Embed Size (px)
Citation preview

ONE YEAR FOLLOW UPON HYBRID SYSTEM INSPINAL TUBERCULOSISSURGERY: A CASEREPORTDepartment Orthopaedic and Traumatology
Faculty of Medicine, Universitas Indonesia
Cipto Mangunkusumo Hospital

INTRODUCTION
▪ Spondylitis TB leads to the instability of the spine due to damage tothe corpus and makes neurologic deficit.1,2
▪ New Procedures conventional technique and minimally invansivetechnique (Hybrid System) allows minimal incisions only at the level ofpathologic vertebrae3,4
▪ Aim of study to asses outcomes of minimally invansive technique inthe surgical treatment of spondylitis TB
1. Kandwal P, Garg B, Upendra B, Jayaswal A. Outcome of minimally invansive surgery in the management of tuberculousspondylitis. Indian J Orthop. 2012;46:159-64.
2. Rigotti S, et al. Minimally invansive posterior stabilization for treating spinal tuberculosis. J Orthopaed Traumatol. 2013;14:143-5.3. Hanaoka N, Kawasaki Y, Sakai T, Nakamura T, Nanamori K, Nakamura E, Uchida K, Yamada H. Percutaneous drainage and
continuous irrigation in patients with severe pyogenic spondylitis, abscess formation, and marked bone destruction. JNeurosurg Spine. 2006;4: 374-9.
4. Ito M, Sudo H, Abumi K, Kotani Y, Takahata M, Fujita M, Minami A. Minimally invasive surgical treatment for tuberculousspondylodiscitis. Minim Invasive Neurosurg.2009; 52: 250–253.

METHODS
▪ A female, 26 yo, with diagnosis spondylitis TB at the level Th12-L1 and L4-L5
▪ Indication of surgery were back pain + neurologic deficit and progressiveparaspinal abscess
▪ Treated by posterior spine stabilization with mini open posterolateraldebridement + fusion + percutaneous abscess drainage
▪ Evaluated : blood loss, duration of surgery, length of stay, Visual AnalogueScale (VAS) scores, fusion status, neurological state and Oswetry DisabilityIndex (ODI)
CASE ILLUSTRATION
▪ Chief complain : back pain radiating to the right hip since 6 months ago
▪ History of tuberculosis, currently on anti tuberculosis regimens at the 4 th
months

PHYSICAL EXAMINATION▪ Tenderness on Th12-L1(VAS 7-8)
▪ No gibbus or sinus
▪ Hypesthesia at right L1 dermatome
▪ Abscess paraspinal
▪ No motoric disturbance

X RAY
- Erosion on Th12-L1spinal body
- Discal narrowing
- Lytic lesion,inferior-anterior of L4
- Fusiformic shadow at rightparavertebral Th7-S2

MRI

STABILIZATION▪ Posterior stabilization
approach
▪ 1 cm incision on 8 places
▪ 8 pedicle screws, size55-40 (Th11-12) and 65-40(L2-3)
▪ 2 Rods, 90 cm length
▪ C-Arm guided
▪ ILLICO MIS (Scientix)
ABSCESS DRAINAGE
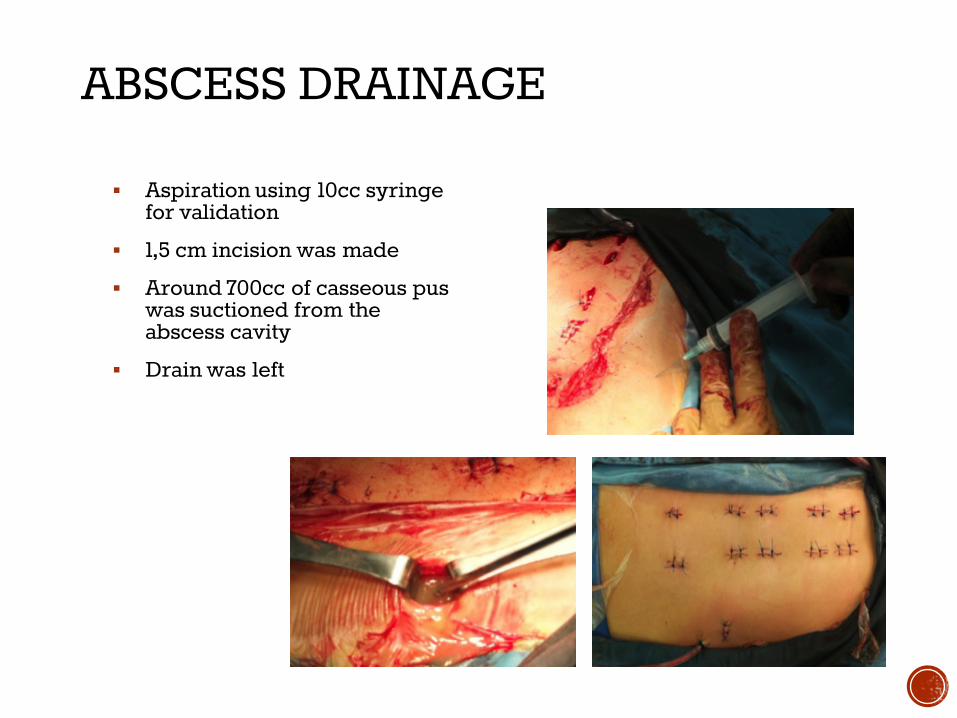
▪ Aspiration using 10cc syringefor validation
▪ 1,5 cm incision was made
▪ Around 700cc of casseous puswas suctioned from theabscess cavity
▪ Drain was left

POST OPERATIVE
▪ Drain was released at the3rd day (total drainproduction was 100cc)
▪ At the 5th day patient wasdischarged. At the day,VAS was 3-4 (from 7-8), andpatient can walk normally
▪ Anti-tuberculosis regimenwas continued 8 monthsafter the surgery (total was12 months of regimen)

FOLLOW UP
▪ One year follow up

RESULT

DISCUSSION▪ Minimal invasive surgery has been providing an alternative that may
decrease the morbidity caused by open surgeries1,2
▪ Intraoperative blood loss was 150cc. This is less than blood loss fromposterior stabilization, which range from 200-800cc. Shorter length stay(10 days to 5 days) `1
▪ On follow up, good fusion was achieved. VAS and ODI score wereimproved in 6 moths and better in 12 months→ clinically patient becamebetter
▪ This case report had same result as Rigotti et al: in overall, minimallyinvasive spine surgery produced a good outcome for spondylitis tb cases2
1. Kandwal P, Garg B, Upendra B, Jayaswal A. Outcome of minimally invansive surgery in themanagement of tuberculous spondylitis. Indian J Orthop. 2012;46:159-64.
2. Rigotti S, et al. Minimally invansive posterior stabilization for treating spinal tuberculosis. JOrthopaed Traumatol. 2013;14:143-5
CONCLUSION
▪ Clinical results of Hybrid System in case of Spondylitis TB aresimilar to conventional open surgery procedure.
▪ Hybrid System is proved to be more effective in reducing :▪ Bleeding
▪ Soft tissue damage
▪ Recovery time





