-
12/2/20
1
Greg Pontone, MD, MHSDirector, Parkinson’s Neuropsychiatry Cl
inical Programs
Johns Hopkins University School of Medicine
Parkinson’s Disease: Moving Toward Improved Understanding and
Treatment
1
DisclosuresDr. Pontone is a consultant for Acadia
Pharmaceuticals Inc
2
Learning Objectives•Explain the pathophysiology of Parkinson’s
disease, including the motor and non-motor symptoms.
•Summarize new data on current and emerging therapies for
Parkinson’s disease•Apply available modalities to patient cases
using evidence-based medicine•Describe the impact of OFF periods on
patient daily life•Formulate strategies for improving education
regarding OFF periods in patients with Parkinson’s disease
3
-
12/2/20
2
Pathophysiology of Parkinson’s disease
4
Parkinson’s DiseaseParkinson’s disease is a progressive
neurodegenerative disorder characterized by aggregates of misfolded
⍺-synuclein called Lewy bodies
Parkinson’s disease has a complex clinical phenotype that
includes motor and non-motor symptoms that vary not only in
severity but also in terms of presence or absence from case to
case
5
Parkinson’s Disease – Substantia Nigra
6
-
12/2/20
3
Dopamine Deficiency in the Nigrostriatal Pathway
Basal ganglia – “extrapyramidal system” includes substantia
nigra, striatum (caudate and putamen), globus pallidus, subthalamic
nucleus, and thalamus
Parkinson’s disease 60% - 80% reduction in dopamine producing
neurons in the substantia nigra
Two output pathways from the striatum: indirect pathway in which
dopamine (D2) has an inhibitory influence and the direct pathway in
which dopamine (D1) has an excitatory influence
In the context of dopamine depletion the indirect inhibitory
pathway mediated via D2 striatal receptors is thought to be
overactive, whereas the direct inhibitory pathway mediated via D1
striatal receptors is underactive
As a consequence, the main pallidal-thalamic outflow pathway
provides excessive inhibitory input to the thalamus, which causes
suppression of thalamo-cortical-spinal pathway, causing slowness of
movement (bradykinesia)
7
Clinical Diagnosis of PDRequires Only Motor SymptomsFirst
essential criterion: • Slowing of physical movement
(bradykinesia)
Plus at least one of the following:• Tremor (4-7hz)• Muscle
rigidity
8
Postuma RB et al Mov Disord 2015
8
Stage and Severity of Parkinson’s DiseaseHoehn and Yahr
Stage
Stage 1 – unilateral involvement only, usually with no
functional disability
Stage 2 – bilateral involvement without impairment of
balance
Stage 3 – bilateral involvement with impairment of postural
reflexes (balance)
Stage 4 – severely disabling disease; still able to walk with
assistive device or stand unassisted
Stage 5 – confinement to bed or wheelchair unless aided
Unified Parkinson’s Disease Rating Scale – part 3 motor exam,
example for rigidity
0: normal: no rigidity
1: slight: rigidity detected only with activation maneuver
2: mild: rigidity detected without activation maneuver, but full
range of motion easily achieved
3: moderate: rigidity detected without activation and full range
of motion is achieved with effort
4: severe: rigidity detected without activation and full range
of motion not achieved
9
-
12/2/20
4
Now let me tell you the rest of the story…Non-motor symptoms of
Parkinson’s diseaseNeuropsychiatric: apathy, anxiety, depression,
psychosis, impulse control disorders
Cognitive impairment, ≤40% have MCI at diagnosis and 80%
demented within 20 years of motor symptom onset
Olfactory loss ≤90%
Dysautonomia ≤70%
Sleep disturbances >30%
10
10
11BRAAK ET AL.
