Embed Size (px)
Citation preview
Revised 11/9/15
2016 PARTICIPATION AGREEMENT
with (INSERT Name of Physician Organization)
and each of its Participating Primary Care Practices
with the
Michigan Department of Health and Human Services (MDHHS)
for the
Michigan Primary Care Transformation (MiPCT) Demonstration Project
The Michigan Primary Care Transformation (MiPCT) Project is a multi-payer advanced primary care demonstration project, originally extending from January 1, 2012 through December 31, 2014, and now extended for an additional two years, ending December 31, 2016. This project involves collaboration among the Michigan Department of Health and Human Services (MDHHS); the University of Michigan Health System (UMHS); public and private Michigan Payers; the Centers for Medicare and Medicaid Services (CMS); Michigan’s Physician Organizations (POs); and Michigan Primary Care Practices that have been designated as Patient-Centered Medical Homes (PCMH). The purposes of the MiPCT Project are: (1) to foster the transformation of participating PCMH primary care practices to enable interventions that impact all persons served by the Practice in a cost-effective manner using evidence-based guidelines and practices, and (2) to evaluate the Demonstration Project according to the Institute for Healthcare Improvement’s Triple Aim goals of improved health outcomes, improved patient experience of care, and reduced preventable healthcare costs.
The major objectives of the MiPCT Demonstration include:
1. I m prove Quality and Outco m es – Improve healthcare access, quality, coordination, experience, and health outcomes for patients in this Demonstration Project through continuous quality improvement of participating Patient-Centered Medical Home (PCMH) Practices supported by a network of participating Physician Organizations in Michigan.
2. Lower Overall Health Care Costs – Reduce unnecessary or avoidable costs through the timely and effective transformation in care delivery by the PCMH Practice.
3. I m prove A c cess – Improve access to high quality health care by ensuring a strong, sustainable primary care network for the state.
4. Create a Su s t aina b l e PCMH Model – Create a successful and sustainable model for public/private Payer and Practice collaborations to improve health care value and transform primary care in ways that are sustainable and can be replicated statewide.
2
A. DEFINITIONS
“Agreement” means this Participation Agreement between the Participating Physician Organization (PO), Participating Practice, and MDHHS, for the MiPCT Demonstration Project.
“Billing Code” refers to Care Management G and CPT codes and modifiers submitted to participating Payers by practices or POs for services provi ded by moderate, hybrid, and/or complex care managers.
“Care Team” means a Participating Practice-based team consisting of a primary care provider, one or more Care Managers for moderate and complex care patients, plus nurse(s), medical assistant(s), and/or other clinical support or allied professional staff within the Participating Practice who participate jointly to manage care for the entire patient panel as well as distinct sub-sets of patients. Other than the primary care provider, Practice staff may participate on more than one Care Team.
“Care Coordination” includes self-management support, preventive services, care management, linkages to community services, and complex care management for high-risk patients.
“Care Coordination Payment” means the payment made by a participating Payer to support care management and care coordination. See Appendix A.
“Care Management” means the application of systems, science, incentives, and information to improve medical practice and assist consumers and their support system to become engaged in a collaborative process designed to manage medical, social, and/or mental health conditions more effectively. The goal of care management is to achieve an optimal level of wellness and improve coordination of care while providing cost effective, non-duplicative services.
"Complex Care Manager” means an individual meeting MiPCT criteria assigned to provide care management services, including targeted interventions to avoid hospitalization, ER visits, ensure standards of care, coordinate care across settings, and help patients understand options. Focus of complex care management is completion of a comprehensive patient assessment, development of an individualized care plan, care coordination, and longitudinal patient follow-up. Complex patients have multiple chronic illnesses, a poorly controlled chronic condition, frailty, and/or significant social and/or economic issues.
“Complex Care Management” means the systematic coordination and assessment of care and services provided to members who have experienced a critical event or diagnosis that requires the extensive use of resources and who need help navigating the system to facilitate appropriate delivery of care and services.
“CHEAR” is the Child Health Evaluation and Research (CHEAR), a unit of the University of Michigan’s Board of Regents, selected by MDHHS to conduct all data acquisition and merging tasks related to Medicaid administrative data.
3
“CMS” means the Centers for Medicare and Medicaid Services, a branch of the U.S.Department of Health and Human Services.
“Eligible Practices” means those PCMH (i.e., PGIP PCMH or NCQA Level 2 or 3) practices that received PCMH designation through aMiPCT-approved organization in 2010 and have continuously maintained that designation through 2016. A practice that loses PCMH Designation in 2011 or in any subsequent year during the Project will be disqualified from further participation in the Project, even if PCMH designation is regained at a future point during the Project.
“G Code billings” refers to specified G codes and modifiers submitted to participating Payers by practices or POs for services provi ded by moderate, hybrid, and/or complex care managers.
“Hybrid Care Manager” means an individual meeting MiPCT criteria for the complex care manager AND the moderate care manager (see definitions for the Moderate Care Manager and the Complex Care Manager).
“Member List” means the list of all beneficiaries of a Participating Payer that have been attributed to the MiPCT Demonstration Project. See Appendix B.
“MDHHS” is the Michigan Department of Health and Human Services, the agency of state government designated by the Governor of Michigan to apply for participation to CMS in this multi-payer medical home demonstration project, and the entity required by CMS to be responsible for oversight and monitoring.
“Michigan Data Collaborative” (MDC) is the central entity that houses the claims and eligibility data from Michigan Payers, and produces regular reports for POs, Practices, and MiPCT Core Team. MDHHS provides direct oversight for the MDC.
“Michigan Public Health Institute” (MPHI) is the non-profit institute that MDHHS has selected to conduct the state-level evaluation of the Michigan Primary Care Transformation Demonstration Project.
“MiPCT Project,” “Demonstration Project” or “Project” is the five-year statewide Michigan Primary Care Transformation Demonstration Project involving public and private Payers, Physician Organizations, and PCMH-designated Practices, as more fully described above.
“MiPCT Core Team” is the group of individuals, assisted by the MiPCT Steering Committee and other advisors, that is responsible for planning and evaluating all aspects of the MiPCT Demonstration Project, composed of representatives from the MDHHS, UMHS, and MPHI.
“Moderate Care Manager” means an individual meeting MiPCT criteria assigned to provide care management services, including proactive population management. This manager works with patients to optimize control of chronic conditions and prevent/minimize long
4
term complications. The focus is on education and self-management support, and/or coordination of care for patients with mild to moderate illness.
“Participating Practice” or “Practice” means a primary care practice that: 1) is affiliated with a Physician Organization (PO) participating in the Physician Group Incentive Program (PGIP) of Blue Cross Blue Shield of Michigan, 2) meets PCMH Designation criteria, and 3) has entered into an agreement with MDHHS to participate in the MiPCT Project. Having successfully achieved at least baseline expectations, the Practice is working toward complete PCMH transformation.
“Participating Payer” or “Payer” means a public or private insurer, health service corporation or health maintenance organization that has entered into an agreement with MDHHS to participate in the MiPCT Demonstration Project.
“Participation Agreement” means this document that outlines the parameters and expectations of participating stakeholders in the MiPCT Demonstration Project.
“Patient Registry” means is an electronic database that contains demographic and clinical data (in data fields accessible for tabulation and population management) on all patients served by the Practice to enable physicians and staff to manage their populations of patients.
“PCMH Designation” means a Practice that received PCMH designation through theBlue Cross Blue Shield of Michigan Physician Group Incentive Program (PGIP) in 2010 and/or NCQA recognition as a Level 2 or 3 PCMH prior to July 2010 or achieved. PCMH Designation subsequent to July 2010 and has been approved for inclusion by MiPCT Leadership. PCMH Designation must be maintained throughout the term of the MiPCT Demonstration Project.
“Performance Incentives” means the funding provided to Physician Organizations and Practices to reward the achievement of desired metrics/outcomes related to MiPCT implementation.
“Performance Incentive Payment” means a variable amount, semi-annual payment made by a Participating Payer for performance on a set of metrics. See Appendix A.
“Physician Organization” or “PO” means a Physician Organization, Physician/Hospital Organization, Independent Practice Association or similar organization participating in the PGIP of Blue Cross Blue Shield of Michigan that has affiliations with PCMH-designated Practices, and which provides supportive services to enhance the Practice’s medical home capabilities and enables continuous quality improvement.
“Practice Transformation” or “PCMH Transformation” refers to the result of enabling a primary care Practice to use both educational and financial support to develop the 1) infrastructure, 2) organizational, and 3) cultural changes characteristic of patient-centered medical homes, i.e., primary care provider-led; prepared and proactive care teams providing comprehensive, whole person care; coordination of care across healthcare settings; enhanced patient access; use of electronic technology; and development of a culture that encourages striving for continual improvement in patients’ experience of care and health

5
outcomes for the entire Practice panel, while reducing preventable costs.
“Practice Transformation Payment” means the payment made by a Participating Payer toParticipating Practices to support PCMH infrastructure. See Appendix A.
“Primary Care Provider” means a primary care physician, and also includes licensed physician assistants and licensed nurses certified as nurse practitioners, who are working under supervision of a physician, as defined in the Michigan Public Health Code, Act 368. “Project Participant” means any Payer, Physician Organization or Primary Care Practice that has signed an Agreement with MDHHS and participates in the Demonstration Project.
“Revenue Withhold” means the reduction of an amount paid to a PO or Practice (without the opportunity for payment recovery).
“UMHS” refers to the University of Michigan Health System, the entity with which MDHHS has contracted to provide operational support for the demonstration.
B. PERIOD OF AGREEMENT
This Agreement will be in effect beginning January 1, 2016 through December 31, 2016, and covers Year Fourive of the five-year Demonstration Project.
C. MDHHS RESPONSIBILITIES
1. MDHHS is responsible for overall direction and control of the Demonstration Project. Assisted by MiPCT advisors and vendors (see Appendix C), MDHHS will assure that programmatic standards are met, provisions in agreements are adhered to, and program objectives are achieved.
2. MDHHS shall enter into a Business Associate Agreement with the UMHS on behalf of its sub-units, including CHEAR and MDC, to protect Personal Health Information.
3. MDHHS shall enter into a Business Associate Agreement (BAA) and a Data Use Agreement (DUA) with each PO and participating PCMH Practice to protect Personal Health Information.
