Embed Size (px)
Citation preview
Part A - Fee and Revenue Plan
FEE & REVENUE PLAN.doc 9/15/2009
Format and Guidance
General Information
For the 2010 – 2013 Municipal Public Health Services Plan cycle, the Fee and Revenue Plan will
require LHD’s to project their costs, revenues and personnel resource list over a four year period.
For a municipality to be eligible for reimbursement under the State Aid for General Public Health
Work Program, a Fee and Revenue Plan must be submitted to the NYS Department of Health for
review and approval. The Fee and Revenue Plan must include:
a list of the environmental, personal health services and other services for which fees
are charged;
a schedule of the fees charged for each service listed above;
a list of the environmental, personal health services and other services for which fees
are not charged, including a justification for not charging a fee;
a description of how fees are calculated and the relationship of the cost of providing
services to the fees;
a description of the procedures used for collecting fees; including provisions for use
of a sliding fee schedule;
an estimate of the amount of revenue from fees and charges, for each year covered by
the Fee and Revenue Plan; and
a list of the resources necessary to implement the public health programs, services
and activities outlined in the Municipal Public Health Services Plan.
Part A - Fee and Revenue Plan
FEE & REVENUE PLAN.doc 9/15/2009
Instructions
1. Listing of environmental, personal health and other services fees.
On Fee and Revenue Form A, provide a list of those environmental, personal health and
other services for which the Local Health Unit charges a fee. Additional copies of this form
may be used if necessary. For those services where the fee may vary, please footnote and
provide an explanation and/or breakdown of the variance on an attached sheet. For services
where a sliding fee schedule is used, that should be noted in the "Fee" column and a copy of
the sliding fee schedule used must accompany the Fee and Revenue Plan. Please note at the
top of each sliding fee schedule submitted the programs to which it applies. Examples of
how to complete Form A are provided below:
Form A1 - Environmental Programs:
Program: Community Sanitation and Food Protection
Service: Restaurant Inspection
Fee: $100
Form A2 - Personal Health Services Programs:
Program: Immunization
Services: Flu immunization
Fee: Sliding ($0 - $20)
2. Listing of environmental, personal health and other services for which fees are not
charged.
On Fee and Revenue Form B, provide a list of those environmental, personal health and other
services for which the Local Health Unit does not charge a fee. Additional copies of this
form may be used if necessary. An adequate justification for not charging a fee must be
provided in the "justification" column. This justification should include why the Local
Health Unit feels charging a fee will impede the delivery of service, the basis upon which
that determination was made and, where applicable, the potential impact assessing a fee
would have on program activities. For services where the State Commissioner of Health has
indicated no fees shall be charged, this should be noted in the "justification" column.
An example of how to complete Form B is provided below:
Program: STD
Service: Gonorrhea Testing
Justification: NYSDOH - no fee to be charged
Part A - Fee and Revenue Plan
FEE & REVENUE PLAN.doc 9/15/2009
3. Fee calculation and collection procedures and use of sliding fee schedule.
The Local Health Unit's written protocol for calculating, assessing and collecting fees, as
well as procedures for collecting third-party billings must be submitted on Form C. The
protocol must include, at a minimum:
a description of how the Local Health Unit calculates fees to be charged for
environmental, personal health and other services, which may include:
a. a breakdown of the estimated total costs by individual category of
expense (i.e. personal service, non-personal service, fringe benefits,
indirect costs);
b. factors used to distribute shared costs (i.e. average person-days) to
individual services;
c. criteria used to establish specific fees based on distributed costs (i.e.
number of seats in restaurant, rooms in a temporary residence, etc);
d. number of billable services (i.e. # of visits, # of permits);
e. unrecoverable costs (i.e. service to other municipal agencies);
f. if applicable, rationale for establishing separate fees for discrete
classes of recipients of services; and
g. local considerations for fee setting;
provisions for use of a sliding fee schedule, including how the sliding fee
schedule is implemented;
a description of the follow-up activities conducted by the Local Health Unit
to maximize revenue from delinquent permittee/patient accounts or rejected
Medicaid, Medicare or third-party billings.
A photocopy of Form C from your previous plan may be inserted if there have been no
changes to this procedure.
Part A - Fee and Revenue Plan
FEE & REVENUE PLAN.doc 9/15/2009
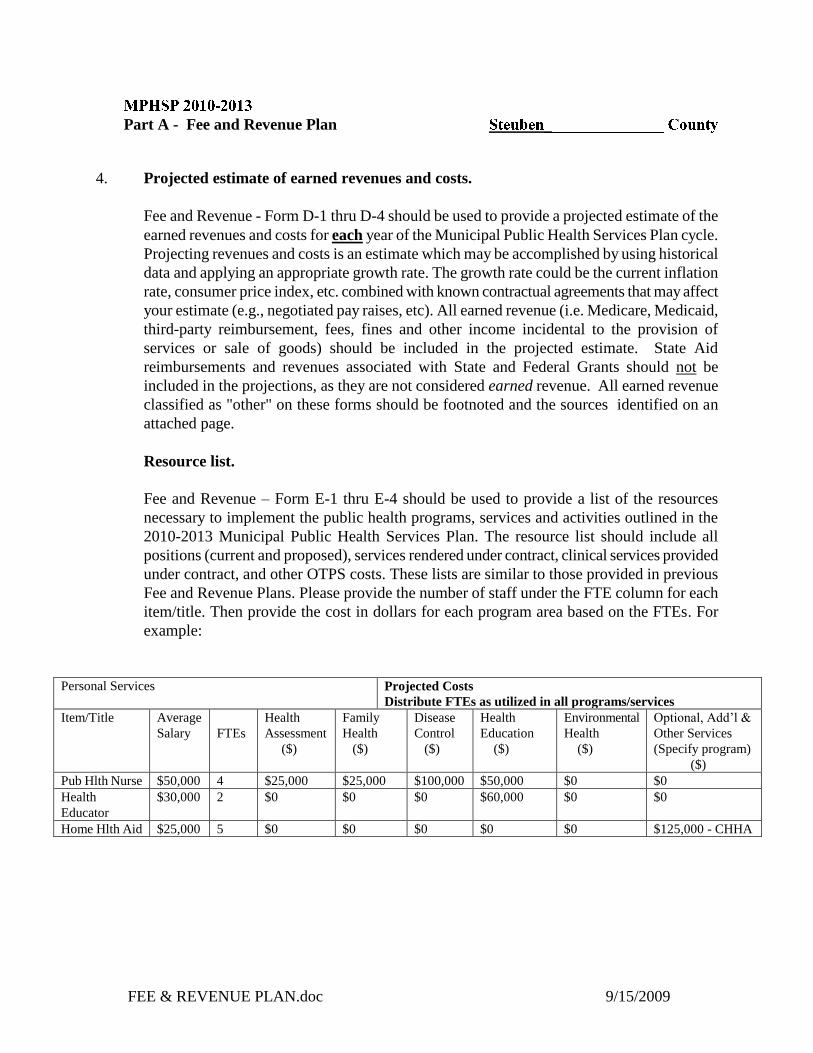
4. Projected estimate of earned revenues and costs.
Fee and Revenue - Form D-1 thru D-4 should be used to provide a projected estimate of the
earned revenues and costs for each year of the Municipal Public Health Services Plan cycle.
Projecting revenues and costs is an estimate which may be accomplished by using historical
data and applying an appropriate growth rate. The growth rate could be the current inflation
rate, consumer price index, etc. combined with known contractual agreements that may affect
your estimate (e.g., negotiated pay raises, etc). All earned revenue (i.e. Medicare, Medicaid,
third-party reimbursement, fees, fines and other income incidental to the provision of
services or sale of goods) should be included in the projected estimate. State Aid
reimbursements and revenues associated with State and Federal Grants should not be
included in the projections, as they are not considered earned revenue. All earned revenue
classified as "other" on these forms should be footnoted and the sources identified on an
attached page.
Resource list.
Fee and Revenue – Form E-1 thru E-4 should be used to provide a list of the resources
necessary to implement the public health programs, services and activities outlined in the
2010-2013 Municipal Public Health Services Plan. The resource list should include all
positions (current and proposed), services rendered under contract, clinical services provided
under contract, and other OTPS costs. These lists are similar to those provided in previous
Fee and Revenue Plans. Please provide the number of staff under the FTE column for each
item/title. Then provide the cost in dollars for each program area based on the FTEs. For
example:
Personal Services Projected Costs
Distribute FTEs as utilized in all programs/services
Item/Title Average
Salary
FTEs
Health
Assessment
($)
Family
Health
($)
Disease
Control
($)
Health
Education
($)
Environmental
Health
($)
Optional, Add’l &
Other Services
(Specify program)
($)
Pub Hlth Nurse $50,000 4 $25,000 $25,000 $100,000 $50,000 $0 $0
Health
Educator
$30,000 2 $0 $0 $0 $60,000 $0 $0
Home Hlth Aid $25,000 5 $0 $0 $0 $0 $0 $125,000 - CHHA

