Embed Size (px)
Citation preview

Partition of Coronary Flow and Cardiac OxygenExtraction Between Coronary Sinus andOther Coronary Drainage Channels
By Robert R. Lafontant, B.S., Harold Feinberg, Ph.D., andLouis N. Katz, M.D.
With the assistance of E. Boyd
• Coronary flow measurements in the intactanimal and in man have been based prin-cipally on the amount of the coronary sinusdrainage. Two assumptions are involved inthe use of the coronary sinus drainage asan index of total and of left ventricularcoronary flow: (1) The coronary sinus flowis a fixed percentage of total coronary flow,and (2) it represents all or a constant portionof the venous drainage of the left ventricle.Determination of the oxygen consumptionof the left ventricle also has been based onthe same assumptions, the calculation beingthe product of coronary sinus flow and thedifference in oxygen content between arterialand coronary sinus blood.
While there is some evidence favoring theseassumptions, there is still doubt as to theirabsolute validity. The present report is pri-marily concerned with an examination of theassumption that the coronary sinus representsa fixed percentage of the total coronary flow,although many of the observations bear on thesecond assumption as well. These assumptionswere tested with a modified coronary flowpreparation currently in use in this depart-ment.1 Appropriate alterations were made topermit analysis of the partition of total coro-nary drainage between the coronary sinus andthe extracoronary sinus pathways. The coro-nary flow partition between these two beds
From the Cardiovascular Institute, Michael ReeseHospital and Medical Center, Chicago, Illinois.
Supported by grants from the Chicago HeartAssociation and the National Heart Institute(H-2276).
Dr. Feinberg is an Established Investigator, Ameri-can Heart Association.
Received for publication January 30, 1962.
686
and the cardiac oxygen consumption valuesmeasured by each were investigated underseveral sets of circumstances.
MethodsMongrel dogs, 15 to 20 Kg., were anesthetized
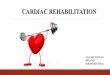
with intravenous sodium pentobarbital (30 mg./Kg.). The chest was opened in the fourth orfifth intercostal space and the animal placed onpositive pressure respiration, 95 per cent O2 and5 per cent CO2. The dogs were heparinized (15mg./Kg.), and a modified "coronary flow" prepa-ration was established (fig. 1). The left pulmo-nary artery was cannulated proximally and dis-tally. The proximal cannula drained the rightventricle; the distal one was used to perfuse theleft lung from a reservoir by means of a Maischpump. A cannula in the distal part of the rightpulmonary artery was also connected to the pumpto perfuse the right lung. The pump was adjustedto set the arterial blood pressure near its pre-operative level and was used to control and main-tain the amount of cardiac input.
The coronary sinus was then cannulated viathe right atrial appendage. A Morawitz typeglass cannula2 without the balloon tip was de-vised for the coronary sinus measurements. Thecannula was tied in place by a ligature passedaround the outside of the coronary7 sinus andsecured around the cannula lip at the level ofthe coronary ostium. The coronary sinus blooddrained into an auxiliary reservoir. In this way,the only blood entering the right ventricle wasthat draining the coronary tree other than via thecoronary7 sinus, the so-called extra-coronary-sinusblood flow. It consisted mainly of the blood fromthe anterior cardiac and thebesian veins (exceptfor the 10 per cent or less draining into the leftheart3). In this manner, the partition of coronaryflow into coronary sinus and extra-coronary-sinuschannels was established.
The vena cavae were eatheterized in order todeflect the systemic venous return from the rightatrium to the main reservoir. To accomplish thisdeflection, the vena cavae were tied between theheart and the catheters, and the azygos vein
Circulation Research, Volume XI, October 1962
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

PARTITION OF CORONARY FLOW 687
was ligated after the cut pericardium wasrepaired.
Arterial blood pressure was controlled by aballoon catheter in the thoracic aorta. Heart ratewas varied by an artificial pacemaker attachedto the junction of the right atrium and ventricle4
and monitored in lead II of the electrocardiogram.The left ventricle ordinarily had an approxi-
mately normal after-load, while the right ven-tricle was hypodynamic, receiving onty the extra-eoronary-sinus blood and being continuously keptas empty as possible by siphonage, which in turnkept the mean pressure in the right ventricleclose to zero.
Both coronary sinus and extra-coronar\T-sinusflows were observed at fixed intervals, and atthe same time, arterial, coronary sinus, and extra-coronary-sinus blood samples were taken andsystemic blood pressure and heart rate recorded.Oxygen content was routinely measured spectro-photometrieally5 and cheeked from time to timeby the Van Slyke manometrie method. Experi-ments which showed arterial O2 content below16 vol. per cent were discarded.
At autopsy, it was demonstrated that thecoronary sinus eannula was in place and securelytied, did not kink the sinus channel, and drainedall of the branches visible (in a good light)entering the coronary sinus near the ostium.Experiments in which the cannulation and liga-tion of the coronary sinus were unsatisfactorywere discarded.
In some experiments, the work of the rightventricle, which otherwise was hypodynamie, wasbrought into the normal range or above it byintroducing a thin, slack, latex balloon attachedto a catheter into the right ventricle via onearm of a wide-bore (1 cm.) Y tube placed inthe main pulmonary artery. Pressure from theballoon cavity was recorded with a strain gaugeby means of this catheter. The second arm ofthe Y tube was used as a siphon to drain thecavity of the right heart outside the balloon ofextra-coronary-sinus blood flowing into it. Theballoon was filled with known amounts of fluidto make the right ventricle either normallydynamic (mean intracavity pressure above 0 andup to 25 mm. Hg) or hyperdynamic (mean pres-sure above 25 mm. Hg). The small elastic com-pression contributed by the balloon itself, asdetermined by inflation of the balloon outsidethe heart, in no instance exceeded 10 mm. Hg.This was subtracted from the pressure recordedin the balloon during the experiment in orderto obtain the compression contributed by the rightventricular wall. After completing the experimentin three of the animals, the coronary tree wasinjected according to a slightly modified Schle-
Circulation Research. Volume XI, October 1902
ECS-FLOW
FIGURE 1
A schematic representation of the hypodynamicright ventricular preparation. ESC is the extra-coronary-sinus and CS the coronary sinus drainageconnected to a special eannula in the coronarysinus; S.V.C. and I.V.G. are the superior andinferior vena cavae; RL and LL are right andleft lungs; RA and LA a>re right and left atria;RV and LV are right and left ventricles; PA isthe main pulmonary artery; CA indicates thecoronary artery ostia. Discussed in text.
