-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
1/20
Child Development, January/February 2008, Volume 79, Number 1,
Pages 45 64
Parental Socialization, Vagal Regulation, and Preschoolers
Anxious
Difficulties: Direct Mothers and Moderated Fathers
Paul D. Hastings, Caroline Sullivan, and
Kelly E. McShaneConcordia University
Robert J. Coplan
Carleton University
William T. UtendaleConcordia University
Johanna D. VynckeUniversitedu Quebec a Montreal
Parental supportiveness and protectiveovercontrol and
preschoolers parasympathetic regulation wereexaminedas predictors
of temperamental inhibition, social wariness, and internalizing
problems. Lower baseline vagal toneand weaker vagal suppression
were expected to mark poorer dispositional self-regulatory
capacity, leavingchildren more susceptible to the influence of
parental socialization. Less supportive mothers had
preschoolerswith more internalizing problems. One interaction
between baseline vagal tone and maternal protectiveovercontrol,
predicting social wariness, conformed to the moderation hypothesis.
Conversely, vagal
suppression moderated several links between paternal
socialization and childrens anxious difficulties in theexpected
pattern. There were more links between mothers self-reported
parenting and child outcomes than werenoted for direct observations
of maternal behavior, whereas the opposite tended to be true for
fathers.
Internalizing problems are one of the most commonkinds of early
childhood difficulties (Zahn-Waxler,Klimes-Dougan, & Slattery,
2000), which frequentlypersist through childhood and into
adolescence andadulthood (Majcher & Pollack, 1996).
Internalizingproblems often become evident or exacerbated in
thetransition from home care to day care or preschool, aschildren
show fear of the novel setting, distress fromparental separations,
and withdrawal from peers(Hirshfeld-Becker & Biederman, 2002).
Young child-rens anxious reactions to early school settings can
setthem on adverse trajectories toward further personal,social, and
academic difficulties (Coplan, Barber, &Lagace-Seguin, 1999).
We examined the joint contri-butions of childrens parasympathetic
regulation andexperiences of parental socialization to their
earlyemerging internalizing problems, social wariness,and
temperamental inhibition. To address gaps andinconsistencies in the
literature, we compared base-
line vagal tone and dynamic vagal suppression,mothers and
fathers use of both adaptive and mal-adaptive parenting, and both
parent-reported andobserved measures of socialization
techniques.
Socialization and Anxious Development
Parental overcontrol is a robust correlate of, andcontributor
to, childrens anxiety, dependence, andsocial withdrawal (Rapee,
1997; Wood, McLeod,Sigman, Hwang, & Chu, 2003). The nature of
controlappears to be key, as parents can assert their
dominancethrough both behavioral and psychological controls(Barber,
2002; Barber & Harmon, 2002). Behavioralcontrol encompasses
rules- and consequences-basedmanagement efforts. Psychological
control involvesparents attempts to manipulate childrens
emotions,intrude on childrens autonomous activity, or restrictthe
kinds of experiences children have. This limits
childrens autonomy and fosters their dependenceupon parents,
putting children at risk for internalizingproblems and anxious
difficulties (Hudson & Rapee,2001; Mills & Rubin, 1998;
Park, Belsky, Putnam, &Crnic, 1997; Pettit, Laird, Dodge,
Bates, & Criss, 2001;Rubin, Burgess, & Hastings, 2002).
Ourthanks to the participating families andteachers; Lisa
Serbinand Rosemary Mills for comments on earlier drafts; and
FarriolaLadha, Ishani De, Samantha Goldwater-Adler, Maryse
Guenette,and the students and staff of the ABCD Lab. This research
wassupportedby the Social Sciences and Humanities Research
Councilof Canada, the Fonds de la Recherche en Sante du Quebec,
theCanada Foundation for Innovation, and Concordia University.
Correspondence concerning this article should be addressed
toPaul D. Hastings, Centre for Research in Human
Development,Department of Psychology, Concordia University, 7141
SherbrookeStreet West, Montreal, Quebec, Canada H4B 1R6. Electronic
mailmay be sent to [email protected].
# 2008 by the Society for Research in Child Development, Inc.All
rights reserved. 0009-3920/2008/7901-0004
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
2/20
Protective overcontrol is one aspect of psycholog-ical control
that has often been linked with youngchildrens anxious difficulties
(Rapee, 1997; Rubin,Hastings, Stewart, Henderson, & Chen 1997).
Thisreflects intrusive actions that emphasize the closenessof the
parent child bond, such as restricting thechilds independent
activities, very strong affection,and unnecessary micromanagement
(Barber, 2002).According to a transactional bidirectional model
ofpsychological control and anxious difficulties (e.g.,Rapee, 1997;
Rubin, Stewart, & Coplan, 1995), phys-iologically overreactive
or temperamentally inhibitedchildren display high levels of
distress and neediness.This evokes parents emotions, including
concern,anxiety, or guilt, which motivate parents to endchildrens
distress and prevent its recurrence. Thus,they use protective
overcontrol to effusively comforttheir children, limit exposure to
unfamiliar or poten-
tially challenging events, or dominate situations oractivities
that they perceive to be beyond their child-rens capacities. In
turn, this restricts childrensopportunities to practice and improve
their self-regulation and active coping skills and communicatesthe
message that they are incapable and requireparental assistance to
handle normal life tasks. Child-rens development of autonomy and
competence isthereby undermined, setting them upon a
trajectorytoward exacerbating internalizing problems.
A small set of longitudinal investigations supportthese
hypothesized parent effects. Rubin et al. (2002)
found that reticence with peers was significantlystable from 2
to 4 years only for those children withmothers who had been
oversolicitous (intrusive buthighly warm). Bayer, Sanson, and
Hemphill (2006)found that higher maternal protectiveness of
toddlerspredicted greater internalizing difficulties in
pre-schoolers. Park et al. (1997) found thatstrong
affectioncontributed to the stability of boys inhibition from2 to 3
years. Thus, there is increasing evidence
forparentalpsychologicalcontrolcontributingtothemain-tenance or
exacerbation of childrens inhibition, wari-ness, and internalizing
problems over development.
Conversely, appropriate, positive, and effective
parenting predicts fewer anxious difficulties. Parentswho are
more authoritative, supportive, or encourag-ing of autonomy have
children who show fewerinternalizing problems or less inhibition or
socialdifficulty (Baumrind & Black, 1967; Chen et al.,1998;
Shipman, Schneider, & Sims, 2005). Maternalsensitivity and
engagement have been found todecrease the stability of early
inhibition and anxiety(Bayer et al., 2006; Crockenberg &
Leerkes, 2006; Earlyet al., 2002). However, few studies of
preschoolershave included both psychological control and posi-
tive parenting or controlled for one in order todetermine
whether the other is uniquely associatedwith childrens
adjustment.
The Biological Basis of Internalizing Problems
Temperamental inhibition in infancy and toddler-hood has also
been linked with later internalizingproblems (Kagan & Snidman,
1999; Prior, Smart,Sanson, & Oberklaid, 2000). Highly inhibited
toddlershave low thresholds for arousal and difficulty adjust-ing
to novelty, and they typically react to unfamiliarsituations with
distress and withdrawal (Kagan,1997). Withdrawing may reduce the
childrens dis-tressed arousal, but this also reinforces a pattern
ofavoidant coping that supplants more effective socialskills. Thus,
there may be a developmental sequencelinking inhibition, a
dispositional tendency to react to
unfamiliarity with fear, first to wariness, the avoid-ance of
peers by withdrawing from social interac-tions, and then to
internalizing problems, those moreserious and maladaptive emotional
and behavioralpatterns that interfere with childrens abilities
toaccomplish developmentally normal activities (Rubinet al.,
2002).
One frequently studied psychophysiological cor-relate of
inhibition, wariness, and internalizing prob-lems in children is
cardiac vagal tone, an index ofparasympathetic regulation of heart
rate variabilityattributable to the influence of the 10th cranial
nerve
(Porges, 1991). The parasympathetic system generallyserves to
downregulate or decrease cardiac activity.Individual differences in
vagal tone are associatedwith the ability to adaptively calm
oneself aftera salient event has produced increased arousal(Porges
& Doussard-Roosevelt, 1997). Over the pre-school period, there
are both maturational changes ofthe cardiac system and moderate
stability in cardiacfunction. Baseline vagal tone increases with
age,though individual differences remain similar (Fox &Field,
1989; Porges, Doussard-Roosevelt, Portales, &Suess, 1994).
Baseline vagal tone (most often mea-sured as respiratory sinus
arrhythmia [RSA]) is useful
for assessing individual differences in character-istic states
of regulation or typical levels of arousal(Beauchaine, 2001;
Calkins, 1997) and is associatedwith emotional reactivity (Stifter
& Fox, 1990). Ac-cording to the polyvagal theory (Porges,
1995),dynamic changes in vagal enervation (suppression)in response
to task demands also should be associatedwith adaptive, active
coping. Childrens withdrawalof parasympathetic influence over
arousal in responseto such mild to moderate challenges as solving a
diffi-cult puzzle reflects an adaptive allocation of energy
46 Hastings et al.
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
3/20
and external focus of attention that should promoteeffective
coping (Calkins & Keane, 2004). Thus, vagalsuppression should
upregulate or increase cardiacactivity.
Lower baseline vagal tone has been related tochildrens anxious
difficulties (El-Sheikh, Harger, &Whitson,2001; Fox& Field,
1989; Garcia Coll, Kagan,&Reznick, 1984). Weaker vagal
suppression also hasbeen linked to childrens problems (Calkins,
1997;Calkins & Dedmon, 2000; El-Sheikh, 2001), and
vagalsuppression may be more strongly linked to emo-tional and
behavioral adjustment than is baselinevagal tone (Blair, 2003;
Calkins & Keane, 2004). Thesestudies suggest that limited
parasympathetic regula-tion of arousal undermines childrens
abilities to copewith stress, contributing to a range of
internalizingproblems.
