Embed Size (px)
Citation preview

PARTNERSHIP HEALTHPLAN OF CALIFORNIA PHYSICIAN ADVISORY COMMITTEE ~ MEETING NOTICE
Members: Jeffrey Bosworth, M.D. Shandi Fuller, M.D. *alternates Jeffrey Gaborko, M.D. (Chair) Michael Ginsberg, M.D. David Gorchoff, M.D.
Steve Gwiazdowski, M.D. excused Michele Herman, M.D. Willard Hunter, M.D. Melissa Marshall, M.D. Mills Matheson, M.D.
Danielle Oryn, D.O. Thomas Paukert, M.D. Mitesh Popat, M.D. Michael Stacey, M.D. *alternates Lisa Ward, M.D.
PHC Staff: Liz Gibboney, Chief Executive Officer –not available Robert Moore, MD, MPH, Chief Medical Officer Wendi West, Northern Executive Director Peggy Hoover, RN, Senior Director, Health Services Patti McFarland, Chief Financial Officer Mary Kerlin, Senior Dir., Provider Relations (PR) Dept. Marshall Kubota, MD, Regional Medical Director Mark Netherda, MD, Assoc. Medical Director of Quality Jeffrey Ribordy, MD, Regional Medical Director Colleen Townsend, MD, Regional Medical Director Stan Leung, Pharm.D., Director, Pharmacy Services Erika Robinson, Director, Quality & Performance Improvement Debra McAllister, RN, Dir. of Utilization Mgmt. (UM) Michael Vovakes, MD, Northern Regional Medical Director
Ad Hoc PHC Sonja Bjork, Chief Operating Officer Kevin Spencer, Director of Member Services Members: Kirt Kemp, Chief Information Officer James Cotter, MD, Associate Medical Director
Lynn Scuri, Regional Director Bettina Spiller, MD, Associate Medical Director Jennifer Chancellor, Northern Regional Manager Mark Glickstein, MD, Associate Medical Director Nancy Steffen, Assoc. Dir. of Quality Improvement (N) David Katz, MD, Associate Medical Director Sharon Hoffman-Spector, RN, N. UM Manager Ledra Guillory, Senior Prov. Relations Rep. Manager Rebecca Boyd Anderson, RN, Director, Care Coord. Margarita Garcia-Hernandez, Manager, Health Analytics Margaret Kisliuk, Behavioral Health Administrator John Hunsaker, Manager, Quality Incentive Programs Sandra McMasters, Senior Health Educator Vic Patel, Pharm.D., Senior Clinical Pharmacist Diane Wong, Pharm.D., Senior Clinical Pharmacist Rachael French, Sr. Mgr. of Quality Compliance & Accreditation
cc: PHC Commission Chair Harris Levin, MD Gabriel Samuel Chua, MD Kali Stanger, MD Voltaire Velarde, MD Richard Fogg Jerry Douglas, MD Amy Brom, Psy.D Karen Relucio, MD David Danzeisen, MD Matthew Symkowick, MD Jeremy Austin, MD
FROM: Linda Largent DATE: March 6, 2019
SUBJECT: PHYSICIAN ADVISORY COMMITTEE MEETING
The Physician Advisory Committee will meet as follows and will continue to meet the second Wednesday of every month (exception / July and December.) Please review the Meeting Agenda and attached packet, as discussion time is limited.
DATE: Wednesday, March 13, 2019 TIME: 7:30 a.m. – 9:00 a.m.
LOCATIONS:
________Via Video Conference________ ____________________________Access Via Teleconference____________________________
Partnership HealthPlan of CA 4665 Business Center Drive (Please Park in Front of Bldg.) Fairfield, CA
PHC – Sonoma Office 495 Tesconi Circle Santa Rosa
Baechtel Creek Medical 1245 S. Main Street Willits
Marin Community Clinic 9 Commercial Blvd., Suite100 Novato
CommuniCare Health 2051 John Jones Road Davis
PHC - Eureka Office 1036 5th Street, Suite E Eureka
PHC – Redding Office 2525 Airpark Drive Redding
Redwood Community Health Coalition 1310 Redwood Way, #135 Petaluma
Napa Valley Nephrology 3443 Villa Lane, Suite 6 Napa
Please contact me at (707) 863-4228, or e-mail [email protected] if you are unable to attend.

Blank Page
2 of 86

Page 1 of 2
REGULAR MEETING OF PARTNERSHIP HEALTHPLAN OF CALIFORNIA’S PHYSICIAN ADVISORY COMMITTEE - MEETING AGENDA
Date: March 13, 2019 Time: 7:30 – 9:00 a.m. Location: PHC
PUBLIC COMMENTS Speaker 2 minutes
Speaker 2 minutes
This Brown Act meeting may be recorded. Any audio or video tape record of this meeting, made by or at the direction of PHC, is subject to inspection under the Public Records Act and will be provided without charge, if requested.
Welcome / Introductions I. Approval of Minutes – Chair 5 – 14 7:30 II. Standing Agenda Items Lead Pg # Time
A. Status Update Administration
Medical / Health Services Report Regional Medical Director Reports
- Napa & Southeast Counties- Southwest Counties- Northwest Counties- Northeast Counties
Ms. Bjork on behalf of Ms. Gibboney
Dr. Townsend for Dr. Moore
Dr. Townsend Dr. Kubota Dr. Ribordy Dr. Vovakes
7:40
7:50
7:55 7:58 8:01 8:04
A1. Update from County Public Health Departments Available Representative(s)
8:07
A2. Committee Member Highlight Dr. Gorchoff 8:10
B. Quality / Utilization Advisory Committee (Q/UAC) Activities Report with attachments – Consent Review Activities & Minutes of the February 20, 2019 meeting: - Minutes – Internal Quality Improvement meeting 01/08/19
* Policies & Procedures: * Summary - See Pages 33 - 34
Note – only pages with significant changes are included for policies
- Quality Improvement Update – February - Grievance & Appeals Report - Physical Accessibility Review Survey (PARS) Report - Initial Health Assessment (IHA) Outreach Pilot - HEDIS Improvement (previously presented to PAC)
Dr. Townsend for Dr. Moore
15 - 59 8:20
C. Pharmacy &Therapeutics (P&T) Committee / Consent Review No meeting February
Dr. Leung / Dr. Moore
N/A --
D. Provider Advisory Group (PAG) Report – Consent Review Minutes of the February 15, 2019 meeting (Deferred to April PAC meeting)
Ms. Kerlin N/A --
E. Credentialing Committee Meeting Summary – Committee approved Summary of the January 9, 2019 meeting, (attached)
Dr. Kubota 60 - 70 8:21
F. Recommended Committee Appointments / Resignations
Physician Advisory Committee – Appointment - Matthew Symkowick, MD, Kaiser Permanente
Dr. Townsend for Dr. Moore
71 8:22
III. Old Business Lead Pg # Time
IV. New Business
A. Physician Advisory Committee policy (MPQP1003) Action Required Dr. Townsend 72 – 74
8:23
B. Hospital Quality Improvement Program 2019/2020 – Action Required Ms. Lasher 75 - 85 8:25
C. HEDIS Best Practice Highlight Dr. Marshall / Dr. Townsend
86 8:45
D. Additional Business:
VI. Adjournment 8:55
This agenda contains a brief description of each item to be considered. Except as provided by law, no action shall be taken on any item not appearing on the agenda.
Continued

Page 2 of 2
Government Code §54957.5 requires that public records related to items on the open session agenda for a regular committee meeting be made available for public inspection. Records distributed less than 72 hours prior to the meeting are available for public inspection at the same time they are distributed to all members, or a majority of the members of the committee. The committee has designated the Administrative Assistant to the Chief Medical Officer as the contact for Partnership HealthPlan of California located at 4665 Business Center Drive, Fairfield, CA 94534, for the purpose of making those public records available for inspection. The Physician Advisory Committee Agenda and supporting documentation is available for review from 8:00 AM to 5:00 PM, Monday through Friday at all PHC regional offices (see locations under the Meeting Notice). It can also be found online at www.partnershiphp.org. In compliance with the Americans with Disabilities Act, PHC meeting rooms are accessible to people with disabilities. Individuals who need special assistance or a disability-related modification or accommodation (including auxiliary aids or services) to participate in this meeting, or who have a disability and wish to request an alternative format for the agenda, meeting notice, agenda packet or other writings that may be distributed at the meeting, should contact the Administrative Assistant to the Chief Medical Officer at least two (2) working days before the meeting at (707) 863-4228 or by email at [email protected]. Notification in advance of the meeting will enable PHC to make reasonable arrangements to ensure accessibility to this meeting and to materials related to it.
Meeting Notes – Physician Advisory Committee – 03/13/2019
Action Items Assigned To:
1.
2.
3.
4.
5.
6.
7.

PARTNERSHIP HEALTHPLAN OF CALIFORNIA MEETING MINUTES
PAGE 1 OF 11 Committee: Physician Advisory Committee Date / Time: February 13, 2019 - 7:35 to 8:59 am
Members Present:
Jeffrey Bosworth, MD - TC Jeffrey Gaborko, MD (Chair) Michael Ginsberg, MD
David Gorchoff, MD - VC Steven Gwiazdowski, MD Michele Herman, MD
Willard Hunter, MD – VC Melissa Marshall, MD - TC Mills Matheson, MD – TC
Danielle Oryn, DO – TC Mitesh Popat, MD - TC Lisa Ward, MD - VC
Members Excused:
Shandi Fuller, MD
Members Absent:
Thomas Paukert, MD
Michael Stacey, MD
Visitors: Matthew Symkowick, MD Coleen Fong, Gilead Sciences Stacey Bannach, Gilead Sciences
Note: via Video Conf. (VC) via Teleconference (TC)
PHC Staff Present:
Patti McFarland, Chief Financial Officer Lynn Scuri, Regional Director - VC Margaret Kisliuk, Behavioral Health Admin. Ledra Guillory, Sr. Prov. Relations Rep. Mgr.
Robert Moore, MD, Chief Medical Officer Peggy Hoover, RN, Senior Director, Health Services Colleen Townsend, MD, Regional Medical Director Mark Netherda, MD, Assoc. Med. Dir., Quality - VC Stan Leung, Pharm.D., Director, Pharmacy Services
Marshall Kubota, MD, Regional Medical Director - VC Michael Vovakes, MD, Northern Regional Med. Dir. -TC Jeffrey Ribordy, MD, Regional Medical Director - VC Erika Robinson, Director, Quality & Perf. Improvement
AGENDA
ITEM DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION TARGET
DATE DATE
RESOLVED
Public Comments Quorum I. Approval of Minutes II.A. Status Update Administration
Committee Chairman, Dr. Gaborko, asked for public comments. The two representatives of Gilead Sciences introduced themselves. The Committee’s Chair presented the meeting minutes from January, 2019 for approval. The HealthPlan’s Chief Medical Officer (CMO), provided the following report on Partnership’s activities on behalf of the Plan’s Chief Operating Officer (COO). Due to significant weather issues in the North (snow and power), the COO was unable to attend the Committee meeting. Because of the challenges in the Northern Region, the COO activated the Plan’s Emergency Response Team. - Future Health Workforce Commission – Recently, the State’s
Commission issued their final report. A number of recommendations were included, which came down to three strategies:
N/A Committee quorum requirements met. MOTION: Dr. Herman moved to approve Agenda Item [I.] as presented, seconded by Dr. Gwiazdowski. ACTION SUMMARY: [12] yes, [0] no, [0] abstentions. Motion carried. For information only, no formal action required.
N/A
02/13/19
02/13/19
5 of 86

Physician Advisory Committee Minutes – 02/13/19 - Page 2 of 11
AGENDA ITEM
DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION
DATE RESOLVED
II.A. Status Update Admin., Continued II.A. Status Update Medical
Increase opportunities for Californians to advance in health professions Align and expand education and training to prepare health workers to meet California’s future health
needs Strengthen the capacity, effectiveness, wellbeing, and retention of the health work force
There were ten major, and seventeen minor recommendations, which is worthwhile reading for those interested in training health professionals. It is hoped that the State’s Legislature will use this document as a blueprint for legislative priorities.
- Strategic Planning Retreat – This year’s annual Board retreat will be held on February 27. The speakers will
include a senior staff member of the Assembly Health Committee, the Deputy Cabinet Secretary, and an expert with the Health Information Exchange. Space availability can be checked for any Committee member interested in attending.
- Whole Child Model (WCM) / California Children Services (CCS) Transition – The shift of services is for a large portion of the approval process for CCS into the WCM, which has gone fairly smoothly. Staff is closely monitoring the costs under existing pharmacy prescriptions, due to the unexpected high cost medications included, and funding from the State that may not be sufficient to cover those expenses.
- Health Homes (HH) Program – The State formally accepted the proposal that the HealthPlan and the Central California Alliance for Health not implement the HH Program. Other counties are still targeted to go live in July 2019. An analysis of the State’s program showed that the regulations were laborious (which would be passed down to provider sites), inadequate funding and no sustainability of funding, and the patient selection that would not save funds, as intended by the State. To undertake the State’s inferior program, PHC would be dismantling its robust Intensive Outpatient Care Management (IOPCM) model. That model was being moved toward Health Homes, but, with this decision, proposals are being developed that would shift it back to its original structure of cost savings for high cost patients (IOPCM version 3). This will be presented to the Plan’s executive team for consideration.
The HealthPlan’s CMO presented an overview of some Health Services activities. - Managing Patients with Persistent Medications Measurement – Along with the National Committee for
Quality Assurance (NCQA), the State is removing this measurement from its list of Healthcare Effectiveness Data and Information Set (HEDIS) requirements, which Medicaid plans are responsible for. The HealthPlan will continue to collect data for 2018, but, reporting of this measure will not be required for 2019. The ten points associated with that measure under the Primary Care Provider (PCP) Quality Improvement Program (QIP) will be redistributed into four other measures that are challenging for the Plan. Details are in the process of being posted, and quality teams at provider sites have been informed of the change.
- Prenatal Care – Areas of opportunity in quality improvement have been identified. Under the Plan’s current mechanism, initial site visits are conducted for primary care practice (PCP) sites when first credentialed.
For information only, no formal action required. For information only, no formal action required. For information only, no formal action required. For information only, no formal action required.
02/13/19
02/13/19
02/13/19
02/13/19
6 of 86

Physician Advisory Committee Minutes – 02/13/19 - Page 3 of 11
AGENDA ITEM
DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION
TARGET DATE
DATE RESOLVED
II.A. Status Update Medical, Continued
After consideration, the same review process used for primary care will be started for prenatal care sites, beginning in July, and will be rolled out gradually. These sites will be visited every three years, as with PCP sites. Dr. Ward asked if the site visit for prenatal care will be incorporated into the PCP site visit, or conducted separately. Staff unable to attend the meeting, due to road closures in the North, will be consulted. The Plan’s CMO will answer this question off-line.
- Department of Health Care Services (DHCS) Medical Audit – The Audit was
concluded one week early, and auditors did not address anything significant. There were some recommendations given. One is from the Centers for Medicare & Medicaid Services (CMS), requiring a comprehensive record of every grievance to be presented to the Plan’s Board. Staff is working on instituting this requirement. Other recommendations were primarily technical in nature.
- Physical and Occupational Therapy – These services have historically required a referral, as well as a Treatment Authorization Request (TAR). The referral requirement is being eliminated, though prescriptions will still be required. The referral was an added barrier for members to receiving this service. Staff will continue to monitor utilization through the TAR review process.
- Enhanced Benefits – The HealthPlan has a committee that reviews potential additions to benefits (i.e. knee scooters or drawing blood at home). A prior authorization will be required, but, knee scooters will be authorized under circumstances where the individual cannot use crutches and is facing an extended immobilization. A price limit will also apply.
PHC’s Regional Medical Director for Napa and the Southeast (SE) counties presented a brief overview. There has been great progress in the Southeast working with larger community health centers on improving HEDIS scores. LaClinia and Community Medical Centers (CMC) have agreed to work closely with Plan staff to help them understand how quality improvement (QI) works in their practices, and how PHC can help support those processes toward improving Quality Improvement Program (QIP) and HEDIS scores for them. Yolo County There has been an outbreak in syphilis. The Yolo County Public Health Officer is working hard to implement changes to increase screening and improve treatment.
The Plan’s CMO will follow-up with Dr. Ward regarding her question if the site visits will be conducted simultaneously, or separate. (Post-Meeting Update – The Plan’s CMO confirmed that the primary care and prenatal care site visits would occur simultaneously at sites offering both services.) For information only, no formal action required.
Feb. 2019
02/15/19
02/13/19
7 of 86

Physician Advisory Committee Minutes – 02/13/19 - Page 4 of 11
AGENDA ITEM
DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION
DATE RESOLVED
II.A. Status Update Medical, Continued
Solano County - Three practices have been approved for the ADVANCE Program, which is in addition to other efforts
these sites have implemented to improve capacity around quality improvement (QI) performance. - NorthBay Healthcare is expanding and developing their own integrated behavioral health services,
adding in some warm handoff capabilities, Licensed Clinical Social Workers (LCSWs) within their practices, and psychiatry support for telephonic consultations.
Napa County 1) There is one health center that has applied to participate in the ADVANCE Program. 2) St. Joseph Health System is working intensively on developing a more standardized health system
across their region. This is starting with some cultural changes within the organization to provide team building and connecting frontline workers, caregivers, and facility leaders on identifying their organization’s mission, vision, and values, and taking those concepts through processes around QI within each department. This standardization will be applied to each hospital within the St. Joseph system so that the hospitals (that have functioned independently), will merge into a region of health care. It is expected that this will extend to their other hospital systems.
PHC’s Regional Medical Director for the Southwestern (SW) counties presented a brief overview. - Access – Due to the ongoing weather conditions, it is expected that the Russian River will flood,
impacting some service areas in that region. - California Primary Care Association (CPCA) Quality Conference – Next Thursday, the CPCA will be
holding its day-long conference in Santa Rosa. - Provider Education – There are several webinars coming up for provider staff:
1) March 13 – Webinar on Treating Addiction in the Primary Care Setting, with Dr. David Kan. This will be an informative webinar.
2) April 30 – There is an all-day focus on Addiction Awareness in the Mental Health Setting 3) Date to be determined - Guidelines on Benzodiazepine Prescribing
Dr. Ward shared that approximately 30 staff from Santa Rosa Community Health recently participated in the day-long ABCs of Quality Care training, presented by the HealthPlan and held at the PHC offices in Santa Rosa. It was extremely successful and well received. PHC’s Regional Medical Director for the Northwestern (NW) counties presented a brief overview. - Access – The provider network is currently stable, and there are no real issues to address. - Family Medicine Residency Program – Along with Dr. Hunter, staff is anxious to hear about the Match
next month. The HealthPlan’s Northern Regional Medical Director shared that he has been out of the office the past two weeks, and had nothing specific to share. However, he did receive a morning text. Due to the weather and power problems in Redding, all of the Shasta Community Health Center sites are closed today.
For information only, no formal action required. For information only, no formal action required. For information only, no formal action required.
02/13/19
02/13/19
02/13/19
8 of 86

Physician Advisory Committee Minutes – 02/13/19 - Page 5 of 11
AGENDA ITEM
DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION
DATE RESOLVED
II.A1. – Update County Public Health II.A.2. Committee Member Highlight
The Plan’s Associate Medical Director of Quality noted that, through his work with Sonoma County Public Health, syphilis is a problem in many Bay Area counties. Sonoma County is doing something similar to Yolo County regarding this health issue, which is particularly hitting the homeless population. Providers who see homeless patients should test when and where possible. The Committee’s Chair advised that there have been a couple of women in their Delivery Ward, who had treatment for syphilis during their pregnancy, and their babies required evaluation. Dr. Ward highlighted some of her personal history, noting that the most unusual part for her at an early age was living in Nairobi, Kenya for two and a half years. Her parents moved their young family to Africa’s first democracy, directly following its first Presidency. This was a fairly radical experience for the entire family, who visited the severely depressed areas in Ethiopia, where starvation was very apparent. Dr. Ward’s younger brother was born in Kenya, and received the typical blessing of being spit upon. These and other events created many indelible memories for the family. From Kenya, the family moved to a rural area in the Sacramento region, Rancho Seco. Her father was a veterinarian, specializing in dairy cattle. High school brought her to Fairfield, attending Armijo High and becoming a Candy Striper at NorthBay in the Obstetrics / Gynecology (OB/GYN) surgical area, which was her first exposure to health care. Dr. Ward attended the University of California (UC), Davis, initially aspiring to be a volleyball player, but her height restricted that pursuit. She then majored in Spanish Literature, primarily to discourage any nudging toward medical school, though, she became very involved in the student run health care. At that time, there were two State Propositions: 1) Universal Health Care Access, which failed to pass, and 2) Proposition 186, which limited immigrant social service access, and did pass, but, was then held up in the court system. These events motivated Dr. Ward to become politically active, and worked on the side as a Legislative Aid in a health policy advocacy office. Since that time, she has been involved in health policy. She attended UC, San Francisco for medical school, which had a nickname at the time of “death star”, due to the lack of interest for providing primary care at a large tertiary health care center. Being disillusioned, Dr. Ward left medical school for a public health school at the London School of Hygiene in Tropical Medicines. This was chosen based on her perception of a “real health care system”, where there was universal access, and, where she would be working with others who were influential in making that system happen. Her experiences and education in London were great. Dr. Ward returned to UC, San Francisco for her Family Medicine Residency, and developed a deep interest in women’s health. After residency, she returned to UC, Davis for her Masters of Science in Health Services Research, doing a fair amount of research on health economics and how those principles are in effect when individuals are cycling on and off health insurance. She continued her clinical skills in obstetrics and women’s health, and developed some expertise in chronic disease management in older women. Dr. Ward joined the faculty at UC, San Francisco, running a health policy course for the medical students, along with working on the curriculum for women’s health and OB/GYN for the residents. She thoroughly enjoyed working in the
For information only, no formal action required.
02/13/19
9 of 86