[4.] MDHHS and the MiPCT Core Team will monitor and review PO quarterly narrative and financial reports submitted by each Physician Organization as well as the PO’s quarterly self-assessment data (SAD) reports forwarded by BCBSM that assesses PCMH capabilities. This review will be done to assure that the Physician Organization and participating Practices are meeting the provisions of this Participation Agreement, or that quality improvement measures are in place to remedy any non-compliance issue(s). If any Physician Organization or Practice has been out of compliance with the provisions of this participation agreement for six (6) months or more, MDHHS has sole authority to make a determination regarding continued participation, continued
6
participation but with a revenue withhold, or termination of the PO and/or Practice from the Demonstration Project. If a PO has experienced more than two consecutive quarters of Care Manager to Patient staffing ratio at a level below 80% of the requirement, MDHHS will implement a revenue withhold that decreases the Medicare and Medicaid care management payments by a percentage amount equivalent to the percentage that the staffing ratio is below 100% percent. MDHHS will also notify other participating payers about POs whose Care Manager to Patient staffing ratio is below 80% for more than two consecutive quarters.
4. If there is evidence that the PO or Practice fails to provide MiPCT Care Manager services as specified in this Agreement, MDHHS has the authority to withhold or terminate payment.
65. MDHHS and the MiPCT Core Team will assure that each MiPCT Care Manager (Moderate, Hybrid, and Complex Care) participates in a combination of meetings and/or other MiPCT-sponsored or MIPCT-approved events as described in Appendices F and G.
6. MDHHS and the MiPCT Core Team will monitor and review quarterly financial reports submitted by each Physician Organization to assure that 1) Care Coordination revenues spent are in alignment with the MiPCT Clinical Model, 2) Care Manager requirements are met, and 3) at least 80% of Medicaid and Medicare incentive payments are distributed to practices (or otherwise approved).
7. MDHHS retains the right to suspend Medicaid and/or Medicare MiPCT Care Coordination payments until such time that Care Coordination revenues and expenses are aligned.
78. MDHHS shall monitor participating Payers to assure that provisions of this Participation Agreement are being met.
89. MDHHS shall approve curricula and plans for learning collaboratives, education and training programs (including identification of approved Moderate, Hybrid and Complex Care Manager training programs), and/or other facilitated practice transformation assistance for Practices and/or for Physician Organizations.
910. MDHHS shall oversee all contractors and subcontractors affiliated with the MiPCT Project.
D. PHYSICIAN ORGANIZATION (PO) RESPONSIBILITIES
The PO is responsible for assisting with implementation of the MiPCT Project and for supporting participating Practices in their development of PCMH capabilities and attainment of the MiPCT objectives. The PO shall:
7
[1.] Enter into a Business Associate Agreement (new for 2015) and a Data Use Agreement with MDHHS, CMS and UMHS (the latter on behalf of the MDC and CHEAR.) The Business Associate Agreement and Data Use Agreement must each be signed by an individual able who is currently in a position to commit the PO to these provisions. (See Attachment I to this agreement.) If the signature on the Data Use Agreement that was signed in Year One or Year Two or Year Three is still current, that Agreement is included as Attachment II to this Participation Agreement. If the signature is not current, a new Data Use Agreement must be signed by an individual able to commit the PO to these provisions.a. The Business Associate Agreement that was signed in Year Four is included as
Attachment I in this Agreement. If the signature is not current, a new Business Associate Agreement must be signed.
b. The most current Data Use Agreement that was signed in Year One or Year Two or Year Three or Year Four is included as Attachment II to this Participation Agreement. If the signature is not current, a new Data Use Agreement must be signed.
[2.] For each Practice that continues to participate in the MiPCT Demonstration Project in Year Fourive: a. Verify that the Practices listed on the worksheet attached to the cover letter for this
Participation Agreement are members of the PO.b. Verify that the names of the Practices or Practice ID’s and the name of the PO are
the same as the names listed with the BCBSM PGIP PCMH program. Exception to this requirement must be approved by MiPCT Leadership.
c. Ensure that each Practice signs this 2016 Participation Agreement. [d.] Ensure that each Practice signs the Business Associate Agreement (BAA) that is
new for 2015 and Data Use Agreement (DUA). If the signature on the 2015 Business Associate Agreement (BAA) from Year Four or the Data Use Agreement (DUA) from Year One or Year Two or Year Three or Year Four is still current and this individual is in a position to commit the Participating Practice to these provisions, a new BAA or DUA Agreement for 2016 is not needed. If the signature is not current on the BAA or the DUA, a new Data Use Agreement(s) must be signed.
[e.] Forward the Participation Agreement (with updated accompanying BAA and DUA agreements if applicable) to MDHHS as soon as possible after each has been signed by the PO and each participating Practice.
1.[3.] Assure that each Practice participating in the MiPCT Demonstration Project is providing services consistent with the MiPCT Care Model (see Appendix E).
4. Assure that each Practice participating in the MiPCT Demonstration Project is meeting and maintaining MiPCT PCMH Infrastructure Requirements (see Appendix D) and all other provisions in this Participation Agreement throughout 2016. a. If the Practice is unable to maintain one or more MiPCT PCMH infrastructure or
other requirement of this agreement during each quarter throughout 2016, the PO must notify the MiPCT Core Team at the earliest opportunity in order to enable MiPCT leadership to respond with assistance whenever possible and to assure reasonable oversight of the Demonstration Project. The Practice may be contacted
8
by the MiPCT Core Team, including onsite visits, to discuss the area(s) of deficiency and obtain additional information.
b. If the Physician Organization does not alert the Core Team in advance about a Practice that is out of compliance with the provisions of this Agreement for longer than one quarter, the Physician Organization will be required to submit a corrective action plan.
5. Arrange to provide Care Manager services for those Practices that choose not to hire their own Moderate, Hybrid, and/or Complex Care Manager(s). All Care Managers must function as integral parts of the Practice’s Care Team, including becoming embedded in the Practice, in order to facilitate frequent communication with the team and access to patient records.
6. Arrange to have a Care Manager available during extended Practice hours as needed to meet the educational and other relevant needs of Members unable to come to the Practice during normal business hours.
7. Maintain a 100% Care Manager-to-Member ratio across the Physician Organization, with a 20% allowance for turnover or special circumstances. (100% of the ratio of Care Manager-to-Members is one (1) Complex Care Manager and one (1) Moderate Care Manager per 5,000 patients, or two (2) Hybrid Care Managers per 5,000 patients calculated across the Physician Organization.) In the event of a care manager vacancy, notify MDHHS via the [email protected] mailbox if the position is not filled within 30 days.
8. Assure that Practices and all other relevant entities are informed that if revenues substantially exceed expected and approved MiPCT expenses, or if spending is not in alignment with the clinical model, MDHHS reserves the right to suspend Medicaid and/or Medicare payments until expenses and revenues are aligned.
9. Distribute MiPCT payments to participating Practices as specified in the MiPCT Demonstration Payment Model (see Appendix A), including assurance that no less than 80% of Performance Incentive payments received are distributed to participating Practices, or as otherwise approved.
10. Support Participating Practices in development of new PCMH capabilities.
11. Identify a Physician Champion who will communicate with all Physicians in the PO and all Participating Practices, encouraging team care and attention to other aspects of the MiPCT model.
12. Utilize Care Team Connect to electronically distribute member lists to Practices and Care Managers, OR dDistribute MiPCT Member Lists to Practices and Care Managers within ten (10) business days of receipt from the MDC.
13. Distribute “Dashboard” reports to Practices and to Care Managers within ten (10) business days of receipt from the MDC.
9
14. Distribute “FLASH for Practices” to every staff person in each participating Practice, including Care Managers, and ensure that the newsletter is discussed in staff meetings and in team discussions.
15. Assure that the PO and each Practice accepts reimbursements from all participating Payers.
16. Assure that Care Managers are serving all attributed at-risk patients from all participating Payers. Assure that Care Managers have a workspace, computer access and telephone in each practice for which they provide care management.
17. Assure that all Practices (and the PO if applicable) are billing G-codes for Care Management of BCBSM-attributed, BCN-attributed, and Priority Health-attributed patients who have been determined to be at moderate or complex risk and who could benefit from care management services.
18. Assure that each MiPCT Care Manager (Moderate, Hybrid, and Complex) completes a combination of MiPCT-sponsored or approved educational offering per year as described in Appendices F and G.
19. Assure that every participating Practice abides by the Practice Learning Activity Guidelines, such that the Physician-led Care Team (i.e., physician, care manager and at least one other practice team member, plus a PO representative if possible) participates in a combination of meetings and/or other MiPCT-sponsored or approved events. See Appendices F and G.
20. Assure that each Practice holds a monthly program of Medical Home Team-based meetings, dedicated to team-based management and review of reports with a Physician, Care Manager(s) and other Care Team members in attendance.
21. Assure that every Physician has frequent contact with the Practice’s Care Manager, at least weekly (as appropriate) for those with patients receiving active care management services. Strongly encourage frequent Physician / Care Manager brief meetings (or huddles) to discuss patients that may need care management services.
22. Alert the MiPCT Core Team of concerns about capacity of the PO to meet the requirements of this agreement or concerns about other issues related to the demonstration, in order to enable MiPCT leadership to respond with assistance whenever possible and to assure reasonable oversight of the Demonstration Project.
23. Submit PO quarterly narrative and financial reports to MDHHS using the MiPCT templates and according to the specified timetable.
24. Inform MDHHS within five (5) days of learning about a change in physician employment or status within a participating Practice.a. For Physicians joining or leaving a Practice, specify the effective date, specialty,
and key identification numbers (NPI, PIN, TIN) by completing a MiPCT Physician
10
and Practice Change Form and forwarding this to the MiPCT Demonstration Mailbox (i.e., [email protected]).
b. Failure to provide this information to the Demonstration Mailbox for notification to CMS may result in a payment lapse or delay for new Physicians, or the need to reimburse CMS for payments made for Physicians who have left the Practice.
25. Provide requested practice-level registry and other data that may be required for project planning, operations, and evaluation. Such data will include, but not be limited to, Practice contact information, PIN numbers, and Payer-mix.a. To reduce the burden of repetitive reporting activities, POs shall authorize BCBSM
to provide their quarterly self-assessment data reports regarding PCMH capabilities, and other data to the MiPCT Core Team for use in planning, monitoring, and evaluation.
b. In accordance with the Data Use Agreement, share relevant data with the MDHHS, MDC, UMHS, MPHI, CMS-contracted evaluator, and Payers with which the Practice has a contractual relationship.
26. Support the MiPCT Project evaluations by: (1) assisting with the dissemination of physician and staff surveys to Practices and monitoring Practices to assure that they respond, and (2) responding directly to PO surveys within the required timeframe.
27. Physician Organizations and Practices with low performance onin the lowest quartile of MIPCT quality and/or utilization metrics may will be requirasked to complete and submit a Quality Improvement Plan and to demonstrate improvement within a reasonable timeframe.
28. Provide support for the MiPCT and Care Management Resource Center team members to conduct practice site visits to facilitate identification of processes and work flows contributing to the delivery of population health management and care management. Site visits may be with PO Leaders and also at the practice.