Part A - Fee and Revenue Plan
FEE & REVENUE PLAN.doc 9/15/2009
Form A
Listing of Environmental, Personal Health and Other Services Fees
Program Service Fee
Lead
Immunization
Tuberculosis
Home Care Services
Physically
Handicapped Children's Program
Early Intervention (ages 0-2)
Preschool Program (ages 3-5)
Lead Screening
Hepatitis B (adult)
Flu
Pneumovax
Adult Tetanus
Meningoccal
Zoster
Mantoux testing
Nursing, Therapy, & Home Health Aide
Service
Payment for treatment
Evaluation and Intervention Service
Preschool Special Services
$0-$25
Sliding Fee scale
(see attached)
$40.00 per dose(3
doses required)
$30.00 per dose
$45.00 per dose
$20.00 per dose
$90.00 per dose
$165.00 Per dose
$6.50 per dose
Medicaid Medicare,
Insurance, &
Private Pay based
on a sliding fee -
see attached
Parent fees
minimum
$200 per
authorization
Third Party Payors
Medicaid & State
Education

Part A - Fee and Revenue Plan
FEE & REVENUE PLAN.doc 9/15/2009
Form B
Listing of "No Fee" Services and Justification
Program Service Justification
Rabies
STD
HIV
Immunization
Tuberculosis
Animal Testing
Pet Immunization
Clinics
Post Exposure Treatment
Shots
Diagnosis Treatment
Screening
Child Immunizations
Doctor Visits
Lab Fees
Medications
Per Regulations
Free*
Third Party Payors are billed
first, then County
Free* Waiver
Free*
Free*
Per regulations, third party payors
are billed first, then County
*Free-Charging
fees would
impede poor or
near poor.

FEE & REVENUE PLAN.doc 9/15/2009
Form C
Fee Calculation and Collection Procedures Description
For the CHHA and LTC agency, rates are determined by LHU's independent auditor. These are
determined using the previous year’s cost per unit of service (hours or visits) and the estimated
cost per unit of service for the rate year. A sliding fee scale is used for patients who pay
privately based on their weekly income and the number of people in their family.
For Lead Screening the fee is based on LHU's cost for the tests. Anyone with Medicaid is billed
directly by Health Research. LHU charges others based on the sliding fee scale.
Adult immunizations Immunizations and Mantoux testing are charged based on costs per test or vaccine.
Sliding fee scales are based on the Federal Poverty Guidelines.
Refer to Fee Policy attached.