Physician Advisory Committee Minutes – 02/13/19 - Page 6 of 11
AGENDA ITEM
DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION
DATE RESOLVED
II.A.2. Committee Member Highlight, Continued II.B. Quality/ Utiliz. Advisory, II.C. Pharmacy & Therapeutics, and II.E. Credentialing Committees III.A. Discussion Topic Continued from January: HEDIS Improvement: Update of PHC Strategy
department, but, her desire to have children and pay off her student loans dictated her moving from San Francisco. In 2008, she moved to Santa Rosa where she wanted to continue her work in obstetrics, work with Federally Qualified Health Center (FQHC) patient populations, and continue to teach. She joined the faculty at the Family Medicine Residency in Santa Rosa. In 2015, she accepted the position of Chief Medical Officer for the Santa Rosa Health Centers. Last year, she became the President for the California Academy of Family Physicians; her term is almost over. She has continued her work in advocacy in that role, mostly with policies regarding immigration, gun ammunition and control, along with Medicaid / Medi-Cal. Dr. Ward feels privileged to have her work, and taking care of patients, align with her political values on a daily basis. There were no items pulled for additional discussion by the Committee. Partnership’s Chief Medical Officer highlighted some areas addressed at the meeting in January. The HEDIS score diagram reflects Partnership’s score as compared to other similar health plans, scores for Kaiser and PHC counties, followed by Quality Improvement Program (QIP) scores, which roughly correlate to the HEDIS scores. PHC’s Director of Quality and Performance Improvement (Quality Director) shared that staff has found 20% of the Plan’s large volume practice sites are driving 80% to 84% of the performance scores and rates. With that in mind, staff is doing more integrated work, and trying to be very focused and strategic in doing needs assessments, and identifying where Partnership can best partner with these entities to help improve the HealthPlan’s scores. This has been previously done (i.e. ADVANCE and some QI capacity building). Over the past couple years, staff has been aligning the PCP QIP with HEDIS more closely, as they are related. Consequently, staff is being more tactical, and doing more formalized engagements, along with setting some standing initiatives, versus relying on an impromptu approach. Partnership’s leadership will be more engaged with the top eight sites, and staff will be using the same principle when doing initial work with some of the Plan’s larger sites, and drilling down on certain measures to determine where the Plan can be most effective with small and medium sized sites. Capacity building will continue, along with looking at some new quality modalities that can be taught to some of these sites. The Plan’s Quality Director highlighted the meeting format for building relationships with practice site CEOs and other leaders of large health centers, along with the preliminary work staff will do in
For information only, no formal action required. MOTION: Dr. Ginsberg moved to approve Agenda Items [II.B., II.C., & II.E.] as presented, seconded by Dr. Gwiazdowski. ACTION SUMMARY: [12] yes, [0] no, [0] abstentions. Motion carried.
02/13/19
02/13/19
10 of 86

Physician Advisory Committee Minutes – 02/13/19 - Page 7 of 11
AGENDA ITEM
DISCUSSION / CONCLUSIONS
III.A. Discussion Topic Continued from January: HEDIS Improvement: Update of PHC Strategy
preparation of those meetings, which will include the HealthPlan’s senior leadership. Additional work is being done around sharing of best practices. Tools have been developed for more concentrated needs assessments, which are meant to be more strategic and taking into account what is working for the practice site, while building the partnership. Another level of engagement addresses access to data, which involves electronic medical records (EMRs) and health information exchanges (HIEs), requiring work with information technology (IT) staff, as well as working with IT and analytics staff at Partnership. Marketing under the Medi-Cal umbrella is different than for commercial health plans. Staff work toward a consistent message that will be shared with providers and their frontline staff, based upon the Plan’s performance improvement, and what works when strategizing to improve care for members. PHC’s experience with social determinants of health, along with communities that can support the Plan’s work, have filtered into the development of a site under Partnership’s website, allowing the user to access different types of community-based organizations. The processes described are somewhat different than how the HealthPlan addressed some challenges before, and NCQA helped to usher in some of the culture changes. PHC continues to work with sister health plans, and taking advantage of lessons and best practices they developed through processes they underwent. The role of public reporting cannot be dismissed, as there is a level of pride when accomplishments are recognized, and can serve as another level of encouragement. The Plan’s CMO advised that staff have been gathering what is determined to be keys of success at some practice sites. The first case study was compiled from input from Marin Community Clinic (MCC). Similar studies will be included in future meeting material for the Committee. The overall focus for MCC was to engage leaders, personally tracking quality outcomes, and infrastructure. This involves different processes. It was noted that one leading indicator for a site doing well on quality is when the CEO knows the performance statistics for its organization, without referring to material. This knowledge reflects the CEO’s engagement in the process. IT optimization is a key component with successful outcomes. Setting up the electronic health record (EHR) to make it easy to do the function needed is an important piece. And, medical assistants (MAs) play a significant role in optimizing provider services, by doing tasks for the clinician and ensuring his/her time with patients captures needed tests or screens. They also perform outreach to patients who are due for visits. MCC also provides a culture of quality by scheduling monthly one hour meetings with providers and MAs to focus on particular quality measures. The time is also used to remind staff how to record properly in EHRs, or what the correct workflow is. Dr. Popat shared that maximizing what the MAs do and building in the workflows at the practice are key. His approach is to not focus on whether MCC’s providers are doing the right thing, as much as taking the excess off of providers who are already feeling there is too much to do within a short visit. The systems need to be built around them. In addition to the MAs’ participation, MCC’s call center is also engaged and make outreach calls, which allows these staff to feel connected to the broader mission. PHC’s CMO asked if there were MCC providers reluctant to give up their control over some of the quality metrics, not wanting the MAs to do those tasks. Dr. Popat advised that there have been challenges getting some providers to let go, and there are those who really struggle with the change. Monitoring the data helps to identify the providers who need help with letting go, and efforts are underway to recognize areas of opportunity sooner. This is a shift for many of them in how some things were previously done. MCC also conducts “refreshers” with providers, to remind them why processes have been put into place. Publishing the data regularly also provides transparency, and encourages them to determine why their scores may not be as good as a colleague’s. The Plan’s Associate Medical Director offered his experience with getting MAs involved when he was in practice. Using community health assessment slides, MAs could readily see the health of the community (i.e. smoking, obesity), which made it real for them, and justified why tests were given to patients..
11 of 86

Physician Advisory Committee Minutes – 02/13/19 - Page 8 of 11
AGENDA ITEM
DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION
DATE RESOLVED
III.A. Discussion Topic Continued from January: HEDIS Improvement: Update of PHC Strategy IV.A. Quality & Performance Improvement Program Description
The Committee’s Chair noted that Kaiser Permanente also utilizes MAs and receptionists, who learn to understand the importance of tests given to patients. The physician who has high scores reflects a team that has high scores, and utilizing electronic tools for reminders helps to keep them on track. The Plan’s CMO asked if there was some sense as to why Kaiser’s scores in the Sacramento area differ from this region. Dr. Symkowick shared that Sacramento was the origin for a targeted program toward Medi-Cal patients called Geographic Managed Care. Theirs is a more robust outreach around first contact, scheduling the first physical, as well as ongoing case management for patients that are high utilizing or have higher needs than average patients. That program has been expanded in various forms in some of the other service areas, but, not as robust as the initial program. Napa and Solano counties are tied with San Leandro’s service area. The Committee’s Chair acknowledged that Kaiser conducts member outreach for all patients, across all insurance populations. A unique group focused only on Medi-Cal patients with their outreach, which included the entire family. It is much more robust than what was done previously, and progress is being made. Of note, staff in Sacramento are also using innovated methods of contacting members who are difficult to reach, ensuring visits encompass all the patient’s needs, along with getting patients out of the emergency room and into their primary care’s office. In summary, Kaiser focuses on the population, along with organizational activities. Dr. Hunter noted that his region typically has very low scores. His perception is that staff have engaged a lot. But, he has noticed a couple of Open Door Community Health sites that scored high on all measures. Those sites are in areas of high affluence, low homelessness rates, better housing, in a more cohesive community. He is wondering if there has been any progress in comparing populations. Dr. Popat acknowledged that Marin County has the best health scores in the state, but there are also the largest health disparities within the county. The progress has been slow, but steady, and the clinic struggled a bit after the Affordable Care Act (ACA). An important factor is having a sufficient workforce, the minimum amount of provider staffing who can do the work. That should be in place before the outreach (or in-reach) is done, as there needs to be spaces to place patients for medical visits. The Plan’s CMO noted that the discussion is beneficial. Next month will showcase some of the best practices shared by CommuniCare. Partnership’s Quality Director reviewed the amended language added to the Quality Performance Improvement Program Description, which reflects NCQA recommendations. - Addition of Doctor of Osteopathic Medicine (DO) as a qualifying practitioner under Mental Health Clinical
Oversight - Specific timing of committee meetings included (i.e. second Wednesday of each month, excluding July and
December for this Committee)
For information and discussion only, no formal action required.
02/13/19
12 of 86

Physician Advisory Committee Minutes – 02/13/19 - Page 9 of 11
AGENDA ITEM
DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION
TARGET DATE
DATE RESOLVED
IV.A. Quality & Performance Improvement Program Description, Continued IV.B. Clinical Practice Guidelines (CPG) for the Diagnosis & Management of Asthma IV.C. CPG for Diabetes Mellitus IV.D. Pharmacy & Therapeutics (P&T) Update
- Section added for analytics support, listing the PHC departments involved and the functions supporting the Quality Improvement Program
- The section regarding the substance use benefit and services was updated with language that it will be updated when the Medi-Cal benefit is launched
Dr. Herman asked what the Partnership can do to influence the mental health network in seeing patients with substance issues. One of the barriers experienced by La Clinica is the resistance they are experiencing in getting their patients seen. The Plan’s Behavioral Health (BH) Administrator asked that she be apprised of any difficulties providers are having with getting PHC patients seen, or getting responses from the county. She will follow-up to see how the Plan can help facilitate, and can certainly elevate the issue with the county. Dr. Herman noted that La Clinica is trying to establish a telehealth option, and there is language within the PHC guidelines restricting this service. The BH Administrator requested a copy of the language that Dr. Herman was referring to, so that the language can be reviewed for possible editing. The Plan’s CMO advised that Committee members can also forward any issues they may have to the Regional Medical Director for their area, if they are unsure who the request should be sent to. The Regional Medical Director can determine who best to address the issue. Partnership’s CMO shared that this is the annual update for the Clinical Practice Guidelines (CPG) for the Diagnosis & Management of Asthma, which contains a couple minor changes. The purpose of the guidelines was updated to reflect the current prevalence of the disease. A few changes were also made to include current, new medications that have come to market, in relation to PHC’s Formulary. The Committee’s Chair advised that the CPG for Diabetes Mellitus has been tabled, due to new recommendations that should be reviewed first. The CPG will be returned at a future meeting. The Plan’s Director of Pharmacy presented a high level overview of recommended changes to the formulary by the P&T Committee. A number of medications were added, which include those for seizures, hypertension, and gout. The step edit for Celecoxib and Micronized Progesterone have been removed. A number of medications had formulary changes, making them more accessible for providers and members with over-the-counter (OTC) designation.
MOTION: Dr. Gwiazdowski moved to approve Agenda Item [IV.A.] as presented, seconded by Dr. Herman. ACTION SUMMARY: [12] yes, [0] no, [0] abstentions. Motion carried. Dr. Herman will forward the Plan guidelines she referred to, so that staff can review for possible clarification. MOTION: Dr. Gwiazdowski moved to approve Agenda Item [IV.B.] as presented, seconded by Dr. Herman. ACTION SUMMARY: [12] yes, [0] no, [0] abstentions. Motion carried. CPG for Diabetes Mellitus pulled from agenda – to be reviewed for approval at a future meeting.
February 2019
April 2019
02/13/19
02/13/19
13 of 86

Physician Advisory Committee Minutes – 02/13/19 - Page 10 of 11
AGENDA ITEM
DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION DATE RESOLVED
IV.D. Pharmacy & Therapeutics (P&T) Update, Continued IV.E. Network Availability Standards policy, IV.F. Reporting of PHC Specialist Physician Network Availability Adjournment
Dr. Ginsberg addressed the Ondansatron solution, which keeps coming up as a logistical problem. The emergency room will prescribe it, but, the family has difficulty getting the prescription filled. PHC’s Pharmacy Director confirmed that the prescription is under formulary for patients up to the age of 14 years. The formulary change will take effect March 1. The Plan’s Pharmacy Director noted that there were some changes made to the Hepatitis C medications, due to the introduction of a generic medication (Epclusa) and Zepatier. Following this Committee’s approval, Zepatier will become the preferred regimen for genotypes 1 through 4, and Epclusa will be the preferred for genotypes 2, 3, 5, and 6 on March 1. The criteria or member eligibility for the treatment does not change. It was noted that there is a difference between prescribing a nebulizer from the pharmacy versus a durable medical equipment (DME) supplier. Pharmacies that carry the product are generally less expensive than a DME vendor. Dr. Ginsberg did some literature review in anticipation of the discussion around nebulizers. At least in the acute setting for beta agonists, evidence seems to show that these units are no better than metered dose inhalers (MDIs) when appropriately used with a spacer. He has a lot of parents requesting nebulizers, and his suspicion is that this is due to a lack of education on how to correctly use an inhaler. And, many pulmonologists tend to favor MDIs. Will MDIs still be available when requested? The Plan’s CMO confirmed that MDIs are still covered, and shared that pharmacy staff is aware of the literature highlighted. The HealthPlan needs to ensure that members are able to receive something (nebulizers) from the pharmacy, which does not require a prior authorization. There was further discussion around prescribing MDIs or nebulizers for pediatric patients when bronchiolitis is suspected, along with the challenge in an emergency department setting, where physicians do not see the condition very often. The Plan’s CMO noted that the two policies were under regular annual review, and follow regulatory requirements by the State. They reflect how the HealthPlan evaluates primary care and specialty practice sites, with relation to availability standards. The Committee adjourned at 8:59 AM Respectfully submitted: Linda Largent
For information only, no formal action required. MOTION: Dr. Ginsberg moved to approve Agenda Items [IV.E. and IV.F.] as presented, seconded by Dr. Herman. ACTION SUMMARY: [12] yes, [0] no, [0] abstentions. Motion carried.
02/13/19
Page 11 of 11 for Signature Only
14 of 86

