Embed Size (px)
Citation preview

www.elsevier.com/locate/braindev
Brain & Development 30 (2008) 425–429
Case report
Partial monosomy Xq(Xq23 fi qter) and trisomy4p(4p15.33 fi pter) in a woman with intractable focal
epilepsy, borderline intellectual functioning,and dysmorphic features
Arnaldo Bartocci a, Pasquale Striano b,c, Maria Margherita Mancardi c, Marco Fichera d,Lucia Castiglia d, Ornella Galesi d, Roberto Michelucci e, Maurizio Elia d,*
a Unit of Neurophysiopathology, Hospital of Perugia, Italyb Epilepsy Center, Department of Neurological Sciences, Federico II University, Napoli, Italy
c Muscular and Neurodegenerative Disease Unit, Institute ‘‘G. Gaslini’’, University of Genova, Genova, Italyd Oasi Institute for Research on Mental Retardation and Brain Aging (IRCCS), Via Conte Ruggero, 73, 94018 Troina, EN, Italy
e Department of Neurosciences, Bellaria Hospital, Bologna, Italy
Received 30 August 2007; received in revised form 19 November 2007; accepted 20 November 2007
Abstract
Studies of epilepsy associated with chromosomal abnormalities may provide information about clinical and EEG phenotypes andpossibly to identify new epilepsy genes. We describe a female patient with intractable focal epilepsy, borderline intellectual function-ing, and facial dysmorphisms, in whom genetic study (i.e., karyotype and array-CGH analysis) revealed a distal trisomy 4p and dis-tal monosomy Xq. Although any genetic hypothesis remains speculative, several genes are located in the 4p chromosome segmentinvolved in the rearrangement, some of which may be related to epilepsy.� 2007 Elsevier B.V. All rights reserved.
Keywords: Epilepsy; Chromosome abnormalities; Trisomy 4p; Monosomy Xq; Array-CGH
1. Introduction
The mechanisms of chromosomal imbalances associ-ated with epilepsy are of considerable neurobiologicinterest as dosage imbalances might, for some neuronalgenes, lay the basis for the observed epilepsy phenotypes[1,2]. Here we report a female patient with intractablefocal epilepsy, borderline intellectual functioning, andfacial dysmorphisms and in whom genetic studyrevealed a distal trisomy 4p and distal monosomy Xq.
0387-7604/$ - see front matter � 2007 Elsevier B.V. All rights reserved.
doi:10.1016/j.braindev.2007.11.004
* Corresponding author. Tel.: +39 0935 936111; fax: +39 0935653327.
E-mail address: [email protected] (M. Elia).
2. Case report
This 22-year-old woman is the first child of unrelatedparents. Family history was unremarkable but themother experienced few brief episodes of gastric auraand deja vu inconstantly followed by loss of conscious-ness during the adolescence. These symptoms were sug-gestive of mild temporal lobe epilepsy and were easilycontrolled by carbamazepine at low doses. The patientwas born at term after a normal pregnancy. Growthmeasurements at birth were normal. Developmentalstages were delayed: she started to walk at age18 months and started using single words at age24 months. Between ages 18 and 20 months, episodesof fallings to the ground occurred more times a day,

426 A. Bartocci et al. / Brain & Development 30 (2008) 425–429
more often provoked by sudden uditive stimuli, withoutimpairment of consciousness. No therapy was given.From age 5 years, the patient experienced prolonged(>60 s), nocturnal seizures characterized by abruptarousal, vocalization, flexion of the head, trunk, andarms, usually occurring in clusters, with frequency upto 1–2 episodes/week. Seizures could occur also atawake, spontaneously or evoked by uditive stimuli,and sometimes followed by falling. Therapy with viga-batrin and clobazam did not give significant benefitand, at age 7 years, the patient manifested daily, brief(<40 s) seizures characterized by sudden left flexion ofthe head, hypertonus and extension of the upper limbs,without loss of consciousness. At age 9 years, she wasreferred to our clinic. Physical examination revealedhypertelorism, bushy eyebrows, broad nasal bridge,short neck and extremities, low frontal hairline, shortand horizontal palpebral fissures, posteriorly rotatedears, bilateral epicanthus, asymmetric face, microgna-thia, high arched palate. The girl was 118 cm tall(<3rd centile), weighed 26 kg (25th–50th centile), andhad a OFC of 51 cm (25th–50th centile). The parents
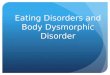
Fig. 1. Ictal EEG recording of a tonic-asymmetric seizure followed by secondsharp waves over the frontal–central regions (A), rapidly followed by seconamplitude delta activity over the anterior regions and sharp- and slow-wave c(C and D).
did not give the consent to show the patient’s face. Neu-rologic examination showed broad-based gait, inten-tional hand tremor, dysmetria, and nystagmus.Neuropsychological testing assessed IQ at 75. Routineblood and urine analyses, lactate and pyruvate levelsin the serum, plasma amino acid concentrations, andlysosomal enzyme activities were normal. InterictalEEG showed slow background activity and isolatedsharp- and slow-wave complexes over left paramediancentral regions, enhanced by sleep deprivation. Withthe video-EEG, we recorded several brief tonic-asym-metric seizures occurring in clusters, usually with pre-served consciousness between the episodes. However,secondary generalization could sometimes occur. Sei-zure onset was accompanied by fast activities and sharpwaves over the frontal–central regions, rapidly followedby secondary generalization. At the end of the seizure,EEG showed high-amplitude delta activity over theanterior regions and sharp- and slow-wave complexesover the vertex and the left paramedian frontal–centralareas (Fig. 1). Brain magnetic resonance imaging(MRI) was unremarkable but spinal cord MRI revealed
ary generalization. Seizure onset was accompanied by fast activities anddary generalization (B). At the end of the seizure, EEG showed high-omplexes over the vertex and the left paramedian frontal–central areas