singer technique.0 The distribution of dye foundwas similar to that previously obtained in thisdepartment in normal hearts.7
ResultsIn this study, the effects of several kinds
of procedures were analyzed: (1) The rightventricle was permitted to operate in a hypo-dynamic fashion while the balloon in thethoracic aorta was inflated in alternate peri-ods. (2) The right ventricle was changedfrom a hypodynamic to a normally dynamicand hyperdynamic state, both in the presenceand absence of aortic balloon inflation. (3)With the right ventricle dynamic, the heart
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

688 LAFONTANT, FEINBERG, KATZ
TABLE 1
Summary of Data on Effect of Change in Effort of Left Ventricle When the flightVentricle Was Hypodyncnnic"
Normal BP—control Raised BP
Xumber of experimentsBP (mm. Hg)HE (beats/min.)HR • B P X 10"Arterial O» content (vol. %)CS 0= content (vol. %)ECS O» content (vol. %)CS A-V O2 difference (vol. %)ECS A-V O2 difference (vol. %)CS O»C (cc./min./lOO Gm. HW)ECS 02C (ce./min./lOO Gm. HW)CS O2 extraction (%)ECS O» extraction (%)CS flow (cc./min./lOO Gm. HW)ECS flow (cc./mhi./lOO Gm. HW)Total CF (cc./nmi./lOO Gm. HW)
1860.4 ±
129.8 ±7.8 ±
19.0 ±3.8 ±4.8 ±
15.2 ±14.1 ±
3.8 ±2.3 ±
80.0 ±74.7 ±30.7 ±20.4 ±51.1 ±
22.416.92.82.93.02.83.23.81.7] . l
11.211.211.7
8.819.7
18110.0 ± 32.4t]18.5 ± 15.412.7 ± 2.6t19.5 ± 2.68.0 ± 2.9t
11.6 ± 2.8t11.5 ± 3.217.8 ± 2.8t5.1 ± 1.3t2.1 ± 0.5
58.9 ± 14.3140.3 ± 12.8t58.6 ± 20.4t39.3 ± 16.4t96.0 ± 33.0t
*Each value given is a mean value of the number of experiments listed with the standarddeviation, f indicates a statistically significant change (p = <0.05) with respect to thecontrol values.
CS = coronary sinus; ECS = extra-coronary-sinus drainage; HW = heart weight; BP =mean aortic blood pressure; HR = heart rate; O2C = oxygen consumption; CF = coronaryflow.
was accelerated with the electric pacemakerin alternate periods. In this same series,Z-epinephrine was injected (4 /xg./min. overa period of three to four minutes in twodogs and 1,000 /xg. in less than one minutein another dog; the animals weighed from16 to 19 Kg.) into the tubing leading to thelungs. Spontaneous tachycardia which devel-oped in two dogs was also analyzed.
In all, 18 dogs were used, with multipleprocedures carried out in some of them. Theeffect of changing left ventricular effort wasstudied in 13 (nine with a hypodynamic andfour with a dynamic right ventricle) ; thealteration of right ventricular effort in four;the effect of Z-epinephrine in three; and theeffect of induced heart rate changes in five.Spontaneous tachycardia occurred in twodogs. The results are summarized in tables1 to 6.
1. CORONARY FLOW (CF)
Increasing the effort of the right ventricleby inflating the balloon in its cavity ledto an augmentation of total coronary flow
(table 3), but the change was not statisticallysignificant. Except for the lack of significance,this observation agrees with the results ofGregg et al.8 in a preparation measuringtotal coronary inflow. Increasing the effortof the right ventricle also led to an increasein coronary sinus (CS) drainage flow (table3), but again this was not statistically sig-nificant. Such an increase has been shownpreviously by Gregg et al.,8 Geller et al.,9
and in this department.10 A more significantincrease in the drainage by the extra-coro-nary-sinus channels (ECS) was also evident(table 3), with the difference between thehyper- and hypodynamic right ventriclesbeing significant.
Increasing the aortic blood pressure (BP)caused total coronary flow (CF) to increasesignificantly (tables 1 and 2). This increasewas associated with an increase in both theCS and ECS flows (tables 1 and 2), thechanges being statistically significant.
When total CF and the CS and ECS flowsof each of the individual experiments were
Circulation Research, Volume XI, October 1962
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

PARTITION Or CORONARY FLOW 689
FIGURE 2
The effect of induced heart rate increase on therelationship of total coronary (A), CS (B), andECS (C) floivs to the HB'BP index in ninesets of observations in five dogs. The right ventriclein each of these animals was dynamic. Coupledobservations of the relationships before and afterthe increase in heart rate are shown by the individ-ual solid lines. The mean aortic pressure remainedfairly constant within ±5 mm. Hg. The dashedlines represent the mean slope of all the observa-tions. Discussed in text.
plotted in relation to the effort index, heartrate times blood pressure (HR • BP), agood correlation was found to exist in thehypodynamic right heart experiments, as wasshown for total coronary flow in previousdepartmental studies.1'n Apparently, then,not only total but the two fractions of coro-nary flow measured are related to the heartrate-blood pressure index of the induced leftventricular effort.
The effect of changes in heart rate on totalCF were similar to the observations ofLaurent et al.4 that total CF increases as theheart rate increases (table 4). HR accelera-tion also augments the CS and ECS flowssignificantly (table 4). The dependency oftotal CF and the CS and ECS flows uponthe HR • BP index was confirmed (fig. 2).