PARTNERSHIP HEALTHPLAN OF CALIFORNIA MEETING MINUTES
Committee: Quality and Utilization Advisory Committee (Q/UAC) Meeting
Date/Time: Wednesday, February 20, 2019 / 7:30 AM – 9:00 AM Napa/Solano Room, 1st Floor
Members Present: Borde, Madhusudan, MD Choudhry, Sara, MD Gwiazdowski, Steven, MD, FAAP Montenegro, Brian, MD Murphy, John, MD
Quon, Robert, MD Stockton, Candy, MD Swales, Chris, MD Thomas, Randolph, MD
Members Absent: Paukert, Thomas, MD Strain, Michael, PHC Consumer Member
Threlfall, Alexander, MD Wilson, Jennifer, MD
PHC Members Present: Banks, La Rae, Associate Director of Grievance and Appeals Becerra, Eric, Grievance and Appeals Resolution Manager Boyd Anderson, Rebecca, RN, Care Coordination Director French, Rachael, Senior Manager, Quality Compliance and Accreditation Glickstein, Mark, MD, Associate Medical Director Guillory, Ledra, Senior Provider Relations Representative Manager Hoover, Peggy, RN, Health Services Senior Director Kubota, Marshall, MD, Regional Medical Director McAllister, Debra, RN, Utilization Management Director
Moore, Robert, MD, MPH, MBA Chief Medical Officer – Chairman Netherda, Mark, MD, Associate Medical Director, Quality Ribordy, Jeff, MD, Northern Region Medical Director Robinson, Erika, Director of Quality and Performance Improvement Scuri, Lynn, Administration Regional Director Townsend, Colleen, MD, Regional Medical Director Vovakes, Michael, MD, Northern Region Medical Director
PHC Members Absent: Cotter, James, MD, Associate Medical Director Fronefield, Carly, RN, Northern Region Health Services Director Katz, Dave, MD, Associate Medical Director
Leung, Stan, PharmD, Pharmacy Services Director Spiller, Bettina, MD, Northern Region Associate Medical Director Steffen, Nancy, Northern Region Associate Director Quality, Analytics and Project Management
Guests: Garnick, Karen, Project Coordinator Hoffman-Spector, Sharon, NR UM Manager Klinger, Ron, Team Manager – Child/Family Unit Nakatani-Phipps, Stephanie, Lead Senior Provider Relations Rep
Patel, Vic, Sr. Clinical Pharmacist Santos, Rose, Manager of Quality Assurance / Patient Safety Speer, Brittany, Market Consultant, Lilly USA LLC Stevenson, Lauri, Manager of Clinical Quality and Patient Safety
AGENDA ITEM DISCUSSION RECOMMENDATIONS /
ACTION DATE
RESOLVED I. Call to Order
Approval of Minutes Dr. Robert Moore called the meeting to order at 7:30 a.m. No public comments were made. Internal Quality Improvement (IQI) Minutes from January 8, 2019 were reviewed and accepted.
Motion for IQI Minute acceptance: Dr. Borde Second for IQI Minute acceptance: Dr. Murphy Motion for QUAC Minute approval:
02/20/19
15 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION
DATE RESOLVED
Quality and Utilization Advisory Committee (Q/UAC) Minutes from January 16, 2019 were reviewed and approved.
Dr. Borde Second for QUAC Minute approval: Dr. Murphy
II. Standing Agenda Items 1. Status of Open
Action Items Dr. Netherda provided an update on questions asked during the presentation of the Potential Quality Issues (PQI) and Provider Reportable Conditions (PPC) report in the January meeting. Question was asked how PHC statistics compare to state averages. Dr. Netherda confirmed that
we don’t have access to that information and that we track internally our year to year changes. In regards to the report of PQIs by county a question was asked if we reach out to facilities to
find out what might be happening. Dr. Netherda advised that we do this for PPCs but not PQIs. We track PQIs by individual provider or facility but not by county. If there are three or more PQIs identified at any facility or provider we have to report that to the state and then we track and trend this information which could result in a more focused review.
For information only, no formal action required.
02/20/19
2. QI Department Update
Erika Robinson gave the Quality Improvement (QI) update found on page 20. We are wrapping up the Quality Improvement Programs (QIPs) 2018 Measurement Year.
Payments and final reports will be distributed in April. The Perinatal QIP Pilot Part 1 is being finalized and a formal evaluation will follow. The Performance Improvement Team led an ABCs of Quality training specifically for Santa
Rosa Community Health Staff in January. Hill Country Community Clinic and Santa Rosa Community Health have each been awarded
funds to establish a Transitions Clinic program at their sites. PHC has learned a sister plan has suspended their texting program due to its “opt-out” approach
in seeking prior consent per the Telephone Consumer Protection Act of 1991. The HEDIS Measure Score Improvement goal team will recommend PHC adopt an “opt-in” approach as a key next step in exploring texting and e-mail as digital member engagement.
PHC will sunset a gift card program with Petaluma Health Center for members who completed the second dose of the HPV vaccine prior to turning 13 as the incentive did not significantly improve performance of the immunization rate.
PHC has completed its first series of monthly conference calls with DHCS to track progress under the formal Corrective Action Plan (CAP) issued last September. Most recently, we met with DHCS in person to provide an update.
The HEDIS annual project has successfully launched and our HEDIS Medical Record project began 2/11/19. The onsite audit was conducted on 2/13/19.
We continue to do outreach and set timeframes for NCQA first survey as well as working with respective departments and teams in preparation for interim survey; deliverables for the interim survey are due at the end of March.
Efforts are underway to launch two new tools for the Patient Safety Team; the eSite Review Tool and a new PQI tool. The eSite Review tool is in user acceptance testing and the testing of the new PQI tool will begin soon.
For information only, no formal action required.
02/20/19
3. HealthPlan Update Dr. Moore provided the HealthPlan update. The National Quality Forum has stated that the Monitoring Patients on Persistent Medications
(MPM) measure will no longer be supported by them, which led to DHCS agreeing to remove the measure for this current measurement year. Within the PCP QIP, the 10 points for the MPM measure will be redistributed equally into four different measures. The updated specifications
For information only, no formal action required.
02/20/19
16 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION
DATE RESOLVED
have been posted on our website. Two-thirds of our DHCS CAPs are on the MPM measure, so these will be now considered done and PHC will focus on the childhood immunization combo-3 measure that remains.
PHC has noticed some quality of care issues related to prenatal care. It’s difficult for PHC to oversee this as the current state requirements are to do an initial review of perinatal sites. Beginning the middle of this year PHC will be looking at the standards of prenatal care with chart review every three years; we will try to coincide these visits with the primary care sites. For sites that are only doing prenatal or OB/GYN care they will have a visit every 3 years.
The DHCS audit was conducted in February. They had some minor suggestions for improvement which we will be following, and we are awaiting the final results from the state.
The California Health Workforce Commission, which our CEO was a member of, issued their final report. They gave a list of recommendations with 10 high priority recommendations in three different areas for the healthcare workforce in California.
PHC will have its Strategic Planning Retreat on February 27. Scott Bain, the Principal Consultant from the Senate Health Committee, and Richard Figueroa, the Deputy Cabinet Secretary, will be in attendance. Additionally, there will be a speaker focusing on the Health Information Exchange.
The state released official notice that PHC and Central California Alliance for Health will not be implementing the Health Homes program. PHC will continue with our Intensive Outpatient Case Management Program (IOPCM). PHC requested this due to the excessive reporting burden for providers, inadequate rates and a focus on a population that we believed would not lead to cost savings. That combination of factors plus the fact that we have a robust IOPCM program led us to want to change direction. PHC will look to make the structure more focused on the original target population which is people at risk of high cost medical care with some other adjustments that will come out over the course of this year.
PHC budgeted a deficit for this year but unfortunately the deficit is larger than expected largely due to an unexpected increase in pharmaceutical costs.
Currently, Native Americans have the opportunity to be designated as special members due to federal law which enables them to be able to go to any tribal health center in the country without needing prior authorization. We will be moving forward in designating Native Americans with a new status which allows them to be assigned for capitation to a primary care provider (PCP) and still meet this requirement. Target implementation will be mid-year, therefore these members will not be counted in this year’s QIP, but will be eligible next year.
Dr. Swales asked where the majority of the Native American members are. Dr. Moore confirmed there is a much larger population in the northern region, but in Yolo county there is Rancheria so there are some Native Americans there as well.
III. Old Business (Committee Members as Applicable) None N/A 02/20/19 IV. New Business (Committee Members as Applicable)Consent Calendar
Quality Improvement: MPQP1006 – Clinical Practice Guidelines MPQP1055 – Provider Preventable Condition (PPC) Reporting Utilization Management/Care Coordination:
Motion to approve: Dr. Gwiazdowski Second: Dr. Borde All consent policies were approved with no changes
02/20/19
17 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION
DATE RESOLVED
MCCP2021 – Women, Infants and Children (WIC) Supplemental Food Program MPUG3112 – Breast Magnetic Resonance Imagining (MRI) Guidelines (to be archived – refer to InterQual Guidelines) MPUP3018 – Health Services Review of Observation Code Billing
1. CGA024 – Medi-Cal Member Grievance System
Eric Becerra reported on CGA024 found on page 45. Eric advised that the majority of the changes are needed for NCQA and incorporates the requirement for a second level grievance. Desktop procedures will be updated and staff will be trained, including the Member Services (MS) department. Section III, removed the Administrative Appeal definition Section III, added the Second Level Grievance definition for NCQA Section VI, Items P and S added Second Level Grievance process for NCQA Section VI, Item H.2 added language around 72 hour timeframe Section VI, Item H.3 removed repetitive language in expedited grievance portion Section VI, Item L updated the grammar in the grievance section Section VII, Item D.2 updated Member Grievance Review Committee language Section VII, Item E.1 updated appeal and extension letter language
Motion to approve: Dr. Gwiazdowski Second: Dr. Quon Approved with no changes
02/20/19
2. MPXG5008 – Clinical Practice Guideline: Pain Management, Chronic Pain Management and Safe Opioid Prescribing
Vic Patel reported on MPXG5008 found on page 62. Vic advised that the changes are primarily to make the policy read more clearly and to ensure references were current. Removed MCUP3049 from Attachments and added it as a Related Policy Updated Attachment A to include the details of CURES recommendations Updated Attachment D to include the details of CURES recommendations Section VI, Item A.3, moved reference to a pain management contract and made it a separate
item Section VI, Item C.2.b.4 and 5 changed to letters c and d; current letter c is now e Section VI, Item C.2.e, added “(90 daily MED)” for clarification Section VII, Items A and E, links for references were updated. Made all other references as
hyperlinks. All references were updated to reflect “Accessibility verified January 26, 2019” Confirmed and updated as needed references/links in all attachments; updated to reflect
“Accessibility verified January 26, 2019” Dr. Stockton commented on Attachment A, Item D.2.d, the last sentence talks about a policy around marijuana which doesn’t seem to apply here. The committee agreed to remove the last sentence. Dr. Stockton commented on Attachment A, Item E.6 that although she understands and supports the concept of 28-day prescriptions, for those patients in remote areas where pharmacies are not local, and they have others prescriptions that are 30-day, this becomes problematic to require multiple trips to the pharmacy. Dr. Stockton asked if this could be phrased more like a suggestion rather than the expectation. Dr. Moore confirmed that this part of the policy is guidelines so they are not required, but are considered best practices.
Motion to approve: Dr. Quon Second: Dr. Borde Approved with change: Attachment A, page 3, Item
D.2.d, remove the sentence that reads “Whatever the policy around marijuana, if it is implemented clinic-wide and regionally, then patients will not be able to switch to a different clinician who would allow continued unsafe dosing”
02/20/19
3. MPXG5009 – Lactation Clinical Practice Guideline
Ron Klinger reported on MPXG5009 found on page 91. Updated to reflect current naming of the Growing Together Program (GTP) Added current reference website for UNICEF Updated verbiage for Jaundice – “it is an important sign” WHO growth charts for breastfed babies rather than WHO growth charts Updated Contraindications
Motion to approve: n/a Second: n/a Policy was not approved; it was pulled from the agenda for further review and updates. Will target to
N/A
18 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION
DATE RESOLVED
Added “of the infant” for Galactosemia Added updated conditions for contraindications for breast feeding To cover all contraindications added “AAP guidelines should be utilized Updated references for medications that may require temporary interruption of breastfeeding
References were updated, removed AM Best website for PPO and added Red Book reference Dr. Gwiazdowski advised that he has several recommendations for this policy. He offered to meet offline to discuss. The committee agreed that it would be best to pull the policy from the agenda and will bring it back next month.
bring the policy back to the committee in March.
4. MCQP1052 – Physical Accessibility Review Survey (PARS) SR Part C
Lauri Stevenson reported on MCQP1052 found on page 102. Lauri advised that most of the changes were grammatical with the exception of adding the delegation language. Section I, added CMP36 as a related policy Section VI, Item E added language to capture the delegation function to Kaiser Section VII, added APL 15-023 as a reference
Motion to approve: Dr. Quon Second: Dr. Gwiazdowski Approved with no changes
02/20/19
5. MPCP2006 – Coordination of Services for Members with Special Health Care Needs (MSHCNs) and Persons with Developmental Disabilities
Rebecca Boyd Anderson reported on MPCP2006 found on page 106. Updated policy for APL 18-023 California Children’s Services Whole Child Model Program
(12/23/2018), which supersedes APL 18-011 Added related policy MCUP3039 Special Case Managed Members Added paragraph on High Risk Infant Follow-Up (HRIF) Services at VI.B.3 Added description of Local Education Agency (LEA) services at VI.B.6 as per request from
State to submit all policies related to LEA. We determined this policy was the best place for further discussion of the topic. LEA wording was previously found in the EPSDT policy MCCP2022 but was removed in 11/2018 during major revisions. Now it will reside in MPCP2006.
Added APL 18-007: Requirements for Coverage of Early and Periodic Screening, Diagnostic, And Treatment Services for Medi-Cal Members under the Age of 21 (03/02/2018) as a reference
Added NCQA PHM 5 Standard as a Reference in VII Dr. Gwiazdowski asked if there was a link in the policy to the list of things that qualify for HRIF. Rebecca advised that a link is not included, but it can be added. Committee agreed to add the link for the HRIF criteria.
Motion to approve: Dr. Gwiazdowski Second: Dr. Borde Approved with change: Section VII References, add a
link to the HRIF criteria
02/20/19
6. MCCP2018 – Advice Nurse Program
Rebecca Boyd Anderson reported on MCCP2018 found on page 111. Section I, added MCUP3044 Urgent Care Services and CMP36 Delegation and Oversight
Monitoring as a Related Policies. Section VI, G.1, updated pediatric triage reference Deleted Section VI, G.2, procedure that stated the advice nurse will notify PCP by fax re: calls
received Updated procedures in Section VI, G to state that information will be sent to PHC instead of
PCP. Updated Section VI, H to include language for delegation oversight:
Vendor will submit samples of quality protocols annually The HS Director and delegated staff will review activity reports from the Advice Nurse
program and will notify vendor of findings monthly.
Motion to approve: Dr. Quon Second: Dr. Gwiazdowski Approved with change: Section VI.A remove the word
“has” in the first sentence. Sentence will read as: “PHC contracts with an Advice Nurse Program to provide after-hours services.”
02/20/19
19 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION
DATE RESOLVED
Frequency of the joint operating meeting with vendor to quarterly instead of every 6 months. Section VII, B, updated pediatric triage reference Dr. Gwiazdowski asked in regards to delegation, are the requirements for the delegated authority included in the policy, or does PHC have some other verbiage globally that covers this. Rachael advised that in the policy we state that we have an agreement in place and that there is an assumption that the agreement will spell out those specific functions, which it does. Dr. Gwiazdowski agreed that what is stated in the policy is sufficient and no changes were needed. Dr. Glickstein commented in Section VI, Item A, the word “has” is not needed now that the tense of the verb has changed. Committee agreed to remove the word “has”.
7. MCUG3019 – Hearing Aid Guidelines
Debbie McAllister reported on MCUG3019 found on page 115. Section VI, B, clarified that a routine authorization is for one hearing aid Section VI, E, relocated and clarified California Children Services (CCS) eligibility wording –
moved up from Section VI, G.1.b Section VI, F.3, updated wording for CCS Section VI, L, new section added to specify batteries and accessories that will be supplied for
cochlear implants up to three times in a rolling 12 month period without prior auth for codes specified
Dr. Quon asked if there was a reason why in Section VI, Item C.1 it specifies an “attending” physician. Dr. Moore advised that we should remove the word “attending”, and leave it as “otolaryngologist or the member’s primary care provider (PCP)” and that this language should be used in Section VI, Item C.2 as well. Committee agreed to both changes. Dr. Swales asked what is done if two hearing aids are needed. Debbie confirmed they would just need an order for two; Dr. Moore added that they just don’t automatically get two and that the policy states the criteria for binaural hearing aids.
Motion to approve: Dr. Quon Second: Dr. Gwiazdowski Approved with changes: Section VI, Item C.1 remove the
words “attending or”. Sentence will read as: “otolaryngologist or the member’s primary care provider (PCP)”
Section VI, Item C.2 will use the same language as C.1 and will read as: “otolaryngologist or the member’s primary care provider (PCP)”
02/20/19
8. MCUP3039 – Special Case Managed Members
Debbie McAllister reported on MCUP3039 found on page 120. Debbie advised that Utilization Management (UM) mirrors the MS guidelines that the state provides about who can be a special member, what qualifies for a special member, what the special member status is for and what it advocates. Section I, added MCCP2024 Whole Child Model for California Children’s Services (CCS) and
CGA024 – Medi-Cal Member Grievance System as related policies Section VI, B, updated description of CCS/WCM special case managed members HP 1 – Added that dialysis may be covered with a TAR HP 2 – Deleted former CCS HP 2 HEALTHCCS1 – deleted and replaced with HealthWCM HP 8 – added exception that members in an inpatient Drug/Rehab facility will be temporarily
placed in HP 8 if the facility is out of the resident county HP 14 – added Potter Valley HP 21 – Changed HIPP to CIP Section VI, E.3, updated policy number to CGA-024 for Medi-Cal Member Grievance System
and wording to say Chief Medical Officer instead of Director
Motion to approve: Dr. Quon Second: Dr. Gwiazdowski Approved with no changes
02/20/19
20 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION
DATE RESOLVED
9. MCUP3103 – Coordination of Care for Members in Foster Care
Debbie McAllister reported on MCUP3103 found on page 129. Section I, added related policies MCUP3039 Special Case Managed Members and MCCP2024
Whole Child Model for California Children’s Services (CCS) Section VI, A.3 added that Foster Care members who are CCS eligible will be assigned to a
medical home In References, section VII, added link for ACWDL 97-02 In References, section VII, added second ACWDL letter 00-22 with a link
Motion to approve: Dr. Quon Second: Dr. Gwiazdowski Approved with no changes
02/20/19
10. MCUP3131 – Genetic Screening and Diagnostics
Dr. Robert Moore reported on MCUP3131 found on page 131. Added codes per OIL 070n-12 to 81243 and 81244 Replaced Attachment B with a new document – Family History Screening Tool Updated per Medi-cal guidelines path molec changes as follows:
Code 81211 for BRCA was deleted. We previously had special “Benefit Comments” about use of Attachment B for this code. We moved those special comments to code 81162.
Code 81162 for BRCA had previously existed in our grid but was updated and revised heavily
The following new codes were all added and refer back to code 81162: 81163- 81167 81216
Two existing codes, 81215 and 81217, were changed to now refer back to 81162 Other new codes added to the grid were:
81171-81174, 81177- 81187, 81188-81190 (CSTB), 81204, 81233, 81234 (DMPK), 81236, 81237, 81239 (DMPK), 81271, 81274, 81284-81286 (FXN), 81289 (FXN), 81305, 81306, 81312, 81320, 81329 (SMN1), 81335, 81336-81337 (SMN1), 81343-81345, 81518
Code 81213 (BRCA) was deleted from the grid Genes deleted:
SMN1 gene was deleted as a qualifier for 81400, 81403, 81405 (but added as its own code per above)
Several genes were deleted as a qualifiers for 81401 CSTB, DMPK, FXN genes were deleted as a qualifiers for 81404 but added as new
codes per above Dr. Stockton commented that on Attachment A, page 2, TAR and/or Billing Requirements, item 2, fourth bullet “Diagnosed at any age with”, the first bullet should be “one or more”, the word “more” is missing. Committee agreed to add the word “more”.
Motion to approve: Dr. Quon Second: Dr. Gwiazdowski Approved with change: Attachment A, page 2, TAR
and/or Billing Requirements, item 2 under the fourth bullet “Diagnosed at any age with”, add the word “more”. Sentence will read as: “One or more close blood relatives with”
02/20/19
11. MCCP2026 – Diabetes Prevention Program (new policy)
Dr. Mark Netherda reported on MCCP2026 found on page 209. Dr. Netherda advised this is a new policy created per state requirement (see APLs 18-020 and 18-008 Revised and CCS NL 16-1218). The program is for individuals who have been identified with pre-diabetes and consists of 22 courses taught by lifestyle coaches. The courses can be in-person, online or a combination of both, and are available in English and Spanish with interpretation services available for other languages. The criteria is very rigorous and we must follow specific guidelines by the CDC. We are coordinating with a vendor to provide this program to members in all of PHC’s service areas.
Motion to approve: Dr. Quon Second: Dr. Borde Approved with no changes
02/20/19
21 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION
DATE RESOLVED
Dr. Swales asked if a larger group like Woodland Healthcare could be trained, or have the coaches come to the clinic for all of their members. Dr. Netherda advised that since this is now a requirement for Medicare it should already be available; it may not be in the clinic but there should be resources available. Dr. Netherda advised that there is training required to become a lifestyle coach/trainer. Dr. Swales asked if Woodland Healthcare could get the training for their group. Dr. Netherda advised the website that is referenced in the policy has information on how someone can become a certified trainer. Dr. Swales asked if they could receive payment if they offered the program in their clinic. Dr. Netherda advised that to receive reimbursement they would need to get signed up with the vendor, who pays the clinic, and PHC pays our vendor. Dr. Moore commented that PHC will be doing an educational campaign as soon as the program is ready; communications will be sent to both members and providers.
V. Presentations 1. Grievance and
Appeals Report La Rae Banks presented the Grievance and Appeals Report. Refer to the report found on page 213 for detailed information. There were 5,887 investigation closed in 2018, which is double from 2017. This includes
grievances, exempts, appeals and state hearings. The increase is due to Final Rule which stated that anytime a member expresses dissatisfaction, PHC is required to investigate it.
Q4 2018 saw an increase in appeals, which triggered an increase in state hearings. We saw the most appeals in the month of October, which is the month that the opioid changes took place.
Medical Transportation Management (MTM) is our transportation vendor and account for 20.86% of the cases in Q4 2018. Overall they do a good job for our members when compared to the total number of rides they provide.
The most common grievances by category are dissatisfaction with MTM, TAR medications, treatment plans and communication.
Q4 2018 saw one complaint for every 1,000 members. The most common exempts by category are MTM customer service, treatment plans, TAR
process and dissatisfactory experience. The most common appeals by category are TAR-opioids, TAR-medications, TAR-diagnostic
testing. There was one state hearing overturned in Q4 2018 for a TAR denial for Jardiance. Q4 2018 saw 0.286 appeals for every 1,000 members. New Reporting Interest (RI) Categories, or identifiers, have been established to support DHCS
and NCQA reporting, as well as internal reporting. The new RI Categories, effective 12/1/18, are RI-TAR, RI-Transportation, RI-RAF, RI-Beacon/Kaiser/VSP, RI-Related to BHT, RI-Related to CCS.
Operational improvements include transformed audit practice that include a new access database and new reporting to evaluate individual and supervisor audit performance.
Dr. Montenegro asked about the number of discrimination grievances; they are the 3rd most common, and asked if PHC knows why. La Rae advised that this is what the members are reporting, so we need to capture them, but about 97% of the time they are determined not to fall under discrimination. PHC had less than 10 in 2018 that were justified as discrimination.
For information only, no formal action required.
02/20/19
22 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION
DATE RESOLVED
2. Physical Accessibility Review Survey (PARS) Report
Lauri Stevenson presented the PARS Report. Refer to the report found on page 235 for detailed information. The purpose of the PARS is to assess the physical accessibility of provider sites using a set of
standards approved by DHCS. Results from the PARS will be made available through the PHC website and provider directories.
There are two levels upon which a provider’s site will be identified as, basic and limited access, in addition to medical equipment access. Basic access demonstrates that the facility met all 29 critical elements and limited access demonstrates that the facility is missing or is incomplete in one or more areas. Medical Equipment Access are two pieces of equipment, one is a height adjustable exam table; the other is a scale that will accommodate a wheelchair or scooter
Please refer to the report for statistics related to the surveys conducted during the reporting period of 7/1/18 to 12/31/18.
For information only, no formal action required.
02/20/19
3. Initial Health Assessment (IHA) Outreach Pilot
Lauri Stevenson presented the IHA Outreach Pilot update. Refer to the update found on page 237 for detailed information. The IHA is required by the state and this outreach pilot is just one of several projects in place to
improve compliance rates. During Facility Site Reviews and IHA training, sites were educated on documentation of
outreach attempts and how they could be compliant in the IHA measure by documenting three outreach attempts, even if the member was not seen in the clinic. A template was provided that sites could use to manually track the three attempts made to reach the member.
The pilot began last spring; there were 83 sites included and PHC received documentation from 30. Feedback from sites indicate it is too manual of a process and difficult to do. This year we will continue to educate the sites and plan to have more frequent contact with the sites and collect data and feedback quarterly.
For information only, no formal action required.
02/20/19
4. HEDIS Improvement: Update of PHC Strategy (continued from January’s presentation)
Dr. Moore and Erika Robinson continued the presentation of the HEDIS Improvement Update. Refer to the presentation found on page 238 for detailed information. This was a continuation from January’s presentation and they began on page 250. We have been working with our leadership team to be more tactical in our approach with
HEDIS. There were some items identified based upon the first few years of doing the better together strategy, and the work that’s been conducted in both regions.
We developed an initiative repository, which is a very robust database, which we log activities that have taken place and includes lessons learned, if initiatives should continue or not, or if they should be reevaluated to determine if they should be modified to be more effective.
We are working to have greater provider engagement and accountability. We have done several things where we are teaching courses but have realized we have greater opportunity, to actually sit down with individual providers with gap lists and help direct them and make sure we are monitoring and making sure there is greater communication about how to actually achieve and close certain gaps. We continue to look to find more creative and different ways to partner with providers and help hold each other accountable to close their gaps.
The presentation includes examples of four interventions that had positive impact, and one that showed no benefit. Refer to page 252 for the details of each intervention.
We pulled together information our annual HEDIS audit and our QIP scores. Refer to the diagram on page 254 that shows a regional comparison between the HEDIS 2017 and the QIP 2017 scores.
For information only, no formal action required.
02/20/19
23 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION
DATE RESOLVED
Dr. Murphy commented that he appreciates all the efforts that have gone into improving HEDIS performance and from a provider perspective he believes what would most helpful to receive from the HealthPlan is data. Providers are not able to get into eReports until March or April, which puts three measures at risk – Adolescent Immunization, Childhood Immunization Combo-3 (CIS) and Asthma Medication Ratio (AMR). Although special reports are available, someone would need to have special knowledge to ask for a special report. Dr. Moore advised that we piloted a report for the CIS measure and although we have this great system, we aren’t able to have two years overlapping. We do need to take the measures where the beginning of the year is important and institutionalize generating the data. Dr. Moore and Erika will take that back to the Partnership Quality Dashboard (PQD) team. Dr. Quon asked if we are reaching out in a proactive manner to determine what data is needed. At Kaiser they are beginning to meet proactively for things that they know will happen annually. Dr. Moore commented we want to support the providers in our regions and it may be worth having a separate offline meeting to brainstorm and figure out what data we can give you and how can we support you. Dr. Moore advised we would continue with the presentation and discussion in the March meeting. Rachael welcomed the committee to email either her or Karen Garnick any additional comments they may have between now and the next meeting.
VI. Additional Business None
N/A
Respectfully submitted by: Karen Garnick, Project Coordinator Signature of Approval: ________________________________________________ Date: ____________________________ Robert Moore, MD, MPH, MBA Chairman
24 of 86
PARTNERSHIP HEALTHPLAN OF CALIFORNIA MEETING MINUTES
Committee: Internal Quality Improvement (IQI) Meeting
Date/Time: Tuesday, January 8, 2019 / 1:30 PM – 3:30 PM Board Room, 3rd Floor Members Present: Banks, La Rae, Associate Director of Grievance and Appeals Frederickson, Paula, Senior Claims Director French, Rachael, Senior Manager Quality Compliance and Accreditation Gibboney, Elizabeth, MA, Chief Executive Officer Hoover, Peggy, RN, Senior Director, Health Services Kerlin, Mary, Senior Director of Provider Relations Kubota, Marshall, MD, Regional Medical Director
Leung, Stan, PharmD, Pharmacy Services Director Moore, Robert, MD, Chief Medical Officer (CMO) McMasters, Sandra, Senior Health Educator Netherda, Mark, MD, Associate Medical Director, Quality Robinson, Erika, Director of Quality and Performance Improvement Scuri, Lynn, Regional Director Steffen, Nancy, Northern Region Associate Director of Quality Improvement Wurden, Meredith, Associate Director of Financial Policy
Guests: Campbell, Anna, Administrative Assistant II Fries, Bonnie, Senior Provider Education Specialist Garnick, Karen, Project Coordinator Hightower, Tony, Associate Director, Pharmacy Operations Hoffman-Spector, Sharon, Team Manager, UM Leslie, Liz, Program Manager, Wellness and Recovery
Millis, Wendy, Project Coordinator Rad, Rose, Supervisor of Credentialing Santos, Rose, Manager of Quality Assurance and Patient Safety Spencer, Kevin, Director of Member Services Thomas, Andrea, QI Communications Coordinator
Members Absent: Becerra, Eric, Grievance and Appeals Resolution Manager Bjork, Sonja, JD, Chief Operating Officer Boyd Anderson, Rebecca, RN, Director of Care Coordination Chancellor, Jennifer, Northern Region Administration, Regional Manager
Fronefield, Carly, RN, Northern Region Health Services Director McAllister, Debra, RN, Director of Utilization Management Turnipseed, Amy, Senior Director of External and Regulatory Affairs Villasenor, Edna, Associate Director of Call Center
AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION DATE
RESOLVED I. Call to Order
Approval of Minutes Dr. Robert Moore called the meeting to order at 1:30 p.m. Minutes from the November 13, 2018 IQI meeting were reviewed and approved.
Motion to Approve: Paula Frederickson Second: Erika Robinson
01/08/2019
II. Standing Agenda Items 1. Status of Open Action
Items None N/A
2. QI Department Update Erika Robinson and Nancy Steffen gave the Quality Improvement update. Refer to the update found on page 10 for detailed information. Interested primary care provider (PCP) sites were given lists of members who will turn
two in early 2019 and whose vaccinations need to be managed in order to be compliant with the Childhood Immunization measure. Providers can use these lists to proactively schedule visits to support measure compliance in 2019.
PHC is in process of closing out the 2018 Quality Improvement Program (QIP) measurement year; we will launch 2019 in early March. Providers will have visibility to gap lists and overall progress in eReports.
Quality Improvement (QI) department staff are being trained on the utilization of the Partnership Quality Dashboard (PQD). The patient safety team, the Performance Improvement team and Medical Directors have received training with more trainings to be scheduled.
N/A 01/08/2019
25 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION DATE RESOLVED
In December, the Improvement Advisors delivered an internal training on Quality Improvement methodologies to support grand analysis activity related to NCQA accreditation. The goal owners (seven directors) and project leads from five internal teams attended the two-day training.
The Birthday Club pilot intervention has been expanded into the NW region. This targets increased well-child visit rates for 3-6 year olds.
The Immunizations for Adolescents (IMA-2) poster contest kicked off its second year with Anderson Middle School with hopes to expand this project with other local schools. Last year we saw a 6% IMA-2 rate gain in the corresponding zip code.
Important HEDIS 2019 dates include: Roadmap to be submitted to our auditor in January On-site audit will be conducted 02/13/19 Medical Record project begins 02/11/19
The Interim NCQA Accreditation mock survey has concluded and PHC is well positioned with an estimated 47 out of 50 points earned. The formal interim survey will be 06/04/19.
DHCS recently conducted 14 directed site reviews of PHC providers in Sonoma County. This is a periodic request of DHCS to evaluate the effectiveness of the site review process as deployed by managed care plans. PHC drafted the resulting corrective action plans (CAP) and is awaiting final CAP criteria from the state before issuing to sites.
A new eSite Review tool is being developed and is currently in user acceptance testing to measure efficiency gains from transitioning from a paper to electronic tool.
III. Old Business None
N/A
IV. New Business (Committee Members as Applicable)Consent Calendar
Quality Improvement: MPQD1001 – Quality and Performance Improvement Program Description MPQP1003 – Physician Advisory Committee (PAC) MPQP1038 – Physician Orders for Life-Sustaining Treatment (POLST) Utilization Management/Care Coordination: MCUP3044 – Urgent Care Services MCUP3053 – Acute Inpatient Administrative Days MCUP3102 – Vision Care MPUG3031 – Nebulizer Guidelines
Motion to approve: Dr. Marshall Kubota Second: Dr. Mark Netherda All consent policies were approved without changes.
01/08/2019
1. MPPRGR210 – Provider Grievance
Mary Kerlin reported on MPPRGR210 found on page 69. Added wording “the Plan’s implementation of DHCS Regulatory or other State and
Federal requirements,” to the Purpose statement Added “Senior” to Health Services Director job title Added “Senior” to Provider Relations Director job title
Motion to approve: Mary Kerlin Second: Rachael French Approved without changes
01/08/2019
2. MPXG5001 – Clinical Practice Guidelines for Diagnosis and Management of Asthma
Stan Leung reported on MPXG5001 found on page 72. Removed reference to Global Initiative for Asthma (GINA) in Attachment A and kept in
references only. Attachment B is now Attachment A QVAR Redihaler, Pulmicort Flexhaler, Armonair Respiclick, and generic AirDuo are
added to the PHC formulary Reference updated to reflect the 2018 GINA Report
Motion to approve: Stan Leung Second: Dr. Marshall Kubota Approved without changes
01/08/2019
26 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION DATE RESOLVED
3. MPXG5002 – Clinical Practice Guidelines for Diabetes Mellitus
Stan Leung reported on MPXG5002 found on page 84. Ertugliflozin (Steglatro), ertugliflozin-metformin (Segluromet) has been added to the
formulary with step therapy required Admelog is formulary preferred rapid-acting insulin. Humalog, Novolog, and Apidra is
now non-formulary Anna asked if we should add MPUG3025 Insulin Infusion Pump and Continuous Glucose Monitor Guidelines and new policy MCUP3141 Diabetes Prevention Policy as a related policies. Dr. Moore agreed these should be added, but will need to wait to add MCUP3141 until it is official.
Motion to approve: Anna Campbell Second: Stan Leung Approved with change Add MPUG3025 to Section I Related
Policies
01/08/2019
4. MCUP3131 – Genetic Screening and Diagnostics
Dr. Moore reported on MCUP3131 found on page 87. Added codes per OIL 070n-12 to 81243 and 81244 Updated per Medi-cal guidelines path molec changes Replaced Attachment B with a new document – Family History Screening Tool Clarified some wording at the beginning of Attachment A for BRCA1/2 Anna advised that code 81335 had been added to the grid in Attachment A, but was not listed on the synopsis of changes. Mary noted in the meeting that we need to be sure any new codes are not capped to Quest. Paula asked if UM had consulted Claims on the code changes prior to updating the policy. Anna advised that they did not, but some of the changes were in response to emails from Claims about OILS and that Claims is flagged on the Synopsis of Changes. Dr. Moore stated that the Claims department should be following the progress of the policy changes after policy revisions are finalized at PAC.
Motion to approve: Rachael French Second: Anna Campbell Approved without changes
01/08/2019
5. MCUP3137 – Palliative Care Intensive Program (Adult)
Dr. Moore reported on MCUP3137 found on page 151. Updated policy as per APL 18-020 Palliative Care 12/07/2018 Updated title and language of policy to specify it is for Adults Added a 5th diagnosis that qualifies for engagement which was End Stage Degenerative
Neurologic Condition and also stated that other patients may be considered on a case-by-case basis.
Updated assessment requirements for enrolled members Added criteria for Re-Enrollment Added criteria for Disenrollment Removed wording that stated PHC will inform and update providers on this benefit Removed wording that said disputes, grievances, and appeals will be handled through
PHC grievance process Removed reference to the Pediatric Palliative Care Waiver program Dr. Kubota recommended to change “End Stage Degenerative” to “Progressive Degenerative” Neurologic Disorder. Dr. Moore agreed this should be changed. Committee also agreed to add “DO” along with the “MD” credential in Section VI, Item B.1.c.2.
Motion to approve: Erika Robinson Second: Rachael French Approved with changes Changed “End Stage Degenerative”
to “Progressive Degenerative” in three places: Section VI, Item B.1.a.5) Section VI, Item B.5.e Attachment A, 5th diagnosis
described Include “DO” with the MD
credential in Section VI, Item B.1.c.2)
01/08/2019
6. MCUG3110 – Evaluation and Management of
Anna Campbell reported on MCUG3110 found on page 184. Anna advised that this policy was approved at the November IQI, but was not approved in QUAC due to no quorum. One additional change is being requested at this time:
Motion to approve: Dr. Robert Moore Second: Dr. Marshall Kubota Approved without changes
01/08/2019
27 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION DATE RESOLVED
Obstructive Sleep Apnea in Adults
Section VI.C.4 fifth line, based on the discussion at the last CMO/MD meeting changed wording from “is preferred” to “is another acceptable option” as related to the option of unattended portable monitoring.
7. MCUP3033 – Out of Area Emergency Admissions
Anna Campbell reported on MCUP3033 found on page 188. Section VI.D specified that capitated hospitals assume financial risk from the time that
PHC notifies them that a patient is stable for transfer Removed wording for practices no longer in use Dr. Kubota recommended in Section VI, Items B and C to indicate how the written notice was delivered. Anna advised that they are via fax; the committee agreed to add this for clarification. Anna advised that the new wording added in Section VI, Item D was redundant, therefore the second sentence that states “The financial responsibility lies with the capitated hospital from the time PHC notifies them that the member is stable for transfer.” will be removed.
Motion to approve: Dr. Robert Moore Second: Rachael French Approved with changes Add “via fax” in two places:
Section VI, Item B will read: will notify in writing “via fax”
Section VI, Item C will read: followed by a written notice “via fax”
Section VI, Item D remove the sentence “The financial responsibility lies with the capitated hospital from the time PHC notifies them that the member is stable for transfer.”
01/08/2019
8. MCUP3041 – TAR Review Process
Anna Campbell reported on MCUP3041 found on page 191. As per July 2018 revision to NCQA guidelines for UM5 H, time frame for urgent
concurrent review and urgent preservice decisions was changed from 24 hours to 72 hours from receipt of the request. Also specified a one-time 14 day time extension for urgent review.
Added statement to Attachment A that “No TAR is required for CPAP supplies for a CPAP machine owned by the member (as per Medi-Cal guidelines for ordering/quantity limits).”
Added codes to Attachment A cochlear implant replacement supplies Dr. Kubota recommended a change to Section VI, Item C.1 to clarify that a member cannot request a TAR be classified as urgent, only a Provider can. Committee agreed to add for clarification that the provider should submit. Rose asked if we should only refer to 72 hours and remove “3 calendar days” in Section VI, Item D.7.a.1 and D.7.b.1. Committee agreed to remove “3 calendar days”. In reviewing Attachment A, a comment was made that there is no further explanation next to Fecal Microbiota Transplant (FMT) like there is with Genetic Testing. Committee agreed to add the same wording next to FMT. Dr. Moore suggested that we may want to add policy number references throughout the document. Anna will review the entire attachment and consult with Peggie and Debbie to add policy references where applicable.
Motion to approve: Dr. Marshall Kubota Second: Stan Leung Approved with changes Section VI, Item C.1, second
sentence will read: Requests for an urgent determination should be submitted “by the provider” and clearly marked Urgent or Expedited
Remove “3 calendar days” in two places: Section VI, Item D.7.a.1 Section VI, Item D.7.b.1
Attachment A, add the following language next to FMT: “A TAR is required for all procedures related to fecal microbiota transplant. (see policy MCUP3136 Fecal Microbiota Transplant)”
Review Attachment A and add policy references where applicable
01/08/2019
9. MPUD3001 – Utilization
Anna Campbell reported on MPUD3001 found on page 209. Made updates as per NCQA Mock Survey results
Motion to approve: Dr. Marshall Kubota Second: Erika Robinson Approved with change
01/08/2019
28 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION DATE RESOLVED
Management (UM) Program Description
Updated staff responsibilities, Description of Criteria review with Board Certified specialists, UM Annual Evaluation
Described how we provide written Provider notice of where to locate policies in the Provider Manual on the website
Dr. Kubota recommended to add “PsyD” as a qualified degree for the Behavioral Health Clinical Director; the committee agreed that it should be added.
In the Program Structure section,
under staffing, add “PsyD” as a qualified degree for the Behavioral Health Clinical Director
V. Presentations 1. 2018 Member
Satisfaction Results Kevin Spencer presented 2018 Member Satisfaction Results. Refer to the presentation found on page 243 for detailed information. The survey was sent to 6,000 members who were continuously enrolled over the last 12
months, excluding seniors and persons with disabilities (SPDs). The response rate was 17.1%, an increase over past years.
PHC continues to receive strong ratings in the following categories: Rating of All Health Care Rating of the Health Plan Frequency of Customer Service Information or Help Given Frequency of Courtesy and Respect Given by Customer Service
Questions regarding Mental Health services were added to the survey in the past few years. Kevin reviewed the results in the following categories: Mental Health Service Providers Have Been Seen Within 14 Days of Making First Appointment Satisfaction with Quality of Service Provided
Changes will be made to the 2019 survey which include: Per NCQA the survey will mirror the state issued Consumer Assessment of
Healthcare Providers and Systems (CAHPS) survey and conducted on an annual basis. The QI department will head this effort and will be using a vendor, Morpace.
The member sample size will be much smaller Per NCQA, we will no longer be able to offer incentives to members for completing
the survey which PHC historically offered with our internal mini-CAHPS.
N/A 01/08/2019
2. HEDIS Score Improvement Update
Erika Robinson and Nancy Steffen presented the HEDIS Score Improvement Update. Refer to the presentation found on page 255 for detailed information. The five key goals of the Score Improvement Strategy include:
Develop plan-wide key performance HEDIS indicators HEDIS Accreditation Measure Spotlight presentations at Operations meetings Complete PQD Module 5 Evaluation plan of PQD for the HEDIS and PCP QIP Modules Complete Project Review Board (PRB) request for digital member engagement
system(s) with target completions date of February 28, 2019 Key drivers for Change include:
Organized Initiatives: Member engagement through a coordinated/sustained population health based strategy
Provider Engagement and Accountability Data Quality Infrastructure
N/A 01/08/2019
29 of 86

