Embed Size (px)
Citation preview

12/14/2016
1
Part 6:
OASIS‐C2 Accuracy
Presented by:Sharon Molinari, RN, HCS‐D, HCS‐O
For:HealthCare Synergy
2

12/14/2016
2
M1501: Scenario
o Patient is being discharged after 2 cert periods. During the first cert period she exhibited heart failure symptoms several times. Her MD was contacted each time and changes in her medication regimen were made and the nursing frequency increased for monitoring and teaching. Since her last recert, she hasn’t exhibited any symptoms of heart failure, but the nurse reinforced prior education.
What would be the correct response for M1501?
3
Answer: M1501 Scenario
o Patient is being discharged after 2 cert periods. During the first cert period she exhibited heart failure symptoms several times. Her MD was contacted each time and changes in her medication regimen were made and the nursing frequency increased for monitoring and teaching. Since her last recert, she has not exhibited any symptoms of heart failure, but the nurse reinforced prior education.
What would be the correct response for M1501?
Response 1 ‐ Yes (Patient exhibited symptoms since the most recent SOC/ROC assessment.)
4

12/14/2016
3
M1511: Scenario
o Which of the following is an example of physician‐ordered patient‐specific parameters for a patient who has CHF and has a weight gain of 4 lbs. in 2 days?
a. The nurse reminds him to take Lasix as ordered –20 mg. daily.
b. The MD ordered an additional 40 mg. of Lasix to be taken if he has a weight gain of 3 lbs. in 2 days.
c. The nurse instructed him on the symptoms of heart failure and gave him a handout on managing CHF.
5
Answer: M1511 Scenario
o Which of the following is an example of physician‐ordered patient‐specific parameters for a patient who has CHF and has a weight gain of 4 lbs. in 2 days?
a. The nurse reminds him to take Lasix as ordered –20 mg. daily.
b. The MD ordered an additional 40 mg. of Lasix to be taken if he has a weight gain of 3 lbs. in 2 days.
c. The nurse instructed him on the symptoms of heart failure and gave him a handout on managing CHF.
6

12/14/2016
4
Scenario: M1600 and M1610
o Patient is admitted to home health following hospitalization for pneumonia. He complained of burning with urination, urinary frequency, and said his urine has a strong odor. The assessing clinician contacted the physician, who ordered a catheterization for a urine culture and an antibiotic for a possible UTI. He denied having any incontinence.
How would you score M1600 (Has this patient been treated for a Urinary Tract Infection in the past 14 days?) andM1610 (Urinary Incontinence or Urinary Catheter Presence)?
7
Answers: M1600 and M1610
o Patient admitted to home health following hospitalization for pneumonia. He complained of burning with urination, urinary frequency, and said his urine has a strong odor. The assessing clinician contacted the physician, who ordered a catheterization for a urine culture and an antibiotic for a possible UTI. He denied having any incontinence.
M1600 = Response 1 ‐ YesThe patient was prescribed an antibiotic within the past 14 days specifically for a suspected UTI. The day of assessment counts, since the antibiotic was ordered as a result of the assessment.
M1610 = Response 0 ‐ No incontinence or catheter A catheter was inserted to obtain a urine culture and was then discontinued during the comprehensive assessment, and the patient denied being incontinent. 8

12/14/2016
5
Scenario: M1620 and M1630
o Patient was referred to home health from the hospital for continued treatment of an infected colostomy.
How should the clinician score M1620 (Bowel Incontinence Frequency) and M1630 (Ostomy for Bowel Elimination)?
9
Answers: M1620 and M1630
o Patient was referred to home health from the hospital for continued treatment of an infected colostomy.
How should the clinician score M1620 and M1630?
M1620 = Response NA ‐ Patient has ostomy for bowel elimination
M1630 = Response 2 ‐ The ostomy was related to an inpatient stay or did necessitate change in medical or treatment regimen.
10
12/14/2016
6
Scenario: M1700, M1710, and M1720
o Patient is admitted to home health following hospitalization for exacerbated COPD. He is alert and oriented, but his mind seems to wander, and he seems confused, at times. His son, who lives with him, said he needs reminders about certain things he hadn’t before, since he came home yesterday. The patient denies feeling anxious, and he doesn’t appear to be so. However, his hospital record shows he was treated for an episode of anxiety 6 days prior to SOC, but hasn’t had any further problem since.
What is the correct response for M1700, M1710 and M1720?
11
Scenario: M1700, M1710, and M1720
o Patient is admitted to home health following hospitalization for exacerbated COPD. He is alert and oriented, but his mind seems to wander, and he seems confused, at times. His son, who lives with him, said he needs reminders about certain things he hadn’t before, since he came home yesterday. The patient denies feeling anxious, and he doesn’t appear to be so. However, his hospital record shows he was treated for an episode of anxiety 6 days prior to SOC, but hasn’t had any further problem since.
What is the correct response for M1700, M1710, and M1720?
M1700 (Cognitive Functioning) = 1 ‐ Requires prompting (cuing, repetition, reminders) only under stressful or unfamiliar conditions.
M1710 (When Confused) = 1 ‐ In new or complex situations only
M1720 (When Anxious) = 1 ‐ Less often than daily 12

12/14/2016
7
Scenario: M1730
o Patient is sitting in a chair during her assessment and does not readily respond to any questions, including the ones on the PHQ‐2. She seems tired, but is cognitively alert and oriented. Her daughter, who is her caregiver, says that her mother has been depressed and seems to have just given up.
How should the clinician answer M1730?
13
Answer: M1730
o Patient is sitting in a chair during her assessment and does not readily respond to any questions, including the ones on the PHQ‐2. She seems tired, but is cognitively alert and oriented. Her daughter, who is her caregiver, says that her mother has been depressed and seems to have just given up.
How should the clinician answer M1730?
Response 0 ‐ No
Patient did not respond to PHQ‐2 questions, and the
response cannot be based on what anyone else says. 14