In spontaneous tachycardia, an increase intotal CF and in CS and ECS flow accom-panied the change in heart rate (table 5).The above changes were not so dramatic asthose induced by the exhibition of Z-epineph-rine in which the classic effect12 occurred,namely, a large increase in total CF, of which
Circulation Retearch, Volume XI. October 1961
CS FLOW% TOTAL
lOOr
75
50
25
FIGURE 3
A graph representing the influence of spontaneoustachycardia and exhibition of l-epinephrine on thepercentage of total coronary flow drained by thecoronary sinus. In each column, the box showsthe standard deviation from the mean, the hori-zontal line within it represents the mean value,and the vertical line joins the maximum and mini-mum values noted. Discussed in text.
the CS component increase was much largerthan the ECS (table 6). While no plotof the individual observations against theITR • BP index was made, it is apparentfrom the means shown in table 5 that the
—1occt—zoo
EOU
TAN
PON
en
!DIA
fCA
R
i -
o
zoo
UJz
ii
-EP
I
XH
I
_l Ul
CS flowt h e
ECS flowIIR-BP ' t h e H R - B P ' a iKl t h e I I R - B Pratios were much different after /-epinephrinefrom those before, as we have shown pre-viously for total CF.12
From the foregoing data, it was possibleto compute the percentage distribution oftotal coronary drainage between the CS andECS. This distribution was found to bevariable. In a single dog, the CS flow variedfrom 52 to 70 per cent of the total CF.The range of CS flow observed in all theanimals was from 49 to 74 per cent of thetotal CF, while the range for ECS was from26 to 51 per cent of the total. The scatteris far too wide to represent experimentalerrors in measurement. On the other hand,
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

690 LAFONTANT, FEINBERG, KATZ
TABLE 2
Summary of Data on Effect of Change in Effort of Left Ventricle When the RightVentricle Was Dynamic*
Number of observationsBP (mm. Hg)HE (beats/min.)HR • BP X 10J
Arterial O» content (vol. %)CS 02 content (vol. %)ECS O2 content (vol. %)CS A-V O2 difference (vol. %)ECS A-V O2 difference (vol. %)CS 0=C (cc./min./lOO Gm. HW)ECS 02C (cc./min./lOO Gm. HW)CS 02 extraction (%)ECS 02 extraction (%)CS flow (cc./min./lOO Gm. HW)ECS flow (cc./min./lOO Gm. HW)Total CF (cc./min./lOO Gm. HW)EVP (mm. Hg)HE. • EVP X 10J
Normal BP—control
1860.1 ± 6.3
158.1 ± 25.510.1 ± 3.622.1 ± 1.87.4 ± 2.69.1 ± 3.4
14.8 ± 2.111.2 ± 3.44.3 ± 1.42.4 ± 0.4
65.5 ± 12.458.9 ± 12.439.3 ± 12.325.7 ± 3.564.7 ± 14.912.1 ± 0.43.0 ± 2.0
Raised BP
8131.9 ± 36.5t153.3 ± 33.118.0 ± 3.4t23.4 ± 0.833.1 ± 4.2t15.0 ± 5.310.3 ± 3.5t8.4 ± 3.66.5 ± 2.3t3.0 ± 0.9
44.4 ± 14.536.3 ± 19.598.5 ± 23.4t54.0 ± 12.8t
152.4 ± 31.0t10.3 ± 4.51.6 ± 0.9
*Each value given is a mean value of the number of observations listed with the standarddeviation, t indicates a significant change with respect to the control (at p = <0.05).
RVP = mean right ventricular pressure; observations is the number of observations madeunder each state in experiments in which they were compared. For other abbreviations,refer to footnotes of table 1.
the means of all observations in a givenanimal and over the whole study were fairlyconsistent in showing that approximately 60per cent of total CF is drained by the coro-nary sinus. This mean is in accordance withthe report of Anrep.13
The following maneuvers, of those studied,had noticeable effects on the partition pattern:(1) augmentation of aortic resistance whenthe right ventricle is dynamic; (2) inductionof heart rate changes either spontaneously orby external pacemaker (fig. 3); (3) exhibitionof Z-epinephrine (fig. 3). In the latter case,the CS flow fraction shifted from 59.3 ± 6per cent of total CF to 70.9 ± 3 per cent.
The validity of the coronary sinus methodof measuring coronary floiv: The reliabilityof coronary sinus outflow as an index to leftventricular coronary perfusion depends onthe constancy of the coronary sinus flow tototal coronary flow. While overall the coro-nary sinus was found to drain 60 per centof total coronary flow, noticeable deviations
were encountered in all experiments, mostmarked during spontaneous tachycardia andi-epinephrine exhibition. These latter effectsare significant since it is now established thatin the conscious, closed-chest dog14 and inman, most of the cardiac adjustments to stressare met primarily by increases in the lieartrate and by inotropic stimulation involvingeatecholamines.
