Embed Size (px)
Citation preview

4/26/2018
1
Partnering for a “Quality Care Culture” to Reduce Avoidable Readmissions
Angela Booher, MAN, RN, CCM Director of Care Transitions Fairview Health Services
Fairview Readmission Goals
Fairview/UMMC Readmission Rates

4/26/2018
2
Definition of a Culture
According to Merriam Webster
the set of shared attitudes, values, goals, and practices
that characterizes an institution or organization a corporate
culture focused on the bottom line
https://www.merriam-webster.com/dictionary/culture

4/26/2018
3
Readmission Culture Planning Areas
Quality Culture• Standardized• Measurable• End-Product Goal• Adaptive Change• Takes a Villiage
Continuous Improvement
• Diet and Exercise
• Innovation• Metrics• Aligned
Communication
Patient Focused
• Listen Leading• Quality focused• Efficient• Individualized• Standardized Tools• Resources
How we “Focus” our Perspective Lens
Patient FocusedPatient
Focused
Quality not CostQuality
not Cost
EfficiencyEfficiency
Innovation Thinking
Innovation Thinking
TransitionsTransitionsMetricsMetrics
ToolsTools
Fairview Alignment of Goals
Readmissions
Length of Stay
Optimal Patient Experience/Care

4/26/2018
4
Patient Focused
Fairview Care ContinuumA “continuum” of nets and coaches to assist you when your health care needs make you feel as though you and your support system are walking a “tight rope” and risk falling
Balancing Pole: Advocacy and Autonomy tools and resources for your care to be tailored to your needs and wants
Ambulatory/Outpatient Support: Clinics, Outpatient Therapy,
Pharmacy, Community Services
Post Acute Facilities: Transitional Care Facilities, Long-Term Care, Assisted Living, Stay By The Day,
Group Home
Home Services Support: HOMECARE, Home Therapy, Social Worker Care Coordination, Lifeline,
Medication Support, Tele-health
Inpatient Support: Inpatient, Observation and Emergency Room
Goal of Partnership with aligned culture of patient and Healthcare Teams
1. Aligned communication
2. Improved Patient Experience
3. Improved Family Experience
4. Improved Staff Experience
5. Improved Collaboration of all key players
1. Decreased Hospitalization Admissions
2. Decreased length of stay for appropriate admissions
3. Decreased Costs
Goals
Measurable Outcomes

4/26/2018
5
Why Quality focus and not Cost?
14
Why do we want to decrease hospitalization Admissions and utilize Community More
Everyone always thinks it’s about Cost but it’s really about quality
Decreased Autonomy of
choicesDeconditioning
Post-Hospital Acute
Syndrome
Hospital Acquired
Conditions
Increased Costs to payers/ families/
Patient(s)
Halo Effect is Financial with optimized efficiency of a Quality perspective

4/26/2018
6
Why is Efficiency Important?
Readmission Bucket Lists
Discharge Planning
Medication Management
Transition Communications
Transition Care
Support
All work associated with coordination across
settings and making sure the plan of care once discharged is followed
All work associated with discharge planning and the process at a Health
Facility prior to the patient moving to their next level
of care
All work associated between communications
about the patients care between the sending and
receiving caregivers
All work associated with the patient understanding
the purpose of their medications and is taking
them appropriately
Patient and Family Engagement and Experience goal setting with the patient voice in all core processes
System Alignment• RAM Screening• Workflow Optimization & Alignment
Outlier Escalation Process

4/26/2018
7
Evidence Based Innovation and creating
Evidence based interventions (The feedback loop of
continuous improvement)
System Analysis of Readmission Workflow
Patient Admitted to
Hospital
Patient Discharges
Readmission within 30
days
RAM Risk (appropriate Interventional matrix
initiated)
RAM Risk (appropriate Interventional matrix
initiated)
Transition ConferenceTransition
ConferenceCommunication
Hand-offCommunication
Hand-off
Discharge Planning Tool
Discharge Planning Tool
Root Cause Analysis
Root Cause Analysis
Qualitative Analysis
Qualitative Analysis
QlikviewDashboard
QlikviewDashboard
Intranet Site
Intranet Site
RAM is a Screening Tool that guides Clinicians Drive Decision
• Only pulls discrete data from inpatient utilization history
• Clinical assessment should drive interventions
• Additional Consult reasons define Care Coordination populations