. Enter into a Business Associate (new for 2015) and a Data Use Agreement with MDHHS, CMS and UMHS (the latter on behalf of the MDC and CHEAR.) The Business Associate Agreement must be signed by an individual able to commit the PO to these provisions. (See Attachment I to this agreement.) If the signature on the Data Use Agreement that was signed in Year One or Year Two or Year Three is still current, that Agreement is included as Attachment II to this Participation Agreement. If the signature is not current, a new Data Use Agreement must be signed by an individual able to commit the PO to these provisions.
29. Ensure that practices (or the PO on behalf of the practice) actively uses the patient registry for MiPCT patients for population health improvement and closing gaps in care for preventive services and chronic conditions. Optimally this would involve the use of a panel manager who reviews the registry, identifies opportunities for proactive care, and discusses with the clinical team for appropriate follow-up.
11
E. PCMH-DESIGNATED PRACTICE RESPONSIBILITIES
Each participating PCMH Practice is responsible for using the additional financial support received from MiPCT Payers to provide effective, efficient, patient-centered services consistent with the MiPCT Model (see Appendix E) that lead to improved health outcomes, improved patient experience of care and reduced healthcare costs. PCMH Practices shall:
1. Maintain PGIP PCMH and/or NCQA Level 2/3 designation throughout the five (5)-year demonstration project.
2. To avoid delays in payment or the need to refund payment for physicians who leave the Practice, notify the PO of any changes in physician employment or standing within five (5) business days and request this information be passed on to MDHHS.
3. Continue to develop PCMH capabilities. This includes standardizing care processes and implementing ‘Best Practices’ to ensure that patients consistently receive efficient, evidence-based, patient-centered care.
4. Assure that every MiPCT PCMH Infrastructure Requirement (see Appendix D) continues to be maintained by the Practice throughout 2016.a. If the Practice is unable to maintain one or more MiPCT PCMH Infrastructure
Requirements in any quarter throughout 2016, the Practice will be contacted by the MiPCT Core Team to discuss the area(s) of deficiency. MiPCT reserves the right to perform an onsite visit at the Practice location to obtain additional information.
b. If the Practice is unable to maintain any MiPCT PCMH Infrastructure Requirement for two quarters during 2016, MDHHS has sole authority to make a determination regarding continued participation, continued participation but with a revenue withhold, or termination of the Practice from the Project. If the Practice is terminated, MDHHS will notify all Payers to suspend any payments to the Practice under the Demonstration Project that are submitted after the termination date.
5. Accept reimbursements from all MiPCT-participating Payers.
6. Educate every staff member in the Practice to assure that each knows that the Practice is a Patient-Centered Medical Home and is able to explain to patients what this designation means.
7. Assure that one or more qualified Care Managers is/are providing care management services to at-risk patients attributed to the MiPCT Project (see Appendix E). Assure that Care Managers have a workspace, computer access and telephone in each Practice setting that he/she/they serve. a. The Moderate, Hybrid, and Complex Care Manager may be employed or
contracted by the Practice or by the Physician Organization.b. Regardless of who employs the Care Manager(s), these individuals will function as
integral parts of the Practice’s Care Team. Care Managers must be embedded in
12
the Practice to enable face-to-face interactions with MiPCT-eligible patients likely to benefit from care management, as well as frequent communications with the Care Team, and direct access to patient records.
c. All Care Managers for the MiPCT demonstration must meet MiPCT Education andTraining requirements.
d. All Care Management services will conform to MiPCT clinical guidelines.
8. Maintain an appropriate Care Manager-to-Member ratio, assuring embedment of the Care Manager(s) within the Practice across the Physician Organization (100% of the ratio of Care Managers-to-Members is one (1) Complex Care Manager and one (1) Moderate Care Manager per 5,000 patients, or two (2) Hybrid Care Managers per 5,000 patients.) In the event of a Care Manager vacancy, notify the PO immediately if the position is not filled within 30 days and request this information to be passed on to MDHHS.
9. Note that if revenues substantially exceed expected and approved MiPCT expenses, or if spending is not in alignment with the clinical model, MDHHS reserves the right to suspend Medicaid and/or Medicare payments until expenses and revenues are aligned.
10. Assure that G and CPT-codes for Care Management services delivered within the Practice are billed for patients determined to be at moderate or complex risk and attributed to BCBSM, BCN, and/or Priority Health.
11. Assure that embedded Care Managers are serving attributed at-risk patients from all participating Payers.
12. Abide by the Practice Learning Activity Guidelines such that the Physician-led Care Team (i.e., Physician, Care Manager and at least one other practice team member, plus a PO representative if possible) participates in a combination of meetings and/or other MiPCT-sponsored or approved events as described in Appendices F and G.
13. Hold a monthly program of Medical Home Team meetings, dedicated to team-based management and review of reports, with a Physician, Care Manager(s) and other Care Team members in attendance.
14. Assure that every Physician has frequent contact with the Practice’s Care Manager, at least weekly (as appropriate) for those with patients receiving active Care Management services. Strongly encourage frequent Physician/Care Manager brief meetings (or huddles) to discuss patients that may need Care Management services.
15. Assure that each MiPCT Care Manager (Moderate, Hybrid, and Complex Care) participates in a combination of meetings and/or other MiPCT-sponsored or MIPCT-approved events as described in Appendices F and G.
16. Practices in the lowest quartile of MIPCT quality and/or utilization metrics may be asked to complete and submit a Quality Improvement Plan and to demonstrate improvement within a reasonable timeframe.
13
17. Practices may be asked to participate in a site visit conducted by MiPCT and/or Care Management Resource Center team members to facilitate identification of processes and work flows contributing to the delivery of population health management and/or care management.
[17.] Enter into a Business Associate Agreement (new for 2015) and a Data Use Agreement with MDHHS, CMS and UMHS (the latter on behalf of the MDC and CHEAR.) The Business Associate Agreement and Data Use Agreement must each be signed by an individual able who is currently in a position to commit the Practice to these provisions. (See Attachment I to this agreement.) If the signature on the Data Use Agreement that was signed in Year One or Year Two or Year Three is still current, that Agreement is included as Attachment II to this Participation Agreement. If the signature is not current, a new Data Use Agreement must be signed by an individual able to commit the Practice to these provisions.
a. The Business Associate Agreement that was signed in Year Four is included as Attachment I in this Agreement. If the signature is not current, a new Business Associate Agreement must be signed.
b. The most current Data Use Agreement that was signed in Year One or Year Two or Year Three or Year Four is included as Attachment II to this Participation Agreement. If the signature is not current, a new Data Use Agreement must be signed.
18. Once a signed Data Use Agreement (DUA) is in place, provide data or any other relevant information when requested for MiPCT evaluation, operations or planning. Respond within the requested timeframe to reasonable requests by the state evaluator for information, data and/or for completion of physician and staff surveys. The state evaluator will conduct physician and staff surveys during the Project.
F. DISPUTES AND REMEDIES
1. Representatives of POs and/or Practices and MDHHS shall discuss any dispute issues and negotiate in good faith in an effort to resolve a dispute without the necessity of any formal proceeding. During the course of dispute resolution, all reasonable requests made by one party to another for non-privileged information reasonably related to the Agreement will be honored in order that each of the parties may be fully advised of the other’s position. Each party agrees to continue performing its obligations under the Agreement while a dispute is being resolved, except to the extent the issue in dispute precludes performance (dispute over payment must not be deemed to preclude performance) and without limiting either party’s right to terminate the Agreement as provided elsewhere in this Agreement.
2. The following issues are not subject to the dispute resolution process described in Section F.1:
a. The MiPCT Model (see Appendix E).b. The MiPCT PCMH Infrastructure Requirements (see Appendix D).c. Required Business Associate and Data Use Agreements.d. Training and Education Requirements for MiPCT Care Managers and Practice
14
Care Teams (see Appendices F and G).e. MDHHS decision to terminate a PO, Practice or Provider from the Project.f. CMS Requirements of States Participating in the Multi-Payer Advanced Primary
Care Practice (MAPCP) Demonstration Project.
G. MISCELLANEOUS PROVISIONS
1. Governing law: This Agreement shall be governed by and construed according to the laws of the State of Michigan.
2. Amendments: This Agreement cannot be amended without the consent of MDHHS.
3. Access to Information and Records: All Project Participants shall provide MDHHS with access to such information and records consistent with relevant federal and state law as may be necessary to assess appropriate reimbursement levels and to otherwise monitor and evaluate the Project.
4. Record Maintenance/Retention: This agreement requires that all participating parties maintain adequate program and financial records and files, include source documentation to support program activities and all expenditures made under the terms of this agreement, as required. Assure that all terms of the agreement will be appropriately adhered to and that records and detailed documentation for the Project identified in this Agreement will be maintained for a period of not less than three (3) years from the date of termination, the date of submission of the final expenditure or until litigation and audit findings have been resolved.
5. Authorized Access and Audit: Permit upon reasonable notification and at reasonable times, access by representatives of the MDHHS, CMS, Comptroller General of the United States, and State Auditor General, any Participating Payer, or any of their duly authorized representatives, upon presentation of documentation to PO or Practice which verifies such representatives’ authorization, to records, files and documentation related to this agreement, to the extent authorized by applicable state or federal law, rule or regulation.
6. Agreement Termination: MDHHS may suspend or terminate this Agreement with a PO or a Practice or a Provider under any of following circumstances or for other reasonable cause:
a. The PO and/or Practice no longer complies with the requirements set forth in this Agreement, subsequent to written notice and opportunity to comply.
b. The PO and/or Practice fails to provide reasonable and necessary services in accordance with professional standards.
c. A Practice is convicted of fraud or a felony.d. A Provider within a Practice is convicted of fraud or a felony. e. A Practice is sanctioned by Medicare or Medicaid.f. A Provider within a Practice is sanctioned by Medicare or Medicaid. g. Revocation of a Provider’s medical license.
7. Procedure for Termination by MiPCT: A termination will be effective sixty (60) days
15
after written notice from MDHHS to the PO or Practice. MDHHS will determine if any semi-annual Incentive Payment is due to a PO or Practice.
a. If the Practice is unable to maintain all MiPCT PCMH Infrastructure Requirements as well as all other provisions in this Agreement, MDHHS has sole authority to make a final determination regarding continued participation status or termination of the Practice from the Project.
b. If a Practice is terminated, MDHHS will inform the Practice and the PO, and will notify all Payers to suspend any future payments under the Demonstration Project.
