Embed Size (px)
Citation preview
Parenteral Nutrition Policy v3
Policy No: RM60
Version: 3.0
Name of Policy: Parenteral Nutrition Policy
Effective From: 18/08/2015
Date Ratified 12/08/2015
Ratified SafeCare Council
Review Date 01/08/2017
Sponsor Director of Nursing, Midwifery and Quality
Expiry Date 11/08/2018
Withdrawn Date
Unless this copy has been taken directly from the Trust intranet site (Pandora) there is no assurance that
this is the most up to date version
This policy supersedes all previous issues

Parenteral Nutrition Policy v3 2
Version Control
Version Release Author/Reviewer Ratified
by/Authorised
by
Date Changes
(Please identify page
no.)
1.0
February
2009
Nutrition and
Dietetics
SafeCare
Council
Feb 2009 General update in line
with national guidelines
Page 7, 9, 14, 18, 20, 22
2.0
December
2011
N&DS SafeCare
Council
Dec 2011 General update page 4
3.0
18/08/2015 N&DS SafeCare
Council
12/08/2015 General update page 4,
5, 7,8, 9, 17, 18

Parenteral Nutrition Policy v3 3
Contents
Section Page
1 Introduction ................................................................................................................................. 4
2 Policy Scope .................................................................................................................................. 4
3 Aim of policy ................................................................................................................................. 4
4 Roles and responsibilities ............................................................................................................. 4
5 Definitions .................................................................................................................................... 5
6 Managing parenteral nutrition ..................................................................................................... 5
6.1 Indications of parenteral nutrition ................................................................................. 5
6.2 Patient Assessment ........................................................................................................ 5
6.3 Parenteral access routes ................................................................................................. 6
6.4 Types of catheters used for parenteral nutrition ............................................................ 7
6.5 Composition of parenteral nutrition .............................................................................. 7
6.6 Prescribing parenteral nutrition ..................................................................................... 8
6.7 Storing parenteral nutrition ........................................................................................... 8
6.8 Administrating parenteral nutrition ............................................................................... 8
6.9 Discontinuing parenteral nutrition ................................................................................. 9
6.10 Monitoring for patient on parenteral nutrition ............................................................. 9
6.11 Laboratory monitoring for patient on parenteral nutrition ............................................ 9
6.12 Ethical Considerations ..................................................................................................... 10
7 Training ......................................................................................................................................... 10
8 Equality and Diversity .................................................................................................................. 10
9 Monitoring compliance with the policy ....................................................................................... 10
10 Consultation and review ............................................................................................................... 10
11 Implementation of the policy ....................................................................................................... 10
12 References ................................................................................................................................... 11
13 Associated documentation ........................................................................................................... 11
Appendices
Appendix 1 Nutrition Risk Score ........................................................................................................ 12
Appendix 2 Nutrition Support team referral document .................................................................... 13
Appendix 3 Parenteral nutrition proforma including prescription .................................................... 14
Appendix 4 Parenteral Nutrition Regimen form ............................................................................... 17
Appendix 5 Emergency out of hours guidelines ................................................................................ 18
Appendix 6 Monitoring patients on PN .............................................................................................. 22
Appendix 7 Biochemical monitoring of patients on PN. .................................................................... 24

Parenteral Nutrition Policy v3 4
Parenteral Nutrition Policy
1 Introduction
Parenteral nutrition (PN) is the administration of nutrients through the intravenous route. It is a
specialised form of nutrition support, with associated complications and should be carefully
considered and planned on an individual basis. This PN policy was reviewed in line with national
guidance ‘Nutrition Support in adults NICE clinical guideline No 32 (2006)’, and National confidential
enquiry into patient outcome and death: A mixed bag: an enquiry into the care of hospital patients
receiving parenteral nutrition. June 2010’.
2 Policy scope
This is a trust wide policy aimed at all health care professionals involved in the care of patients
receiving parenteral nutrition, to ensure best practice is applied in accordance with national
guidelines.
3 Aim of Policy
The aim of the PN policy is to ensure that PN is used in appropriate circumstances, that it is
administered safely and with appropriate monitoring to prevent potential complications.
4 Roles and Responsibilities
Nursing Staff
Ward nurses have a responsibility to assess all patients’ nutritional status using the Trust’s Nutrition
Risk Score (NRS) tool on admission, and then repeated weekly and if a patient’s clinical condition
changes (Appendix 1). Nursing staff must inform the Nutrition and Dietetics department if a patient
is due to begin PN. Nursing staff are responsible for administering PN with aseptic technique and
monitoring the patients fluid balance, GI function and vital signs for potential line sepsis.
Medical Staff
Medical staff have a responsibility to consider patients for PN if they are unable to maintain or
improve their nutritional status via the oral or enteral route. The decision to commence PN should
be discussed with the Consultant with overall clinical care for the patient. Nasogastric and
nasojejunal feeding must be considered prior to requesting PN. Medical staff are responsible for
organising insertion of appropriate venous access, ideally a central line. They are also responsible
for requesting and monitoring daily biochemistry and considering whether the patient is at risk of
re-feeding syndrome. If there is a significant risk of re-feeding, Pabrinex should be prescribed in
addition to PN. The medical staff are responsible for assessing the patient’s fluid balance and
prescribing appropriate fluids. The volume of PN prescribed should always be taken into account to
avoid inappropriate fluid overload.
Dietitian
Patients who are identified as requiring PN should be referred to the ward dietitian immediately.
The dietitian has a responsibility to assess the patient’s nutritional requirements and to ensure that
the most appropriate PN solution and infusion rate is chosen. They should highlight if the patient is
at risk of re-feeding syndrome, which requires close monitoring of electrolytes and the prescription
of additional vitamins. They should review the patient on a daily basis until the patient is
established on PN to allow alterations to the prescription in terms of electrolytes, macronutrients
and volume delivered.