4/26/2018
8
Model Overview
Readmission Risk Screening with the Readmission Assessment Measure “RAM”
• The RAM is a logistic regression model that calculates a patient’s risk of readmission using:AgeLength of StayLocation
– North (Northland / Lakes / Range)
– South (Southdale / Ridges)
– UMMC
Acuity
– Through ED?
– Transfer?
Select admitting diagnoses
– High Risk Dx Group = Diseases of the Blood and Blood-forming Organs and Certain Disorders
– Elevated Risk Dx Group = Certain Infectious and Parasitic Diseases
Cancer Treatment?Birth?Hospital History (6-month)
– Inpatient
– ED
– Observation
Scoring Categories1-2% 30-day Risk
1-2% 90-day Risk
5-6% 30-day Risk
9-10% 90-day Risk
11-12% 30-day Risk
19-20% 90-day Risk
22-23% 30-day Risk
37-38% 90-day Risk
33-37% 30-day Risk
53-57% 90-day Risk
44-49% 30-day Risk
66-71% 90-day Risk
62-69% 30-day Risk
80-85% 90-day Risk
Extreme
High
Very High
Elevated
Average
Low
Very Low
• Define Workgroup Expectations of Care for each RAM category
• Create Communication Plan for implementation of new workflows
• Develop measurement strategy for appropriate interventions per category on outcome Readmission scores
• Develop and implement a efficient, standardized, patient friendly system-wide strategy, workflow and measurement plan that reduces avoidable readmissions to a Fairview hospital
Objectives Goal
Readmission Assessment Measure (RAM)

4/26/2018
9
Risk Screening and Standardizing Best Practice along the Continuum
Patient has an inpatient
Stay
Patient has an inpatient
Stay
R.A.M. category
assigned in EPIC
header
R.A.M. category
assigned in EPIC
header
Care Coordinator Assesses Risk for
elevated and up
Care Coordinator Assesses Risk for
elevated and up
Clinic Care Coordination – Primary /Specialty
Clinic Care Coordination – Primary /Specialty
HomecareHomecare
PharmacyPharmacy
Skilled Nursing FacilitiesSkilled Nursing Facilities
Primary CarePrimary Care
Geriatric ServicesGeriatric Services
Best Practice Protocol based
on Category initiated prior to
discharge
Best Practice Protocol based
on Category initiated prior to
discharge
Extreme Very High High Elevated
Inpatient
• Home Assessment within 24 hours
• Follow-up Appointment within 24 hours of discharge
• Transition Conference
• Home Assessment within 24-72 hours
• Follow-up Appointment within 24-72 hours of discharge
• Pharmacy MedicationReconciliation
• Follow-up within first week
• Care Transitions Assessment• Follow-up within first week to 10
days• Communication Hand-off• MTM appointment scheduled • Specialty Scheduled• Complex Barrier Assessment
completed
Clinic (Primary/ Specialty_
• PCP/Specialist conference with RNCC
• RN call patient 48-72 hours post discharge and initiate clinical pathway for patients:
• Transplant• Oncology• HF
• RN CC attends Drappointment with the patient.
• RN call patient 48-72 hours post discharge.• RN visit with patient for post-discharge for
care management within 7 days of discharge.
• Review diagnosis• Focused physical assessment• RN initiate clinical pathway for
patients with high risk diagnosis: • Update and review care team• Social Services consultation• Update and provide care plan
• RN call patient 48-72 hours post discharge
• Targeted education• Add patient to patient panel/list
with scheduled follow-up outreach (may be completed via phone)
• Office visit with provider within 14 days post discharge
Homecare
• Visits daily for first 3 days• Enlist assist from Manager to reschedule all patient cancelled visits, or
refused services• Patient Rounds with Care Team within first week • SOC within 24 hours• Include all identified Disciplines in POC SN, PT, OT, ST, SW and HHA• Targeted consistency with staffing • Reschedule all patient cancelled visits• Medication Management including MTM and Mediation set up • Initiate Telemonitor
• Frontload visits at least 3 visits in first 7 days• Falls risk interventions
including Lifeline• Add SW / Verify Caregiver
Support• Verify PCP/Specialty Appts.
made / transportation• Initiate Stoplight Tool• Assess for Rehosp. Risks not
included in RAM score
“Discharge Planning Tool” Goal of Work
More Efficient Communication on Key patient discharge information from all key stakeholders to all (Efficiency)
System wide standardized best practice documentation expectations from Health Care Team (Quality)
Advantages
Adaptive Change for System (not entity specific)
IT build and goal of not having duplicate documentation
Barriers