FEE & REVENUE PLAN.doc 9/15/2009
=========================================================================
TOPIC: Fees Policy (Includes self-pay, insurance, and bad debt and collections)
Approved Date: Signature of Approver:
Next Revision Due Date: 8/04 Effective Date:
Originator: Business Office: 8/03 Division Name: BO
# of pages: 2 plus 3 attachments
=========================================================================
POLICY:
To provide quality patient care to all individuals who qualify for Public Health Nursing Services without regard to patient’s ability to pay or
source of payment.
PURPOSE: To provide uniform methods for applying rates, collections and bad debt processes.
REFERENCE (S): Public Health Law 760.5(h)(4), 763.11 (11), 763.5 (f) of Title 10NYCRR regarding
provision of free care.
Department of Health and Human Services Poverty Guidelines, Research, and
Measurement website; http://aspe.os.dhhs.gov/poverty/poverty.shtml
GENERAL INFORMATION:
A patient is eligible for charity care if ALL of the following conditions are met:
o the patient is unable to pay full charges and;
is not eligible for covered benefits under Title XVIII (Medicare) or XIX
(Medicaid) of the Social Security Act and;
is not covered by any form of private insurance and whose household income
is less than 200% of the Federal Poverty levels.
Note: Charity Care is reflected on the Agency’s sliding scale based upon the most current Federal Poverty levels.
In the event that a patient refuses to complete a Financial Index Form, the SPHN and/or Administrative Assistant will be notified and a
decision may be made to either not provide services or a negotiated rate may be considered.

FEE & REVENUE PLAN.doc 9/15/2009
PROCEDURE:
Cost of services will be determined at regular intervals by a cost study. A full fee or sliding fee scale will be established on the basis of these costs.
There is a minimum charge on a sliding fee scale basis for Nursing visits, Therapy, Home Health Aide, and Personal Care Aide Services (see attached
fee schedule).
A Financial Index Form is completed by the Nurse at the first visit and is used to determine the fees and payment source. The Financial Index Form
and the Consent & Acknowledgement Form must be signed permitting authorization to release information and permitting the Agency to bill third-
party payers, when available.
All third party resources (Medicare, Medicaid, and insurance companies) will be billed and exhausted prior to billing the patient.
When third party payers cover all of the agreed cost, the service will be provided at no charge to the patient. When third party payers cover part of the
cost, the patient will be billed the deductible or coinsurance portion.
Private Pay: Families and individuals receiving services not covered by third party payers should meet the costs of service to the extent that their
resources permit.
Families who can afford to pay full fee are expected to do so. If the family does not wish to divulge financial information, full fee will be billed.
When a family is unable to pay full fee, a fee adjustment will be made. A fee adjustment is a reduction in the fee based on resources of the patient.
Resources of the family or individual will be considered as their present income out of which they meet the costs of day-to-day living, whether the
source is salary, Social Security, pensions, dividends, interest or other sources. Other resources, such as savings, property, and investments, will not
be investigated or taken into consideration in determining the extent to which income is available to meet costs of service.
Based on the families resources, as defined above, a fee will be established using the sliding fee scale. The nurse should review the last Federal Tax
Return and determine the fee based on the gross income. If the patient does not have a tax return, the nurse must review monthly statements, stubs,
etc. Indexes will be updated annually in May or upon changes in income. If the income is less than the first column of the sliding fee scale and it is
felt the patient is unable to pay anything, an exception may be made. The nurse should give all information to the Supervisor, who will make a
decision after discussing the case with the Health Care Fiscal Specialist. The patient should be assured that all information will be treated as
confidential and that whatever fee is arrived at can be adjusted as changes occur in the patient’s overall economic status. The patient should also be
advised that if necessary, someone from the agency may phone to clarify the data submitted.
If the patient dies, and it becomes known that the estate might have the resources to meet the cost of services rendered, the estate will be billed for any
unpaid balance.
Government regulations require that patients and other payors be invoiced full fee; however, the fee adjustment will also be shown on the invoice,
FEE & REVENUE PLAN.doc 9/15/2009
leaving a net amount due the agency.
In cases where a lawsuit is pending for injuries for which the agency is treating the patient, partial payment should not be accepted unless there is a
signed statement in the record that the patient and his family realize he is paying part fee and agree to full fee upon settlement of the suit. It is
preferable, in these cases to bill the client full fee, insuring that the lawyer handling the suit is aware of the full fee services.
Account Clerk and County Attorney’s Responsibilities in Declaring Bad Debts:
The same effort will be made to collect Medicare deductibles and coinsurance amounts as is to collect comparable amount from Non-Medicare
patients. The collection effort will be documented in the patient’s file by copies of bills, follow-up letters, reports of phone calls, and personal
contacts.
If a bill is unpaid after two (2) billing statements have been sent, a series of two (2) letters will be mailed monthly (the last letter should be Return
receipt requested), each followed by a phone call to see if there is any other insurance or Medicaid-if not, then to encourage payment. If no payments
are received, the debt may be deemed uncollectible and will be declared a bad debt. Any outstanding bills over $500.00 will be considered for
litigation and sent to the County Attorney. (Please refer to the sample letters attached.)
When families or patients refuse to pay and it is determined that they could make payment without endangering their future, service may be
terminated after a reasonable time has been provided for the client to make other arrangements for essential service. However, if the recipient of care
cannot control payment and would suffer for lack of service, service will not be terminated.
FEE & REVENUE PLAN.doc 9/15/2009
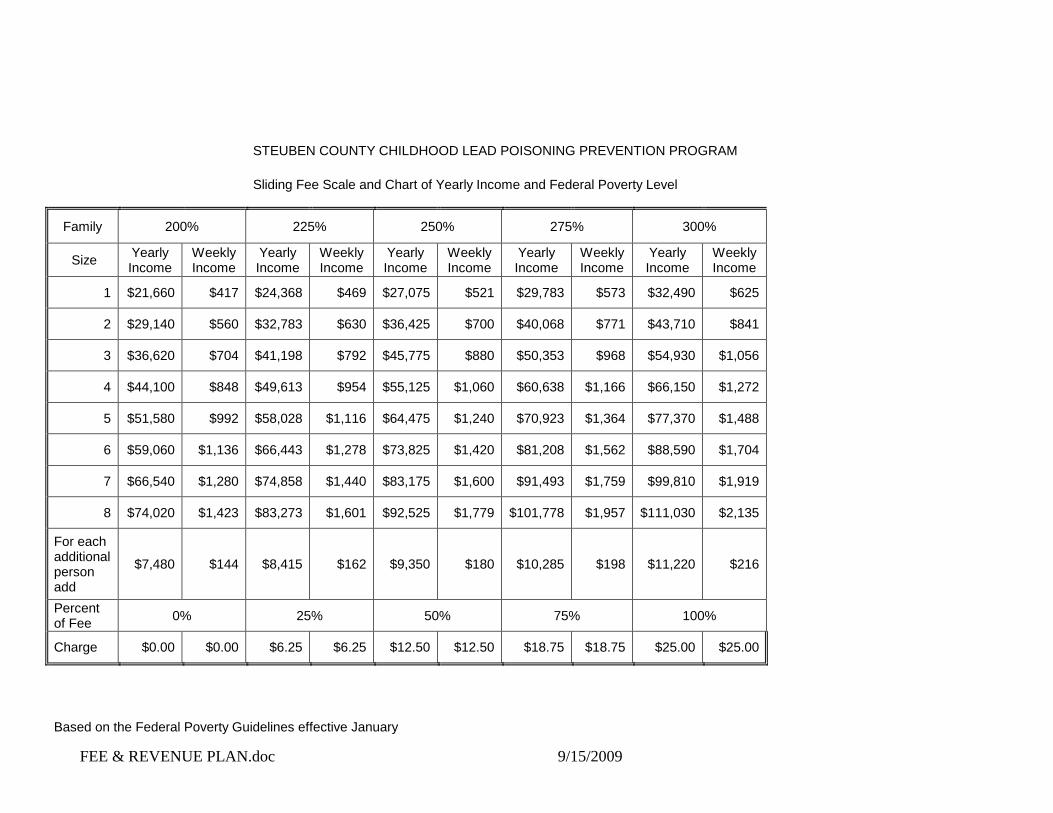
STEUBEN COUNTY CHILDHOOD LEAD POISONING PREVENTION PROGRAM
Sliding Fee Scale and Chart of Yearly Income and Federal Poverty Level
Family 200% 225% 250% 275% 300%
Size Yearly Income
Weekly Income
Yearly Income
Weekly Income
Yearly Income
Weekly Income
Yearly Income
Weekly Income
Yearly Income
Weekly Income
1 $21,660 $417 $24,368 $469 $27,075 $521 $29,783 $573 $32,490 $625
2 $29,140 $560 $32,783 $630 $36,425 $700 $40,068 $771 $43,710 $841
3 $36,620 $704 $41,198 $792 $45,775 $880 $50,353 $968 $54,930 $1,056
4 $44,100 $848 $49,613 $954 $55,125 $1,060 $60,638 $1,166 $66,150 $1,272
5 $51,580 $992 $58,028 $1,116 $64,475 $1,240 $70,923 $1,364 $77,370 $1,488
6 $59,060 $1,136 $66,443 $1,278 $73,825 $1,420 $81,208 $1,562 $88,590 $1,704
7 $66,540 $1,280 $74,858 $1,440 $83,175 $1,600 $91,493 $1,759 $99,810 $1,919
8 $74,020 $1,423 $83,273 $1,601 $92,525 $1,779 $101,778 $1,957 $111,030 $2,135
For each additional person add
$7,480 $144 $8,415 $162 $9,350 $180 $10,285 $198 $11,220 $216
Percent of Fee
0% 25% 50% 75% 100%
Charge $0.00 $0.00 $6.25 $6.25 $12.50 $12.50 $18.75 $18.75 $25.00 $25.00
Based on the Federal Poverty Guidelines effective January