However, many studies have failed to find rela-
tions between vagal tone and inhibition or internal-izing
problems (Calkins & Fox, 1992; Gerlach,Wilhelm, & Roth,
2003; Marshall & Stevenson-Hinde,1998; Schmidt, Fox, Schulkin,
& Gold, 1999; Steven-son-Hinde & Marshall, 1999). This may
suggest thatthe links between vagal tone and anxious adjustmentare
not robust. Alternatively, decreased parasympa-thetic regulation
may act as a vulnerability that putschildren at risk for
manifesting difficulties dependingon other characteristics or
experiences. Thus, psycho-logical control may be particularly
disadvantageousfor children with low vagal tone.
The Joint Contributions of Physiology and Socialization
toAnxious Adjustment
The contention that having lower vagal tone mayincrease a childs
susceptibility to maladaptive social-ization conforms to the tenets
of the diathesis stressand transactional models that have become
predom-inant in developmental psychopathology (Sameroff,1975;
Steinberg & Avenevoli, 2000). A small set ofstudies on vagal
regulation and childrens socializa-tion experiences within the
family have begun toprovide support for a model of the interactive
con-
tributions of physiological and experiential factors
tointernalizing problems.
Scheeringa, Zeanah, Myers, and Putnam (2004)reported that
preschoolers with elevated posttrau-matic stress symptoms and low
positive maternaldiscipline showed poor vagal regulation during
recallof stressful experiences. El-Sheikh (2001; El-Sheikh
&Harger, 2001; El-Sheikh & Whitson, 2006) reportedthat both
lower baseline vagal tone and poorer vagalregulation to an
emotional stressor moderated asso-ciations between parental
difficulties and internaliz-
ing problems; parental alcoholism or marital conflictonly
predicted problems for less well-regulated chil-dren. Katz (Katz
& Gottman, 1995, 1997) reported thatmarital problems predicted
a range of problems forchildren with lower RSA and that vagal
suppression(but not baseline vagal tone) moderated linksbetween
hostile coparenting (but not cohesive par-enting) and social
difficulties with peers (Leary &Katz, 2004).
This work supports a biopsychosocial model of thedevelopment of
anxious difficulties, in which poorparasympathetic regulation of
arousal and adversesocialization experiences are jointly associated
withgreater maladjustment. However, several issues havenot been
adequately addressed in the existing litera-ture. First, it is
unclear whether low baseline vagaltone or weak vagal suppression
most accuratelyreflects childrens physiological risk. Second,
the
relative contributions of protective overcontrol andsupportive
parenting to anxious adjustment need tobe considered. Third, many
previous studies havefocused on parental psychopathology or family
prob-lems, rather than parental socialization styles orpractices,
such that results may not speak directly tothe proposed roles of
protective overcontrol andsupportiveness. Fourth, most studies have
includeda single technique to assess parenting of
preschoolers,either self-report or direct observation. Each has
itsown strengths but carries well-identified limits tovalidity when
used alone (Janssens, De Bruyn,
Manders, & Scholte, 2005; Miller, 1998). Using multi-ple
methods to assess parenting could reveal con-vergent validity of
predictive relations with childoutcomes. Fifth, studies have tended
to assess eitherchildrens internalizing problems, or social
wariness,or inhibition, and the biopsychosocial model mayvary for
these. As well, the ecological validity of somemeasures of
adjustment may be questioned, as child-rens social wariness has
typically been measured inlaboratory observations of wary and
reticent behaviorwith unfamiliar peers. Although related to parent
andteacher reports of child behavior problems (e.g.,Coplan, 2000;
Coplan, Rubin, Fox, Calkins, & Stewart,
1994), reticence with unfamiliar peers may not gen-eralize to
childrens play with familiar peers in knownsettings, such as day
care.
Sixth, and perhaps most important, little is knownabout
relations between fathers socialization andchildrens anxious
difficulties. Studies of adolescentssocialization have shown that
fathers value promotingautonomy more than mothers (Kenny &
Gallagher,2002) and mothers use more psychological controlthan
fathers (Barber, Bean, & Erickson, 2002), al-though this has
not been seen with younger children
Vagal Tone, Parenting, and Adjustment 47
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
4/20
(Nelson & Crick, 2002; Rubin, Nelson, Hastings,
&Asendorpf, 1999). The limited research suggests thatthe links
between fathers psychological control andchildrens characteristics
are similar to those seenwith mothers (Park et al., 1997; Rogers,
Buchanan, &Winchel, 2003). There is reason to propose,
then,that fathers use of psychological control is alsomaladaptive
for childrens development of anxiousdifficulties.
Goals of the Current Investigation
We tested a biopsychosocial model of childrensanxious
difficulties. Vagal tone was used to measureparasympathetic
regulation and was expected tomoderate the associations between
mothers andfathers parenting and childrens adjustment. Pro-tective
overcontrol was assessed as an aspect of
psychological control that could be particularly mal-adaptive
for vulnerable children, and supportiveparenting was examined as a
factor promoting morepositive functioning. We looked at both
normativeaspects of childrens anxious difficulties, includingsocial
wariness and temperamental inhibition, andmore clinically relevant
internalizing problems. Thestudy was designed to address the six
identifiedlimitations of the past literature.
Four main hypotheses were tested. (a) Childrenwere expected to
manifest more inhibition, socialwariness, and internalizing
problems when their
parents reported using more protective overcontroland less
supportive parenting and (b) when theyshowed lower baseline vagal
tone and less vagalsuppression to mild challenge.
Parasympatheticregulation was expected to moderate parental
social-ization, such that (c) mothers and fathers high pro-tective
overcontrol and low supportive parentingwere expected to predict
anxious difficulties morestrongly for children with lower vagal
tone and lessvagal suppression. (d) Weak vagal suppression
wasexpected to be a better index of childrens physiolog-ical
vulnerability, moderating the relations of parentalsocialization
and child adjustment more consistently
than baseline vagal tone.
Method
Participants
Recruitment strategy. Participants were recruitedthrough
advertisements placed in newspapers, post-ers in community centers
and libraries, and lettersdistributed to day cares and preschools.
In order tofind children ranging in likelihood of manifesting
adjustment difficulty, some advertisements and post-ers were
targeted toward parents of children withspecific characteristics,
for example, Is your childquiet and cautious? or Is your child
upbeat andeasy-going?
Sample. The final sample included 133 families,with 72 girls and
61 boys, from 2.08 to 4.92 years old atrecruitment (M 5 3.50, SD 5
0.76). A total of 87children were enrolled in day care and 44 were
inpreschool (2 children were withdrawn from day careor preschool
after the family enrolled in the study). Toassess the effectiveness
of the recruitment strategy,mothers were administered the items
composing theinternalizing problems scale of the Child
BehaviorChecklist (CBCL) for 1.5 5 years (Achenbach &Rescorla,
2000) during the telephone screening (seemeasures below). Forty-two
children were in theborderline clinical to clinical range for
internalizing
problems (T! 60;M5 65.93, SD5 4.96, range5 60 76), 48 were less
than 1 SD above their gender- andage-normed average (51 T 59; M 5
54.77, SD 52.17), and 43 were at or below that average (T 50;M 5
42.95, SD5 5.56, range5 2949).
There were 113 two-parent families, including 3separated couples
who shared custody of the childand both parents participated, and
20 single-motherfamilies. All mothers and 105 fathers
participated.Mothers age ranged from 19.75 to 50.50 years (M
535.32, SD5 5.10), and fathers age ranged from 23.58to 56.92 years
(M 5 37.66, SD 5 5.65). There were 98
Caucasian families, 21 families with mixed ethnic-ities, 7 Asian
families, and 7 families with otherethnicities (Hispanic, Black,
Middle Eastern, or other).The families were predominantly middle
class.Twenty percent of mothers and 22% of fathers hada graduate
degree, 42% of mothers and 30% of fathershad an undergraduate
degree, 26% of mothers and34% of fathers had some university
education, 11% ofmothers and fathershad completed high school,and
1mother and 3 fathers had not finished high school.Annual household
income before taxes ranged fromunder $20,000 to over $200,000
Canadian (M 5$80,229.17, mode 5 $50,000, SD5 $47,777.21).
Teacher reports were completed by 1 male and 107female teachers
who worked in 97 establishments,with 1 to 4 participating children
enrolled in each daycare and preschool.
Procedure
Data for this study were collected during a visit toeach familys
home, a visit to each childs day care orpreschool, and a visit to
the laboratory by each family.Parents completed measures at home
and in the
48 Hastings et al.
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
5/20
laboratory. Teachers completed questionnaires thatwere returned
by mail. An overview of the timelinefor the components of the study
is provided inTable 1.
Temperamental inhibition. To assess childrens inhi-bition,
mothers completed the Childrens BehaviorQuestionnaire (CBQ;
Rothbart, Ahadi, Hershey, &Fisher, 2001) and teachers completed
the Social Com-petence and Behavior Evaluation Preschool
Edition(SCBE; La Freniere & Dumas, 1995). The Fearful andShy
scales of the CBQ include 13 items each. For thissample of
mothers,a5 .76 and .94 for the Fearful andShy scales, respectively.
These scales were aggre-gated, r 5 .46, p , .001, to form an index
of mother-reported inhibition (n5112,M5 3.54, SD50.98). TheAnxious
and Isolated scales of the SCBE include 10items each. For this
sample of teachers, as 5 .78and .82, respectively. These scales
were aggregated,
r5 .65,p, .001, to form the index of teacher-reportedinhibition
(n 5 115, M5 49.93, SD 5 8.69).
Internalizing problems. To assess internalizingproblems, mothers
completed the full CBCL 1.5 5years and teachers completed the
Caregiver TeacherReport Form (Achenbach & Rescorla, 2000).
TheInternalizing Problems scale includes 36 items forparents and 32
items for teachers and has demon-strated good internal reliability
and 1-week testretest reliability (Achenbach & Rescorla, 2000).
Inthe current sample, the reliability coefficients a 5.87 for
mothers (n 5 116, M5 50.17, SD5 10.98) anda 5 .87 for teachers (n 5
114, M5 51.39, SD 5 9.87).
