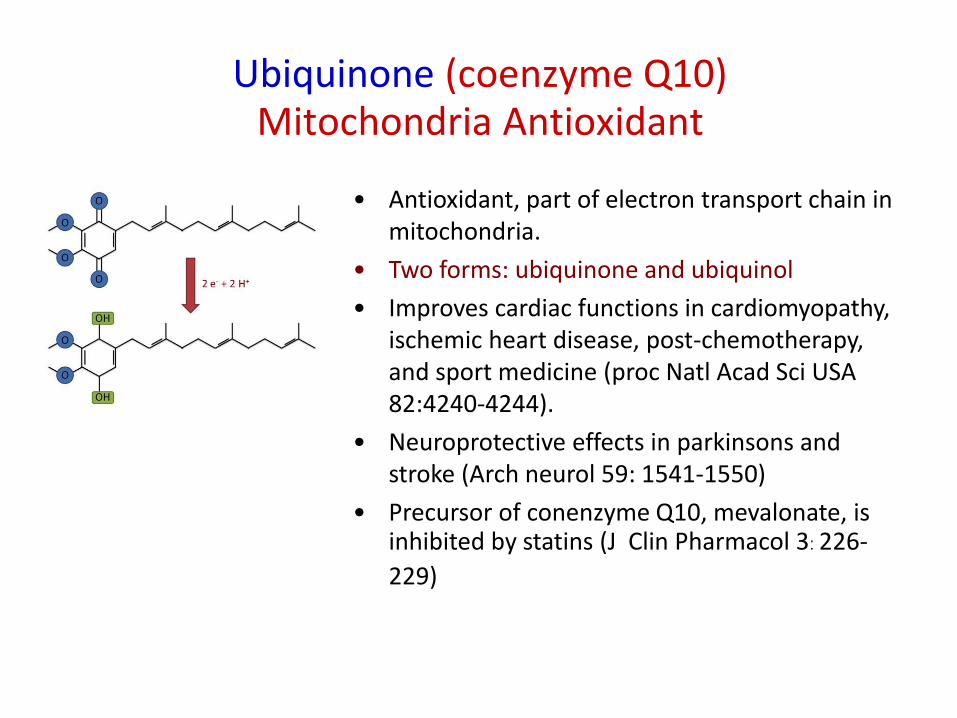
• Antioxidant, part of electron transport chain in mitochondria.
• Two forms: ubiquinone and ubiquinol
• Improves cardiac functions in cardiomyopathy, ischemic heart disease, post-chemotherapy, and sport medicine (proc Natl Acad Sci USA 82:4240-4244).
• Neuroprotective effects in parkinsons and stroke (Arch neurol 59: 1541-1550)
• Precursor of conenzyme Q10, mevalonate, is inhibited by statins (J Clin Pharmacol 3: 226-
229)
Ubiquinone (coenzyme Q10)Mitochondria Antioxidant

Human cells synthesize CoQ10 from tyrosine, through eight
enzymatic steps that require farnesyl diphosphate and vitamin B
cofactors such as folic acid, niacin, riboflavin, and pyridoxine. Statins
inhibit farnesyl diphosphate production resulting in CoQ10 deficiency.