Anrep13 was among the early workers whoconcluded that the coronary sinus representeda fixed percentage of the total venous outflowin the heart-lung preparation. There havebeen other studies since then, however, show-ing even greater variations than those foundby us. Thus, Katz et al.10> 15 showed thatthere was an even wider variability of thepercentage of total coronary inflow drainedby the coronary sinus under the conditionsof their experiments. Similarly, the studiesof Wearn16 in man do not warrant the ideaof a fixed flow portion going to the coronarysinus. Geller et al.9 and Johnson and Wig-
Circulation Research, Volume XI, October 1962
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

PARTITION OF CORONARY FLOW 691
TABLE 3
Summary of Data on Effect of Changes in Effort of Eight Ventricle*
Number of observationsBP (mm. Hg)HE, (beats/min.)HB • BP X 10"3
Arterial O2 content (vol. %)CS O2 content (vol. %)ECS O2 content (vol. %)CS A-V O2 difference (vol. %)ECS A-V O2 difference (vol. %)CS O2C (cc./min./lOO Gm. HW)ECS O2C (cc./min./lOO Gm. HW)CS O2 extraction {%)ECS O» extraction (%)CS flow (ce./min./lOO Gm. HW)ECS flow (ce./min./lOO Gm. HW)Total CF (cc./min./lOO Gm. HW)RVP (mm. Hg)HR • RVP X 10J
Hypodynamicright ventricle
466.8 ±
152.5 ±10.3 ±20.5 ±6.2 ±7.7 ±
14.2 ±12.7 ±
3.7 ±2.1 ±
69.8 ±61.0 ±36.0 ±22.3 ±58.3 ±
o§o§
7.933.0
2.63.12.33.92.01.51.20.57.8
20.515.0
5.317.8
Dynamicright ventricle
60.1158.110.122.1
7.49.1
14.811.2
4.32.4
65.558.339.325.764.712.13.0
18± 6.31± 25.5± 3.6t± 1.8± 2.6± 3.4± 2.1± 3.4± 1.4± 0.4± 12.4± 12.4± 12.3± 3.5± 14.9± 0.4+± 2.0t
Hyperdynamicright ventricle
68.9172.712.322.3
6.26.6
16.011.8
6.03.4
71.971.047.927.975.936.54.8
9± 12.1± 46.lt± 5.1± 2.2± 1.5± 2.9± 1.2± 1.3t± 3.2± O.lt± 4.4± 11.0± 28.3± 5.1t± 29.7± 7.31± 3.0J
*Each value given is a mean value of the number of observations listed with the standarddeviation, t indicates a significant change with respect to the data given in first columnonly; t indicates a significant change with respect to both the first and second columns,each significant at p = <0.05; § indicates that the value zero is asumed.
For abbreviations, refer to footnotes of tables 1 and 2.
gers,17 on the basis of their observations, havechallenged the validity of using the coronarysinus in the assessment of total coronary flow.
There are limits, therefore, to the use ofcoronary sinus drainage as an index of totalcoronary flow when the performance of theheart deviates more and more from the normalor when the heart is diseased.
. . , „ coronary sinus flowThis variability of the ———;— 3 —
total coronary nowratio raises the question of the reliabilityof coronary sinus flow as an index of leftventricular coronary perfusion. The relia-bility depends on the assumption that thereis either no contribution of blood from theright ventricular coronary perfusion to thecoronary sinus or that the contribution fromthis source is fixed. Also, this assumptionrequires that none of the blood entering theleft coronary artery perfuses the right ven-tricle, or that a fixed and predictable amountis shunted to its perfusion. Obviously, eitherof these assumptions requires that a complexmixing from the two sides of the coronaryarterial tree occur in an unvarying fashion.Circulation Research, Volume XI, October lies
Since the early work of Anrep,13 it hasbeen held that the coronary sinus venousblood received contributions from both maincoronary trunks, although the amount comingfrom the left side constitutes the largest por-tion. Thus, Anrep demonstrated that the leftcircumflex contributed 70 per cent of its flowto the coronary sinus, the left descendens64 per cent, and the right coronary about37 per cent of its flow. Katz et al.,13 however,found considerable variability in the venousdrainage from these three coronary arteriesunder the conditions of their experiments.With the advent of cardiac catheterizationand the use of the coronary sinus as an indexof the left ventricular coronary flow, studieswere conducted which showed that 73 to 89per cent of the left coronary artery inflow18
was drained by the coronary sinus. A morerecent analysis showed a still greater range,71 to 92 per cent, with the range in 82 percent of the cases falling between 76 and87 per cent.19 When a right heart bypasswas added, the variation of the percentageof the left coronary artery inflow drained
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

692 LAFONTANT, FEINBERG, KATZ
TABLE 4
Summary of Data on Effect of Induced Changes in Heart Rate When the RightVentricle Was Dynamic0
Number of experimentsBP (mm. Hg)HE (beats/min.)HE • BP X 10-1
Arterial O2 content (vol. %)CS' O2 content (vol. %)ECS 0= content (vol. %)CS A-V O2 difference (vol.ECS A-V O2 difference (vol.CS 02C (cc./min./lOO Gm.ECS 0»C (cc./min./lOO Gin.CS Os extraction (%)ECS O2 extraction (%)CS flow (cc./min./lOO Gm.ECS flow (cc./min./lOO GmTotal CF (ce./min./lOO Gm.KVP (mm. Hg)HE • RVP X 10J
% )%)
H W )H W )
H W ). HW)HW)
Control
] 0
69.6 ± 20.2129.1 i t 25.1
8.9 ± 3.120.6 ± 2.35.5 i t 2.56.0 ± 2.9
15.1 i t 2.814.6 i t 2.6
3.6 i t 0.72.1 ± 0.6
73.6 ± 12.071.2 i t 12.934.1 i t 6.220.9 i t 3.955.0 i t 9.212.0 ± 6.42.0 i t 0.5
Heart rateincreased
1071.9 ± 19.1
171.0 i t 19.7112.5 ± 3.7t20.1 i t 2.34.6 i t 2.816.0 ± 2.8
14.4 i t 2.814.3 ± 2.15.0 i t 0.813.5 i t 1.2)
76.0 i t 12.372.1 ± 14.246.8 i t 10.7)35.5 ± 11.8t82.3 ± 9.3t21.0 ± 4.53.8 ± 0.8
*Each value given is a mean value of the number of experiments listed with the standarddeviation, t indicates a significant change (p = <0.05) with respect to the control.
For abbreviations, refer to footnotes of tables 1 and 2.
via the coronary sinus was increased further.19
It must be clearly recognized that leftand right coronary artery inflows are notsynonymous with left and right ventricularcoronary perfusions. Some data obtained inthe present experiments bear on this pointsince our studies dealt with the relation ofthe partition of coronary drainage to varia-tions in the performance of each of the twoventricles. Increasing the effort of the rightventricle results primarily in an increasein extra-coronary-sinus drainage without af-fecting coronary sinus drainage. Apparently,the coronary vessels from the right ventricle,under the conditions of our experiments, con-tributed little to the coronary sinus drainage.On the other hand, increase of the left ven-tricular effort resulted in an increase in bothcoronary sinus flow and extra-coronary-sinusflow, more or less proportional on the whole.