12/14/2016
8
M1740 and M1745: Scenario
o Patient was admitted for SN for management of his CHF and PT for strengthening. He was instructed to use his walker for safety, due to his weakness. However, he refuses to do so…insists he walks fine without it. He doesn’t seem to have any cognitive impairment. His wife says he’s “as sharp as a tack, but is just stubborn.”
How should the clinician score M1740 and M1745?
15
Answers: M1740 and M1745
o Patient was admitted for SN for management of his CHF and PT for strengthening. He was instructed to use his walker for safety, due to his weakness. However, he refuses to do so…insists he walks fine without it. He doesn’t seem to have any cognitive impairment. His wife says he’s “as sharp as a tack, but is just stubborn.”
How should the clinician score M1740 and M1745?
M1740 = 7 ‐ None of the above behaviors demonstrated
M1745 = 0 ‐ Never
Patient was cognitively intact and chose not to adhere to
the instructions to use his walker.16

12/14/2016
9
How would you score M1820?
o Patient has compression stockings and needs assistance from another person with putting them on. He is able to put on all other lower body items as long as someone lays them out.
What is the most appropriate response to M1820?
17
Answer: M1820
o Patient has compression stockings and needs assistance from another person with putting them on. He is able to put on all other lower body items as long as someone lays them out.
What is the most appropriate response to M1820?• Response 1 ‐ Able to dress lower body without assistance if
clothing and shoes are laid out or handed to the patient.
Remember, the majority rules! Per Q&A 132.2, “select the response that represents the patient’s status in the “majority of tasks.” Do not consider which items are more important than others
18

12/14/2016
10
How would you score M1830?
o Patient with considerable balance problems that result in him being very unsteady is able to bathe self in the shower once assisted into the shower.
o Patient with dementia who requires regular cueing to bathe himself is unable to use his shower because the plumbing is broken and bathes at the sink.
19
Answers: M1830
o Patient with considerable balance problems that result in him being very unsteady is able to bathe self in the shower once assisted into the shower.
Response 3 ‐ Patient not safe in shower by himself
o Patient with dementia who requires regular cueing to bathe himself is unable to use his shower because the plumbing is broken and bathes at the sink.
Response 5 ‐ Unable to use tub/shower but able to participate in bathing at sink
20

12/14/2016
11
How would you score M1840?
o Patient uses a commode at night for convenience but can walk to and from the toilet and transfer safely during the day.
What is the most appropriate response for M1840?
o Patient lives alone and walks to the bathroom using her cane, but is assessed to be safe only with assistance.
What response would you select for M1840?
21
Answers: M1840
o Patient uses a commode at night for convenience but can walk to and from the toilet and transfer safely during the day.
What is the most appropriate response for M1840?
Response 0 ‐ Able to get to and from the toilet and transfer independently with or without a device
o Patient lives alone and walks to the bathroom using her cane, but is assessed to be safe only with assistance.
What response would you select for M1840?
Response 1 ‐When reminded, assisted, or supervised by another person, able to get to and from the toilet and transfer
22
12/14/2016
12
Scenario: M1840/M1845
o Patient is post‐op hip replacement and admitted to agency for rehab. At the time of admission, he is using a walker and his wife is walking with him to the toilet, assisting him on and off, and helping him adjust his clothing. The elevated commode seat, ordered by his surgeon, has not been delivered to the home yet.
What are the most appropriate responses for M1840 and M1845?
23
Answers: M1840/M1845
o Patient is post‐op hip replacement and admitted to agency for rehab. At the time of admission he is using a walker and his wife is walking with him to the toilet, assisting him on and off, and helping him adjust his clothing. The elevated commode seat, ordered by his surgeon, has not been delivered to the home yet.
o What are the most appropriate responses for M1840 and M1845?
M1840 = Response 1 ‐When reminded, assisted, or supervised by another person, able to get to and from the toilet and transfer.
M1845 = Response 2 ‐ Someone must help patient to maintain perineal hygiene.
24

12/14/2016
13
Scenario: M1850
o Patient requires the assistance of his wife to come to a sitting position in bed. Once sitting on the bedside, he is able to use his walker to rise and transfer from his bed to his chair.
How would you score M1850?
25
Answer: M1850
o Patient requires the assistance of his wife to come to a sitting position in bed. Once sitting on the bedside, he is able to use his walker to rise and transfer from his bed to his chair.
How would you score M1850?Response 2 ‐ Able to bear weight and pivot during the transfer process but unable to transfer self.
• Per CMS, when a patient requires BOTH an assistive device AND minimal human assistance to transfer, Response 2 is appropriate.
Minimal human assistance = any combination of verbal cueing, environmental set‐up and/or hands on assist < 25% of total effort.
26

12/14/2016
14
GG0170C: Scenario #1
Your patient just had a lumbar laminectomy and is hesitant to move her legs on her own. During the SOC assessment, the RN provides great effort with helping the patient sit up from supine in moving both the trunk and the legs. The patient is unhappy with her current status, as she states she was able to do everything all by herself before the surgery.
27
Scoring Scenario #1
28
6020

12/14/2016
15
GG0170C: Scenario #2
At SOC, the patient’s wife had to provide most of the effort in order for him to sit on the edge of the bed from a sitting position. He said he wishes he could get out of bed himself rather than depending
on his wife to help. Based on the patient’s prior functional status, his current diagnoses, the expected length of stay, and his motivation to improve, the clinician expects that, by discharge, the patient would likely only require assistance getting his legs off the bed to complete the supine to sitting task.
29
Scoring Scenario #2
30
3020