Our body can make Coenzyme Q10; however, the
production is less when we are older.
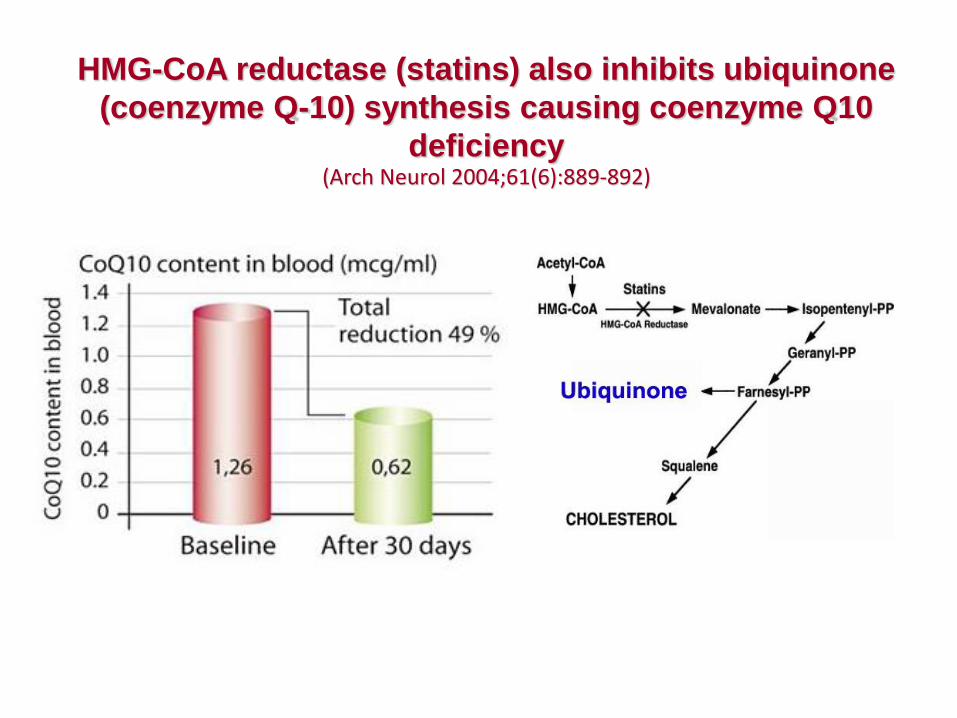
HMG-CoA reductase (statins) also inhibits ubiquinone
(coenzyme Q-10) synthesis causing coenzyme Q10
deficiency(Arch Neurol 2004;61(6):889-892)
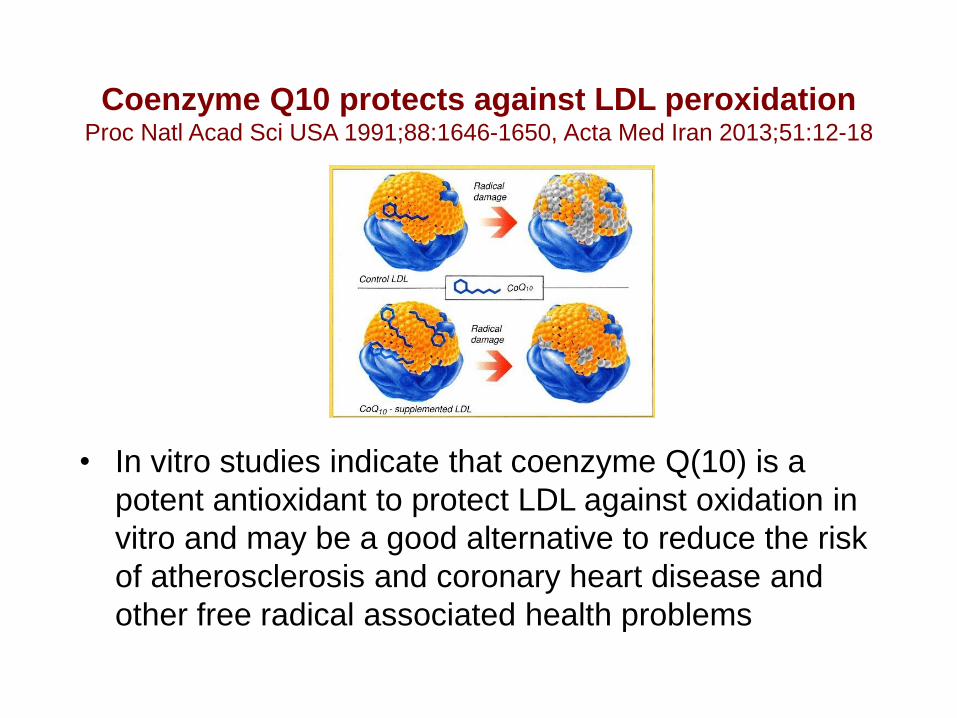
Coenzyme Q10 protects against LDL peroxidationProc Natl Acad Sci USA 1991;88:1646-1650, Acta Med Iran 2013;51:12-18
• In vitro studies indicate that coenzyme Q(10) is a
potent antioxidant to protect LDL against oxidation in
vitro and may be a good alternative to reduce the risk
of atherosclerosis and coronary heart disease and
other free radical associated health problems

Coenzyme Q-10 and Congestive Heart Failure
A number of intervention trials that administered supplemental conezyme Q10 (100-200 mg/d of coenzyme Q10 for one to three months) to congestive heart failure patients, in conjunction with conventional medical therapy, have demonstrated improvements in some cardiac functions, reduced morbidity and mortality.
• Belardinelli R, et al. Coenzyme Q10 and exercise training in chronic heart failure. Eur Heart J. 2006.
• Mortensen SA et al. The effect of conenzyme Q10 on morbidity and mortality in chronic heart failure. JACC Heart Failure 2014.
• Alehagen U. et al. Reduced cardiovascular mortality 10 years after supplementation with selenium and coenzyme Q10 for four years. PLoS One 2015.
• Alehagen U. et al. Supplementation with selenium and coenzyme Q10 reduces cardiovascular mortality in elderly with low selenium status. PLoS One 2016.
Coenzyme Q10 Supplement
Ubiquinol or Ubiquinone?
• Ubiquinone is an oxidized form of coenzyme Q10 while ubiquinol
is a reduced form and claimed to have better absorption.
• CoQ10 supplement usually sold in the form of ubiquinone and our
body can converted ubiquinone into ubiquinol.
• However, ubiquinol is very expensive and clinical studies using
ubiquinol is quite limited.
• Clinical studies have shown that high dose of coenzyme Q10
(100-200 mg/day) provides clinical benefits.