FEE & REVENUE PLAN.doc 9/15/2009
2009
STEUBEN COUNTY PUBLIC HEALTH & NURSING SERVICES
SLIDING FEE SCALE
Determine income by looking at the previous years tax return. Choose the first column which is more than
the patients income. Their fee will be at the bottom of the column.
# 1 Step #2 Step #3 Step #4 Step # 5 Step Full Fee
FAMILY ANNUAL MONTHLY ANNUAL MONTHLY ANNUAL MONTHLY ANNUAL MONTHLY ANNUAL MONTHLY
SIZE INCOME INCOME INCOME INCOME INCOME INCOME INCOME INCOME INCOME INCOME
1 21660 1805 25271 2106 28808 2401 32490 2708 36107 3009
2 29140 2428 33998 2833 38756 3230 43710 3643 48576 4048
3 36620 3052 42725 3560 48705 4059 54930 4578 61046 5087
4 44100 3675 51451 4288 58653 4888 66150 5513 73515 6126
5 51580 4298 60178 5015 68601 5717 77370 6448 85984 7165
6 59060 4922 68905 5742 78550 6546 88590 7383 98453 8204
7 66540 5545 77632 6469 88498 7375 99810 8318 110922 9244
8 74020 6168 86359 7197 98447 8204 111030 9253 123391 10283
FEE ** **
SN-VISIT 10 38 75 113 150
PT-VISIT 10 34 68 101 135
OT-VISIT 10 34 68 101 135
ST-VISIT 10 34 68 101 135
MSW-VIS 10 34 68 101 135
NUT-VIS 10 31 63 94 125
HHA-HR 5 10 28 41 55
Effective 02/01/2009
** Persons with incomes less than the first column may be considered for free or reduced fee services.
Please refer all information to your supervisor.