Reported parenting. To assess patterns of socializa-tion,
parents completed the Child-Rearing PracticesReport (CRPR; Block,
1981). The CRPR uses a 91-itemQ-Sort methodology to measure
parenting attitudes,beliefs, and behaviors. The measure is well
validated,
with an 8-month test retest average correlation ofr 5 .71
(Block, 1981) and has been used in previousstudies of parental
psychological control (Chen et al.,1998; Hastings & Rubin,
1999; Kennedy, Rubin,Hastings, & Maisel, 2004) and
authoritative parenting(Hastings, Zahn-Waxler, Robinson, Usher,
& Bridges,2000; Kochanska, Kuczynski, & Radke-Yarrow,
1989).A total of 133 mothers and 105 fathers completed theCRPR
during the home visit.
Subscale scores were computed representing pro-tective
overcontrol (8 items: 13, 20, 44-R, 54, 68, 75-R,79, and 80, e.g.,
I stop my child from playing rough
games or doing things where he/she might get hurt)and supportive
parenting (10 items: 1, 11, 18, 22, 34,38, 40, 42, 51, and 52,
e.g., I respect my childsopinions and encourage him/her to express
them).For the latter, the original authoritative scale definedby
Kochanska et al. (1989) was modified by removingfour items with
poor item whole correlations tomaximize internal consistency.
Coefficient alphas forprotective overcontrol and supportive
parenting formothers were, respectively, as 5 .49 and .60,
anddescriptive statistics were, respectively, Ms 5 3.34and 6.07,
SDs 5 0.70 and 0.48. Coefficient alphas forfathers were,
respectively, as 5 .43 and .62, and
descriptive statistics were, respectively, Ms 5 3.29and 5.96,
SDs 5 0.69 and 0.54. Due to the forced-choice ranking procedure of
the Q-Sort methodology,CRPR scales often have low internal
consistencyscores (Hastings & Rubin, 1999) despite evidence
fortheir convergent and predictive validity.
Observed parenting. Each parent (in counterbal-anced order for
two-parent families) and child werevideotaped at home completing a
series of activities.Parental behaviors were observed in the final
threeactivities. In co-constructed narratives, the parent and
Table 1
Overview and Timeline of Data Collection Procedures
Months Procedure Measures
April to August Recruitment Phone screening:
Initial internalizing
problems
June to August Home visit Reported parenting: CRPR
Observed parenting:
Parent child interactionsco-constructed narratives
origami teaching
cleanup
Baseline vagal tone:
Video or story
Task vagal tone:
Challenging puzzle
October to
December
Preschool visit Social wariness: Familiar
peer interactions
January to April Teacher
questionnaire
Temperamental inhibition:
SCBE
Internalizing problems:
CTRF
February to April Laboratory visit Social wariness:
Unfamiliarpeer interactions
Temperamental inhibition:
CBQ (mother)
Internalizing problems:
CBCL (mother)
Note. CRPR5Child-Rearing Practices Report (Block, 1981);
SCBE5Social Competence andBehaviorEvaluation (La Freniere &
Dumas,1995); CTRF 5 Caregiver Teacher Report Form (Achenbach
&Rescorla,2000); CBQ5Childrens Behavior
Questionnaire(Rothbart,Ahadi, Hershey, & Fisher, 2001); CBCL 5
Child Behavior Checklist(Achenbach & Rescorla, 2000).
Vagal Tone, Parenting, and Adjustment 49
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
6/20
childused a setof figures and toyprops to resolve twosocial
situations involving peers. In origami teaching,the parent guided
the child in how to fold paper intoan origami shape. In cleanup,
the parent and childtidied the interaction area. In two-parent
homes,activities were adapted slightly (e.g., different
socialsituations for the co-constructed narratives; differentshapes
for the origami teaching) so that children didnot repeat identical
tasks with each parent. In single-mother homes, either the first or
the second set ofactivities was randomly assigned to the
family.Mechanical error, experimenter error, and/or failureto
attain child cooperation with the tasks resulted inthe loss of all
videotaped data for two mother childdyads (n 5 131) and three
father child dyads(n 5 102).
The co-constructed narratives were based on pastresearch in
which the MacArthur Story Stem Battery
was administered to parents and children together(Oppenheim,
Emde, & Wamboldt, 1996; Oppenheim,Nir, & Warren, 1997) but
adapted to tap parentalreactions to preschoolers coping with
challengingpeer interactions. The experimenter set up two
sce-narios for each parent child dyad, the first depictingthe dyad
arriving at a situation (preschool, birthdayparty) in which three
other children were alreadyplaying and the second depicting the
dyad meetingone unfamiliar peer and adult (playdate, park) andthe
target child acting shyly. After establishing thesituation, the
experimenter said You finish the story.
Parent behaviors were observed from this point untilthe target
childs first interaction with the otherchild(ren) or for a maximum
of 5 min (mothers: M 51 min 51.33 s, SD5 1 min 33.89 s; fathers: M
5 2 min15.84 s, SD5 1 min 44.64 s; paired t52.30, p, .05).Two
children with mothers and 2 children withfathers immediately (,10
s) moved their figurine intoboth social interactions without any
behaviors byparents; these dyads were notincludedin
theanalyses.
Coders used event sampling to record the fre-quency of 13 parent
behaviors. Inter-rater agreementwas computed for 20% of tapes that
were examinedby two coders using coefficient kappa, mean j 5
.86
(range 5 .61 1.00). Scores were proportionalized fortotal time
observed. Six codes were seen as Protectiveor discouraging peer
interaction (act as childs play-mate, enact joining peer play with
child, enact otheradult interacting with child, support child
interactingwith other adult, support nonsocial play by child,
anddescribe child as shy or reluctant). Five were seen
asEncouraging of Engagement (familiarize child withsetting,
encourage child to interact, suggest how toinitiate interaction,
enact peer interacting with child,and ask child why s/he isnt
interacting with peers).
Two were seen as Supportive (model greeting orinteracting with
others and provide reasons for childinteracting). Descriptive
statistics for these three setsof codes for mothers were,
respectively, Ms 5 0.09,0.30, and 0.19, SDs 5 0.12, 0.23, and 0.21,
and forfathers were, respectively, Ms 5 0.08, 0.36, and 0.14,SDs5
0.08, 0.22, and 0.18.
For the origami task, parents were asked to followpictorial
instructions to teach their child how to folda piece ofpaper intoa
shape but not totouchthe paperthemselves. Parent behaviors were
coded until theshape was completed, the parent gave up the task,
or5 min passed (mothers:M5 3 min 48.20 s, SD5 1min23.88 s;
fathers:M5 3 min 50.70s, SD5 1 min 30.32 s;paired t 5 0.65). Coders
completed time-sampledratings of parents actions; for each 20-s
time sample,coders rated each parent behavior from 1 (absent) to
5(strong and repeated). Inter-rater agreement was com-
puted for 25% of the tapes examined by two codersusing
coefficient alpha, mean a 5 .77 (range5 0.67 0.93). Scores were
proportionalized for total timeobserved. Codes used in the current
analysesincluded Positive (warmth, affection, praising,
andencouraging) and Supportive (point out steps, showillustrations,
explain actions necessary, and providereasons). Descriptive
statistics for these for motherswere, respectively,Ms5 1.46 and
1.94, SDs5 0.31 and0.45, and for fathers were, respectively,Ms5
1.39 and2.00, SDs 5 0.28 and 0.49.
For the cleanup task, parents were asked to get
their child to return all play materials to their originalboxes.
Parent behaviors were coded until the playmaterials were returned
to their containers, the parentstated that they were finished (even
if they were not),or 6 min passed (mothers: M 5 4 min 37.52 s, SD
51 min 06.05 s; fathers: M5 4 min 37.81 s, SD 5 1 min01.03 s;
paired t 5 0.49). Using time sample coding,coders evaluated each
parent behavior as Absent orPresent in each 10-s time sample of the
cleanup task.Inter-rater agreement was computed for 20% of
tapes,mean j 5 .71 (range 5 .67 1.00). Scores were
pro-portionalized for total time observed. Codes includedAssist
(help child put object into box), Take Over (put
object away without childs assistance; accept
childsnoncompliance with task), Positive (praise, affection),and
Encourage (gentle control through requests andreasoning).
Descriptive statistics for these four sets ofcodes for mothers
were, respectively, Ms5 0.20, 0.08,0.12, and 0.14, SDs5 0.12, 0.09,
0.10, and 0.08, and forfathers were, respectively, Ms 5 0.23, 0.08,
0.12, and0.16, SDs 5 0.13, 0.08, 0.11, and 0.08.
Vagal tone. Each childs baseline cardiac activitywas recorded
using the Mini-Logger 2000 (Mini-Mitter, Inc., Bend, OR), a
light-weight ambulatory
50 Hastings et al.
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
7/20
monitor. Continuous interbeat interval (IBI) record-ing was
obtained through a recording band that wasconnected to the childs
chest using either two adhe-sive electrodes or an adhesive-free
elasticized beltaround the torso. IBIs were recorded between
succes-sive R-waves to the nearest millisecond. The recordingband
transmitted the data to the Mini-Logger 2000unit, which the child
wore in a fanny-pouch around hisor her waist and which could store
up to 2 hr ofcontinuously recorded IBI data. Data were down-loaded
from the Mini-Logger 2000 unit using cus-tomized software, andthen
IBI files were transferred toMxedit (Delta-Biometrics Inc.,
Bethesda, MD) for edit-ing of recording artifacts and computation
of cardiacRSA (equivalent to vagal tone or V; Porges, 1985).
Baseline vagal tone (baseline V) recordings wereobtained near
the start of the home visit prior toinitiating the parent child
interaction tasks. Children
were allowed to inspect the monitor and pretend toput it onto a
stuffed animal until they felt comfortableenough to wear it
themselves (5 children refused towear the monitor). Baseline
recording began approx-imately 5 min after attaching the monitor.
To keepchildren still and calm during the baseline
recordings,parents were asked to sit with their children andwatch a
low-action animated videotape (Dragon Tales)or read a childrens
picture book (Curious George).These techniques have been found to
be effective forkeeping children stationary and arousing little
affect(see Calkins & Dedmon, 2000; Rubin et al., 1997). The
goal was to record at least 3 min of cardiac activitywhile the
child was in a stationary and calm state (M54 min 43.89 s, SD 5 1
min 2.52 s). Baseline Vdid notdiffer depending on the use of video
or book, t , 1.0.