Parenteral Nutrition Policy v3 5
Pharmacy
The aseptic services pharmacist should liaise with the dietitian on a daily basis (Monday to Friday)
to check for updates on the patient, discuss biochemistry and the PN prescription. They should
check that the alterations to the electrolytes are clinically appropriate and within the limits of
stability for the regimen and the route of administration.
Nutrition Support Team
This is a multidisciplinary team led by a Gastroenterologist. The team will accept referrals from
medical and surgical teams to advise on the management of patients with complicated nutritional
issues. The team is happy to review patients being considered for PN. The team is also responsible
for providing support and education on the methods of PN and also to ensure that policies and
guidelines are up to date in accordance with national guidelines to ensure best practice.
Acute Response Team
ART provide daily reviews of all central lines, to ensure that best practice is maintained. ART
provide support and advice regarding all aspects of central line management and PN
administration.
Infection Control Team
The Infection Control Team provides support and advice regarding good aseptic technique for all
staff administering PN. They also have a responsibility to monitor and investigate episodes of line
sepsis.
5 Definitions
The term ‘total parenteral nutrition’ (TPN) is used when patients are receiving their full
requirements through the venous route without any enteral nutrition.
6. Parenteral Nutrition Policy v3
6.1 Indications for Usage of parenteral nutrition
PN should only be considered when it is not possible to meet the patients full nutritional
requirements using oral or enteral feeding routes (nasogastric or nasojejunal feeding), i.e. if
the gut works, use it.
Examples of appropriate conditions where PN may be used:
• Extended non-absorption of enteral nutrition (This must include a trial of
Nasojejunal feeding)
• Post operative ileus
• Intractable vomiting
• Major GI surgery where enteral nutrition is contraindicated, e.g. perforation
• Short bowel syndrome
• Extensive Crohn’s disease where nutrient absorption is severely impaired
• High output fistula where position and volume prevent enteral feeding
• Motility disorders such as Sclerodema and chronic intestinal obstruction syndromes
This list is not exhaustive and the risks/benefits of providing PN and the expected duration
of PN should be considered on an individual basis.
6.2 Patient Assessment
A multidisciplinary team can improve patient care while reducing the complications of PN.

Parenteral Nutrition Policy v3 6
When concerns are expressed about a patient’s nutritional status contact the dietitian who
covers your ward via bleep or on ext 2074 (Nutrition and Dietetic Department) or refer to
the Nutrition Support Team (see Appendix 2).
The following assessments should also be carried out within the team:
Initial
Assessment
Rationale
Responsibility
Weight and
height
Measured on admission and weekly
thereafter. To assess nutritional status
Nursing staff and dietitian
Hydration
status
To ensure adequate hydration. Oedema
and ascites should be noted.
Nursing and medical staff
Fluid balance Input and output should be clearly
documented. Ensure adequate
hydration and avoid over hydration. NB
volume of PN should be taken into
account when calculating fluid input.
Nursing and medical staff
Temperature To ensure no underlying infections or
complications.
Nursing and medical staff
Biochemistry Urea and electrolytes, glucose, liver
function tests, phosphate, magnesium,
calcium, haemoglobin,
coagulation and trace elements
Medical staff, dietitian
Gut function Is the gut functioning?
Are there any gastrointestinal
problems?
Tolerance to enteral nutrition?
Medical staff
Nutritional
assessment
Any changes in weight?
Any changes in appetite?
History of oral intake?
Any intake at present?
Nursing and medical staff,
dietitian
Venous access Ensure good venous access with no
complications
Medical staff
Medications Drug-nutrient interactions.
Establish whether medications are
affecting GI function/clinical condition.
Medical staff, pharmacist,
dietitian
Adapted from NICE (2006) Nutrition support in adults
6.3 Parenteral Access Routes
Peripheral access
Peripheral PN may be considered via a large peripheral vein but it is not routinely
recommended. Peripheral PN carries a high risk of thrombophlebitis and venflons need to
be changed on a daily basis. With care and attention the peripheral route can be used for
short term PN prior to central access being obtained. It should be ensured that the
osmolarity of the solution is compatible with the peripheral route. When using peripheral
access a small (20G) cannula should be used only for PN. Cyclical delivery of parenteral