12/14/2016
16
How would you score M2020 & M2102c?
Mrs. Q just got home from the hospital today. She is assessed as being able to take all her medications correctly and uses a pill planner which she fills herself. Her daughter is picking up a new prescription (same drug, different dose), and Mrs. Q is
able to tell the SN how the drug is to be taken.
What is the correct response to M2020, Oral Medication Management?
What about M2102c, Sources of Assistance, Medication administration?
31
Answers: M2020 and M2102c
Ms. Q just got home from the hospital today. She is assessed as being able to take all her medications correctly and uses a pill planner which she fills herself. Her daughter is picking up a new prescription (same drug, different dose), and Mrs. Q is able to tell the SN how the drug is to be taken.
What is the correct response to M2020, Oral Medication Management? Response 3 – Unable to take medication unless administered by another person, since new medication is not available.
What about M2102c, Sources of Assistance, Medication administration? Response 1 – Caregiver provides assistance
32

12/14/2016
17
How would you score M1860?
o A patient who is assessed as safe walking with a walker, but refuses to use the walker and regularly walks with a single point cane.
o Patient with poor cognition can ambulate safely with a walker, but he forgets to use it or uses it improperly.
33
Answers: M1860
o A patient who is assessed as safe walking with a walker, but refuses to use the walker and regularly walks with a single point cane.
Response 2 ‐ Can only walk safely with a walker
o Patient with poor cognition can ambulate safely with a walker, but he “forgets” to use it or uses it improperly.
Response 3 ‐ Requires supervision/assistance at all times to ambulate safely
34
12/14/2016
18
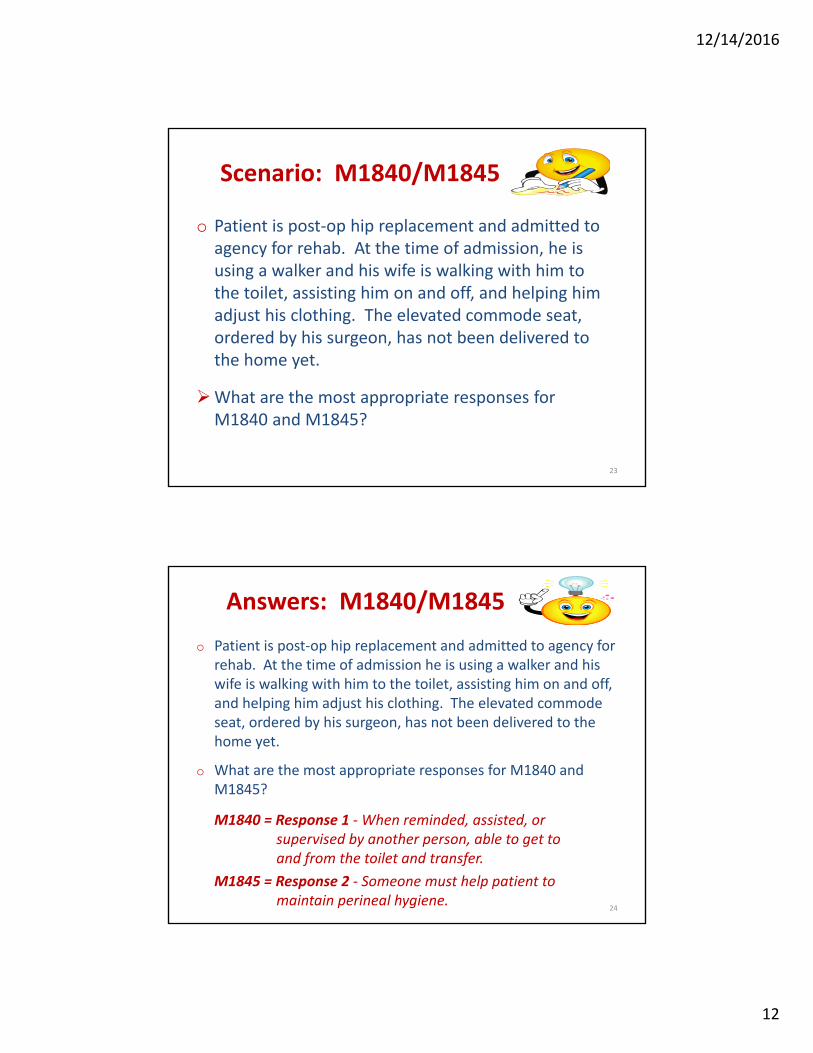
Care ManagementM2102
(M2102)
36

12/14/2016
19
(M2102)
37
(M2102)
38

12/14/2016
20
M2102: Guidance
o Identifies availability and ability of the caregiver(s), other than home health agency staff, to provide categories of assistance needed by the patient.
o Staff providing care employed by a Medicaid In‐Home provider would be considered non‐agency caregivers for the purpose of responding to M2102 if there are separate and distinct provider numbers for each provider type.
o Report what is known on the day of assessmentregarding availability and ability of caregiver(s) to provide assistance for the upcoming episode of care.
o At discharge, report what is known on the day of assessment regarding availability and ability of caregiver(s) to provide assistance at the time of discharge.
39
M2102: Types of Assistance
o ADL Assistance• Includes basic self‐care activities – for example, transfer/ambulation,
bathing, dressing, toileting, eating/feeding
o IADL Assistance • Includes activities associated with independent living necessary to
support the ADLS – for example, shopping, telephone, meals, housekeeping, laundry, finances
o Medication Administration • All types of medication (OTC or prescribed) and by any route (oral,
inhalant, injectable, topical, or via G‐tube/J‐tube, etc.)
o Medical Procedures/Treatments• Physician‐ordered treatment to improve health status• Wound care and dressing changes, ROM exercises, intermittent urinary
catheterization, postural drainage, electromodalities (e.g., TENS), etc.• Anti‐embolism stockings, prosthetic/orthotic devices that have medical
or therapeutic impact (not ADL/dressing items) 40