Following the baseline, a portable video camerawas set up to
record parent child interactions. Intwo-parent homes, the order of
observing child withmother versus father first was counterbalanced
acrossfamilies. Children were given a difficult puzzle tosolve in
order to record vagal tone (task V) under mildchallenge conditions
(Calkins & Keane, 2004). Chil-dren aged 2 3.5 years were given
a puzzle recom-mended for children 4 years and older, and
children
aged 3.5 4.9 years were given a puzzle recommen-ded for children
6 years andolder. Parents were askedto give only as much help as
they thought their childneeded. For all children, cardiac recording
duringpuzzle completion with the first parent was used tocompute
task V. Five more children removed thecardiac monitor between the
baseline and the puzzletask procedure.
The files of sequential IBIs were examined inMxedit software
(Delta-Biometrics Inc., Bethesda,MD) to visually identify artifacts
and outliers pro-
duced by movement or recording error (e.g., twosuccessive IBIs
added together because the monitorfailed to detect the intervening
R-wave). Baseline datahad to be discarded for 4 children because it
wasunusable (multiple consecutive recording errorsthroughout the
baseline period), such that baselinedata were available for 124
children. Three or moreminutes of usable IBI data were obtained for
107children; for the remaining 17 children, at least 60 s
oferror-free baseline data were available. Puzzle taskdata had to
be discarded for 7 children because it wasunusable. In total,
puzzle task data were obtainedfrom 112 children, all but 1 of whom
also providedusable baseline data. Cardiac data throughout
thepuzzle task were usable for most children (M5 4min21.31 s, SD5 1
min 35.91 s), and all children providedat least 60 s of error-free
puzzle task data.
Mxedit uses a moving 21-point polynomial algo-
rithm that isolates heart rate variability at the ampli-tude and
period of the oscillations associated withbreathing, reported in
units of ln(ms)2. Age-specificfrequency band-pass parameters are
used to quantifyRSA that corresponds to developmentally
normativespontaneous respiration. The frequency band for
RSAcomputation used for this preschool-age sampleranged from 0.24
to 1.04 Hz. RSA was computed foreach sequential 20-s interval in
each IBI data file, andthe mean of these sequential values was used
as themeasure of RSA for each child.
The durations of usable IBI data during baseline
and puzzle task were not significantly correlated withV, rs 5
.15 and .01, respectively. Children showeda significant decrease in
V from baseline (M 5 5.25,SD 5 1.35, range 5 2.20 9.46) to puzzle
(M 5 4.05,SD5 1.11, range 5 1.46 6.45), paired t(110) 5 13.45,p ,
.001. Vagal suppression (task Vlower than base-line V) was shown by
90.1% (100/111) of the children.Although there has been debate
about how best tomeasure and analyze change scores (e.g.,
Llabre,Spitzer, Saab, Ironson, & Schneiderman 1991;
Wainer,1991), residualized change scores have becomewidely used in
recent studies of cardiovascular reac-tivity (e.g., Krantz et al.,
1996; Nazzaro et al., 2005),
and they are recognized as particularly appropriatewhen there is
significant and positive relationbetween baseline and episode
measures (Calkins &Keane, 2004, p. 107). Baseline V and task V
weresignificantly positively correlated, r 5 .71, p ,
.001;therefore, the standardized residual of the predictionof task
V from baseline V was used as the index ofchange in vagal tone (DV)
under mild cognitivechallenge conditions. DV corresponds to the
inverseof vagal suppression, as higher values ofDVreflectincreases
(or smaller decreases) in Vfrom baseline to
Vagal Tone, Parenting, and Adjustment 51
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
8/20
puzzle task. DVdid not differ between children whocompleted the
puzzle with mother or with father,t(109) 5 1.47.
Observations of social wariness. Social wariness wasobserved in
two contexts. First, 122 children werevisited at their day care or
preschool on a day thatbegan with a free-play period. Each childs
play withhis or her familiar preschool peers was observed for12
min, beginning2 5 min after the child had enteredthe playroom and
separated from the parent.
Second, triads of same-sex, same-age unfamiliarchildren were
invited to the laboratory for a visit.Arrival times of families
were staggered, and eachfamily was greeted by an examiner and taken
toa separate waiting room so that children would notsee each other
prior to entering the laboratory play-room. The 20 ft 20 ft
playroom contained a varietyof age-appropriate toysthat were
conducive for either
individual or social play. The first activity was a 10-min
free-play period; this was videotaped for 112children from three
corner-mounted cameras.
Childrens displays of wariness during play ses-sions with
familiar peers at preschool and unfamiliarpeers in the laboratory
were made using the PlayObservation Scale (POS; Rubin, 1989). In
both con-texts, play behavior was coded in 10-s time samples.Live
observations were done in the preschool visits,and laboratory
visits were coded from videotape.Coders had to attain j ! .70 for
POS coding of60 min of videotaped play and at least two 1-hr
live
preschool visits before being the primary coder ona preschool
visit for a participant. Repeated reliabilitycoding of videotaped
laboratory interactions ensuredthat all coders maintained j ! .70.
Social wariness ineach context was defined as the proportion
ofobserved 10-s time segments spent as onlooker/unoccupied:
watching others play without trying tojoin, not playing on ones
own, inactivity or lack offocus, and isolation. For observed
wariness at pre-school, M 5 .17, SD 5 0.16 (range 5 0.00 0.81),
andfor observed wariness in the laboratory, M 5 0.23,SD 5 0.26
(range 5 0.00 1.00), paired t 5 1.33.
Results
Preliminary Analyses: Data Reduction
Observed parenting. Observed parenting behavioracross tasks was
aggregated to form scores forobserved protective overcontrol and
supportiveness.Protective overcontrol included Protect and
Encour-age Engagement (reversed) scores from narrativesand Assist
and Take Over scores from cleanup. Scoreswere z-transformed and
averaged (single-factor sol-
utions were supported for both mothers and fathers,with
eigenvalues5 1.20 and 1.41, respectively, and allfactor loadings
!.48). Supportive parenting includedthe Supportive score from
narratives, Positive andSupportive scores from origami, and
Positive andEncouraging scores from cleanup; scores were
z-transformed and averaged (single-factor solutionswere supported
for both mothers and fathers, witheigenvalues 5 1.53 and 1.72,
respectively, and allfactor loadings ! .30). Observed parenting
scoreswere computed for 131 mothers and 102 fathers.
Temperamental inhibition. Mothers and teachersreports of
inhibition were significantly correlated,r 5 .26, p , .01. Thus,
their reports were first z-transformed and then averaged (n5 128).
When onlyone report was available, this was used as the index.
Internalizing problems. The correlation betweenmothers and
teachers reports of childrens inter-
nalizing problems approached significance, r 5 .17,p , .10,
comparable to the correspondence betweenseparate CBCL reports on
young childrens inter-nalizing problems seen in prior studies
(e.g., Hay etal., 1999). Mothers and teachers reports of
internal-izing problems were averaged (n5 127), M5 50.72,SD 5 8.72
(range 5 33 72). When only one reportwas available, this was used
as the index.
Observed social wariness. Preschoolers onlooker/unoccupied
behaviors with familiar peers at pre-school and unfamiliar peers in
the laboratory weresignificantly correlated, r 5 .22, p , .05.
Therefore,
onlooker/unoccupied behaviors at preschool and inthe laboratory
were averaged to form the index ofobserved social wariness (n 5
128), M 5 0.20, SD 50.18 (range 5 0.00 1.00). Wariness was based
onbehavior in only one context when observations inboth contexts
were not available.
Relations Between Predictors and Outcomes
The first-order correlations between baseline V,task V, DV,
maternal and paternal reported andobserved parenting, and the three
measures of child-rens anxious difficulties are presented in Table
2.
There were no significant correlations involving themeasures of
vagal tone. The corresponding indices ofmothers observed and
reported protective overcon-trol, and of fathers supportiveness,
were positivelycorrelated, indicative of moderate convergence
acrossmeasures. Two of the four corresponding maternaland paternal
parenting scores were positively corre-lated, indicative of
moderate consistency in childrenssocialization experiences across
parents in two-parenthomes. Children with more internalizing
problemshad mothers who were more protective (reported)
52 Hastings et al.
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
9/20
and less supportive (observed and reported). Fathersand mothers
reported protective overcontrol wasalso positively correlated with
internalizing problemsand temperamental inhibition, respectively.
Moreinhibited children had more internalizing problems
and showed more social wariness, although the lattertwo were not
significantly correlated.
Regression Analyses
Check for control variables. Six potentially con-founding
variables were examined to determine ifthey were associated with
the variables of interest inthis study: sex and age of child,
family structure(number of parents), order of observing parent
childinteractions, type of school, and availability of
teacherreports. Four of these were associated with thevariables of
interest. (a) Girls internalizing problems
scores (M5 52.25, SD5 8.92) were higher than thoseof boys (M5
48.67, SD5 8.75), t(104)5 2.08, p, .05.(b) Older children had
higher baseline V, r(109)5 .27,p , .01. (c) Mothers in two-parent
homes reportedmore supportiveparenting than single mothers(Ms56.14,
5.74; SDs5 0.42, 0.67, respectively), t(109)5 3.27,p , .01. (d)
Compared to families for which teacherreports were returned, in
families lacking teacherreports mothers were less supportive on
reported(Ms5 6.12, 5.72; SDs5 0.42, 0.75, respectively), t(109)5
2.87, p , .01, and observed measures (Ms 5 0.12,
0.54; SDs 5 0.96, 0.96, respectively), t(107) 5 2.34,p , .05.
The same difference in fathers reportedsupportiveness was seen (Ms
5 6.01, 5.50; SDs 50.53, 0.71, respectively), t(83)5 2.22,p, .05.