8. Procedure for PO/Practice Withdrawal from Project: A PO or Practice may end its participation in the Project by providing sixty (60) days written notice of its intent to withdraw to MDHHS and by completing a MiPCT Physician and Practice Change Form and forwarding this to the MiPCT Demonstration Mailbox at: [email protected]. Providers are obligated to continue to provide all PCMH services through the end of the effective date of their elected termination.
a. A Payer shall be responsible for paying the Practice for Practice Transformation and Care Coordination Payment obligations incurred prior to the termination date.
b. A Payer providing reimbursement to the Practice shall not be required to pay any Practice Transformation or Care Coordination payments for services rendered after the termination date.
c. A PO or a Practice that terminates participation in the Demonstration during Project Year Four shall not be eligible for Performance Incentive payments earned before the termination date if the termination date falls before the mid-point of the Incentive Period.
9. Termination by Payer: Nothing in this Agreement shall be construed to disallow a Payer from terminating its relationship with a clinician, subject to the contractual terms of an independent agreement with that clinician. Nothing in this Agreement shall prevent a Payer from seeking recovery of payments made after the effective date of termination.
10. Insurance Coverage: Participating Practices shall maintain the types and amounts of insurance coverage as they deem necessary for their protection. Nothing contained herein shall constitute an agreement by the State of Michigan to provide legal representation or liability coverage to Participating Practices.
16
SPECIAL CERTIFICATION
The individual or officer signing this 2016 Participation Agreement certifies by his or her signature that he or she is authorized to sign this agreement on behalf of the responsible governing board, official or contractor, and agrees to abide by the specific responsibilities outlined herein.
Attached to the Participation Agreement are Attachments I and II – the Business Associate Agreement (BAA) that is new for 2015was signed in Year Four and the Data Use Agreement (DUA) that was signed in Year One or Year Two or Year Three or Year Four. both of which must be signed by anIf the individual authorized to sign such agreementswho signed the Business Associate Agreement (BAA). If the signature on the and Data Use Agreement (DUA)that was signed in Year One or Year Two or Year Three is still in a position to commit the Physician Organization to thecurrent, that Agreement terms, a new BAA or DUA does not need to be signed. is included as Attachment II to this Participation Agreement. Otherwise, a new BAA or DUA must be signed. The Physician Organization will continue to abide by the terms in those agreements in 2016.
SIGNATURE SECTION
For the Michigan Department of Health and Human Services:
Kim Stephen Director, Bureau of Budget and PurchasingName Title
Signature Date
For [Insert Name of PO]:
Name (print) Title (pri nt)
Signature Date
17
SPECIAL CERTIFICATION
The individual or officer signing this 2016 Participation Agreement certifies by his or her signature that he or she is authorized to sign this agreement on behalf of the responsible governing board, official or contractor, and agrees to abide by the specific responsibilities outlined herein.
Attached to the Participation Agreement are Attachments I and II – a the Business Associate Agreement (BAA) that was signed in Year Fouris new for 2015, and a Data Use Agreement (DUA) that was signed in Year One or Year Two or Year Three or Year Four. If the individual who signed the Business Associate Agreement (BAA) and Data Use Agreement (DUA) in Year One or Year Two or Year Three is still current and that individual is still in a position to commit the Practice to the Agreement terms (see Attachment II to this Agreement), a new BAA or DUA does not need to be signed. Otherwise, a new BAA or DUA must be signed. The Practice will continue to abide by the terms in those agreements in 2016.
SIGNATURE SECTION
For the Michigan Department of Health and Human Services:
Kim Stephen Director, Bureau of Budget and PurchasingName Title
Signature Date
For the (Name of Practice):
Name (print) Title (pri nt)
Signature Date
18
APPENDIX A
MiPCT DEMONSTRATION PAYMENT MODEL
MiPCT Demonstration Payment fees are designed to provide financial support to participating PCMH Practices and POs to enable them to develop and/or strengthen advanced capabilities for delivering patient-centered care, i.e., PCMH infrastructure development and proactive, effective patient-centered services that can improve patient outcomes, provide better experiences of care, and reduce unnecessary healthcare costs.
MiPCT payments will be calculated on a per member per month basis. Attribution to Primary Care Providers for Medicare and for non-HMO commercially-insured patients will be done according to the model in Appendix B.
A MiPCT funding and crediting process is used to identify the amount of funds Payers currently are investing in support of PCMH transformation that corresponds to one or more of the MiPCT payment components. Credited funds are made available to participating Practices/POs, but may decrease the total amount of new dollars an individual Payer is expected to contribute.
If revenues substantially exceed expected and approved MiPCT expenses, MDHHS reserves the right to suspend Medicaid and Medicare payments until expenses and revenues are aligned.
1. A Practice Transformation Payment of $1.50 per member per month (PMPM) paid monthly, quarterly or an equivalent amount paid as an E & M uplift** ($2.00 for Medicare) will be paid to the Practice. These funds are expected to be used to provide funding to Practices to offset infrastructure requirements related to MiPCT goals, e.g., incremental additional costs related to registry or EHR enhancements to meet MiPCT reporting requirements; expense of physician and staff time to attend Learning Collaboratives or other MiPCT-approved training opportunity; staff training; staffing costs associated with front office and team support of Care Managers; implementing extended office hours; proactive outreach by staff to patients to close gaps in care; overtime pay for data entry into a registry or EMR.
2. A Care Coordination Payment of $3.00 PMPM paid monthly or quarterly for Medicaid patients and $4.50 PMPM for Medicare patients will be paid to the PO. BCBSM, BCN and Priority Health will pay Care Management via G and CPT care management codes to the PO or practice (depending upon the billing entity). This may be more or less than $3.00 PMPM depending on the volume of care management claims billed and paid.
3. A semi-annual retrospective Performance Incentive payment of variable amount, based on the extent to which performance criteria are met, will be paid to the PO. The PO will assure that no less than 80% of the Performance Incentive payments received are distributed to its participating Practices. These funds are intended to reward achievement of PCMH services and metrics specified in the Performance Incentive Plan for Year Four. Payers will contribute $3.00 PMPM to the performance incentive pool and all funds for each six-month period will be paid out during that period.
4. Payers also will contribute $0.26 PMPM for central administrative costs to manage the Project.
** Medicare will make monthly PMPM payments. Medicaid will make quarterly payments. Blue Cross will pay an E&Muplift and will base Care Coordination payments on G codes submitted. Priority Health will pay on G and CPT codes.
19
APPENDIX B
I. Primary Care Attribution Methodology for all Participating Payers
a. Payments will conform to a common Attribution Model. For Medicaid managed care and other HMO participating payers, members are attributed based on their designated primary care provider (PCP). For commercial insurers, attribution calculations can be performed centrally via the Michigan Data Collaborative or at the individual Payer level. All Medicare Fee-For-Service beneficiaries will be included.
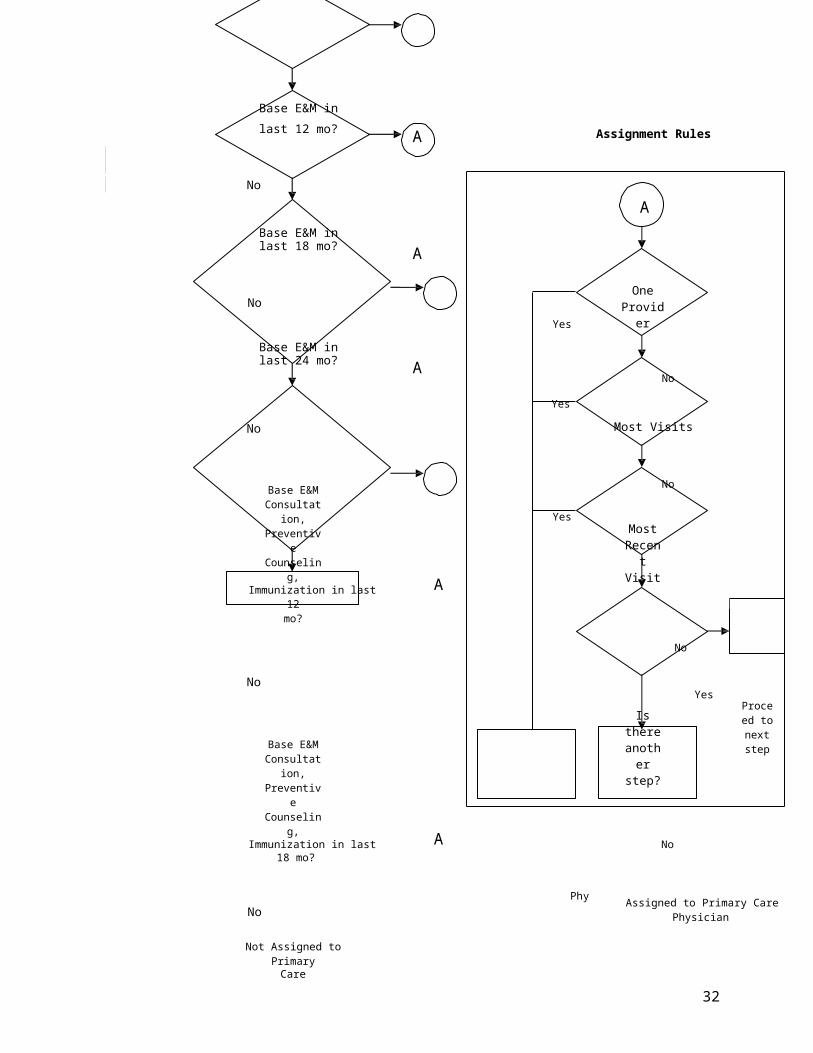
b. To ensure that the most recent available claims history determines attribution, a five-step tiered attribution process will be used (Figure 1). The first tier will assign care relationships based on twelve months of claims history using the base Evaluation and Management (E&M) procedure codes. When members are not assigned in the first tier, the process will then progress to the second tier and will include 18 months of claimshistory using only the base E&M procedure codes. Members still not assigned will progress into the third tier where 24 months of claims history and the base E&M codes will be used for care relationship assignment. Members not assigned in the three tiers of expanded claims history will progress into the fourth tier of the care assignment process, which will use twelve months of claims history with the addition of procedure codes for consultations, preventive counseling, and immunizations. The fifth and final tier will use 18 months of claims history with the expanded list of procedure codes.
c. Eligible procedure codes will include base E&M codes, with the addition of consultations performed by primary care specialties, preventive counseling and immunizations performed in an outpatient or office setting. This includes consultations performed by primary care specialties enabling relationship assignments when base E&M codes are absent. Preventive counseling codes and immunizations represent activities often associated with primary care. The inclusion of these procedure code groups will lead to an estimated gain of two percent of eligible members assigned a primary care relationship.