AGENDA ITEM DISCUSSION RECOMMENDATIONS / ACTION DATE RESOLVED
Interdepartmental Support Community Partnerships
Quality Improvement Initiatives include: Childhood Immunizations (CIS-3) Immunizations for Adolescents (IMA) Asthma Medication Ratio (AMR) Comprehensive Diabetes Care (CDC-Nephropathy)
QI-led technical assistance and training is provided to support practices. This includes education webinars, PCP site visits, ABCs of QI and ADVANCE training.
Now that PQD is fully launched, focus will be on training internal and provider users to fully leverage visualization of performance data
Continue with member engagement efforts and test new outreach strategies Continue efforts to provide actionable data to practices and PHC staff
3. Over/Under Utilization Update
Dr. Moore provided an update on Over/Under Utilization. Refer to the meeting minutes from the last Over/Under Utilization Workgroup found on page 265 for detailed information. Key points include: The PCP Visit Report shows underutilization in PCP visits; if members are non-capitated
it could be an access issue. Dr. Moore to look at the data to determine if there is a denominator issue.
Information regarding underutilization in the AMR measure is included. The QI and Pharmacy departments are working on several programs to improve rates.
California Children Services (CCS) claims review data was presented. The state’s data in comparison to PHC’s carve-in data is extremely different. This suggests that the data coming from the state is incomplete.
There is no evidence of overutilization in pregnancy length of stay (LOS) by hospital. There is no evidence of overutilization in podiatry visits.
N/A 01/08/2019
4. Potential Quality Issues (PQI) and Provider Preventable Conditions (PPC) Report
Rose Santos presented the Q1 and Q2 2018 PQI and PPC Report, which includes both NR and SR. Refer to the report found on page 269 for detailed information. There was a total of 174 PQI referrals received. PQI case processing is 120 days from the date the PQI referral is received in the QI
department. A total of 144 cases were closed. Four PQI cases (two from each region) were reviewed with the Peer Review Committee. There were six PPCs reported; two of which were confirmed PPCs. Dr. Moore suggested to remove the name of the provider or hospital and specific details from the PPC report. Rose will make these edits before presenting at Q/UAC.
N/A 01/08/2019
VI. Additional Business None
N/A N/A
Respectfully submitted by: Karen Garnick, Project Coordinator Signature of Approval: ________________________________________________ Date: ____________________________ Robert Moore, MD, MPH, MBA Chairman 30 of 86

QI Department Update
February 2019
Prepared by Erika Robinson, Director, Quality and Performance Improvement
Quality Improvement Programs (QIPs)
The Primary Care Provider (PCP) QIP wrapped up the 2018 Measurement Year (MY) 12/31/18. Payment and final reports will be distributed in April.
The PCP QIP team hosted a 2019 Kick‐off webinar on 1/30/19 focusing on the 2019 measures.
The Long Term Care QIP concluded the 2018 MY 12/31/18. Data will be collected through early March with payment/final reports distributed in April.
The Palliative Care QIP hosted a 2019 Kick‐off webinar on 1/16/19, which highlighted minor changes to the 2019 measurement specifications.
Payment for the Perinatal QIP Pilot Part I (April ‐ September 2018) is being finalized. Approximately $180,000 will be paid to 40 providers for timely prenatal visits, postpartum visits, and Tdap immunizations. Formal evaluation to follow.
The QIP Team has trained the majority of the QI Department on the Partnership Quality Dashboard and is now expanding training to other departments. Training with providers is ongoing.
eReports 2019 is in final development with user acceptance testing in progress and on track for release March 2019.
Quality Improvement Trainings The Performance Improvement team led an ABCs of QI training specifically for Santa Rosa
Community Health staff on 1/30/19.
Hill Country Community Clinic and Santa Rosa Community Health have each been awarded $100,000 to establish a Transitions Clinic program at their sites. A Transitions Clinic is a medical home for individuals with chronic diseases recently released from incarceration. Both sites will participate in the Transitions Clinic Network of California, which entails one year of technical assistance through the Transitions Clinic Network and California Health Care Foundation.
HEDIS Score Improvement ‐ Highlights
PHC learned a sister plan suspended its texting program due to its “opt‐out” approach in seeking prior express consent per the Telephone Consumer Protection Act of 1991. The HEDIS Measure Score Improvement goal team will recommend PHC adopt an “opt‐in” approach as a key next step in proceeding with exploring texting and e‐mail as digital member engagement.
In 2018, Petaluma Health Center offered a $25 gift card (sponsored by PHC) to members who completed the second dose of the HPV vaccine prior to turning 13. The incentive did not significantly improve performance of the immunization rate; per the clinic’s data, the Immunizations for Adolescents (IMA‐2) rate for December 2017 and 2018 were 68% and 69%, respectively.
State Mandated Work ‐ Performance Improvement Plan (PIP), Plan‐Do‐Study‐Act (PDSA), Corrective Action Plan (CAP)
PHC completed its first series of monthly conference calls with DHCS to track progress under the formal CAP issued last September. Both calls focused on status updates specific to active PDSAs in the Northern Region (NR) for low performing HEDIS measures: Annual Monitoring for Patients on Persistent Medications (MPM), Breast Cancer Screening (BCS), Asthma Medication Ratio (AMR), Immunizations for Adolescents (IMA‐2), and Well Child Visits for 3‐6 year olds (W34). Additionally, PHC highlighted the plan‐wide direct member outreach campaign for MPM in 4Q 2018, the sharing of CIS‐3 population health immunization reports across the PCP QIP, and recent advances in data quality initiatives. Feedback from DHCS has been very favorable. The February update will be an in‐person status update meeting on 2/4/19 in Sacramento with DHCS and PHC senior leadership in attendance. A quarterly executive summary status report has been generated to share during the upcoming meeting.
31 of 86

PHC submitted updated submissions to DHCS in January outlining the results and next steps from PDSA cycles initiated last fall in the NR under MPM, BCS, and IMA‐2. Based on the results and learnings gained, new adapted cycles are planned to start over January/February for each PDSA with the same provider partners as in the first cycles.
PHC is working with providers and community stakeholders in Humboldt and Del Norte Counties to develop an immunization media campaign that will aid in influencing vaccine hesitant patients, estimated as 20‐30% of the overall patient population in the NW region. The audience of this campaign is parents of children ages 0‐2 and pregnant women. This is in the final approval stages along with media planning. In 1Q 2019, the team is focused on completing a Best Practice Guide for providers, offering provider and community organization training events, and executing its media plan. The campaign is targeted for the NW communities March‐May 2019.
The “Plan” portion of Module 4 for two interventions was submitted in mid‐December for the mandated Disparity PIP on Comprehensive Diabetes Care Medical Attention for Nephropathy. Petaluma Health Center, the provider partner, began testing the first intervention in January 2019.
Healthcare Effectiveness Data Information Set (HEDIS)
The HEDIS 2019 on‐site audit will be conducted on 2/13/19.
The HEDIS 2019 Annual project has successfully launched, and our HEDIS Medical Record project will begin 2/11/19. o Health Data Vision, Inc. (HDVI), PHC’s contracted medical records retrieval vendor, will begin
contacting providers to schedule a date for on‐site and provider method (i.e., fax, mail) medical record retrieval on 2/11/19.
o KDJ Consultants, PHC’s contracted medical records retrieval vendor, will outreach to providers who have requested EMR remote retrieval by 2/11/19. If a site would like to request EMR remote retrieval, they should contact the HEDIS team as soon as possible by phone at (866) 828‐2302 or by email at [email protected]. All inquiries regarding HEDIS Medical Record Retrieval can be directed to the HEDIS team: HEDIS Hotline: (866) 828‐2302 HEDIS Email: [email protected] HEDIS Fax: (707) 863‐4314
Quality Compliance and Accreditation
NCQA has officially outreached to PHC confirming our scheduled Interim Survey, 6/4/19. In addition, NCQA introduced PHC’s assigned Accreditation Survey Coordinator (ASC), who is now our point of contact for any questions related to Interim Survey preparation. The ASC will contact PHC 9 to 12 weeks prior to submission to schedule an introductory call.
PHC set a plan‐wide goal to obtain 80% compliance across all First Survey Standards by 6/30/19 and 100% compliance by 12/31/19. As of January 15, PHC is at 37% compliance. PHC remains on track and continues to prioritize Interim and First Survey Accreditation activities.
Quality Assurance and Patient Safety Team (Cross Regional Update)
Efforts are still underway to launch the new eSite Review Tool. Training for all nurses and
coordinators has been completed. The team is conducting user acceptance testing (UAT) via side‐by‐
side site reviews and desktop test cases. A mid‐February go‐live is currently estimated.
Potential Quality Issue (PQI) for the period of 11/28/18 to 1/24/19:
There were 24 PQI referrals received ‐ 15 from Complaints/Grievance/Appeals; 2 from Utilization
Management; 4 from Care Coordination; 1 from Assistant Medical Director; and 2 from providers.
The most common referral indicators were related to assessment, treatment, and misdiagnosis.
There were 37 PQI cases processed and closed. 5 cases were reviewed by the Peer Review
Committee; 4 cases were closed beyond the 120‐calendar day review timeframe.
Site Review (SR) for the period of 11/28/18 to 1/24/19:
The team conducted 22 Facility Site Reviews (FSR); 22 Medical Record Reviews (MRR); and 4 Ob/Gyn Specialty Provider Reviews. As a result, 5 sites were issued FSR Corrective Action Plans (CAP), and 10 sites were issued MRR CAPs.
32 of 86