12/14/2016
21
M2102: Types of Assistance (cont.)
o Management of Equipment
• Includes CPM (Continuous Passive Motion) machine, Hoyer lift, enteral/parenteral nutrition, wheelchair, oxygen, ventilator or respiratory equipment or supplies, emptying wound vac canisters, etc.
o Supervision and Safety
• Activities necessary to ensure patient’s safety, including phone calls made to patient for medication reminders
• In‐person home visits to ensure home safety
• Presence of another person in home to ensure patient does not wander, fall, etc.
o Advocacy and Facilitation (in medical care of patient)
• Taking patient to medical appointments, filling prescriptions, making follow‐up appointments, etc.
41
M2102: Sources of Assistance
o If patient needs assistance with any aspect of a category, consider the aspect that represents the most need and the availability and ability of the caregiver(s) to meet the need. • For example, patient needs assistance bathing and dressing but not
ambulating or toileting.
o For each row a‐g, enter one description of caregiver assistance.
o If more than one response in a row applies – select response that represents the greatest need(s).• For example, caregiver provides assistance currently but also needs
training/supportive services to provide assistance.
o Select Response 3 when non‐agency caregiver indicated unwillingness or is physically or cognitively unable to provide needed care ormay express willingness to provide care but ability to do so is in question or there is reluctance on the part of the caregiver that raises questions as to whether the caregiver will provide needed assistance.
42

12/14/2016
22
How would you score M2020 & M2102c?
Mrs. Q just got home from the hospital today. She is assessed as being able to take all her medications correctly and uses a pill planner which she fills herself. Her daughter is picking up a new prescription (same drug, different dose), and Mrs. Q is
able to tell the SN how the drug is to be taken.
What is the correct response to M2020, Oral Medication Management?
How would you score M2102c, Sources of Assistance, Medication administration?
43
Answers: M2020 and M2102c
Ms. Q just got home from the hospital today. She is assessed as being able to take all her medications correctly and uses a pill planner which she fills herself. Her daughter is picking up a new prescription (same drug, different dose), and Mrs. Q is able to tell the SN how the drug is to be taken.
What is the correct response to M2020, Oral Medication Management?
Response 3 ‐ Unable to take medication unless administered
by another person, since new medication is not available.
How would you score M2102c, Sources of Assistance, Medication administration? Response 1 ‐ Non‐agency caregiver(s) currently provide assistance
44

12/14/2016
23
$$$ (M2200)
o Identifies the total number of therapy visits (physical, occupational, or speech therapy combined) planned for the Medicare payment episode for which this assessment will determine the case mix group, and only applies to payers utilizing a payment model based on case mix group assignment.
oOnly the SOC and FU (Recertification) result in a case mix assignment.
45
M2200: Guidance
o Therapy visits must relate directly and specifically to a treatment regimen plan established between the MD and therapist and be reasonable and necessary to the treatment of the patient’s illness or injury.
o For multidisciplinary cases, therapists are responsible to inform the RN completing this item of the number of visits ordered. Coordination of patient care is a Condition of Participation.• Per the Q&As, "If the number of visits that will be needed is uncertain,
provide your best estimate."
o When a patient is discharged home from an inpatient facility in the last 5 days of a certification period, report the total number of therapy visits planned for the upcoming 60‐day episode on the ROC.
o If the number of therapy visits differs from M2200, Medicare will make the adjustment when the final claim is submitted.• The agency does not have to go back and make any changes or
corrections to M2200 at the SOC or other time points. 46

12/14/2016
24
M2250: Plan of Care Synopsisand
M2401: Intervention Synopsis
M2250 / M2401 Measures (* = measure requires a standardized, validated assessment to respond NA)
M2250: Plan of Care
• Patient‐specific parameters
• Diabetic foot care
• Fall prevention*• *
• Depression*
• Pain monitoring and mitigation*
• Pressure ulcer prevention
• Pressure ulcer treatment using principles of moist wound healing
M2401: Intervention Synopsis
• Parameters not included
• Diabetic foot care
• Fall prevention*
• Depression*
• Pain monitoring and mitigation*
• Pressure ulcer prevention*
• Pressure ulcer treatment using principles of moist wound healing
48

12/14/2016
25
(M2250)
49
PCollected at SOC & ROC
Physician‐Ordered Plan of Care
o The “physician‐ordered plan of care” means that the patient’s condition has been discussed and there is agreement as to the POC between the home health agency staff and the physician.
o Orders may be obtained ONLY from “physician.”
• MDs, DOs, DPMs within legal scope of practice
o Measures initiated on the POC synopsis should be reflected in the physician‐ordered POC.
o The physician plan of care includes all additional orders as an extension of the original POC.
50

12/14/2016
26
M2250: Guidance
Question:
Regarding the physician‐ordered Plan of Care, when documenting that orders were obtained in the Plan of Care Synopsis, is it acceptable to incorporate the general wording of the current process measures into the Plan of Care or are orders expected to be more specifically documented? (e.g. SN to monitor and mitigate pain, instruct on fall prevention measures, etc.)
51
M2250: Guidance
Answer: When completing M2250, Plan of Care Synopsis, it is not required that you include the exact words used in the M2250 item, just that interventions representing the specified best practice be included in the physician‐ordered Plan of Care. In some cases, if all you included were the exact words, it would not meet the requirements. For example, if the order read “Monitor and mitigate pain,” the phrase “mitigate pain” would not be a specific intervention that could be followed in an effort to relieve pain. It would be expected that an order for a specific intervention be included, e.g. Tylenol 500 mg q6h, teach guided imagery techniques to relieve pain, etc. However, in other cases, using the exact words from the M item would suffice. For example, “Monitor lower extremities for lesions and teach patient/caregiver proper diabetic foot care.”
52