FEE & REVENUE PLAN.doc 9/15/2009
Form D-1
Projected Costs and Revenues – 2010
Program
Medicare
Medicaid
3rd Party
Fees
Fines
Other
Total
Revenue
Gross
Costs
1. Health Administration __________ __________ __________ __________ __________ __________ __________ __________
Basic Services
2. Family Health Core _________ __$115,000_ __________ ___$3000__ __________ __________ _$118,000_ __________
3. Disease Control Core __$30,000 __________ __________ ___$1,500 __________ __________ __$31,500_ __________
4. Health Education __________ __________ __________ __________ __________ __________ __________ __________
5. Community Health Assessment __________ __________ __________ __________ __________ __________ __________ __________
6. Basic Laboratory __________ __________ __________ __________ __________ __________ __________ __________
7. Environmental Health Core __________ __________ __________ __________ __________ __________ __________ __________
Selected Services
8. Dental Health Services __________ __________ __________ __________ __________ __________ __________ __________
9. Home Health Services $2,800,000_ $450,000 _$444,921 $15,000 __________ _$6,000_ 3,715,921 __________
10. Radioactive Materials __________ __________ __________ __________ __________ __________ __________ __________
11. Rad Producing Materials __________ __________ __________ __________ __________ __________ __________ __________
12. Housing Hygiene __________ __________ __________ __________ __________ __________ __________ __________
13. Other Environmental Services __________ __________ __________ __________ __________ __________ __________ __________
14. Emergency Medical Services __________ __________ __________ __________ __________ __________ __________ __________
15. Long Term Home Health Care _$61,000_ _$250,000_ __________ __________ __________ _$311,000_ __________
16. Optional Laboratory __________ __________ __________ __________ __________ __________ __________
17. EI Administration __________ _$80,000_ __________ __________ __________ $80,000 __________
18. EI Service Coordination __________ _$40,000_ __________ __________ _$22,000__ $62,000 __________
19. All Others __________ __________ __________ __________ __________ __________ __________ __________
Other Services
20. Inpatient TB __________ __________ __________ __________ __________ __________ __________ __________
21. ME and ME Lab __________ __________ __________ __________ __________ __________ __________ __________
Additional Services
22. PHCP __________ __________ __________ _$8,000__ __________ __________ _$8,000_ __________
23. EI Services (0-3) __________ _$580,000_ _$60,000_ __________ __________ _$294,383 _$934,383 __________
24. 3-5 Program Services __________ _$500,000 __________ __________ __________ $2,460,325_ _$2,960,325 __________
25. General Medical Clinics __________ __________ __________ __________ __________ __________ __________ __________
26. DEC Programs __________ __________ __________ __________ __________ __________ __________ __________
TOTAL ALL PROGRAMS $2,891,000 $2,015,000 $504,921 $27,500 $2,782,708 $8,221,129 __________

FEE & REVENUE PLAN.doc 9/15/2009
Form D-2
Projected Costs and Revenues – 2011
Program
Medicare
Medicaid
3rd Party
Fees
Fines
Other
Total
Revenue
Gross
Costs
1. Health Administration __________ __________ __________ __________ __________ __________ __________ __________
Basic Services
2. Family Health Core $117,300 $3,060 $120,360
3. Disease Control Core $30,600 $1,530 $32,130
4. Health Education
5. Community Health Assessment
6. Basic Laboratory
7. Environmental Health Core
Selected Services
8. Dental Health Services
9. Home Health Services $2,856,000 $459,000 $453,819 $15,300 $6,120 $3,790,329
10. Radioactive Materials
11. Rad Producing Materials
12. Housing Hygiene
13. Other Environmental Services
14. Emergency Medical Services
15. Long Term Home Health Care $62,220 $255,000 $317,220
16. Optional Laboratory
17. EI Administration $81,600 $81,600
18. EI Service Coordination $40,800 $22,440 $63,240
19. All Others
Other Services
20. Inpatient TB
21. ME and ME Lab
Additional Services
22. PHCP $8,160 $ 8,160
23. EI Services (0-3) $591,600 $61,200 $300,271 $953,071
24. 3-5 Program Services $510,000 $2,509,532 $3,019,532
25. General Medical Clinics
26. DEC Programs
TOTAL ALL PROGRAMS $2,948,820 $2,055,300 $515,019 $28,050 $2,838,362 $8,385,552