Page 1 of 2
Policy/Procedures/Guidelines Old Number
New Assigned Number
Comments Provider Manual
Reminder - Effective January 2018, Approval Date reflects that of the Physician Advisory Committee’s meeting date.
Health Services - Quality
Physician Advisory Committee MPQP1003 Regular review; updated to reflect current processes and staff as recommended by the National Committee for Quality Assurance (NCQA)
X
The following documents were reviewed by the Quality / Utilization Advisory Committee (Q/UAC) in February 2019
Clinical Practice Guidelines
MPQP1006 Regular review; no changes to policy content
X
Provider Preventable Condition (PPC) Reporting
MPQP1055 Regular review; Definitions and References updated; language clarifications and applicable hyperlinks added
X
Physical Accessibility Review Survey – SR Part C Attachments: A. Physical Accessibility Review Survey
Guidelines Tool B. Hospital Letter – 1st C. Hospital Letter – 2nd D. Provider Determination Letter
MCQP1052 Regular review; updated per contractual obligations; minor language clarifications added; section on Delegation of Physical Accessibility Review Survey (PARS) functions added; References updated
X
Administration
Medi-Cal Member Grievance System CGA-024 Regular review; updated to reflect NCQA requirements
X
Health Services – Clinical Practice Guidelines
Clinical Practice Guideline: Pain Management, Chronic Pain Management, and Safe Opioid Prescribing Attachments: updated (previous A reference removed – attachment hierarchy updated) A. PHC Recommendations for Safe Use
of Opioid Medications: PCP B. PHC Recommendations for Safe
Use…: Community Pharmacy C. PHC Recommendations for Safe
Use…: Emergency Department D. PHC Recommendations for Safe
Use…: Dentist Prescribing
MPXG5008 Regular review; language clarifications added; some verbiage repositioned for clarity; References updated
Attachments A & D updated with Controlled substance Utilization Review and Evaluation System (CURES) recommendations
X
Lactation Clinical Practice Guideline MPXG5009 Regular review; language clarifications added; hyperlinks to Baby Friendly Hospital Initiative and American Academy of Pediatrics (AAP), and References updated
X
PHCSystem Updates
March 2019
33 of 86
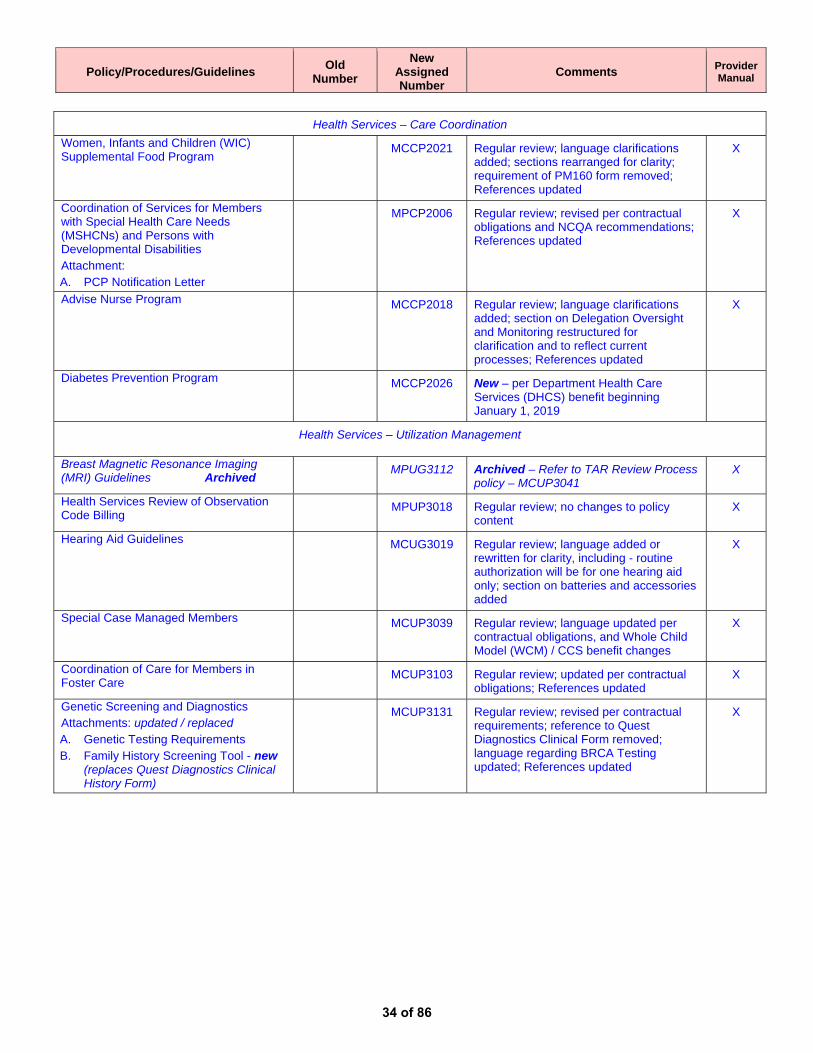
Policy/Procedures/Guidelines Old Number
New Assigned Number
Comments Provider Manual
Health Services – Care Coordination
Women, Infants and Children (WIC) Supplemental Food Program
MCCP2021 Regular review; language clarifications added; sections rearranged for clarity; requirement of PM160 form removed; References updated
X
Coordination of Services for Members with Special Health Care Needs (MSHCNs) and Persons with Developmental Disabilities Attachment: A. PCP Notification Letter
MPCP2006 Regular review; revised per contractual obligations and NCQA recommendations; References updated
X
Advise Nurse Program MCCP2018 Regular review; language clarifications added; section on Delegation Oversight and Monitoring restructured for clarification and to reflect current processes; References updated
X
Diabetes Prevention Program MCCP2026 New – per Department Health Care Services (DHCS) benefit beginning January 1, 2019
Health Services – Utilization Management
Breast Magnetic Resonance Imaging (MRI) Guidelines Archived
MPUG3112 Archived – Refer to TAR Review Process policy – MCUP3041
X
Health Services Review of Observation Code Billing
MPUP3018 Regular review; no changes to policy content
X
Hearing Aid Guidelines MCUG3019 Regular review; language added or rewritten for clarity, including - routine authorization will be for one hearing aid only; section on batteries and accessories added
X
Special Case Managed Members
MCUP3039 Regular review; language updated per contractual obligations, and Whole Child Model (WCM) / CCS benefit changes
X
Coordination of Care for Members in Foster Care
MCUP3103 Regular review; updated per contractual obligations; References updated
X
Genetic Screening and Diagnostics Attachments: updated / replaced A. Genetic Testing Requirements B. Family History Screening Tool - new
(replaces Quest Diagnostics Clinical History Form)
MCUP3131 Regular review; revised per contractual requirements; reference to Quest Diagnostics Clinical Form removed; language regarding BRCA Testing updated; References updated
X
34 of 86

Quality Utilization Advisory Committee (QUAC) Meeting
Grievance & Appeals
February 20, 2019
La Rae Banks, MBA-HMAssociate Director
35 of 86

Eureka | Fairfield | Redding | Santa Rosa
AGENDA
Trends
Drivers
Operational Improvements
There are changes everywhere!
What is causing members to complain?
How many members are dissatisfied?
Note: Excludes cases for members assigned to Kaiser Permanente as their PMG/PCP. Also excludes cases by members regarding Beacon
Health Options (Beacon). PHC is contacted with Beacon to provide outpatient mental health services to our members. Kaiser and Beacon are
delegates for managing exempts, grievances, appeals, and State Hearing for these services on behalf of PHC. 36 of 86

Eureka | Fairfield | Redding | Santa Rosa
Case Trends
1Q18436 =Avg CCPM
2Q18447 =Avg CCPM
3Q18532 =Avg CCPM 4Q18
519 =Avg CCPM
# Closed Cases by Month2018 in Review
Closed 5,887 Investigations!(vs. 2,990 in 2017)
2,874 = Grievances 1,779 = Exempts 1,133= Appeals 98 = State Hearings 2 = L2 Grievances
279 Case Extensions Filed & 13 cases missed DHCS 30-day TAT
652 cases in a single month – August historical high
150 Appeal cases in a single month –October historicalhigh
22 20 22 21 22 21 21 23 19 23 20 18
MED 90
11 11 11 11 12 14 14 13 13 13 1311 # GC’s
# working days
Notes: CCPM refers to Closed Cases per Month. TAT refers to Turnaround Time. GC refers to Grievance Coordinator.
37 of 86
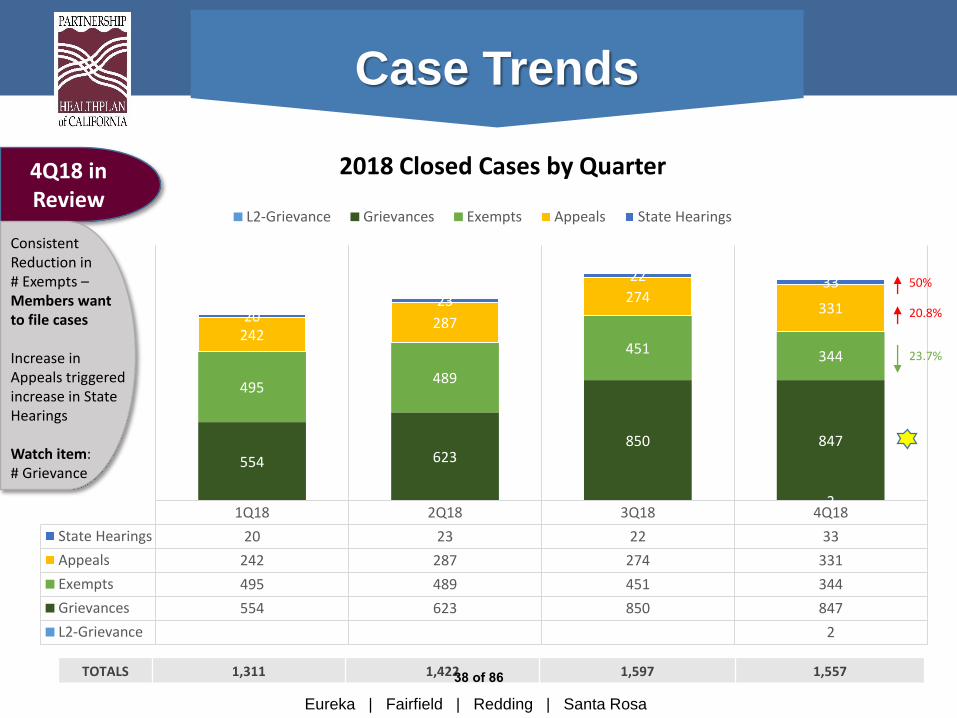
Eureka | Fairfield | Redding | Santa Rosa
1Q18 2Q18 3Q18 4Q18
State Hearings 20 23 22 33
Appeals 242 287 274 331
Exempts 495 489 451 344
Grievances 554 623 850 847
L2-Grievance 2
2
554 623850 847
495489
451 344
242287
274331
2023
22 33
L2-Grievance Grievances Exempts Appeals State Hearings
4Q18 in Review
TOTALS 1,311 1,422 1,597 1,557
2018 Closed Cases by Quarter
Case Trends
Consistent Reduction in# Exempts –Members want to file cases
Increase in Appeals triggered increase in State Hearings
Watch item: # Grievance
50%
20.8%
23.7%
38 of 86

Eureka | Fairfield | Redding | Santa Rosa
Jan Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec
State Hearings 8 6 6 4 6 13 4 9 9 12 14 7
Appeals 78 73 91 106 105 76 90 99 85 150 108 72
Exempts 131 196 168 172 142 175 157 181 113 141 116 87
Grievances 165 153 236 182 227 214 239 363 248 326 289 232
L2 Grievances 2
2
165 153236
182 227 214 239
363
248326 289
232
131 196
168172
142 175 157
181
113
141116
87
7873
91106 105 76 90
99
85
150
108
7286
64 6 13 4
9
9
12
14
7
L2 Grievances Grievances Exempts Appeals State Hearings
4Q18 in Review
2018 Closed Cases by Month
2%
19%
31%
48%
.03%
TTL
98
1,133
1,779
2,874
2
Reduction -Exempts represent 22%of cases
Increase -Grievances represent 55%
Increase –Appeals represent 22%
Case Trends
5,887
39 of 86

Eureka | Fairfield | Redding | Santa Rosa
Non-Medical Transportation (NMT) Benefit• Covers transportation to/from covered Medi-Cal appointment
• Lowest cost option applies, as medically appropriate
• Taxi, bus, public/private transportation
• Mileage reimbursement to family & friends
• No restriction on number of rides
• Member cannot own personal vehicle
• Benefit managed by Medical Transportation Management (MTM)
Case Trends
MTM complaints represent 20.86% of cases in 4Q18
40 of 86
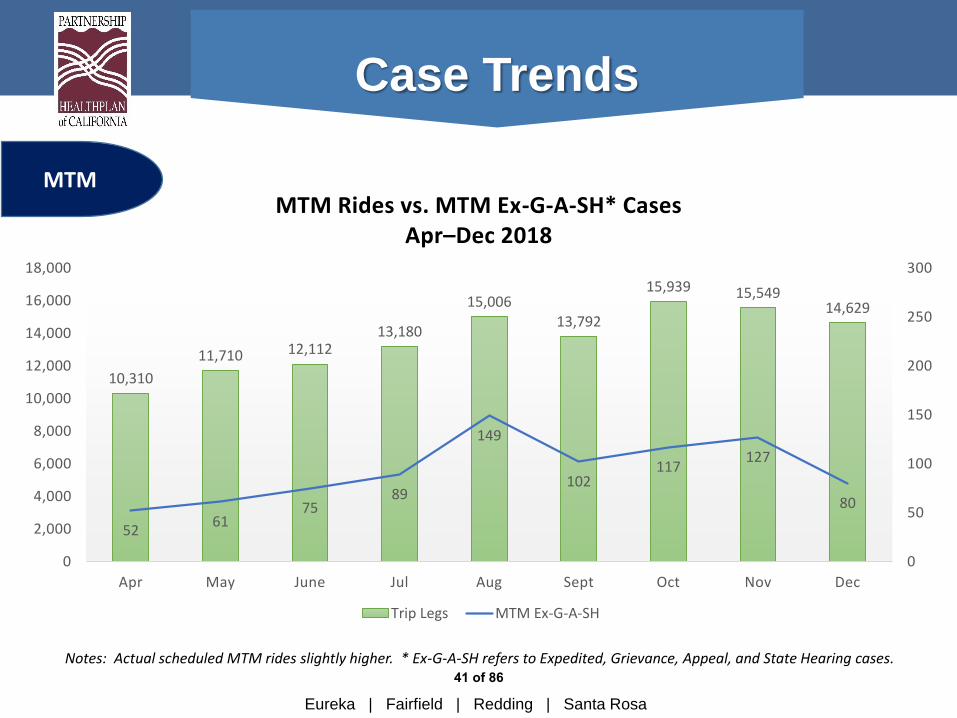
Eureka | Fairfield | Redding | Santa Rosa
10,310
11,710 12,11213,180
15,00613,792
15,939 15,54914,629
5261
7589
149
102117
127
80
0
50
100
150
200
250
300
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
Apr May June Jul Aug Sept Oct Nov Dec
MTM Rides vs. MTM Ex-G-A-SH* CasesApr–Dec 2018
Trip Legs MTM Ex-G-A-SH
MTM
Case Trends
Notes: Actual scheduled MTM rides slightly higher. * Ex-G-A-SH refers to Expedited, Grievance, Appeal, and State Hearing cases. 41 of 86

Eureka | Fairfield | Redding | Santa Rosa
464
580
478 491
653
454
631
532
401
5261
75 89
149102
117 127
80
0
100
200
300
400
500
600
700
Apr May June Jul Aug Sept Oct Nov Dec
G&A Closed Cases vs. MTM Closed CasesApr-Dec 2018
Ttl Cases MTM
22.8% 18.5%
MTM
22.5%15.6%
11.2%
10.5%
18.1%
Note: % value represents the % of MTM cases as a subset of overall G&A cases for the stated month
23.9%
Case Trends
20.2%
42 of 86

Eureka | Fairfield | Redding | Santa Rosa
39
10
20
42
65
111
257
44
17
17
51
51
187
488
12
17
20
33
65
91
557
2
15
13
34
70
54
609
0 100 200 300 400 500 600 700
Withdrawn
Billing
Rudeness
Quality of Care
Discrimination
Access
Quality of Service
4Q18
3Q18
2Q18
1Q18
Driver of Trends
Note: Categorization represents major grouping of grievances. It does not account for all grievances.
Grievances by Categories
Dissatisfaction w/MTM TAR-Medications Treatment Plans Communication
Most Common
DHCS Reporting
Trends
43 of 86

Eureka | Fairfield | Redding | Santa Rosa
Driver of Trends
NCQA Grievance Reporting
Grievance Volume Report (NCQA reporting based on total members)
GRIEVANCE
Quarter 1 Quarter 2 Quarter 3 Quarter 4
# ComplaintsComplaints Per
1,000 Members# Complaints
Complaints Per
1,000 Members# Complaints
Complaints Per
1,000 Members# Complaints
Complaints Per
1,000 Members
Quality of Care 163 0.29 132 0.23 213 0.38 154 0.28
Access 95 0.17 134 0.24 60 0.11 41 0.07
Attitude/Service 257 0.45 284 0.50 508 0.91 352 0.64
Billing/Financial 26 0.05 0 0.00 7 0.01 7 0.01
Quality of Provider Site 8 0.01 2 0.00 2 0.00 0 0.00
Total/Number per
1,000549 0.97 552 0.98 790 1.42 554 1.00
44 of 86
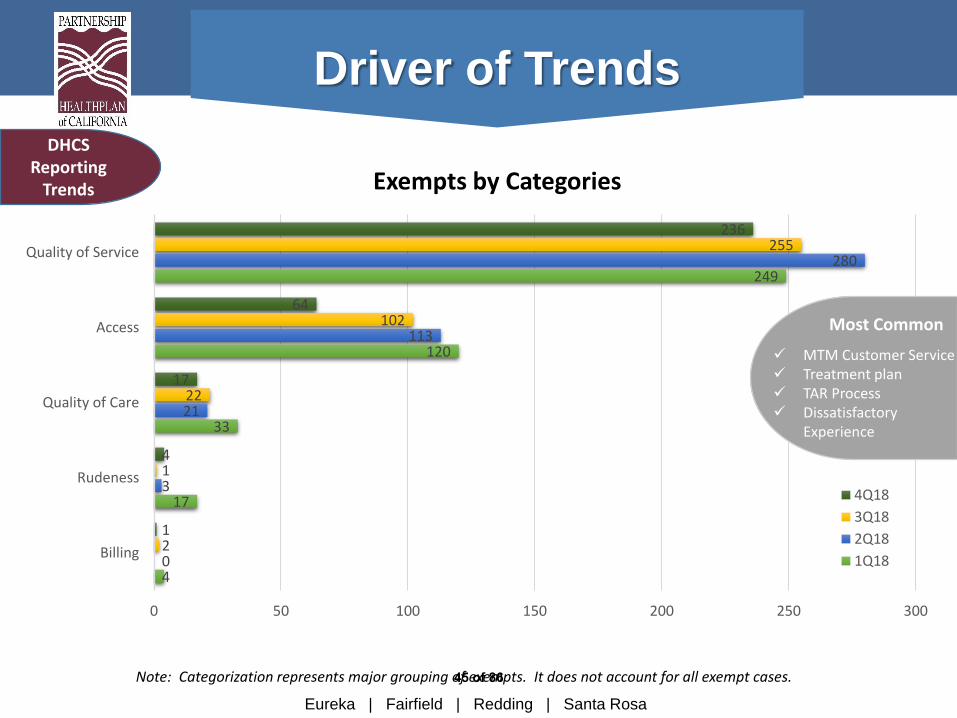
Eureka | Fairfield | Redding | Santa Rosa
4
17
33
120
249
0
3
21
113
280
2
1
22
102
255
1
4
17
64
236
0 50 100 150 200 250 300
Billing
Rudeness
Quality of Care
Access
Quality of Service
4Q18
3Q18
2Q18
1Q18
Note: Categorization represents major grouping of exempts. It does not account for all exempt cases.
Exempts by Categories
MTM Customer Service Treatment plan TAR Process Dissatisfactory
Experience
Most Common
Driver of TrendsDHCS
Reporting Trends
45 of 86

Eureka | Fairfield | Redding | Santa Rosa
134
89
36
146
94
48
143
92
39
177
114
39
0 20 40 60 80 100 120 140 160 180 200
Upheld
Overturned
Withdrawn
4Q18
3Q18
2Q18
1Q18
Appeals by Categories
TAR – Opioids TAR - Medications TAR – Diagnostic testing
Most Common
Driver of TrendsDHCS
Reporting Trends
46 of 86

Eureka | Fairfield | Redding | Santa Rosa
10
3
7
1
1
15
3
2
2
1
13
3
5
1
0
18
7
6
1
1
0 2 4 6 8 10 12 14 16 18 20
Withdrawn
Dismissed
Upheld
Stipulated
Overturned
4Q183Q182Q181Q18
State Hearings by Categories Highlights
1 Overturned TAR denial for Jardiance
Most common SH are pharmacy-related TARs
Driver of TrendsDHCS
Reporting Trends
Quarter Withdrawn Dismissed Upheld Stipulated Overturned
Q1 45.5% 13.6% 31.8% 4.5% 4.5%
Q2 65.2% 13.0% 8.6% 8.6% 4.3%
Q3 59.1% 13.6% 22.7% 4.5% 0%
Q4 54.5% 21.2% 18.2% 3% 3%47 of 86

Eureka | Fairfield | Redding | Santa Rosa
Driver of Trends
NCQA Appeals Reporting
Appeals Volume Report (NCQA reporting based on total members)
Appeal
Quarter 1 Quarter 2 Quarter 3 Quarter 4
# AppealsAppeals Per 1,000
Members# Appeals
Appeals Per 1,000
Members# Appeals
Appeals Per 1,000
Members# Appeals
Appeals Per 1,000
Members
Quality of Care 0 0 0 0 0 0 0 0
Access 0 0 0 0 0 0 0 0
Attitude/Service 164 0.289 210 0.37 236 0.423 157 0.284
Billing/Financial 6 0.011 13 0.023 19 0.034 1 0.002
Quality of Provider Site 0 0 0 0 0 0 0 0
Total/Number per
1,000170 0.3 223 0.393 255 0.457 158 0.286
48 of 86

Reporting Interest (RI) Categories
Improves ability to report to DHCS-mandated reports
Promotes internal reporting -actionable insight beyond DHCS/NCQA regulatory reporting categories
New classifications apply to all case types
Categories defined based on case trends
Multiple RI per case based on investigators’ perspective
Driver of Trends
49 of 86
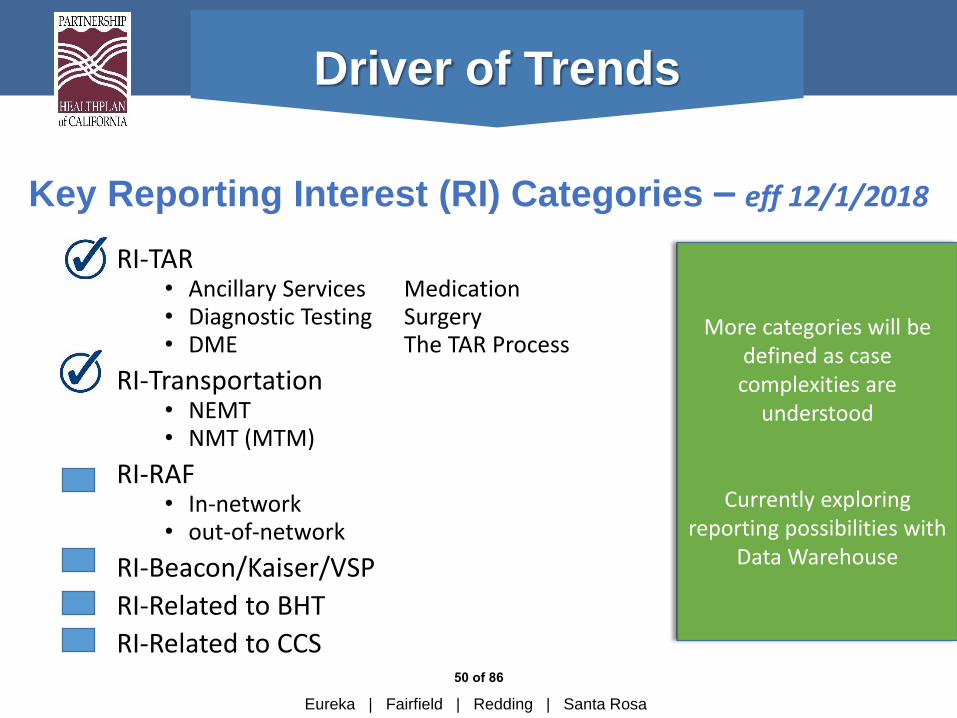
Eureka | Fairfield | Redding | Santa Rosa
Driver of Trends
Key Reporting Interest (RI) Categories – eff 12/1/2018
RI-TAR• Ancillary Services Medication• Diagnostic Testing Surgery• DME The TAR Process
RI-Transportation• NEMT• NMT (MTM)
RI-RAF • In-network• out-of-network
RI-Beacon/Kaiser/VSP
RI-Related to BHT
RI-Related to CCS
More categories will be defined as case complexities are
understood
Currently exploring reporting possibilities with
Data Warehouse
50 of 86