Several factors may explain the wide devi-ations from the mean of 60 per cent of totalcoronary flow drained via the coronary sinus.Anatomical studies have documented the im-portant territorial overlap between the two
main coronary arteries.20 This is the case inthe area of the interventricular septum, bothanteriorly and posteriorly.
The application to man of data from thedog is an extrapolation. For instance, whilethe coronary arterial circulation in dogs showsleft arterial inflow dominance in 50 per centof cases, in the human heart, right predomi-nance prevails in about 40 per cent of theeases, with left predominance in 20 per centand a balanced ratio between the two in 34per cent.20
The data obtained in the healthy heartmay not apply to the diseased heart. Forexample, there is evidence of the presence ofcollateral channels in the myocardium.6' 21~23
These communications, which may be usedonly to a limited extent in the normal heart,appear to proliferate and become functionallysignificant in abnormal hearts.3' "• 22~20 Thiseffect, obviously, could alter the coronarydrainage pattern of such hearts.
While no better method than the coronarysinus catheterization has yet been developedas an index of coronary flow in the intact
Circulation Research, Volume XI, October 1962
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

PARTITION OF CORONARY FLOW 693
TABLE 5
Summary of Data on Effect of Spontaneous Tachycardia When the Right VentricleWas Dynamic"
Number of observationsBP (mm. Hg)HR (beats/min.)HR • BP X 10 *Arterial O» content (vol. %)CS O» content (vol. %)ECS O2 content (vol. %)CS A-V 0, difference (vol. %)ECS A-V O2 difference (vol. %)CS O»C (ee./min./lOO Gm. HW)ECS O2C (cc./min./lOO Gm. HW)CS O2 extraction (%)ECS O2 extraction (%)CS flow (ec./min./lOO Gm. HW)ECS flow (cc./min./lOO Gm. HW)Total CF (cc./min./lOO Gm. HW)RVP (mm. Hg)HR • RVP X lO"3
Control
549.2 ±
160.0 ±7.9 ±
21.1 ±6.8 ±7.1 ±
14.3 ±6.7 ±3.7 ±2.7 ±
67.7 ±66.4 ±40.0 ±28.9 ±68.9 ±10.6 ±1.7 ±
1.110.01.90.32.22.72.41.11.00.3
10.913.44.05.09.22.51.0
Spontaneoustachycardia
257.5 ±
195.0 ±11.2 ±21. J ±6.1 ±6.7 ±
15.5 ±12.6 ±6.0 ±5.3 ±
71.7 ±69.0 ±60.0 ±54.5 ±
114.5 ±17.5 ±3.4 ±
10.67.11.60.20.50.90.42.71.00.72.33.18.54.9
13.410.6
2.0
*Each value given is a mean value of the number of observations listed with the standarddeviation. Tests of significance were not made.
For abbreviations, refer to footnotes of tables 1 and 2.
dog (without extensive surgery) or in man,it should be borne in mind that there areinadequacies in its use. These depend on thevariability of the coronary distribution onboth the arterial and venous sides.
2. OXYGEN CONSUMPTION (O2C)OF THE HEART
In previous experiments,27 O2C has beencalculated as the product of CP and thearteriovenous O2 difference across the totalcoronary bed. If the venous O2 of the CSand ECS drainage channels differs consider-ably, as the work of Moe and Visscher28
suggests, this difference would introduceanother source of error when using thecoronary sinus method as an index of totalmyocardial or left ventricular oxygen con-sumption. This possible source of error wasexamined in the present experiments.
A. The CS and ECS Venous O2 Leveland A-V O2 Difference
Arterial Oo content in these preparationsvaried little in a given experiment (the hy-poxemic preparations having been discarded),by no more than 2.5 vol. per cent during
Circuiatior. Research, Volume XI, October 1902
any experiment on any one dog. The changesin coronary venous Oo, of necessity, variedproportionately but in an inverse fashionwith the arteriovenous oxygen difference. Con-sequently, the discussion will be confined tothe level of Oo in the two venous drainagepathways. The actual data are given as meansin tables 1 to 6.
The CS Oa content differed markedly fromthat in the ECS channels both for individualsets of determinations and for mean values(tables 1 to 6). By and large, CS O2 waslower than ECS O2, indicating a greaterextraction in the former. However, there wereexceptions.
Venous Oo content rose in both drainagechannels when aortic pressure was elevated(tables 1 and 2). Changes in the effort ofthe right ventricle were without effect (table3). With increase in heart rate, only the CSvenous Oo fell (table 4). The exhibition of/-epinephrine produced a striking rise in theO2 content of both channels from 5.6 to18.9 vol. per cent in CS and from 7.7 to17.6 in ECS (table 6).
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

694 LATONTANT, FBINBEEG, KATZ
TOTAL 0 2 C/STROKE(CC/IOOGM HW)
06 r „
04
02
0
oa
aooo
CS O2 C/STROKE(CC/IOO GM HW)
04
02
B
flA
ECS 02C/STROKE(CC/IOOGM HW)
02
0
0°. 90
10 20
RVP
30 40
(MM HG)
50 60
FIGURE 4
The relation between the mean pressure in theright ventricle (MVP) and the total cardiac oxy-gen consumption (020) per stroke (A), thatmeasured by the coronary sinus (S), and that•measured by the extra-coronary-sinus channels (C).Each point represents a separate observation.Discussed in text.
B. Variations of O2CIn these experiments, O2C was calculated
for each of the two venous drainage beds,CS and ECS, by multiplying the flow fromeach bed by the A-V 02 difference existingin each. The mean CS 02C and ECS 02Cfound under different circumstances are givenin tables 1 to 6.
Increasing right ventricular effort causeda small increase of ECS 02C and CS 02C,but only the latter was significant (table 3).This increase is also suggested in a differentway in figure 4 where the average 02C perstroke is plotted against mean right ventricu-lar pressure.