Parenteral Nutrition Policy v3 7
nutrition should be considered with planned routine cannula change, eg, deliver PN over 18
hrs, remove the cannula post infusion and resite a new cannula in the other arm.
Central access
Central access is normally used for those patients requiring PN. The decision regarding
appropriate line insertion should be taken by the referring team on discussion with the
Nutrition team. Only healthcare professionals competent in catheter placement should
place catheters and should be aware of monitoring and managing them safely. Catheter
insertion should be planned and performed using aseptic precautions. (See Central Venous
Line Policy.)
The referring team need to discuss tunnelled line insertion with the Interventional
radiology department or Vascular Surgery. If there is a significant delay in inserting a
tunnelled line or the duration of PN is such that this is deemed unnecessary the referring
team should refer the patient to Anaesthetics for line insertion. The referrer needs to
ensure that the Anaesthetist inserting the line is aware it will be used for PN so that an
appropriate line is inserted (single rather than a quadruple lumen).
An X-ray will confirm the correct placement of the catheter tip. A single lumen dedicated
catheter is recommended for PN to minimise the risk of line sepsis. The tip should be
positioned in the lower one third of the SVC or at the junction of the SVC and right atrium.
Correct positioning reduces the risk of thrombotic and mechanical complications. The date
and site of insertion and tip position should be documented in the patient’s notes.
Other Access Routes
PICC lines are not commonly used in Gateshead. These can also be used to deliver
hyperosmolar solutions as the catheter tip lies in the superior vena cava.
6.4 Types of Central Catheters Used
Multi-lumen
These are used in patients who require other additional infusions, however can be
associated with an increased risk of infection due to increased handling and greater number
of ports available for bacterial colonisation. Strict aseptic techniques should be carried out
when changing infusion or handling the multiple ports. If a multi lumen line is used for PN a
line should be dedicated to PN only.
Single lumen
Traditionally preferred lumen to be used for administration of PN as there is reduced risk of
infection.
Double lumen
May be appropriate if the patient is likely to require an additional infusion alongside the PN
(e.g. antibiotics, or fluid).
Tunnelled Central Line
Tunnelled lines such as Groshong or Hickman Lines are sited for long term PN access, ie
more than 7 days.
6.5 Composition of parenteral nutrition
An all-in-one parenteral bag is used in Gateshead Health NHS Foundation Trust which
contains a combination of amino acid solution, fat emulsion, glucose solution, water and fat
soluble vitamins, trace elements, minerals and electrolytes to desired volume. Additional

Parenteral Nutrition Policy v3 8
ingredients may be added if required. Additions must be added aseptically in the hospital
pharmacy only.
6.6 Prescribing parenteral nutrition
Nutritional requirements must be assessed by the ward’s dietitian. Following a dietetic
assessment a bag of PN will be recommended based on the patient’s nutritional
requirements. A PN proforma, which includes a prescription, must be completed to ensure
PN is given safely and appropriately (see Appendix 3). The dietitian will complete a PN
regimen form for the ward staff to follow (see appendix 4).
The prescription must be completed and signed by the doctor. It should be delivered to the
pharmacy department before 2pm on the day it is required. When a patient is stable a PN a
prescription may be written for a week at a time. It also must be prescribed on the fluid
balance chart on a daily basis.
PN is not an emergency intervention and is therefore rarely indicated outside normal
working hours. However if PN is required outside pharmacy hours then an emergency
Triomel 6 g bag can be used (see Appendix 5 for emergency out of hours regimen). These
are stored in the pharmacy emergency drug cupboard and may be accessed via the site
manager. The on-call pharmacist is available for advice via switchboard. Each PN bag will
be prescribed according to their nutritional requirements.
Modifications of parenteral nutrition bags
The electrolyte content (sodium etc) of the PN bag can be altered within certain limits. The
ward dietitian will advise and liaise with pharmacy regarding changes to the PN electrolyte
content. Manipulation of the PN in Pharmacy is time consuming and carries a very small risk
of introducing infection, therefore minor changes should be avoided.
6.7 Storage of parenteral nutrition
PN should be stored in a drug refrigerator (2-8oC) and has a limited storage life. Occasional
minor separation of the emulsion may be visible. Always agitate the bag gently before use.
Protect PN from strong light using the grey bag covers supplied by pharmacy. Once
removed from the refrigerator the bag should be warmed to room temperature before use.
Warming should be achieved gradually by putting the bag on a work surface in the
treatment room at ambient temperature for a period of 1-2 hours out of direct sunlight.
Artificial heat, for example, placing the bag on a radiator or using a light source should
never be used as it poses a significant risk to bag stability. Any bag that has been stored
below 2oC must not be used.
6.8 Administering parenteral nutrition
The PN bag will arrive on the ward late afternoon or early evening. If the patient is at risk
of Refeeding Syndrome, PN should be introduced progressively as advised by the dietitian,
usually starting at no more than 50% of estimated requirements for the first 24-48 hours.
(See Refeeding Syndrome Guidelines). All PN mixtures will be administered through
standard IV giving set using a volumetric pump with occlusion and air line alarms.
Continuous administration of PN should be offered as the preferred method of infusion in
severely ill patients. Gradual change from continuous to cyclical delivery should be
considered in patients requiring PN for more than 2 weeks, it is important to adhere to
recommendations from the CCOT reduce central line associated sepsis.