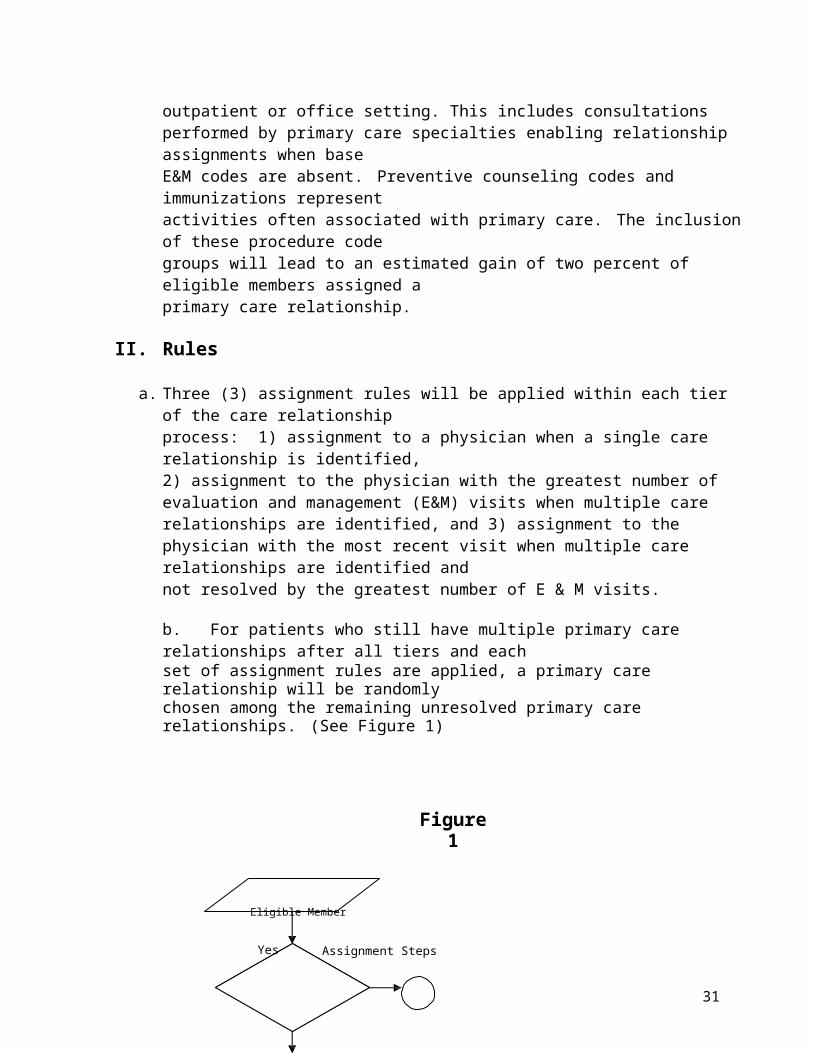
II. Rules
a. Three (3) assignment rules will be applied within each tier of the care relationship process: 1) assignment to a physician when a single care relationship is identified, 2) assignment to the physician with the greatest number of evaluation and management (E&M) visits when multiple care relationships are identified, and 3) assignment to the physician with the most recent visit when multiple care relationships are identified and not resolved by the greatest number of E & M visits.
b. For patients who still have multiple primary care relationships after all tiers and eachset of assignment rules are applied, a primary care relationship will be randomly chosen among the remaining unresolved primary care relationships. (See Figure 1)
20
Figure 1
Eligible Member
Yes Assignment Steps
Base E&M inlast 12 mo? A Assignment Rules
No
ABase E&M inlast 18 mo? A
No
Base E&M inlast 24 mo? A
Yes
OneProvider
No
Yes
No Most Visits
Base E&M Consultation,
Preventive Counseling,
Immunization in last A12 mo?
Yes
No
Most Recent Visit
No
No
Base E&M Consultation,
Preventive Counseling,
Is there another step?
YesProceed to next
step
Immunization in last A No18 mo?
No
Not Assigned to PrimaryCare Physician
Assigned to Primary Care
Physician
Randomly Assigned to
Primary Care Physician
21
APPENDIX C
MiPCT ORGANIZATIONAL RELATIONSHIPS
PAYERS (Medicare, Medicaid and Commercial)
VENDORSUMHS
MI DataCollaborative
CHEAR
MPHI
MDHHS(MiPCT Core Team)
POs/PHOs/IPAs
PRACTICES
MiPCT Steering
Committee
ADVISORSPatient Advisory
Council
22
APPENDIX D
MiPCT PCMH Infrastructure Requirements
The following capabilities required to be in place by end of Year One, must be maintained throughout 2016:
1. All-Payer, All-Patient Registry or Registry Functionality. A patient registry is an electronic database that contains demographic and clinical data (in data fields accessible for tabulation and population management) on all patients served by the Practice to enable physicians and staff to manage their populations of patients. The Registry may be a component of an EHR for basic-level functioning, as long as the Practice or the PO has the capability to use the EHR to generate population-level performance reports and identify subsets of patients requiring active management. Practices must have electronic systems in place capable of providing decision support prompts and care alerts and able to track evidence-based care for the following:
a. Age and gender-appropriate preventive care i. Smoking status
ii. Mammograms iii. Pap smearsiv. Colorectal cancer screeningv. Immunizations (MCIR may be used to track immunizations if practice level reports
are generated to identify individuals for outreach who are due or past due for immunizations)
b. Chronic illness care for prevalent conditions: i. Diabetes: AIC levels, blood pressure, retinal exam
ii. Hypertension: Blood pressureiii. Coronary Artery Disease and CHF: Blood pressure, LDL-C levels iv. Obesity: BMIv. Asthma: Self-management plan or asthma action plan
vi. Depression: Screening for those with chronic conditions
c. Identify gaps in care and generate communications to patients regarding needed care.
d. Generate clinical metric reports for use in assessing and improving care forsub-populations of patients.
e. Record patient’s demographic information including age, sex, race/ethnicity and link, if possible, with their clinical data. If a direct link is not currently possible, a description of a work around process and/or a plan with timeline for achieving the link will suffice.
2. Care Management Documentation Tools built into EHR/registry products or separate software.
3. Advanced Accessa. 24-hour access to a Clinical Decision Maker, i.e., MD, DO, NP or PA. b. Access to after-hours urgent care for at least 12 hours per week.c. 30% of appointments reserved for same-day care across the patient population or acceptable
alternative.
Complex Care Management Functional Tier 4
All Tier 1-2-3 services plus: Home care team Comprehensive care plan Palliative and end-of life care
Care Management
Functional Tier 3
All Tier 1-2 services plus: Planned visits to optimize
chronic conditions Self-management support Patient education Advance directives
Transition Care
Functional Tier 2
All Tier 1 services plus: Notification of admit/discharge PCP and/or specialist follow-up Medication reconciliation
Navigating the MedicalNeighborhood
Functional Tier 1
Optimize relationships with specialists and hospitals
Coordinate referrals and tests Link to community resources
Prepared Proactive Healthcare TeamEngaging, Informing and Activating Patients
P O P U L A T I O N M A N A G E M E N T
23
APPENDIX E
Michigan Primary Care Transformation Project Advancing Population Management
PCMH Services PCMH Infrastructure
Health IT- Registry / EHR registry functionality *- Care management documentation *- E-prescribing (optional)- Patient portal (advanced/optional)- Community portal/HIE (adv/optional)- Home monitoring (advanced/optional)
Patient Access- 24/7 access to decision-maker *- 30% open access slots *- Extended hours *- Group visits (advanced/optional)- Electronic visits (advanced/optional)
Infrastructure Support- PO/PHO and practice determine
optimal balance of shared support- Patient risk assessment- Population stratification- Clinical metrics reporting
*denotes requirement by end of year 1
APPENDIX F
20156 MiPCT Learning Activity Requirements
Care Manager Learning RequirementEach Care Manager must complete a total of twelve (12) hours of Care Manager education per year. This can be satisfied by either:
a. Twelve (12) hours of MiPCT-led Care Manager webinars/sessions (e.g., Annual MiPCT Summit Care Manager Skill Building), OR
b. Six (6) hours of MiPCT-led Care Manager webinars/sessions PLUS six (6) hours of PO-led Care Manager training per year. No preapproval is necessary for PO-led Care Manager training sessions.
Practice Learning RequirementEach Practice’s Care Team (including one or more Physicians from the Practice, the Care Manager PLUS one or more other Practice Care Team members) must complete:
[1.] Eight (8) hours of learning activity requirements during calendar year 20156. Note: MiPCT will finalize all additional practice learning activities, based on needs identified by the MiPCT Physician Organizations, by 2nd Quarter 2015. The learning activities below along with any additional practice learning activities identified by the end of Quarter 2, 2015, will remain in place for the entire calendar year. The following activities do not require preapproval to be counted toward the Practice’s Learning Activity Requirement: a.
a. Annual MiPCT Summit Participation (4 hours) (To receive credit the Practice Team as defined above, including the Physician must attend.)b.
b. Billing Learning Collaborative (4 hours) Attendance at in-person session and submission of pre-work from team including Care Manager and front office/billing/coding team member(s) (but not Physician) as well as participation in monthly team webinars and metric reporting on Practice billing and coding goals for a minimum of eight (8) months. (Note: Physician involvement from each Practice team would require active participation in one Physician-focused billing webinar.) c.
c. Appropriateness/Choosing Wisely MiPCT Initiative Participation (4 2 hours)** (To receive credit the Practice Team as defined above, including the Physician must attend.)
This learning option may be offered, based on resource availability and stakeholder interest. If it is operationalized, it will be announced in the MiPCT FLASH.
23
d. d. Practice-Based Patient and Family Advisors (“Voice of the Patient” Initiative). This option includes operating PO- or Practice-based Patient Councils or Advisor Programs (up to 4 hours credit per year if council meetings/advisor feedback is accomplished at least quarterly). (To receive credit, the Physician must attend at least two of the four Patient Advisor meetings per year.).e. Social Determinants of Health training (2 hours) This option consists of training to assist practice team members with knowledge and use of resources available to help patients who have needs with food, transportation, housing, etc. f. Collaborative Behavioral Health (2 hours) This option consists of shared learning to support behavioral health coordination in practices, including operationalizing the infrastructure and standard processes and roles, as well as coordination with a consulting psychiatrist/expert.
g.
[d.] e. Sustainability Planning (2 hours) This option consists of training and support to ensure that the practice formalizes and incorporates into daily work and processes the improvements made during the demonstration, and provides for continuation after the demonstration period ends,
h. Physician Champion Leadership Training (2 hours) This option consists of Physician to Physician training and best practice sharing that supports team-based care and embedded Care Management. This learning option may be offered, based on resource availability and stakeholder interest. If it is operationalized, it will be announced in the MiPCT FLASH.
i. i . Submission of formal best practice consisting of documentation that includes the underlying policy, process, workflow, data illustrating the implementation and improvement resulted from results, standardized tool, protocol, and a contact person willing to take questions from other POs and Practices. (2 points for submission). In addition to the above, at the request of MiPCT Leadership, presenting at a CM Best Practice, PGIP, Summit, MiPCT Best Practice Webinars and other venues. (4 points for submission, invitation to present from MiPCT Leadership and completion of presentation)**.