11
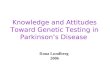
Parkinson’s as a Disease Model for Neuropsychiatric Symptoms
12
locus coeru leus
m edu lla ry raphe nuc le i
nuc leus subcoeru leus
stag es 5 & 6
stag e 1
stag e 2
stag e 3
stag e 4
Dysautonomia:gastrointestinaldisturbances,constipation,genito-urinarydysfunction,sexualdysfunction,orthostatichypotension,cardiacsympatheticdenervationOlfactoryloss;hyposmia:impairmentsinodordetection,identification&discrimination
Sleepdisturbances:REMbehaviordisorder;excessivedaytimesleepiness,insomnia,restlesslegssyndrome
Motorsymptoms:bradykinesia,rigidity,tremor
Cognitivedisorders:mildcognitiveimpairmentanddementia
Mooddisorders:
Anxiety
Depression
au tonom ic nervous sys tem
dorsa l m oto r X nuc leus
o lfac to ry nerve
substan tia n ig ra
am ygda la
basa l nuc leus
h ippocam pus
fron ta l co rtex
parie ta l co rtex
Psychosis:hallucinations,delusions
F igure 1 .C lin ica lcorre la teso fpatho log ica lstag ing in
PD .
12
-
12/2/20
5
13KALIA AND LANG ET AL.
Parkinson’s as a Disease Model for Neuropsychiatric Symptoms
13
New Landscape of Parkinson’s Disease
Prodromal PD Symptomatic PD PD Dementia
PD diagnosed by motor symptoms
14
New ‘stages’ of Parkinson’s disease
Prodromal: pre-motor, hyposmia, RBD, cardiac sympathetic
denervation
Symptomatic: motor symptom onset and progression
Dementia: progressive cognitive decline due to Lewy body disease
or comorbidity
15
-
12/2/20
6
Key Points
• Parkinson’s disease, in most cases, starts years before motor
symptoms are present
• Non-motor symptoms such as autonomic dysfunction, REM sleep
behavior disorder, and loss of smell are biomarkers of early
disease
• Going forward, early recognition and disease modifying
treatments will likely significantly lower the burden of PD
16
Current and emerging therapies for Parkinson’s disease
17
Interventions for Parkinson’s disease
1. Prevention or delay of disease progression (‘disease
modifying’)
2. Symptomatic monotherapy
3. Adjunctive therapies
4. Prevent or delay of motor complications
5. Motor complication therapies
18
-
12/2/20
7
Disease Modifying InterventionsExercise – has insufficient
evidence and considered investigational, but is widely
recommended
No clinically useful interventions to prevent or delay disease
progression (Fox SH et al 2018)
Notable negative studies – MAOIs, CoQ10, creatine, vitamin D,
dopamine agonists
Promising candidates – BIIB054 (cinpanemab) targets abnormal
alpha-synuclein, BIIB094 (LRRK2 ASO) antisense oligonucleotide
helps reduce LRRK2 protein, small molecules may also be helpful,
agents that down regulate inflammation especially via type-2
astrocytes
19
Symptomatic MonotherapyEfficacious – clinically useful• Dopamine
agonists – non-ergot, ergot• Levodopa + peripheral decarboxylase
inhibitor – immediate release, controlled
release, extended release
• Monoamine oxidase inhibitors – B-selective, eg, rasagiline,
selegiline
Likely efficacious – clinically useful or possibly useful•
Anticholinergics• Amantadine
20
Adjunctive TherapiesEfficacious – clinically useful• Dopamine
agonists• Rasagiline
Likely efficacious – clinically useful or possibly useful•
Anticholinergics• Amantadine
21
-
12/2/20
8
Okun MS. N EnglJ Med 2012;367:1529-1538.
Electrode Implantation for Deep-Brain Stimulation.