FEE & REVENUE PLAN.doc 9/15/2009
Form D-3
Projected Costs and Revenues – 2012
Program
Medicare
Medicaid
3rd Party
Fees
Fines
Other
Total
Revenue
Gross
Costs
1. Health Administration __________ __________ __________ __________ __________ __________ __________ __________
Basic Services
2. Family Health Core $ 120,750 $ 3,150 $123,900
3. Disease Control Core $ 31,500 $ 1,575 $ 33,075
4. Health Education
5. Community Health Assessment
6. Basic Laboratory
7. Environmental Health Core
Selected Services
8. Dental Health Services
9. Home Health Services $ 2,940,000 $ 472,500 $467,167 $ 15,750 $6,300 $3,901,717
10. Radioactive Materials
11. Rad Producing Materials
12. Housing Hygiene
13. Other Environmental Services
14. Emergency Medical Services
15. Long Term Home Health Care $64,050 $262,500 $326,550
16. Optional Laboratory
17. EI Administration $84,000 $84,000
18. EI Service Coordination $42,000 $23,100 $65,100
19. All Others
Other Services
20. Inpatient TB
21. ME and ME Lab
Additional Services
22. PHCP $8,400 $8,400
23. EI Services (0-3) $609,000 $63,000 $981,102
24. 3-5 Program Services $525,000 $3,108,341
25. General Medical Clinics
26. DEC Programs
TOTAL ALL PROGRAMS $3,035,550 $2,115,750 $530,167 $28,875 $2,291,843 $8,632,185
FEE & REVENUE PLAN.doc 9/15/2009
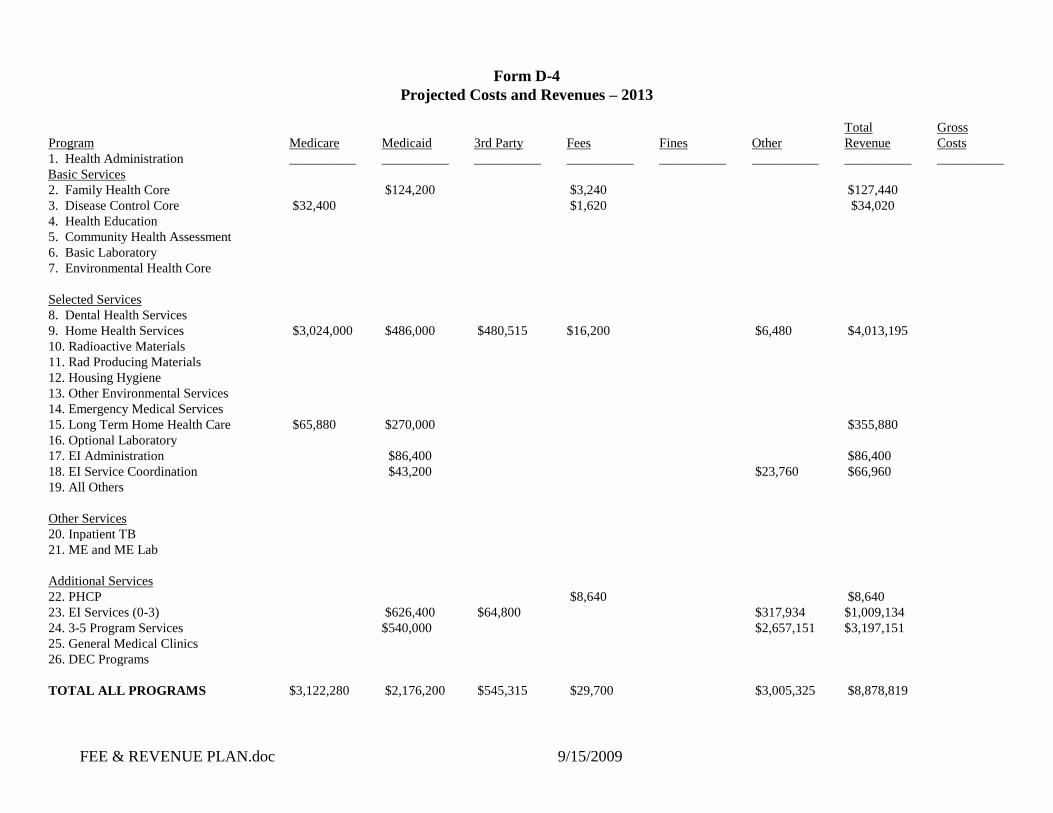
Form D-4
Projected Costs and Revenues – 2013
Program
Medicare
Medicaid
3rd Party
Fees
Fines
Other
Total
Revenue
Gross
Costs
1. Health Administration __________ __________ __________ __________ __________ __________ __________ __________
Basic Services
2. Family Health Core $124,200 $3,240 $127,440
3. Disease Control Core $32,400 $1,620 $34,020
4. Health Education
5. Community Health Assessment
6. Basic Laboratory
7. Environmental Health Core
Selected Services
8. Dental Health Services
9. Home Health Services $3,024,000 $486,000 $480,515 $16,200 $6,480 $4,013,195
10. Radioactive Materials
11. Rad Producing Materials
12. Housing Hygiene
13. Other Environmental Services
14. Emergency Medical Services
15. Long Term Home Health Care $65,880 $270,000 $355,880
16. Optional Laboratory
17. EI Administration $86,400 $86,400
18. EI Service Coordination $43,200 $23,760 $66,960
19. All Others
Other Services
20. Inpatient TB
21. ME and ME Lab
Additional Services
22. PHCP $8,640 $8,640
23. EI Services (0-3) $626,400 $64,800 $317,934 $1,009,134
24. 3-5 Program Services $540,000 $2,657,151 $3,197,151
25. General Medical Clinics
26. DEC Programs
TOTAL ALL PROGRAMS $3,122,280 $2,176,200 $545,315 $29,700 $3,005,325 $8,878,819

FEE & REVENUE PLAN.doc 9/15/2009
Form E-1
Personal Services Resource List – 2010
Personal Services Projected Costs
Distribute FTEs as utilized in all programs/services
Item/Title Average
Salary
FTEs Health
Assessment
($)
Family Health
($)
Disease Control
($)
Health
Education
($)
Basic
Laboratory
($)
Environmental
Health
($)
Optional, Add’l &
Other Services
(Specify program)
($)
Administration
$70,521 2 .02 .3 .48 .2 1
Supervising Nurses
$46,453 3 .26 .19 .03 2.52
Nurses
$41,148 18 1.43 1.6 .02 14.95
HHA’s
$30,990 9.5 9.5
Public Heath Educator
$51,412 1 .39 .58 .03
Clerical
$38,348 17 3.55 1 1 11.45
Home Care Coordinator
$55,745 1 1
Public Health Coordinator
$59,011 1 .39 .58 .03
MSW
$5,000 .01 .01
Medical Director
$21,000 .13 .05 .015
.065
Administrative Officer-
SCS
$51,616 1 .15 .85
Service Coord.
$49,443 3 .2 2.8
Total Personnel Services Cost: _$2,432,390________
FEE & REVENUE PLAN.doc 9/15/2009
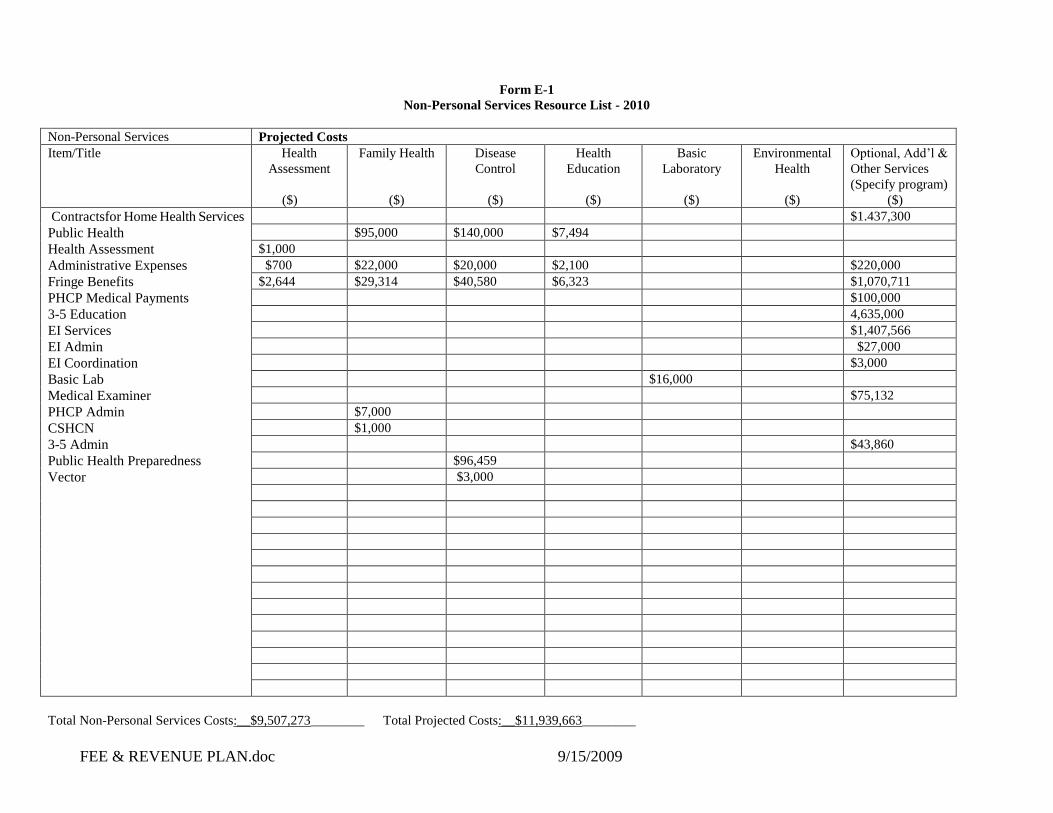
Form E-1
Non-Personal Services Resource List - 2010
Non-Personal Services Projected Costs
Item/Title
Health
Assessment
($)
Family Health
($)
Disease
Control
($)
Health
Education
($)
Basic
Laboratory
($)
Environmental
Health
($)
Optional, Add’l &
Other Services
(Specify program)
($)
Contractsfor Home Health Services
Public Health
Health Assessment
Administrative Expenses
Fringe Benefits
PHCP Medical Payments
3-5 Education
EI Services
EI Admin
EI Coordination
Basic Lab
Medical Examiner
PHCP Admin
CSHCN
3-5 Admin
Public Health Preparedness
Vector
$1.437,300
$95,000 $140,000 $7,494
$1,000
$700 $22,000 $20,000 $2,100 $220,000
$2,644 $29,314 $40,580 $6,323 $1,070,711
$100,000
4,635,000
$1,407,566
$27,000
$3,000
$16,000
$75,132
$7,000
$1,000
$43,860
$96,459
$3,000
Total Non-Personal Services Costs:__$9,507,273________ Total Projected Costs:__$11,939,663________