Childrenlacking teacher reports also had more internalizing
problems (Ms5
56.89, 49.93; SDs5
11.01, 8.60,respectively), t(104) 5 2.27, p, .05.Preliminary
analyses were conducted to examine
whether any of these six variables needed to becontrolled in the
predictive regressions. Age, familystructure, observation order,
and type of school didnot affect the strength of the regressions.
Sex andavailability of teacher reports predicted
childrensinternalizing problems (across analyses, maximumbs5 .20
and.22, respectively,p, .05), and includingthem influenced whether
some associations betweentargeted predictors and outcomes reached
traditionallevels of significance. Therefore, sex of child and
availability of teacher reports were entered as controlvariables
in all analyses.
Preliminary regression analyses were also per-formed to
determine whether sex and age of childmoderated the relations
between V, DV, maternal andpaternal parenting, as predictors, and
anxious diffi-culties, as outcomes. None of the two-way
interactionterms involving sex significantly predicted child
out-comes. Only 1 of 18 interactions (5.6%) involving agewas
significant at p , .05, attributable to chance.Therefore, sex and
age of child did not appear to
Table 2
Intercorrelations of Predictor and Outcome Variables
Variable 4 5 6 7 8 9 10 11 12 13 14
Child Physiology
1. Baseline V .07 .04 .11 .01 .02 .17y .03 .03 .03 .09 .04
2. Task V .01 .01 .07 .01 .01 .13 .05 .00 .03 .09 .08
3. DV .08 .04 .01 .01 .02 .04 .02 .01 .03 .04 .08
Mothers Parenting
4. Reported protective .27** .28** .13 .23* .05 .01 .14 .25**
.20* .09
5. Reported supportive .11 .17y .10 .10 .06 .15 .34*** .05
.10
6. Observed protective .04 .14 .07 .11 .10 .07 .09 .00
7. Observed supportive .15 .07 .09 .24* .19* .09 .05
Fathers Parenting
8. Reported protective .14 .08 .02 .20* .19y .05
9. Reported supportive .20* .24* .07 .08 .06
10. Observed protective .11 .03 .03 .13
11. Observed supportive .12 .13 .13
Child Outcomes
12. Internalizing problems .45***
.0513. Inhibited temperament .33***
14. Social wariness
Note. Reported parenting is from Child-Rearing Practices Report
(Block, 1981); observed parenting is from home visits.yp , .10. *p
, .05. **p , .01. ***p , .001.
Vagal Tone, Parenting, and Adjustment 53
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
10/20
influence the relations of principal interest in
thisinvestigation.
General format for regression analyses. Hierarchicallinear
regression analyses were used to predict inter-nalizing problems,
temperamental inhibition, andsocial wariness from baseline Vand
DVand mothersand fathers reported and observed parenting. Withtwo
indices of vagal regulation and two methods ofassessing parenting
used to predict three outcomes,there were 12 regressions examined
for fathers and 12for mothers. For each regression, the control
variablesof child sex and availability of teacher reports
wereentered first,DV(or V) and the measures of
protectiveovercontrol and supportive parenting were enteredon the
second step, and the two interactions ofDV(orV) Parenting were
entered third. As recommendedby Aiken and West (1991), predictor
variables werecentered prior to computing interaction terms,
and
centered variables were entered into the regressionanalyses.
Significant (p , .05) interaction terms wereexamined by regressing
the dependent variable onthe parenting score at low (1 SD) and high
(+1 SD)values ofDV(or V) in order to clarify how childrensDV(or V)
moderated the association between parent-ing and the index of
anxious adjustment.
Predictions from paternal parenting and DV. Theregression
analyses involving paternal parentingand vagal suppression are
presented in Table 3. Twoof the six interactions were significant,
and two moreapproached significance. There were no significant
direct effects, but fathers who were observed to bemore
supportive had children who tended (.08,p,.11) to show less of all
three anxious difficulties. Fiveof the 12 interactions (42%)
involving DVand fathersparenting were significant; two illustrative
effects aredepicted in Figure 1. All the significant
interactioneffects were consistent with the hypothesis that
pro-tective overcontrol would predict more anxious diffi-culties
and supportive parenting would predict feweranxious difficulties,
specifically for children with lessparasympathetic self-regulation
as indexed byweaker vagal suppression. From the measures ofreported
parenting, DV Protective Overcontrol
predicted childrens inhibition (Figure 1a) and DVSupportive
predicted their wariness. More protectiveparenting predicted more
inhibition when vagalsuppression was weaker (b 5 .40, p , .02) but
notwhen vagal suppression was stronger (b 5 .07, ns).More
supportive parenting was associated withless wariness when vagal
suppression was weaker(b 5 .30, p , .20) but not when vagal
suppressionwas stronger (b5 .13). For the analyses with
observedparenting, DV Supportive predicted both internal-izing
problems (Figure 1b) and inhibition and DV
Protective predicted wariness. When vagal suppres-sion was
weaker, more supportive parenting byfathers predicted fewer
internalizing problems (b 5.41, p , .01) and less inhibition (b 5
.39, p , .01)and more protective parenting was weakly
associatedwith more wariness (b 5 .25, p , .20). With strongervagal
suppression, supportive parenting did notpredict either
internalizing problems or inhibition(bs5 .08 and .04, respectively)
and protective parent-ing predicted less wariness (b 5 .40, p ,
.01).
Predictions from maternal parenting and DV. Theregression
analyses involving maternal parentingand vagal suppression are
presented in Table 4. Threeof the six regressions were significant.
Children withmore internalizing problems had mothers who re-ported
significantly less supportive parenting andwho tended to report
more protective overcontrol.Mothers observed supportive parenting
predicted
fewer internalizing problems. In the prediction ofwariness from
reported parenting, the DV Pro-tective interaction was significant
and the DV Supportive interaction approached significance.Examining
the significant interaction, the moderationeffect was counter to
the hypothesis (Figure 2): Moreprotective parenting predicted more
wariness whenvagal suppression was stronger (b 5 .38, p, .01)
butnot when vagal suppression was weaker (b 5 .27,p , .10).
Predictions from paternal parenting and baseline V. Ofthe six
regression analyses involving paternal parent-
ing and baseline V, only the prediction of socialwariness from
observed parenting was significant,adjusted R2 5 .116, F(7, 83) 5
2.70, p , .05. (In theinterests of conserving space, the
predominantly non-significant regression analyses involving
baseline Vare not presented in tables. Readers interested in
thedetailed results of these analyses may contact the firstauthor
for copies.) Social wariness was significantlypredicted by Baseline
V Observed Protective (b 5.25, p , .05); this was the only 1 of the
12 testedinteraction effects that was significant.
Protectiveovercontrol did not predict wariness at higher levelsof
baseline V (b 5 .10, ns), but counter to the
hypothesis, protective predicted less wariness atlower levels of
baseline V (b 5 .38, p , .01). Therewere no significant direct
effects in any analyses, butthe children of fathers who reported
more protectiveovercontrol tended to have more internalizing
prob-lems and greater inhibition (both p , .10).
Predictions from maternal parenting and baseline V. Ofthe six
regression analyses involving maternalparenting and baseline V,
only the prediction of inter-nalizing problems from reported
parenting was sig-nificant, adjusted R25 .161, F(7, 110)5 4.21, p,
.001.
54 Hastings et al.
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
11/20
Table3
PredictionofInternalizingProblems(IP
),TemperamentalInhibition(TI),a
ndSocialW
ariness(SW)FromDVandFathersReportedandObservedParenting
IP
TI
SW
MultR
DR2
B
p
MultR
DR2
B
p
MultR
DR2
B
p
ReportedParenting
Step2
.347
.051
ns
.303
.038
ns
.151
.014
ns
DV
.0
5
ns
.02
ns
.04
ns
FProtective
.16
ns
.14
ns
.11
ns
FSupportive
.1
2
ns
.1
2
ns
.00
ns
Step3
.348
.001
ns
.409
.075
.039
.296
.065
.079
DV
FProtective
.02
ns
.32
.012
.1
8
ns
DV
FSupportive
.04
ns
.09
ns
.3
2
.029
Modelsummary
AdjustedR2
5
.039,
F(7,
75)5
1.48,
ns
AdjustedR2
5
.089,F
(7,7
5)5
2.1
5,p,
.05
AdjustedR2
5
.001,F(7,
74)5
1.01,n
s
ObservedParenting
Step2
.320
.036
ns
.314
.049
ns
.298
.063
ns
DV
.0
5
ns
.04
ns
.06
ns
FProtective
.0
1
ns
.1
0
ns
.1
3
ns
FSupportive
.1
8
.103
.1
8
.105
.1
9
.089
Step3
.406
.063
.071
.408
.068
.056
.418
.086
.028
DV
FProtective
.00
ns
.13
ns
.31
.010
DV
FSupportive
.2
6
.022
.2
5
.028
.1
1
ns
ModelSummary
AdjustedR2
5
.085,F
(7,
73)5
2.0
6,p,
.06
AdjustedR2
5
.087,F
(7,7
3)5
2.0
9,p,
.06
AdjustedR2
5
.094,
F(7,72
)5
2.1
7,p,
.05
Note.Sexofchildandavailabilityof
teacherreportwereenteredinStep1ofallanalyses.F5
father.
Vagal Tone, Parenting, and Adjustment 55
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
12/20
The same direct effects of maternal parenting forchildrens
internalizing problems noted previouslywere evident in these
analyses. Only 1 of the 12 testedinteraction effects was
significant. The Baseline VReported Protective Overcontrol
interaction signifi-cantly predicted social wariness (b 5 .29, p ,
.01).Examining the significant interaction (Figure 3), and
in accord with the hypothesis, maternal protective-ness
predicted more wariness at lower levels ofbaseline V (b 5 .26, p ,
.05) but tended to predictless wariness at higher levels of
baseline V(b5.20,p , .10).
Summary. Overall, compared to baseline V, vagalsuppression
appeared to be a more consistent indica-tor of child vulnerability
and susceptibility to social-ization and specifically to fathers
parenting. All fivesignificant associations between paternal
socializa-tion measures and childrens anxious difficulties thatwere
moderated by vagal suppression matched thevulnerability hypothesis.