[e.] j. f. Physician Champion Leadership Training** (4 hours) This option consists of Physician to
Physician training and best practice sharing that supports team-based care and embedded Care Management.Practice team participates in a site visit (4 points) conducted by MiPCT team members which is focused on identification of processes and work flows contributing to the delivery of population health management and/or care management. Site visit participants may include: MiPCT Care Manager, Physician from the Practice, Practice manager, PLUS one or more other Practice Care Team members.
1.[2.] [3.] Alternatively, POs and Practices may elect to apply to conduct their own activities
consistent with MiPCT goals. These require preapproval using the form available at: http://mipctdemo.wordpress.com/resources/mipct-documents-and-presentations/mipct-learning-activity-approval-form. Submit completed form at least
23
four weeks prior to the event to: [email protected]. (See Appendix G.)
3. POs should be prepared to provide information on how the learning requirements were met on their quarterly narrative report.
** Additional details and scheduling will be available in early 2015.
23
APPENDIX G
Guidelines for Approval of non-MiPCT-Sponsored Proposed Learning Activity
Requests for approval of "Other MiPCT Learning Activities" must:
a. Address at least one of the MiPCT functional tiers (see Appendix A).
b. Be attended by at least one Care Team in the Practice including, at a minimum, a Physician, Care Manager, and at least one other Practice member.
c. If the activity provides continuing medical education credits for Physician, Care Manager or other clinicians, provide details of which team members are eligible for credits and the accrediting body. Applications for activities that provide CME or CEU credits and that are directly related to one or more MiPCT functional tiers will strengthen the application and are more likely to receive approval.
d. In addition, Learning Activities related to palliative care, end of life, and wise use of resources (e.g., Choosing Wisely) are especially encouraged.
e. Complete the form at the following website regarding the proposed Learning Activity: http://mipctdemo.wordpress.com/resources/mipct-documents-and-presentations/mipct-learning-activity-approval-form.
f. Submit the completed form to [email protected] mailbox at least four weeks prior to the activity.
25
ATTACHMENT I
HIPAA BUSINESS ASSOCIATE AGREEMENT ADDENDUM
This Business Associate Agreement Addendum (“Addendum”) is made a part of the contract (“Contract”) between the Michigan Department of Health and Human Services (“Covered Entity”), and __________________________________________, (“Business Associate”).
The Business Associate performs certain services for the Covered Entity under the Contract that requires the exchange of information including protected health information under the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”), as amended by the American Recovery and Reinvestment Act of 2009 (Pub.L. No. 111-5). The Michigan Department of Health and Human Services is a hybrid covered entity under HIPAA and the parties to the Contract are entering into this Addendum to establish the responsibilities of both parties regarding HIPAA-covered information and have the underlying Contract comply with HIPAA.
RECITALS
A. Under the terms of the Contract, the Covered Entity wishes to disclose certain information to the Business Associate, some of which may constitute Protected Health Information (“PHI”). In consideration of the receipt of PHI, the Business Associate agrees to protect the privacy and security of the information as set forth in this Addendum.
B. The Covered Entity and the Business Associate intend to protect the privacy and provide for the security of PHI disclosed to the Business Associate under the Contract in compliance with HIPAA and the HIPAA Rules.
C. The HIPAA Rules require the Covered Entity to enter into a contract containing specific requirements with the Business Associate before the Covered Entity may disclose PHI to the Business Associate.
1. Definitions.
a. The following terms used in this Agreement have the same meaning as those terms in the HIPAA Rules: Breach; Data Aggregation; Designated Record Set; Disclosure; Health Care Obligations; Individual; Minimum Necessary; Notice of Privacy Practices; Protected Health Information; Required by Law; Secretary; Security Incident; Security Measures, Subcontractor; Unsecured Protected Health Information, and Use.
b. “Business Associate” has the same meaning as the term “business associate” at 45 CFR 160.103 and regarding this Addendum means [Insert Name of Business Associate]
26
c. “Covered Entity” has the same meaning as the term “covered entity” at 45 CFR 160.103 and regarding this Addendum means the Michigan Department of Health and Human Services.
d. “HIPAA Rules” means the Privacy, Security, Breach Notification, and Enforcement Rules at 45 CFR Part 160 and Part 164.
e. “Agreement” means both the Contract and this Addendum.
f. “Contract” means the underlying written agreement or purchase order between the parties for the goods or services to which this Addendum is added.
2. Obligations of Business Associate.
The Business Associate agrees to
a. use and disclose PHI only as permitted or required by this Addendum or as required by law.
b. implement and use appropriate safeguards, and comply with Subpart C of 45 CFR 164 regarding electronic protected health information, to prevent use or disclosure of PHI other than as provided in this Addendum. Business Associate must maintain, and provide a copy to the Covered Entity within 10 days of a request from the Covered Entity, a comprehensive written information privacy and security program that includes security measures that reasonably and appropriately protect the confidentiality, integrity, and availability of PHI relative to the size and complexity of the Business Associate’s operations and the nature and the scope of its activities.
c. report to the Covered Entity within 24 hours of any use or disclosure of PHI not provided for by this Addendum of which it becomes aware, including breaches of Unsecured Protected Health Information as required by 45 CFR 164.410, and any Security Incident of which it becomes aware. If the Business Associate is responsible for any unauthorized use or disclosure of PHI, it must promptly act as required by applicable federal and State laws and regulations. Covered Entity and the Business Associate will cooperate in investigating whether a breach has occurred, to decide how to provide breach notifications to individuals, the federal Health and Human Services’ Office for Civil Rights, and potentially the media.
d. ensure, according to 45 CFR 164.502(e)(1)(ii) and 164.308(b)(2), if applicable, that any subcontractors that create, receive, maintain, or transmit PHI on behalf of the Business Associate agree to the same restrictions, conditions, and requirements that apply to the Business Associate regarding such information. Each subcontractor must sign an agreement with the Business Associate containing substantially the same provisions as this Addendum and further identifying the Covered Entity as a third party beneficiary of the agreement with the subcontractor. Business
27
Associate must implement and maintain sanctions against subcontractors that violate such restrictions and conditions and must mitigate the effects of any such violation.
e. make available PHI in a Designated Record Set to the Covered Entity within 10 days of a request from the Covered Entity to satisfy the Covered Entity’s obligations under 45 CFR 164.524.
f. within ten days of a request from the Covered Entity, amend PHI in a Designated Record Set under 45 CFR § 164.526. If any individual requests an amendment of PHI directly from the Business Associate or its agents or subcontractors, the Business Associate must notify the Covered Entity in writing within ten days of the request, and then, in that case, only the Covered Entity may either grant or deny the request.
g. maintain, and within ten days of a request from the Covered Entity make available the information required to enable the Covered Entity to fulfill its obligations under 45 CFR § 164.528. Business Associate is not required to provide an accounting to the Covered Entity of disclosures : (i) to carry out treatment, payment or health care operations, as set forth in 45 CFR § 164.506; (ii) to individuals of PHI about them as set forth in 45 CFR § 164.502; (iii) under an authorization as provided in 45 CFR § 164.508; (iv) to persons involved in the individual’s care or other notification purposes as set forth in 45 CFR § 164.510; (v) for national security or intelligence purposes as set forth in 45 CFR § 164.512(k)(2); or (vi) to correctional institutions or law enforcement officials as set forth in 45 CFR § 164.512(k)(5); (vii) as part of a limited data set according to 45 CFR 164.514(e); or (viii) that occurred before the compliance date for the Covered Entity. Business Associate agrees to implement a process that allows for an accounting to be collected and maintained by the Business Associate and its agents or subcontractors for at least six years before the request, but not before the compliance date of the Privacy Rule. At a minimum, such information must include: (i) the date of disclosure; (ii) the name of the entity or person who received PHI and, if known, the address of the entity or person; (iii) a brief description of PHI disclosed; and (iv) a brief statement of purpose of the disclosure that reasonably informs the individual of the basis for the disclosure, or a copy of the individual’s authorization, or a copy of the written request for disclosure. If the request for an accounting is delivered directly to the Business Associate or its agents or subcontractors, the Business Associate must forward it within ten days of the receipt of the request to the Covered Entity in writing.
h. to the extent the Business Associate is to carry out one or more of the Covered Entity’s obligations under Subpart E of 45 CFR Part 164, comply with the requirements of Subpart E that apply to the Covered Entity when performing those obligations.
i. make its internal practices, books, and records relating to the Business Associate’s use and disclosure of PHI available to the Secretary for purposes of determining compliance with the HIPAA Rules. Business Associate must concurrently provide to the Covered Entity a copy of any PHI that the Business Associate provides to the Secretary.
28
j. retain all PHI throughout the term of the Agreement and for a period of six years from the date of creation or the date when it last was in effect, whichever is later, or as required by law. This obligation survives the termination of the Agreement.
k. implement policies and procedures for the final disposition of electronic PHI and the hardware and equipment on which it is stored, including but not limited to, the removal of PHI before re-use.
l. within ten days after a written request by the Covered Entity, the Business Associate and its agents or subcontractors must allow the Covered Entity to conduct a reasonable inspection of the facilities, systems, books, records, agreements, policies and procedures relating to the use or disclosure of PHI under this Addendum for the purpose of determining whether the Business Associate has complied with this Addendum; provided, however, that: (i) the Business Associate and the Covered Entity must mutually agree in advance upon the scope, timing and location of such an inspection; (ii) the Covered Entity must protect the confidentiality of all confidential and proprietary information of the Business Associate to which the Covered Entity has access during the course of such inspection; and (iii) the Covered Entity or the Business Associate must execute a nondisclosure agreement, if requested by the other party. The fact that the Covered Entity inspects, or fails to inspect, or has the right to inspect, the Business Associate’s facilities, systems, books, records, agreements, policies and procedures does not relieve the Business Associate of its responsibility to comply with this Addendum. The Covered Entity’s (i) failure to detect or (ii) detection, but failure to notify the Business Associate or require the Business Associate’s remediation of any unsatisfactory practices, does not constitute acceptance of such practice or a waiver of the Covered Entity’s enforcement rights under this Addendum.