Eureka | Fairfield | Redding | Santa Rosa
RI-TARCategory
Appeals Grievance Exempts
Ancillary 1 0 0
Diagnostic 4 3 0
DME 4 5 2
Medication 29 11 6
TAR Process 0 12 1
Surgery 2 0 0
Other 1 0 0
TOTALS 41 31 9
Driver of Trends
General Category # Sub-Category # Sub-Category Detail #
RI-TAR 81 Ancillary 1
Diagnostic 7 CT 3
MRI 4
DME 11 Wheelchairs\accessories 3
Oxygen 1
Walkers 1
CPAP Supplies 1
Other 5
Medication 46 Oxycodone 7
Tramadol 6
Hydrocodone 4
Methylphenidate 2
Lyrica\Pregabalin 1
DMR 1
Dextroamphetamine 2
Alprazolam\Xanax 1
Botox 1
Methadone 1
Other 20
Surgery 2 Back 1
Transgender 1
The TAR Process 13 Delayed by Pharmacy 5
Delayed Provider 2
Member dislikes overall 4
Refused by Provider 1
Other 1
Other 1
RI-TARs
Big Picture View
Detail View
12/1/2018 to 12/31/2018
51 of 86

Eureka | Fairfield | Redding | Santa Rosa
Driver of Trends
What we learned about MTM through Reporting
Interest categories….
Missed/Failed Rides are the most commonly reported
MTM complaints
The top 5 cities with the most issues: Petaluma, Redding, Cloverdale,
Clearlake, Santa Rosa
RI-NMT Appeals Grievances Exempts
NMT - 80 7 67 6
Mileage Reimbursem
ent18%
Missed/Fail Ride34%
Transportation Service
12%
Benefit Dispute
19%
Interruption to Care
2%
MTM Customer
Service10%
Other5%
MTM Reasons for Dissatisfaction
52 of 86

Eureka | Fairfield | Redding | Santa Rosa
Driver of TrendsNMT Sub-Category Detail Volume
Mileage Reimbursement 22
Mileage Reimb-DEFAULT 9
Mileage Reimb-No trip log 5
Mileage Reimb-COMDATA 4
Mileage Reimb-No credentials 4
Missed/Failed Rides 42
Missed Ride-Driver no show 18
Missed Ride-Driver Late 7
Missed Ride-DEFAULT 2
Ride Returned-No vendor 11
Scheduling Issue 4
Transportation Service 23
Conditions-Odor\Vehicle 2
Rude\Behavior 9
Unsafe Driver 3
Taxi Company Preference 9
Benefit Dispute 12
Denied Transport-Protocols 5
Mode of Transportation 7
Meals\Lodging 2
Interruption to Care 3
MTM Customer Service 12
Other 6
Total RI Selections 122
Total Unique Cases 80
Big Picture View
Detail View
RI-Transportation
12/1/2018 to 12/31/2018
RI-NMT Appeals Grievances Exempts
NMT (MTM) -80 7 67 6
NEMT – 4 1 3 0
TOTALS 8 70 6
53 of 86

Eureka | Fairfield | Redding | Santa Rosa
Driver of Trends
A Closer Look at MTM Top 5 Cities with Highest Reporting Interest Trends
14 RI 12 RI 9 RI 7 RI 6 RI
Petaluma, CA Redding, CA Cloverdale, CA Clearlake, CA Santa Rosa, CA
Mileage Reimb-DEFAULT Conditions-Odor\Vehicle Interruption to Care Ride Returned-No vendor Denied Transport-Protocols
Mileage Reimb-DEFAULT Meals\Lodging Missed Ride-Driver no show Missed Ride-Driver no show Rude\Behavior
Missed Ride-Driver no show Mileage Reimb-DEFAULT Missed Ride-Driver no show Missed Ride-Driver no show Mileage Reimb-COMDATA
Missed Ride-Driver no show Mileage Reimb-No trip log MTM Customer Service Rude\Behavior Mileage Reimb-DEFAULT
Missed Ride-Driver no show Mode of Transportation Ride Returned-No vendor Mode of Transportation Ride Returned-No vendor
Missed Ride-Driver no show Mode of Transportation Scheduling Issue MTM Customer Service Rude\Behavior
Missed Ride-Driver no show Rude\Behavior Scheduling Issue z_DEFAULT-Quality of Service
MTM Customer Service Taxi Company Preference Taxi Company Preference
MTM Customer Service Taxi Company Preference z_DEFAULT-Quality of Service
MTM Customer Service Taxi Company Preference
Ride Returned-No vendor z_DEFAULT-Quality of Service
Ride Returned-No vendor Mileage Reimb-No credentials
Ride Returned-No vendor
Scheduling Issue
54 of 86
Eureka | Fairfield | Redding | Santa Rosa
Transformed Audit Practices• Implemented retrospective audit methodology
• New audit criteria to align with DHCS timelines and G&A Best Practices
• New access database to quantify & qualify audit performance
• New reporting to evaluate individual & supervisor audit performanceImmediate feedback on case-specific audit resultsMonthly scorecard for all GCs reflecting audit performanceMonthly scorecard for each Supervisor reflecting team performance
Operational Improvements
55 of 86

Eureka | Fairfield | Redding | Santa Rosa
Questions
56 of 86

Reporting Period: 07/01/2018 – 12/31/2018 Presented by: Lauri Stevenson, RN, Manager of Clinical Quality and Patient Safety
Note: Data excludes PHC members assigned to Kaiser
Physical Accessibility Review Survey (PARS) Report
The purpose of the PARS is to assess the physical accessibility of provider sites using a set of standards approved by DHCS. Results from the PARS will be made available through the PHC website and provider directories. There are two levels upon which a provider’s site will be identified as; they are; basic and limited access, in addition to medical equipment access. Basic Access: Demonstrates that the facility met all 29 critical elements that identify a site’s capability of accommodating members who are seniors and persons with disabilities (SPDs). Limited Access: Demonstrated that the facility is missing or is incomplete in one or more critical elements. Medical Equipment Access: PCP sites only. Demonstrates if a site has a height adjustable exam table and patient accessible weight scales per guidelines (for wheelchair/scooter plus a patient).
Total Part C Surveys Conducted During Time Period: 85 PCP Sites Reviewed: 70 Specialty Sites Reviewed: 15
Counties
Del Norte Humboldt Modoc Shasta Siskiyou Trinity Grand Total
PCP 4 11 3 10 4 1 33
Basic 1 2 5 1 9
Limited 3 9 3 5 3 1 24
SPEC 1 3 4
Limited 1 3 4
Grand Total 4 12 3 13 4 1 37
Counties Marin Mendocino Napa Solano Sonoma Yolo Grand Total
PCP 5 2 6 12 8 4 37
Basic 3 8 4 2 17
Limited 2 2 6 4 4 2 20
SPEC 1 1 1 6 2 11
Basic 1 1 2
Limited 1 6 2 9
Grand Total 6 3 6 13 14 6 48
57 of 86

Reporting Period: 07/01/2018 – 12/31/2018 Presented by: Lauri Stevenson, RN, Manager of Clinical Quality and Patient Safety
Note: Data excludes PHC members assigned to Kaiser
0
1
2
3
4
5
6
7
Access Levels for SPEC Sites Reviewed Jul-Dec 2018
SPEC Basic
SPEC Limited
SPEC ME
0
1
2
3
4
5
6
7
8
9
10
Access Levels for PCP Sites Reviewed Jul-Dec 2018
PCP Basic
PCP Limited
PCP ME
58 of 86

Initial Heath Assessment (IHA) Outreach Pilot
As of 01/15/2019
Background: Per DHCS contractual requirements, an Initial Health Assessment (IHA),
including an Individual Health Education Behavioral Assessment (IHEBA) is to be performed
within 120 days of a member’s enrollment in Partnership HealthPlan of California (PHC) or
within 12 months prior to plan enrollment. The subsequent IHEBA is re-administered at
appropriate age intervals. The below summary highlights PHC’s recent outreach efforts to
support improving the completion rate of IHA’s.
Outreach Efforts Pilot:
During each Facility Site Review and IHA training, sites were educated on documentation of
outreach attempts and how they could be compliant in the IHA measure by documenting three
outreach attempts, even if the member was not seen in clinic. A template sample of an IHA excel
spreadsheet to document the attempts was provided. We asked the sites to utilize the new patient
reports received monthly from PHC Provider Relations (PR). These include a prepopulated
mailing label created by PHC, so this takes care of the initial outreach. We were performing this
pilot to capture the other two outreach attempts. Sites were also educated that PHC would be
asking for the documentation in the form of said spreadsheet, or an Electronic Health Record
(EHR) report, proceeding from the education or site review date to the end of the year. Recently
we sent an email to the 83 sites included in this pilot. We have received documentation for 30
sites, and have received responses from the administrations of two of our largest provider sites
stating that this is too difficult to accommodate and that there was no streamlined way they could
retrieve the information requested. We are working closely with administration at both of the
sites to identify workflows and EHR capability to provide this information in the future.
Looking forward to 2019:
There has been discussion to request that the IHA outreach be included in the sites policies and
procedures. This will need to include their methodology on how they complete this task.
Region # of Sites
Contacted
# of Sites
Responded
# of Pt's
Eligible
# of Pt's with 3
attempts
North 40 20 2412 320
South 43 9 472 104
Grand Total 83 29 2884 424
59 of 86

CREDENTIALING COMMITTEE SUMMARY FOR
PARTNERSHIP HEALTHPLAN OF CALIFORNIA PHYSICIAN ADVISORY COMMITTEE
Pg. 1 of 1* = by phone conference
Committee: Credentialing Committee Date/Time: January 9, 2019 7:00 a.m. – 7:30 a.m. Members Present: Jeffrey Gaborko, MD; David Gorchoff,* MD; Michele Herman, MD; Bradley Sandler, MD PHC Staff: Robert Moore, MD MPH MBA, PHC Chief Medical Officer; Marshall Kubota, MD*, PHC
Regional Medical Director; Mary Kerlin, Senior Director of Provider Relations; Heather Brandeburg, Director of Provider Relations; Rose Rad, Credentialing Supervisor; Carol Kriek, Credentialing Specialist II; Camille Williams, Credentialing Specialist; Mark Netherda, MD*, Regional Medical Director; Kelly Sewell*, Director of Member Services & PR – NR; Bettina Spiller, MD*, PHC Northern Region Medical Director; Michael Vovakes, MD*, PHC Northern Region Medical Director;
AGENDA ITEM DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION TARGET
DATE DATE
RESOLVED
I. Meeting called to order a. Voting member reminder
I. PHC Regional Medical Director Marshall Kubota, MD called the meeting to order at 7:02 am. Dr. Kubota reminded everyone that all items discussed are confidential. a. Marshall Kubota, MD, Regional Medical Director, reminded The Committee of who the voting members are, and voting is restricted to non-PHC staff.
01-09-2019
01-09-2019
II. Review and Approval of previous minutes
II. The Credentialing Committee meeting minutes for December 12, 2018 were reviewed by the Committee. No changes were made.
II. Motion made by: Bradley Sandler, MD. And second by: Michele Herman, MD. Meeting minutes were unanimously approved without changes.
01-09-2019
III. Old Business: a. Review and Approval of Amended Credentialing Minutes from November 14, 2018. b. Status update on provider regarding agreement on restrictions to practice as a continued PHC contracted provider. Provider has accepted a letter from PHC
III. Old Business: a. Review and Approval of Amended Credentialing Minutes from November 14, 2018. b. Status update presented by Dr. Marshall Kubota on provider regarding agreement on restrictions to practice as a continued PHC contracted provider. Dr. Robert Moore reminded the Committee that they voted during the December meeting to require provider to voluntarily agree that they would adhere to the requirements in the Oregon Medical Board’s Action Report as a condition of continued credentialing, pending actions by the Medical
III. Old Business a. Motion made by: Bradley Sandler, MD. And second by: Jeffrey Gaborko, MD. Amended meeting minutes from November 14, 2018 were unanimously approved without changes. b. Motion made by: Bradley Sandler, MD. And second by: Jeffrey Gaborko, MD. Approval for practitioner to continue credentialing with PHC with the conditions outlined in the letter contained on page 8 of the meeting packet.
01-09-2019
01-09-2019
01-09-2019
60 of 86

Page 2 of 5
AGENDA ITEM DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION TARGET DATE
DATE RESOLVED
outlining restrictions on practice.
Board of California. Dr. Moore reviewed the letter with the Committee that provider signed and also gave a overview of the restrictions outlined in the letter.
IV. New Business a. Review and Approval of Routine Practitioner List
IV. New Business a. Please see approved list of Routine Providers on Pages 9-25. The Committee reviewed the routine list of fourteen (14) Physicians, three (3) Non-Physician Medical Practitioners, six (6) Behavioral Health Analysts for Initial Credentialing; twenty-eight (28) Physicians, twelve (12) Non-Physician Medical Practitioners, six (6) Physical Therapists, two (2) Chiropractors, three (3) Occupational Therapists, and three (3) Speech/Language/Pathologist for Re-Credentialing.
IV. New Business a. The Committee reviewed the list of routine practitioners that met PHC credentialing criteria. Motion was made by: Jeffrey Gaborko, MD and second by: Bradley Sandler, MD. The Committee unanimously approved the list of fourteen (14) Physicians, three (3) Non-Physician Medical Practitioners, six (6) Behavioral Health Analysts for Initial Credentialing; twenty-eight (28) Physicians, twelve (12) Non-Physician Medical Practitioners, six (6) Physical Therapists, two (2) Chiropractors, three (3) Occupational Therapists, and three (3) Speech/Language/Pathologist for Re-Credentialing.
01-09-2019 01-09-2019
V. Update on Ongoing Monitoring of Sanctions
V. Update on Ongoing Monitoring of Sanctions Dr. Kubota reviewed the Ongoing Monitoring Of Sanctions Report dated January 9, 2019 and noted there was one license provider identified during the monitoring process: a. MBOC License Alerts (Includes Physical Therapy Board): Provider issued Cease Practice Order effective 01/02/2019. This provider and was termed by PHC on 01/02/2019. b. Heather Brandeburg, Director of Provider Relations, explained that the Monthly Credentialing Committee Report includes those practitioners that the Committee or CMO have asked PHC staff to specifically report out monthly in the event of new items that arise from monitoring related to probation, accusations or other limitation. The Committee reviewed both reports.
V. Providers will remain on monthly monitoring with continued reporting to the Committee. Motion for approval by: Jeffrey Gaborko, MD and second by: Bradley Sandler, MD. Ongoing Monitoring of Sanctions Report and the Monthly Credentialing Committee Monitoring Report unanimously approved by the Credentialing Committee.
01-09-2019
01-09-2019
01-09-2019
61 of 86

Page 3 of 5
AGENDA ITEM DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION TARGET DATE
DATE RESOLVED
VI. Review and Approval of Consent Calendar Items a. Report of Long Term Care Facility, Hospital, and Ancillary provider list. b. Beacon – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. c. Lucille Packard Children’s Hospital (LPCH) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. d. Vision Service Plan (VSP) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. e. Kaiser-San Rafael – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. f. Kaiser-Santa Rosa – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. g. Kaiser-Vacaville –
VI. Credentialing Committee members reviewed and approved consent calendar items: a. Report of Long Term Care Facility, Hospital, and Ancillary provider list. b. Beacon – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. c. Lucille Packard Children’s Hospital (LPCH) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. Dr. Bradley Sandler wanted clarification on where LPCH was located. d. Vision Service Plan (VSP) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. e. Kaiser-San Rafael – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. f. Kaiser-Santa Rosa – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. g. Kaiser-Vacaville – 3rd Quarter 2018 Delegated
VI. Motion for approval by Jeffrey Gaborko, MD and second by: Bradley Sandler, MD. Consent calendar items unanimously approved by the Credentialing Committee. Mary Kerlin clarified that LPCH was located in Palo Alto at the Stanford Hospital Campus.
01-09-2019
01-09-2019
01-09-2019
01-09-2019
01-09-2019
01-09-2019
01-09-2019
01-09-2019 62 of 86

Page 4 of 5
AGENDA ITEM DISCUSSION / CONCLUSIONS RECOMMENDATIONS / ACTION TARGET DATE
DATE RESOLVED
3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. h. Kaiser-Vallejo – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. i. Sutter (Solano) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. j. Sutter (Yolo/Sac) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. k. Dignity (Woodland Clinic Medical Group) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. l. Dignity (Mercy Medical Group) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities.
Credentialing/Re-Credentialing Activities. h. Kaiser-Vallejo – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. i. Sutter (Solano) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. j. Sutter (Yolo/Sac) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. k. Dignity (Woodland Clinic Medical Group) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities. l. Dignity (Mercy Medical Group) – 3rd Quarter 2018 Delegated Credentialing/Re-Credentialing Activities.
01-09-2019
01-09-2019
01-09-2019
01-09-2019
01-09-2019
VII. Meeting Adjourned VII. Meeting adjourned at 7:11 am. 01-09-2019
Page 5 of 5 for Signature Only
63 of 86

January 2019 Credentialing Meeting List
App. Type Practitioner Name Provider Type Practice Name County Name Specialty Description Board Name Board Certified Hospital Name Staff Cat
I Ahrens, Jillian A.,MD SPECOne Community Health - HIV CARE ONLY Yolo Infectious Disease
ABMS of Internal Medicine Yes
Transfer Agreement No Privileges
I Ahrens, Jillian A.,MD SPECOne Community Health - HIV CARE ONLY Yolo Internal Medicine
ABMS of Internal Medicine Yes
Transfer Agreement No Privileges
R Almullahassani, Ameer MD SPEC NBHG: Neurology Solano NeurologyABMS of Psychiatry & Neurology Yes
Northbay Medical Center Active Attending
R Bajada, Diane E.,NP PCP Lake County Tribal Health Center Lake Nurse Practitioner None NoR Bertsch, Audrey J.,DC SPEC Long Valley Health Center Mendocino Chiropractic None No
I Bhela, Serena MD SPEC Nagarathna G. Manjappa MD Inc Napa Internal MedicineABMS of Internal Medicine Yes
Queen of the Valley Provisional
I Bhela, Serena MD SPEC Nagarathna G. Manjappa MD Inc Napa Nephrology None NoQueen of the Valley Provisional
R Breneisen, Jeffrey R.,MD SPEC
NBHG: Heart and Vascular Center - Medical, A Northbay Affiliate Solano
Cardiovascular Disease
ABMS of Internal Medicine Yes
Northbay Medical Center Active Attending
R Breneisen, Jeffrey R.,MD SPEC
NBHG: Heart and Vascular Center - Medical, A Northbay Affiliate Solano Internal Medicine
ABMS of Internal Medicine No
Northbay Medical Center Active Attending
R Burkhalter, Jenifer L.,MD SPEC Camellia Women's Health YoloObstetrics and Gynecology
ABMS of Obstetrics and Gynecology Yes
Mercy San Juan Hospital Active
R Burkhalter, Jenifer L.,MD SPEC Camellia Women's Health YoloObstetrics and Gynecology
ABMS of Obstetrics and Gynecology Yes
Mercy San Juan Hospital Active
R Camilleri, Linda M.,OT Allied Grove Andersen and Ghiringhelli Solano Occupational Therapy None No
I Candrian, Amy BCBA BHP Moonstone Behavioral Solutions Humboldt Behavioral HealthBehavior Analyst Certification Board Yes
R Carrillo, Joseph M.,MD PCP Harvest Pediatrics Napa Pediatrics ABMS of Pediatrics YesQueen of the Valley Active
R Caserza, Nicholas M.,PT SPEC Solano Sports Physical Therapy Solano Physical Therapy None No
I Chang, Simon Y.,MD PCPGN Medical Associates Inc. dba CareConnect Medical Group Orange Family Medicine
ABMS of Internal Medicine No
Admitting Agreement No Privileges
I Chang, Simon Y.,MD PCPGN Medical Associates Inc. dba CareConnect Medical Group Orange SNFist None No
Admitting Agreement No Privileges
R Chen, Iun-Iu A.,DO PCP Petaluma Health Center Sonoma Family MedicineABMS of Family Medicine Yes
Transfer Agreement No Privileges
R Chen, Iun-Iu A.,DO PCPPetaluma Health Center: Rohnert Park Health Center Sonoma Family Medicine
ABMS of Family Medicine Yes
Transfer Agreement No Privileges
I Cohen, Tamar BCBA BHP Gateway Learning Group Behavioral HealthBehavior Analyst Certification Board Yes
ICollado, Orlando A.,Jr., MD SPEC
GN Medical Associates Inc. dba CareConnect Medical Group Orange Family Medicine
ABMS of Family Medicine Yes
Admitting Agreement No Privileges
ICollado, Orlando A.,Jr., MD SPEC
GN Medical Associates Inc. dba CareConnect Medical Group Orange SNFist None Not Applicable
Admitting Agreement No Privileges
R Crume, Brian D.,DC SPECSCHC: Shasta Community Health Center Shasta Chiropractic None No
I Dajnowicz, Wojtek M.,MD SPEC Vohra Wound Physicians of CA Solano Wound Care None NoAdmitting Agreement No Privileges
R Daquioag, Rodolfo A.,MD PCP Rodolfo Daquioag, M.D. Solano Family Practice None NoHospitalist Coverage No Privileges
R David, Consuelo V.,MD SPECDirect Dermatology Professionals, P.C., Solano Dermatology ABMS of Dermatology Yes
No Direct Patient Contact No Privileges
January 201964 of 86
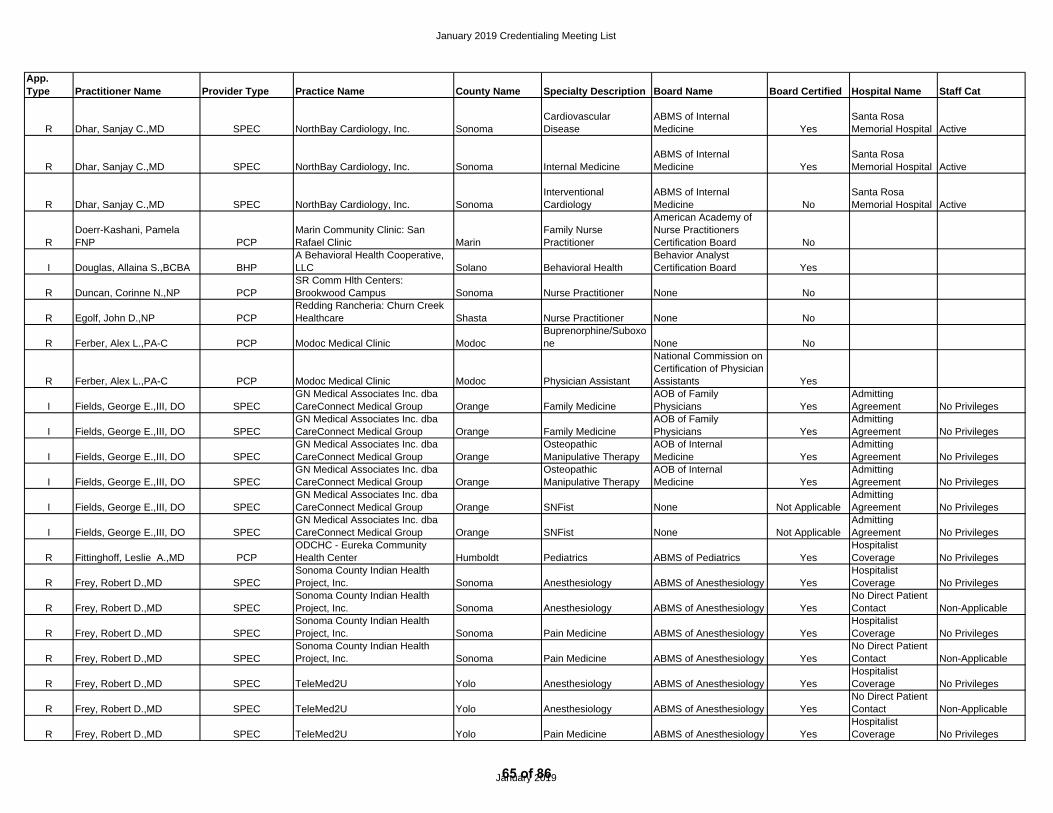
January 2019 Credentialing Meeting List
App. Type Practitioner Name Provider Type Practice Name County Name Specialty Description Board Name Board Certified Hospital Name Staff Cat
R Dhar, Sanjay C.,MD SPEC NorthBay Cardiology, Inc. SonomaCardiovascular Disease
ABMS of Internal Medicine Yes
Santa Rosa Memorial Hospital Active
R Dhar, Sanjay C.,MD SPEC NorthBay Cardiology, Inc. Sonoma Internal MedicineABMS of Internal Medicine Yes
Santa Rosa Memorial Hospital Active
R Dhar, Sanjay C.,MD SPEC NorthBay Cardiology, Inc. SonomaInterventional Cardiology
ABMS of Internal Medicine No
Santa Rosa Memorial Hospital Active
RDoerr-Kashani, Pamela FNP PCP
Marin Community Clinic: San Rafael Clinic Marin
Family Nurse Practitioner
American Academy of Nurse Practitioners Certification Board No
I Douglas, Allaina S.,BCBA BHPA Behavioral Health Cooperative, LLC Solano Behavioral Health
Behavior Analyst Certification Board Yes
R Duncan, Corinne N.,NP PCPSR Comm Hlth Centers: Brookwood Campus Sonoma Nurse Practitioner None No
R Egolf, John D.,NP PCPRedding Rancheria: Churn Creek Healthcare Shasta Nurse Practitioner None No
R Ferber, Alex L.,PA-C PCP Modoc Medical Clinic ModocBuprenorphine/Suboxone None No
R Ferber, Alex L.,PA-C PCP Modoc Medical Clinic Modoc Physician Assistant
National Commission on Certification of Physician Assistants Yes
I Fields, George E.,III, DO SPECGN Medical Associates Inc. dba CareConnect Medical Group Orange Family Medicine
AOB of Family Physicians Yes
Admitting Agreement No Privileges
I Fields, George E.,III, DO SPECGN Medical Associates Inc. dba CareConnect Medical Group Orange Family Medicine
AOB of Family Physicians Yes
Admitting Agreement No Privileges
I Fields, George E.,III, DO SPECGN Medical Associates Inc. dba CareConnect Medical Group Orange
Osteopathic Manipulative Therapy
AOB of Internal Medicine Yes
Admitting Agreement No Privileges
I Fields, George E.,III, DO SPECGN Medical Associates Inc. dba CareConnect Medical Group Orange
Osteopathic Manipulative Therapy
AOB of Internal Medicine Yes
Admitting Agreement No Privileges
I Fields, George E.,III, DO SPECGN Medical Associates Inc. dba CareConnect Medical Group Orange SNFist None Not Applicable
Admitting Agreement No Privileges
I Fields, George E.,III, DO SPECGN Medical Associates Inc. dba CareConnect Medical Group Orange SNFist None Not Applicable
Admitting Agreement No Privileges
R Fittinghoff, Leslie A.,MD PCPODCHC - Eureka Community Health Center Humboldt Pediatrics ABMS of Pediatrics Yes
Hospitalist Coverage No Privileges
R Frey, Robert D.,MD SPECSonoma County Indian Health Project, Inc. Sonoma Anesthesiology ABMS of Anesthesiology Yes
Hospitalist Coverage No Privileges
R Frey, Robert D.,MD SPECSonoma County Indian Health Project, Inc. Sonoma Anesthesiology ABMS of Anesthesiology Yes
No Direct Patient Contact Non-Applicable
R Frey, Robert D.,MD SPECSonoma County Indian Health Project, Inc. Sonoma Pain Medicine ABMS of Anesthesiology Yes
Hospitalist Coverage No Privileges
R Frey, Robert D.,MD SPECSonoma County Indian Health Project, Inc. Sonoma Pain Medicine ABMS of Anesthesiology Yes
No Direct Patient Contact Non-Applicable
R Frey, Robert D.,MD SPEC TeleMed2U Yolo Anesthesiology ABMS of Anesthesiology YesHospitalist Coverage No Privileges
R Frey, Robert D.,MD SPEC TeleMed2U Yolo Anesthesiology ABMS of Anesthesiology YesNo Direct Patient Contact Non-Applicable
R Frey, Robert D.,MD SPEC TeleMed2U Yolo Pain Medicine ABMS of Anesthesiology YesHospitalist Coverage No Privileges
January 201965 of 86