FEE & REVENUE PLAN.doc 9/15/2009
Form E-2
Personal Services Resource List – 2011
Personal Services Projected Costs
Distribute FTEs as utilized in all programs/services
Item/Title Average
Salary
FTEs Health
Assessment
($)
Family Health
($)
Disease Control
($)
Health
Education
($)
Basic
Laboratory
($)
Environmental
Health
($)
Optional, Add’l &
Other Services
(Specify program)
($)
Administration
$72,919 2 .02 .3 .48 .2 1
Supervising Nurses
$48,032 3 .26 .19 .03 2.52
Nurses
$42,547 18 1.43 1.6 .02 14.95
HHA’s
$32,044 9.5 9.5
Public Heath Educator
$53,160 1 .39 .58 .03
Clerical
$39,652 17 3.55 1 1 11.45
Home Care Coordinator
$57,640 1 1
Public Health Coordinator
$61,017 1 .39 .58 .03
MSW
$5,170 .01 .01
Medical Director
$21,714 .13 .05 .015
.065
Administrative Officer-
SCS
$53,371 1 .15 .85
Service Coord.
51,124 3 .2 2.8
Total Personnel Services Cost: _$2,515,091________

FEE & REVENUE PLAN.doc 9/15/2009
Form E-2
Non-Personal Services Resource List - 2011
Non-Personal Services Projected Costs
Item/Title
Health
Assessment
($)
Family Health
($)
Disease
Control
($)
Health
Education
($)
Basic
Laboratory
($)
Environmental
Health
($)
Optional, Add’l &
Other Services
(Specify program)
($)
Contracts for Home Health Services
Public Health
Health Assessment
Administrative Expenses
Fringe Benefits
PHCP Medical Payments
3-5 Education
EI Services
EI Admin
EI Coordination
Basic Lab
Medical Examiner
PHCP Admin
CSHCN
3-5 Admin
Public Health Preparedness
Vector
$1.466,046
$96,900 $142,800 $7,644
$1,020
$714 $22,440 $20,400 $2,142 $224,400
$2,697 $29,900 $41,391 $6,449 $1,092,126
$102,000
4,727,700
$1,435,717
$27,540
$3,060
$16,320
$76,635
$7,140
$1,020
$44,737
$98,480
$3,060
Total Non-Personal Services Costs:__$9,697,418________ Total Projected Costs:__$12,212,510________

FEE & REVENUE PLAN.doc 9/15/2009
Form E-3
Personal Services Resource List – 2012
Personal Services Projected Costs
Distribute FTEs as utilized in all programs/services
Item/Title Average
Salary
FTEs Health
Assessment
($)
Family Health
($)
Disease Control
($)
Health
Education
($)
Basic
Laboratory
($)
Environmental
Health
($)
Optional, Add’l &
Other Services
(Specify program)
($)
Administration
$74,752 2 .02 .3 .48 .2 1
Supervising Nurses
$49,240 3 .26 .19 .03 2.52
Nurses
$43,617 18 1.43 1.6 .02 14.95
HHA’s
$32,849 9.5 9.5
Public Heath Educator
$54,497 1 .39 .58 .03
Clerical
$40,649 17 3.55 1 1 11.45
Home Care Coordinator
$59,090 1 1
Public Health Coordinator
$62,552 1 .39 .58 .03
MSW
$5,300 .01 .01
Medical Director
$22,260 .13 .05 .015
.065
Administrative Officer-
SCS
$54,713 1 .15 .85
Service Coord.
$52,410 3 .2 2.8
Total Personnel Services Cost: __$2,578,333_______