3. Permitted Uses and Disclosures by the Business Associate.
a. Business Associate may use or disclose PHI:
(i) for the proper management and administration of the Business Associate or to carry out the legal responsibilities of the Business Associate; provided, however, either (A) the disclosures are required by law, or (B) the Business Associate obtains reasonable assurances from the person to whom the information is disclosed that the information will remain confidential and used or further disclosed only as required by law or for the purposes for which it was disclosed to the person, and the person notifies the Business Associate of any instances of which it is aware in which the confidentiality of the information has been breached;
(ii) as required by law; (iii) for Data Aggregation services relating to the health care operations of the Covered
Entity;(iv) to de-identify, consistent with 45 CFR 164.514(a) – (c), PHI it receives from the Covered
Entity. If the Business Associates de-identifies the PHI it receives from the Covered Entity, the Business Associate may use the de-identified information for any purpose not prohibited by the HIPAA Rules; and
(v) for any other purpose listed here: carrying out the Business Associate’s duties under the
29
Contract.
b. Business Associate agrees to make uses and disclosures and requests for PHI consistent with the Covered Entity’s minimum necessary policies and procedures.
c. Business Associate may not use or disclose PHI in a manner that would violate Subpart E of 45 CFR Part 164 if done by the Covered Entity except for the specific uses and disclosures described above in 3(a)(i) and (iii).
4. Covered Entity’s Obligations
Covered entity agrees to
a. use its Security Measures to reasonably and appropriately maintain and ensure the confidentiality, integrity, and availability of PHI transmitted to the Business Associate under the Agreement until the PHI is received by the Business Associate.
b. provide the Business Associate with a copy of its Notice of Privacy Practices and must notify the Business Associate of any limitations in the Notice of Privacy Practices of the Covered Entity under 45 CFR 164.520 to the extent that such limitation may affect the Business Associate’s use or disclosure of PHI.
c. notify the Business Associate of any changes in, or revocation of, the permission by an individual to use or disclose the individual’s PHI to the extent that such changes may affect the Business Associate’s use or disclosure of PHI.
d. notify the Business Associate of any restriction on the use or disclosure of PHI that the Covered Entity has agreed to or is required to abide by under 45 CFR 164.522 to the extent that such restriction may affect the Business Associate’s use or disclosure of PHI.
5. Term. This Addendum must continue in effect as to each Contract to which it applies until such Contract is terminated or is replaced with a new contract between the parties containing provisions meeting the requirements of the HIPAA Rules, whichever first occurs.
6. Termination.
a. Material Breach. In addition to any other provisions in the Contract regarding breach, a breach by the Business Associate of any provision of this Addendum, as determined by the Covered Entity, constitutes a material breach of the Addendum and is grounds for termination of the Contract by the Covered Entity under the provisions of the Contract covering termination for cause. If the Contract contains no express provisions regarding termination for cause, the following apply to termination for breach of this Addendum, subject to 6.b.:
(i) Default. If the Business Associate refuses or fails to timely perform any of the provisions of this Addendum, the Covered Entity may notify the Business Associate in writing of the non-
30

performance, and if not corrected within thirty days, the Covered Entity may immediately terminate the Contract. Business Associate must continue performance of the Contract to the extent it is not terminated.
(ii) Associate’s Duties. Notwithstanding termination of the Contract, and subject to any directions from the Covered Entity, the Business Associate must timely, reasonably and necessarily act to protect and preserve property in the possession of the Business Associate in which the Covered Entity has an interest.
(iii) Compensation. Payment for completed performance delivered and accepted by the Covered Entity must be at the Contract price.
(iv) Erroneous Termination for Default. If the Covered Entity terminates the Contract under Section 6(a) and after such termination it is determined, for any reason, that the Business Associate was not in default, or that the Business Associate’s action/inaction was excusable, such termination will be treated as a termination for convenience, and the rights and obligations of the parties will be the same as if the Contract had been terminated for convenience.
b. Reasonable Steps to Cure Breach. If the Covered Entity knows of a pattern of activity or practice of the Business Associate that constitutes a material breach or violation of the Business Associate’s obligations under the provisions of this Addendum or another arrangement and does not terminate this Contract under Section 6(a), then the Covered Entity must notify the Business Associate of the pattern of activity or practice. The Business Associate must then take reasonable steps to cure such breach or end such violation, as applicable. If the Business Associate’s efforts to cure such breach or end such violation are unsuccessful, the Covered Entity must either (i) terminate this Agreement, if feasible or (ii) if termination of this Agreement is not feasible, the Covered Entity must report the Business Associate’s breach or violation to the Secretary of the Department of Health and Human Services.
c. Effect of Termination. After termination of this Agreement for any reason, the Business Associate, with respect to PHI it received from the Covered Entity, or created, maintained, or received by the Business Associate on behalf of the Covered Entity, must:
(i) retain only that PHI which is necessary for the Business Associate to continue its proper management and administration or to carry out its legal responsibilities;
(ii) return to the Covered Entity (or, if agreed to by the Covered Entity in writing, destroy) the remaining PHI that the Business Associate still maintains in any form;
(iii) continue to use appropriate safeguards and comply with Subpart C of 45 CFR Part 164 with respect to electronic protected health information to prevent use or disclosure of the PHI, other than as provided for in this Section, for as long as the Business Associate retains the PHI;
(iv) not use or disclose the PHI retained by the Business Associate other than for the purposes for which such PHI was retained and subject to the same conditions set out at Section 3(a)(1) which applied before termination; and
(v) return to the Covered Entity (or, if agreed to by the Covered Entity in writing, destroy) the PHI retained by the Business Associate when it is no longer needed by the Business Associate for its proper management and administration or to carry out its legal responsibilities.
31
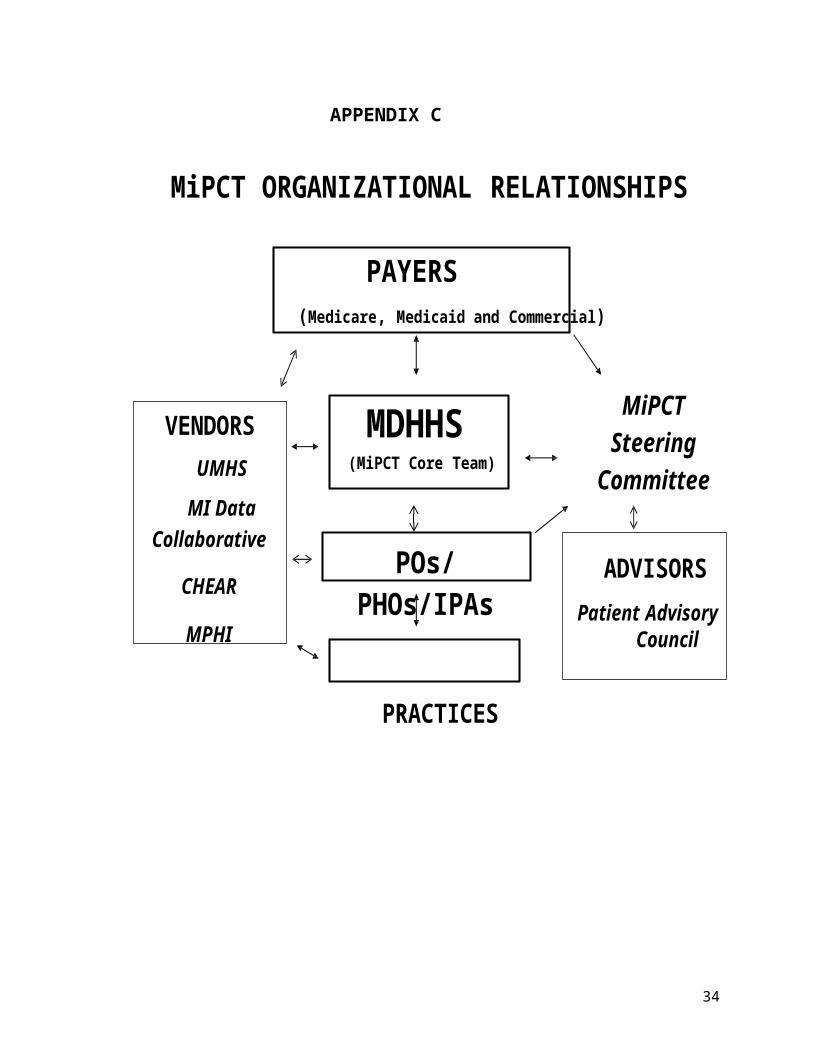
7. No Waiver of Immunity. The parties do not intend to waive any of the immunities, rights, benefits, protection, or other provisions of the Michigan Governmental Immunity Act, MCL 691.1401, et seq., the Federal Tort Claims Act, 28 U.S.C. 2671 et seq., or the common law.
8. Data Ownership. The Business Associate has no ownership rights in the PHI. The covered entity retains all ownership rights of the PHI.
9. Disclaimer. The Covered Entity makes no warranty or representation that compliance by the Business Associate with this Addendum, HIPAA or the HIPAA Rules will be adequate or satisfactory for the Business Associate’s own purposes. Business Associate is solely responsible for all decisions made by the Business Associate regarding the safeguarding of PHI.
10. Certification. If the Covered Entity determines an examination is necessary to comply with the Covered Entity’s legal obligations under HIPAA relating to certification of its security practices, the Covered Entity or its authorized agents or contractors, may, at the Covered Entity’s expense, examine the Business Associate’s facilities, systems, procedures and records as may be necessary for such agents or contractors to certify to the Covered Entity the extent to which the Business Associate’s security safeguards comply with HIPAA, the HIPAA Rules or this Addendum.
11. Amendment.
a. The parties acknowledge that state and federal laws relating to data security and privacy are rapidly evolving and that amendment of this Addendum may be required to provide for procedures to ensure compliance with such developments. The parties specifically agree to take such action as is necessary to implement the standards and requirements of HIPAA and the HIPAA Rules. Upon the request of either party, the other party agrees to promptly enter into negotiations concerning the terms of an amendment to this Addendum embodying written assurances consistent with the standards and requirements of HIPAA and the HIPAA Rules. Either party may terminate the Agreement upon thirty days written notice if (i) the Business Associate does not promptly enter into negotiations to amend this Agreement when requested by the Covered Entity under this Section or (ii) the Business Associate does not enter into an amendment to this Agreement providing assurances regarding the safeguarding of PHI that the Covered Entity, in its sole discretion, deems sufficient to satisfy the standards and requirements of HIPAA and the HIPAA Rules.
12. Assistance in Litigation or Administrative Proceedings. Business Associate must make itself, and any subcontractors, employees or agents assisting Business Associate in the performance of its obligations under this Agreement, available to Covered Entity, at no cost to Covered Entity, to testify as witnesses, or otherwise, if someone commences litigation or administrative proceedings against the Covered Entity, its directors, officers or employees, departments, agencies, or divisions based upon a claimed violation of HIPAA or the HIPAA Rules relating to the Business Associate’s or its subcontractors use or disclosure of PHI under this Agreement, except where the Business Associate or its subcontractor, employee or agent is a named adverse party.
13. No Third Party Beneficiaries. Nothing express or implied in this Addendum is intended to
32
confer any rights, remedies, obligations or liabilities upon any person other than the Covered Entity, the Business Associate and their respective successors or assigns.