12/14/2016
27
(M2401)
53
PCollected at Transfer & DC
M2250/M2401: Content and Timing
o M2250: Does the physician‐ordered plan of care include the following intervention(s)?• Orders must be in place within the 5‐day window at SOC or 2‐day window at ROC, except for M2250g ‐ Pressure ulcer treatment based on the principles of moist wound healing. If orders were requested for moist wound healing within the allowed timeframe, “Yes” may be marked.
o M2401: At the time of or at any time since the most recent SOC/ROC OASIS, were the following interventions BOTH: • Included in the physician‐ordered plan of care AND
• Implemented54
12/14/2016
28
M2250/M2401: General Guidance
o Clinical record documentation should detail:
• The tool or clinical factors used to assess the patient;
• The findings as they relate to the assessment; and
• An analysis to support the OASIS response selected.
o Standardized and validated tool(s) is (are):
• Required to respond “NA” for pain, fall risk, and depression assessment in M2250/M2401.
• Optional for pressure ulcer risk assessment in M2250, but required to respond “NA” for pressure ulcer risk assessment in M2401.
55
M2250/M2401: General Guidance
o M2250: May include patient‐specific preventive measures as orders on the POC, answer “Yes” to M2250, and earn credit for positive processes for your agency, even when the patient is notassessed to have a problem or to be at risk.• Orders related to individual M2250 items should be specific to the
patient, when appropriate.
o M2401: May respond “Yes,” even if patient was not assessed to be at risk as long as interventions were in the physician‐ordered POC and were implemented.
For example:• Orders to monitor and mitigate pain
• Orders to implement fall risk prevention measure
• Orders to prevent skin breakdown and improve skin integrity
56

12/14/2016
29
M2250: Plan of Care Synopsis
o The assessing clinician may wait to complete the comprehensive assessment until after discussion with another discipline who has completed his/her assessment and POC development. (e.g., PT evaluation).
o Best practice orders that were received at SOC and are continued as current orders at the ROC may be considered for M2250 items.
o When the ROC comprehensive assessment is late:• Respond “Yes” on a M2250 best practice item IF relevant orders
for best practices were present within the 48 hour ROC time frame or within 2 days of the agency becoming aware of inpatient facility discharge.
• Document reason for late assessment in record.
• Enter the date the ROC comprehensive was completed in M0090. 57
M2250: What “Yes” Means
o May be answered “Yes” prior to receipt of signed orders if the clinical record reflects evidence of communication with the physician that includes best practice interventions in the POC.
o Requires discussion with the physician and agreement as to the POC between the home health agency staff and the physician (Exception is M2250g, but orders must have been requested within the 5‐day window.)
o Is an appropriate response if the intervention is in the POC, even if assessment indicated intervention wasn’t applicable, if the assessing clinician discusses this with the physician and obtains an order … Per CMS, “just checking off an intervention on a plan of care does not equate to obtaining a physician order.” (CMS Q&A, Cat. 4b, Q 9, 01/14)
o If all other OASIS information is completed when orders obtained, M0090 (Date Assessment Completed) becomes the date of the communication with the physician to establish the POC that includes interventions listed in M2250. 58

12/14/2016
30
M2250: What “No” Means
o Best practice interventions specified in M2250 are not included in the Plan of Care that was developed as a result of the comprehensive assessment.• Exception: M2250g – If orders for moist wound healing have
been requested from the MD but are not in place within the 5‐day window, select “Yes.”
Note: The parallel item in M2401f does not offer this option. So, at M2401f, if the MD does not order treatment based on principles of moist wound healing, “No" must be reported on Row f, unless the patient meets the criteria listed to mark NA.
o Orders for interventions, except for M2250g, have been requested but not authorized by the end of the comprehensive assessment time period.
• SOC: 5‐day window
• ROC: 2‐day window59
o “Yes” means the POC includes specific parameters ordered by physician or physician agrees to use agency parameters for this specific patient.
o “Yes” means the POC includes specific parameters ordered by physician or physician agrees to use agency parameters for this specific patient.
o “No” means there are no specific parameters on POC and the agency will not use standardized physician notification guidelines.
o “NA” means the agency will use standardized clinical guidelines accessible for care providers which physician has not agreed to.
o Only one patient‐specific parameter is necessary to meet this standard.
60