Conversely, mothers sup-
portive parenting was directly associated with inter-nalizing
problems, there were only two moderatedeffects of maternal
parenting, and baseline Vwas themoderator of associations between
protective over-control and social wariness that matched the
hypoth-esis. Finally, the patterns of predictive relations
werefairly consistent across reported and observed par-enting,
although few direct comparisons matched.
Do maternal and paternal parenting jointly predictchildrens
anxious difficulties? The predictions of inter-nalizing problems
from DVand observed parenting
included significant effectsfor mothersand fathers, asdid the
predictions of social wariness from DVandreported parenting. To
determine whether fathersandmothers made significant unique
contributions tochildrens anxious difficulties, two additional
analy-ses were conducted. (a) In a prediction of internaliz-ing
problems from DVand observed parenting, the
control variables were entered on Step 1,D
V andmaternal and paternal supportive were entered onStep 2, and
the DV Paternal Supportive interactionwas entered on Step 3. The
analysis was significant,adjusted R2 5 .155, F(6, 72) 5 3.39, p ,
.01, and boththe direct effect of maternal supportive (b 5 .24,p ,
.05) and DV Paternal Supportive interaction(b 5 .28, p , .05) were
significant. (b) A similarlystructured regression predicting social
wariness fromDV and reported parenting included DV,
maternalprotective, and paternal supportive on Step 2 and DV
Paternal Supportive and DVMaternal Protectiveinteraction terms on
Step 3. The overall model was not
significant, but Step 3 was significant, DR2 5 .079,F(2, 72) 5
3.20, p , .05. Both the paternal and thematernal interaction terms
approached significance(bs 5 .25 and .21, respectively, p ,
.10).
Discussion
In this investigation, we obtained support for a
biopsy-chosocial model of the contributions of fathers
social-ization to the anxious difficulties of physiologically
-0.5
-0.375
-0.25
-0.125
0
0.125
0.25
Low Protective High Protective
Fathers' Parenting
Inhibition
45
46
47
48
49
50
51
52
53
54
55
Low Supportive High Supportive
Fathers' Parenting
InternalizingP
roblems
Less Vagal
Suppression
More Vagal
Suppression
Less Vagal
Suppression
More Vagal
Suppression
(a) (b)
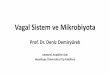
Figure 1. (a) Childrens vagal suppression moderates the relation
between fathers reported protective overcontrol and
childrenstemperamental inhibition. (b) Childrens vagal suppression
moderates the relation between fathers observed supportive
parenting andchildrens internalizing problems.
56 Hastings et al.
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
13/20
Table4
PredictionofInternalizingProblems(IP
),TemperamentalInhibition(TI),a
ndSocialW
ariness(SW)FromDVandMothersReportedandObservedParenting
IP
TI
SW
MultR
DR2
B
p
MultR
DR2
B
p
MultR
DR2
B
p
ReportedParenting
Step2
.474
.139
.001
.210
.033
ns
.242
.023
ns
DV
.00
ns
.0
6
ns
.1
0
ns
MProtective
.17
.076
.16
ns
.05
ns
MSupportive
.3
1
.002
.0
4
ns
.1
1
ns
Step3
.486
.012
ns
.216
.003
ns
.430
.127
.001
DV
MProtective
.0
1
ns
.0
5
ns
.2
8
.005
DV
MSupportive
.1
1
ns
.0
3
ns
.18
.061
Modelsummary
Adju
stedR2
5
.182,
F(7,98)5
4.34,
p,
.001
AdjustedR2
5
.000,
F(7,
98)5
0.69
,ns
AdjustedR2
5
.126,F
(7,96
)5
3.12,p,
.01
ObservedParenting
Step2
.372
.058
.091
.163
.015
ns
.211
.009
ns
DV
.08
ns
.0
1
ns
.0
9
ns
MProtective
.11
ns
.08
ns
.0
3
ns
MSupportive
.2
2
.027
.1
0
ns
.0
1
ns
Step3
.384
.009
ns
.213
.019
ns
.285
.037
ns
DV
MProtective
.0
6
ns
.03
ns
.1
2
ns
DV
MSupportive
.0
7
ns
.14
ns
.17
.106
ModelSummary
AdjustedR2
5
.085,
F(7,96)5
2.37,p,
.05
AdjustedR2
5
.000,
F(7,
97)5
0.66
,ns
AdjustedR2
5
.014,F
(7,96)5
1.2
1,ns
Note.Sexofchildandavailabilityof
teacherreportwereenteredinStep1ofallanalyses.M5
mother.
Vagal Tone, Parenting, and Adjustment 57
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
14/20
vulnerable children. Assessing parasympathetic reg-ulation as a
dynamic process within appropriatelychallenging contexts appeared
to be most revealing ofits developmental role, as childrens
adaptive vagalsuppression to a mild cognitive challenge was a
moreconsistent moderator of paternal socialization thanwas their
baseline vagal tone. Conversely, all childrenappeared to benefit
from mothers supportive parent-ing, and the evidence for maternal
protective over-control predicting social wariness most strongly
inchildren with poor parasympathetic self-regulationwas mixed.
There were more associations betweenchildrens anxious difficulties
and their receipt ofsupport than their experiences of protective
over-control, although for both aspects of parenting, rela-tions
were predominantly in accord with the
socialization hypotheses. As well, there were moreassociations
for reported than observed measures ofmothers parenting, whereas
the converse tended tobe true for fathers parenting, but when
mothers andfathers parenting were considered simultaneously,both
mothers and fathers in two-parent familiescontributed to their
childrens anxious difficulties.The results for paternal
socialization were particu-larly noteworthy, as only fathers
parenting predictedchildrens inhibition, and fathers
supportivenesscontributed to the predictions of childrens
internal-izing problems and anxious difficulties independentof
maternal socialization.
The principal goal of this investigation was toexamine a
possible mechanism by which childrenmanifest adaptive versus
maladaptive social, emo-tional, and behavioral adjustment.
Physiological vul-nerability, as indexed by less vagal suppression
under
conditions requiring attention and active coping(Beauchaine,
2001; Calkins & Keane, 2004; Porges,1995), was expected to
demarcate children who wererelatively lacking in internal
self-regulatory resour-ces. These children were expected to be more
depen-dent upon external sources of regulation throughparental
socialization, such that they would bothexperience more benefit
from supportive parentingbut also be more susceptible to the
adverse influencesof parents psychological control. Intriguingly,
sup-port for these hypothesized moderation effects wasevident only
for fathers parenting.
Our results indicated that, on their own, baselinevagal tone and
vagal suppression were not stronglyassociated with childrens
anxious difficulties, mir-roring the literatures generally weak
associationsbetween vagal tone and childrens inhibition, wari-ness,
and internalizing problems (e.g., Rubin et al.,1997; Schmidt et
al., 1999). The moderating functionsof vagal suppression on the
relations between pater-nal socialization and adjustment were more
salient,and there was also evidence of vagal tone moderatingthe
relations between maternal protective overcontroland adjustment.
This may shed light on the apparentinconsistency of the links
between vagal tone and
childrens adjustment (e.g., El-Sheikh et al., 2001;Schmidt et
al., 1999). Parasympathetic regulation doesnot function in
isolation, and physiological vulnera-bility is not tantamount to
biological determinism.Whether a vulnerable child develops
problems, andthe natureand severity of those problems, depends
onthe childs socialization experiences.
Examining low vagal suppression as a physiologi-cal risk factor
thereby extended the findings of pre-vious studies that have used
behavioral inhibition asa marker of dispositional vulnerability
(Rubin et al.,
0.1
0.15
0.2
0.25
0.3
Low Protective High Protective
Mothers' Parenting
Warine
ss
Less Vagal
Suppression
More Vagal
Suppression
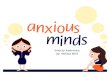
Figure 2. Childrens vagal suppression moderates the
relationbetween mothers reported protective overcontrol and
childrenssocially wary behaviors with peers.
0.1
0.15
0.2
0.25
Low Protective High Protective
Mothers' Parenting
Wariness
Lower
Baseline
Vagal Tone
Higher
Baseline
Vagal Tone
Figure 3. Childrens baseline vagal tone moderates the
relationbetween mothers reported protective overcontrol and
childrenssocially wary behaviors with peers.
58 Hastings et al.
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
15/20
1999, 2002). Children with lower vagal suppression tothe puzzle
task were described as having moreinternalizing problems and being
more inhibited bytheir mothers and teachers, and they displayed
moresocial wariness with peers, when their fathers weremore
protective and less supportive. Conversely, theadjustment of
children with greater vagal suppres-sion was relatively independent
of paternal socializa-tion, and there was a notable lack of robust
directrelations between fathers parenting and childrensadjustment.
Thus, we have provided some of the firstevidence of biopsychosocial
processes involving fa-thers socialization of young children.
Overprotectivefathers may perceive their less well-regulated
chil-dren as incapable of autonomous activity or in need ofextra
assistance, causing them to be intrusive, over-bearing, and
restricting of the childrens experiences.This could suggest to
children that they are incapable
or that the world is unsafe, such that they requireparental
assistance (Mills & Rubin, 1998). Conversely,more supportive
fathers may structure interactions ororganize situations in ways
that their vulnerablechildren find manageable, such that they have
oppor-tunities to practice autonomous coping and experi-ence
positive results, building their self-confidenceand reducing their
likelihood of developing anxiousadjustment difficulties.
It was also intriguing that there were more associ-ations of
paternal parenting with childrens inhibitionand wariness than with
their internalizing problems.