14. Effect on Contract. Except as specifically required to implement the purposes of this Addendum, or to the extent inconsistent with this Addendum, all other terms of the Contract must remain in force and effect. The parties expressly acknowledge and agree that sufficient mutual consideration exists to make this Addendum legally binding in accordance with its terms. Business Associate and the Covered Entity expressly waive any claim or defense that this Addendum is not part of the Contract.
15. Interpretation and Order of Precedence. This Addendum is incorporated into and becomes part of the Contract. Together, this Addendum and each separate Contract constitute the “Agreement” of the parties with respect to their Business Associate relationship under HIPAA and the HIPAA Rules. The provisions of this Addendum must prevail over any provisions in the Contract that may conflict or appear inconsistent with any provision in this Addendum. This Addendum and the Contract must be interpreted as broadly as necessary to implement and comply with HIPAA and the HIPAA Rules. The parties agree that any ambiguity in this Addendum must be resolved in favor of a meaning that complies and is consistent with HIPAA and the HIPAA Rules. This Addendum supersedes and replaces any previous separately executed HIPAA addendum between the parties. If this Addendum conflicts with the mandatory provisions of the HIPAA Rules, then the HIPAA Rules control. Where the provisions of this Addendum differ from those mandated by the HIPAA Rules, but are nonetheless permitted by the HIPAA Rules, the provisions of this Addendum control.
16. Effective Date. This Addendum is effective upon receipt of the last approval necessary and the affixing of the last signature required.
17. Survival of Certain Contract Terms. Notwithstanding anything in this Addendum to the contrary, the Business Associate’s obligations under Section 6(d) and record retention laws (“Effect of Termination”) and Section 13 (“No Third Party Beneficiaries”) survive termination of this Addendum and are enforceable by the Covered Entity if the Business Associate fails to perform or comply with this Addendum.
33
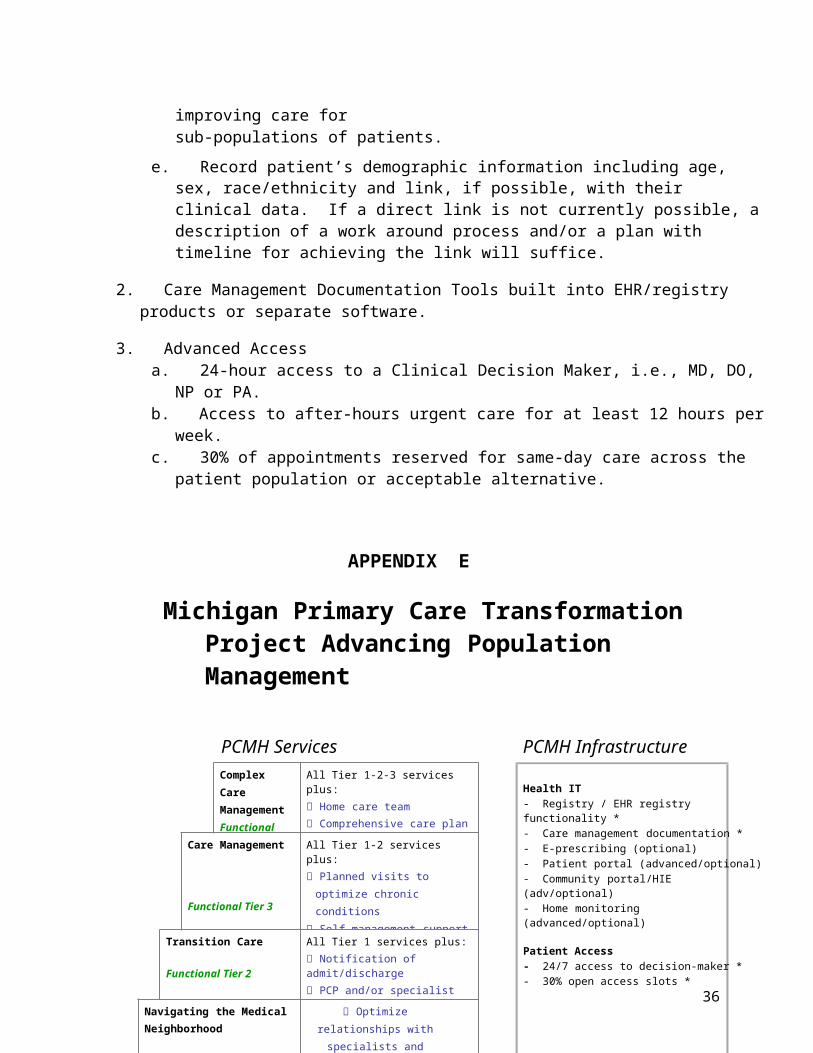
BUSINESS ASSOCIATE AGREEMENT WITH MDHHS: P.O. TO COMPLETE and SIGN:
18. Representatives and Notice.
a. Representatives. For the purpose of this Addendum, the individuals identified in the Contract must be the representatives of the respective parties. If no representatives are identified in the Contract, the individuals listed below are designated as the parties’ respective representatives for purposes of this Addendum. Either party may from time to time designate in writing new or substitute representatives.
b. Notices. All required notices must be in writing and must be hand delivered or given by certified or registered mail to the representatives at the addresses set forth below.
Covered Entity Representative:
Name: Susan Moran
Title: Senior Deputy Director
Department and Division: MDHHS, Public Health Administration
Address: PO Box 30195, Lansing, MI 48909
Business Associate Representative (PO/PHO/IPA):
Name: _________________________ _______________________________
Title: ________________________________________________________________________
Name of PO: ___________________________ ______________________
Address: _____________________________________________________________________
_____________________________________________________________________________
Any notice given to a party under this Addendum must be deemed effective, if addressed to such party, upon: (i) delivery, if hand delivered; or (ii) the third (3rd) Business Day after being sent by certified or registered mail.
Business Associate Covered Entity[SIGNATURE]
By:__________________________________
Date:________________________________
[MDHHS SIGNATURE]
By:____________________________________
Date: __________________________________
Print Name: __________________________ Print Name: Susan Moran
Title: _______________________________ Title: Senior Deputy Director, Public Health
34
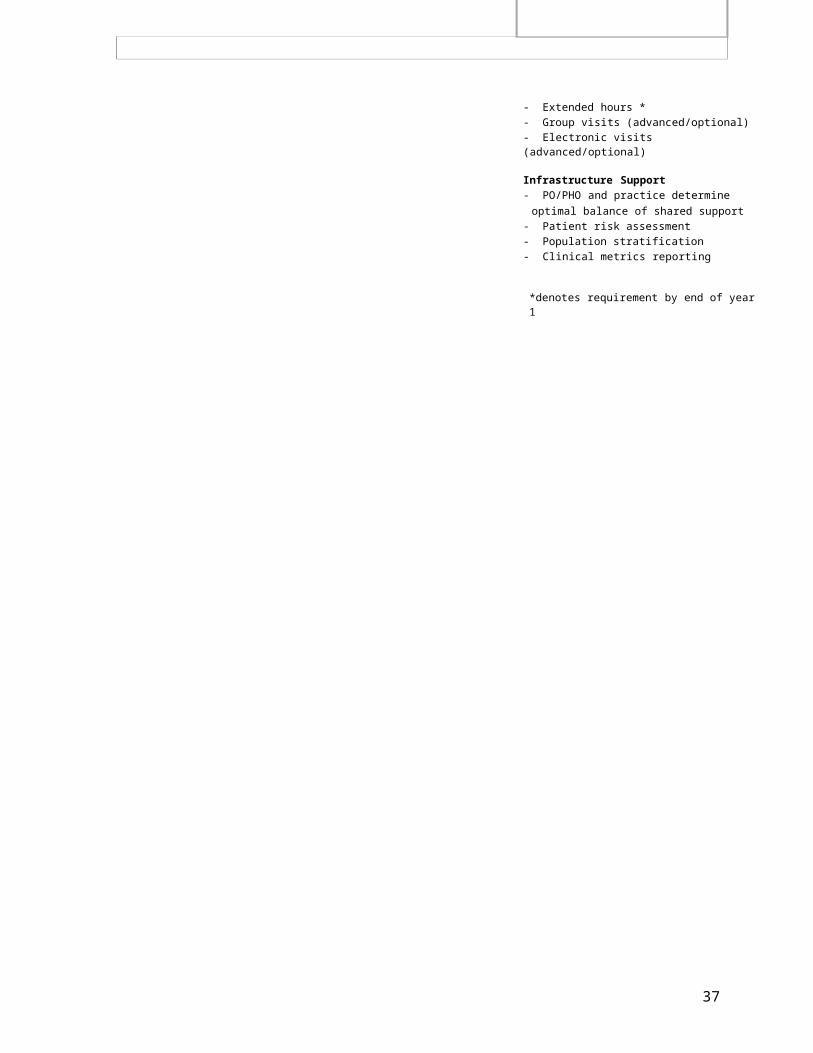
Administration, MDHHSBUSINESS ASSOCIATE AGREEMENT WITH MDHHS: PRACTICE TO COMPLETE and SIGN:
18. Representatives and Notice.
a. Representatives. For the purpose of this Addendum, the individuals identified in the Contract must be the representatives of the respective parties. If no representatives are identified in the Contract, the individuals listed below are designated as the parties’ respective representatives for purposes of this Addendum. Either party may from time to time designate in writing new or substitute representatives.
b. Notices. All required notices must be in writing and must be hand delivered or given by certified or registered mail to the representatives at the addresses set forth below.
Covered Entity Representative:
Name: Susan Moran
Title: Senior Deputy Director
Department and Division: MDHHS, Public Health Administration
Address: PO Box 30195, Lansing, MI 48909
Business Associate Representative (PRACTICE):
Name: _________________________ _______________________________
Title: ________________________________________________________________________
Name of Practice: ___________________________ ___________________
Address: _____________________________________________________________________
_____________________________________________________________________________
Any notice given to a party under this Addendum must be deemed effective, if addressed to such party, upon: (i) delivery, if hand delivered; or (ii) the third (3rd) Business Day after being sent by certified or registered mail.
Business Associate Covered Entity[SIGNATURE]
By:__________________________________
Date:________________________________
[MDHHS SIGNATURE]
By:____________________________________
Date: __________________________________
Print Name: __________________________ Print Name: Susan Moran
Title: _______________________________ Title: Senior Deputy Director, Public Health35
Administration, MDHHS
36
ATTACHMENT II
DATA USE AGREEMENT(insert signed Data Use Agreement here with PO and its Practices)
37







![ANDS · Web view2016-08-29 · Certificate Of Participation [Recipient Name] is thanked for their participation in . 23 (research data) Things](https://img.pdfslide.us/doc/110x75/5f21453753aa0a17882afd14/web-view-2016-08-29-certificate-of-participation-recipient-name-is-thanked-for.jpg)





