5 e8
l
HYPERDYNAMIC
DYNAMIC
HYPOOYNAMIC
6 8 10
HR-BP-tO'3
16
FIGURE 5
The relation of total cardiac oxygen consumptionto the cardiac effort index HB'BP is shown inthree separate regressions. The line of leaist sloperepresents the observations made in eight dogswith a hypodynamic right ventricle. The line ofintermediate slope represents the observations infour dogs with a normally dynamic right ventricle.The line of greatest slope represents the obser-vations in two of these four dogs with a hyper-dynamic right ventricle. No change in aorticresistance occurred while the right ventricularperformance ivas increased in these latter fourdogs. Discussed in text.
Figure 5 shows this effect in still anotherway. It represents the regression of total02C on HR • BP for the three states of theright ventricle analyzed: the hypodynamic,dynamic, and hyperdynamic. It shows thatthe regression line shifted upward towarda greater total 02C when the right ventricleeffort increased. This shift indicates one ofthe defects of an effort index, like theHR • BP index we have employed1' n whichis based on the performance of the left ven-tricle, namely, that it overlooks the smallinfluence of a changing performance of theright heart. At the same time, there is evi-dence in figure 5 of an increase in slope ofthe regression line as the right ventricle be-comes lryperdynamic.
Increasing left ventricular effort by elevat-ing systemic arterial blood pressure has amore noticeable effect than increase in effortof the right. With the right ventricle hypo-dynamic (table 1), only the CS 02C showeda significant rise when the left ventriculareffort was increased, ECS being unchanged.
Circulation Research, Volume XI, October 1961
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

PARTITION OF CORONARY FLOW 695
This was also the case when the right ven-tricle was dynamic (table 2).
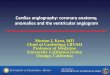
When all of the data obtained in theexperiments with a hypodynamic right ven-tricle were plotted as a scattergram againstHE. • BP, the observed total O2C data showeda different correlation from that of O2C cal-culated by multiplying CS O2C by 5/3 (fig.6). A similar deduction was derived in theexperiments dealing with the dynamic rightventricle.
CS and ECS O2C increased significantlywith an induced increase in heart rate (table4), and hence, so did total O2C. This increasealso occurred when spontaneous tachycardiadeveloped (table 5). Exhibition of Z-epineph-rine also raised the CS O2C and ECS O2C(and total O2C) in a striking fashion (table6).
C. Validity of the Coronary Sinus Methodof Measuring Myocardial OxygenConsumption
In line with the arguments regarding mix-ing of coronary blood flow discussed above,it is difficult to ascribe the resultant cardiacoxygen consumption data computed from thecoronary sinus and extra-coronary-sinus drain-age channels as representing, respectively,the distinct and independent influence of theleft and right ventricles. This difficulty isshown by the fact that while there is acorrelation between oxygen consumption com-puted from the coronary sinus drainage andthe effort index, HR 'BP , applicable to theleft ventricle, an increase in the effort ofthe left ventricle also resulted in a smallbut measurable increase in oxygen consump-tion computed from the extra-coronary-sinusdrainage channels. That the variability in thepartition of the calculated oxygen consump-tion is greater than that of coronary flowbetween the two drainage channel systemsis due to the greater variability between thetwo systems in the amount of oxygen extrac-tion. Because of this variability, the oxygenconsumption computed from the coronarysinus cannot adequately represent the totaloxygen consumption of the heart or, forthat matter, that of the left ventricle (see
COMPARATIVE DATA FOR TOTAL OXYGEN CONSUMPTION
I. ARROWHEADS SHOW ACTUAL VALUES.
2 POINTS SHOW CALCULATED VALUES.
161
12
40 60 120 160 ZOO
HR • BP « IO"Z
240
FIGURE 6
The graph shows the difference between calculatedand observed individual values of total cardiacOSG in 18 dogs with hypodynamic right ventriclesplotted against the HR'BP index. In these ani-mals, the systemic arterial pressure was varied.The calculated total cardiac 02C xvas obtainedby multiplying the individual CS OeC by 5/3.Discussed in text.
above). This statement is particularly truewhen heart rate changes or when Z-epineph-rine is exhibited and would apply also underabnormal conditions of the heart for thereasons given above.
While no better method than the coronarysinus catheterization has yet been developedto compute the oxygen metabolism of theleft ventricle in the closed-chest animal (with-out extensive surgery) or in man, it shouldbe kept in mind that this method is notcompletely reliable in assessing the oxygenconsumed by the whole heart or by the left
Circulation Research, Volume XI, October 196S
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

696 LAFONTANT, FEINBEEG, KATZ
TABLE 6
Summary of Data on Effect of Exhibition of l-Epinephrine When the Right VentricleWas Dynamic*
Number of experimentsBP (mm. Hg)HR (beats/min.)HE • BP X 10"3
Arterial O» content (vol. %)CS 0= content (vol. %)ECS 02 conteiit (vol. %)CS A-V 02 difference (vol. %)ECS A-V 02 difference (vol. %)CS 02C (cc./min./lOO Gm. HW)ECS 02C (cc./min./lOO Gm. HW)CS 02 extraction (%)ECS 02 extraction (%)CS flow (cc./min./lOO Gm. HW)ECS flow (cc./min./lOO Gm. HW)Total CF (ce./min./lOO Gm. HW)RVP (mm. Hg)HR • RVP X W
Control
364.0 ± 5.3
163.3 ± 5.810.4 ± 0.723.4 ± 1.15.6 ± 1.17.7 ± 1.1
17.8 ± 2.115.7 ± 2.13.6 ± 0.32.2 ± 0.6
75.9 ± 5.866.1 ± 7.131.3 ± 1.222.0 ± 6.053.3 ± 7.011.3 ± 6.41.8 ± 1.0
i-Epinephrineexhibited
3160.0 ±180.0 ±28.8 ±24.4 ±18.9 ±17.6 ±5.5 ±6.7 ±
11.0 ±5.3 ±
22.6 ±22.5 ±
326.3 ±131.3 ±457.7 ±20.0 ±3.3 ±
0.028.3
5.50.42.44.02.74.35.42.9
10.817.829.429.049.712.1
2.1
*Each value given is a mean value of the number of experiments listed with the standarddeviation. Tests of significance were not made.