Alpha Lipoic Acid(R-Lipoic Acid)
Another Mitochondria Antioxidants
• Sulfur containing anti-oxidant
• Higher R-forms, better absorption.
• Functions everywhere! (blood, cell membrane, cytosol, and mitochondria)
• Vitamin C and other anti-oxidants re-generator
• Stabilizing NF kappa B transcription factor: anti-inflammatory effects
• Delay progression of chronic kidney disease in animal studies.
• Metal ion chelator (de-toxification)
• Side effect is prickly itchy skin

• Water soluble anti-oxidant for YOUR BLOOD
• Stimulate collagen synthesis good for the skin and bone
• Chelate heavy metal
• Instability, take it in the morning and drink plenty of water
• Excessive dose is excreted by kidney
• In patients with impaired kidney function, vitamin C is converted to oxalate leading to stone formation.

Rose Hip Oil
• Rich in ascorbic acid
• Anti-inflammatory fatty acids (oleic acid, gamma linolenicacid)
• Prevent obesity by the activation of adenosine 5′-monophosphate-activated protein kinase (AMPK) (Eur J Med
Chem. 2011;46:5189–5195)

Magnesium
• The adult human body contains about 25 grams of magnesium. Over 60% of all the magnesium in the body is found in the skeleton, about 27% is found in muscle.
• Magnesium is involved in more than 300 essential metabolic reactions including ATP production and active vitamin D synthesis.
• Magnesium helps relaxation of nerve and muscle and magnesium supplement has been used for the treatment of anxiety, cramp, eclampsia, and hypertension.
• Magnesium hydroxide is used as a laxative agent.

Food enriched with magnesium

Vitamin K2 promotes healthy bones and
prevent calcified blood vessels
• Menatetrenone is Vitamin K2, not Vitamin K1.
• Osteoblasts produce the vitamin K-dependent protein osteocalcin that binds calcium to the bone matrix and builds healthy bones.
• Vitamin K2 availablity decreases with aging. As a result, osteocalcin is not able to bind calcium and transport it to the bone matrix. This is one reason why calcium accumulates in the arterial wall.
• Another important Vitamin K2 protein called Matrix G1a protein. This essential K2 dependent protein is an inhibitor of arterial calcification.
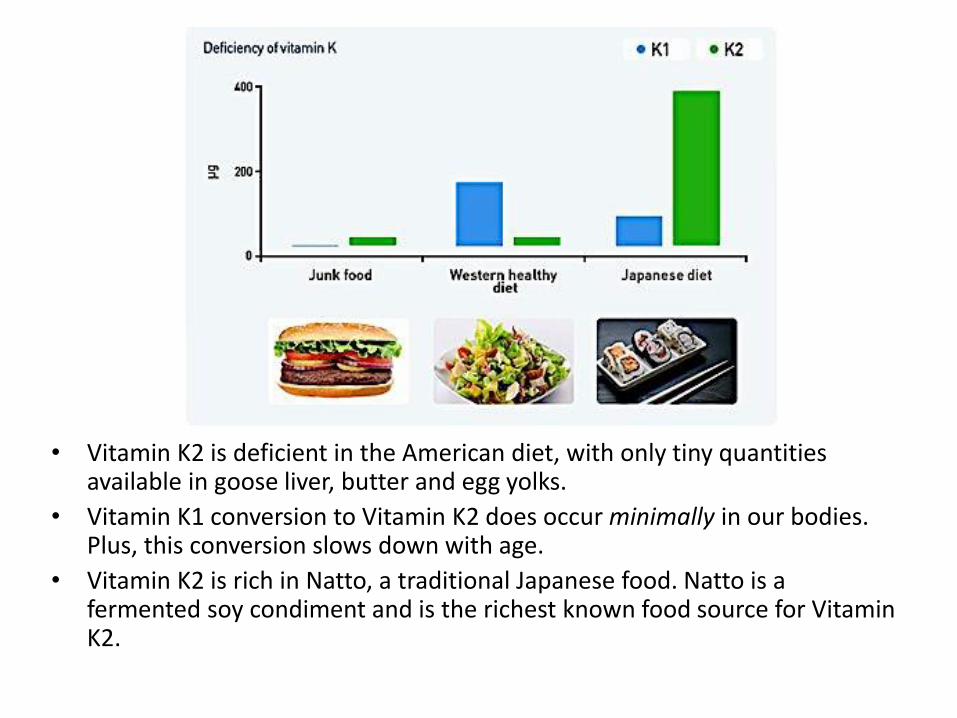
• Vitamin K2 is deficient in the American diet, with only tiny quantities available in goose liver, butter and egg yolks.
• Vitamin K1 conversion to Vitamin K2 does occur minimally in our bodies. Plus, this conversion slows down with age.
• Vitamin K2 is rich in Natto, a traditional Japanese food. Natto is a fermented soy condiment and is the richest known food source for Vitamin K2.