Whereas inhibition and wariness may be conceptual-ized as
normative aspects of social behavior that allyoung children
manifest to greater or lesser degrees,high levels of internalizing
problems are more clearlyindicative of atypical and clinical
maladjustment.It has often been argued that positive
paternalsocialization is particularly important for
childrensdevelopment of social competence within peer
rela-tionships (Parke, 1995; Pettit, Brown, Mize, &
Lindsey,1998). The current results may be seen as convergentwith
this view, as physiologically vulnerable child-rens shyness and
withdrawal from social engage-ment werelower if their fatherswere
more supportive
and less overprotective.The only inconsistencies in the current
results
concerned the role of childrens vagal regulation inthe relations
between social wariness with peers andparental protective
overcontrol. Vagal suppressionmoderated fathers observed protective
in accordwith the vulnerability hypothesis, but fathersobserved
protective predicted less wariness in chil-dren with low baseline
vagal tone. In direct contrast,mothers reported protective
predicted greater wari-ness both in children with low baseline
vagal tone and
in children with stronger vagal suppression. Consid-ered another
way, these results showed that lowbaseline vagal tone characterized
children vulnerableto the protective overcontrol of mothers but not
that offathers, whereas weak vagal suppression demarcatedchildren
susceptible to the protective overcontrol offathers but not that of
mothers. Resting and reactivemeasures of physiological regulation,
therefore, maydemarcate different qualities of vulnerability.
Base-line vagal tone is conceptualized as more reflectiveof a
childs typical or trait-like level of arousal(Beauchaine, 2001),
akin to temperament, and vagalsuppression as a more dynamic and
state-like indica-tor of adaptive allocation of resources under
demand-ing conditions (Porges, 1995). Despite generationalchanges
in family roles and great variability acrossfamilies, it is still
the case that mothers have greaterresponsibility for child care,
are involved in a greater
range of activities, and share more time with theiryoung
children than do fathers (Coltrane, 2000;Wood & Repetti, 2004);
fathers interactions are morelimited in context, activity, and
time. Thus, childrenmay experience maternal parenting as
amalgama-tions of diverse kinds of contact throughout day-to-day
routines and across their typical range of arousalstates. Paternal
parenting may be experienced asmore in the moment or situation
specific whenchildren are in moreactivated states.
Correspondingly,it is plausible that childrens trait-like
self-regulatorycapacity would moderate mothers socialization
efforts,
whereas their state-like reactivity would moderatesocialization
by fathers. Of course, this is a highlyspeculative post hoc
explanation for a small set ofrelated results and only one of the
several possibleinterpretations of these data. It will require
replicationand rigorous evaluation in future studies to clarify
themeanings of these relations.
The more consistent pattern for maternal sociali-zation was
that, overall, it was similarly important forchildrenwith
bothweaker and stronger self-regulatorycapacities. The strongest
finding for mothers parent-ing was that internalizing problems were
most severein those children who had less supportive mothers.
Mothers who described themselves as more support-ive also
reported being less protective, and thesignificant first-order
correlation between internaliz-ing problems and maternal protective
overcontrolwas weakened when maternal supportiveness wascontrolled.
Thus, it was chiefly young childrensexperiences with mothers who
were appropriatelywarm, more encouraging, and more prone to the
useof teaching and gentle control that were associatedwith their
displays of fewer internalizing problemsmonths later, echoing the
results of one recent report
Vagal Tone, Parenting, and Adjustment 59
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
16/20
that examined both supportive parenting and psy-chological
control (Bayer et al., 2006).
The report by Bayer et al. (2006) is rather excep-tional, as few
researchers have assessed both adaptiveor appropriate parenting and
maladaptive or inap-propriate parenting within the same
investigation. Inparticular, most past studies of the relations
betweenparental protective overcontrol and young childrensproblems
have not also consideredthe possible role ofpositive parenting. The
inverse relation betweenmaternal supportive and overprotective
parentingraises the possibility that the often replicated
linksbetween psychological control and anxious adjust-ment (e.g.,
Hudson & Rapee, 2001; Mills & Rubin,1998) may be
attributable to young childrens simul-taneous experiences of less
supportive parenting. Theimportance of appropriate maternal warmth,
nurtur-ance, and support for autonomy may be particularly
important for the developmental period targeted inthis study
(Early et al., 2002). Such parenting wouldcontribute to a young
childs felt security and devel-opment of an attachment
relationship, promotingexploration and a childs developing
competence(Bretherton, Golby, & Cho, 1997). Lacking the
benefitsconferred by such positive maternal
socializationexperiences may leave all toddlers and
preschoolersvulnerable to the kinds of anxious difficulties
thatcharacterize early emerging internalizing problems(Zahn-Waxler
et al., 2000). It is also possible that theadverse effects of
maternal psychological control
become more pronounced or directly associated
withadjustmentbeyond the preschool years (Barber, 2002).This
investigation documented a number of addi-
tional findings worthy of attention. To begin, weprovided
moderate support for the utility and vali-dity of the CRPR as a
measure of socialization byshowing that mothers reported protective
overcon-trol and fathers reported supportive parenting
weresignificantly associated with direct observations
ofcorresponding parenting behavior during interac-tions with
children. Although low in magnitude, thecorrespondences between
observed and reportedparenting were comparable or better than
those
reported in other recent studies (e.g., Bayer et al.,2006;
Janssens et al., 2005). The similarity in therelations of both
observed and reported parentingwith childrens anxious difficulties
also providedmultimethod evidence of convergent validity forthese
socialization influences.
In addition, we demonstrated correspondencebetween preschoolers
wary behaviors with familiarpeers in the natural settings of day
cares and pre-schools and with unfamiliar peers in the novel
settingof a laboratory playroom. To our knowledge, this is
the first direct demonstration of the ecological vali-dity of
the unfamiliar peer procedure that has beenwidely used to assess
inhibition and reticence (e.g.,Kochanska & Radke-Yarrow, 1992;
Rubin et al., 1997,2002). Although the correlation across contexts
wassignificant, it was of small magnitude, suggesting thatthere
were a number of children with discordantdisplays of wariness
across social contexts. Attentionto the factors contributing to
behavioral rigidity orflexibility appears warranted.
It was also intriguing to note that reported childinhibition was
associated with both observed warinessand reported internalizing
problems, although the lattertwo were not significantly correlated.
This might sug-gestthattemperamentalinhibition is a common
elementof both normative shy behaviors and clinical anxietyproblems
(Prior et al., 2000). However, direct briefobservations of
childrens social behaviors with peers
may not be effective means of identifying which chil-dren are
likely to have serious and persistent problems.
Finally, although the rather low correspondencebetween mothers
and teachers reports of pre-schoolers internalizing problems is in
accord withpast research (Hayet al., 1999), it suggests that
parentsare not the most accurate reporters of their youngchildrens
risk for maladjustment within early edu-cational settings. Most
mothers have limited oppor-tunity to observe their preschool-age
children inlarge-group social settings with peers, which mayleave
them somewhat unaware of their childrens
levels of social comfort or difficulties at day care
orpreschool. Still, this has implications for the identifi-cation
of risk for school maladjustment and theeffective targeting of
children or families who maybenefit from early assistance.
Limitations and Suggestions for Future Research
Despite evidence for convergent and predictivevalidity, the low
internal consistency of the self-reportmeasures of parenting may
have limited the ability toshow their association with childrens
anxious diffi-culties. Conversely, mothers reports of their
child-
rens functioning were components of the scores forinhibition and
internalizing problems, such that com-mon source variance may have
contributed to theassociations between these variables and
mothersreported parenting. Given the correlational design,causality
cannot be inferred and the presumed direc-tion of effects of
parental socialization cannot be takenfor granted; despite being
measured later in time,childrens anxious difficulties may have
influencedparents socialization techniques. Furthermore, giventhe
contemporaneous measurement of parental
60 Hastings et al.
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
17/20
socialization and childrens physiology, the role
ofparasympathetic regulation as a moderator is hypo-thetical only;
it would have been just as plausible tosuggest that socialization
moderated the relationsbetween vagal tone or vagal suppression and
child-rens anxious difficulties. One could also questionwhether the
puzzle task was an appropriate challengefor assessing dynamic vagal
change as it pertains tosocial and emotional functioning. Although
pastresearch has shown that young childrens vagalchange to a puzzle
task is positively correlated withvagal change to emotionally
demanding procedures(Calkins & Keane, 2004), it is still
plausible that thelatter would be uniquely linked to problems.
In response to these issues, researchers shouldexpand upon the
range of contextual modifiers ofself-regulatory processes that have
been considered.Examining childrens dynamic physiological pro-
cesses under such naturalistic social conditions aspeer play, or
in response to emotionally challengingtasks such as mood induction
procedures, might yieldstronger associations with their social and
emotionalfunctioning. Similarly, improving and refining
instru-ments to measure salient aspects of parental sociali-zation
will continue to be important. Repeatedassessment of
self-regulation, parenting, and adjust-ment over a longer
developmental time course wouldhelp to disentangle
direction-of-effect issues andcould reveal whether the identified
relations haveenduring impacts on childrens well-being.
Despite recognizing the limits of the current studyand the need
for further research, this investigationhas provided novel and
important information on thecontributions of childrens
physiological functioningand parental socialization to childrens
internalizingproblems and anxious adjustment. This work empha-sizes
the connections in childrens experiences acrosshome, school, and
peer contexts, the varying needs ofindividual children, and the
contributions made byboth mothers and fathers to their childrens
well-being. Building on these insights will be essential
forimproving the identification of children who may beat risk for
maladjustment and developing more
effective interventions to support childrens develop-ment of
social comfort and competence.
References
Achenbach, T. M., & Rescorla, L. A. (2000). Manual for
theASEBA preschool forms and profiles. Burlington: Univer-sity of
Vermont, Department of Psychiatry.
Aiken, L. S., & West, S. G. (1991). Multiple regression:
Testingand interpreting interactions. Newbury Park, CA: Sage.
Barber, B. K. (2002). Intrusive parenting: How
psychologicalcontrol affects children and adolescents. Washington,
DC:American Psychological Association.
Barber, B. K., Bean, R. L., & Erickson, L. D.
(2002).Expanding the study and understanding of psycholog-ical
control. In B. K. Barber (Ed.), Intrusive parenting: How
psychological control affects children and adolescents (pp.263
289). Washington, DC: American PsychologicalAssociation.
Barber, B. K., & Harmon, E. L. (2002). Violating the
self:Parental psychological control of children and adoles-cents.
In B. K. Barber (Ed.), Intrusive parenting: How
psychological control affects children and adolescents (pp.15
52). Washington, DC: American Psychological Asso-ciation.