A. Bartocci et al. / Brain & Development 30 (2008) 425–429 427
occult spinal dysraphism. The patient was under car-bamazepine (400 mg/day) and phenytoin (100 mg/day)and was attending a school for mentally retarded peo-ple. In the following years, several antiepileptic drugs(carbamazepine, oxcarbazepine, topiramate, valproate,phenobarbital, gabapentin, clonazepam, felbamate, phe-nytoin, pregabalin, levetiracetam, zonisamide) – usedsingly or in association – did not allow seizure control.Vagus nerve stimulation was also uneffective. Fromthe age of 20 years, the patient experienced increased sei-zure frequency and several episodes of convulsive statusepilepticus, only partially improved by lamotrigine givenin add-on. The patient refused to undergo functionalstudies such as ictal or interictal 2-[18F]fluoro-2-deoxy-D-glucose positron emission tomography (SPECT) orsingle-photon-emission computed tomography (PET),and magnetoencephalography (MEG) in view of a pos-sible epilepsy surgery.
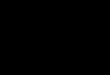
Fig. 2. (A) Array-CGH mapping Xqter deletion (35 Mb from telomere to thfrom the distal ZNF595 to the centromeric MED28 gene. (B) The methylashowed a preferential inactivation (95%) of the paternal rearranged X chrom
3. Genetic study
Routine analysis of G-banded chromosomes (550bands) karyotype from lymphocyte cultures revealed adeletion of the long arm of X chromosome [46,XX,del (X) (q27 fi qter)]. A single array-CGH (aCGH)experiment on the proband was performed using theHuman Genome CGH Microarray Kit 44B (AgilentTechnologies, Palo Alto, CA, USA) which consists of�44,000 60-mer oligonucleotide probes that span bothcoding and non-coding sequences with an average spa-tial resolution of �75 kb. Briefly, 5 lg of DNA fromthe test and a sex-matched pooled normal reference wereprocessed according to the manufacturer’s protocol. Thedye emission capture was performed by a dual-laserscanner. Images were extracted using Agilent FeatureExtraction Software 9.1 and analysed by CGH Analyt-ics 3.4 software. A log ratio plot between test and refer-
e ATP1 gene), and a 17.4 Mb duplication on chromosome 4p spanningtion analysis was assayed at the human androgen receptor locus andosome.