FEE & REVENUE PLAN.doc 9/15/2009
Form E-3
Non-Personal Services Resource List – 2012
Non-Personal Services Projected Costs
Item/Title
Health
Assessment
($)
Family Health
($)
Disease
Control
($)
Health
Education
($)
Basic
Laboratory
($)
Environmental
Health
($)
Optional, Add’l &
Other Services
(Specify program)
($)
Contracts for Home Health
Services
Public Health
Health Assessment
Administrative Expenses
Fringe Benefits
PHCP Medical Payments
3-5 Education
EI Services
EI Admin
EI Coordination
Basic Lab
Medical Examiner
PHCP Admin
CSHCN
3-5 Admin
Public Health Preparedness
Vector
$1.494,792
$98,800 $145,600 $7,794
$1,040
$728 $22,880 $20,800 $2,184 $228,800
$2,750 $30,487 $42,203 $6,576 $1,113,540
$104,000
$4,820,400
$1,463,869
$28,080
$3,120
$16,320
$78,137
$7,140
$1,020
$44,737
$98,480
$3,060
Total Non-Personal Services Costs:__$9,887,564________ Total Projected Costs:_$12,465,897_________
FEE & REVENUE PLAN.doc 9/15/2009
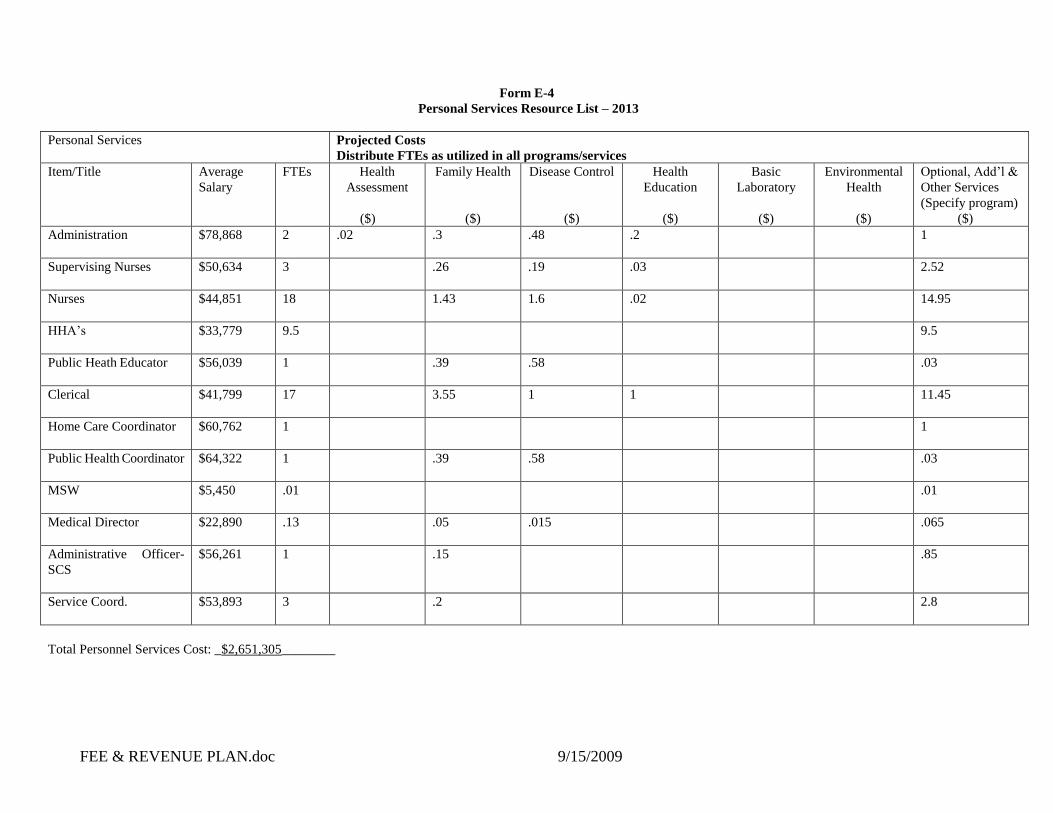
Form E-4
Personal Services Resource List – 2013
Personal Services Projected Costs
Distribute FTEs as utilized in all programs/services
Item/Title Average
Salary
FTEs Health
Assessment
($)
Family Health
($)
Disease Control
($)
Health
Education
($)
Basic
Laboratory
($)
Environmental
Health
($)
Optional, Add’l &
Other Services
(Specify program)
($)
Administration
$78,868 2 .02 .3 .48 .2 1
Supervising Nurses
$50,634 3 .26 .19 .03 2.52
Nurses
$44,851 18 1.43 1.6 .02 14.95
HHA’s
$33,779 9.5 9.5
Public Heath Educator
$56,039 1 .39 .58 .03
Clerical
$41,799 17 3.55 1 1 11.45
Home Care Coordinator
$60,762 1 1
Public Health Coordinator
$64,322 1 .39 .58 .03
MSW
$5,450 .01 .01
Medical Director
$22,890 .13 .05 .015
.065
Administrative Officer-
SCS
$56,261 1 .15 .85
Service Coord.
$53,893 3 .2 2.8
Total Personnel Services Cost: _$2,651,305________

FEE & REVENUE PLAN.doc 9/15/2009
Form E-4
Non-Personal Services Resource List - 2013
Non-Personal Services Projected Costs
Item/Title
Health
Assessment
($)
Family Health
($)
Disease
Control
($)
Health
Education
($)
Basic
Laboratory
($)
Environmental
Health
($)
Optional, Add’l &
Other Services
(Specify program)
($)
Contracts for Home Health
Services
Public Health
Health Assessment
Administrative Expenses
Fringe Benefits
PHCP Medical Payments
3-5 Education
EI Services
EI Admin
EI Coordination
Basic Lab
Medical Examiner
PHCP Admin
CSHCN
3-5 Admin
Public Health Preparedness
Vector
$1,523,538
$100,700 $148,400 $7,944
$1,060
$742 $23,320 $21,200 $2,226 $233,200
$2,803 $31,073 $43,015 $6,702 $1,134,954
$106,000
$4,913,100
$1,492,020
$28,620
$3,180
$16,960
$79,640
$7,420
$1,060
$46,492
$102,342
$3,180
Total Non-Personal Services Costs:__$10,077,709________ Total Projected Costs:__$12,729,014________