12/14/2016
31
M2250: Guidance
M2250a (Patient‐Specific Parameters):
o In order to select "Yes" for M2250a, Patient‐Specific Parameters, the physician‐ordered Plan of Care must include specific parameters, e.g. notify physician if INR <2.0 or >3.0. Just including the name of a set of guidelines, e.g. AHA guidelines, ABC Agency guidelines, ADA guidelines, etc. would not meet the requirements of this best practice.
M2250b (Diabetic Foot Care):
o “NA” is the appropriate response for a patient that has Diabetes Insipidus, not Diabetes Mellitus. M2250b best practice interventions are intended for patients with Diabetes Mellitus.
61
o “Yes” means interventions are present on the POC to:
• Monitor for the presence of skin lesions on the lower extremities; and
• Provide diabetic foot care education to the patient/caregiver.
62
12/14/2016
32
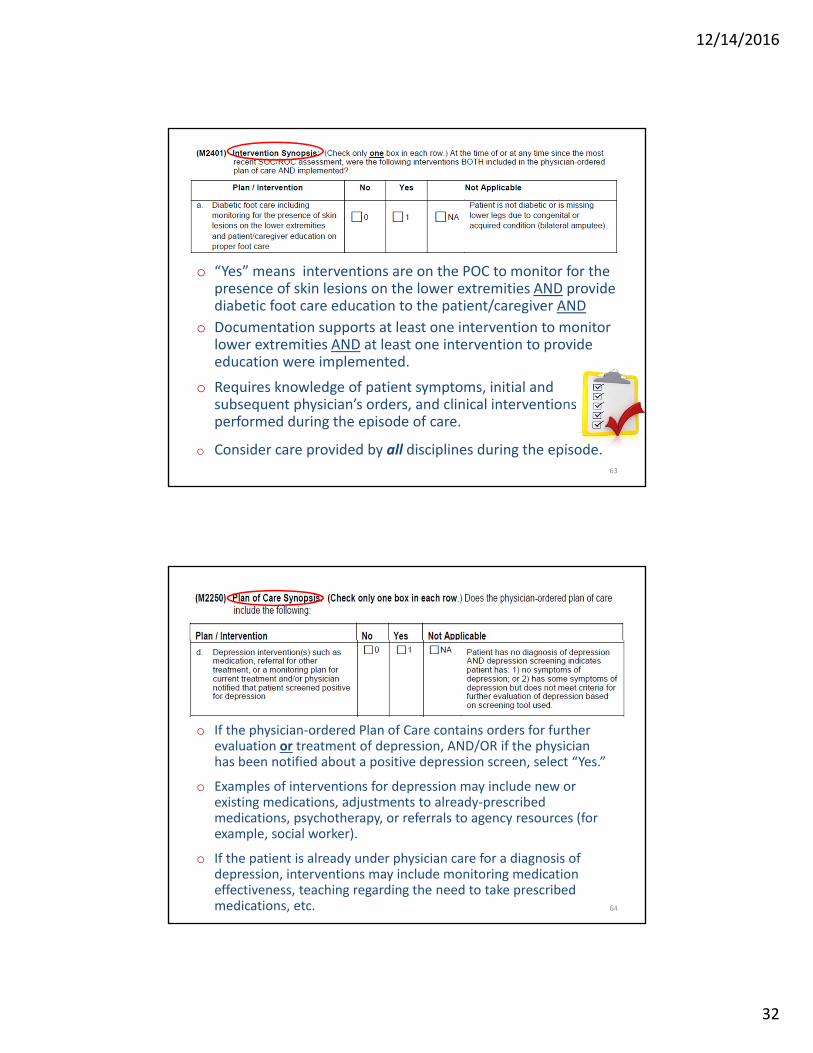
o “Yes” means interventions are on the POC to monitor for the presence of skin lesions on the lower extremities AND provide diabetic foot care education to the patient/caregiver AND
o Documentation supports at least one intervention to monitor lower extremities AND at least one intervention to provide education were implemented.
o Requires knowledge of patient symptoms, initial and subsequent physician’s orders, and clinical interventions performed during the episode of care.
o Consider care provided by all disciplines during the episode.63
o If the physician‐ordered Plan of Care contains orders for further evaluation or treatment of depression, AND/OR if the physician has been notified about a positive depression screen, select “Yes.”
o Examples of interventions for depression may include new or existing medications, adjustments to already‐prescribed medications, psychotherapy, or referrals to agency resources (for example, social worker).
o If the patient is already under physician care for a diagnosis of depression, interventions may include monitoring medication effectiveness, teaching regarding the need to take prescribed medications, etc. 64

12/14/2016
33
M2250d/M2401c: Guidance
When completing M2250d, the assessing clinician may answer "Yes" in cases where the physician was notified of the positive depression screening by the end of the allowed assessment time period. Communication to the physician made by telephone, voicemail, electronic means, fax, or any other means that appropriately conveys the message of patient status is sufficient. There is no requirement that you receive acknowledgement of your message in order to select “Yes.”
M2401c does not offer the option of notifying the physician of a positive depression screening. When scoring M2401c, “No" must be reported if no orders for depression are received or no referral for other treatment made, unless the patient meets the criteria listed to mark “NA.”
65
M2250d/M2401c: Guidance
Question:
For M2250d, except for situations of physician notification of a positive depression screening, do I have to obtain a physician’s order for an intervention in order to answer "Yes.”
Answer:
Yes, other than for situations of physician notification regarding a positive depression screen, a physician's order for the depression intervention is required.
66

12/14/2016
34
M2250: Guidance
M2250e (Pain Interventions):
o In order to select "Yes" for a best practice intervention in M2250, there must be a physician order for an intervention(s) that specifically addresses the patient's needs as required in each best practice area (M2250 row). In order to select "Yes" for Row e, Pain, the physician‐ordered plan of care must include both an order to assess pain and an order intended to relieve/mitigate the individual patient's specific pain.
o An ordered pain medication is considered an intervention to mitigate pain. Assessing for the effectiveness of the pain medication is considered an intervention to monitor pain. If both the pain medication and an order related to pain assessment are included in the physician‐ordered Plan of Care, M2250e would be “Yes.” 67
M2401: Guidance
Question:If I included a physician‐ordered intervention in my Plan of Care and attempted to implement it, but the patient either refused or did not need the intervention, can I report the education as being implemented in M2400 Intervention Synopsis? For example, my Plan of Care included diabetic foot care including monitoring and patient education on proper foot care. I provided the foot care, monitored the feet throughout the episode, but when evaluating the patient’s knowledge base prior to educating, I discovered there was no identified need for education
68

12/14/2016
35
M2401: Guidance
Answer:
If the education component of the intervention was ordered, attempted and not provided because of a documented lack of need for the education, the clinician can answer “Yes” to the Intervention Synopsis item. The intervention was implemented when the attempt to provide it was made, and the lack of need identified. This is distinctly different than stating an attempt was made to educate and the patient refused or otherwise declined to receive the needed instruction with no further attempt, in which case, the refused education should not be reported as being “implemented” on M2401.
69
Getting M2250/M2401 Right
o First: Can you answer “Yes” to a specific item?
• Understand what must be included in the interventions/orders.
• Understand the CMS guidance (including Q&As).
o Next: If item cannot be answered “Yes,” is “NA” appropriate?
• Understand NA criteria for the item.
o If “Yes” and “NA” are not appropriate, then “No” is the only option left.
70