Parenteral Nutrition Policy v3 9
Cyclical delivery of PN may be considered when using short term peripheral venous
cannulae with planned routine catheter changes. The rate of administration is usually
identified on the label of the PN bag; however alterations to the rate can be made following
discussion with the dietitian or aseptic pharmacist. PN should only be administered over a
maximum 24 hour period and bags should be changed every 24 hours.
6.9 Discontinuing parenteral nutrition
PN can be withdrawn once adequate oral or enteral nutrition is tolerated and nutritional
status is stable. There is usually a period of overlap while enteral feeding is being
established and the rate of PN can be reduced. The dietitian will provide a step by step
weaning plan for the PN and introduction of enteral or oral nutrition which will be reviewed
daily. Stopping PN abruptly may put the patient at risk of rebound hypoglycaemia and
should be avoided.
6.10 Monitoring of parenteral nutrition (NICE, 2006)
It is the responsibility of the ward doctors to monitor the patient appropriately for possible
complications of PN. These are predominately metabolic and line related complications.
The functioning of the gut and the possibility of introducing enteral feeding should also be
monitored (see appendix 6).
6.11 Laboratory Monitoring (NICE, 2006)
Please refer to Appendix 7. The Nutrition team, ward dietitian and pharmacist can advise
regarding vitamin supplementation and the addition of electrolytes to PN. Manganese,
selenium and bone densitometry need to be measured in patients on long term home PN,
however home PN is managed by the Nutrition team at Freeman Hospital
Biochemical Abnormalities in patients on PN
Both acute and long-term liver function abnormalities are associated with the provision of
parenteral nutrition. It can be difficult to establish whether the liver problem is caused by
the administration of parenteral nutrition in the acute setting, or if it is due to other clinical
problems eg:
• Sepsis
• Biliary obstruction
• Unrecognised previous chronic liver disease
• New-onset liver disease (eg liver abscess, adverse drug reaction, hepatitis)
• Portal bacterial translocation
A modest increase in ALT sometimes seen within the first few days to weeks is usually a
consequence of steatosis and is commonly seen following excessive glucose provision in a
malnourished patient. There is usually very little or no change in the liver’s synthetic
function and the increase in ALT is generally not clinically significant. Following prolonged
administration (several weeks to months) of parenteral nutrition a cholestatic picture may
develop. The commonest reason for the development of intra-hepatic cholestasis is the
overprovision on lipid and/or glucose. Patients at risk of developing intra-hepatic
cholestasis may benefit from a reduction in lipid and glucose load (contact ward dietitian
for advice). Cholestatic problems are also commonly encountered in patients with very
short bowel syndrome or high stomal losses. Bacterial translocation across the damaged
gut wall may also result in liver damage and a course of appropriate antibiotics may be
required.

Parenteral Nutrition Policy v3 10
6.12 Ethical Considerations
Parenteral nutrition is an invasive procedure, and therefore members of staff are expected
to have assessed the patient’s capacity to consent, and taken into consideration any
advanced decision to refuse treatment, or best interest assessment. Further information is
available in OP 57 Deprivation of Liberty Safeguards and OP25 Advanced Decisions to
Refuse Treatment.
7 Training
The trust’s nutrition team can provide training to all health care professionals involved in parenteral
nutrition. The team is actively involved in the F1 and F2 teaching program and parenteral nutrition
forms part of their training. Dietitians working within the hospital receive training by the critical
care dietitian.
8 Equality and Diversity
Patients who cannot be fed sufficiently via enteral nutrition have a fundamental right to
consideration of parenteral nutrition, because this supports the right to life. This policy therefore
promotes a human rights based approach to healthcare. However staff should refer to other
policies for information about issues of consent, capacity, advance care plans, refusing or
withdrawing treatment. This policy has been appropriately equality impact assessed.
9 Monitoring compliance with the policy
Standard/process/issue Assurance
Method By Committee Frequency
NICE G32 Adult nutrition
support
Regional PN
audits
Nutrition
and
Dietetics
Nutrition
Steering
committee
Annually
PN policy compliance
exceptions
All exceptions to
be Datix
By staff
who
identify
exception
Correlated by
Risk
Management
Department
As required
All patients on TPN in the
Queen Elizabeth
Discussion Nutrition
tean MDT
Nutrition
Steering
Committee
quarterly
The effectiveness of the policy will be monitored by the nutrition & dietetics service in line with
national guidance. PN audits will be undertaken on a yearly basis as part of Nutrition Support Team
audit program. Any incident involving parenteral nutrition should be recorded via Datix reporting.
10 Consultation and review
The policy will be reviewed every 2 years. Consultation will include Nutrition and Dietetics,
Pharmacy, the trust’s Nutrition, Critical care outreach and Infection control teams.
11 Implementation of the policy
The policy will be shared with all staff involved in the direct care of patients receiving parenteral
nutrition, all ward managers and modern matrons, and all staff receiving training on parenteral
nutrition.
Parenteral Nutrition Policy v3 11
12 References
1 Nutrition Support in adults NICE clinical guideline No 32 (2006).
2 Bozzetti F, Braga, Gianotti C, Mariani L, Cozzaglio L et al. Perioperative PN in
malnourished, gastrointestinal cancer patients: a randomized, clinical trial. JPEN
(2000),24(1):7-14.
3 The Veterans Affairs Total PN Cooperative Study Group. Perioperative total PN in surgical
patients. New England Journal of Medicing (1991), 325(8):525-32.
4 Infection control: prevention of healthcare-associated infection in primary and community
care. NICE Clinical Guideline. No 2 (2003).
5 Mallet, J Bailey C. Manual of clinical nursing procedures. The Royal Marsden Trust 1996.
6 National confidential enquiry into patient outcome and death: A mixed bag: an enquiry into
the care of hospital patients receiving parenteral nutrition. June 2010.
7 Prescribing Adult Intravenous Nutrition (eds. Austin and Stroud). 2007. Pharmaceutical
Press
13 Associated documentation
• Care standards: 9C and 9D
• Nutrition policy RM61
• Central Venous Line policy OP41
• Refeeding Syndrome guidelines
• Nutrition Risk Score
• Parenteral Nutrition proforma
• Parenteral Nutrition regimen information