4/26/2018
10
Discharge Planning ToolTool built into Electronic Health Record to capture most updated information from Healthcare treatment team for discharge planning
•Patient plan for D/C•Current status•Barriers to retain to prior living situation/rationale for D/C recommendation•Recommendations for D/C•Summary from each Therapy Specialty
Therapy Services
•Prior authorization requirements/formulary•Restrictions (provider/pharmacy, etc.)•Drug follow-ups (INR checks, abx levels, etc.)•Home med/TCU recommendations•Adherence concerns – (cost, formulary, knowledge, additional education)
Pharmacy
•Accomplishments needed for discharge•In nursing shift notes•Barriers (1:1, Foley, Central lines, Wound Care, BM•Ride informationNursing
•Expected discharge to (home/TCU/***) in *** days or living arranged Once ***•Not clinically improved•Message enter required specific goals hereHospitalist
•Date of expected discharge (MD source of truth)/ time and mode of transportation•Disposition and services needed•Barriers (e.g.financial)•Where we are in the planning process
RN/SW Care Coordinator
Quarterly Quality Connections
Metrics/ToolsMetrics/Tools
ObjectivesObjectives
ScopeScope
MembershipMembership
SNF/TCU Team• Administrator• Director of Nursing• Nurse Manager• Admissions• Nurse Practitioner
As Needed:Therapy ServicesPharmacyMedical Director
Hospital Team• Director of Care Transitions• Manager of Care Transitions• Medical Director and others
as needed
• Quarterly Readmission• ED visits• Observation Stays• Referrals
• Length of Stay• Avoidable Days • Best Practices
• Goal Plans for identified work• Process Improvement Plans• Root cause analysis and trend identification• What is going well and what can be improved
g y
• Chart Audit Tool• Reports• Readmissions• Utilization• Referrals• Length of Stay