12/14/2016
36
How would you answer the following?
Mr. R was discharged from the hospital 12/6, but refused a visit for the ROC assessment on 12/7 and was assessed on 12/8. The assessments for M1240, M1300, and M1910 were all completed on 12/8, but physician orders for relevant best practices were not received by the agency until 12/9. The patient refused to be screened for depression.
1. What are the correct responses to M2250 (Fall interventions, Depression interventions, Pain interventions, Pressure ulcer prevention interventions?
2. What is the M0090 date?
71
Answers
Mr. R was discharged from the hospital 12/6, but refused a visit for the ROC assessment on 12/7 and was assessed on 12/8. The assessments for M1240, M1300, and M1910 were all completed on 12/8, but physician orders for relevant best practices were not received by the agency until 12/9. The patient refused to be screened for depression.
1. What are the correct responses to M2250 (Fall interventions, Depression interventions, Pain interventions, Pressure ulcer prevention interventions? No – Though the assessments were done within the 48 hour timeframe, the physician orders were not obtained by then.
2. What is the M0090 date? 12/9 – The day the physician confirmed the POC would be the M0090 date, if all other data needed to complete the OASIS had been obtained.
72

12/14/2016
37
Emergent CareM2301 – M2310
(M2301)
o Identifies whether the patient was seen in a hospital emergency department at the time of or at any time since the most recent SOC/ROC assessment.
o Responses to this item include the entire period at or since the most recent SOC/ROC assessment, including use of hospital emergency department that results in a qualifying hospital admission, necessitating Transfer OASIS data collection.
o This item includes current events.

12/14/2016
38
M2301: Inclusions, Exclusions, Definitions
o Includes: Use of hospital ER department and holding / observation in a hospital ER setting.
o Excludes: Urgent care services not provided in a hospital ER, care by an ambulance crew without transport, and physician office visits scheduled < 24 hours in advance.
o Holding / Observation Status: Access to and use of a hospital ER for emergent care services and observation without hospital admission without regard for the length of the observation or “hold” in ER.
o Admission / Qualifying Stay: Defined as admission to a hospital where the stay is ≥ 24 hours for reasons other than diagnostic testing.
Injury not due to fall or other reason not listed
Regardless of where fall occurred

12/14/2016
39
M2310: Guidance
o This item ONLY addresses services provided in a hospital emergency department – not urgent care, MD office, emergency crew without transport.
o If a patient seeks care in a hospital emergency department for a specific suspected condition, report that condition, even if the suspected condition was ruled out (e.g., patient was sent to the emergency department for suspected DVT, but diagnostic testing and evaluation was negative for DVT).
o If the patient has received emergent care in a hospital emergency department multiple times since the last time OASIS data were collected, include the reasons for all visits.
7777
Scenario: Emergent Care
o At discharge, how should you respond to M2301 (Emergent Care) and M2310 (Reason for Emergent Care), if the patient developed pneumonia and dehydration which caused her to fall fracturing her wrist. She was taken to the ER and was admitted to the hospital.
– M2301:
– M2310:

12/14/2016
40
Scenario: Emergent Care
o At discharge, how should you respond to M2300 (Emergent Care) and M2310 (Reason for Emergent Care) if the patient developed pneumonia and dehydration which caused her to fall fracturing her wrist. She was taken to the ER and was admitted to the hospital. – M2301: Response 2 ‐ Yes, with hospital admission
– M2310:
• Response 2 ‐ Injury caused by fall
• Response 3 ‐ Respiratory infection
• Response 12 ‐ Dehydration
79
Transfer and DischargeM2420 – M2440
M0903 and M0906

12/14/2016
41
(M2420)
o Identifies where the patient resides after discharge from the home health agency.
o Response 2 – Patient remained in the community (with formal assistive services) – is appropriate for patients who are in assisted living facilities and board and care homes.
o Non‐institutional hospice is defined as hospice care in the home, not an inpatient facility.
81
M2420: Discharge Disposition
o Formal assistive services: community‐based services provided through organizations or by paid helpers, such as:• Homemaking services under Medicaid waiver programs, personal
care services provided by a home health agency, paid assistance provided by an individual, home‐delivered meals provided by organizations like Meals‐on‐Wheels.
• Therapy services provided in an outpatient setting are NOT considered formal assistance.
• Informal services: those provided by friends, family, neighbors, or other individuals in the community for which no financial compensation is provided. For example:• Assistance with ADLs provided by a family member, transportation
provided by a friend, meals provided by church members (specifically, meals not provided by the church organization itself, but by individual volunteers).

12/14/2016
42
(M2430)
83
Regardless of where fall occurred
Injury not due to fall or other reason not listed
• Avoid answering “Unknown.”
• Document circumstances
of admission in the record.
(M2430) Reason for HospitalizationFor what reason(s) did the patient require hospitalization? (Mark all that apply.)
1 ‐ Improper medication administration, adverse drug reactions, medication side effects, toxicity,anaphylaxis
2 ‐ Injury caused by fall 3 ‐ Respiratory infection (for example., pneumonia, bronchitis) 4 ‐ Other respiratory problem 5 ‐ Heart failure (for example, fluid overload) 6 ‐ Cardiac dysrhythmia (irregular heartbeat) 7 ‐Myocardial infarction or chest pain 8 ‐ Other heart disease 9 ‐ Stroke (CVA) or TIA 10 ‐ Hypo/Hyperglycemia, diabetes out of control 11 ‐ GI bleeding, obstruction, constipation, impaction 12 ‐ Dehydration, malnutrition 13 ‐ Urinary tract infection 14 ‐ IV catheter‐related infection or complication 15 ‐Wound infection or deterioration 16 ‐ Uncontrolled pain 17 ‐ Acute mental/behavioral health problem 18 ‐ Deep vein thrombosis, pulmonary embolus 19 ‐ Scheduled treatment or procedure 20 ‐ Other than above reasons UK ‐ Reason unknown 84
Regardless of where occurred
Injury not due to fall
• Avoid answering “Unknown.”• Document circumstances of
admission in the record.