Parenteral Nutrition Policy v3 12
Appendix 1

Parenteral Nutrition Policy v3 13
Appendix 2
Gateshead Health NHS Foundation Trust
Nutrition Support Team
REFERRAL FORM
Date of referral: …………………………………………………..
Patient’s name: …………………………………………………..
Hospital
No: ……………………………..
Address: ………………………………………………….. DOA: ……………………………..
…………………………………………………..
…………………………………………………..
Contact number: …………………………………………………..
Ward: …………………… Directorate: ……………………………… Consultant: …………………………..
DOB: …………………… Age: ……………………………...
Medical History: …………………………………………………………………………………………………………..
…………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………
Social History: ………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………
Reason for referral to NST: ……………………………………………………………………………………………….
…………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………
Medication: …………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………
Weight: ………………… NRS: ………………
Current nutritional support:
Y/N If Y: date started: ...............................
Naso-gastric feeding IV fluids
Sub cut fluids Other Please specify ………………………
Oral nutrition …………………………………………
Note: Please complete page two if referring for PEG
Referred by: …………………………………………
(Print) ……………………………………………
Signed: …………………………………………………..

Parenteral Nutrition Policy v3 14
Appendix 3
Parenteral Nutrition (PN) Proforma
Name: Ward:
DOB: Consultant:
Hospital number: NHS no.
Start Date:
Indication for PN:
Appropriate indications include: intestinal failure, extended non-absorption of enteral nutrition (including a
trial of nasojejunal (NJ) feeding), perforated or obstructed gut not expected to recover within 7 days.
Is nasogastric and nasojejunal feeding contraindicated or has it been unsuccessful? Please circle
Yes/No
PN treatment goal
Is there a risk of refeeding syndrome? Please Circle
Yes/No
Access: Central/peripheral (delete as appropriate)
Type: Single/multiple lumen (delete as appropriate)
Date of insertion:
Weight (kg):
Mid upper arm circumference (cm): (if not possible to obtain weight)
Doctor’s signature …………………...........……...…........... Name: ...................................
(print)
Date …….........…….. Bleep/Ext ………………….….......
Time ......................
Please refer to Nutrition and Dietetics intranet page for guidelines on the use of PN out of hours.
Please file behind Section 5 of the Health Record

Parenteral Nutrition Policy v3 15
Parenteral Nutrition Prescription
Name: Ward:
DOB: Consultant:
Hospital number: Weight (kg):
Date PN started: Prescription start date:
Tick required regimen - For further information contact pharmacy (ext. 2316)
Figures in brackets represent usual maximum electrolyte content per bag – these limits may be extended in
certain circumstances – contact pharmacy for advice.
� g
N
Volum
e
ml
Kcal
Total
non-protein
Na
mmol
K
mmol
Mg
mmol
Ca
mmol
PO4
Mmol
Adult 6
6
1515
1050
900
31.5
(225)
24
(225)
3.3
(8.4)
3
(5.3)
12.7
(22.5)
Starter/refeed
ing bag
Adult 10
1
0
2515
1750
1500
52.5
(375)
40
(375)
5.5
(14)
5
(8.7)
21.2
(37.5)
Low
requirements
Adult 14
1
4
2015
2270
1920
70
(300)
60
(300)
8
(11.2)
7
(7)
30
(30)
Increased
requirements
Adult 18
1
8
2015
2140
1680
70
(300)
60
(300)
8
(11.2)
7
(7)
30
(30)*
Increased N
requirements
Fat-free
14
1
4
2015
1540
1200
70
(300)
60
(300)
5
(30)
4.5
(15)
30
(30)
Fat free bag
Clinimix 14
Other
..............
*Note phosphate limit is only 16mmol if adding Addiphos®
to electrolyte-free N9 2000ml bag
Rate of administration:
Route (delete as
appropriate):
Central/Peripheral*
*Check that the regimen is appropriate for the route of administration - only Adult 6 and Adult 10 can be given
peripherally
Please ensure that the regimen is prescribed on the fluid balance chart on a daily basis.
Dietitian’s Name (print): Signature: Date:
Grade: Bleep: Time:
Doctor’s Name (print): Signature: Date:

Parenteral Nutrition Policy v3 16
Grade: Bleep: Time:
Date
Dietitian
Confirmed
By
(pharmacy
staff)
Pharmacist
Check
Given by: Checked by: Time
Commenced
Version 10 – Approved by David Sproates June 2015 Please check Trust Intranet for the
latest version of this document. Page 16 of 24

Parenteral Nutrition Policy v3 17
Appendix 4
NUTRITION AND DIETETIC SERVICE
Parenteral Nutrition Regimen
Name ........................................................................ Hospital ………………………
Date of Birth ....................................................................... Ward ………………………
Weight ........................................................................
Estimated daily requirements: Kcal ………………………
Nitrogen (g) ………………………
Fluid (ml) ………………………
Sodium (mmol) ………………………
Route of feeding: Peripheral/Central* Potassium (mmol) ………………………
Phosphate (mmol) ………………………
Parenteral Nutrition Bag: ……………………………………... Magnesium (mmol) ………………………
Calcium (mmol) . ................................
Day Rate
ml/hr
Time
(hr)
Rest
(hr)
Provides per 24 hours
Kcal Nitrogen
(g)
Fluid
(ml)
Na+
(mmol)
K+
(mmol)
Ca2+
(mmol)
Mg2+
(mmol)
PO2-
4
(mmol)
Continue as Day: ……………………………. of regimen.
Additional instructions: ...……………………………………………………………………...
……………………………………………………………………………………………………
• Daily bloods including U&E’s, magnesium, phosphate and calcium until stable.
• Check blood glucose 1-2 times daily (more often if needed)
• Check bag is suitable to be given via chosen route
• Change bag every 24 hours, discard any remaining solution
• Document volume administered on fluid balance chart
Dietitian (print name) ………………………… Date....../....../...... Time: ......................
Signature: ..................................................... Contact No: ................ Bleep: .....................
Parenteral Nutrition Policy v3 18
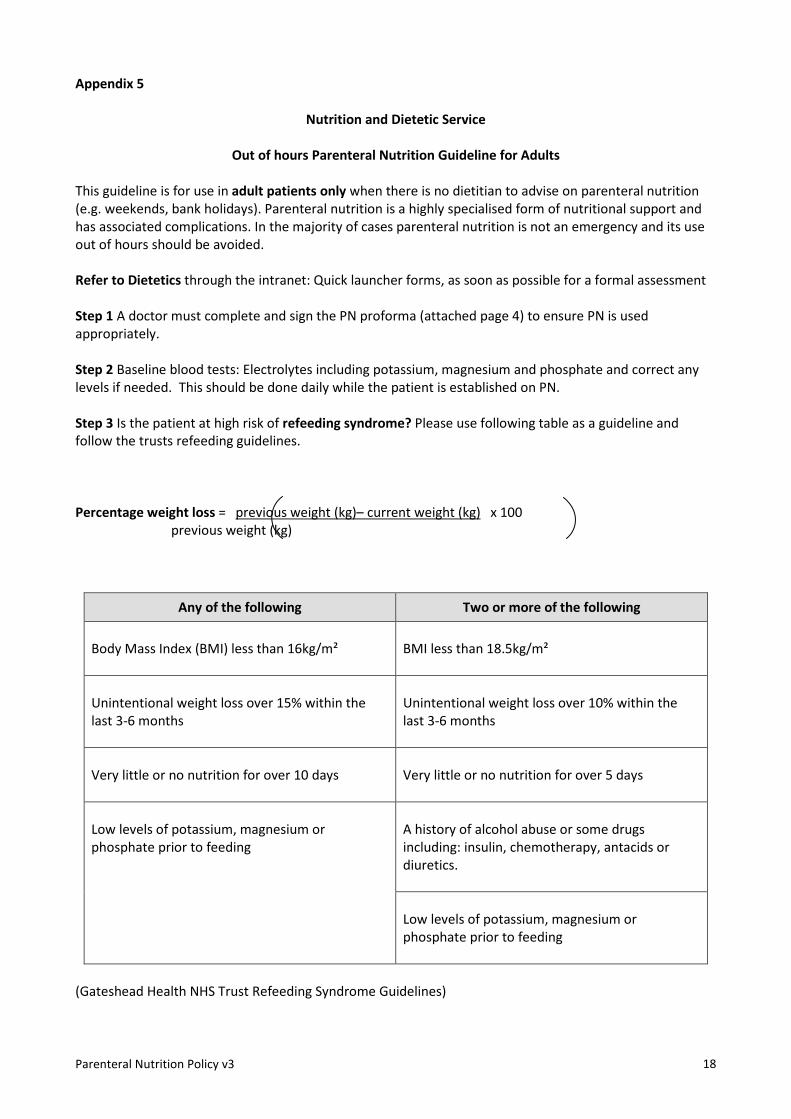
Appendix 5
Nutrition and Dietetic Service
Out of hours Parenteral Nutrition Guideline for Adults
This guideline is for use in adult patients only when there is no dietitian to advise on parenteral nutrition
(e.g. weekends, bank holidays). Parenteral nutrition is a highly specialised form of nutritional support and
has associated complications. In the majority of cases parenteral nutrition is not an emergency and its use
out of hours should be avoided.
Refer to Dietetics through the intranet: Quick launcher forms, as soon as possible for a formal assessment
Step 1 A doctor must complete and sign the PN proforma (attached page 4) to ensure PN is used
appropriately.
Step 2 Baseline blood tests: Electrolytes including potassium, magnesium and phosphate and correct any
levels if needed. This should be done daily while the patient is established on PN.
Step 3 Is the patient at high risk of refeeding syndrome? Please use following table as a guideline and
follow the trusts refeeding guidelines.
Percentage weight loss = previous weight (kg)– current weight (kg) x 100
previous weight (kg)
Any of the following Two or more of the following
Body Mass Index (BMI) less than 16kg/m²
BMI less than 18.5kg/m²
Unintentional weight loss over 15% within the
last 3-6 months
Unintentional weight loss over 10% within the
last 3-6 months
Very little or no nutrition for over 10 days
Very little or no nutrition for over 5 days
Low levels of potassium, magnesium or
phosphate prior to feeding
A history of alcohol abuse or some drugs
including: insulin, chemotherapy, antacids or
diuretics.
Low levels of potassium, magnesium or
phosphate prior to feeding
(Gateshead Health NHS Trust Refeeding Syndrome Guidelines)