428 A. Bartocci et al. / Brain & Development 30 (2008) 425–429
ence genomic DNA was assigned such that aberrationsin test DNA copy number at a particular locus areobserved as the deviation of the ratio plots from a modalvalue of 0. The aCGH mapped the identified Xqter dele-tion (35 Mb from telomere to the ATP1 gene), but alsounveiled a 17.4 Mb duplication on chromosome 4pspanning from the distal ZNF595 to the centromericMED28 gene (Fig. 2A). The segregation pattern of themicrosatellites located inside the involved regionsexcluded a maternal origin of the rearranged chromo-somes, whereas the unavailability of any biological sam-ple from her father did not allow us to establish whetherthe chromosomal aneuploidy in our patient resultedfrom unbalanced segregation of a paternal balancedtranslocation. To establish the X chromosome inactiva-tion pattern, the methylation analysis was assayed at thehuman androgen receptor locus and showed a preferen-tial inactivation (95%) of the paternal rearranged Xchromosome (Fig. 2B).
4. Discussion
A detailed analysis of the electroclinical pattern ofepilepsy associated with chromosomal disorders canhelp to define the phenotype and to detect genes relatedto seizure susceptibility [1,2]. This patient showed a par-tial monosomy Xq (Xq23 fi qter) and trisomy 4p(4p15.33 fi pter) and presented a typical malformativepicture and drug-refractory epilepsy, with focal and sec-ondarily generalized seizures as well as focal EEGabnormalities. The clinical semiology, with hypermotorsigns, abrupt onset and brief seizures duration, suggestsa frontal lobe origin [3]. It is conceivable that also other(e.g., non-genetic, environmental) factors contributed tothe severe epilepsy phenotype and to its poor prognosis,both in terms of seizure control and evolution. Func-tional studies such as ictal or interictal PET or SPECT,or MEG would have been potentially useful for theidentification of the genuine epileptic focus/i. In addi-tion, these non-invasive investigations could also pro-vide further information in view of a possible epilepsysurgery that should still be taken into consideration inthis patient in spite of the likely genetic origin.
In the propositus, the deletion was of paternal originand the X-inactivation pattern demonstrates that thepaternal rearranged X chromosome is almost com-pletely inactivated, protecting her from partial mono-somy of the Xq. On the other hand, the spread of X-inactivation has been shown to be relatively inefficientin X;autosome translocations [4], suggesting in ourpatient the functional trisomy of the duplicated 4pterregion. The patient’s mother suffered from focal seizuresduring adolescence, but had normal genetic study. Thus,this association is likely a chance event.
More than 75 cases of trisomy 4p have been reportedthus far, most of them due to unbalanced translocations.
In half of the cases, an acrocentric chromosome wasinvolved, most frequently chromosome 22 [5]. The largevariability of the phenotype in trisomy 4p syndromemay be explained by the variation in length of the dupli-cated segments [6,7]. Most of the physical features ofour patient are peculiar of the trisomy 4p phenotype:short stature, hypertelorism, bushy eyebrows, broadnasal bridge, low-set hair, short neck, micrognathia,posterior angulated ears, asymmetric facies, and higharched palate [7]. Although the association of trisomy4p and epilepsy is not unusual [7], the only full descrip-tion of epilepsy phenotype was in a girl with a der(17)t(4;17)(p16.1;q23.3) and West syndrome with excellentresponse to the therapy [8]. The relatively small size ofthe 4p fragment involved in that case (4p16.1-pter),could explain this finding. In fact, in our patient the tri-somy is larger (4p15.33-pter) resulting in a more severephenotype with refractory epilepsy. These data wouldsuggest a correlation between the size of the duplicationand the phenotypic expression but, due to the poormolecular characterization of duplications in the previ-ous reports, it is difficult to perform genotype–pheno-type correlations. Furthermore, different geneticbackground as well as other contributing factors mayplay a role in phenotypic variability showed by thesecases. Although any genetic hypothesis remains specula-tive, several genes that are located in the chromosomesegment involved in the rearrangement may be relatedto epilepsy. In particular, a possible dosage effect ofWHSC1, WHSC2, ZNF141 – that are candidate genesfor Wolf-Hirschhorn or 4p- syndrome – should be con-sidered [9,10].
All three genes are located in 4p16.3 that is distal tothe breakpoint of the patient fully described by Ger-ard-Blanluet et al. [8].
In summary, we described the first patient withintractable focal epilepsy, borderline intellectual func-tioning, and facial dysmorphisms associated to a distalduplication of the short arm of chromosome 4. Theidentification of additional cases will clarify whether thischromosomal abnormality is associated to a specific epi-leptic syndrome and the role of specific genes at4p15.33 fi pter in determining the phenotype of thesepatients.
References
[1] Elia M, Musumeci SA, Ferri R, Ayala GF. Chromosomeabnormalities and epilepsy. Epilepsia 2001;42(Suppl 1):24–7.
[2] Grosso S, Farnetani MA, Di Bartolo RM, Berardi R, Pucci L,Mostardini R, et al. Electroencephalographic and epileptic pat-terns in X chromosomal anomalies. J Clin Neurophysiol2004;21:249–53.
[3] Bancaud J, Talairach J. Clinical semiology of frontal lobeseizures. In: Chauvel P, Delgado-Escueta AV, Halgren E,Bauncaud J, editors. Advances in neurology, vol. 57. NY: RavenPress, Ltd.; 1992. p. 3–58.

A. Bartocci et al. / Brain & Development 30 (2008) 425–429 429
[4] Popova BC, Tada T, Takagi N, Brockdorff N, Nesterova TB.Attenuated spread of X-inactivation in an X;autosome translo-cation. Proc Natl Acad Sci USA 2006;103:7706–11.
[5] de Almeida JC, Reis DF, Llerena Junior JC. Pure 4p trisomy dueto a de novo 4q;22p dicentric translocated chromosome karyotype46,XX, 22,+t(4;22)(q1200;p13). Ann Genet 1991;34:108–10.
[6] Reynolds JF, Shires MA, Wyandt HE, Kelly TE. Trisomy 4p infour relatives: variability and lack of distinctive features inphenotypic expression. Clin Genet 1983;24:365–74.
[7] Patel SV, Dagnew H, Parekh AJ, Koenig E, Conte RA, MaceraMJ, et al. Manifestations of trisomy 4p syndrome. Eur J Pediatr1995;154:425–31.
[8] Gerard-Blanluet M, Romana S, Munier C, Le Lorc’h M,Kanafani S, Sinico M, et al. Classical West ‘‘syndrome’’ pheno-type with a subtelomeric 4p trisomy. Am J Med Genet A2004;130:299–302.
[9] Battaglia A, Carey JC. Seizure and EEG patterns inWolf-Hirschhorn (4p-) syndrome. Brain Dev 2005;27:362–4.
[10] Gobbi G, Genton P, Pini A, Guerrieri F, Livet MO. Epilepsiesand chromosomal disorders. In: Roger J, Bureau M, Dravet Ch,Genton P, Tassinari CA, Wolf P, editors. Epileptic syndromes ininfancy. Childhood and adolescence. London: John Libbey &Co; 2002. p. 431–55.