12/14/2016
43
(M0903)
o Identifies the last or most recent home visit by any agency provider that is included in the Plan of Care.
o If the agency policy is to have an RN complete the comprehensive assessment in a therapy‐only case, the RN can perform the discharge assessment after the last visit by the therapist. The RN visit is non‐billable.
(M0906)
o The discharge date is determined by agency policy or physician order.
o The transfer date is the actual date the patient was admitted to an inpatient facility.
o The death date is the actual date of death at home.
o Excludes death occurring in an inpatient facility or in an emergency department. Both situations would result in a Transfer OASIS collection and would report the date of transfer.
o Includes death that occurs while a patient is being transported to an emergency department or inpatient facility (before being seen in the ED or admitted to the inpatient facility).
86

12/14/2016
44
Anything else?
87
88

12/14/2016
45
I think this means we’re done!
About the HCS‐O Exam

12/14/2016
46
Purpose of the HCS‐O Certification
• The exam assesses the knowledge of OASIS guidance for clinician’s collecting this data and the reviewer and his/her ability to apply guidance correctly in patient‐
specific scenarios.
• The exam validates that the clinician is able to complete the OASIS an appropriate level of competence.
OASIS competency is a key component in attaining accurate clinical patient outcomes and reimbursement!
91
Exam and Competency Areas
For exam details, go to: www.decisionhealth.com
• 80 questions; 3 hours; 75%
• Standard conventions and how OASIS works with the Payment System
• Clinical Items including diagnosis coding rules (as related to OASIS)
• Wound Items
• Functional Items
• Process Measures 92

12/14/2016
47
Core Documents
• Core documents:
– The OASIS‐C2 Guidance Manual• Chapter 1
• Chapter 3
– CMS OASIS Q&As
– OASIS Considerations for Medicare PPS Patients
– WOCN OASIS‐C2 Wound Guidance
• Other documents
– Medicare HH CoPs
93
Facts to Know
94
12/14/2016
48
OASIS and PPS
• Time points for OASIS data collection:– Start of Care (SOC)
– Resumption of Care (ROC) following an inpatient admission
– Follow up – at the end of a 60 day episode
– Other Follow up ‐ when there is an unanticipated improvement or decline in patient’s condition
– Transfer to an inpatient facility
– Discharge, not to a facility
– Death at Home
Note: only SOC and Follow‐up (Recertification) are used for determining payment based on a HHRG.
95
Purpose of OASIS
• Performs systematic comparative measurements of home health patient outcomes at two points in time.
• Identifies potentially avoidable outcomes of care.
• Identifies a HHA’s use of best practices in managing patients.
• Provides additional information about patient case‐mix characteristics and utilization of resources.
• Risk adjusts outcome data when computing patient outcomes.
96

12/14/2016
49
OASIS as a Payment Tool
• Patients receiving 5 or more visits are assigned one of 153 case mix weights based on equations that are determined by:
– Clinical severity score
– Functional status score
– Service utilization score
– Timing of Episode (early/later) – M0110
– Therapy visits – M2200
97
3 Dimensions or Domains
• Clinical Severity
– Primary and secondary diagnosis codes
– Diagnosis to diagnosis interactions or combinations
– Diagnosis to case‐mix item interactions or combinations
– Individual case mix items – e.g. M1030, M1242, M1400, M1830
• Functional Status
– Functional items – dressing, bathing, toileting, transferring and ambulation
• Service Utilization (based on therapy services)
– 0‐13
– 14‐19
– 20 +98

12/14/2016
50
Definitions
• Active treatment
• Day of assessment
• At the time of or at any time since the most recent SOC/ROC
• Assistance
• Bedfast
99
OASIS Conventions
• Understand the time period under consideration for each item.
– Report what is true on the day of the assessment unless a different timeframe is specified in the item or related guidance.
• What is a care episode/quality episode?
– Must have a beginning (i.e., a SOC or ROC assessment) and a conclusion (i.e., a Transfer or Discharge assessment)
• If the patient’s ability varies on the day of the assessment, report the patient’s “usual status” or what is true greater than 50% of the assessment time frame, unless the item specifies differently. 100

12/14/2016
51
More Conventions
• Responses to items documenting a patient’s current status should be based on independent observation of the patient’s condition and ability at the time of the assessment without referring back to previous assessments.
• Combine observation, interview, and other relevant strategies to complete OASIS data items as needed.
• Minimize use of NA and unknown responses.
101
Test TakingSkills and Tips

12/14/2016
52
Rule #1: Know the OASIS Conventions!
103
Rule #2:Make Chapter 3 and the Q&As Your Best Friends!
104

12/14/2016
53
Rule #3: Read Scenarios Carefully
Read everything…it all means something!
105
Rule # 4: Don’t Assume
Remember what they say about “assume.”
Don’t Do It!
106

12/14/2016
54
Types of Questions
What is the appropriate response in the following scenario?
What is the appropriate date or episode equation?
Which of the following is true?
Which of the following is false ?
If any part of a statement is not true,then the whole thing is not true!
107
Selecting Your Answer
• Highlight important phrases and information, if taking a paper test.̶ If NOT taking the exam at an approved workshop, research PSI sites in your area.
• Answer the questions you’re sure of first – this helps to build your confidence.
• Hold the difficult questions for last and look at the guidance or Q&As to help you determine the correct answer, if you have time.
108

12/14/2016
55
Resources Allowed for the Exam
• OASIS‐C2 Guidance Manual ‐ Chapters 1 and 3
• CMS OASIS Q&As
• OASIS Considerations for Medicare PPS Patients
• WOCN OASIS‐C2 Wound Guidance
109
Thank you for attending and GOOD LUCK!
Sharon Molinari
RN, HCS‐D, HCS‐O
110
![OASIS-D Handouts [Read-Only]€¦ · • Describe the major changes from OASIS-C2 to OASIS-D • Understand OASIS M-item coding instructions to accurately code new and revised OASIS](https://img.pdfslide.us/doc/110x75/5ec3637ace40ce0748747c2e/oasis-d-handouts-read-only-a-describe-the-major-changes-from-oasis-c2-to-oasis-d.jpg)