For abbreviations, refer to footnotes of tables 1 and 2.
ventricle. The results obtained with the coro-nary sinus technique, on the basis of ourexperiments, appear to be fairly consistentfor such induced hemodynamic changes asincreased right ventricular effort, somewhatless adequate for elevation of aortic bloodpressure, and much less satisfactory whenheart rate changes or when inotropic agentslike Z-epinephrine are exhibited.
D. Mechanical Efficiency of the Preparation
There was opportunity in these experimentsto calculate the external work of the leftventricle under the different conditions asthe product of stroke output and mean aorticblood pressure and, by comparing it withtotal OoC, to calculate the (external work)mechanical efficiency of the left ventricle.In the various circumstances analyzed intables 1 to 6, the mean left ventricular ex-ternal work varied from 31.4 ± 2.7 to 106.4± 0.0 Kg.-M., which is of the order previouslyfound by us.29 Furthermore, the mechanicalefficiency was low, varying in different circum-stances, as means of experiments, from 5.5 ±1.9 to 12.9 ± 7.0 per cent. This result is
also of the order previously found by us29
and suggests again that the heart has a lowmechanical efficiency for its external work.
SummaryThe open-chest anesthetized dog was pre-
pared to permit the partition of coronaryoutflow into the coronary sinus and the extra-coronary sinus venous channels. The effects ofincreased resistance-load of the left ventricle,of augmented effort of the right ventricle,and of induced acceleration of the heart ratewere analyzed. Tn several animals, the effectof Z-epinephrinp exhibition was also deter-mined. The effect of spontaneous tachycardiawhich developed in two dogs was also ana-lyzed. A balloon inserted into the right ven-tricular cavity was used to augment its effortunder isovolumic conditions.
Overall, the coronary sinus was found todrain approximately 60 per cent of the totalcoronary flow. Notable deviations from thismean were encountered in all experiments.The most marked occurred during spontane-ous tachycardia and Z-epinephrine exhibition,Significant changes also were observed when
Circulation Research, Volume XI, October 1962
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

PABTITION OF CORONARY FLOW 697
heart rate changes were induced. Increasingright ventricular effort had no apparent effecton the amount of blood drained via the coro-nary sinus. Augmenting left ventricular effortincreased both coronary sinus and extra-coro-nary-sinus drainage more or less proportion-ately on the whole.
Myocardial oxygen consumption was meas-ured as the sum of the oxygen consumptioncalculated from the coronary sinus and fromthe extra-coronary-sinus channels. In eachcase, this measurement was the product offlow in the drainage system and the arterio-venous oxygen difference found in that system.The venous oxygen content in the two drain-age systems differed significantly and alteredto varying degrees when conditions changed.Augmentation of left ventricular effort pri-marily increased the oxygen usage measuredfrom the coronary sinus, while increased effortof the right ventricle primarily augmentedthat measured from the extra-coronary-sinuschannels.
These observations lend support to thehypothesis that the coronary sinus representsblood draining primarily from the left ven-tricle and the extra-coronary-sinus channelsprimarily that from the right ventricle. How-ever, the extra-coronary-sinus channels alsodrain the left ventricle, and the percentagedistribution between them and the coronarysinus can vary significantly as far as cardiacoxygen consumption is concerned, especiallywhen i-epinephrine is exhibited or when theheart changes its rate spontaneously or withan artificial pacemaker.
It is concluded that while the coronarysinus eatheterization method is the best avail-able to compute the oxygen usage of the leftventricle in the closed-chest animal or inman, it has limits of accuracy as a completelyreliable method for assessing the oxygen con-sumed by the whole heart or the left ventricle.This limitation applies especially (1) duringstress when the heart speeds up, (2) in heartsthat are abnormal or diseased, and (3) whenthe effects of inotropic agents are beingexamined.
AcknowledgmentWe are indebted to both Dr. Leroy Hirsch and
Mrs. Alice Bromley for assistance in preparing thereport.
References1. FEINBERG, H., KATZ, II. N., AND BOYD, E.:
Determinants of coronary flow and myocardialoxygen consumption. Am. J. Physiol. 202: 45,1962.
2. MORAWITZ, P., AND ZAHN, A.: Untersuchungen
iiber den Coronarkreislauf. Deutseh. Arch. f.klin. Med. 116: 364, 1914.
3. LENDRUM, B . , KONDO, B. , AND KATZ, L. N . :
Role of thebesian drainage in the dynamicsof coronary flow. Am. J. Physiol. 143: 243,1945.
4. LAURENT, D., BOLENE-WILLIAMS, C, WILLIAMS,
F. L., AND KATZ, L. N".: Effects of heart rateon coronary flow and cardiac oxygen consump-tion. Am. J. Physiol. 185: 355, 1956.
5. FEINBERG, H., AND SISTER MART ALMA: Spec-
trophotometric determination of blood oxygencontent. J. Lab. & Clin. Med. 55: 784, 1960.
6. SCHLESINGER, M. J.: Injection plus dissectionstudy of coronary artery occlusions and anasto-moses. Am. Heart J. 15: 528, 1938.
7. MARCUS, E., HASBROUCK, E. E., AND WONG.
S. N. T.: Myocardial revaseularization: Ex-perimental and clinical critique. A.M.A. Arch.Surg. 74: 225, 1957.
8. GREGG, D. E., PRITCHARD, W. H., SHIPLEY, R. E.,
AND WEARN, J. T.: Augmentation of bloodflow in the coronary arteries with elevationof right ventricular pressure. Am. J. Physiol.139: 726, 1943.
9. GELLER, H. M., BRANDFONBRENER, M., AND
WIGGERS, C. J.: Derivation of coronary sinusflow during elevation of right ventricularpressure. Circulation Research 1: 152, 1953.
30. KATZ, L. N., JOCHIM, K., AND BOHNING, A.:
Effect of the extravascular support of theventricles on the flow in the coronary vessels.Am. J. Physiol. 122: 236, 1938.
