Embed Size (px)
Citation preview

INTRODUCTION
METHODS
RESULTS
DISCUSSION
§ Attention-deficit/hyperactivitydisorder(ADHD)ischaracterizedbyinattention,hyperactivity,andimpulsivitythatimpairdailyfunctioning(AmericanPsychiatricAssociation,APA,2013).Approximately5-11%ofschool-agedchildrenintheUnitedStateshavebeendiagnosedwithADHD(APA,2013;CentersforDiseaseControl,2011).
§ ChildrenwithADHDexhibitdeficitsinsocialfunctioning(Maedgen &Carlson,2000),haveimpairedrelationshipswiththeirpeers(Hoza etal.,2005),scoresignificantlylowerinacademicachievement(Latimeretal.,2003),andhaveanincreasedriskofsuspensionandexpulsionfromschoolcomparedtochildrenwithoutADHD(Martin,2014).Additionally,childrenwithADHDfrequentlyexhibitexternalizingbehaviorproblems(Kuja-Halkola,Lichtenstein,D'Onofrio,&Larsson,2015),and27%haveacomorbiddiagnosisofconductdisorder(Larson,Russ,Kahn,&Halfon,2011).
§ ResearchhasdemonstratedthatcaregiversofchildrenwithADHDhavepoorerparentingpracticeswhencomparedtocaregiversoftypicallydevelopingchildren(e.g.,Johnston&Mash,2001).Thiscanbeespeciallyproblematic,asnegativeparentingandconductproblemsmayhaveabidirectionalrelationinfamiliesofachildwithADHD(e.g.,Johnston&Mash,2001).
§ Forexample,studieshavefoundthatnegativeparentingpracticescanpredictconductproblemsovertime(e.g.,August,Realmuto,Joyce,&Hektner,1999).Additionally,thepresenceofchildconductproblemshasbeenshowntoincreasenegativeparentingbehaviors(Pardini,Fite,&Burke,2008).Further,negativeparentingmayinteractwithchildren’sADHDsymptomstoputthematgreaterriskforconductproblems(Loeber,Green,Lahey,Frick,&McBurnett,2000),
§ However,therelationsbetweenADHDsymptoms,conductproblems,andparentingpracticesstillremainunclear,andfurtherresearchisneededtobetterunderstandhowfamilyfactorsinfluencebothADHDandconductproblems(Johnston&Mash,2001).Toaddressthisissue,thepresentstudyevaluatedthethree-wayinteractionamongADHDsymptoms,negativeparenting,andpositiveparentingpredictingconductproblems.
§ Asexpected,negativeparentingpredicteduniquevarianceinchildconductproblems,withelevatedlevelsofnegativeparentingpredictingmoresevereconductproblems.Positiveparentingpredictedanamountofvarianceapproachingsignificance,withelevatedlevelsofpositiveparentingpredictinglowerlevelsofconductproblems.AlthoughADHDsymptomsweresignificantlycorrelatedwithconductproblems,itdidnotpredictuniquevarianceinthismodelconsideringotherpredictors.
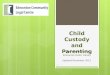
§ TheinteractionbetweennegativeparentingandADHDsymptomswasnonsignificant.TherewasasignificantinteractionbetweenpositiveparentingandADHDsymptomswithconductproblemsbeinglowerwhenADHDsymptomswerelowerregardlessofpositiveparenting.However,whenADHDsymptomswerehigher,conductproblemswerelowerifpositiveparentingwashigher.
§ Theinteractionbetweennegativeandpositiveparentingapproachedsignificancewithconductproblemstendingtobehighestwithhighernegativeparentingandlowerpositiveparenting,andconductproblemstendingtobelowestwithlowernegativeparentingandhigherpositiveparenting.
§ Thethree-wayinteractionamongADHDsymptoms,negativeparenting,andpositiveparentingwasnonsignificant.Overall,resultssuggesttheimportanceofparentingbehaviorsonchildconductproblems,forchildrenwithandwithoutADHDsymptoms.
§ ThisstudywaslimitedbyitsrelianceonparentreportforchildADHDsymptomsandconductproblems.Studiesshouldincludebehavioralobservationsforchildreninadditiontostandardassessments,asbehavioralobservationsareconsideredthestandardforobjectivityinbehavioralresearch(Pelham,Fabiano,&Massetti,2005).
§ Futureresearchshouldincludealargersampleofcaregiversfromamorediversebackgroundtoincreasethegeneralizabilityoftheresults.Becausethesedataarecorrelational,causalrelationsbetweenvariablescannotbeassumed.Futurestudiesshouldimplementalongitudinaldesignsotemporalsequencingofthevariablescanbedetermined,thussheddingmorelightonpotentialcausalrelations.
§ Additionally,futurestudiesshouldcontinuetodiscoverwaystodecreasenegativeparenting,asdecreasesinnegativeparentinghavebeenassociatedwithdecreasesindisruptivebehaviorforchildrenwithADHD(Chronis-Tuscano etal.,2011).
ParentingBehaviorandChildADHDSymptomsPredictingConductProblemsRebeccaA.Lindsey,StephanieSaltness,&TammyD.Barry
WashingtonStateUniversity
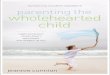
*p <.05,**p < .01,***p <.001
Table1.BivariateCorrelationsbetweenParentingXXXBehaviors,ChildADHDSymptoms,andChildConductProblems
§ PositiveparentingwasnegativelycorrelatedwithADHDsymptoms,r =-.27,p=.04,conductproblems, r =-.32,p=.01,andnegativeparenting, r =-.29,p =.03.NegativeparentingwaspositivelycorrelatedwithADHDsymptoms,r =.45,p<.001,andconductproblems, r =.44,p<.001.ADHDsymptomsandconductproblemswerepositivelycorrelated,r =.46,p<.001(Table1).