22
Deep Brain StimulationPotential benefits:• Reduces motor signs
of the disease• Improves off time• Improves dyskinesia, especially
GPi DBS• STN may allow dopamine reduction
Potential adverse effects:• Speech and cognitive impairment•
Gait changes
23
Key Points
• Symptomatic therapies are predominantly focused on motor
symptoms and are based on increasing dopamine levels
• Adjunctive therapies are used when patients are deemed to be
“undertreated” with monotherapy
• Deep brain stimulation is a viable option for many and earlier
use and broader application of this intervention is being
explored
24
-
12/2/20
9
Motor complications of dopaminergic therapy
25
Levodopa Induced DyskinesiaHyperkinetic involuntary movements of
upper and lower limbs, trunk, and less often facial muscles
May occasionally have dystonic posturing
~40% experience dyskinesia after 4-6 years of levodopa
treatment
Dyskinesia is associated with longer duration of PD and higher
levodopa doses (more than length of time on levodopa therapy)
Dyskinesia is most likely at ‘peak’ dose—high levodopa
concentrations
26
On-off dopamine medication fluctuations
Stacey M. and Hauser R. 2007
27
-
12/2/20
10
On-off Dopamine Medication Fluctuations
Most of end-of-dose deterioration (return of motor symptoms)
Occur in >50% of patients at 5 years and nearly 100% at 10
years
Disease duration, exposure to levodopa and cumulative dose,
delayed or erratic gastric emptying, female sex, low body weight,
and young disease onset
High protein meals interfere with absorption
In rare cases, can occur as early as 6 months after initiating
dopaminergic therapy
Most associated with levodopa, but can occur with agonists
Non-motor fluctuations often occur in conjunction with motor
fluctuations
28
Recognizing Off-Periods (and Other Complications of Therapy)
Ask patients to keep a symptom journal
Suggest they anchor journal entries by noting the time they take
PD medications
Do off-periods occur at every dosing interval? Or only after
meals?
During what interval of time, relative to medication dosing, do
off-periods occur? Dose failure? End-of-dose wearing off?
Do any other (non-motor) symptoms occur during off periods?
29
Prevent or Delay of Motor ComplicationsEfficacious – clinically
useful• Dopamine agonists
30
-
12/2/20
11
Treatments for Motor FluctuationsEfficacious – clinically
useful• Dopamine agonists
• Levodopa with peripheral decarboxylase inhibitor, several
forms, standard, extended release, intestinal infusion
• COMT inhibitors, eg, entacapone• MAOI-B or MAOI-B plus channel
blockers• Bilateral STN or GPi DBS
• Unilateral pallidotomy
Likely efficacious – possibly useful• Istradefylline (adenosine
A2A antagonist)• Apomorphine SC
31
Treatments for DyskinesiaEfficacious – clinically useful•
Amantadine• Clozapine, but requires special monitoring• Bilateral
STN or GPi DBS• Unilateral pallidotomy
Likely efficacious – clinically useful• Intestinal infusion of
levodopa
32
Key Points
• Motor complications of dopaminergic therapy include dyskinesia
and on-off fluctuations
• Disease duration, rather than time of exposure to levodopa, is
thought to be the main factor associated with the development of
motor complications
• Motor complications are most typical of moderate to advanced
disease
33
-
12/2/20
12
Case vignettes
34
63 year old right handed male with new onset rest tremor in left
hand, mild bradykinesia and rigidity
carbidopa/levodopa 25/100mg 1 tablet 3 times daily
rasagiline 1 mg daily
rotigotine transdermal patch
trihexyphenidyl
35
72 year old right handed male with an 8 year PD hx, no tremor,
moderate bradykinesia and rigidity, severe dyskinesia on standard
levodopa Q3 hours
amantadine
rasagiline 1 mg daily
surgery, eg, GPi DBS
transition to extended release levodopa
36
-
12/2/20
13
56 year old right handed female with PD onset at age 42, now
with bilateral symptoms, severe on-off fluctuations and moderate
dyskinesia on levodopa 5/day
amantadine
bilateral deep brain stimulation
pramipexole extended release
COMT inhibitor
37
Any Questions?
38
ReferencesArmstrong MJ, Okun MS. Diagnosis and Treatment of
Parkinson Disease: A Review. JAMA. 2020 Feb 11;323(6):548-560. doi:
10.1001/jama.2019.22360. PMID: 32044947.
Fox SH, Katzenschlager R, Lim SY, Barton B, de Bie RMA, Seppi K,
Coelho M, Sampaio C; Movement Disorder Society Evidence-Based
Medicine Committee. International Parkinson and movement disorder
society evidence-based medicine review: Update on treatments for
the motor symptoms of Parkinson's disease. Mov Disord. 2018
Aug;33(8):1248-1266. doi: 10.1002/mds.27372. Epub 2018 Mar 23.
Erratum in: Mov Disord. 2018 Dec;33(12):1992. PMID: 29570866.
Reich SG, Savitt JM. Parkinson's Disease. Med Clin North Am.
2019 Mar;103(2):337-350. doi: 10.1016/j.mcna.2018.10.014. Epub 2018
Dec 3. PMID: 30704685.
39