January 2019 Credentialing Meeting List
App. Type Practitioner Name Provider Type Practice Name County Name Specialty Description Board Name Board Certified Hospital Name Staff Cat
R Frey, Robert D.,MD SPEC TeleMed2U Yolo Pain Medicine ABMS of Anesthesiology YesNo Direct Patient Contact Non-Applicable
R Gibson, Cheryl L.,NP PCP Annadel Medical Group Sonoma Nurse Practitioner None No
R Gibson, Cheryl L.,NP PCPAnnadel Medical Group (Family Practice) Sonoma Nurse Practitioner None No
R Gibson, Cheryl L.,NP PCPAnnadel Medical Group: Sebastopol Family Medicine Sonoma Nurse Practitioner None No
I Gikuhi, Jotham K.,FNP PCP Annadel Medical Group SonomaFamily Nurse Practitioner
American Academy of Nurse Practitioners Certification Board Yes
I Gikuhi, Jotham K.,FNP PCPAnnadel Medical Group (Family Med and Internal Med) Sonoma
Family Nurse Practitioner
American Academy of Nurse Practitioners Certification Board Yes
I Gikuhi, Jotham K.,FNP PCPAnnadel Medical Group (Family Practice) Sonoma
Family Nurse Practitioner
American Academy of Nurse Practitioners Certification Board Yes
I Gikuhi, Jotham K.,FNP PCPAnnadel Medical Group: Sebastopol Family Medicine Sonoma
Family Nurse Practitioner
American Academy of Nurse Practitioners Certification Board Yes
R Gott, Dione M.,NP PCPAnnadel Medical Group (Family Med and Internal Med) Sonoma Nurse Practitioner None No
R Gott, Dione M.,NP PCPAnnadel Medical Group: After Hours Care Sonoma Nurse Practitioner None No
I Gutierrez, Rita BCBA BHP Behavior Matters California, LLC Solano Behavioral HealthBehavior Analyst Certification Board Yes
R Halpern, Stephen W.,MD SPEC NorthBay Cardiology, Inc. SonomaCardiovascular Disease
ABMS of Internal Medicine Yes
Santa Rosa Memorial Hospital Active
R Halpern, Stephen W.,MD SPEC NorthBay Cardiology, Inc. Sonoma Internal MedicineABMS of Internal Medicine Yes
Santa Rosa Memorial Hospital Active
R Heller, Lisa M.,PT AlliedNBHG: Northbay Rehab Services-OT/PT Solano Physical Therapy None No
R Hess, Gretchen A.,SLP AlliedNBHG: Northbay Rehab Services OT/PT Solano
Speech & Language Pathology None No
R Hinton, Douglas W.,PT AlliedNBHG: Northbay Rehab Services OT/PT Solano Physical Therapy None No
R Hinton, Douglas W.,PT AlliedNBHG: Northbay Rehab Services-OT/PT Solano Physical Therapy None No
R Hinton, Douglas W.,PT AlliedNBHG: Northbay Rehab Services-OT/PT/SLP Solano Physical Therapy None No
I Hong, Richard MD SPEC Solano Diagnostic Imaging Solano Diagnostic Radiology ABMS of Radiology NoNo Direct Patient Contact No Privileges
I Hong, Richard MD SPEC Solano Diagnostic Imaging Solano
Interventional Radiology & Diagnostic Radiology ABMS of Radiology Yes
No Direct Patient Contact No Privileges
I Hong, Richard MD SPEC Solano Diagnostic Imaging Solano
Vascular & Interventional Radiology ABMS of Radiology No
No Direct Patient Contact No Privileges
R Horta, Elisa E.,MD BOTH Elisa Horta, M.D. Yolo Family MedicineABMS of Family Medicine Yes
Sutter Davis Hospital Active
January 201966 of 86

January 2019 Credentialing Meeting List
App. Type Practitioner Name Provider Type Practice Name County Name Specialty Description Board Name Board Certified Hospital Name Staff Cat
R Horta, Elisa E.,MD BOTH Elisa Horta, M.D. Yolo Obstetrics None NoSutter Davis Hospital Active
R Hurwitz, John P.,DO SPEC Hurwitz, John MD Sonoma SNFistABMS of Internal Medicine Yes
Santa Rosa Memorial Hospital Active
R Illovsky, Michael A.,MD SPEC Health Diagnostics of California MarinCardiovascular Disease
ABMS of Internal Medicine Yes
No Direct Patient Contact No Privileges
R Illovsky, Michael A.,MD SPEC Health Diagnostics of California Marin Diagnostic Radiology None NoNo Direct Patient Contact No Privileges
R Illovsky, Michael A.,MD SPEC Health Diagnostics of California Marin Internal MedicineABMS of Internal Medicine No
No Direct Patient Contact No Privileges
R Kafi, Reza MD SPECDirect Dermatology Professionals, P.C., Solano Dermatology ABMS of Dermatology Yes
No Direct Patient Contact Non-Applicable
RKhalsa, Gurudarshan S.,MD PCP UIHS - Klamath Health Center Del Norte Family Medicine
ABMS of Family Medicine Yes
Hospitalist Coverage No Privileges
I Klein, Phyllis MD SPECDignity Health dba Mercy Regional Cancer Center Shasta Hematology
ABMS of Family Medicine Yes
Mercy Medical Center of Redding Courtesy
I Klein, Phyllis MD SPECDignity Health dba Mercy Regional Cancer Center Shasta Internal Medicine
ABMS of Internal Medicine Yes
Mercy Medical Center of Redding Courtesy
I Klein, Phyllis MD SPECDignity Health dba Mercy Regional Cancer Center Shasta Medical Oncology
ABMS of Internal Medicine Yes
Mercy Medical Center of Redding Courtesy
R Krolikowski, Jeanette DO PCPMarin Community Clinic: Novato Clinic Marin Internal Medicine
ABMS of Internal Medicine Yes
Transfer Agreement No Privileges
RLimvarapuss, Chainarong MD SPEC Solano Hematology Oncology Solano Internal Medicine
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC Solano Hematology Oncology Solano Internal Medicine
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC Solano Hematology Oncology Solano Internal Medicine
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC Solano Hematology Oncology Solano Internal Medicine
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC Solano Hematology Oncology Solano Medical Oncology
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC Solano Hematology Oncology Solano Medical Oncology
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC Solano Hematology Oncology Solano Medical Oncology
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC Solano Hematology Oncology Solano Medical Oncology
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC
Solano Hematology Oncology: Cancer Treat. Ctr. of Vacaville Solano Internal Medicine
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC
Solano Hematology Oncology: Cancer Treat. Ctr. of Vacaville Solano Internal Medicine
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC
Solano Hematology Oncology: Cancer Treat. Ctr. of Vacaville Solano Internal Medicine
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC
Solano Hematology Oncology: Cancer Treat. Ctr. of Vacaville Solano Internal Medicine
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
January 201967 of 86

January 2019 Credentialing Meeting List
App. Type Practitioner Name Provider Type Practice Name County Name Specialty Description Board Name Board Certified Hospital Name Staff Cat
RLimvarapuss, Chainarong MD SPEC
Solano Hematology Oncology: Cancer Treat. Ctr. of Vacaville Solano Medical Oncology
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC
Solano Hematology Oncology: Cancer Treat. Ctr. of Vacaville Solano Medical Oncology
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC
Solano Hematology Oncology: Cancer Treat. Ctr. of Vacaville Solano Medical Oncology
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
RLimvarapuss, Chainarong MD SPEC
Solano Hematology Oncology: Cancer Treat. Ctr. of Vacaville Solano Medical Oncology
ABMS of Internal Medicine Yes
Sutter Solano Medical Center Active
I LiWanPo, Christine A.,DO PCPRedding Rancheria: Churn Creek Healthcare Shasta Family Medicine None No
Mercy Medical Center of Redding Active
R Longoria, James MD SPECSacramento Cardiovascular Surgeons Medical Grp Yolo Surgery ABMS of Surgery Yes
Sutter Medical Center Sacramento Active
R Longoria, James MD SPECSacramento Cardiovascular Surgeons Medical Grp Yolo Surgery ABMS of Surgery Yes
Sutter Medical Center Sacramento Active
R Longoria, James MD SPECSacramento Cardiovascular Surgeons Medical Grp Yolo
Thoracic & Cardiovascular Surgery
ABMS of Thoracic Surgery Yes
Sutter Medical Center Sacramento Active
R Longoria, James MD SPECSacramento Cardiovascular Surgeons Medical Grp Yolo
Thoracic & Cardiovascular Surgery
ABMS of Thoracic Surgery Yes
Sutter Medical Center Sacramento Active
I Manchester, Kathryn CNM SPECMendocino Community Health Clinic: Hillside Health Center Mendocino Nurse - Midwifery
American Midwifery Certification Board Yes
I Manchester, Kathryn CNM SPECMendocino Community Health Clinic: Lakeview Health Center Lake Nurse - Midwifery
American Midwifery Certification Board Yes
I Manchester, Kathryn CNM SPECMendocino Community Health Clinic: Little Lake Health Center Mendocino Nurse - Midwifery
American Midwifery Certification Board Yes
R Marengo, Jason J.,MD SPECNBHG: Center for Specialty Care, A NorthBay Affiliate Solano Plastic Surgery ABMS of Plastic Surgery Yes
Northbay Medical Center Active Attending
R Marengo, Jason J.,MD SPECNBHG: Center for Specialty Care, A NorthBay Affiliate Solano Surgery ABMS of Surgery Yes
Northbay Medical Center Active Attending
R Marengo, Jason J.,MD SPECNBHG: NorthBay Cancer Center: Plastic Surgery Solano Plastic Surgery ABMS of Plastic Surgery Yes
Northbay Medical Center Active Attending
R Marengo, Jason J.,MD SPECNBHG: NorthBay Cancer Center: Plastic Surgery Solano Surgery ABMS of Surgery Yes
Northbay Medical Center Active Attending
R Marengo, Jason J.,MD SPECNBHG: NorthBay Center for Wound Care- Vacaville Solano Plastic Surgery ABMS of Plastic Surgery Yes
Northbay Medical Center Active Attending
R Marengo, Jason J.,MD SPECNBHG: NorthBay Center for Wound Care- Vacaville Solano Surgery ABMS of Surgery Yes
Northbay Medical Center Active Attending
R Martinez, Marcee A.,PT SPECWestern Physical Therapy, Inc.: Mountain View Physical Therapy Shasta Physical Therapy None No
R McMahon, Kelly A.,SLP AlliedNBHG: Northbay Rehab Services-OT/PT/SLP Solano
Speech & Language Pathology None No
I Medina, David M.,PA-C PCPSt Joseph Health Rural Health Clinic Humboldt
Physician Assistant Certified
National Commission on Certification of Physician Assistants Yes
R Nonato, Margaret M.,PA SPECSolano Dermatology Associates, Inc Solano Physician Assistant
National Commission on Certification of Physician Assistants Yes
January 201968 of 86

January 2019 Credentialing Meeting List
App. Type Practitioner Name Provider Type Practice Name County Name Specialty Description Board Name Board Certified Hospital Name Staff Cat
R Nonato, Margaret M.,PA SPECSolano Dermatology Associates, Inc. Solano Physician Assistant
National Commission on Certification of Physician Assistants Yes
R Northfield, Mark R.,MD SPECAnnadel Medical Group - Orthopaedic Surgery Sonoma Orthopaedic Surgery
ABMS of Orthopaedic Surgery Yes
Petaluma Valley Hospital Active
R Peterson, Robert K.,MD SPECNBHG: Ortho Surg A Northbay Affiliate Solano Orthopaedic Surgery
ABMS of Orthopaedic Surgery Yes
Sutter Davis Hospital Active
R Peterson, Robert K.,MD SPECNBHG: Ortho Surg A Northbay Affiliate Solano Orthopaedic Surgery
ABMS of Orthopaedic Surgery Yes
Sutter Davis Hospital Active
R Peterson, Robert K.,MD SPECNBHG: Ortho Surg A Northbay Affiliate Solano Orthopaedic Surgery
ABMS of Orthopaedic Surgery Yes
Sutter Davis Hospital Active
R Peterson, Robert K.,MD SPECNBHG: Ortho Surg A Northbay Affiliate Solano Sports Medicine None No
Sutter Davis Hospital Active
R Peterson, Robert K.,MD SPECNBHG: Ortho Surg A Northbay Affiliate Solano Sports Medicine None No
Sutter Davis Hospital Active
R Peterson, Robert K.,MD SPECNBHG: Ortho Surg A Northbay Affiliate Solano Sports Medicine None No
Sutter Davis Hospital Active
I Pinon, Denise MD PCPCommunity Health Clinic Ole: DBA: Ole Health Napa Family Medicine
ABMS of Family Medicine Yes
Transfer Agreement No Privileges
R Pope, Emily A.,NP PCP Annadel Medical Group Sonoma Nurse Practitioner None No
I Rawlings, Luke M.,MD PCPDignity Health - Mercy Family Practice Clinic Shasta Family Medicine
ABMS of Family Medicine Yes
Mercy Medical Center of Redding Active
I Robinson, Andrew Y.,MD SPEC NBHG: Neurology SolanoClinical Neurophysiology
ABMS of Psychiatry & Neurology Yes
Hospitalist Coverage No Privileges
I Robinson, Andrew Y.,MD SPEC NBHG: Neurology Solano NeurologyABMS of Psychiatry & Neurology Yes
Hospitalist Coverage No Privileges
R Russell, Lori R.,OT AlliedNBHG: Northbay Rehab Services OT/PT Solano Occupational Therapy None No
R Russell, Lori R.,OT AlliedNBHG: Northbay Rehab Services-OT/PT Solano Occupational Therapy None No
R Russell, Lori R.,OT AlliedNBHG: Northbay Rehab Services-OT/PT/SLP Solano Occupational Therapy None No
R Sandhu, Amrita DO PCP Petaluma Health Center Sonoma Family Medicine AOB-Family Medicine YesTransfer Agreement No Privileges
R Sandhu, Amrita DO PCP Petaluma Health Center SonomaOsteopathic Manipulative Therapy AOB-Family Medicine Yes
Transfer Agreement No Privileges
R Sandhu, Amrita DO PCPPetaluma Health Center: Rohnert Park Health Center Sonoma Family Medicine AOB-Family Medicine Yes
Transfer Agreement No Privileges
R Sandhu, Amrita DO PCPPetaluma Health Center: Rohnert Park Health Center Sonoma
Osteopathic Manipulative Therapy AOB-Family Medicine Yes
Transfer Agreement No Privileges
I Shea, Whitney E.,BCBA BHPCenter for Autism and Related Disorders, LLC Solano Behavioral Health
Behavior Analyst Certification Board Yes
R Shipp, Jennifer T.,NP SPEC St. Joseph House Calls Sonoma Nurse Practitioner None No
R Singh, Paramvir MD SPEC Paramvir Singh, MD Inc. Shasta GastroenterologyABMS of Internal Medicine Yes
Shasta Regional Medical Center Active
R Singh, Paramvir MD SPEC Paramvir Singh, MD Inc. Shasta Internal MedicineABMS of Internal Medicine No
Shasta Regional Medical Center Active
RSivakumaran, Muthumanimoli MD PCP
Elica Health Centers-Halyard Medical Center Yolo
Pediatric Infectious Diseases ABMS of Pediatrics Yes
Admitting Agreement No Privileges
January 201969 of 86

January 2019 Credentialing Meeting List
App. Type Practitioner Name Provider Type Practice Name County Name Specialty Description Board Name Board Certified Hospital Name Staff Cat
RSivakumaran, Muthumanimoli MD PCP
Elica Health Centers-Halyard Medical Center Yolo Pediatrics ABMS of Pediatrics Yes
Admitting Agreement No Privileges
R Sloan, Mark P.,MD PCPSR Comm Hlth Centers: Vista Family Health Center Sonoma Pediatrics ABMS of Pediatrics Yes
Hospitalist Coverage No Privileges
R Smircich, Kristine T.,SLP AlliedNBHG: Northbay Rehab Services-OT/PT/SLP Solano
Speech & Language Pathology None No
R Smith, Kathleen A.,OT AlliedNBHG: Northbay Rehab Services OT/PT Solano Occupational Therapy None No
R Stephen, F. O.,MD SPEC Annadel Medical Group Sonoma GastroenterologyABMS of Internal Medicine Yes
Santa Rosa Memorial Hospital Active
R Stephen, F. O.,MD SPEC Annadel Medical Group Sonoma Internal MedicineABMS of Internal Medicine No
Santa Rosa Memorial Hospital Active
R Tang, Emily NP PCP Lake County Tribal Health Center Lake Nurse Practitioner None No
R Tepora, Napoleon H.,PT AlliedNBHG: Northbay Rehab Services-OT/PT Solano Physical Therapy None No
I Terry, Carey R.,MD PCP Alliance Medical Center Sonoma Family MedicineABMS of Family Medicine Yes
Transfer Agreement No Privileges
I Tong, Kathleen MD SPECAdventist Health Physicians Network: Adventist Heart Institute Napa
Advanced Heart Failure and Transplant
ABMS of Internal Medicine Yes St Helena Hospital Provisional
I Tong, Kathleen MD SPECAdventist Health Physicians Network: Adventist Heart Institute Napa
Cardiovascular Disease
ABMS of Internal Medicine Yes St Helena Hospital Provisional
I Tong, Kathleen MD SPECAdventist Health Physicians Network: Adventist Heart Institute Napa Internal Medicine
ABMS of Internal Medicine No St Helena Hospital Provisional
R Truong, Khanh Y.,MD SPECNorCal Dermatology and Cosmetics Sonoma Dermatology ABMS of Dermatology Yes Group Coverage No Privileges
I Turrini, Corinne BCBA BHP Gateway Learning Group Behavioral HealthBehavior Analyst Certification Board Yes
R Warnock, Iden J.,PT AlliedCotati-Rohnert Park Physical Therapy, Inc. Sonoma Physical Therapy None No
R Williams, Helen Y.,FNP PCPSCHC: Anderson Family Heatlh Center Shasta
Family Nurse Practitioner
American Academy of Nurse Practitioners Certification Board Yes
MedicalDirector/ Physician Approval of Routine List
________________________________________ Marshall Kubota, M.D., PHC Credentialing Chairman
January 201970 of 86