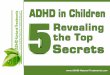
§ Athree-wayinteractionmodelwithADHDsymptoms,negativeparenting,andpositiveparentingpredictingchildconductproblemswastested.Theoverallmodelaccountedforastatisticallysignificantamountvarianceinchildconductproblems,R2 =.41,F (7,51)=5.00,p =.0002(Table2).
§ Therewasamaineffectfornegativeparenting,b=3.95,SE=1.45,p=.009,butnotforADHDsymptoms,b=.18,SE=.18,p=.32.Themaineffectforpositiveparentingapproachedsignificance,b=-6.38,SE=3.28,p=.06(Table2).
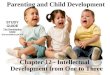
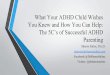
§ TherewasnointeractionbetweennegativeparentingandADHDsymptoms,b=.05,SE=.12,p=.67.TherewasasignificantinteractionbetweenpositiveparentingandADHDsymptoms,b=-.75,SE=.30,p=.02(Table2; plottedinFigure1).Theinteractionbetweenpositiveparentingandnegativeparentingapproachedsignificance,b=4.10,SE=2.18,p=.07(Table2;plottedinFigure2).
§ Thethree-wayinteractionwasnotsignificant,b=.24,SE=.30,p=.44(Table2).
Table2.ResultsofModeratedMultipleRegressionofChildADHDSymptomsandParentingBehaviorsPredictingChildConductProblems
Note.R2 andR2∆forinteractionmodelareshowninbold.Unstandardized regressioncoefficientsarereportedforeachpredictor.Standarderrorsareshowninparentheses.*p <.05.***p <.001.† Trend;p<.10.
PositiveParenting
NegativeParenting
ADHDSymptoms
ConductProblems
PositiveParenting ---
NegativeParenting -.29* ---
ADHDSymptoms -.27* .45*** ---
ConductProblems -.32** .44*** .46*** ---
Predictors ChildConductProblems
InteractionModelR2 5.00***InteractionModelR2∆ .03ChildADHDSymptoms .18(0.18)NegativeParenting 3.95(1.45)***PositiveParenting -6.38(3.28) †ChildADHDSymptomsXNegativeParenting .05(0.12)ChildADHDSymptomsXPositiveParenting -.75(0.30)*PositiveParentingXNegativeParenting 4.10(2.18) †ChildADHDSymptomsXNegativeParentingXPositiveParenting .24(0.30)
Figure1.ReducedRegressionModelwithChildADHDSymptomsPredictingChildConductProblemsatDifferentLevelsofPositiveParenting
Figure2.ReducedRegressionModelwithNegativeParentingPredictingChildConductProblemsatDifferentLevelsofPositiveParenting
Participants§ Participantswere59caregivers(56females,3males)andtheir59children(25females,34males).Caregivers
wereages24to68years(M =38.11;SD =8.32).§ Childrenwereages8to13years(M =10.53;SD =1.22),andthemajoritywereidentifiedasEuropeanAmerican
(67.8%)andAfricanAmerican(30.2%).
Measures§ Caregiverscompletedabatteryofassessmentsincluding:
§ DSM-IVADHDChecklist– ParentForm,adaptedfromtheDiagnosticandStatisticalManualofMentalDisorders(DSM-IV;AmericanPsychiatricAssociation,1994).Thischecklistincludesalistofthenineinattentionsymptomsandtheninehyperactivity-impulsivitysymptomsofADHD.
§ BehaviorAssessmentSystemforChildren- ParentRatingScale(BASC-PRS;Reynolds&Kamphaus,1992).TheBASC-PRSisanomnibusratingscaledesignedtotakeabroadsamplingofachild’sbehavior.Caregiversratehowoftentheyobservethechildengaginginvariousbehaviorsona4-pointscale,rangingfrom“never”to“always.”TheConductProblemsSubscaleT-scorewasusedastheoutcomevariable.
§ AlabamaParentingQuestionnaire(APQ;Sheltonetal.,1996).TheAPQisa42-itemmeasurewhichassessesthefrequencyofthefollowingparentingpractices:ParentalInvolvement,PositiveParenting,PoorMonitoring/Supervision,InconsistentDiscipline,andCorporalPunishment.Itemsareratedona5-pointscale,rangingfrom1(never)to5(always).§ ThePositiveParentingdomainwasusedtomeasurepositiveparenting.ThePoor
Monitoring/Supervision,InconsistentDiscipline,andCorporalPunishmentdomainswerecombinedtocreateanegativeparentingvariable.
Procedures§ ThisprojectwasapprovedandconductedincompliancewiththeUniversityInstitutionalReviewBoard.
ParticipantswerepartofalargerstudyinvestigatingADHDsymptomatologyandaggression.§ Caregiversreadtheinformedconsentletterpriortoparticipation.Theyreceived$20fortheirparticipationinthe
study ascompensationfortheirtime.
0
10
20
30
40
50
60
70
Low ADHD High ADHD
Cond
uct P
robl
ems
Low Positive Parenting
High Positive Parenting
b =.69, SE =.20,p =.001
b =.24, SE =.22,p =.27
0
10
20
30
40
50
60
70
Low Negative Parenting High Negative Parenting
Cond
uct P
robl
ems
Low Positive Parenting
High Positive Parenting
b =2.18, SE =1.91,p =.26
b =6.37, SE =1.84,p =.001