4/26/2018
11

4/26/2018
12
Transition Conferences
34
Criteria for Transition Conference
• RAM Very High, Extreme• Unplanned Readmission of 30 days based on patient choice or
adherence concerns from patient and family • Avoidable days attributed to family or patient decision making • Multiple co-morbidities that could contribute to Post Hospital
Syndrome and impact healing at home • Complex discharge plan with multiple agencies or departments
that is dependent on adherence to multiple interventions • Patient or family refusing key interventions at discharge for
achieving health goals (pt/family may or may not agree to the conference if they are refusing other key interventions – need to know why they are refusing first, etc.)
Transition Conferences
• Very High and Extreme Patients- Identified by the RAM
• Meeting to determine the patients discharge goals, the patients families discharge goals and the health care teams goals (How can we make the patients wishes a safe reality)
MD (as needed)
Bedside RN
CTS RN/SW
Patient/Family
Post Acute Providers
Primary MD/Clinic Coordinator
4/26/2018
13
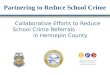
What is the difference between a
37
Care Conference and Transition Conference
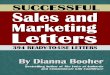
“Connect the Dots” SBAR Tool
• Prioritizes patient clinical need
• Standardized clinical assessment for all nurses
• Standardized clinical information provided to Providers
• Ease of Use for employee satisfaction
• Nurse brain to Doctor brain focus
• Decreased movement for patient
• Prioritizes patient clinical need
• Standardized clinical assessment for all nurses
• Standardized clinical information provided to Providers
• Ease of Use for employee satisfaction
• Nurse brain to Doctor brain focus
• Decreased movement for patient
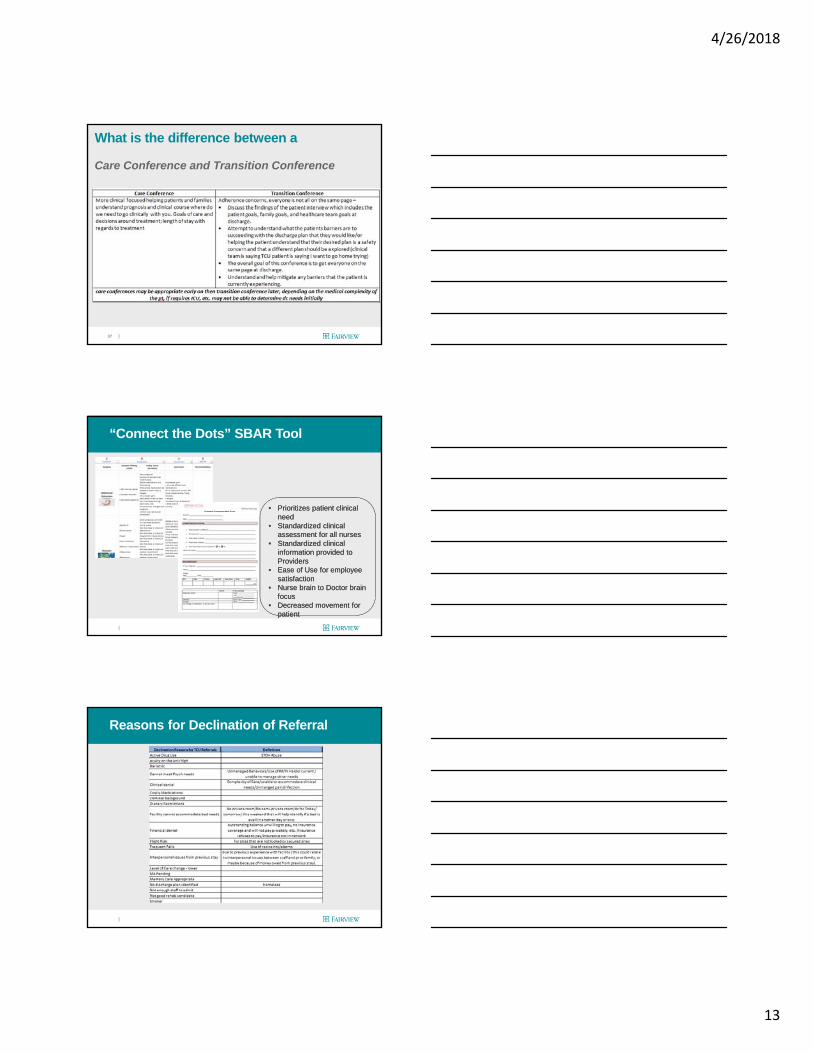
Reasons for Declination of Referral