11. KATZ, L. X.: Performance of the heart. Circu-lation 21: 483, 1960.
12. GEROLA, A., FEINBERG, H., AND KATZ, L. N.:
Role of catecholamines on energetics of theheart and its blood supply. Am. J. Physiol.196: 394, 1959.
13. ANREP, G. V., BLALOCK, A., AND HAMMOUDA,
M.: Distribution of blood in the coronaryvessels. .J. Physiol. 67: 87, 1929.
14. RUSHMER, R. F . : Cardiovascular Dynamics, ed.2. Philadelphia, W. B. Sawders Co., 1961,p. 78.
Circulation Research, Volume XI, October 1962
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

698 LAFONTANT, FEINBERG, KATZ
15. KATZ, L. N., JOOHIM, K., AND WEINSTEIN, V.:Distribution of the coronary blood flow. Am.J. Physiol. 122: 252, 1938.
16. WEAEN, J. T.: Role of the thebesian vessels inthe circulation of the heart. J. Exper. Med.47: 293, 1928.
17. JOHNSON, J. R., AND WIGGERS, C. J.: Alleged
validity of coronary sinus outflow as a cri-terion of coronary reaction. Am. J. Physiol.118: 38, 1937.
18. GEEGO, D. E.: Coronary Circulation in Healthand Disease. Philadelphia, Lea & Febiger,1950.
19. RATFOED, C. R., KHOUBI, E. M., LEWIS, F. B.,AND GREGG, D. E.: Evaluation of use of leftcoronary artery inflow and oxygen content ofcoronary sinus blood as a measure of leftventricular metabolism. J. Appl. Physiol. 14:817, 1959.
20. SCHLESINGEE, M. J. : Significant variations inthe anatomic pattern of the coronary ves-sels. In Blood, Heart and Circulation, editedby F. R. Moulton. Lancaster, Pa., AmericanAssociation for the Advancement of Science,1940, vol. 13, p. 61.
21. PRINZMETAII, M., SIMPKIN, B., BERGMAN, H. C,
AND KRUGEE, H. E.: Studies on coronarycirculation: I I . Collateral circulation of thenormal human heart by coronary perfusionwith radioactive erythrocytes and glass spheres.Am. Heart J. 33: 420, 1947.
22. PITT, B.: Interarterial coronary anastomoses:Occurrence in normal hearts and in certain
pathological conditions. Circulation <su: 816,1959.
23. ZOLL, P. M., WESSLER, S., AND SCHLESINGER,M. J.: Interarterial coronary anastomoses inthe human heart with particular reference toanemia and relative cardiac anoxia. Circula-tion 4: 797, 1951.
24. BLUMGART, H. L., SCHLESINGER, M. J., ANDDAVIS, D.: Studies of the relation of clinicalmanifestations of angina pectoris, coronarythrombosis and myocardial infarction to thepathological findings with particular referenceto the significance of the collateral circulation.Am. Heart J. 19: 1, 1940.
25. RAVIN, A., AND GEEVER, E. F.: Coronary arterio-sclerosis, coronary anastomoses and myocardialinfarction. Arch. Int. Med. 78: 125, 1946.
26. ZIMMERMAN, H. A.: Coronary circulation inpatients with severe emphysema, cor pulmonale,cyanotic congenital heart disease and severeanemia. Dis. of Chest 22: 269, 1952.
27. ALELLA, A., WILLIAMS, F. L., BOLENE-WILLIAMS,C, AND KATZ, L. N.: Interrelation betweencardiac oxygen consumption and coronaryblood flow. Am. J. Physiol. 183: 570, 1955.
28. MOE, G. K., AND VISSCHER, M. B.: Mechanism
of failure in the completely isolated mam-malian heart. Am. J. Physiol. 125: 461, 1939.
29. ALELLA, A., WILLIAMS, F. L., BOLENE-WILLIAMS,C, AND KATZ, L. N.: Role of oxygen andexogenous glucose and lactic acid in the per-formance of the heart. Am. J. Physiol. 185:487, 1956.
Book Reviews
Rheumatic Heart Disease, Jacques B. Wallachand Edgar F. Borgatta, in collaboration withAlfred A. Angrist. Springfield, Illinois, CharlesC Thomas, 1962, 174 pages, illustrated. $7.50.The analysis of 509 autopsied cases with rheu-
matic heart disease is contained in this report.The presentation includes tabular material examin-ing the effects of age, sex, color, and time periodon the location and severity of valvular disease,complicating lesions, and cause of death. Thedevelopment of either heart failure or bacterialendocarditis accounted for 65 per cent of thedeaths. Embolism was the cause of death in 19per cent, which is lower than 48 per cent reportedby another group. The pathological data containedin this book will prove to be useful to manycardiologists.
A Guide to Cardiology, J. C. Leonard and E. G.Galea. Baltimore, Williams & TVilkins Co., 1961.267 pages, illustrated. $6.50.
The emphasis throughout this book has beenplaced on clinical features, diagnosis, and treat-ment of the commoner diseases of the heart.The principles and clinical relevance of eleetro-cardiography are discussed, and a brief outlineis given of some of the newer diagnostic methods."No references are given because these mayreadily be found in any of the more compre-hensive texts."
The authors have accomplished their purposeof writing their book primarily for undergraduatestudents, house physicians, and general practi-tioners. It might be helpful for American readersto append a list of synonyms for the drugsidentified by British names. It would also behelpful to add a range of average doses forthe various drugs to eliminate the necessity ofconsulting a more comprehensive text book incardiology.
Circulation Research, Volume XI, October 196t
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from

Robert R. Lafontant, Harold Feinberg and Louis N. KatzOther Coronary Drainage Channels
Partition of Coronary Flow and Cardiac Oxygen Extraction Between Coronary Sinus and
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 1962 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.11.4.6861962;11:686-698Circ Res.
http://circres.ahajournals.org/content/11/4/686World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Research Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 2, 2018http://circres.ahajournals.org/
Dow
nloaded from