• Double-blind, placebo-controlled, randomized trial enrolling 1708 patients aged 50 years or older who had experienced a myocardial infarction at least 6 weeks prior and had serum creatinine levels of 2.0 mg/dL or less.
• Patients were randomized to receive 40 infusions of a 500 ml chelation solution (3 g of disodium EDTA, 7 g of ascorbate, B vitamins, electrolytes, procaine, and heparin) (n=839) vs placebo (n=869) and oral vitamin-mineral regimen vs oral placebo. Infusions were administered weekly for 30 weeks, follwed by 10 infusions 2-8 weeks apart.
• The primary end point was a composite of total mortality, recurrent MI, stroke, coronary revascularization, or hospitalization for angina.
JAMA 2013;309(12):1241-1250

JAMA 2013;309(12):1241-1250
End Points Chelation(n=839)
Placebo(n=869)
Hazard Ratio
(95% CI)
P Value
Primary end point 222 (26) 261(30) 0.82 .035
Death 87 (10) 93 (11) 0.93 .64
Myocardial infarction 52 (6) 67 (8) 0.77 .17
Stroke 10 (1) 13 (1) 0.77 .53
Coronary revascularization 130 (15) 157 (18) 0.81 .08
Hospitalization for angina 13 (2) 18 (2) 0.72 .36
About 16% of patients in chelation group and 15% of patients in placebo group were dropped-out; however, sensitivity analyses examining the effect of patient dropout and treatment adherence did not alter the results

JAMA 2013;309(12):1241-1250
Kaplan-Meier estimates of the primary composite end pointThe primary end point was a composite of death from any cause, reinfarction, stroke, coronary revascularization, or hospitalization for angina
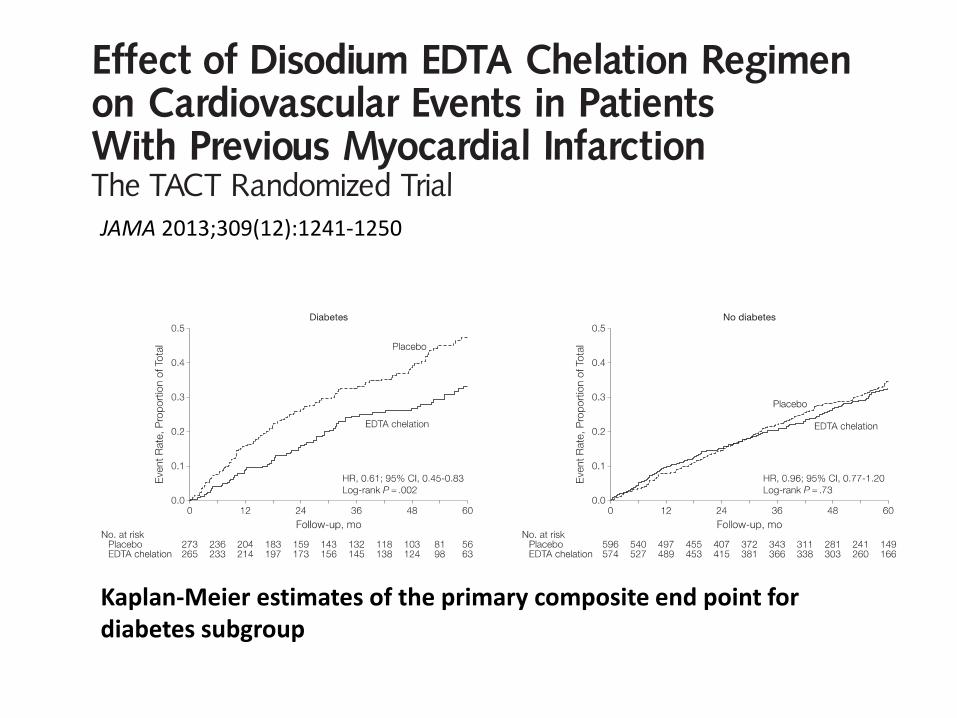
JAMA 2013;309(12):1241-1250
Kaplan-Meier estimates of the primary composite end point for diabetes subgroup
Concept of Diabetic CareGoal of diabetes treatment is not about achieving
fasting plasma glucose
• Lifestyle modification including weight reduction, diet control and increasing physical activity is the mainstay of diabetes treatment.
• Prevent complications.
• Prevent progression.