4/26/2018
14
Level of Care Tool “Guide”
HomeHomeOutpatient ServicesOutpatient Services
HomecareHomecare
LTACHLTACH
ARCARC
SNF/TCUSNF/TCU
Discharge Disposition Guidelines
• Assess for impairments that may impact self-care
• Assess level of independence or if there is a willing and able caregiver
Home
• Same as Home• Assess need for skilled home
care services for assessment, treatment, monitoring or education
• Set expectation that home care services are temporary and intermittent while skilled need exists
• Discuss reason for need and goals of care to be achieved with care team and patient
Home Care• Skilled Nursing Facility • Outpatient or home care services unavailable or
inappropriate due to clinical complexity • Patient or caregiver unable to manage care that is a
change from their baseline level• Cognitive limitation without appropriate support
• Communication deficit prevents learning care tasks• Memory deficit prevents managing care tasks• Perception or processing deficit
• Physical Limitation• Physically unable to render care (e.g. obese, wound
location, contractures, unable to lift patient)• Lacks dexterity, motor strength, or skills required to
manage care• Co-morbidity prevents management of care (e.g.
blindness, paralysis)• Medical practitioner oversight at least 1 time per week• Nursing daily or skilled therapy 1-2 hours per day at
least 5 days per week
(SNF)
Process for Disposition Decision
Step 1Determine Medical Plan needed for discharge (goals and medical needs)
Step 2Assess Barriers to dischargeAssess ability to mitigate barriers
Step 3Determine appropriate disposition to meet plan and goals

4/26/2018
15
Top Twenty Readmission Initiatives
1. Readmission Assessment Measure (RAM) Risk Scoring2. Evidence Based Workflows across the continue for each risk category
• Homecare• Inpatient• Outpatient• Geriatric Services• Therapy Services• DME Services
3. Communication Hand-offs to next level of care providers4. Aligned Care Coordination across the system5. Post Follow-up Calls triaged for Risk6. Extended time Follow –up Primary Care or Specialty Visits7. Aligned System work group for continuous process improvement8. Transition Conferences and Care Conferences9. Community Paramedic Program10. Medical and Behavioral Health Home Models11. Patient Activation Measure (PAM) Assessments 12. System Evidence Based Educational Materials13. Data tools to identify Risk areas within system within 48 hours14. Readmission Best Practice Alert in EPIC15. Pharmacy Medication Reconciliation at discharge for high-risk patients16. Medication Therapy Management (MTM) appointments and counseling17. Skilled Nursing Care Quality Improvement Quarterly Meetings18. Geriatric Services Triage Line19. Evidence Based Chart Audits to trend for optimization20. Evidence Based Readmission Assessment Root Cause analysis tool and summary data reports for
optimized quality improvement
Transitions
Fairview Care Continuumanalogy of a relay race is suggested, where success is influenced by four factors: sequence, timing, baton-passing technique, and communication. These four factors are used as a framework for professionals assisting the patient and their support system along the care continuum
The Place in between passing the baton to another person is the Hand-off or Transitions time
For the pieces to be put together for the patient and their support system the hand-off participants must know what the expectations are and convey to one another and the patient and who they are
handing off next in the rely

4/26/2018
16
Inpatient enrolling Patient in Clinic Care Coordination
Patients attend Follow-up appointments for high-risk patients
Triage Risk
Triage Risk
Assess Patient
Activation
Assess Patient
Activation
Assess BarriersAssess Barriers
GoalsGoals
ScheduleSchedule
Work with FacilitiesWork with Facilities
Sell the appointment
Sell the appointment
Audit and Improve
Audit and Improve
• Lifeline
• Assisted Living w/o Services
• Assisted Living w/Services
• Group Home
• FMG• Primary Care• Geriatric
Services• Complex Team• Integrated
Team
• UMP
• FPA
• TCU
• Assisted Living
• Acute Rehab
• LTACH
• Homecare
• Hospice
• Independent Residence
• Tele-Monitoring
• Private Pay Services
• Senior Services
• Care Coordination
• Parish Nursing
• County
• External
Communication across the Continuum Hand-off