AGENDA ITEM: II.F. DATE: 03/13/2019
PARTNERSHIP HEALTHPLAN OF CALIFORNIA
TO: Physician Advisory Committee FROM: Robert Moore, MD, MPH, Chief Medical Officer DATE: 03/13/2019 SUBJECT: PHC Committee Memberships
Physician Advisory Committee Appointment: Matthew Symkowick, MD, Physician-in-charge at Kaiser Permanente, Vallejo, has indicated his interest in membership on the Physician Advisory Committee. Dr. Symkowick is Board Certified in Family Medicine. His appointment is recommended.
71 of 86

PARTNERSHIP HEALTHPLAN OF CALIFORNIA
POLICY / PROCEDURE
Page 1 of 3
Policy/Procedure Number: MPQP1003 (previously QP100103) Lead Department: Health Services Policy/Procedure Title: Physician Advisory Committee (PAC) Policy
External Policy Internal Policy
Original Date: 07/19/1993 - Medi-Cal (Charter)
Next Review Date: 06/13/201902/13/202003/13/2020 Last Review Date: 06/13/201802/13/201903/13/2019
Applies to: Medi-Cal Employees
Reviewing Entities:
IQI P & T QUAC
OPERATIONS EXECUTIVE COMPLIANCE DEPARTMENT
Approving Entities:
BOARD COMPLIANCE FINANCE PAC
CEO COO CREDENTIALING DEPT. DIRECTOR/OFFICER
Approval Signature: Jeffrey Gaborko, M.D. Approval Date: 06/13/201802/13/201903/13/2019
I. RELATED POLICIES:
A. MCUP3042 – Technology Assessment B. MPQP1002 – Quality/Utilization Advisory Committee (Q/UAC) C. MPRP4001 – Pharmacy & Therapeutics (P&T) Committee D. MPCR200 – Credentialing Committee and CMO Credentialing Program Responsibilities
II. IMPACTED DEPTS:
N/A
III. DEFINITIONS: N/A
IV. ATTACHMENTS: A. N/A
V. PURPOSE: The Physician Advisory Committee (PAC) is responsible for oversight and monitoring of the quality and cost-effectiveness of medical care provided to Partnership HealthPlan of California's (PHC’s) members. The PAC reviews the activities of the Quality/Utilization Advisory Committee (Q/UAC), Provider Advisory Group (PAG), Pharmacy and Therapeutics Committee (P&T), the Quality Improvement Program Advisory Group, and the Credentials Committee, makes recommendations, and assists PHC in other ways as defined in this policy.
VI. POLICY / PROCEDURE:
A. COMMITTEE STRUCTURE 1. Membership:
a. The PAC is comprised of the PHC CEO, Deputy Executive Director/Chief Operating Officer, Chief Medical Officer, Regional Medical Directors, Chief Financial Officer, Health Services Director, Provider Relations Director, Quality and Performance Improvement Director, Pharmacy Director, Clinical Director of Behavioral Health and 15-25 other members that may include: 1) Participating physician representatives from primary and specialty care, including at least
one behavioral health provider. 2) Advanced practice clinicians such as certified nurse midwives, nurse practitioners or
physician assistants. 3) Members representing active medical staffs of hospitals, community-based practices, and
72 of 86

Policy/Procedure Number: MPQP1003 (previously QP100103) Lead Department: Health Services
Policy/Procedure Title: Physician Advisory Committee ☒External Policy ☐Internal Policy
Original Date: 07/19/1993 - Medi-Cal (Charter)
Next Review Date: 06/13/201902/13/202003/13/2020 Last Review Date: 06/13/2018032/13/2019
Applies to: ☒ Medi-Cal ☐ Employees
Page 2 of 3
medical groups in the PHC service area. b. Members with annual attendance of <50% are evaluated for termination from the PAC. c. Other health plan staff may make special or periodic reports to the committee or may attend
selected meetings ex-officio. 2. Minutes: MeetingsMinutes are recorded for the purpose of preparing minutes, but recordings are not
retained past thirty days after the meeting date, in accordance with Brown Act Regulationsof all meetings and are maintained.
3. Chair: A PHC Physician on the Committee chairs the meeting and when unavailable, the Chief Medical Officer chairs the Committee.
4. Meetings: The Committee meets at least nine (9) times a year, but does not convene in the months of July or December, with the option to add additional meetings if needed.
5. Voting: Only committee members who are not PHC staff may vote. The Chief Medical Officer serves in a tie breaking capacity as necessary. A quorum is that number of members present as described in the PHC By-Laws which specifies 50% plus one of voting members.
B. COMMITTEE RESPONSIBILITIES 1. Reviews and makes recommendations for corrective action based upon other committee reports
including: a. Q/UAC b. P&T Committee c. Credentials Committee d. PAG
2. Annually reviews, recommends and approves the Quality Improvement Program Description, Quality Improvement Department Program Evaluation and the Quality Improvement Work planPlan, along with the Utilization Management Program Description and the Care Coordination Program Description. Performance in utilization management activities is included in the annual Quality Improvement Evaluation.
3. Provides medical opinion regarding technological advances in consideration of benefit enhancements, inclusions, and exclusions.
4. Technology Review: The Chief Medical Officer or physician designee may request input from an appropriate specialist within the community prior to presenting the request to the Pharmacy and Therapeutics (P&T) Committee, Quality/Utilization Advisory Committee (QUAC), or the Physician Advisory Committee (PAC). This specialist must have expertise in the technology under review. The decision to consult a specialist will depend on the nature of the technology being considered, and will be made on a case-by-case basis.
5. Makes recommendations for HealthPlan policy and protocol changes based on guidelines and standards of practice, and select PHC policies that affect quality improvement, clinical care, or provider issues.
6. Oversight responsibility for utilization, quality, and other staff reports, which monitor the utilization of services and outcomes of quality within the delivery system.
7. Reviews and approves Clinical Practice Guidelines adopted by PHC. 8. Provides oversight to the PCP and Hospital Quality Improvement Programs (QIPs) for providers and
hospitals, which includes: approval of the measures and payment methodologies; in addition to overseeing the implementation and evaluation of the QIP.
9. Advises and assists in the selection of Chief Medical Officer, as needed. C. COMMITTEE ACCOUNTABILITY
1. The Physician Advisory Committee has oversight responsibility for the above listed committees and is accountable to the PHC Board of Commissioners.
VII. REFERENCES:
73 of 86

Policy/Procedure Number: MPQP1003 (previously QP100103) Lead Department: Health Services
Policy/Procedure Title: Physician Advisory Committee ☒External Policy ☐Internal Policy
Original Date: 07/19/1993 - Medi-Cal (Charter)
Next Review Date: 06/13/201902/13/202003/13/2020 Last Review Date: 06/13/2018032/13/2019
Applies to: ☒ Medi-Cal ☐ Employees
Page 3 of 3
N/A VIII. DISTRIBUTION:
A. PHC Department Directors B. PHC Provider Manual
IX. POSITION RESPONSIBLE FOR IMPLEMENTING PROCEDURE: Committee Chairman X. REVISION DATES:
Medi-Cal 10/14/98; 06/14/00; 03/14/01; 06/12/02; 10/13/04; 02/8/06; 04/11/07; 05/14/08; 05/13/09; 06/09/10; 10/10/12; 10/09/13; 04/09/14; 05/13/15; 06/8/16; 06/14/17; *06/13/18; 023/13/19 *Through 2017, Approval Date reflective of the Quality/Utilization Advisory Committee meeting date. Effective January 2018, Approval Date reflects that of the Physician Advisory Committee’s meeting date. PREVIOUSLY APPLIED TO: PartnershipAdvantage MPQP1003 - 04/11/2007 to 01/01/2015 Healthy Families MPQP1003 - 10/10/2012 to 03/01/2013 Healthy Kids 04/11/2007; 05/14/08; 05/13/09; 06/09/10; 10/10/12; 10/09/13; 04/09/14; 5/13/15; 5/11/16 to 12/01/16 (Healthy Kids program ended 12/01/2016)
74 of 86

2018-19 Hospital QIP (HQIP) Proposed Measurement Set: Large Hospitals
2018-19 Large Hospital Measures/Requirements Proposed 2019-20 Large Hospital Measures/Requirements Considerations Health Information Exchange All hospitals. By the end of the measurement year, both of the following:
1. Live with Emergency Department Interface Exchange (EDIE) including a mechanism for the EDIE data to be pushed to ED physicians for patients who are seen.
2. ADT interface with a community HIE. If not met, entire incentive amount will be withheld.
No Change.
Delegation Requirement All capitated hospitals. Capitated hospitals must submit timely and accurate delegation deliverables, according to deadlines outlined in your hospital’s delegation agreement. Deliverables include 1) Utilization Program Structure and 2) delegation reporting requirements. Impact: • Timely submitting > 90.0% of requirements results in 100% incentive. • Timely submitting > 75.0% and < 90.0% of requirements results in 10% cut from incentive. • Timely submitting < 75.0% of requirements results in a 20% cut from incentive.
No Change.
75 of 86

2018-19 Large Hospital Measures/Requirements Proposed 2019-20 Large Hospital Measures/Requirements Considerations
1. All-Cause Adult Readmission Rate
1. All-Cause Readmissions No Change.
2. Palliative Care Capacity. Two options: - Option 1: Dedicated inpatient palliative care team (all hospitals):
o One Physician Champion o One trained Licensed Clinical Social Worker o One trained Licensed RN, NP, or PA (Registered Nurse,
Nurse Practitioner, or Physician Assistant) o Availability of video or in-person consult with a Palliative
Care Physician - Option 2: Inpatient palliative care capacity (small hospitals only):
o Two licensed staff: RN, NP, or PA o Availability of either video or in-person consult with a
Palliative Care Physician
2. Palliative Care Capacity Small Hospitals: 2 options - Option 1: Dedicated inpatient palliative care team (all hospitals):
o One Physician Champion o One trained Licensed Clinical Social Worker OR Licensed RN, NP,
or PA o Availability of video or in-person consult with a Palliative Care
Physician - Option 2: Inpatient palliative care capacity (small hospitals only):
o Two licensed staff: RN, NP, or PA o Availability of either video or in-person consult with a Palliative
Care Physician Large Hospitals: Require Palliative Care Quality Network (PCQN) participation. Participation entails:
• Report summarizing the number of Palliative Care Consults per month (minimum 25 consults in last 3 months of the measurement year).
• Rate of all consults who have completed Advance Directive • Rate of all consults who have a signed POLST on the chart
PCQN participation will apply only to hospitals >100 beds.
6 out of 13 large hospitals already participating.
76 of 86

2018-19 Large Hospital Measures/Requirements Proposed 2019-20 Large Hospital Measures/Requirements Considerations
3. Elective Delivery before 39 weeks Percent of patients with newborn deliveries at ≥ 37 to < 39 weeks gestation completed, where the delivery was elective.
Hospitals submit data to California Maternal Quality Care Collaborative (CMQCC), and PHC will work directly with CMQCC for reports.
3. Elective Delivery before 39 weeks No Change.
4. Exclusive Breast Milk Feeding
Hospitals submit data to California Maternal Quality Care Collaborative (CMQCC), and PHC will work directly with CMQCC for reports.
4. Exclusive Breast Milk Feeding Rate No Change.
5. Nulliparous, Term, Singleton, Vertex (NTSV) Cesarean Birth Rate
Hospitals submit data to California Maternal Quality Care Collaborative (CMQCC), and PHC will work directly with CMQCC for reports.
5. Nulliparous, Term, Singleton, Vertex (NTSV) Cesarean Birth Rate No Change.
6. Venous thromboembolism (VTE)-6 – Hospital-Acquired Potentially-Preventable VTE
Remove. Retired from Joint Commission. High plan wide performance past two years.
7. California Hospital Patient Safety Organization (CHPSO) Patient Safety Organization Participation
• Large hospitals (> 50 licensed general acute beds):
o Submit 50 events o Attend one Safe Table Forum
“Events” include near misses, unsafe conditions, and all levels of harm.
6. CHPSO Patient Safety Organization Participation
• Large hospitals (> 50 licensed general acute beds): o Submit 100 events o Attend 4 Safe Table Forums
Large hospitals only (small hospitals stay the same, see below). The purpose of submitting safety events is for CHPSO to provide each hospital with an analysis of patient safety trends. For an appropriate analysis, CHPSO recommends reporting requirements be increased for large hospitals. The purpose of Safe Table Forums is to share Best Practices and Patient Safety knowledge across hospitals and staff. Safe Tables are remote meetings.
2018-19 Large Hospital Measures/Requirements Proposed 2019-20 Large Hospital Measures/Requirements Considerations
77 of 86

8. California Immunization Registry (CAIR) utilization measure Pay for reporting first year. To earn points for this measure, two steps must be met: 1. Join CAIR and provide CAIRID to PHC 2. Create a CAIR Utilization Policy for your hospital, and send to PHC
Remove. Replace with Pay for Performance Measure. Remove Pay for Reporting measure and replace with Pay for Performance measure.
9. Quality Improvement (QI) Capacity Part I: Summary of a QI training attended
• At least 2 staff members participate in an in-person, PHC-approved program or training (min. 4 CE/CME hours per person) aimed at improving one aspect of hospital quality.
Part II: Summary of a QI Project • Summarize one QI project taking place at your hospital. May
be unrelated to training from Part I.
Remove (from large hospital measurement set only).
The QI team has been successful in creating an archive of QI projects from this measure. Going forward, measure seems most meaningful and appropriate for small hospitals.
78 of 86

2018-19 Large Hospital Measures/Requirements Proposed 2019-20 Large Hospital Measures/Requirements Considerations
7. Substance Abuse Bundle Small Hospitals: Full Points= 2 components, Partial Points= 1 component Large Hospitals: Full Points= 3 components, Partial Points= 2 components i. Voluntary Inpatient Detox (VID): At least 5 patients (large hospital) or 2 patients (small hospital) admitted for VID. Due to billing lag, must be completed in first 9 months of the measurement year. PHC will obtain this data from the state. OR Hospital creates policy for VID. Policy must identify team members who will administer VID ii. Naloxone Fill/Distribution: 50% of patients admitted for opioid overdose or seen in ED with opioid overdose/intoxication have a filled prescription for Naloxone within 6 months of that hospitalization. PHC will use state data on carved out medications for numerator, and admissions diagnosis code for denominator. OR Hospitals submit to PHC a log detailing the amount of Naloxone they took in, and amount that was dispense during the measurement year. iii. Medication Assisted Treatment (MAT) in ED: At least 5 patients (large hospital) or 2 patients (small hospital) started on Medication Assisted Treatment (MAT) in the ED setting. This process entails screening patients on opioids who present in ED, switching appropriate patients to buprenorphine, and arranging follow up with outpatient provider. Screenings may be conducted by either trained in-house staff or a telemedicine provider (e.g. Bright Heart Health). PHC will use state claims data and outpatient provider data to validate hospital-reported information. iv. Medication Assisted Treatment (MAT) in inpatient setting: At least 5 patients (large hospital) or 2 patients (small hospital) started on Medication Assisted Treatment (MAT) in the inpatient setting. v. Support for Hospital Opioid Use Treatment (SHOUT) Hospital adopts Support for Hospital Opioid Use Treatment (SHOUT) program protocols in the ED/Inpatient setting.
Proposed New Measure. Opportunity to treat patients presenting in hospital for substance abuse.
79 of 86

2018-19 Large Hospital Measures/Requirements Proposed 2019-20 Large Hospital Measures/Requirements Considerations 8. Hep B Vaccination for Newborns, capture via CAIR
Rates of Hep B utilization and data capture are currently low. Use PHC delivery data for denominator, and CAIR data for numerator. Numerator: # of Hep B vaccinations in CAIR Denominator: # of deliveries
Proposed New Measure. Meets CAIR requirement from DHCS. This denominator would not take into account twins, triplets, etc., or births that were not live.
80 of 86

2018-19 Hospital QIP Proposed Measurement Set: Small Hospitals
2018-19 Small Hospitals Measures/Requirements Proposed 2019-20 Small Hospitals Measures/Requirements Change Rationale Health Information Exchange All hospitals. By the end of the measurement year, both of the following:
3. Live with Emergency Department Interface Exchange (EDIE) including a mechanism for the EDIE data to be pushed to ED physicians for patients who are seen.
4. ADT interface with a community HIE. If not met, entire incentive amount will be withheld.
No Change.
Delegation Requirement All capitated hospitals. Capitated hospitals must submit timely and accurate delegation deliverables, according to deadlines outlined in your hospital’s delegation agreement. Deliverables include 1) Utilization Program Structure and 2) delegation reporting requirements. Impact: • Timely submitting > 90.0% of requirements results in 100% incentive. • Timely submitting > 75.0% and < 90.0% of requirements results in 10% cut from incentive. • Timely submitting < 75.0% of requirements results in a 20% cut from incentive.
No Change.
81 of 86

2018-19 Small Hospitals Measures/Requirements Proposed 2019-20 Small Hospitals Measures/Requirements Change Rationale 1. All-Cause Adult Readmission Rate
1. All-Cause Readmissions No Change.
2. Palliative Care Capacity. Two options: - Option 1: Dedicated inpatient palliative care team (all hospitals):
o One Physician Champion o One trained Licensed Clinical Social Worker o One trained Licensed RN, NP, or PA (Registered Nurse,
Nurse Practitioner, or Physician Assistant) o Availability of video or in-person consult with a Palliative
Care Physician - Option 2: Inpatient palliative care capacity (small hospitals only):
o Two licensed staff: RN, NP, or PA o Availability of either video or in-person consult with a
Palliative Care Physician
2. Palliative Care Capacity No Change.
3. Elective Delivery before 39 weeks Percent of patients with newborn deliveries at ≥ 37 to < 39 weeks gestation completed, where the delivery was elective.
Hospitals submit data to California Maternal Quality Care Collaborative (CMQCC), and PHC will work directly with CMQCC for reports.
3. Elective Delivery before 39 weeks No Change.
4. Exclusive Breast Milk Feeding
Hospitals submit data to California Maternal Quality Care Collaborative (CMQCC), and PHC will work directly with CMQCC for reports.
4. Exclusive Breast Milk Feeding Rate No Change.
82 of 86

2018-19 Small Hospitals Measures/Requirements Proposed 2019-20 Small Hospitals Measures/Requirements Change Rationale 5. Nulliparous, Term, Singleton, Vertex (NTSV) Cesarean Birth Rate
Hospitals submit data to California Maternal Quality Care Collaborative (CMQCC), and PHC will work directly with CMQCC for reports.
5. Nulliparous, Term, Singleton, Vertex (NTSV) Cesarean Birth Rate No Change.
6. California Hospital Patient Safety Organization (CHPSO) Patient Safety Organization Participation
• Small hospitals (< 50 licensed general acute beds): No change.
o Submit 50 events o Attend one Safe Table Forum
“Events” include near misses, unsafe conditions, and all levels of harm.
6. CHPSO Patient Safety Organization Participation No Change.
7. California Immunization Registry (CAIR) utilization measure Pay for reporting first year. To earn points for this measure, two steps must be met: 1. Join CAIR and provide CAIRID to PHC 2. Create a CAIR Utilization Policy for your hospital, and send to PHC
Remove. Replace with Pay for Performance Measure. Remove Pay for Reporting measure and replace with Pay for Performance measure.
8. Quality Improvement (QI) Capacity Part I: Summary of a QI training attended
• At least 2 staff members participate in an in-person, PHC-approved program or training (min. 4 CE/CME hours per person) aimed at improving one aspect of hospital quality.
Part II: Summary of a QI Project • Summarize one QI project taking place at your hospital. May
be unrelated to training from Part I.
7. Quality Improvement (QI) Capacity No Change.
83 of 86

2018-19 Small Hospitals Measures/Requirements Proposed 2019-20 Small Hospitals Measures/Requirements Change Rationale 8. Substance Abuse Bundle
Small Hospitals: Full Points= 2 components, Partial Points= 1 component Large Hospitals: Full Points= 3 components, Partial Points= 2 components i. Voluntary Inpatient Detox (VID): At least 5 patients (large hospital) or 2 patients (small hospital) admitted for VID. Due to billing lag, must be completed in first 9 months of the measurement year. PHC will obtain this data from the state. OR Hospital creates policy for VID. Policy must identify team members who will administer VID ii. Naloxone Fill/Distribution: 50% of patients admitted for opioid overdose or seen in ED with opioid overdose/intoxication have a filled prescription for Naloxone within 6 months of that hospitalization. PHC will use state data on carved out medications for numerator, and admissions diagnosis code for denominator. OR Hospitals submit to PHC a log detailing the amount of Naloxone they took in, and amount that was dispense during the measurement year. iii. Medication Assisted Treatment (MAT) in ED: At least 5 patients (large hospital) or 2 patients (small hospital) started on Medication Assisted Treatment (MAT) in the ED setting. This process entails screening patients on opioids who present in ED, switching appropriate patients to buprenorphine, and arranging follow up with outpatient provider. Screenings may be conducted by either trained in-house staff or a telemedicine provider (e.g. Bright Heart Health). PHC will use state claims data and outpatient provider data to validate hospital-reported information. iv. Medication Assisted Treatment (MAT) in inpatient setting: At least 5 patients (large hospital) or 2 patients (small hospital) started on Medication Assisted Treatment (MAT) in the inpatient setting. v. Support for Hospital Opioid Use Treatment (SHOUT) Hospital adopts Support for Hospital Opioid Use Treatment (SHOUT) program protocols in the ED/Inpatient setting.
Proposed New Measure. Opportunity to treat patients presenting in hospital for substance abuse.
84 of 86

2018-19 Small Hospitals Measures/Requirements Proposed 2019-20 Small Hospitals Measures/Requirements Change Rationale 9. Hep B Vaccination for Newborns, capture via CAIR
Rates of Hep B utilization and data capture are currently low. Use PHC delivery data for denominator, and CAIR data for numerator. Numerator: # of Hep B vaccinations in CAIR Denominator: # of deliveries
Proposed New Measure. Meets CAIR requirement from DHCS. This denominator would not take into account twins, triplets, etc., or births that were not live.
85 of 86

Eureka | Fairfield | Redding | Santa Rosa
CommunicareCase Study
1) Democratic QI culture. Everyone has a role. Functionally it is both centralized and decentralized. We have a central CQO and data team but also have a Preventive Care Coordinator role at each site.
2) Care teams. The care teams have ownership of their respective patient panels and know the patients. They know that Ms. Sanchez in the CRC denominator is visiting her family in Mexico. Mr. Jones is in the hospital. They call to make sure he has his creatinine checked given that he is on an ACE.
3) Data analytics. We have invested with RCHC in a data platform that allows for real‐time, comparative data reporting drilling down to the patient level. This gives access to information that can be used to drive results.
4) Leadership and focus on results. The QI culture at CommuniCare started before my tenure but has evolved. Without leadership and an attention to the importance of quality, we could not deliver the care that we do.
5) Bianca ‐ the new clinic manager who found that last colonoscopy.
86 of 86





