Baumrind, D., & Black, A. E. (1967). Socialization
practicesassociated with dimensions of competence in preschool
boys and girls. Child Development, 38, 291 327.Bayer, J. K.,
Sanson, A. V., & Hemphill, S. A. (2006). Parent
influences on early childhood internalizing difficulties.Journal
of Applied Developmental Psychology, 27, 542559.
Beauchaine, T. P. (2001). Vagal tone, development, andGrays
motivation theory: Toward an integrated modelof autonomic nervous
system functioning in psychopa-thology. Development and
Psychopathology, 12, 183 214.
Blair, C. (2003). Behavioral inhibition and behavioralactivation
in young children: Relations with self-regulationand adaptation to
preschool in children attending HeadStart. Developmental
Psychobiology, 42, 301 311.
Block, J. (1981). The Child-Rearing Practices Report (CRPR):A
set of Q items for the description of parental
socializationattitudes and values. Berkeley: University of
California,Institute of Human Development.
Bretherton, I., Golby, B., & Cho, E. (1997). Attachment
andthe transmission of values. In J. E. Grusec & L.
Kuczynski(Eds.), Parenting and childrens internalization of values:
Ahandbook of contemporary theory (pp. 103 134). New York:Wiley.
Calkins, S. D. (1997). Cardiac vagal tone indices of
tem-peramental reactivity and behavioral regulation in
youngchildren. Developmental Psychobiology, 31, 125 135.
Calkins, S. D., & Dedmon, S. E. (2000). Physiological
andbehavioral regulation in two-year-old children
withaggressive/destructive behavior problems. Journal of
Abnormal Child Psychology, 28, 103118.Calkins, S. D., & Fox,
N. A. (1992). The relations among
infant temperament, security of attachment, and behav-
ioral inhibition at 24 months. Child Development, 63,1456
1472.
Calkins, S. D., & Keane, S. P. (2004). Cardiac
vagalregulation across the preschool period: Stability,
conti-nuity, and implications for childhood adjustment.
Devel-opmental Psychobiology, 45, 101112.
Chen, X., Hastings, P. D., Rubin, K. H., Chen, H., Cen, G.,
&Stewart, S. L. (1998). Child rearing practices and be-havioral
inhibition in Chinese and Canadian toddlers:A cross-cultural study.
Developmental Psychology, 34,677686.
Vagal Tone, Parenting, and Adjustment 61
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
18/20
Coltrane, S. (2000). Research on household labor: Modelingand
measuring the social embeddedness of routinefamily work. Journal of
Marriage and Family, 62, 12081233.
Coplan, R. J. (2000). Assessing nonsocial play in
earlychildhood: Conceptual and methodological approaches.
In K. Gitlin-Weiner, A. Sandgrund, & C. Schaefer (Eds.),Play
diagnosis and assessment (2nd ed., pp. 563 598).New York:
Wiley.
Coplan, R. J., Barber, A. M., & Lagace-Seguin, D. G.
(1999).The role of child temperament as a predictor of
earlyliteracy and numeracy skills in preschoolers. Early Child-hood
Research Quarterly, 14, 537553.
Coplan, R. J., Rubin, K. H., Fox, N. A., Calkins, S. D.,
&Stewart, S. L. (1994). Being alone, playing alone, andacting
alone: Distinguishing among reticence and pas-sive and active
solitude in young children. Child Devel-opment, 65, 129 137.
Crockenberg, S. C., & Leerkes, E. M. (2006). Infant
andmaternal behavior moderate reactivity to novelty topredict
anxious behavior at 2.5 years. Development andPsychopathology, 18,
17 34.
Early, D. M., Rimm-Kaufman, S. E., Cox, M. J., Saluja,
G.,Pianta, R. C., Bradley, R. H., et al. (2002).
Maternalsensitivity and child wariness in the transition to
kin-dergarten. Parenting: Science and Practice, 2, 355 377.
El-Sheikh, M. (2001). Parental drinking problems andchildrens
adjustment: Vagal regulation and emotionalreactivity as pathways
and moderators of risk. Journal of
Abnormal Psychology, 110, 499 515.El-Sheikh, M., & Harger,
J. (2001). Appraisals of marital
conflict and childrens adjustment, health, and physio-logical
reactivity. Developmental Psychology, 37, 875885.
El-Sheikh, M., Harger, J., & Whitson, S. (2001). Exposure
tointerpersonal conflict and childrens adjustment andphysical
health: The moderating role of vagal tone. ChildDevelopment, 72,
1617 1636.
El-Sheikh, M., & Whitson, S. (2006). Longitudinal
relationsbetween marital conflict and child adjustment:
Vagalregulation as a protective factor. Journal of Family
Psy-chology, 20, 30 39.
Fox, N. A., & Field, T. M. (1989). Individual differences
inpreschool entry behavior. Journal of Applied Developmen-tal
Psychology, 10, 527540.
Garcia Coll, C., Kagan, J., & Reznick, J. S. (1984).
Behavi-oral inhibition in young children. Child Development,
55,1005 1019.
Gerlach, A. L., Wilhelm, F. H., & Roth, W. T. (2003).
Em-barrassment and social phobia: The role of parasympa-thetic
activation. Journal of Anxiety Disorders, 17, 197 210.
Hastings, P. D., & Rubin, K. H. (1999). Predicting
mothersbeliefs about preschool-aged childrens social
behavior:Evidence for maternal attitude moderating child
effects.Child Development, 70, 722741.
Hastings, P. D., Zahn-Waxler, C., Robinson, J., Usher, B.,
&Bridges, D. (2000). The development of concern forothers in
children with behavior problems. Developmen-tal Psychology, 36,
531546.
Hay, D. F., Pawlby, S., Sharp, D., Schmucker, G., Mills,
A.,Allen, H., et al. (1999). Parents judgements about
youngchildrens problems: Why mothers and fathers mightdisagree yet
still predict later outcomes. Journal of ChildPsychology and
Psychiatry, 8, 1249 1258.
Hirshfeld-Becker, D. R., & Biederman, J. (2002).
Rationale
and principles for early intervention with young chil-dren at
risk for anxiety disorders. Clinical Child andFamily Psychology
Review, 5, 161 172.
Hudson, J. L., & Rapee, R. M. (2001). Parent-child
inter-actions and anxiety disorders: An observational
study.Behavior Research and Therapy, 39, 1411 1427.
Janssens, J. M. A. M., De Bruyn, E. E. J., Manders, W. A.,
&Scholte, R. H. J. (2005). The multitrait-multimethodapproach
in family assessment. European Journal ofPsychological Assessment,
21, 232239.
Kagan, J. (1997). Temperament and the reactions to
unfa-miliarity. Child Development, 68, 139 143.
Kagan, J., & Snidman, N. (1999). Early childhood predic-tors
of adult anxiety disorders. Biological Psychiatry, 46,1536
1541.
Katz, L. F., & Gottman, J. M. (1995). Vagal tone
protectschildren from marital conflict. Development and Psycho-
pathology, 7, 83 92.Katz, L. F., & Gottman, J. M. (1997).
Buffering children
from marital conflict and dissolution. Journal of ClinicalChild
Psychology, 26, 157 171.
Kennedy, A. E., Rubin, K. H., Hastings, P. D., & Maisel,
B.(2004). Longitudinal relations between child vagal toneand
parenting behavior: 2 to 4 years. DevelopmentalPsychobiology, 45,
10 21.
Kenny, M. E., & Gallagher, L. A. (2002). Instrumental
andsocial/relational correlates of perceived maternal and
paternal attachment in adolescence. Journal of Adoles-cence, 25,
203 219.
Kochanska, G., Kuczynski, L., & Radke-Yarrow, M.
(1989).Correspondence between mothers self-reported andobserved
child-rearing practices. Child Development, 60,5663.
Kochanska, G., & Radke-Yarrow, M. (1992). Early child-hood
inhibition and the dynamics of the childs inter-actions with an
unfamiliar peer at age five. ChildDevelopment, 63, 325 335.
Krantz, D. S., Kop, W. J., Gabbay, F. H., Rozanski, A.,Barnard,
M., Klein, J., et al. (1996). Circadian variationof ambulatory
myocardial ischemia. Circulation, 93, 1364 1371.
La Freniere, P. J., & Dumas, J. E. (1995). Manual for the
socialcompetence and behavior evaluation preschool edition.
LosAngeles: Western Psychological Services.
Leary, A., & Katz, L. F. (2004). Coparenting,
family-levelprocesses, and peer outcomes: The moderating role
ofvagal tone. Development and Psychopathology, 16, 593 608.
Llabre, M. M., Spitzer, S. B., Saab, P. G., Ironson, G. H.,
&Schneiderman, N. (1991). The reliability and specificityof
delta versus residualized change as measures ofcardiovascular
reactivity to behavioral challenges. Psy-chophysiology, 28,
701711.
62 Hastings et al.
-
7/31/2019 Parental Socialization, Vagal Regulation, and
Preschoolers Anxious
19/20
Majcher, D., & Pollack, M. H. (1996). Childhood
anxietydisorders. In L. T. Hechtman (Ed.), Do they grow out of
it?Long-term outcomes of childhood disorders (pp. 139
169).Washington, DC: American Psychiatric Press.
Marshall, P. J., & Stevenson-Hinde, J. (1998).
Behavioralinhibition, heart period, and respiratory sinus
arrhyth-
mia in young children. Developmental Psychobiology,
33,283292.
Miller, S. A. (1998). Research methods in
developmentalpsychology. Upper Saddle River, NJ: Prentice Hall.
Mills, R. S. L., & Rubin, K. H. (1998). Are behavioural
andpsychological control both differentially associated
withchildhood aggression and social withdrawal? Canadian
Journal of Behavioural Science, 30, 132 136.Nazzaro, P., Seccia,
T., Vulpis, V., Schirosi, G., Serio, G.,
Battistia, L., et al. (2005). Measures of total stress-induced
blood pressure responses are associated withvascular damage.
American Journal of Hypertension, 18,1226 1232.
Nelson, D. A., & Crick, N. R. (2002). Parental
psychologicalcontrol: Implications for childhood physical and
rela-tional aggression. In B. K. Barber (Ed.), Intrusive
parent-in