Parenteral Nutrition Policy v3 19
Step 4 Contact pharmacy to request the PN. The only PN bag available out of hours is the Triomel
Peripheral N4 1500ml (referred to as Triomel 6gN) which is kept in the pharmacy emergency drug
cupboard.
Step 5 Mixing guidelines
• Remove the overpouch by tearing from the notch close to the ports along the upper edge, then
tear the long sides, pull off the overpouch and discard it along with the oxygen absorber.
• Place the bag on a flat surface. Tightly roll up the bag from the handle side until the vertical
seals are broken. Ensure that the liquids mix easily although the horizontal seal remains closed.
• Mix the contents of the three chambers by inverting the bag a minimum of three times until
all the components are thoroughly mixed.
Step 6 Follow the flow chart (page 5) to establish the correct rate of administration for the PN.
Do not increase the rate of PN until potassium, phosphate and magnesium levels are within normal range.
PN should only be administered over a maximum 24 hour period and bags should be changed every 24
hours, any remaining solution in the bag must be discarded.
Note if you are unsure whether the patient is at risk of refeeding syndrome, exercise caution by following
the steps for refeeding syndrome.

Parenteral Nutrition Policy v3 20
Out of hours Parenteral Nutrition Regimen
Access Route Peripheral* Central
At risk of refeeding syndrome? (use table as guideline)
At risk of refeeding syndrome? (use table as guideline)
Yes No Yes No
Day 1:
Commence Triomel 6gN 42 ml/hr x 18 hrs
Day 1:
Commence Triomel 6gN 83 ml/hr x 18 hrs
Day 1:
Commence Triomel 6gN 31 ml/hr x 24 hrs
Day 1:
Commence Triomel 6gN 62 ml/hr x 24 hrs
Day 2:
Triomel 6gN 83 ml/hr x 18 hrs
Day 2: Triomel 6gN 62 ml/hr x 24 hrs
Key points
For peripheral access: rotate site of entry every 24 hours Do not increase rate until potassium, phosphate and magnesium are within normal range. Final regimen (i.e. day 2) provides 1050 kcal, 6g nitrogen, 1500ml, 31.5mmol Na, 24mmol K, 3.3mmol Mg, 3mmol Ca, 12.7mmol Phosphate

Parenteral Nutrition Policy v3
Step 3 Monitoring
Parameter Frequency Rationale
Urea and electrolytes,
magnesium, phosphate and
calcium
Daily until stable
Assessment of renal
function, depletion is
common
Glucose
Baseline
1 or 2 times a day (or
more if needed) until
stable
Good glycaemic control is
necessary
Fluid balance
Daily
Ensure PN taken into
account when prescribing
additional fluids
References
1 National confidential enquiry into patient outcome and death: A mixed bag: an enquiry into the
care of hospital patients receiving parenteral nutrition. June 2010.
2 Nutrition Support in adults NICE clinical guideline No 32 (2006).
3 Parenteral Nutrition Policy, Gateshead Health NHS Foundation Trust