4/26/2018
17
Transition Communications
Next Steps:1. Define impact tracking
1. How do we measure1. Readmission Impact2. Value add to patient care3. How do we tie “key
recommendations” to plan of care goals and next levels of the continuum
4. What are the workflows from Receiving and sending staff with hand-offs
5. Formulate Work-groups
Primary Care/
Specialty
Primary Care/
Specialty
Care Coordination
Care Coordination
Geriatric ServicesGeriatric Services HomecareHomecare
TCUs/ LTACHs/
ARUs
TCUs/ LTACHs/
ARUsMTMMTM
Areas ImpactedAreas Impacted
Standard Communication Hand-off
Building a Communication Hand-in ToolFor patients with cognitive deficits
What is the patient's normal morning routine (early rises, sleep in,
assistance needed, time they eat meals etc)
What is the patient's normal evening routine
Preferred bathing routine
Favorites:snack, beverage, music,
location to sit, stuff animal or other security
blanket, etc
Does the patient typically get up at night?
How often? Times?
What are stress inducers for the
patient?
What tactics do you use to calm or what soothes the patient? Or if they have
paranoia or delusions what can distract them? What
helps the patient/client calm down.
Who is important in the patient's life - who can
help in stressful moment? maybe have a video clip or picture to
pull out.
What assist do they need with ambulation
or cares?

4/26/2018
18
“Heads Up” to Homecare
Metrics/Tools
Fairview Health Network Readmission Tools
Discharge Planning
Tool
Continuum Hand-offs
Dashboard Qlikview
Optimization Meetings/
Root Cause Analysis
Readmission Assessment
Measure “RAM”
prioritization workflows
Transition Conferences

4/26/2018
19
Readmission Dashboard
• Develop a scalable level approach that is both effective and sustainable
• Focus on Readmissions that are avoidable• Identify areas of improvement to the discrete
level
Goal
• Team approach• Rapid Performance Improvement focused• Just in Time data that is actionableStrategy
• Which interventions have the greatest impact?
• What is the best timing for interventions?• Where is the intervention needed?• Where are the gaps for the patient needs?
Questions to Answer
Mock – Up of Post Continuum Qlikview

4/26/2018
20
Patient Transitional Care Continuum Model (Patient Centered) {APPLES to APPLES data}
Hospital Post-Acute Clinic Homecare Hospice
Services Provided (Utilization)
Psychosocial Physical
SNF/TCU
LTACH
Assisted Living
Psychosocial Physical
Psychosocial PhysicalPsychosocial Physical
Psychosocial Physical
• Each box or point of service is a perspective and place of service to the patient with a short-term goal based on criteria that sent them to that point of care which that place is responsible for until they transition the patient to the next level of care based on gaps identified in the assessment and outcome data from the assessment
• Each point of service has an aligned assessment criteria to document and track that includes both psycho-social and physical components to assess and identify needed services and goals to achieve in each area (e.g. no support system – referral to clinic or homecare to work with patient to identify a support system)
• The development of criteria and aligned assessment criteria builds a walk-way between each of the silos in healthcare so the patient visits the appropriate area and understands when they are transitioning to the next area.
• Benefits to aligned assessments and standardized criteria
Long Term Goal is patient goal and determines different services along the continuum – each point of care has a short-term goal to determine graduation or need from one point of service to another
• Support system
• Payer• Living
situation• Future needs• Quality goals• Support
needs
• Ambulation• Medications• Chronic
Conditions• DME current• DME needed• Pain• Cognition
Examples of Assessment Metrics
SAME ASSESSMENT QUESTIONS ALONG EACH POINT IN THE CONTINUUM
Supplies in the Suitcase
Discharge on the Double Reports Metrics tracking
Quality Improvement Meetings Outlier Escalation Process/Avoidable Day Tracking Discharge Criteria Tool Tours (in person/virtual) Scripting Communication SBAR Tool Readmission Chart Reviews Community Resources Tracking Patient Needs Assessment for Utilization/Barriers Patient Choice (STARS, location, word of mouth,
expectation) System Standardization for metrics tracking and
efficiency
Packing List for Outcomes