Parenteral Nutrition Policy v3 22
Appendix 6
Montitoring patients on parenteral Nutrition
Parameter Frequency Rationale Responsibility
Nutritional
Nutrient intake from oral,
enteral or PN (including
any change in conditions
that are affecting food
intake).
Actual volume of PN
delivered.
Fluid balance charts
Daily, reducing to twice
weekly when stable.
Daily initially, reducing to
twice weekly when
stable.
Daily initially, reducing to
twice weekly when
stable.
To ensure that
patient is receiving
nutrients to meet
requirements and
that current method of
feeding is still the most
appropriate.
To allow alteration of
intake as indicated.
To ensure patient is not
becoming over/ under
hydrated. To ensure
appropriate prescription
of additional fluids if
required. Always take
into account the volume
of PN when assessing a
patient’s fluid
requirements to avoid
fluid overload.
Dietitian and nursing
staff.
Dietitian, nursing
and medical staff.
Medical and nursing
staff.
Anthropometric
Weight.
Mid arm
circumference/mid arm
muscle circumference.
Daily if concerns
regarding fluid balance,
otherwise weekly
reducing to monthly. If
clinical condition
changes.
Weekly if patient cannot
be weighed, reduce to
monthly once stable.
To assess ongoing
nutritional status,
determine whether
nutritional goals are
being achieved and take
into account both body
fat and muscle.
Nursing staff and
dietitian.
Dietitian
Gastrointestinal symptoms
Nausea/vomiting.
Diarrhoea.
Constipation.
Daily initially, reducing to
twice weekly.
Daily initially, reducing to
twice weekly.
Daily initially, reducing to
twice weekly.
To identify and rule out
any cause of vomiting, eg
obstruction.
To identify and rule out
any causes of diarrhoea.
To rule out other causes
of constipation.
Nursing and medical
staff, dietitian.
Nursing and medical
staff, dietitian.
Nursing and medical
staff, dietitian.

Parenteral Nutrition Policy v3 23
Abdominal distension.
As necessary
To identify cause.
Nursing and medical
staff.
Devices and equipment
Catheter entry site.
Dressings.
Daily.
Daily.
To identify signs of
infection.
To ensure they are secure
and hygienic
Nursing staff.
Nursing staff.
Clinical Condition
General condition
Temperature.
Blood pressure.
Drug therapy.
Daily.
Daily initially then as
needed.
Daily initially then as
needed.
Daily initially and then
monthly when stable.
To ensure the PN is
tolerated.
To identify any signs of
infection.
Monitor clinical condition
and fluid balance.
To prevent/reduce drug
nutrient interaction.
All team.
Nursing and medical
staff.
Nursing and medical
staff.
Nursing and medical
team

Parenteral Nutrition Policy v3 24
Appendix 7
Biochemical monitoring of patients on PN
Parameter Frequency Rationale Interpretation
Sodium, potassium,
urea, creatinine.
Baseline.
Daily until stable.
Then 1-2 times a week.
Assessment of renal
function, fluid status
and Na and K status.
Interpret with knowledge
of fluid balance and
medication.
Glucose. Baseline.
1 or 2 times a day (or more
if needed) until stable.
Then weekly.
Good glycaemic control
is necessary.
Glucose intolerance is
common – administer
insulin if necessary.
Magnesium,
phosphate.
Baseline.
Daily if risk of refeeding
syndrome.
Three times a week until
stable. Then weekly.
Depletion is common
and under recognised.
Low concentrations
indicate poor status.
Replacement vital to
avoid refeeding
syndrome.
Liver function tests
including
International
Normalised Ratio
(INR)/PT
Baseline. Twice weekly
until stable. Then weekly.
Abnormalities common
during PN.
Complex. May be due to
sepsis, other disease or
nutritional intake. May
need to consider reducing
fat content of PN.
Calcium, albumin. Baseline.
Then weekly.
Hypocalcaemia or
hypercalcaemia may
occur.
Correct measured
serum calcium
concentration for
albumin.
Hypocalcaemia may be
secondary to Mg
deficiency.
Low albumin reflects
disease not protein
status.
C-reactive protein Baseline.
Then 2 or 3 times a week
until stable.
Assists interpretation of
protein, trace elements
and vitamin results
To assess the presence
of an acute phase
reaction (APR). The
trends of the results are
important.
Zinc, copper Baseline. Deficiency common,
especially when
increased losses.
People most at risk
when anabolic APR
causes Zn and Cu
deficiency
Selenium Baseline for risk of
depletion. Further testing
dependent on baseline
Se deficiency likely if
severe illness and
sepsis, or long-term
Nutrition support.
APR causes Se depletion.
Long term status better
assessed by glutathione
peroxidise.
Full blood count and
MCV
Baseline. 1 or 2 times a
week until stable. Then
weekly
Anaemia due to iron
and folate deficiency is
common.
Effects of sepsis may be
important.
Iron, ferritin. Baseline. Then every 3-6
months.
Iron deficiency common
to long-term PN.
Iron status difficult to
assess if there is an acute
phase reaction.
Folate, B12. Baseline. Iron deficiency is
common
Serum folate/B12
sufficient, with full blood
count.























![Parenteral Nutrition[1]](https://img.pdfslide.us/doc/110x75/5469fe10af79593b558b4f0d/parenteral-nutrition1.jpg)


